
Impact of [18F]FDG-PET and [18F]FLT-PET-Parameters in Patients with Suspected Relapse of Irradiated Lung Cancer

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Imaging
2.3. Image Analyses
2.4. Outcome
2.5. Statistics
3. Results
3.1. FDG-SUVmax and FLT-SUVmax
3.2. Relapse Detection
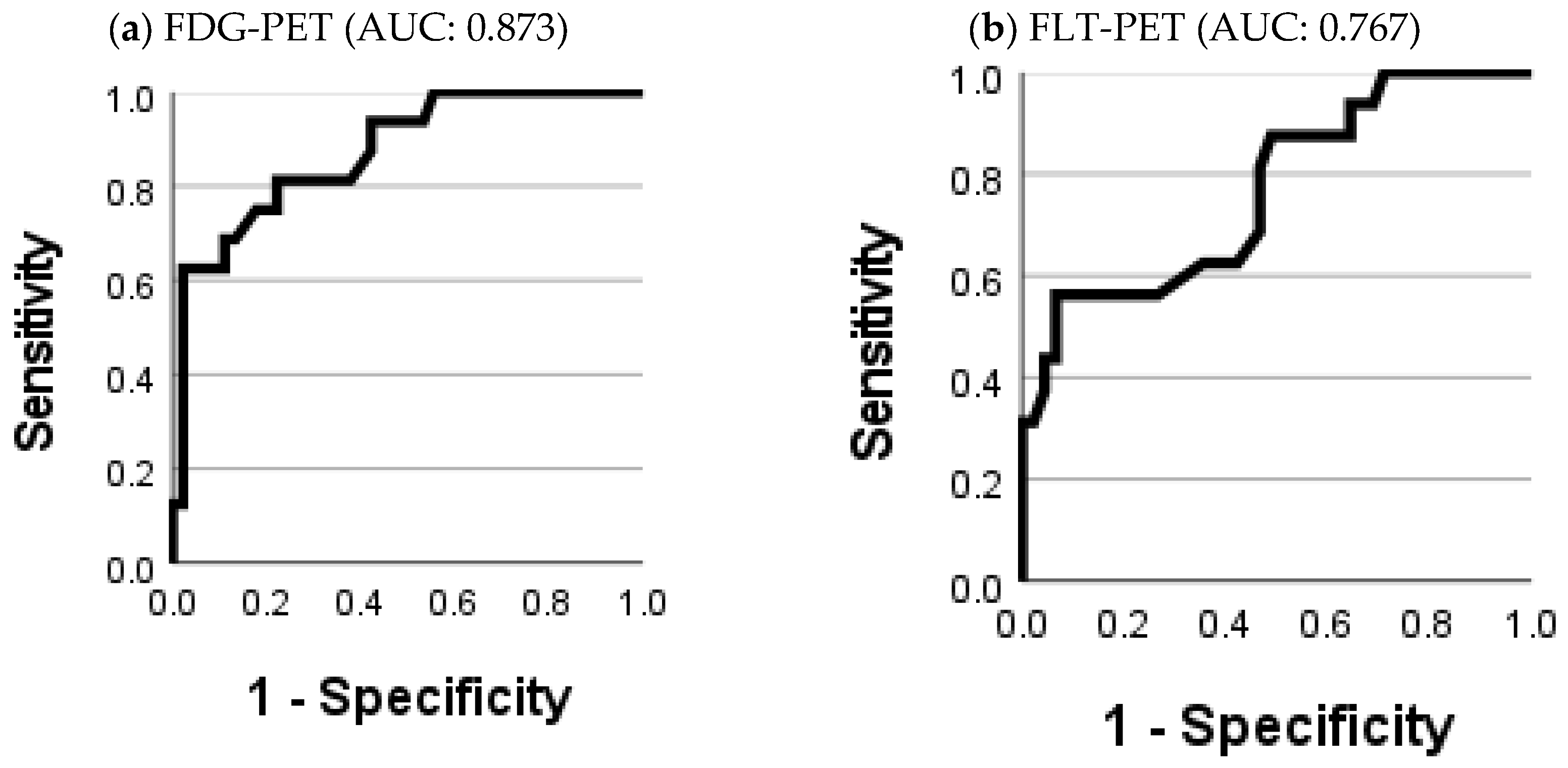
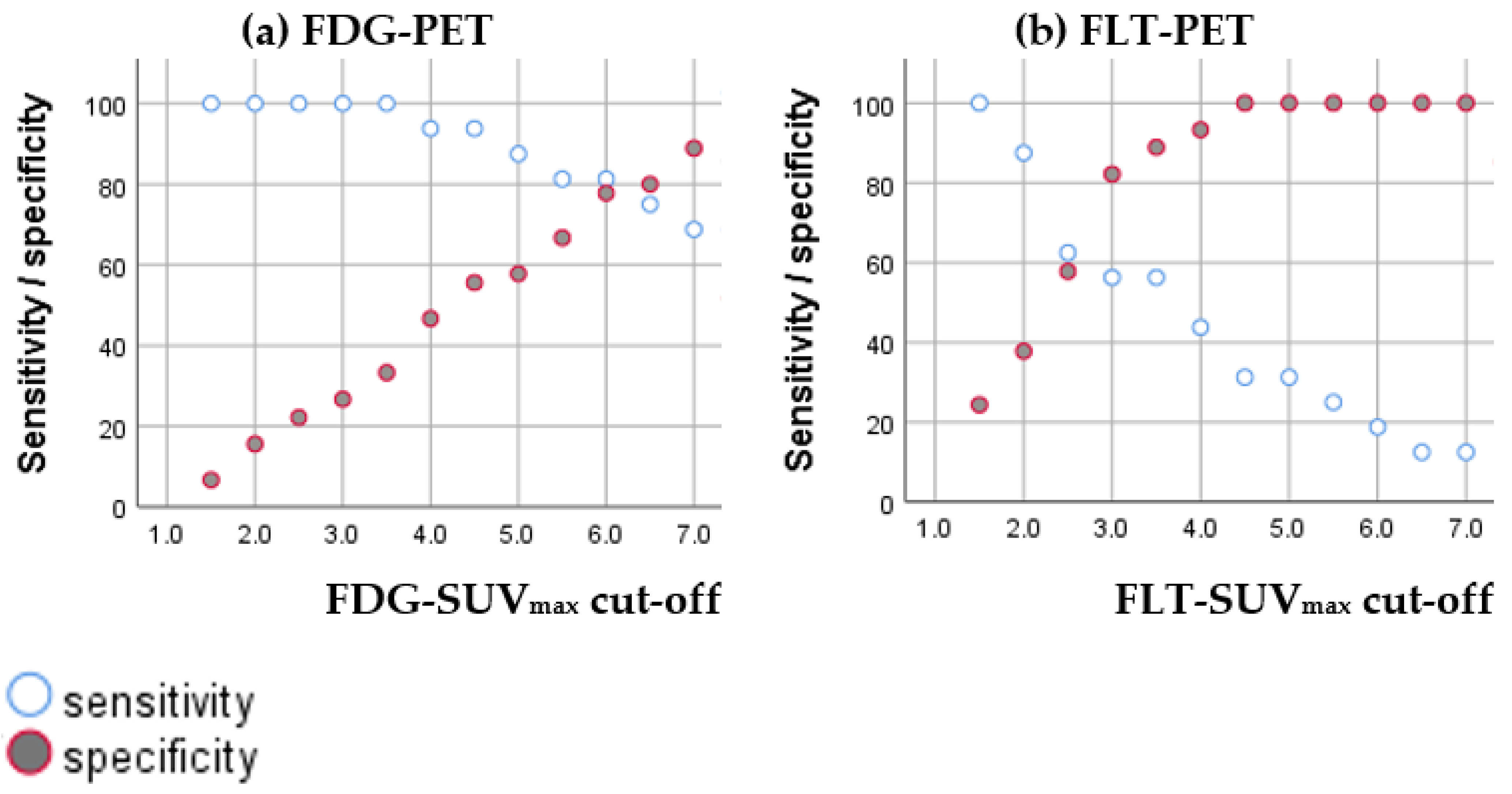
3.2.1. Diagnostic Accuracy of FDG-SUVmax and FLT-SUVmax
3.2.2. Diagnostic Value of Combining FDG-SUVmax and FLT-SUVmax
3.3. Prognosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matsuo, Y. A Systematic Literature Review on Salvage Radiotherapy for Local or Regional Recurrence After Previous Stereotactic Body Radiotherapy for Lung Cancer. Technol. Cancer Res. Treat. 2018, 17, 1533033818798633. [Google Scholar] [CrossRef]
- Sheikhbahaei, S.; Mena, E.; Yanamadala, A.; Reddy, S.; Solnes, L.B.; Wachsmann, J.; Subramaniam, R.M. The Value of FDG PET/CT in Treatment Response Assessment, Follow-Up, and Surveillance of Lung Cancer. AJR Am. J. Roentgenol. 2017, 208, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; Committee, E.G. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), iv1–iv21. [Google Scholar] [CrossRef]
- Christensen, T.N.; Langer, S.W.; Persson, G.F.; Larsen, K.R.; Loft, A.; Amtoft, A.G.; Berthelsen, A.K.; Johannesen, H.H.; Keller, S.H.; Kjaer, A.; et al. (18)F-FLT-PET/CT adds value to (18)F-FDG-PET/CT for diagnosing relapse after definitive radiotherapy in patients with lung cancer. Results of a prospective clinical trial. J. Nucl. Med. 2020. [Google Scholar] [CrossRef]
- Inoue, T.; Kim, E.E.; Komaki, R.; Wong, F.C.; Bassa, P.; Wong, W.H.; Yang, D.J.; Endo, K.; Podoloff, D.A. Detecting recurrent or residual lung cancer with FDG-PET. J. Nucl. Med. 1995, 36, 788–793. [Google Scholar] [PubMed]
- Nakajima, N.; Sugawara, Y.; Kataoka, M.; Hamamoto, Y.; Ochi, T.; Sakai, S.; Takahashi, T.; Kajihara, M.; Teramoto, N.; Yamashita, M.; et al. Differentiation of tumor recurrence from radiation-induced pulmonary fibrosis after stereotactic ablative radiotherapy for lung cancer: Characterization of 18F-FDG PET/CT findings. Ann. Nucl. Med. 2013, 27, 261–270. [Google Scholar] [CrossRef]
