Recent and Current Advances in FDG-PET Imaging within the Field of Clinical Oncology in NSCLC: A Review of the Literature

Department of Thoracic Surgery, Sagamihara Kyodo Hospital, Kanagawa 252-5188, Japan
Diagnostics 2020, 10(8), 561; https://doi.org/10.3390/diagnostics10080561
Submission received: 3 July 2020
/
Revised: 29 July 2020
/
Accepted: 3 August 2020
/
Published: 5 August 2020
(This article belongs to the Special Issue Role of Radiological Imaging in Cancer Histopathology and Staging)
Abstract
:Lung cancer is the leading cause of cancer-related deaths around the world, the most common type of which is non-small-cell lung cancer (NSCLC). Computed tomography (CT) is required for patients with NSCLC, but often involves diagnostic issues and large intra- and interobserver variability. The anatomic data obtained using CT can be supplemented by the metabolic data obtained using fluorodeoxyglucose F 18 (FDG) positron emission tomography (PET); therefore, the use of FDG-PET/CT for staging NSCLC is recommended, as it provides more accuracy than either modality alone. Furthermore, FDG-PET/magnetic resonance imaging (MRI) provides useful information on metabolic activity and tumor cellularity, and has become increasingly popular. A number of studies have described FDG-PET/MRI as having a high diagnostic performance in NSCLC staging. Therefore, multidimensional functional imaging using FDG-PET/MRI is promising for evaluating the activity of the intratumoral environment. Radiomics is the quantitative extraction of imaging features from medical scans. The chief advantages of FDG-PET/CT radiomics are the ability to capture information beyond the capabilities of the human eye, non-invasiveness, the (virtually) real-time response, and full-field analysis of the lesion. This review summarizes the recent advances in FDG-PET imaging within the field of clinical oncology in NSCLC, with a focus on surgery and prognostication, and investigates the site-specific strengths and limitations of FDG-PET/CT. Overall, the goal of treatment for NSCLC is to provide the best opportunity for long-term survival; therefore, FDG-PET/CT is expected to play an increasingly important role in deciding the appropriate treatment for such patients.
1. Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide [1]. Non-small-cell lung cancer (NSCLC) is the most common type of lung cancer, with subtypes including adenocarcinoma, squamous cell carcinoma, and large cell carcinoma [2]. The optimal management of NSCLC depends on the histological subtype, the molecular characteristics, and the tumor stage [3].
Computed tomography (CT) is the required examination for patients with NSCLC [4]. Moreover, the histological characteristics caused by gene expression and cytokines can affect the imaging appearance either directly or indirectly [5].
Fluorodeoxyglucose F 18 (FDG)-positron emission tomography (PET), which enables tumoral features such as tumor metabolism or receptor expression to be visualized and quantified on a molecular level, has also become more clinically significant in the management of patients with NSCLC [6]. Both FDG-PET alone and that combined with CT (FDG-PET/CT) can combine anatomic data and metabolic information for NSCLC [7]. The anatomic data obtained using CT, including tumor size and location, is supplemented by the metabolic information obtained using FDG-PET. The standardized uptake value (SUV) is a semiquantitative measure of the tracer uptake in a region of interest that normalizes the lesion activity to the injected activity and a measure of the volume of distribution. In general, SUV was calculated as follows: tumor activity concentration/(injected dose/body weight) [8]. It is known that, in NSCLC, the expression of both hexokinase activity and glucose transporter proteins are upregulated [9]. The National Comprehensive Cancer Network (NCCN) guidelines recommend FDG-PET/CT for the evaluation of patients with NSCLC in all stages [10]. The utility of FDG-PET/CT for staging patients with NSCLC is also made reference to in the American College of Radiology Appropriateness Criteria and American College of Chest Physicians guidelines [11,12].
In a prospective, multicenter, randomized trial, conventional work-up combined with FDG-PET resulted in a 51% relative reduction in futile thoracotomy, with an overall one in five reduction in unnecessary surgery, compared with conventional work-up only [13]. In addition, in a large meta-analysis, going beyond unnecessary surgery, FDG-PET was found to have superior mediastinal staging compared with CT [14]. Overall, the combined information obtained from FDG-PET/CT hybrid imaging has been found to provide more accurate staging than either imaging modality alone [15,16,17,18,19].
FDG has become the most common tracer used in PET, owing to a number of favorable characteristics. First, FDG has to use membrane transport proteins, such as glucose transporters [20], because it does not enter tissues passively. Second, phosphorylation makes FDG incapable of export back to the extracellular space. Third, compared with adjacent tissues, the glucose transporters and hexokinase enzymes that phosphorylate and transport FDG are often overexpressed in solid tumors [7]. The high imaging contrast enhances these characteristics in many types of cancer, including NSCLC.
This review focuses on recent advances in FDG-PET imaging within the field of clinical oncology in NSCLC, with a particular emphasis on surgery and prognostication, and investigates the site-specific strengths and limitations of FDG-PET/CT.
2. Association between Maximum SUV (SUVmax) of the Primary Tumor in NSCLC and Pathological Findings and Prognosis
In NSCLC, bronchioloalveolar carcinoma has relatively low FDG uptake, and poorly differentiated carcinoma have been shown to have a wide range of FDG accumulation [21,22]. These findings can be explained by the varying expression levels of glucose transporter-1 and P-glycoprotein [21,22,23]. Accordingly, the World Health Organization updated its NSCLC classification criteria in 2015 [2]. FDG uptake is reported to be heterogeneous in different histological subtypes of lung adenocarcinoma, and several studies have found that histological subtypes are independent predictors of nodal metastasis, recurrence, and survival in patients with lung adenocarcinoma [2,24,25].
However, different conclusions have been reached in previous studies on the prognostic significance of SUVmax in NSCLC. Some have reported that SUVmax is not significantly related to survival in patients with resectable and advanced NSCLC [26,27,28], whereas others have claimed that in early stage NSCLC, preoperative SUVmax is a significant prognostic factor [23,25,29,30,31,32]. Kwon et al. demonstrated that the SUVmax of the primary tumor in stage I NSCLC is predictive of survival and time to recurrence [32]. An analysis of variance demonstrated that the mean SUVmax was significantly lower for adenocarcinoma than for squamous cell carcinoma and other histologies. This parameter may serve as a biomarker to guide selection of patients for adjuvant chemotherapy or other more aggressive therapies. The contrary conclusions in these studies may have been the result of patient selection, tumor stage, or the small numbers of cases. Moreover, differences in terms of the acquisition and interpretation of SUVmax can also produce inconsistent results. Therefore, the standardization of FDG-PET/CT imaging, including patient preparation, image acquisition, image reconstruction, and quantitative image analysis, is needed.
