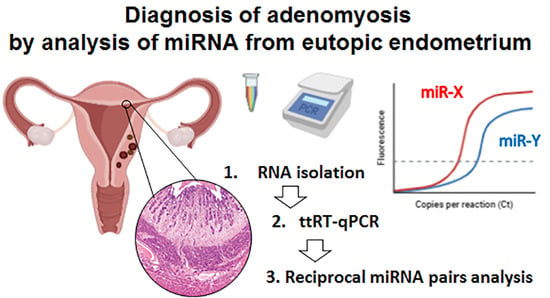
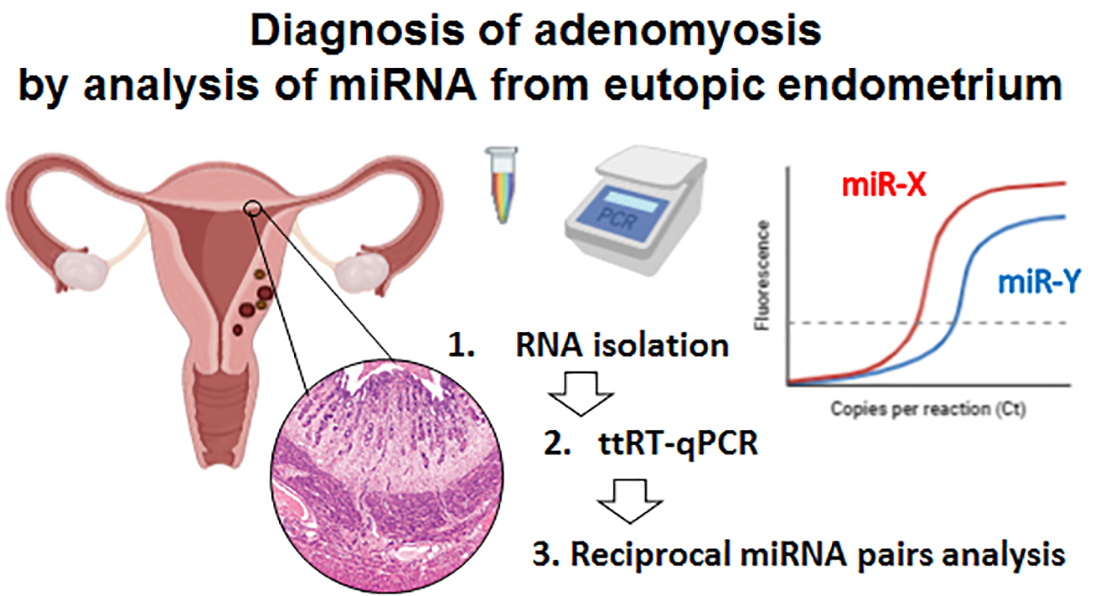
Analysis of Reciprocally Dysregulated miRNAs in Eutopic Endometrium Is a Promising Approach for Low Invasive Diagnostics of Adenomyosis

 , ,
, , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Study Design
2.2. Participants
2.3. RNA Sampling
2.4. miRNA Expression Profiling Using Exiqon microRNA PCR Panel
