
The Diagnosis of Perineural Invasion: A Crucial Factor in Novel Algorithm of Coexistence of Conventional and Nerve-Sparing Radical Hysterectomy


Abstract
:1. Introduction
2. The Purpose
3. The Data Dealing with PNI in CC
3.1. Pelvic Nerve Involvement in Cervical Cancer and Other Malignancies
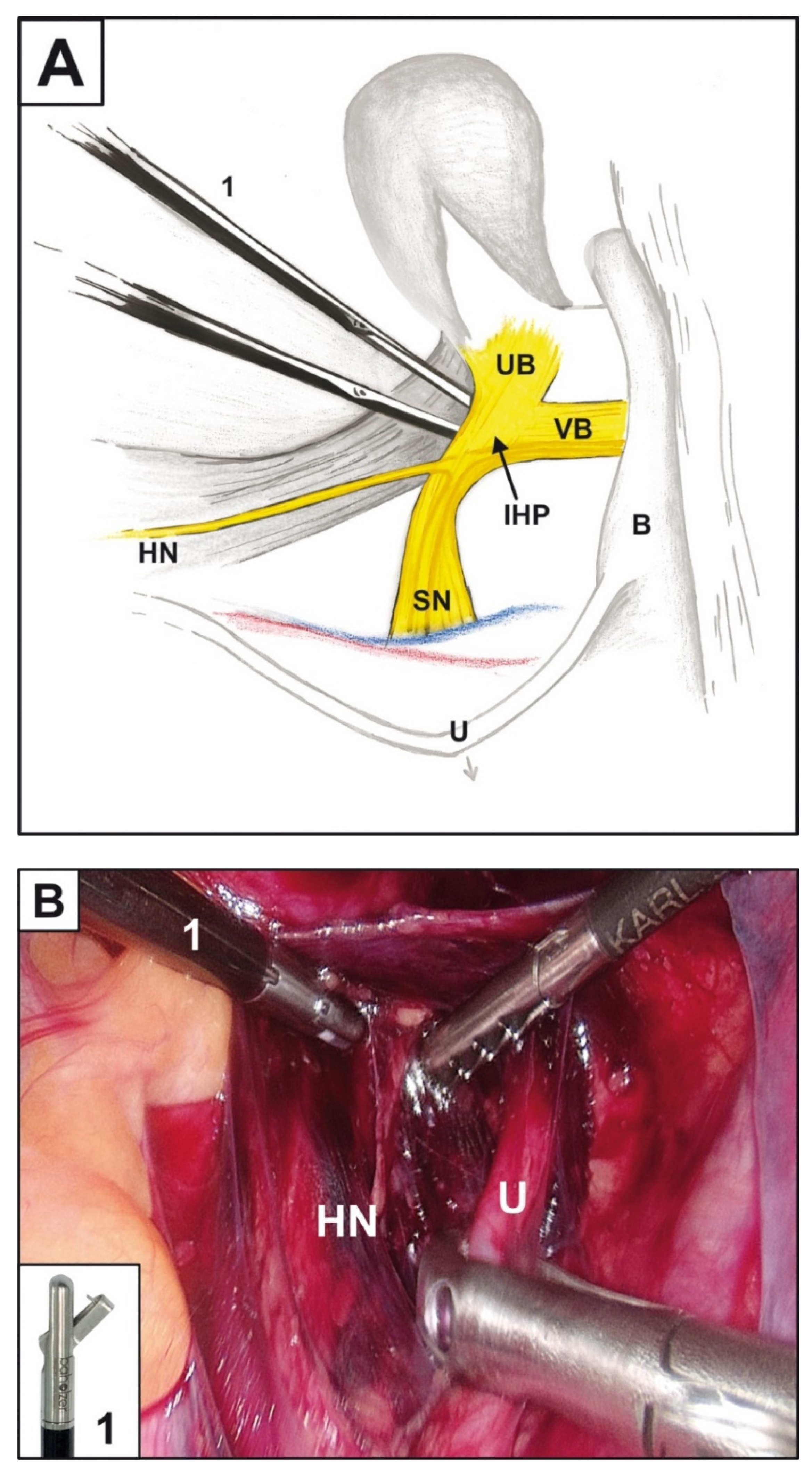
3.2. NSRH
3.3. PNI Diagnostic Methods
3.3.1. Imaging Methods
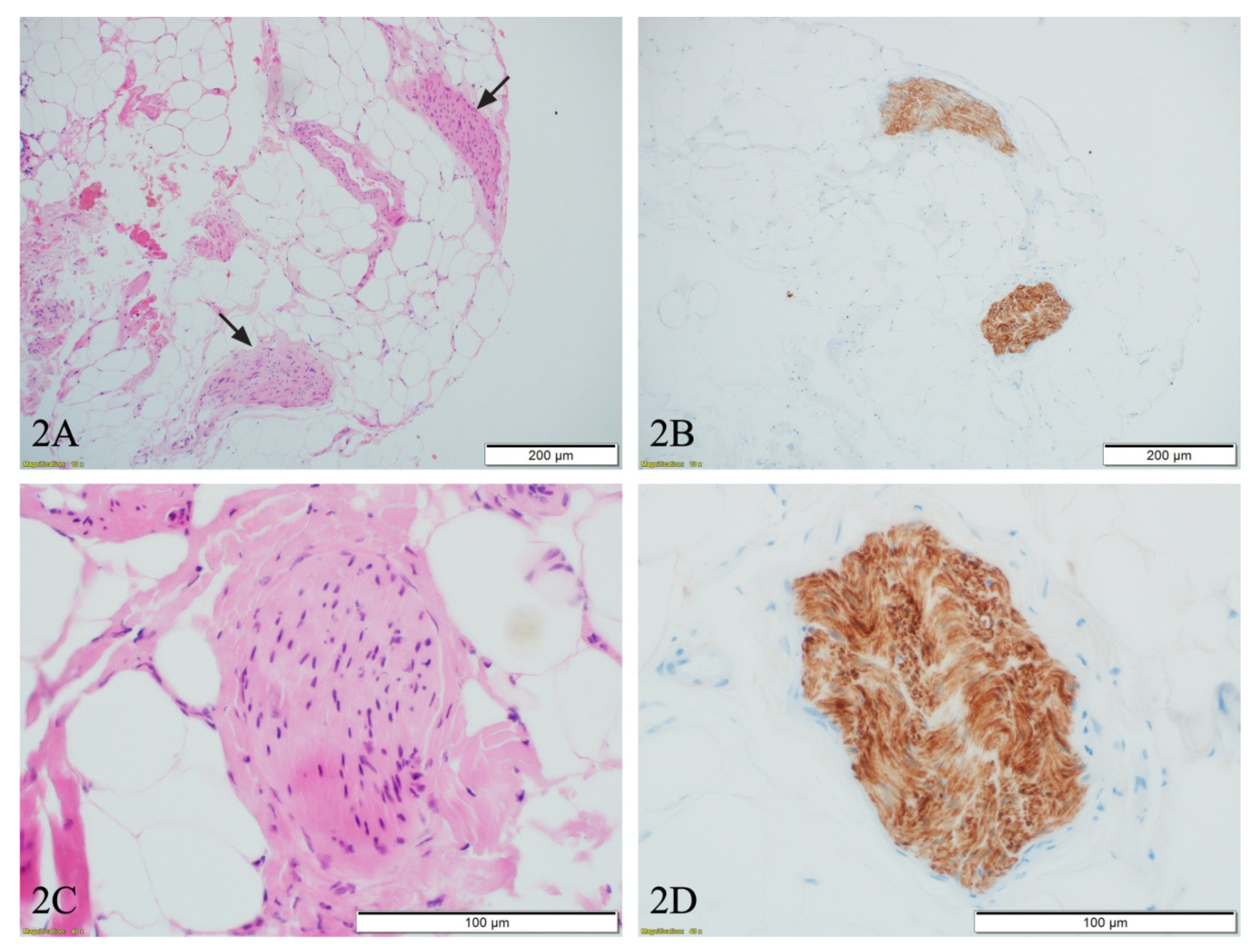
3.3.2. Biopsy
3.4. Cancer Nerve Crosstalk and Diagnostic/Therapeutic Methods Based on It
4. Oncological Outcome in Cervical Cancer Patients with PNI
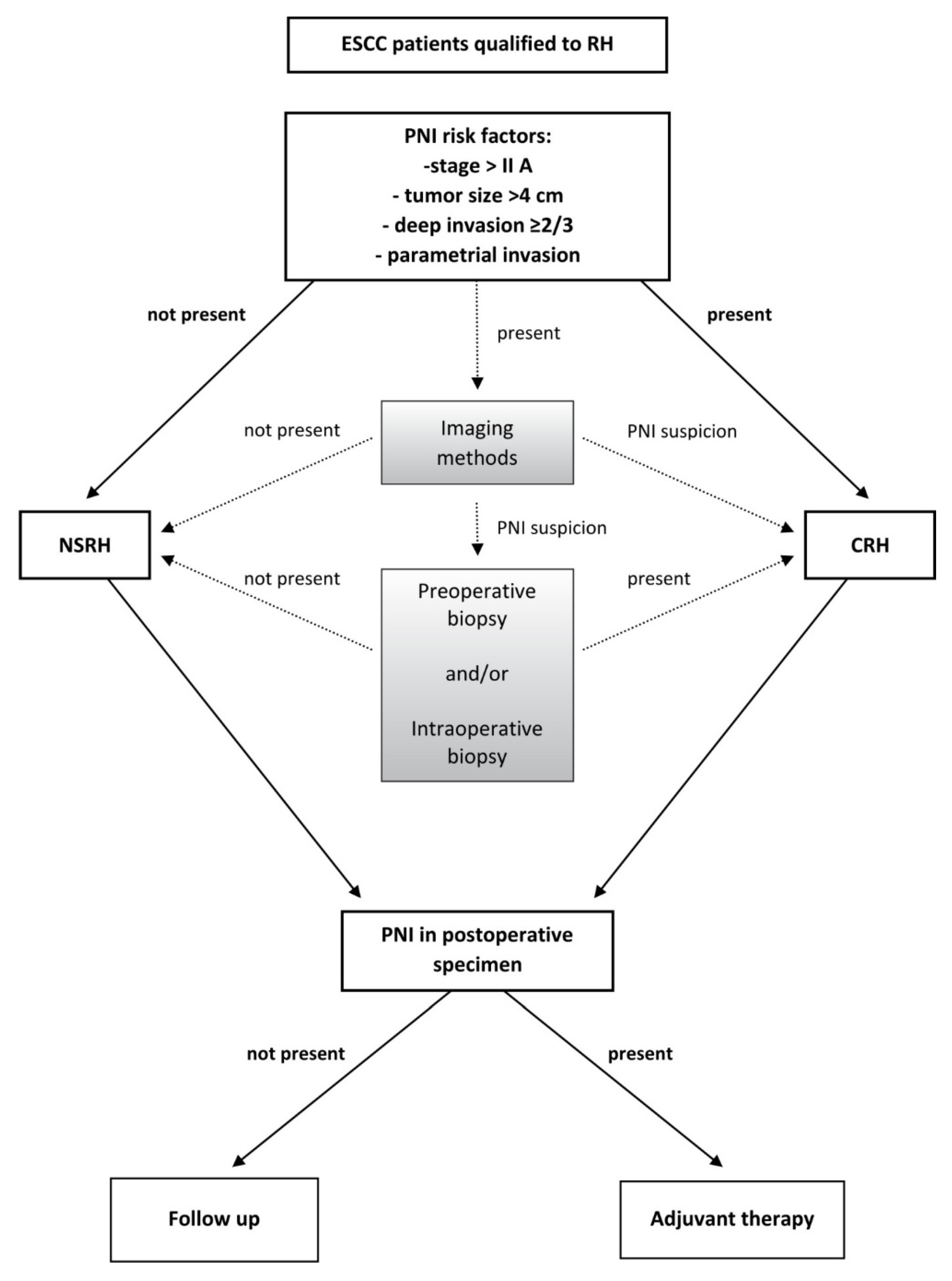
5. The PNI Diagnostic Algorithm in ESCC Patients Qualified for Surgical Treatment with RH
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- de Kroon, C.D.; Gaarenstroom, K.N.; van Poelgeest, M.I.; Peters, A.A.; Trimbos, J.B. Nerve sparing in radical surgery for early-stage cervical cancer: Yes we should! Int. J. Gynecol. Cancer 2010, 20, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, G.N.; Shi, Y.; Cui, L.; Leng, X.F.; Huang, J.M. Perineural invasion in cervical cancer: Pay attention to the indications of nerve-sparing radical hysterectomy. Ann. Transl. Med. 2019, 7, 203. [Google Scholar] [CrossRef]
- Chen, C.; Li, W.; Li, F.; Liu, P.; Zhou, J.; Lu, L.; Su, G.; Li, X.; Guo, Y.; Huang, L. Classical and nerve-sparing radical hysterectomy: An evaluation of the nerve trauma in cardinal ligament. Gynecol. Oncol. 2012, 125, 245–251. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, W.N.; Zhang, S.M.; Yang, Z.H.; Zhang, P. Effect of laparoscopic nerve-sparing radical hysterectomy on bladder function, intestinal function recovery and quality of sexual life in patients with cervical carcinoma. Asian Pac. J. Cancer Prev. 2014, 15, 10971–10975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roh, J.-W.; Lee, D.O.; Suh, D.H.; Lim, M.C.; Seo, S.-S.; Chung, J.; Lee, S.; Park, S.-Y. Efficacy and oncologic safety of nerve-sparing radical hysterectomy for cervical cancer: A randomized controlled trial. J. Gynecol. Oncol. 2015, 26, 90–99. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Liu, X.; Hua, K.; Hu, C.; Chen, X.; Lu, X. Effect of nerve sparing radical hysterectomy on bladder function recovery and quality of life in patients with cervical carcinoma. Int. J. Gynecol. Cancer 2010, 20, 905–909. [Google Scholar] [CrossRef]