In NSCLC, false negative FDG-PET results tend to be seen in small nodules, most frequently those with a diameter < 8–10 mm, invasive mucinous adenocarcinomas with a reduced amount of cells, and carcinomas with minimally invasive adenocarcinoma and low-grade malignancy such as carcinoma in situ [33], the CT findings of which can manifest as ground-glass or part-solid ground-glass nodules. By contrast, lepidic-predominant invasive adenocarcinomas appear as mixed solid and ground-glass nodules [34]. As reported by MacMahon et al., FDG-PET/CT is indicated for the evaluation of sub-solid ground-glass nodules only if the solid component is > 8 mm [35]. Lepidic adenocarcinomas and solid-type lung cancer lesions < 8–10 mm are reportedly associated with false negative FDG-PET/CT results [36]. Among solid-type lung cancers, lesion size and histopathological findings were associated with FDG uptake [36]. In particular, it warrants attention that lesions ≤2 cm in diameter or solid-types of bronchioloalveolar carcinoma and well-differentiated carcinoma on thin-section CT images have a tendency for negative findings on FDG-PET/CT. Therefore, solid-type nodules should be observed by follow-up CT scans even though the FDG-PET findings are negative.
On the other hand, false positive FDG-PET results in NSCLC are sometimes seen in patients with inflammatory disease caused by inflammation or infection [37]. Feng et al. reported finding a 7% false positive FDG-PET/CT rate in patients with lung cancer, the causes for which included inflammatory pseudotumor (43%), tuberculoma (37%), and organizing pneumonia (6%). In a multivariate analysis, a relationship was found between the false positive rate and higher levels of interleukin-6, positive findings on an interferon-gamma release assay for tuberculosis, age < 50 years, and nondiabetic status [38].
3. Predictive Value of FDG-PET/CT for the Detection of Lymph Node Metastasis in Patients with NSCLC
In patients with NSCLC, lymph nodes > 1 cm in the short axis on CT are considered to show metastatic disease [39]. The nodal status of NSCLC is of particular concern to surgeons because lymph node metastasis is an important determinant of stage and prognosis [40]. However, surgeons sometimes face a discrepancy between the clinical and pathological N status. Even if tumors are diagnosed as clinical N0 (no nodal involvement), based on preoperative radiological findings, microscopic lymph node metastasis is sometimes detected by pathological evaluation after surgery [41,42,43,44,45,46,47,48,49,50,51,52,53,54].
Nodal status remains one of the most important factors in the determination of treatment strategies. As N2 (ipsilateral mediastinal or subcarinal lymphadenopathy) NSCLC is considered a systemic disease, multimodal treatment is suitable for such patients, whereas adjuvant chemotherapy is more suitable for those with N1 (ipsilateral nodes within the lung up to hilar nodes) NSCLC. For optimal treatment, nodal status needs to be diagnosed with high accuracy.
Recent studies have reported finding pathological lymph node metastasis in 6–34% of clinical N0 lung cancer cases (Table 1) [42,43,45,46,47,48,49,50,51,52,53,54,55]. If unexpected N2 metastasis is detected during an operation, lung resection will be justified to the extent that no disease will be left behind [56]. However, if N2 metastasis is detected during the preoperative evaluation, the patient becomes a candidate for multimodal treatment. Because N0 and N2 diseases should have different treatment strategies, the frequency of unexpected N2 lesions should be reduced.
The reported ranges for the sensitivity and specificity of CT for the detection of lymph node metastasis are 51–64% and 74–86%, respectively [57]. FDG-PET/CT has been shown to have a sensitivity of 58–94% and a specificity of 76–96% for the detection of mediastinal lymph node metastasis [58]. The low sensitivity indicates a high possibility of false negative results, which may be due to low FDG uptake in a low-volume malignancy or in a malignancy with a low metabolic rate [59] (Figure 1). Therefore, surgeons cannot conclude that enlarged nodes on CT but negative findings on FDG-PET/CT are truly negative.
According to Wang et al., who carried out a meta-analysis of 10 studies using either FDG-PET/CT or a visual combination of FDG-PET and CT, the negative predictive values for mediastinal lymph node metastases were 94% and 89% in T1 and T2 tumors, respectively [60]. Therefore, invasive mediastinal staging may be omitted for patients with T1 tumors; however, it remains necessary for patients with higher-stage tumors, even if the FDG-PET/CT of the mediastinal lymph nodes is negative [61,62]. The NCCN guidelines recommend pathological and optional pathological mediastinal lymph node evaluation before resection for all stage II and solid tumors < 1 cm or purely nonsolid tumors < 3 cm with no diseased nodes identified on FDG-PET or CT [10,63].
Regarding false positive lymph node metastasis in NSCLC staging with FDG-PET/CT, age > 65 years and non-adenocarcinoma histology have been found to be independent factors for false positive hilar and mediastinal lymph nodes [64]. In addition, nodal involvement with inflammatory lesions, such as sarcoidosis, and with granulomatous infections, such as tuberculosis, can result in false positive findings on FDG-PET, and may be related to the presence of silicosis, emphysema, or interstitial pneumonitis [65,66] (Figure 2).
Based on these findings, patients observed to have enlarged mediastinal lymph nodes on CT, regardless of whether the FDG-PET/CT findings are positive, may be candidates for invasive mediastinal staging [61,67]. Similarly, if no enlarged lymph nodes are found on CT, but the FDG-PET/CT findings in the mediastinal nodes are positive, invasive mediastinal staging is needed. Ghosh et al. reported that CT and FDG-PET/CT may both be falsely negative (CT: 20–25%, FDG-PET/CT: 24–83%) in patients with a central tumor [68]. Therefore, invasive mediastinal staging is especially recommended for patients with central and higher-stage tumors (i.e., evidence of clinical N1 disease).
