
A High-Accuracy Model Based on Plasma miRNAs Diagnoses Intrahepatic Cholangiocarcinoma: A Single Center with 1001 Samples

 and
and
Abstract
:1. Introduction
2. Patients and Methods
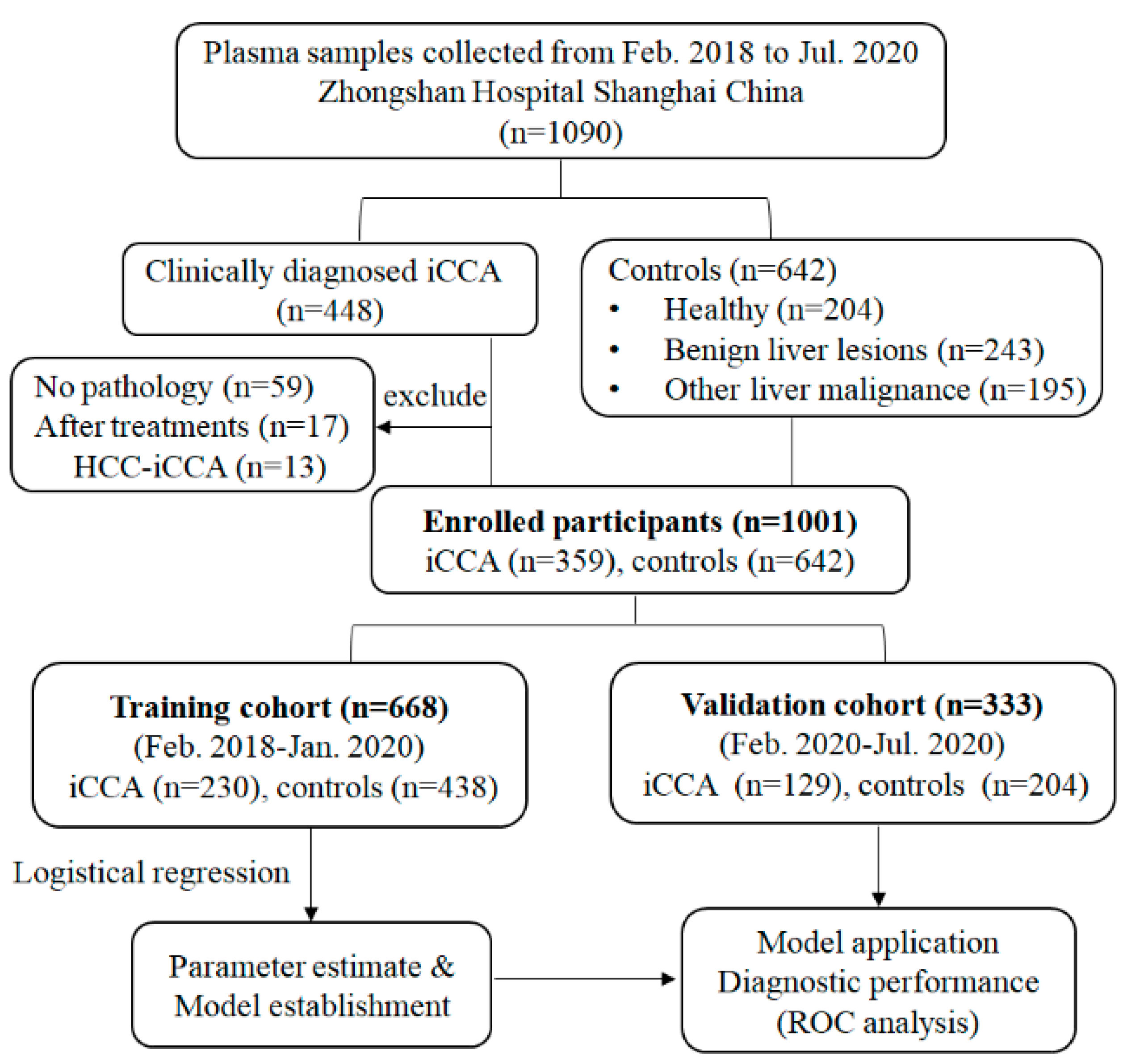
2.1. Study Design and Patients
2.2. Quantification of Plasma miR-21 and miR-122
2.3. Model Construction and Validation
2.4. Statistical Analysis
2.5. Target Gene Prediction and Enrichment Analysis
3. Results
3.1. Patient Characteristics
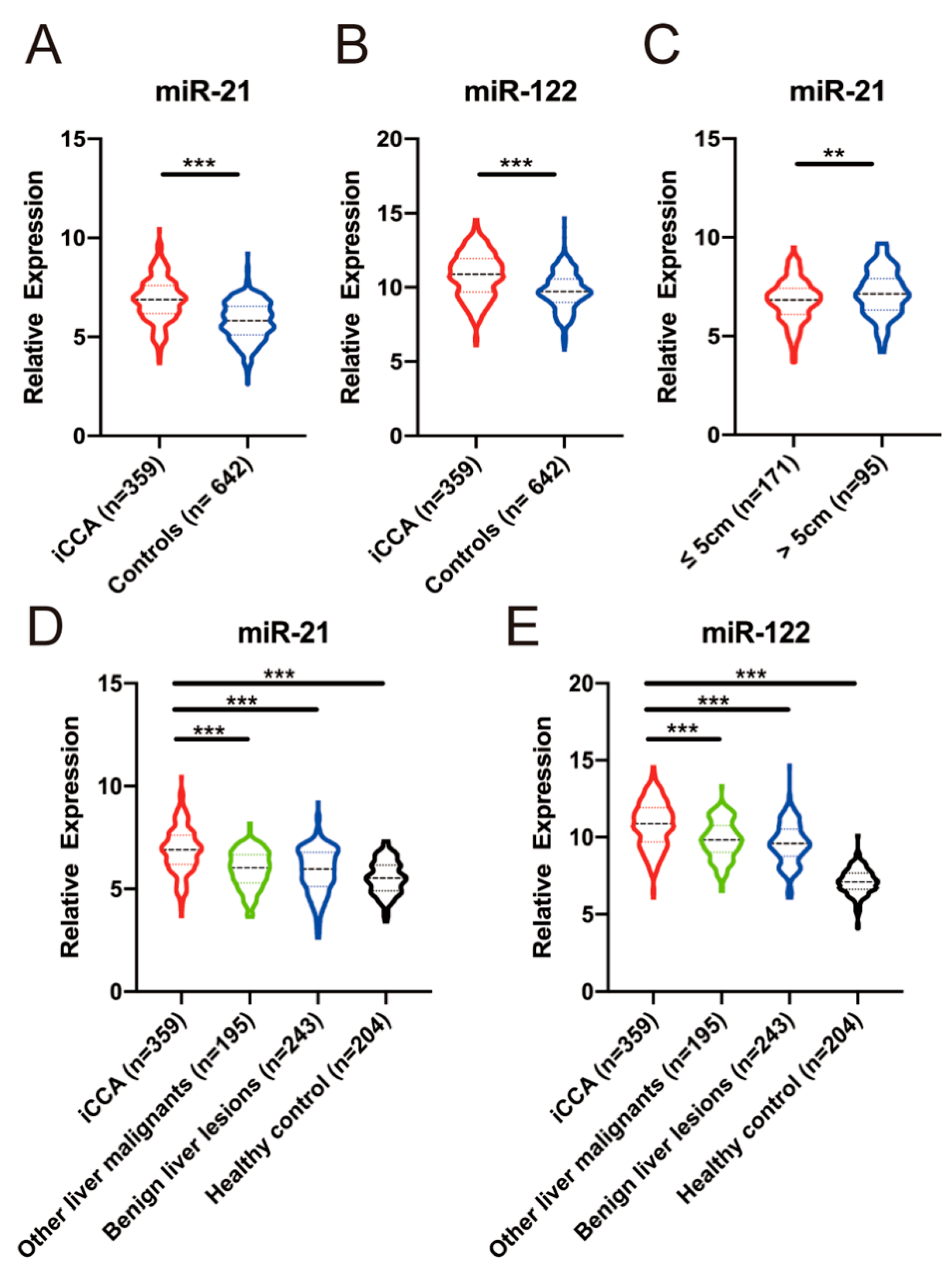
3.2. The Expression of Plasma miR-21 and miR-122
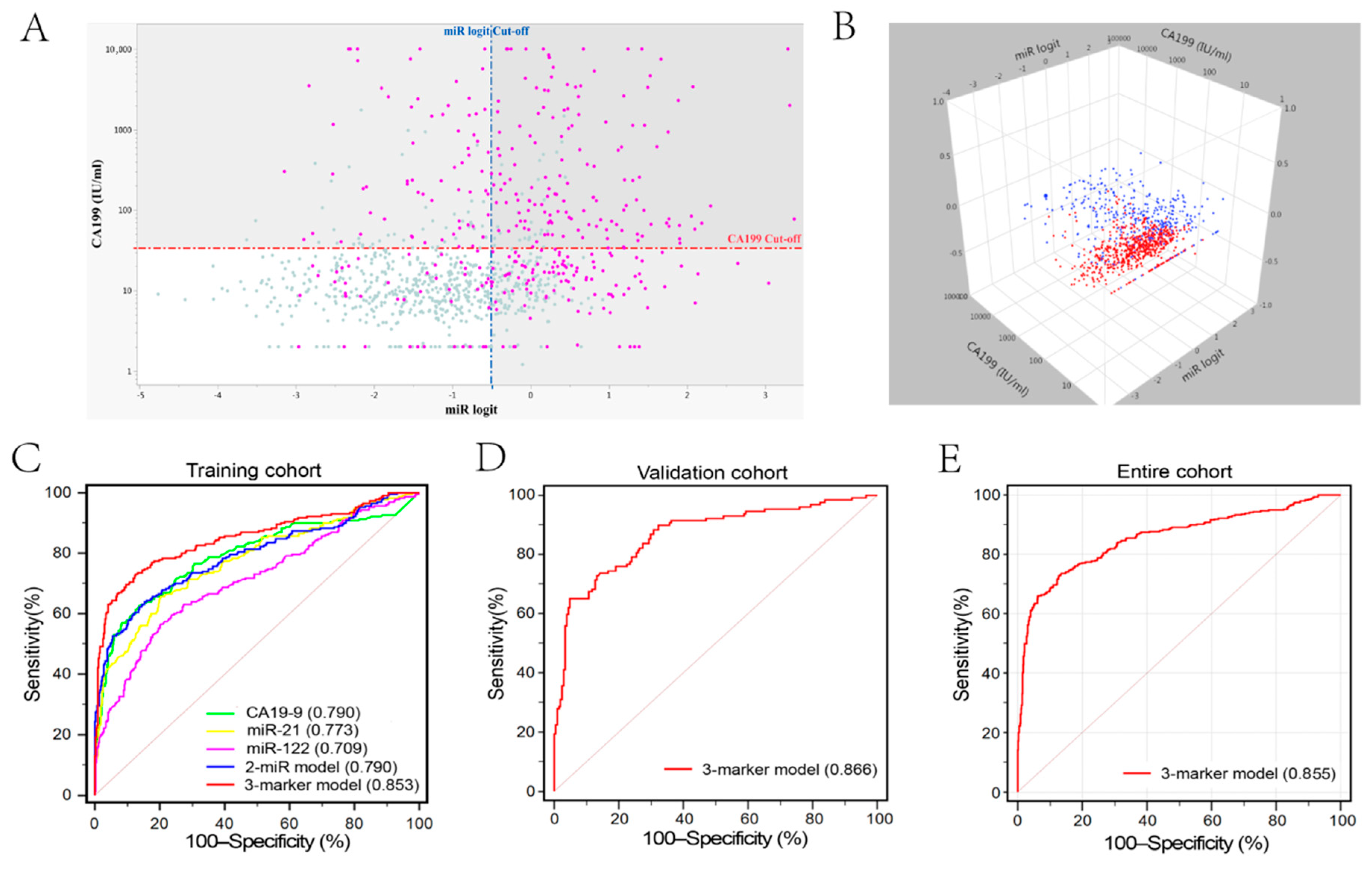
3.3. Model Construction in Training Cohort
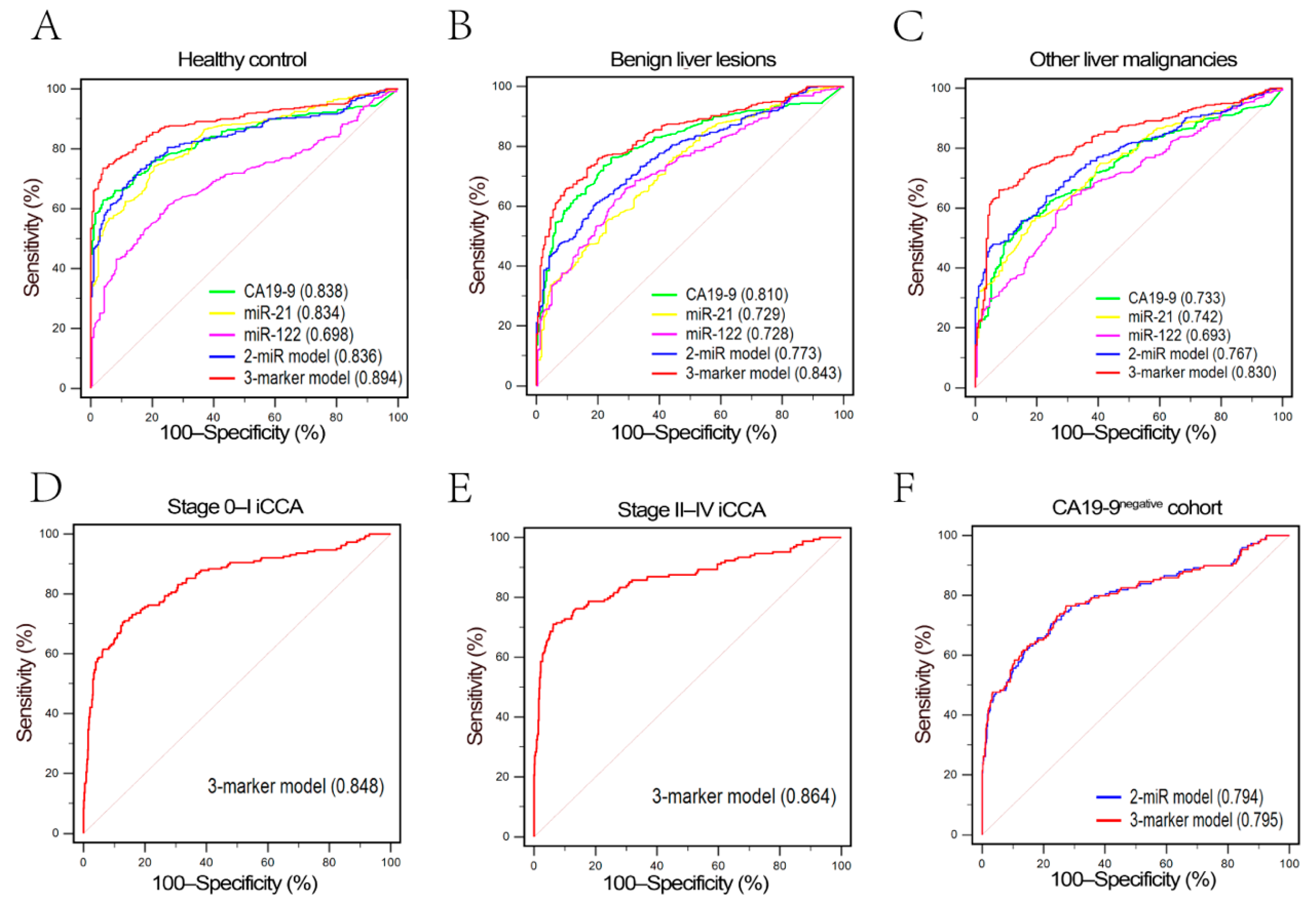
3.4. Model Validation
3.5. Function Prediction of miR21 and miR-122
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sirica, A.E.; Gores, G.J.; Groopman, J.D.; Selaru, F.M.; Strazzabosco, M.; Wang, X.W.; Zhu, A.X. Intrahepatic Cholangiocarcinoma: Continuing Challenges and Translational Advances. Hepatology 2019, 69, 1803–1815. [Google Scholar] [CrossRef]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef]
- Bertuccio, P.; Malvezzi, M.; Carioli, G.; Hashim, D.; Boffetta, P.; El-Serag, H.B.; La Vecchia, C.; Negri, E. Global trends in mortality from intrahepatic and extrahepatic cholangiocarcinoma. J. Hepatol. 2019, 71, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Mavros, M.N.; Economopoulos, K.P.; Alexiou, V.G.; Pawlik, T.M. Treatment and Prognosis for Patients With Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-analysis. JAMA Surg. 2014, 149, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Wirth, T.C.; Vogel, A. Surveillance in cholangiocellular carcinoma. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 987–999. [Google Scholar] [CrossRef]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.S.; Javle, M. Systemic and Adjuvant Therapies for Intrahepatic Cholangiocarcinoma. Cancer Control. 