2.5. Quantitative Real-Time RT-PCR (qPCR)
2.6. Calculation and Statistics
3. Results
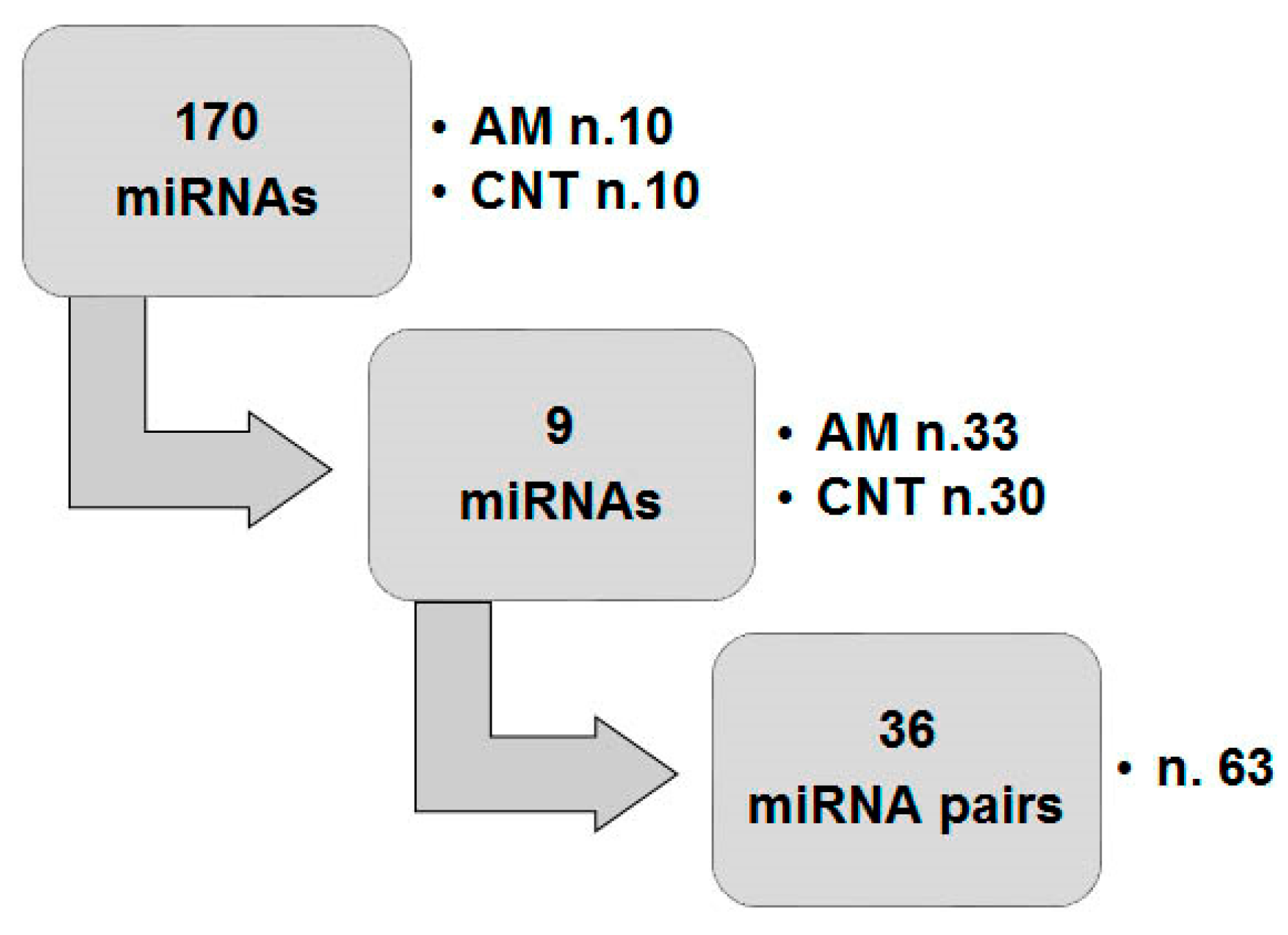
3.1. Preliminary miRNA Profiling
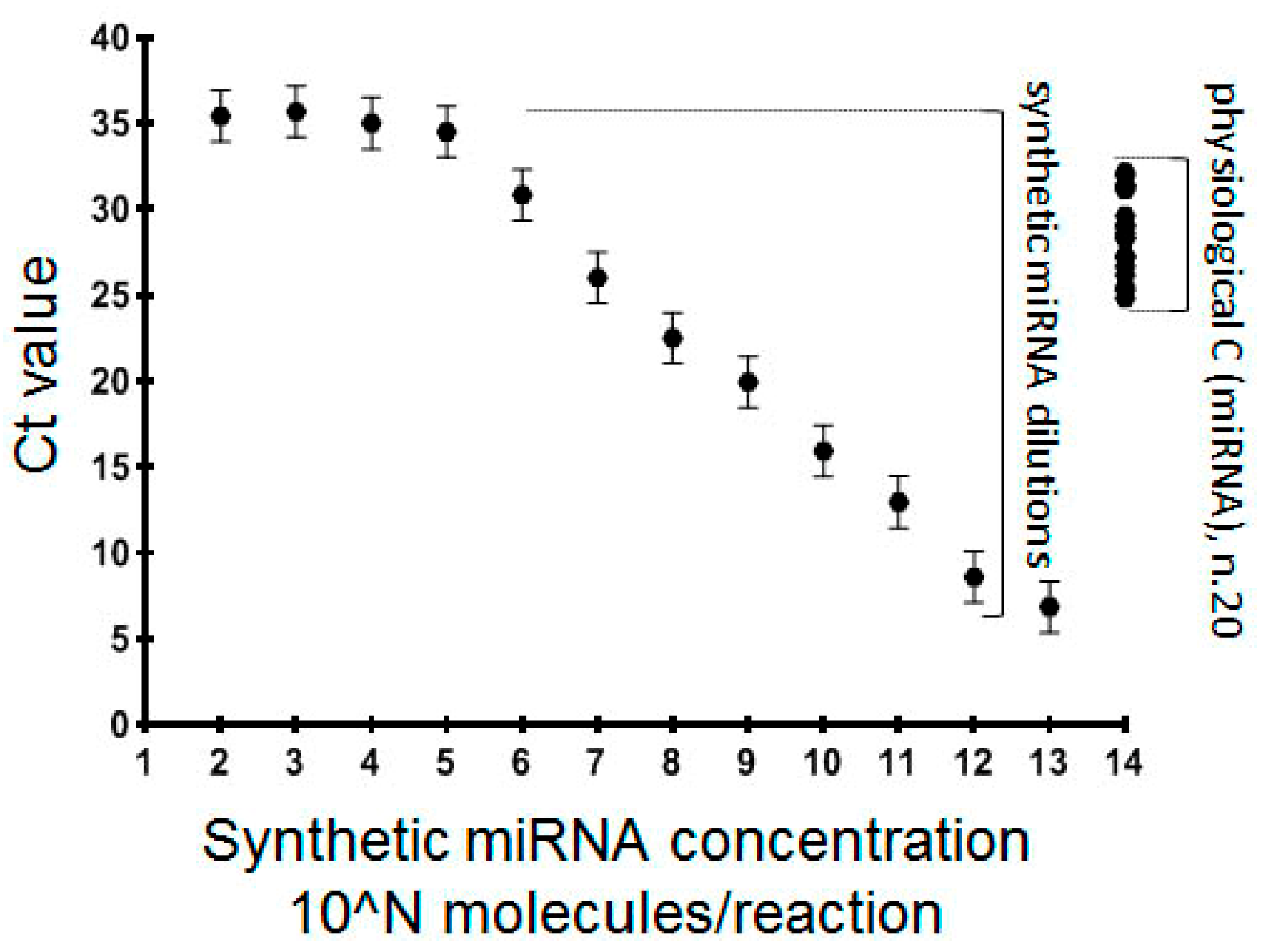
3.2. Creation and Validation of ttRT-qPCR Systems for Individual miRNA Analysis
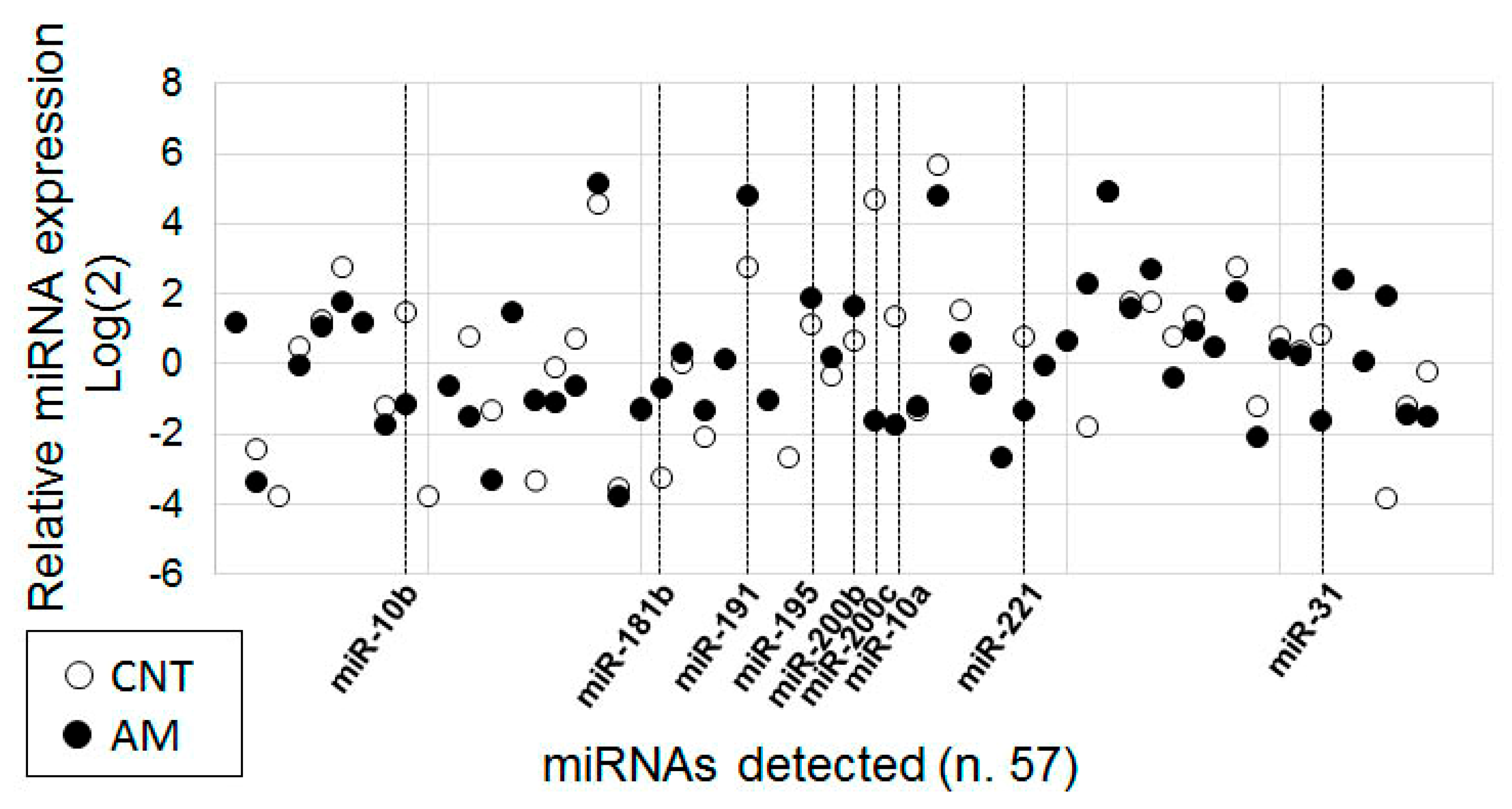
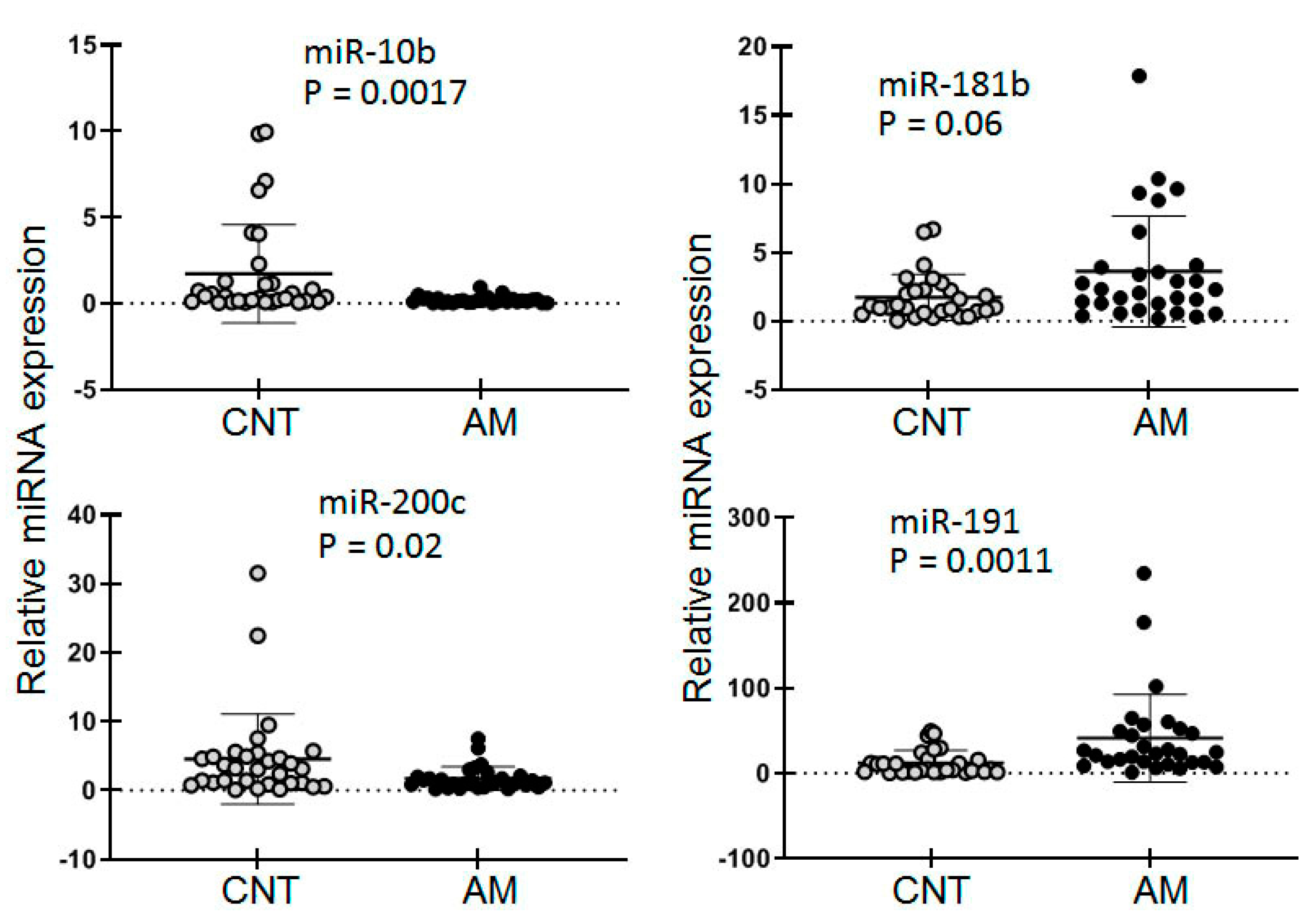
3.3. Analysis of Selected miRNAs by ttRT-qPCR Systems