4. Role of FDG-PET/CT in NSCLC Staging
The significance of the SUVmax on FDG-PET remains controversial [26,27,30,31]. The management of NSCLC depends on the stage, and numerous studies have reported that FDG-PET/CT is highly accurate for tumor–node–metastasis staging in patients with NSCLC [10,69]. FDG-PET/CT may be used in patients with locally advanced NSCLC suitable for treatment with curative intent to identify unsuspected metastases, which can reduce the frequency of futile thoracotomies. Progression-free and overall survival rates have been shown to be significantly worse in upstaged disease using FDG-PET/CT [70]. In NSCLC, cells show altered metabolism and utilize excess glucose as an energy source, and histological factors are modulated by FDG uptake. This method leads to gaining a better understanding of the molecular biology of NSCLC.
Based on the results of a prospective multicenter trial, when FDG-PET/CT was carried out, management strategies changed in approximately 72% of lung cancer cases [71]. In addition, according to the results of a meta-analysis of 56 studies conducted to evaluate the diagnostic value of FDG-PET/CT in NSCLC, the pooled sensitivities and specificities of FDG-PET/CT for identifying mediastinal lymph node metastasis were 72% and 91%, respectively. Moreover, FDG-PET/CT is the first-line modality for evaluating extracranial metastases in patients with NSCLC.
Distant metastases are known to occur in about 11–36% of patients with NSCLC, with the adrenal glands, liver, brain, bones, and abdominal lymph nodes comprising the most common metastatic sites [72]. The pooled sensitivities and specificities of FDG-PET/CT for detecting all extrathoracic metastases have been reported to be 77% and 95%, respectively [73]. Another meta-analysis of nine studies found that FDG-PET/CT had a sensitivity, specificity, and positive predictive value of 93%, 96%, and 28.4%, respectively, and a negative predictive value of 0.08%, for detecting distant metastases [74]. The NCCN guidelines regarding imaging appropriateness recommend that FDG-PET/CT be conducted from the base of the skull to the knees (i.e., whole-body PET/CT) for the evaluation of patients with NSCLC in all stages [10,37]. According to these guidelines, FDG-PET/CT findings confirmed to be positive for distant disease require histological or another type of radiologic confirmation, as does FDG uptake in mediastinal lymph nodes. In patients with advanced stage tumors, to identify abnormal areas that would confer the highest stage, the NCCN guidelines recommend FDG-PET before diagnostic biopsy, as well as FDG-PET/CT for the evaluation of incidentally detected lung nodules measuring >8 mm. A standardized uptake value greater than that of the baseline mediastinal blood pool is considered a positive result on FDG-PET [37,75]. Patients with a single extrathoracic metastatic lesion in a single organ (e.g., the brain, liver, bones, distant lymph nodes, skin, peritoneum, adrenal glands) have been reported to have better survival than patients with multiple extrathoracic lesions, and therefore may be candidates for local ablative therapy or surgical resection. However, in surgical candidates with a single atypical lesion, pathological confirmation is needed [76]. By contrast, the NCCN guidelines do not recommend routine bone scintigraphy for NSCLC staging.
5. Correlation between FDG-PET/CT and Tumor Immunometabolic Phenotypes in NSCLC
A paradigm shift has occurred in the management of NSCLC as a result of recent success in the treatment of locally advanced and metastatic NSCLC with immunotherapy [77,78,79,80]. Some studies have reported finding inverse correlations between tumor glycolytic metabolism and/or FDG uptake and tumor infiltration by effector immune cells [81,82,83]. Mitchell et al. reported identifying an association between elevated FDG retention and highly glycolytic metabolism, the expression of enhanced programmed death-ligand 1 (PD-L1), and an immunosuppressive phenotype in surgically resected NSCLCs [84]. They found that each FDG-PET parameter (SUVmax, SUVtotal, SUVmean, Total lesion glycolysis) was positively correlated with tumor expression of glycolysis-related genes. Elevated FDG SUVmax was more discriminatory of glycolysis-associated changes in tumor immune phenotypes than other FDG-PET parameters. Increased SUVmax was associated with multiple immune factors characteristic of an immunosuppressive and poorly immune infiltrated tumor microenvironment, including elevated PD-L1 expression, reduced CD57+ cell density, and increased T cell exhaustion gene signature. Elevated SUVmax identified immune-related transcriptomic signatures that were associated with enhanced tumor glycolytic gene expression and poor clinical outcomes. Their findings suggest that in patients with resectable NSCLC, FDG-PET could serve as a noninvasive clinical indicator of tumor metabolic and immune phenotypes. In addition, Faubert et al. provided direct evidence that the uptake of tumor cell-autonomous lactate, but not glucose, is a major contributor to central metabolism in human NSCLCs with high FDG-PET uptake and aggressive oncological behavior [85]. Further studies are needed to uncover more details about the contributions of immune and cancer cells to the intratumoral metabolic phenotype. Therefore, additional investigations in larger cohorts are needed to characterize fully the immunometabolic differences between NSCLC histologic subtypes, disease stages, tumor genomic features, and previous therapies, as well as the effect of these differences on the noninvasive assessment of tumor phenotypes based on FDG uptake.
6. FDG-PET/Magnetic Resonance Imaging (MRI)
FDG-PET/MRI technology, which can provide useful information regarding metabolic activity and tumor cellularity simultaneously, has become increasingly available. FDG-PET/MRI is a hybrid imaging modality that offers high quality morphological and functional imaging and reduces radiation exposure in comparison to FDG-PET/CT at the same time. FDG-PET/MRI is expected to be superior to FDG-PET/CT due to the superior detectability of pleural and mediastinal involvement with MRI and due to high sensitivity for the detection of brain, liver and bone metastases [86,87]. Thus, FDG-PET/MRI may be advantageous compared to FDG-PET/CT when assessing advanced tumors of the chest, both with regard to local staging accuracy and radiation dose management. For prognostic evaluation as well as tumor response assessment, the combination of metabolic information depicted by FDG-PET and functional MR imaging biomarkers could excel currently used imaging methods [88,89]. A number of studies have recently described FDG-PET/MRI as having an equivalently high diagnostic performance in staging of NSCLC [90,91,92]. Schaarschmidt et al. reported that despite the variability of FDG-PET/CT and FDG-PET/MRI in tumor, node, metastasis (TNM) staging, both modalities lead to comparable therapeutic decisions in NSCLC patients. Hence, FDG-PET/MRI can be considered a possible alternative to FDG-PET/CT for clinical NSCLC staging. These studies suggest that multidimensional functional imaging using FDG-PET/MRI is a promising method for evaluating the activity of the intratumoral environment. Still, the introduction of FDG-PET/MRI in clinical practice is hindered by several reasons. Apart from the obvious advantages of FDG-PET/CT such as the high availability and widespread experience of radiologists and nuclear medicine physicians or the shorter acquisition time if nonoptimized FDG-PET/MRI protocols are used, the sensitivity of FDG-PET/MRI for the detection of pulmonary nodules is still a matter of ongoing debate. A validation cohort in a larger population is needed to confirm these findings and establish the utility of FDG-PET/MRI.