- Wei, Y.S.; Yao, D.S.; Long, Y. Evaluation of the association between perineural invasion and clinical and histopathological features of cervical cancer. Mol. Clin. Oncol. 2016, 5, 307–311. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.E.; Palla, B.; Chen, Q.; Elashoff, D.A.; Abemayor, E.; St John, M.A.; Lai, C.K. A novel classification system for perineural invasion in noncutaneous head and neck squamous cell carcinoma: Histologic subcategories and patient outcomes. Am. J. Otolaryngol. 2012, 33, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, G.; Yang, Y.; Cui, L.; Jia, S.; Shi, Y.; Song, S.; Xu, S. Perineural invasion in early-stage cervical cancer and its relevance following surgery. Oncol. Lett. 2018, 15, 6555–6561. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.; Liu, Q.; Yang, X.; Chen, L.; Yu, J.; Qi, X.; Wang, Y. Perineural invasion as a prognostic risk factor in patients with early cervical cancer. Oncol. Lett. 2019, 17, 1101–1107. [Google Scholar] [CrossRef] [Green Version]
- Skręt-Magierło, J.E.; Soja, P.J.; Skręt, A.; Kruczek, A.; Kaznowska, E.; Wicherek, Ł. Perineural space invasion in cervical cancer (FIGO IB1-IIB) accompanied by high-risk factors for recurrence. J. Cancer Res. Ther. 2014, 10, 957–961. [Google Scholar] [CrossRef]
- Horn, L.C.; Meinel, A.; Fischer, U.; Bilek, K.; Hentschel, B. Perineural invasion in carcinoma of the cervix—Prognostic impact. J. Cancer Res. Clin. Oncol. 2010, 136, 1557–1562. [Google Scholar] [CrossRef]
- Meinel, A.; Fischer, U.; Bilek, K.; Hentschel, B.; Horn, L.C. Morphological parameters associated with perineural invasion (PNI) in carcinoma of the cervix uteri. Int. J. Surg. Pathol. 2011, 19, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Elsahwi, K.S.; Barber, E.; Illuzzi, J.; Buza, N.; Ratner, E.; Silasi, D.A.; Santin, A.D.; Azodi, M.; Schwartz, P.E.; Rutherford, T.J. The significance of perineural invasion in early-stage cervical cancer. Gynecol. Oncol. 