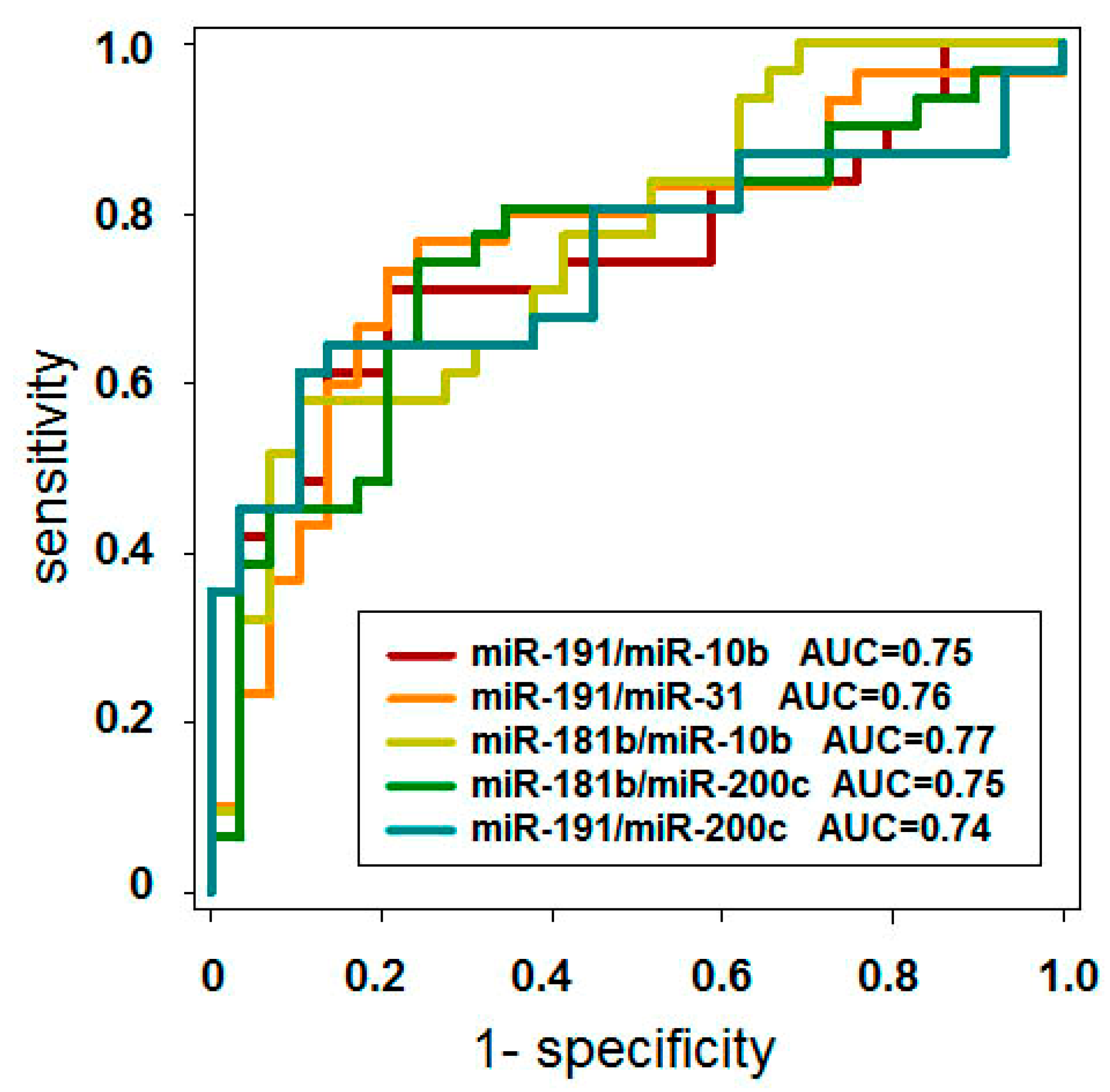
3.4. Identification of Reciprocally Dysregulated miRNA Pairs and Analysis of Their Diagnostic Potency
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mason, B.R.; Chatterjee, D.; Menias, C.O.; Thaker, P.H.; Siegel, C.L.; Yano, M. Encyclopedia of endometriosis: A pictorial rad-path review. Abdom. Radiol. 2020, 45, 1587–1607. [Google Scholar] [CrossRef]
- Johnson, N.P.; Hummelshoj, L.; Adamson, G.D.; Keckstein, J.; Taylor, H.S.; Abrao, M.S.; Bush, D.; Kiesel, L.; Tamimi, R.; Sharpe-Timms, K.L.; et al. World endometriosis society consensus on the classification of endometriosis. Hum. Reprod. 2017, 32, 315–324. [Google Scholar] [CrossRef]
- Ministry of Health of the Russian Federation Endometriosis: Clinical recommendation. Clin. Recom. ID KP259 2016, ID: KP259 .
- National Guideline Alliance (UK). Endometriosis: Diagnosis and Management; National Institute for Health and Care Excellence: London, UK, 2017; (NICE Guideline, No. 73.). Available online: https://www.ncbi.nlm.nih.gov/books/NBK453273/ (accessed on 3 October 2020).
- Collège National des Gynécologues et Obstétriciens Français Management of endometriosis. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 265–274.