7. FDG-PET/CT Radiomics and Radiogenomics
Radiomics is quantitative extraction of imaging features from medical scans. It is believed that radiomics has the potential to improve on traditional, manual interpretation by detecting features and patterns that otherwise would go unnoticed to the human eye [93,94]. By leveraging on large datasets and artificial intelligence techniques, radiomics could help predict the type of disease, survival, and response to therapy [95,96]. There are also a number of logistic advantages in this approach, such as providing nearly real-time results and not requiring any invasive procedure for the patient [97]. The overall objective of radiomics is to build classification and/or regression models based on some quantitative features extracted from the imaging data. The typical workflow in radiomics is rather independent of the underlying disease and consists of six sequential steps (acquisition, pre-processing, segmentation, feature extraction, post-processing, data analysis) [98]. Many recent studies have consistently emphasized the potential advantages of FDG-PET/CT radiomics in lung cancer [99]. The results available in the literature are undoubtedly promising, but they also need to be considered with care. The lack of reproducibility, for instance, is a well-known problem in radiomics, and is mostly a consequence of the absence of standardized methods and settings in all the steps of the workflow [98,100]. A number of studies also suffer from serious limitations at the validation level, among them improper statistical analysis and/or the absence of an independent validation dataset to confirm the results. This may easily lead to biased discovery rates and inflation of type-I errors, as correctly pointed out in [101]. As of now, the evidence of the superiority of radiomics beyond standard imaging analysis tools including SUV, kinetic data, etc. is yet to be confirmed. The availability of large, possibly multi-center, image datasets is crucial for the development and validation of radiomics methods. On the other hand, for NSCLC patients, radiomics studies have shown that several CT and FDG-PET/CT image features can predict mutation status. Ninatti et al. reported the current state of the art of imaging-derived biomarkers predictive of genetic alterations in NSCLC by using a systematic literature review [102]. CT and FDG-PET imaging-derived radiomic features, convolutional neural networks (CNN)-based approaches, FDG-PET parameters, and visual qualitative CT features were tested for the prediction of actionable mutations. Most of the published studies were focused on epidermal growth factor receptor (EGFR) alterations, which are the most commonly encountered actionable mutations in clinical practice, being present in 40–50% and 10–20% of NSCLC patients of Asian and non-Asian ethnicity, respectively [103,104,105]. The imaging-based predictive models were able to predict EGFR status, with performances ranging from poor (area under the curve (AUC) = 0.6 to 0.7, n = 5) to acceptable (AUC = 0.7 to 0.8, n = 11), excellent (AUC = 0.8 to 0.9, n = 18), and outstanding (AUC > 0.90, n = 1) in the validation set. However, the AUC of a model is not itself informative, since many other significant items, each contributing for a predetermined rate, account for the reliability of a study. Positive outcomes were also reported for the prediction of other molecular alterations, including anaplastic lymphoma kinase (ALK) rearrangement and ALK/proto-oncogene 1 (ROS1)/rearranged during transfection (RET) fusions. However, very few studies have been published with this aim, and more advanced image analyses are thus needed to confirm these preliminary results. The predictive potential of FDG-PET parameters and visual qualitative features was investigated. Zhang et al. found that a lower peak standardized uptake value (SUVpeak) was associated with EGFR mutations, while spiculation, the absence of emphysema, pleural indentation and the subsolid nodule were the semantic CT features most commonly associated with EGFR mutations [106]. However, there are no standardized definitions for visual qualitative features, and this may affect the reproducibility of results. Radiomics provides objective, repeatable and quantitative assessments. On the other hand, the possibility of analyzing images with “intelligent” methods (e.g., unsupervised), and the development of strategies to address the “black-box” and accountability issues make CNN-based approaches even more attractive in the field of medical imaging [107]. Reported results suggest that combining different methods for image biomarker extraction may help to improve the predictive performances of the models and be a winning strategy towards their implementation into clinical practice. Particularly useful were the combinations of (1) CT and FDG-PET radiomic features and FDG-PET parameters; (2) CT radiomic features and visual qualitative CT features; and (3) CT radiomic features and CNN-based approaches. The potential of combined models, therefore, needs to be investigated further with future studies. Moreover, the importance of adding clinical features to improve the performance of imaging-based predictive models must be underlined. For example, most of the included studies reported a statistically significant association of the female sex and non-smoking status with EGFR mutation. These findings were consistent with large-scale molecular epidemiological investigations that were done in patients affected by NSCLC [105,108]. Nonetheless, they did not find common, reliable radiomic features among the studies. This finding may be related to the different tools applied for feature calculation and different approaches to data analysis. Despite the promising results in terms of predictive performance, image-based models suffering from methodological bias require further validation before replacing traditional molecular pathology testing.
8. Conclusions
This review summarizes the recent advances in FDG-PET imaging within the field of clinical oncology in NSCLC. In terms of an overall strategy, the goal of NSCLC treatment is to provide the best opportunity for long-term survival. In that sense, FDG-PET/CT plays a very important role in deciding the appropriate treatment for patients with NSCLC. Additional multicenter prospective studies with larger cohorts and randomized controlled trials with comparator arms are needed to guide clinical management of patients with NSCLC.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflict of interest.