- Matsuo, Y.; Nakamoto, Y.; Nagata, Y.; Shibuya, K.; Takayama, K.; Norihisa, Y.; Narabayashi, M.; Mizowaki, T.; Saga, T.; Higashi, T.; et al. Characterization of FDG-PET images after stereotactic body radiation therapy for lung cancer. Radiother. Oncol. 2010, 97, 200–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoopes, D.J.; Tann, M.; Fletcher, J.W.; Forquer, J.A.; Lin, P.F.; Lo, S.S.; Timmerman, R.D.; McGarry, R.C. FDG-PET and stereotactic body radiotherapy (SBRT) for stage I non-small-cell lung cancer. Lung Cancer 2007, 56, 229–234. [Google Scholar] [CrossRef]
- Hoeben, B.A.; Troost, E.G.; Bussink, J.; van Herpen, C.M.; Oyen, W.J.; Kaanders, J.H. 18F-FLT PET changes during radiotherapy combined with cetuximab in head and neck squamous cell carcinoma patients. Nukl. Nucl. Med. 2014, 53. [Google Scholar] [CrossRef]
- Hoshikawa, H.; Mori, T.; Kishino, T.; Yamamoto, Y.; Inamoto, R.; Akiyama, K.; Mori, N.; Nishiyama, Y. Changes in (18)F-fluorothymidine and (18)F-fluorodeoxyglucose positron emission tomography imaging in patients with head and neck cancer treated with chemoradiotherapy. Ann. Nucl. Med. 2013, 27, 363–370. [Google Scholar] [CrossRef]
- Hoeben, B.A.; Troost, E.G.; Span, P.N.; van Herpen, C.M.; Bussink, J.; Oyen, W.J.; Kaanders, J.H. 18F-FLT PET during radiotherapy or chemoradiotherapy in head and neck squamous cell carcinoma is an early predictor of outcome. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2013, 54, 532–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, L.P.; Kim, C.K.; Viswanathan, A.N. Pilot study assessing (18)F-fluorothymidine PET/CT in cervical and vaginal cancers before and after external beam radiation. Gynecol. Oncol. Rep. 2015, 14, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Everitt, S.J.; Ball, D.L.; Hicks, R.J.; Callahan, J.; Plumridge, N.; Collins, M.; Herschtal, A.; Binns, D.; Kron, T.; Schneider, M.; et al. Differential (18)F-FDG and (18)F-FLT Uptake on Serial PET/CT Imaging Before and During Definitive Chemoradiation for Non-Small Cell Lung Cancer. J. Nucl. Med. 2014, 55, 1069–1074. [Google Scholar] [CrossRef] [Green Version]
- Vera, P.; Bohn, P.; Edet-Sanson, A.; Salles, A.; Hapdey, S.; Gardin, I.; Menard, J.F.; Modzelewski, R.; Thiberville, L.; Dubray, B. Simultaneous positron emission tomography (PET) assessment of metabolism with (1)(8)F-fluoro-2-deoxy-d-glucose (FDG), proliferation with (1)(8)F-fluoro-thymidine (FLT), and hypoxia with (1)(8)fluoro-misonidazole (F-miso) before and during radiotherapy in patients with non-small-cell lung cancer (NSCLC): A pilot study. Radiother. Oncol. 