- Kossmann, R. Die Abstammung der Drüseneinschlüsse in den Adenomyomen des Uterus und der Tuben-Eine kritische Studie. Arch. Gynakol. 1897, 54, 359–383. [Google Scholar]
- Sampson, J.A. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am. J. Obstet. Gynecol. 1927, 14, 422–469. [Google Scholar] [CrossRef]
- Sourial, S.; Tempest, N.; Hapangama, D.K. Theories on the Pathogenesis of Endometriosis. Int. J. Reprod. Med. 2014, 179515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laganà, A.S.; Garzon, S.; Götte, M.; Viganò, P.; Franchi, M.; Ghezzi, F.; Martin, D.C. The Pathogenesis of Endometriosis: Molecular and Cell Biology Insights. Int. J. Mol. Sci. 2019, 20, 5615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, L.M.; Ferreira, M.C.; Rocha, A.L.L.; Carneiro, M.M.; Reis, F.M. New biomarkers in endometriosis. Adv. Clin. Chem. 2019, 89, 59–77. [Google Scholar]
- Anastasiu, C.V.; Moga, M.A.; Elena Neculau, A.; Bălan, A.; Scârneciu, I.; Dragomir, R.M.; Dull, A.-M.; Chicea, L.-M. Biomarkers for the Noninvasive Diagnosis of Endometriosis: State of the Art and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 1750. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.J.; Yang, H.L.; Shao, J.; Mei, J.; Chang, K.K.; Zhu, R.; Li, M.Q. Anti-inflammatory cytokines in endometriosis. Cell. Mol. Life Sci. 2019, 76, 2111–2132. [Google Scholar] [CrossRef]
- Riccio, L.D.G.C.; Santulli, P.; Marcellin, L.; Abrão, M.S.; Batteux, F.; Chapron, C. Immunology of endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 50, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Turgut, A.; Hocaoglu, M.; Ozdamar, O.; Usta, A.; Gunay, T.; Akdeniz, E. Could hematologic parameters be useful biomarkers for the diagnosis of endometriosis? Bratisl. Med. J. 2019, 120, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, Z.; Yang, F.; Wang, H.; Liang, S.; Wang, H.; Yang, J.; Lin, J. The role of endometrial stem cells in the pathogenesis of endometriosis and their application to its early diagnosis†. Biol. Reprod. 2020, 102, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Liutkevičienė, R.; Mečėjus, G.; Žilovič, D.; Bumbulienė, Ž. Endometrial biopsy and density of nerve fibers in eutopic endometrium. Looking for easier ways to diagnose endometriosis. Gynecol. Endocrinol. 2019, 35, 1107–1110. [Google Scholar] [CrossRef] [PubMed]
- Burney, R.O.; Hamilton, A.E.; Aghajanova, L.; Vo, K.C.; Nezhat, C.N.; Lessey, B.A.; Giudice, L.C. MicroRNA expression profiling of eutopic secretory endometrium in women with versus without endometriosis. Mol. Hum. Reprod. 2009, 15, 625–631. [Google Scholar] [CrossRef]
- Braza-Boïls, A.; Marí-Alexandre, J.; Gilabert, J.; Sánchez-Izquierdo, D.; España, F.; Estellés, A.; Gilabert-Estellés, J. MicroRNA expression profile in endometriosis: Its relation to angiogenesis and fibrinolytic factors. Hum. Reprod. 2014, 29, 978–988. [Google Scholar] [CrossRef] [Green Version]
- Zheng, B.; Xue, X.; Zhao, Y.; Chen, J.; Xu, C.Y.; Duan, P. The differential expression of microRNA-143,145 in endometriosis. Iran. J. Reprod. Med. 2014, 12, 555. [Google Scholar]
- Gao, S.; Liu, S.; Gao, Z.-M.; Deng, P.; Wang, D.-B. Reduced microRNA-451 expression in eutopic endometrium contributes to the pathogenesis of endometriosis. World J. Clin. Cases 2019, 7, 2155. [Google Scholar] [CrossRef]
- Bjorkman, S.; Taylor, H.S. MicroRNAs in endometriosis: Biological function and emerging biomarker candidates†. Biol. Reprod. 2019, 101, 1167–1178. [Google Scholar] [CrossRef]
- Van Den Bosch, T.; Dueholm, M.; Leone, F.P.G.; Valentin, L.; Rasmussen, C.K.; Votino, A.; Van Schoubroeck, D.; Landolfo, C.; Installé, A.J.F.; Guerriero, S.; et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: A consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound Obstet. Gynecol. 2015, 46, 284–298. [Google Scholar] [CrossRef]
- Van den Bosch, T.; de Bruijn, A.M.; de Leeuw, R.A.; Dueholm, M.; Exacoustos, C.; Valentin, L.; Bourne, T.; Timmerman, D.; Huirne, J.A.F. Sonographic classification and reporting system for diagnosing adenomyosis. Ultrasound Obstet. Gynecol. 2019, 53, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Exacoustos, C.; Morosetti, G.; Conway, F.; Camilli, S.; Martire, F.G.; Lazzeri, L.; Piccione, E.; Zupi, E. New Sonographic Classification of Adenomyosis: Do Type and Degree of Adenomyosis Correlate to Severity of Symptoms? J. Minim. Invasive Gynecol. 2020, 27, 1308–1315. [Google Scholar] [CrossRef]