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. WHO Panel. The 2015 World Health Organization classification of lung tumors: Impact of genetic, clinical and radiologic advances since the 2004 classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zappa, C.; Mousa, S.A. Non-small cell lung cancer: Current treatment and future advances. Transl. Lung Cancer Res. 2016, 3, 288–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aokage, K.; Miyoshi, T.; Ishii, G.; Kusumoto, M.; Nomura, S.; Katsumata, S.; Sekihara, K.; Hishida, T.; Tsuboi, M. Clinical and Pathological Staging Validation in the Eighth Edition of the TNM Classification for Lung Cancer: Correlation between Solid Size on Thin-Section Computed Tomography and Invasive Size in Pathological Findings in the New T Classification. J. Thorac. Oncol. 2017, 12, 1403–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Q.; Fen, Z.; Liang, Q.; Li, M.; Deng, J.; Ma, M.; Wang, W.; Liu, J.; Liu, P.; Rong, P. Machine learning-based radiomics strategy for prediction of cell proliferation in non-small cell lung cancer. Eur. J. Radiol. 2019, 118, 32–37. [Google Scholar] [CrossRef]
- Steinert, H.C. PET and PET-CT of lung cancer. Methods Mol. Biol. 2011, 727, 33–51. [Google Scholar]
- Gambhir, S.S. Molecular imaging of cancer with positron emission tomography. Nat. Rev. Cancer 2002, 2, 683–693. [Google Scholar] [CrossRef]
- Shankar, L.K.; Hoffman, J.M.; Bacharach, S.; Graham, K.M.; Karp, J.; Lammertsma, A.A.; Larson, S.; Mankoff, D.A.; Siegel, B.A.; Abbeele, A.V.; et al. Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute Trials. J. Nucl. Med. 2006, 47, 1059–1066. [Google Scholar]
- Nelson, C.A.; Wang, J.Q.; Leav, I.; Crane, P.D. The interaction among glucose transport, hexokinase, and glucose-6-phosphatase with respect to 3H-2-deoxyglucose retention in murine tumor models. Nucl. Med. Biol. 1996, 23, 533–541. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.; Chirieac, L.R.; D’Amico, T.A.; DeCamp, M.M.; Dilling, T.J.; Dobelbower, M.; et al. Non–small cell lung cancer, version 5.2017: Clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 2017, 15, 504–535. [Google Scholar] [CrossRef]
- Silvestri, G.A.; Gonzalez, A.V.; Jantz, M.A.; Margolis, M.L.; Gould, M.K.; Tanoue, L.T.; Harris, L.J.; Detterbeck, F.C. Methods for staging non-small cell lung cancer: Diagnosis and management of lung cancer: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e211S–e250S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravenel, J.G.; Rosenzweig, K.E.; Kirsch, J.; Ginsburg, M.E.; Kanne, J.P.; Kestin, L.L.; Parker, J.A.; Rimner, A.; Saleh, A.G.; Mohammed, T.H. ACR Appropriateness Criteria non-invasive clinical staging of bronchogenic carcinoma. J. Am. Coll. Radiol. 2014, 11, 849–856. [Google Scholar] [CrossRef] [PubMed]
- van Tinteren, H.; Hoekstra, O.S.; Smit, E.F.; van den Bergh, J.; Schreurs, A.J.M.; Stallaert, R.A.L.M.; van Velthoven, P.C.; Comans, E.F.I.; Diepenhorst, F.W.; Verboom, P.; et al. Effectiveness of positron emission tomography in the preoperative assessment of patients with suspected non-small-cell lung cancer: The PLUS multicentre randomised trial. Lancet 2002, 359, 1388–1392. [Google Scholar] [CrossRef]
- Gould, M.K.; Kuschner, W.G.; Rydzak, C.E.; Maclean, C.C.; Demas, A.N.; Shigemitsu, H.; Chan, J.K.; Owens, D.K. Test performance of positron emission tomography and computed tomography for mediastinal staging in patients with non–small-cell lung cancer: A meta-analysis. Ann. Intern. Med. 2003, 139, 879–892. [Google Scholar] [CrossRef]
- Antoch, G.; Stattaus, J.; Nemat, A.T.; Marnitz, H.; Beyer, T.; Kuehl, H.; Bockisch, A.; Debatin, J.F.; Freudenberg, L.S. Non–small cell lung cancer: Dual-modality PET/CT in preoperative staging. Radiology 2003, 229, 526–533. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Ojha, B.; Bryant, A.S.; Raghuveer, V.; Mountz, J.M.; Bartolucci, A.A. The accuracy of integrated PET-CT compared with dedicated PET alone for the staging of patients with nonsmall cell lung cancer. Ann. Thorac. Surg. 2004, 78, 1017–1023. [Google Scholar] [CrossRef]
- De Wever, W.; Ceyssens, S.; Mortelmans, L.; Stroobants, S.; Marchal, G.; Bogaert, J.; Verschakelen, J.A. Additional value of PET-CT in the staging of lung cancer: Comparison with CT alone, PET alone and visual correlation of PET and CT. Eur. Radiol. 2007, 17, 23–32. [Google Scholar] [CrossRef]
- Lardinois, D.; Weder, W.; Hany, T.F.; Kamel, E.M.; Korom, S.; Seifert, B.; von Schulthess, G.K.; Steinert, H.C. Staging of non–small-cell lung cancer with integrated positron-emission tomography and computed tomography. N. Engl. J. Med. 2003, 348, 2500–2507. [Google Scholar] [CrossRef] [Green Version]
- Shim, S.S.; Lee, K.S.; Kim, B.T.; Chung, M.J.; Lee, E.J.; Han, J.; Choi, J.Y.; Kwon, O.J.; Shim, Y.M.; Kim, S. Non–small cell lung cancer: Prospective comparison of integrated FDG PET/CT and CT alone for preoperative staging. Radiology 2005, 236, 1011–1019. [Google Scholar] [CrossRef]