2017, 24, 1073274817729241. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wang, Z.; Liao, B.-Y.; Yu, L.; Gao, X.; Lu, S.; Wang, S.; Dai, Z.; Zhang, X.; Chen, Q.; et al. Human miR-1228 as a stable endogenous control for the quantification of circulating microRNAs in cancer patients. Int. J. Cancer 2014, 135, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.; Gores, G.J. Pathogenesis, diagnosis, and management of cholangiocarcinoma. Gastroenterology 2013, 145, 1215–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, L.; Zhang, L.; Gong, Z.; Hou, X.; Xu, Y.; Feng, X.; Wang, H.; You, H. FoxO3 inactivation promotes human cholangiocarcinoma tumorigenesis and chemoresistance through Keap1-Nrf2 signaling. Hepatology 2016, 63, 1914–1927. [Google Scholar] [CrossRef] [Green Version]
- Zou, S.; Li, J.; Zhou, H.; Frech, C.; Jiang, X.; Chu, J.S.C.; Zhao, X.; Li, Y.; Li, Q.; Wang, H.; et al. Mutational landscape of intrahepatic cholangiocarcinoma. Nat. Commun. 2014, 5, 5696. [Google Scholar] [CrossRef]
- Jusakul, A.; Cutcutache, I.; Yong, C.H.; Lim, J.Q.; Ni Huang, M.; Padmanabhan, N.; Nellore, V.; Kongpetch, S.; Ng, A.W.T.; Ng, L.M.; et al. Whole-Genome and Epigenomic Landscapes of Etiologically Distinct Subtypes of Cholangiocarcinoma. Cancer Discov. 2017, 7, 1116–1135. [Google Scholar] [CrossRef] [Green Version]
- Tiemin, P.; Fanzheng, M.; Peng, X.; Jihua, H.; Ruipeng, S.; Yaliang, L.; Yan, W.; Junlin, X.; Qingfu, L.; Zhefeng, H.; et al. MUC13 promotes intrahepatic cholangiocarcinoma progression via EGFR/PI3K/AKT pathways. J. Hepatol. 2020, 72, 761–773. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Shi, L.; Shen, X.; Zhao, Y. UCP2 regulates cholangiocarcinoma cell plasticity via mitochondria-to-AMPK signals. Biochem. Pharmacol. 2019, 166, 174–184. [Google Scholar] [CrossRef]