2011, 98, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Everitt, S.; Hicks, R.J.; Ball, D.; Kron, T.; Schneider-Kolsky, M.; Walter, T.; Binns, D.; Mac Manus, M. Imaging cellular proliferation during chemo-radiotherapy: A pilot study of serial 18F-FLT positron emission tomography/computed tomography imaging for non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Trigonis, I.; Koh, P.K.; Taylor, B.; Tamal, M.; Ryder, D.; Earl, M.; Anton-Rodriguez, J.; Haslett, K.; Young, H.; Faivre-Finn, C.; et al. Early reduction in tumour [18F]fluorothymidine (FLT) uptake in patients with non-small cell lung cancer (NSCLC) treated with radiotherapy alone. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 682–693. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Wang, Y.; Sui, X.; Zhang, W.; Shi, R.; Zhang, Y.; Dang, Y.; Qiao, Z.; Zhang, B.; Song, W.; et al. Performance of FLT-PET for pulmonary lesion diagnosis compared with traditional FDG-PET: A meta-analysis. Eur. J. Radiol. 2015, 84, 1371–1377. [Google Scholar] [CrossRef]
- Hiniker, S.M.; Sodji, Q.; Quon, A.; Gutkin, P.M.; Arksey, N.; Graves, E.E.; Chin, F.T.; Maxim, P.G.; Diehn, M.; Loo, B.W., Jr. FLT-PET-CT for the Detection of Disease Recurrence After Stereotactic Ablative Radiotherapy or Hyperfractionation for Thoracic Malignancy: A Prospective Pilot Study. Front. Oncol. 2019, 9, 467. [Google Scholar] [CrossRef]
- Saga, T.; Koizumi, M.; Inubushi, M.; Yoshikawa, K.; Tanimoto, K.; Fukumura, T.; Miyamoto, T.; Nakajima, M.; Yamamoto, N.; Baba, M. PET/CT with 3’-deoxy-3’-[18F]fluorothymidine for lung cancer patients receiving carbon-ion radiotherapy. Nucl. Med. Commun. 2011, 32, 348–355. [Google Scholar] [CrossRef]
- Lopez Guerra, J.L.; Gladish, G.; Komaki, R.; Gomez, D.; Zhuang, Y.; Liao, Z. Large decreases in standardized uptake values after definitive radiation are associated with better survival of patients with locally advanced non-small cell lung cancer. J. Nucl. Med. 2012, 53, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Bollineni, V.R.; Widder, J.; Pruim, J.; Langendijk, J.A.; Wiegman, E.M. Residual (1)(8)F-FDG-PET uptake 12 weeks after stereotactic ablative radiotherapy for stage I non-small-cell lung cancer predicts local control. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e551-5. [Google Scholar] [CrossRef]