- Goodwin, J.; Neugent, M.L.; Lee, S.Y.; Choe, J.H.; Choi, H.; Jenkins, D.M.R.; Ruthenborg, R.J.; Robinson, M.W.; Jeong, J.Y.; Wake, M.; et al. The distinct metabolic phenotype of lung squamous cell carcinoma defines selective vulnerability to glycolytic inhibition. Nat. Commun. 2017, 8, 15503. [Google Scholar] [CrossRef]
- Song, Y.S.; Lee, W.W.; Chung, J.H.; Park, S.Y.; Kim, Y.K.; Kim, S.E. Correlation between FDG uptake and glucose transporter type 1 expression in neuroendocrine tumors of the lung. Lung Cancer 2008, 61, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Khandani, A.H.; Whitney, K.D.; Keller, S.M.; Isasi, C.R.; Blaufox, M.D. Sensitivity of FDG PET, GLUT1 expression and proliferative index in bronchioloalveolar lung cancer. Nucl. Med. Commun. 2007, 28, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Jadvar, H.; Alavi, A.; Gambhir, S.S. 18F-FDG uptake in lung, breast, and colon cancers: Molecular biology correlates and disease characterization. J. Nucl. Med. 2009, 50, 1820–1827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Jian, H.; Shen, L.; Zhu, L.; Luet, S. Lymph node involvement influenced by lung adenocarcinoma subtypes in tumor size ≤3 cm disease: A study of 2268 cases. Eur. J. Surg. Oncol. 2016, 42, 1714–1719. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, H.; Kadota, K.; Chaft, J.E.; Buitrago, D.; Sima, C.S.; Lee, M.-C.; Huang, J.; Travis, W.D.; Rizk, N.P.; Rudin, C.M.; et al. Solid predominant histologic subtype in resected stage I lung adenocarcinoma is an independent predictor of early, extrathoracic, multisite recurrence and of poor postrecurrence survival. J. Clin. Oncol. 2015, 33, 2877–2884. [Google Scholar] [CrossRef] [PubMed]
- Downey, R.J.; Akhurst, T.; Gonen, M.; Park, B.; Rusch, V. Fluorine-18 fluorodeoxyglucose positron emission tomographic maximal standardized uptake value predicts survival independent of clinical but not pathologic TNM staging of resected non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2007, 133, 1419–1427. [Google Scholar] [CrossRef] [Green Version]
- Vesselle, H.; Freeman, J.D.; Wiens, L.; Stern, J.; Nguyen, H.Q.; Hawes, S.E.; Bastian, P.; Salskov, A.; Vallières, E.; Wood, D.E. Fluorodeoxyglucose uptake of primary non-small cell lung cancer at positron emission tomography: New contrary data on prognostic role. Clin. Cancer Res. 2007, 13, 3255–3263. [Google Scholar] [CrossRef] [Green Version]
- Hoang, J.K.; Hoagland, L.F.; Coleman, R.E.; Coan, A.D.; Herndon, J.E., 2nd; Patz, E.F., Jr. Prognostic value of fluorine-18 fluorodeoxyglucose positron emission tomography imaging in patients with advanced-stage non-small-cell lung carcinoma. J. Clin. Oncol. 2008, 26, 1459–1464. [Google Scholar] [CrossRef]
- Higashi, K.; Ueda, Y.; Yagishita, M.; Arisaka, Y.; Sakurai, A.; Oguchi, M.; Seki, H.; Nambu, Y.; Tonami, H.; Yamamoto, I. FDG PET measurement of the proliferative potential of non-small cell lung cancer. J. Nucl. Med. 2000, 41, 85–92. [Google Scholar]
- Higashi, K.; Ueda, Y.; Arisaka, Y.; Sakuma, T.; Nambu, Y.; Oguchi, M.; Seki, H.; Taki, S.; Tonami, H.; Yamamoto, I. 18F-FDG uptake as a biologic prognostic factor for recurrence in patients with surgically resected non-small cell lung cancer. J. Nucl. Med. 2002, 43, 39–45. [Google Scholar]
- Higashi, K.; Ito, K.; Hiramatsu, Y.; Ishikawa, T.; Sakuma, T.; Matsunari, I.; Kuga, G.; Miura, K.; Higuchi, T.; Tonami, H.; et al. 18F-FDG uptake by primary tumor as a predictor of intratumoral lymphatic vessel invasion and lymph node involvement in non-small cell lung cancer: Analysis of a multicenter study. J. Nucl. Med. 2005, 46, 267–273. [Google Scholar] [PubMed]
- Kwon, W.; Howard, B.A.; Herndon, J.E.; Patz, E.F., Jr. FDG uptake on positron emission tomography correlates with survival and time to recurrence in patients with stage I non-small-cell lung cancer. J. Thorac. Oncol. 2015, 10, 897–902. [Google Scholar] [CrossRef] [Green Version]
- Greenspan, B.S. Role of PET/CT for precision medicine in lung cancer: Perspective of the Society of Nuclear Medicine and Molecular Imaging. Transl. Lung Cancer Res. 2017, 6, 617–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Park, C.M.; Koh, J.M.; Lee, S.M.; Goo, J.M. Pulmonary subsolid nodules: What radiologists need to know about the imaging features and management strategy. Diagn. Interv. Radiol. 2014, 20, 47–57. [Google Scholar] [CrossRef] [PubMed]
- MacMahon, H.; Naidich, D.P.; Goo, J.M.; Lee, K.S.; Leung, A.N.C.; Mayo, J.R.; Mehta, A.C.; Ohno, Y.; Powell, C.A.; Prokop, M.; et al. Guidelines for management of incidental pulmonary nodules detected on CT images: From the Fleischner Society 2017. Radiology 2017, 284, 228–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwano, S.; Ito, S.; Tsuchiya, K.; Kato, K.; Naganawa, S. What causes false-negative PET findings for solid-type lung cancer? Lung Cancer 2013, 79, 132–136. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Imaging Appropriate Use Criteria (NCCN Imaging AUC™). National Comprehensive Cancer Network Website. Available online: https://triticeaetoolbox.org/ (accessed on 4 July 2020).