- Papoutsoglou, P.; Louis, C.; Coulouarn, C. Transforming Growth Factor-Beta (TGFbeta) Signaling Pathway in Cholangiocarcinoma. Cells 2019, 8, 960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sia, D.; Villanueva, A.; Friedman, S.L.; Llovet, J.M. Liver Cancer Cell of Origin, Molecular Class, and Effects on Patient Prognosis. Gastroenterology 2017, 152, 745–761. [Google Scholar] [CrossRef] [Green Version]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control. 2017, 24, 1073274817729245. [Google Scholar] [CrossRef] [PubMed]
- Beyoglu, D.; Idle, J.R. The metabolomic window into hepatobiliary disease. J. Hepatol. 2013, 59, 842–858. [Google Scholar] [CrossRef] [Green Version]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.-W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [Green Version]
- Loosen, S.H.; Vucur, M.; Trautwein, C.; Roderburg, C.; Luedde, T. Circulating Biomarkers for Cholangiocarcinoma. Dig. Dis. 2018, 36, 281–288. [Google Scholar] [CrossRef]
- Puik, J.R.; Meijer, L.L.; Le Large, T.Y.S.; Prado, M.M.; Frampton, A.E.; Kazemier, G.; Giovannetti, E. miRNA profiling for diagnosis, prognosis and stratification of cancer treatment in cholangiocarcinoma. Pharmacogenomics 2017, 18, 1343–1358. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Nishida, N.; Calin, G.A.; Pantel, K. Clinical relevance of circulating cell-free microRNAs in cancer. Nat. Rev. Clin. Oncol. 2014, 11, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Schwarzenbach, H. Clinical Relevance of Circulating, Cell-Free and Exosomal microRNAs in Plasma and Serum of Breast Cancer Patients. Oncol. Res. Treat. 2017, 40, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Byrnes, K.; Han, C.; Wang, Y.; Wu, T. miR-21 targets 15-PGDH and promotes cholangiocarcinoma growth. Mol. Cancer Res. 2014, 12, 890–900. [Google Scholar] [CrossRef] [Green Version]