2011, 123, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.C.; Kim, H.; Cho, H.Y.; Kim, K.; No, J.H.; Kim, Y.B. Prognostic significance of perineural invasion in cervical cancer. Int. J. Gynecol. Pathol. 2013, 32, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Baiocchi, G.; de Brot, L.; Faloppa, C.C.; Mantoan, H.; Duque, M.R.; Badiglian-Filho, L.; da Costa, A.B.; Kumagai, L.Y. Is parametrectomy always necessary in early-stage cervical cancer? Gynecol. Oncol. 2017, 146, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Vural, C.; Bayrak, B.Y.; Muezzınoglu, B.; Yucesoy, I. Perineural invasion is a valuable prognostic factor in advanced stage and/or node (+) cervical cancer. Indian. J. Pathol. Microbiol. 2017, 60, 27–32. [Google Scholar]
- Memarzadeh, S.; Natarajan, S.; Dandade, D.P.; Ostrzega, N.; Saber, P.A.; Busuttil, A.; Lentz, S.E.; Berek, J.S. Lymphovascular and perineural invasion in the parametria: A prognostic factor for early-stage cervical cancer. Obs. Gynecol. 2003, 102, 612–619. [Google Scholar] [CrossRef]
- Tavares, M.B.A.C.; Sousa, R.B.; Silva, T.O.; Moreira, L.A.; Silva, L.T.T.L.; Tavares, C.B.A.C.; Vieira, S.C. Prevalence of prognostic factors for cancer of the uterine cervix after radical hysterectomy. Sao Paulo Med. J. 2009, 127, 145–149. [Google Scholar] [CrossRef] [Green Version]
- Ozan, H.; Ozuysal, S.; Ediz, B. Perineural invasion in early-stage cervical carcinoma. Eur. J. Gynaecol. Oncol. 2009, 30, 379–383. [Google Scholar]
- Kato, K.; Suzuka, K.; Osaki, T.; Tanaka, N. Unilateral or bilateral nerve-sparing radical hysterectomy: A surgical technique to preserve the pelvic autonomic nerves while increasing radicality. Int. J. Gynecol. Cancer 2007, 17, 1172–1178. [Google Scholar] [CrossRef]
- Li, B.; Li, W.; Sun, Y.C.; Zhang, R.; Zhang, G.Y.; Yu, G.Z.; Wu, L.Y. Nerve plane-sparing radical hysterectomy: A simplified technique of nerve-sparing radical hysterectomy for invasive cervical cancer. Chin. Med. J. 2011, 124, 1807–1812. [Google Scholar]