- Feng, M.; Yang, X.; Ma, Q.; He, Y. Retrospective analysis for the false positive diagnosis of PET-CT scan in lung cancer patients. Medicine 2017, 96, e7415. [Google Scholar] [CrossRef]
- Birim, O.; Kappetein, A.P.; Stijnen, T.; Bogers, A.J.J.C. Meta-analysis of positron emission tomographic and computed tomographic imaging in detecting mediastinal lymph node metastases in nonsmall cell lung cancer. Ann. Thorac. Surg. 2005, 79, 375–382. [Google Scholar] [CrossRef]
- Asamura, H.; Chansky, K.; Crowley, J.; Goldstraw, P.; Rusch, V.W.; Vansteenkiste, J.F.; Watanabe, H.; Wu, Y.-L.; Zielinski, M.; Ball, D.; et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for the revision of the N descriptors in the forthcoming 8th Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2015, 10, 1675–1684. [Google Scholar] [CrossRef] [Green Version]
- Ye, B.; Cheng, M.; Li, W.; Ge, X.-X.; Geng, J.-F.; Feng, J.; Yang, Y.; Hu, D.-Z. Predictive factors for lymph node metastasis in clinical stage IA lung adenocarcinoma. Ann. Thorac. Surg. 2014, 98, 217–223. [Google Scholar] [CrossRef]
- Koike, T.; Koike, T.; Yamato, Y.; Yoshiya, K.; Toyabe, S. Predictive risk factors for mediastinal lymph node metastasis in clinical stage IA non-small-cell lung cancer patients. J. Thorac. Oncol. 2012, 7, 1246–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.; Song, I.H.; Yang, H.C.; Kim, K.; Jheon, S. Predictive factors for node metastasis in patients with clinical stage I non-small cell lung cancer. Ann. Thorac. Surg. 2013, 96, 239–245. [Google Scholar] [CrossRef]
- Tsutani, Y.; Miyata, Y.; Nakayama, H.; Okumura, S.; Adachi, S.; Yoshimura, M.; Okada, M. Prediction of pathologic node-negative clinical stage IA lung adenocarcinoma for optimal candidates undergoing sublobar resection. J. Thorac. Cardiovasc. Surg. 2012, 144, 1365–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez-Caro, A.; Boada, M.; Cabanas, M.; Sanchez, M.; Arguis, P.; Lomeña, F.; Ramirez, J.; Molins, L. False-negative rate after positron emission tomography/computer tomography scan for mediastinal staging in cI stage non-small-cell lung cancer. Eur. J. Cardiothorac. Surg. 2012, 42, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, M.; Nakayama, H.; Okumura, S.; Daisaki, H.; Adachi, S.; Yoshimura, M.; Miyata, Y. Multicenter analysis of high-resolution computed tomography and positron emission tomography/computed tomography findings to choose therapeutic strategies for clinical stage IA lung adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2011, 141, 1384–1391. [Google Scholar] [CrossRef] [Green Version]
- Takenaka, T.; Yano, T.; Morodomi, Y.; Ito, K.; Miura, N.; Kawano, D.; Shoji, F.; Baba, S.; Abe, K.; Honda, H.; et al. Prediction of true-negative lymph node metastasis in clinical IA non-small cell lung cancer by measuring standardized uptake values on positron emission tomography. Surg. Today 2012, 42, 934–939. [Google Scholar] [CrossRef]
- Miyasaka, Y.; Suzuki, K.; Takamochi, K.; Matsunaga, T.; Oh, S. The maximum standardized uptake value of fluorodeoxyglucose positron emission tomography of the primary tumour is a good predictor of pathological nodal involvement in clinical N0 non-small-cell lung cancer. Eur. J. Cardiothorac Surg. 2013, 44, 83–87. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Sun, Y.; Xiang, J.; Zhang, Y.; Hu, H.; Chen, H. A prediction model for N2 disease in T1 non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2012, 144, 1360–1364. [Google Scholar] [CrossRef] [Green Version]
- Tsutani, Y.; Murakami, S.; Miyata, Y.; Nakayama, H.; Yoshimura, M.; Okada, M. Prediction of lymph node status in clinical stage IA squamous cell carcinoma of the lung. Eur. J. Cardiothorac. Surg. 2015, 47, 1022–1026. [Google Scholar] [CrossRef] [Green Version]
- Bao, F.; Yuan, P.; Yuan, X.; Lv, X.; Wang, Z.; Hu, J. Predictive risk factors for lymph node metastasis in patients with small size non-small cell lung cancer. J. Thorac. Dis. 2014, 6, 1697–1703. [Google Scholar]
- Shiono, S.; Yanagawa, N.; Abiko, M.; Sato, T. Detection of non-aggressive stage IA lung cancer using chest computed tomography and positron emission tomography/computed tomography. Interact Cardiovasc Thorac. Surg. 2014, 19, 637–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, B.; Cheng, M.; Ge, X.X.; Geng, J.-F.; Li, W.; Feng, J.; Hu, D.-Z.; Zhao, H. Factors that predict lymph node status in clinical stage T1aN0M0 lung adenocarcinomas. World J. Surg. Oncol. 2014, 12, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Jiang, W.; Zhan, C.; Shi, Y.; Zhang, Y.; Lin, Z.; Yuan, Y.; Wang, Q. Lymph node metastasis in clinical stage IA peripheral lung cancer. Lung Cancer 2015, 90, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Kaseda, K.; Asakura, K.; Kazama, A.; Ozawa, Y. Risk factors for predicting occult lymph node metastasis in patients with clinical stage I non-small cell lung cancer staged by integrated fluorodeoxyglucose positron emission tomography/computed tomography. World J. Surg. 2016, 40, 2976–2983. [Google Scholar] [CrossRef] [PubMed]
- Detterbeck, F. What to do with “Surprise” N2?: Intraoperative management of patients with non-small cell lung cancer. J. Thorac. Oncol. 2008, 3, 289–302. [Google Scholar] [CrossRef] [Green Version]
- Walker, C.M.; Chung, J.H.; Abbott, G.F.; Little, B.P.; El-Sherief, A.H.; Shepard, J.-A.O.; Lanuti, M. Mediastinal lymph node staging: From noninvasive to surgical. AJR Am. J. Roentgenol. 2012, 199, W54–W64. [Google Scholar] [CrossRef]
- Schimmer, C.; Neukam, K.; Elert, O. Staging of non-small cell lung cancer: Clinical value of positron emission tomography and mediastinoscopy. Interact. Cardiovasc. Thorac. Surg. 2006, 5, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Hansen, M.; Baldwin, D.R.; Hasler, E.; Zamora, J.; Abraira, V.; Figuls, M.R.I. PET-CT for assessing mediastinal lymph node involvement in patients with suspected resectable non-small cell lung cancer. Cochrane Database Syst. Rev. 2014, 2014, CD009519. [Google Scholar] [CrossRef]
- Wang, J.; Welch, K.; Wang, L.; Kong, F.-M.S. Negative predictive value of positron emission tomography and computed tomography for stage T1-2N0 non-small-cell lung cancer: A meta-analysis. Clin. Lung Cancer 2012, 13, 81–89. [Google Scholar] [CrossRef] [Green Version]
- PEBC guideline 17-6 Invasive Mediastinal Staging. Available online: www.cancercare.ontario/en/guidelines-advice (accessed on 4 July 2020).