- Pierson, C.; Grinchak, T.; Sokolovic, C.; Holland, B.; Parent, T.; Bowling, M.; Arastu, H.; Walker, P.; Ju, A. Response criteria in solid tumors (PERCIST/RECIST) and SUVmax in early-stage non-small cell lung cancer patients treated with stereotactic body radiotherapy. Radiat. Oncol. 2018, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, J.O.; Jung, C.K.; Kim, Y.S.; Yoo Ie, R.; Choi, W.H.; Jeon, E.K.; Hong, S.H.; Chun, S.H.; Kim, S.J.; et al. Metabolic activity on [18f]-fluorodeoxyglucose-positron emission tomography/computed tomography and glucose transporter-1 expression might predict clinical outcomes in patients with limited disease small-cell lung cancer who receive concurrent chemoradiation. Clin. Lung Cancer 2014, 15, e13-21. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. European Association of Nuclear M. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Shusharina, N.; Cho, J.; Sharp, G.C.; Choi, N.C. Correlation of (18)F-FDG avid volumes on pre-radiation therapy and post-radiation therapy FDG PET scans in recurrent lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, M.P.; Hruby, G.; Metser, U.; Sridharan, S.; Capp, A.; Kumar, M.; Gallagher, S.; Rutherford, N.; Holder, C.; Oldmeadow, C.; et al. FDG-PET parameters predict for recurrence in anal cancer-results from a prospective, multicentre clinical trial. Radiat. Oncol. 2019, 14, 140. [Google Scholar] [CrossRef] [Green Version]
- Boellaard, R.; O’Doherty, M.J.; Weber, W.A.; Mottaghy, F.M.; Lonsdale, M.N.; Stroobants, S.G.; Oyen, W.J.; Kotzerke, J.; Hoekstra, O.S.; Pruim, J.; et al. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 181–200. [Google Scholar] [CrossRef] [Green Version]
- Van Waarde, A.; Cobben, D.C.; Suurmeijer, A.J.; Maas, B.; Vaalburg, W.; de Vries, E.F.; Jager, P.L.; Hoekstra, H.J.; Elsinga, P.H. Selectivity of 18F-FLT and 18F-FDG for differentiating tumor from inflammation in a rodent model. J. Nucl. Med. 2004, 45, 695–700. [Google Scholar]
- Lee, T.S.; Ahn, S.H.; Moon, B.S.; Chun, K.S.; Kang, J.H.; Cheon, G.J.; Choi, C.W.; Lim, S.M. Comparison of 18F-FDG, 18F-FET and 18F-FLT for differentiation between tumor and inflammation in rats. Nucl. Med. Biol. 2009, 36, 681–686. [Google Scholar] [CrossRef]
- Yue, J.; Chen, L.; Cabrera, A.R.; Sun, X.; Zhao, S.; Zheng, F.; Han, A.; Zheng, J.; Teng, X.; Ma, L.; et al. Measuring tumor cell proliferation with 18F-FLT PET during radiotherapy of esophageal squamous cell carcinoma: A pilot clinical study. J. Nucl. Med. 2010, 51, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Andersen, F.L.; Klausen, T.L.; Loft, A.; Beyer, T.; Holm, S. Clinical evaluation of PET image reconstruction using a spatial resolution model. Eur. J. Radiol. 2013, 82, 862–869. [Google Scholar] [CrossRef]