- Munro, M.G. Classification and Reporting Systems for Adenomyosis. J. Minim. Invasive Gynecol. 2020, 27, 296–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Androvic, P.; Valihrach, L.; Elling, J.; Sjoback, R.; Kubista, M. Two-tailed RT-qPCR: A novel method for highly accurate miRNA quantification. Nucleic Acids Res. 2017, 45, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, R.; Sacan, A. A novel method for the normalization of microRNA RT-PCR data. BMC Med. Genom. 2013, 6 (Suppl. 1), S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mestdagh, P.; Van Vlierberghe, P.; De Weer, A.; Muth, D.; Westermann, F.; Speleman, F.; Vandesompele, J. A novel and universal method for microRNA RT-qPCR data normalization. Genome Biol. 2009, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benes, V.; Castoldi, M. Expression profiling of microRNA using real-time quantitative PCR, how to use it and what is available. Methods 2010, 50, 244–249. [Google Scholar] [CrossRef]
- Ivanov, M.; Titov, S.; Glushkov, S.; Dzyubenko, V.; Malek, A.; Arkhangelskaya, P.; Samsonov, R.; Mikhetko, A.; Bakhidze, E.; Berlev, I.; et al. Detection of high-grade neoplasia in air-dried cervical PAP smears by a microRNA-based classifier. Oncol. Rep. 2018, 39, 1099–1111. [Google Scholar] [CrossRef]
- Kolesnikov, N.N.; Titov, S.E.; Veryaskina, Y.A.; Vladimirova, A.V.; Samsonov, R.B.; Artem’eva, A.S.; Novik, V.I.; Bershteyn, L.M.; Zhimulev, I.F.; Malek, A.V. Improvement of accuracy and diagnostic significance of breast tumor fine-needle aspiration biopsy by miRNA analysis of material isolated from cytological smears. Adv. Mol. Oncol. 2016, 3, 44–52. [Google Scholar] [CrossRef]
- Hua, F. miR-191 Modulates Malignant Transformation of Endometriosis Through Regulating TIMP3. Med. Sci. Monit. 2015, 21, 915–920. [Google Scholar] [CrossRef] [Green Version]
- Graham, A.; Holbert, J.; Nothnick, W.B. miR-181b-5p Modulates Cell Migratory Proteins, Tissue Inhibitor of Metalloproteinase 3, and Annexin A2 During In Vitro Decidualization in a Human Endometrial Stromal Cell Line. Reprod. Sci. 2017, 24, 1264–1274. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.; Kässens, N.; Greve, B.; Hassan, H.; Schüring, A.N.; Starzinski-Powitz, A.; Kiesel, L.; Seidler, D.G.; Götte, M. Targeting of syndecan-1 by micro-ribonucleic acid miR-10b modulates invasiveness of endometriotic cells via dysregulation of the proteolytic milieu and interleukin-6 secretion. Fertil. Steril. 2013, 99, 871–881.e1. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Chen, Y.; Zhao, Y.; Xu, C.; Zhang, A.; Zhang, Q.; Wang, D.; He, J.; Hua, W.; Duan, P. MiR-200c suppresses endometriosis by targeting MALAT1 in vitro and in vivo. Stem Cell Res. Ther. 2017, 8, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Causin, R.; Pessa-Pereira, D.; Souza, K.; Evangelista, A.; Reis, R.; Fregnani, J.; Marques, M. Identification and performance evaluation of housekeeping genes for microRNA expression normalization by reverse transcription-quantitative PCR using liquid-based cervical cytology samples. Oncol. Lett. 2019, 18, 4753–4761. [Google Scholar] [CrossRef] [Green Version]
- Titov, S.E.; Demenkov, P.S.; Ivanov, M.K.; Malakhina, E.S.; Poloz, T.L.; Tsivlikova, E.V.; Ganzha, M.S.; Shevchenko, S.P.; Gulyaeva, L.F.; Kolesnikov, N.N. Selection and validation of miRNAs as normalizers for profiling expression of microRNAs isolated from thyroid fine needle aspiration smears. Oncol. Rep. 2016, 36, 2501–2510. [Google Scholar] [CrossRef]
- Danese, E.; Minicozzi, A.M.; Benati, M.; Paviati, E.; Lima-Oliveira, G.; Gusella, M.; Pasini, F.; Salvagno, G.L.; Montagnana, M.; Lippi, G. Reference miRNAs for colorectal cancer: Analysis and verification of current data. Sci. Rep. 2017, 7, 8413. [Google Scholar] [CrossRef]
- Inada, K.; Okoshi, Y.; Cho-Isoda, Y.; Ishiguro, S.; Suzuki, H.; Oki, A.; Tamaki, Y.; Shimazui, T.; Saito, H.; Hori, M.; et al. Endogenous reference RNAs for microRNA quantitation in formalin-fixed, paraffin-embedded lymph node tissue. Sci. Rep. 2018, 8, 5918. [Google Scholar] [CrossRef]