- Meng, F.; Henson, R.; Lang, M.; Wehbe, H.; Maheshwari, S.; Mendell, J.T.; Jiang, J.; Schmittgen, T.D.; Patel, T. Involvement of human micro-RNA in growth and response to chemotherapy in human cholangiocarcinoma cell lines. Gastroenterology 2006, 130, 2113–2129. [Google Scholar] [CrossRef] [Green Version]
- Correa-Gallego, C.; Maddalo, D.; Doussot, A.; Kemeny, N.; Kingham, T.P.; Allen, P.J.; D’Angelica, M.I.; DeMatteo, R.P.; Betel, D.; Klimstra, D.; et al. Circulating Plasma Levels of MicroRNA-21 and MicroRNA-221 Are Potential Diagnostic Markers for Primary Intrahepatic Cholangiocarcinoma. PLoS ONE 2016, 11, e0163699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Yang, Z.-S.; Zhou, Y.-Z.; Deng, Y.; Jiang, P.; Tan, S.-L. Dihydromyricetin inhibits cell proliferation, migration, invasion and promotes apoptosis via regulating miR-21 in Human Cholangiocarcinoma Cells. J. Cancer 2020, 11, 5689–5699. [Google Scholar] [CrossRef]
- Zou, Y.; Li, R.; Kuang, D.; Zuo, M.; Li, W.; Tong, W.; Jiang, L.; Zhou, M.; Chen, Y.; Gong, W.; et al. Galangin Inhibits Cholangiocarcinoma Cell Growth and Metastasis through Downregulation of MicroRNA-21 Expression. Biomed. Res. Int. 2020, 2020, 5846938. [Google Scholar] [CrossRef]
- Selaru, F.M.; Olaru, A.V.; Kan, T.; David, S.; Cheng, Y.; Mori, Y.; Yang, J.; Paun, B.; Jin, Z.; Agarwal, R.; et al. MicroRNA-21 is overexpressed in human cholangiocarcinoma and regulates programmed cell death 4 and tissue inhibitor of metalloproteinase 3. Hepatology 2009, 49, 1595–1601. [Google Scholar] [CrossRef]
- Liu, Z.; Jin, Z.-Y.; Liu, C.-H.; Xie, F.; Lin, X.-S.; Huang, Q. MicroRNA-21 regulates biological behavior by inducing EMT in human cholangiocarcinoma. Int. J. Clin. Exp. Pathol. 2015, 8, 4684–4694. [Google Scholar]