- Sakuragi, N.; Murakami, G.; Konno, Y.; Kaneuchi, M.; Watari, H. Nerve-sparing radical hysterectomy in the precision surgery for cervical cancer. J. Gynecol. Oncol. 2020, 31, e49. [Google Scholar] [CrossRef] [PubMed]
- NCCN Guidelines Version 4.2019-March, 29, 2019. Cervical Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Available online: http://www.nccn.org (accessed on 2 June 2021).
- Haldorsen, I.S.; Lura, N.; Blaakær, J.; Fischerova, D.; Werner, H.M.J. What Is the Role of Imaging at Primary Diagnostic Work-Up in Uterine Cervical Cancer? Curr. Oncol. Rep. 2019, 21, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capek, S.; Howe, B.M.; Amrami, K.K.; Spinner, R.J. Perineural spread of pelvic malignancies to the lumbosacral plexus and beyond: Clinical and imaging patterns. Neurosurg. Focus 2015, 39, E14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darios, E.S.; Seitz, B.; Watts, S.W. Smooth muscle pharmacology in the isolated virgin and pregnant rat uterus and cervix. J. Pharm. Exp. 2012, 341, 587–596. [Google Scholar] [CrossRef] [Green Version]
- Cole, S.W.; Nagaraja, A.; Lutgendorf, S.K.; Green, P.; Sood, A.K. Sympathetic nervous system regulation of the tumour microenvironment. Nat. Rev. Cancer 2015, 15, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Bunimovich, Y.L.; Keskinov, A.A.; Shurin, G.V.; Shurin, M. Schwann cells: A new player in the tumor microenvironment. Cancer Immunol. Immunother. 2017, 66, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Deborde, S.; Omelchenko, T.; Lyubchik, A.; Zhou, Y.; He, S.; McNamara, W.F.; Chernichenko, N.; Lee, S.-Y.; Barajas, F.; Chen, C.-H.; et al. Schwann cells induce cancer cell dispersion and invasion. J. Clin. Investig. 2016, 126, 1538–1554. [Google Scholar] [CrossRef] [Green Version]
- Demir, I.E.; Boldis, A.; Pfitzinger, P.L.; Teller, S.; Brunner, E.; Klose, N.; Kehl, T.; Maak, M.; Lesina, M.; Laschinger, M.; et al. Investigation of Schwann cells at neoplastic cell sites before the onset of cancer invasion. J. Natl. Cancer Inst. 2014. [Google Scholar] [CrossRef] [Green Version]