- Lamba, V.; Ghodke-Puranik, Y.; Guan, W.; Lamba, J.K. Identification of suitable reference genes for hepatic microRNA quantitation. BMC Res. Notes 2014, 7, 129. [Google Scholar] [CrossRef] [Green Version]
- Torres, A.; Torres, K.; Wdowiak, P.; Paszkowski, T.; Maciejewski, R. Selection and validation of endogenous controls for microRNA expression studies in endometrioid endometrial cancer tissues. Gynecol. Oncol. 2013, 130, 588–594. [Google Scholar] [CrossRef] [Green Version]
- Galiveti, C.R.; Rozhdestvensky, T.S.; Brosius, J.; Lehrach, H.; Konthur, Z. Application of housekeeping npcRNAs for quantitative expression analysis of human transcriptome by real-time PCR. RNA 2010, 16, 450–461. [Google Scholar] [CrossRef] [Green Version]
- Vigneron, N.; Meryet-Figuière, M.; Guttin, A.; Issartel, J.P.; Lambert, B.; Briand, M.; Louis, M.H.; Vernon, M.; Lebailly, P.; Lecluse, Y.; et al. Towards a new standardized method for circulating miRNAs profiling in clinical studies: Interest of the exogenous normalization to improve miRNA signature accuracy. Mol. Oncol. 2016, 10, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Dartmouth, K. A systematic review with meta-analysis: The common sonographic characteristics of adenomyosis. Ultrasound 2014, 22, 148–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Location (Uteri Wall) | Anterior = 4 | Posterior = 22 | Mixed/Other = 7 | |
|---|---|---|---|---|
| Differentiation | Focal = 10 | Diffuse = 17 | Adenomyoma = 6 | |
| Cystic | Yes = 28 | No = 5 | ||
| Uterine layer involvement | Type 1–2 = 19 | Type 2–3 = 8 | Type 1–3 = 6 | |
| Extent of adenomyosis | Moderate = 21 | Severe = 12 | ||
| Size of lesions | 3–6 cm = 8 | 7–9 cm = 22 | 10 and >=3 | |
| miRNA | Method Sensitivity Limit for Synthetic miRNA | Results of miRNA Analysis in Biological Samples(Ct Value Range and Median) | |
|---|---|---|---|
| Plateau of Ct Value | Minimal Concentration (Molecules/Reaction) | ||
| -10a | 36.3 | 104 | 29.32–33.41 (31.80) |
| -10b | 34.7 | 105 | 28.12–31.97 (30.60) |
| -31 | 30.4 | 105 | 26.03–28.78 (27.45) |
| -181b | 29.5 | 107 | 27.03–28.03 (27.45) |
| -191 | 31.4 | 105 | 21.42–25.44 (23.67) |
| -195 | 32.5 | 105 | 25.31–29.12 (27.31) |
| -200b | 33.4 | 105 | 24.11–25.25 (26.87) |
| -200c | 33.7 | 105 | 25.18–30.22 (27.53) |
| -221 | 32.6 | 106 | 29.55–31.88 (30.88) |
| miRNA- | -10a | -10b | -31 | -181b | -191 | -195 | -200b | -200c | -221 | |
|---|---|---|---|---|---|---|---|---|---|---|
| CNT | Mean | 0.23 | 1.72 | 3.49 | 2.38 | 20.04 | 7.56 | 3.48 | 4.57 | 0.43 |
| SEM | 0.06 | 0.51 | 0.76 | 0.71 | 6.18 | 2.77 | 0.93 | 1.17 | 0.14 | |
| AM | Mean | 0.24 | 0.19 | 3.05 | 3.63 | 41.34 | 8.48 | 5.71 | 1.73 | 0.22 |
| SEM | 0.06 | 0.04 | 0.55 | 0.75 | 9.56 | 2.16 | 3.02 | 0.32 | 0.07 | |
| Mann–Whitney | NS | 0.0017 | 0.9490 | 0.0680 | 0.0011 | NS | NS | 0.0200 | NS | |
| miR-191/-10b | miR-191/-31 | miR-181b/-10b | miR-181b/200c | miR-191/-200c | |
|---|---|---|---|---|---|
| Diagnostic potency (AUC) | 0.75 | 0.76 | 0.77 | 0.75 | 0.74 |
| Sensitivity (%) | 70.97 | 73.33 | 61.29 | 74.19 | 64.52 |
| Specificity (%) | 79.31 | 79.31 | 72.41 | 75.86 | 86.21 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borisov, E.; Knyazeva, M.; Novak, V.; Zabegina, L.; Prisyazhnaya, T.; Karizkiy, A.; Berlev, I.; Malek, A. Analysis of Reciprocally Dysregulated miRNAs in Eutopic Endometrium Is a Promising Approach for Low Invasive Diagnostics of Adenomyosis. Diagnostics 2020, 10, 782. https://doi.org/10.3390/diagnostics10100782
Borisov E, Knyazeva M, Novak V, Zabegina L, Prisyazhnaya T, Karizkiy A, Berlev I, Malek A. Analysis of Reciprocally Dysregulated miRNAs in Eutopic Endometrium Is a Promising Approach for Low Invasive Diagnostics of Adenomyosis. Diagnostics. 2020; 10(10):782. https://doi.org/10.3390/diagnostics10100782
Chicago/Turabian StyleBorisov, Evgeny, Margarita Knyazeva, Veronika Novak, Lidia Zabegina, Tatyana Prisyazhnaya, Aleksey Karizkiy, Igor Berlev, and Anastasia Malek. 2020. "Analysis of Reciprocally Dysregulated miRNAs in Eutopic Endometrium Is a Promising Approach for Low Invasive Diagnostics of Adenomyosis" Diagnostics 10, no. 10: 782. https://doi.org/10.3390/diagnostics10100782