- Liu, N.; Jiang, F.; He, T.-L.; Zhang, J.-K.; Zhao, J.; Wang, C.; Jiang, G.-X.; Cao, L.-P.; Kang, P.-C.; Zhong, X.-Y.; et al. The Roles of MicroRNA-122 Overexpression in Inhibiting Proliferation and Invasion and Stimulating Apoptosis of Human Cholangiocarcinoma Cells. Sci. Rep. 2015, 5, 16566. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Zhang, J.; Cao, X.; Yang, Q.; Xia, D. Effect of Mir-122 on Human Cholangiocarcinoma Proliferation, Invasion, and Apoptosis Through P53 Expression. Med. Sci. Monit. 2016, 22, 2685–2690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Z.; Liu, G.; Zhang, M.; Zhang, Z.; Jia, Y.; Peng, L.; Zhu, Y.; Hu, J.; Huang, R.; Sun, X. miR-122-5p Inhibits the Proliferation, Invasion and Growth of Bile Duct Carcinoma Cells by Targeting ALDOA. Cell Physiol. Biochem. 2018, 48, 2596–2606. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Lurje, G.; Wiltberger, G.; Vucur, M.; Koch, A.; Kather, J.N.; Paffenholz, P.; Tacke, F.; Ulmer, F.T.; Trautwein, C.; et al. Serum levels of miR-29, miR-122, miR-155 and miR-192 are elevated in patients with cholangiocarcinoma. PLoS ONE 2019, 14, e0210944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, J.; Wang, Z.; Tan, C.-J.; Liao, B.-Y.; Zhang, X.; Xu, M.; Dai, Z.; Qiu, S.-J.; Huang, X.-W.; Sun, J.; et al. Plasma microRNA, a potential biomarker for acute rejection after liver transplantation. Transplantation 2013, 95, 991–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishimoto, T.; Eguchi, H.; Nagano, H.; Kobayashi, S.; Akita, H.; Hama, N.; Wada, H.; Kawamoto, K.; Tomokuni, A.; Tomimaru, Y.; et al. Plasma miR-21 is a novel diagnostic biomarker for biliary tract cancer. Cancer Sci. 2013, 104, 1626–1631. [Google Scholar] [CrossRef]