- Azam, S.H.; Pecot, C.V. Cancer’s got nerve: Schwann cells drive perineural invasion. J. Clin. Investig. 2016, 126, 1242–1244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lolas, G.; Bianchi, A.; Syrigos, K.N. Tumour-induced neoneurogenesis and perineural tumour growth:a mathematical approach. Sci. Rep. 2016, 6, 20684. [Google Scholar] [CrossRef] [PubMed]
- Prueitt, R.L.; Yi, M.; Hudson, R.S.; Wallace, T.A.; Howe, T.M.; Yfantis, H.G.; Lee, D.H.; Stephens, R.M.; Liu, C.G.; Calin, G.A.; et al. Expression of microRNAs and protein-coding genes associated with perineural invasion in prostate cancer. Prostate 2008, 68, 1152–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchesi, F.; Piemonti, L.; Fedele, G.; Destro, A.; Roncalli, M.; Albarello, L.; Doglioni, C.; Anselmo, A.; Doni, A.; Bianchi, P.; et al. The chemokine receptor CX3CR1 is involved in the neural tropism and malignant behavior of pancreatic ductal adenocarcinoma. Cancer Res. 2008, 68, 9060–9069. [Google Scholar] [CrossRef] [Green Version]
- Prueitt, R.L.; Yi, M.; Hudson, R.S.; Wallace, T.A.; Howe, T.M.; Yfantis, H.G.; Ambs, S. Hematopoietic colony-stimulating factors mediate tumor-nerve interactions and bone cancer pain. Nat. Med. 2009, 15, 802–807. [Google Scholar]
- Zhang, M.; Zhu, Z.L.; Gao, X.L.; Wu, J.S.; Liang, X.H.; Tang, Y.L. Functions of chemokines in the perineural invasion of tumors (Review). Int. J. Oncol. 2018, 52, 1369–1379. [Google Scholar] [CrossRef]
- Abbadie, C. Chemokines, chemokine receptors and pain. Trends Immunol. 2005, 26, 529–534. [Google Scholar] [CrossRef]
- Sommer, C.; Kress, M. Recent findings on how proinflammatory cytokines cause pain: Peripheral mechanisms in inflammatory and neuropathic hyperalgesia. Neurosci. Lett. 2004, 361, 184–187. [Google Scholar] [CrossRef]
- Charo, I.F.; Ransohoff, R.M. The many roles of chemokines and chemokine receptors in inflammation. N. Engl. J. Med. 2006, 354, 610–621. [Google Scholar] [CrossRef]
- Sevin, B.-U.; Lu, Y.; Bloch, D.A.; Nadji, M.; Koechli, O.R.; Averette, H.E. Surgically defined prognostic parameters in patients with early cervical carcinoma. A multivariate survival tree analysis. Cancer 1996, 78, 1438–1446. [Google Scholar] [CrossRef]