- Riegler, G.; Karanikas, G.; Rausch, I.; Hirtl, A.; El-Rabadi, K.; Marik, W.; Pivec, C.; Weber, M.; Prosch, H.; Mayerhoefer, M. Influence of PET reconstruction technique and matrix size on qualitative and quantitative assessment of lung lesions on [18F]-FDG-PET: A prospective study in 37 cancer patients. Eur. J. Radiol. 2017, 90, 20–26. [Google Scholar] [CrossRef]
- He, Y.Q.; Gong, H.L.; Deng, Y.F.; Li, W.M. Diagnostic efficacy of PET and PET/CT for recurrent lung cancer: A meta-analysis. Acta Radiol. 2014, 55, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Hellwig, D.; Groschel, A.; Graeter, T.P.; Hellwig, A.P.; Nestle, U.; Schafers, H.J.; Sybrecht, G.W.; Kirsch, C.M. Diagnostic performance and prognostic impact of FDG-PET in suspected recurrence of surgically treated non-small cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Im, H.J.; Pak, K.; Cheon, G.J.; Kang, K.W.; Kim, S.J.; Kim, I.J.; Chung, J.K.; Kim, E.E.; Lee, D.S. Prognostic value of volumetric parameters of (18)F-FDG PET in non-small-cell lung cancer: A meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Nygard, L.; Vogelius, I.R.; Fischer, B.M.; Kjaer, A.; Langer, S.W.; Aznar, M.C.; Persson, G.F.; Bentzen, S.M. A Competing Risk Model of First Failure Site after Definitive Chemoradiation Therapy for Locally Advanced Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2018, 13, 559–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheffler, M.; Zander, T.; Nogova, L.; Kobe, C.; Kahraman, D.; Dietlein, M.; Papachristou, I.; Heukamp, L.; Buttner, R.; Boellaard, R.; et al. Prognostic impact of [18F]fluorothymidine and [18F]fluoro-D-glucose baseline uptakes in patients with lung cancer treated first-line with erlotinib. PLoS ONE 2013, 8, e53081. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Number/Median | |
|---|---|---|
| Age, at day of suspicion (median (IQ)) | 70 (65–77) | |
| Sex (male/female) | 34/27 | |
| Histology | Adenocarcinoma | 29 |
| Squamous cell carcinoma | 25 | |
| SCLC | 2 | |
| Not otherwise specified (NOS) | 3 | |
| Mixed NSCLC/SCLC | 2 | |
| Stadium: | IA | 12 |
| Ib | 6 | |
| IIa | 2 | |
| IIb | 5 | |
| IIIa | 14 | |
| IIIb | 16 | |
| IV | 6 | |
| Chemotherapy (yes/no) | 34/27 | |
| Radiotherapy: | SBRT (45-72 Gy) | 28 |
| Normofractionated radiotherapy (66 Gy) | 29 | |
| Hyperfractionated radiotherapy (45-60 Gy) | 3 | |
| Normofractionated radiotherapy (66 Gy) and SBRT (45 Gy) | 1 | |