- Wang, L.-J.; Zhang, K.-L.; Zhang, N.; Ma, X.-W.; Yan, S.-W.; Cao, D.-H.; Shi, S.-J. Serum miR-26a as a diagnostic and prognostic biomarker in cholangiocarcinoma. Oncotarget 2015, 6, 18631–18640. [Google Scholar] [CrossRef] [Green Version]
- Bernuzzi, F.; Marabita, F.; Lleo, A.; Carbone, M.; Mirolo, M.; Marzioni, M.; Alpini, G.; Alvaro, D.; Boberg, K.M.; Locati, M.; et al. Serum microRNAs as novel biomarkers for primary sclerosing cholangitis and cholangiocarcinoma. Clin. Exp. Immunol. 2016, 185, 61–71. [Google Scholar] [CrossRef] [Green Version]
- Voigtländer, T.; Gupta, S.K.; Thum, S.; Fendrich, J.; Manns, M.P.; Lankisch, T.O.; Thum, T. MicroRNAs in Serum and Bile of Patients with Primary Sclerosing Cholangitis and/or Cholangiocarcinoma. PLoS ONE 2015, 10, e0139305. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Yin, J.; Li, T.; Yuan, L.; Wang, N.; He, J.; Du, X.; Lu, J. Upregulated circulating miR-150 is associated with the risk of intrahepatic cholangiocarcinoma. Oncol. Rep. 2015, 33, 819–825. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | iCCA Cohort | ||
|---|---|---|---|
| Total iCCA (n = 359) | Radical Surgery (n = 266) | Liver Biopsy (n = 93) | |
| Age > 60 yrs | 215 (59.9%) | 158 (59.4%) | 57 (61.3%) |
| Male | 218 (60.7) | 160 (60.2%) | 58 (62.4%) |
| Diagnosed by specimen after | |||
| Radical surgery | 266 (74.1%) | 266 (100.0%) | − |
| Liver resection | 261 (72.7%) | 261 (98.1%) | − |
| Liver transplantation | 5 (1.4%) | 5 (1.9%) | − |
| Liver biopsy | 93 (25.9%) | − | 93 (100.0%) |
| Serum tumor biomarker, median (range) | |||
| CA19-9 (IU/mL) | 57.2 (2.0–10,000.0) | 40.4 (2.0–10,000.0) | 339.0 (2.0–10,000.0) |
| AFP (ng/mL) | 2.9 (0.9–19,998) | 2.9 (0.9–19,998) | 3.0 (0.9–1115.0) |
| Tumor characteristics | |||
| Tumor size (cm) | 5.44 (±2.96) | 4.87 (±2.78) | 7.09 (±2.90) |