- Buda, A.; Fossati, R.; Colombo, N.; Fei, F.; Floriani, I.; Alletti, D.G.; Katsaros, D.; Landoni, F.; Lissoni, A.; Malzoni, C.; et al. Randomized trial of neoadjuvant chemotherapy comparing paclitaxel, ifosfamide, and cisplatin with ifosfamide and cisplatin followed by radical surgery in patients with locally advanced squamous cell cervical carcinoma: The SNAP01 (Studio Neo-Adjuvante Portio) Italian Collaborative Study. J. Clin. Oncol. 2005, 23, 4137–4145. [Google Scholar] [PubMed]
- Vizza, E.; Pellegrino, A.; Milani, R.; Fruscio, R.; Baiocco, E.; Cognetti, F.; Savarese, A.; Tomao, F.; Chen, C.; Corrado, G. Total laparoscopic radical hysterectomy and pelvic lymphadenectomy in locally advanced stage IB2-IIB cervical cancer patients after neoadjuvant chemotherapy. Eur. J. Surg. Oncol. 2011, 37, 364–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitd, L.B.; Beesley, L.; Russo, N.; Bellile, E.L.; Inglehart, R.C.; Liu, M.; Romanowicz, G.; Wolf, G.T.; Taylor, J.M.; D’Silva, N.J. Redefining perineural invasion: Integration of biology with clinical outcome. Neoplasia 2018, 20, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Gil, Z.; Kelly, K.J.; Brader, P.; Shah, J.P.; Fong, Y.; Wong, R.J. Utility of a herpes oncolytic virus for the detection of neural invasion by cancer. Neoplasia 2008, 10, 347–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Authors, Years, References | Samples/ with PNI (N) | Localization of PNI | Frequency of PNI (%) | Stage | Grade | Tumor Size with PNI | Depth of Invasion with PNI |
|---|---|---|---|---|---|---|---|
| Wei et al., 2016 [7] | 206/33 | Cervix n = 28, Cervix and parametrium n = 5 | 16 | IB1-B | G1-3 | <4 cm n = 16 >4 cm n = 17 | <1/2 n = 6 >1/2 n = 27 |
| Zhu et al., 2018 [9] | 201/18 | Cervix n = 15 Cervix and parametrium n = 3 | 8.57 | IA2-IIA2 | N/A | <4 cm n = 5 >4 cm n = 13 | <2/3 n = 2 >2/3 n = 16 |
| Tang et al., 2019 [10] | 406/43 | Cervix n = 43 | 10.59 | IA2-IIA1 | N/A | <4 cm n = 27 >4 cm n = 16 | <2/3 n = 6 >2/3 n = 37 |