| Timing between scans | ||
| Time from the end of radiotherapy to relapse suspicion; in months (median (IQ)) | 7 (5–12) | |
| Time from relapse suspicion to FDG-PET/CT; in days (median (IQ)) | 21 (15–27) | |
| Time from relapse suspicion to FLT-PET/CT; in days (median (IQ)) | 23 (21–29) | |
| Time between FLT-PET/CT and FDG-PET/CT; in days (median (IQ)) | 6 (3–9) | |
| Outcome | ||
| Overall relapse (yes/no) | 32/29 | |
| HDV relapse (yes/no) | 16/45 | |
| Intra-pulmonary relapse (yes/no) | 30/31 | |
| Extra-pulmonary relapse (yes/no) | 7/54 | |
| Deceased (yes/no) | 33/28 | |
| Follow-up (from suspicion of relapse); in months (median (IQ)) | 25 (16–44) | |
| FDG-PET-Parameters | All Lesion Median [IQ] (n = 30) | Lesions within HDV Median [IQ] (n = 16) | Lesions Outside of HDV Median [IQ] (n = 14) | p-Value |
|---|---|---|---|---|
| SUVmax | 8.6 [5.1–16.0] | 12.8 [6.4–16.2] | 6.2 [3.3–13.7] | 0.095 |
| SUVpeak | 4.7 [3.1–9.0] | 7.1 [4.1–10.0] | 3.5 [1.9–5.7] | 0.014 * |
| MTV3.0 | 1.7 [0.5–10.5] | 6.6 [1.6–52.2] | 0.9 [0.2–2.0] | 0.016 * |
| MTV80% | 0.1 [0.1–0.5] | 0.2 [0.1–0.6] | 0.1 [0.1–0.2] | 0.113 |
| MTV50% | 1.2 [0.5–3.6] | 2.5 [1.2–7.9] | 0.7 [0.4–1.2] | 0.014 * |
| FLT-PET-parameters | ||||
| SUVmax | 3.7 [2.0–5.1] | 3.9 [1.2–7.9] | 3.3 [1.4–4.4] | 0.188 |
| SUVpeak | 2.3 [1.3–3.3] | 2.5 [1.6–3.5] | 2.0 [1.0–2.9] | 0.145 |
| PTV3.0 | 0.2 [0.0–2.0] | 0.3 [0.0–4.0] | 0.1 [0.0–0.4] | 0.128 |
| PTV80% | 0.2 [0.1–0.3] | 0.3 [0.1–0.5] | 0.1 [0.1–0.2] | 0.311 |
| PTV50% | 1.3 [0.8–4.3] | 2.7 [0.8–10.1] | 1.2 [0.5–1.5] | 0.066 |
| FDG-PET-Parameters in Recurrent Lesions, Continuous Variable | Hazard Ratio [95% CI] | p-Value |
|---|---|---|
| SUVmax (per unit) | 1.02 [0.94–1.10] | 0.675 |
| SUVpeak (per unit) | 1.07 [0.94–1.21] | 0.335 |
| MTV3.0 (per cm3) | 1.01 [0.99–1.02] | 0.485 |
| MTV80% (per cm3) | 3.63 [0.95–13.91] | 0.060 |
| MTV50% (per cm3) | 1.13 [1.00–1.27] | 0.054 |
| FDG-PET-parameters in recurrent lesions, dichotomized variable | ||
| SUVmax (>8.6) | 1.09 [0.43–2.76] | 0.853 |
| SUVpeak (>4.7) | 1.17 [0.46–2.96] | 0.741 |
| MTV3.0 (>1.7 cm3) | 0.81 [0.32–2.07] | 0.665 |
| MTV80% (>0.1 cm3) | 1.43 [0.56–3.64] | 0.454 |
| MTV50% (>1.2 cm3) | 1.56 [0.61–3.97] | 0.355 |
| FLT-PET-parameters in recurrent lesions, continuous variable | ||
| SUVmax (per unit) | 0.93 [0.75–1.15] | 0.496 |
| SUVpeak (per unit) | 0.92 [0.64–1.31] | 0.635 |
| PTV3.0 (per cm3) | 1.05 [0.94–1.17] | 0.411 |