| Multiple | 73 (20.3%) | 50 (18.8%) | 23 (24.7%) |
| Capsular invasion | − | 179 (67.3%) | − |
| Perineural invasion | − | 69 (25.9%) | − |
| MVI | − | 75 (28.2%) | − |
| AJCC Stage II–IV | 169 (47.1%) | 93 (35.0%) | 76 (81.7%) |
| Lymphatic metastasis | − | 42 (15.8%) | − |
| Characteristics | iCCA Patients Receiving Radical Surgery (n = 266) | |||||
|---|---|---|---|---|---|---|
| Plasma miR-21 | Plasma miR-122 | |||||
| Low (n = 133) | High (n = 133) | p | Low (n = 133) | High (n = 133) | p | |
| Tumor size, cm | 0.030 | 0.096 | ||||
| ≤5 cm | 94 | 77 | 79 | 92 | ||
| >5 cm | 39 | 56 | 54 | 41 | ||
| Tumor number | 0.754 | 1.000 | ||||
| Single | 107 | 109 | 108 | 108 | ||
| Multiple | 26 | 24 | 25 | 25 | ||
| Capsular invasion | ||||||
| No | 39 | 48 | 36 | 51 | ||
| Yes | 94 | 85 | 97 | 82 | ||
| Microvascular invasion | 0.496 | 0.683 | ||||
| No | 98 | 93 | 97 | 94 | ||
| Yes | 35 | 40 | 36 | 39 | ||
| Perineural invasion | ||||||
| No | 98 | 99 | 101 | 96 | ||
| Yes | 35 | 34 | 32 | 37 | ||
| Lymphatic metastasis | ||||||
| No | 112 | 112 | 107 | 117 | ||
| Yes | 21 | 21 | 26 | 16 | ||
| CA19-9 level, IU/mL | ||||||
| ≤ 34 | 63 | 63 | 64 | 62 | ||
| > 34 | 70 | 70 | 69 | 71 | ||
| AJCC Stage | 0.898 | 0.247 | ||||
| 0−I | 87 | 86 | 82 | 91 | ||
| II−III | 46 | 47 | 51 | 42 | ||
| Markers | iCCA vs. Control | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Training Cohort | Validation Cohort | |||||||||||
| AUC (95% CI) | NPV (%) | PPV (%) | Sensitivity (%) | Specificity (%) | p | AUC (95% CI) | NPV (%) | PPV (%) | Sensitivity (%) | Specificity (%) | p | |
| CA19-9 | 0.790 (0.757–0.820) | 72.1 | 87.7 | 62.6 | 86.3 | <0.001 | 0.805 (0.759–0.846) | 68.8 | 86.7 | 62.8 | 86.8 | <0.001 |
| miR-21 | 0.773 (0.740–0.805) | 77.3 | 71.0 | 65.7 | 79.7 | <0.001 | 0.785 (0.737–0.828) | 72.5 | 65.0 | 72.9 | 70.6 | <0.001 |