| Skręt-Magierło et al., 2014 [11] | 50/9 | Parametria n = 9 | 18 | IB1-IIB | G1-G3 | <4 cm n = 3 >4 cm n = 6 | <15 mm n = 1 >15 mm n = 8 |
| Horn et al., 2010 [12] | 194/68 | Cervix | 35.1 | IB1-IIB | G1-G3 | N/A | N/A |
| Meinel et al., 2011 [13] | 194/68 | cervix | 35.1 | IB1-IIB | G1-G3 | N/A | <66% n = 67 >66% n = 126 |
| Elshawi et al., 2011 [14] | 190/24 | Cervical stroma n = 24 | 12.5 | IB1-IIA | G1-G3 | >4 cm n = 10 <4 cm n = 14 | >2/3 n = 18 <2/3 n = 6 |
| Cho et al., 2013 [15] | 185/13 | Cervix n =13 Parametrium n = 8 | 7 | IA2-IIA2 | N/A | <4 cm n = 6 >4 cm n = 7 | <1/3 n = 2 >1/3 n = 11 |
| Baiocchi et al., 2017 [16] | 345/16 | Cervix n = 42 Parametrium n = 16 | 4.6 | IA2-IB2 | G1-G3 | N/A | N/A |
| Vural et al., 2017 [17] | 111/ 34 | Parametrium n = 26 | IIA-IIB | N/A | <4 cm n = 15 >4 cm n = 19 | <2/3 n = 1 >2/3 n = 33 | |
| Memarzadeh et al., 2003 [18] | 93 | Parametrium | 7.5 | IA2-IIA | N/A | N/A | N/A |
| Tavares et al., 2009 [19] | 301 | Cervix | 27 | I-II | N/A | N/A | N/A |
| Ozan et al., 2008 [20] | 36 | N/A | 33 | IB1-IB2 | N/A | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skręt, A.; Skręt-Magierło, J.E.; Książek, M.; Gawlik, B.; Bielatowicz, J.; Barnaś, E. The Diagnosis of Perineural Invasion: A Crucial Factor in Novel Algorithm of Coexistence of Conventional and Nerve-Sparing Radical Hysterectomy. Diagnostics 2021, 11, 1308. https://doi.org/10.3390/diagnostics11081308
Skręt A, Skręt-Magierło JE, Książek M, Gawlik B, Bielatowicz J, Barnaś E. The Diagnosis of Perineural Invasion: A Crucial Factor in Novel Algorithm of Coexistence of Conventional and Nerve-Sparing Radical Hysterectomy. Diagnostics. 2021; 11(8):1308. https://doi.org/10.3390/diagnostics11081308
Chicago/Turabian StyleSkręt, Andrzej, Joanna Ewa Skręt-Magierło, Mariusz Książek, Bogusław Gawlik, Joanna Bielatowicz, and Edyta Barnaś. 2021. "The Diagnosis of Perineural Invasion: A Crucial Factor in Novel Algorithm of Coexistence of Conventional and Nerve-Sparing Radical Hysterectomy" Diagnostics 11, no. 8: 1308. https://doi.org/10.3390/diagnostics11081308