| PTV80% (per cm3) | 4.13 [0.85–20.16] | 0.080 |
| PTV50% (per cm3) | 1.07 [1.01–1.13] | 0.014 * |
| FLT-PET-parameters in recurrent lesions, dichotomized variable | ||
| SUVmax (>3.7) | 0.80 [0.31–2.01] | 0.644 |
| SUVpeak (>2.3) | 0.96 [0.38–2.47] | 0.939 |
| PTV3.0 (>0.2 cm3) | 0.78 [0.30–2.07] | 0.619 |
| PTV80% (>0.2 cm3) | 1.67 [0.65–4.26] | 0.285 |
| PTV50% (>1.3 cm3) | 1.42 [0.56–3.61] | 0.465 |
| Clinical parameters | ||
| Age (at suspicion) (per year) | 1.04 [0.97–1.11] | 0.268 |
| Sex (male) | 2.74 [0.98–7.67] | 0.055 |
| Stadium (III vs. I–II) | 1.18 [0.45–3.14] | 0.736 |
| (IV vs. I–II) | 0.59 [0.07–4.83] | 0.622 |
| Radiotherapy (Conventionally fractionated radiotherapy vs. SBRT) | 0.97 [0.38–2.52] | 0.956 |
| Histology (Squamous cell carcinoma vs. adenocarcinoma) | 1.24 [0.48–3.20] | 0.659 |
| Time since the end of radiotherapy (per month) | 0.99 [0.90–1.09] | 0.837 |
| Site of relapse (within HDV vs. outside HDV) | 1.53 [0.59–3.94] | 0.381 |
| Intention for the relapse treatment (palliation vs. curative) | 1.33 [0.51–3.46] | 0.564 |
| Extra-pulmonary metastases (present) | 2.18 [0.70–6.77] | 0.180 |
| Covariate | Hazard Ratio [95% CI] | p-Value |
|---|---|---|
| MTV50% (per cm3) | 1.19 [0.99–1.44] | 0.063 |
| PTV50% (per cm3) | 1.02 [0.95–1.09] | 0.650 |
| Sex (male) | 4.32 [1.34–13.92] | 0.014 * |
| Age (at suspicion) (per year) | 1.08 [1.00–1.17] | 0.054 |
| Time since the end of radiotherapy (per month) | 0.96 [0.88–1.05] | 0.349 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christensen, T.N.; Langer, S.W.; Persson, G.; Larsen, K.R.; Amtoft, A.G.; Keller, S.H.; Kjaer, A.; Fischer, B.M. Impact of [18F]FDG-PET and [18F]FLT-PET-Parameters in Patients with Suspected Relapse of Irradiated Lung Cancer. Diagnostics 2021, 11, 279. https://doi.org/10.3390/diagnostics11020279
Christensen TN, Langer SW, Persson G, Larsen KR, Amtoft AG, Keller SH, Kjaer A, Fischer BM. Impact of [18F]FDG-PET and [18F]FLT-PET-Parameters in Patients with Suspected Relapse of Irradiated Lung Cancer. Diagnostics. 2021; 11(2):279. https://doi.org/10.3390/diagnostics11020279
Chicago/Turabian StyleChristensen, Tine N., Seppo W. Langer, Gitte Persson, Klaus Richter Larsen, Annemarie G. Amtoft, Sune H. Keller, Andreas Kjaer, and Barbara Malene Fischer. 2021. "Impact of [18F]FDG-PET and [18F]FLT-PET-Parameters in Patients with Suspected Relapse of Irradiated Lung Cancer" Diagnostics 11, no. 2: 279. https://doi.org/10.3390/diagnostics11020279