| miR-122 | 0.709 (0.673–0.744) | 73.7 | 65.5 | 56.5 | 70.7 | <0.001 | 0.707 (0.655–0.755) | 71.6 | 69.9 | 53.5 | 80.9 | <0.001 |
| 2-miR model * | 0.790 (0.757–0.820) | 80.1 | 73.9 | 63.9 | 84.7 | <0.001 | 0.801 (0.754–0.842) | 75.8 | 69.8 | 81.4 | 69.6 | <0.001 |
| 3-marker model # | 0.853 (0.824–0.879) | 83.3 | 86.5 | 73.0 | 87.4 | <0.001 | 0.866 (0.825–0.901) | 81.0 | 87.5 | 65.1 | 95.1 | <0.001 |
| Markers | iCCA Cohort with Negative CA19-9 (n = 149) vs. Control (n = 571) | |||||
|---|---|---|---|---|---|---|
| AUC (95% CI) | NPV (%) | PPV (%) | Sensitivity (%) | Specificity (%) | p | |
| miR-21 | 0.771 (0.739–0.802) | 83.4 | 80.4 | 77.2 | 65.8 | <0.001 |
| miR-122 | 0.712 (0.677–0.725) | 81.8 | 82.1 | 63.8 | 74.1 | <0.001 |
| 2-miR model * | 0.794 (0.762–0.823) | 85.5 | 84.4 | 70.5 | 77.6 | <0.001 |
| 3-marker model # | 0.795 (0.763–0.824) | 85.9 | 85.1 | 76.5 | 72.7 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, J.; Wang, Y.-N.; Song, D.-J.; Tan, J.-P.; Cao, Y.; Fan, J.; Wang, Z.; Zhou, J. A High-Accuracy Model Based on Plasma miRNAs Diagnoses Intrahepatic Cholangiocarcinoma: A Single Center with 1001 Samples. Diagnostics 2021, 11, 610. https://doi.org/10.3390/diagnostics11040610
Hu J, Wang Y-N, Song D-J, Tan J-P, Cao Y, Fan J, Wang Z, Zhou J. A High-Accuracy Model Based on Plasma miRNAs Diagnoses Intrahepatic Cholangiocarcinoma: A Single Center with 1001 Samples. Diagnostics. 2021; 11(4):610. https://doi.org/10.3390/diagnostics11040610
Chicago/Turabian StyleHu, Jie, Yi-Ning Wang, Dan-Jun Song, Jin-Peng Tan, Ya Cao, Jia Fan, Zheng Wang, and Jian Zhou. 2021. "A High-Accuracy Model Based on Plasma miRNAs Diagnoses Intrahepatic Cholangiocarcinoma: A Single Center with 1001 Samples" Diagnostics 11, no. 4: 610. https://doi.org/10.3390/diagnostics11040610