- Darling, G.E.; Maziak, D.E.; Inculet, R.I.; Gulenchyn, K.Y.; Driedger, A.A.; Ung, Y.C.; Gu, C.-S.; Kuruvilla, M.S.; Cline, K.J.; Julian, J.A.; et al. Positron emission tomography-computed tomography compared with invasive mediastinal staging in non-small cell lung cancer: Results of mediastinal staging in the early lung positron emission tomography trial. J. Thorac. Oncol. 2011, 6, 1367–1372. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.J.; Kim, A.W.; Puchalski, J.T.; Bramley, K.; Detterbeck, F.C.; Boffa, D.J.; Decker, R.H. Indications for invasive mediastinal staging in patients with early non-small cell lung cancer staged with PET-CT. Lung Cancer 2017, 109, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zheng, Q.; Ma, Y.; Wang, Y.; Feng, Y.; Zhao, B.; Yang, Y. Implications of false negative and false positive diagnosis in lymph node staging of NSCLC by means of FDG PET/CT. PLoS ONE 2013, 8, e78552. [Google Scholar] [CrossRef] [PubMed]
- Konishi, J.; Yamazaki, K.; Tsukamoto, E.; Tamaki, N.; Onodera, Y.; Otake, T.; Morikawa, T.; Kinoshita, I.; Dosaka-Akita, H.; Nishimura, M. Mediastinal lymph node staging by FDG-PET in patients with non-small cell lung cancer: Analysis of false-positive FDG-PET findings. Respiration 2003, 70, 500–506. [Google Scholar] [CrossRef]
- Betancourt-Cuellar, S.L.; Carter, B.W.; Palacio, D.; Erasmus, J.J. Pitfalls and limitations in non-small cell lung cancer staging. Semin. Roentgenol. 2015, 50, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Al-Sarraf, N.; Gately, K.; Lucey, J.; Wilson, L.; McGovern, E.; Young, V. Lymph node staging by means of positron emission tomography is less accurate in non-small cell lung cancer patients with enlarged lymph nodes: Analysis of 1145 lymph nodes. Lung Cancer 2008, 60, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Nanjiah, P.; Dunning, J. Should all patients with non-small cell lung cancer who are surgical candidates have cervical mediastinoscopy preoperatively? Interact. Cardiovasc. Thorac. Surg. 2006, 5, 20–24. [Google Scholar] [CrossRef]
- Juweid, M.E.; Cheson, B.D. Positron-emission tomography and assessment of cancer therapy. N. Engl. J. Med. 2006, 354, 496–507. [Google Scholar] [CrossRef]
- Takeuchi, S.; Khiewvan, B.; Fox, P.S.; Swisher, S.G.; Rohren, E.M.; Bassett, R.L., Jr.; Macapinlac, H.A. Impact of initial PET/CT staging in terms of clinical stage, management plan, and prognosis in 592 patients with non-small-cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 906–914. [Google Scholar] [CrossRef]
- Kubota, K.; Matsuno, S.; Morioka, N.; Adachi, S.; Koizumi, M.; Seto, H.; Kojo, M.; Nishioka, S.; Nishimura, M.; Yamamoto, H. Impact of FDG-PET findings on decisions regarding patient management strategies: A multicenter trial in patients with lung cancer and other types of cancer. Ann. Nucl. Med. 2015, 29, 431–441. [Google Scholar] [CrossRef] [Green Version]
- Erasmus, J.J.; Macapinlac, H.A.; Swisher, S.G. Positron emission tomography imaging in nonsmall-cell lung cancer. Cancer 2007, 110, 2155–2168. [Google Scholar] [CrossRef]
- Wu, Y.; Li, P.; Zhang, H.; Shi, Y.; Wu, H.; Zhang, J.; Qian, Y.; Li, C.; Yang, J. Diagnostic value of fluorine 18 fluorodeoxyglucose positron emission tomography/computed tomography for the detection of metastases in non-small-cell lung cancer patients. Int. J. Cancer. 2013, 132, E37–E47. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xu, W.; Kong, F.; Sun, X.; Zuo, X. Meta-analysis: Accuracy of 18FDG PET-CT for distant metastasis staging in lung cancer patients. Surg. Oncol. 2013, 22, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Vansteenkiste, J.F.; Stroobants, S.G.; De Leyn, P.R.; Dupont, P.J.; Bogaert, J.; Maes, A.; Deneffe, G.J.; Nackaerts, K.L.; Verschakelen, J.A.; Lerut, T.E.; et al. Lymph node staging in non-small-cell lung cancer with FDG-PET scan: A prospective study on 690 lymph node stations from 68 patients. J. Clin. Oncol. 1998, 16, 2142–2149. [Google Scholar] [CrossRef] [PubMed]
- Varela, G.; Thomas, P.A. Surgical management of advanced non-small cell lung cancer. J. Thorac. Dis. 2014, 6, S217–S223. [Google Scholar]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced squamous-cell non–small-cell lung cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [Green Version]
- Forde, P.M.; Chaft, J.E.; Smith, K.N.; Anagnostou, V.; Cottrell, T.R.; Hellmann, M.D.; Zahurak, M.; Yang, S.C.; Jones, D.R.; Broderick, S.; et al. Neoadjuvant PD-1 blockade in resectable lung cancer. N. Engl. J. Med. 2018, 378, 1976–1986. [Google Scholar] [CrossRef]
- Kwon, H.R.; Pahk, K.; Park, S.; Kwon, H.W.; Kim, S. Prognostic value of metabolic information in advanced gastric cancer using preoperative (18)F-FDG PET/CT. Nucl. Med. Mol. Imaging 2019, 53, 386–395. [Google Scholar] [CrossRef]
- Brand, A.; Singer, K.; Koehl Gudrun, E.; Kolitzus, M.; Schoenhammer, G.; Thiel, A.; Matos, C.; Bruss, C.; Klobuch, S.; Peter, K.; et al. LDHA-associated lactic acid production blunts tumor immunosurveillance by T and NK cells. Cell Metab. 2016, 24, 657–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopci, E.; Toschi, L.; Grizzi, F.; Rahal, D.; Olivari, L.; Castino, G.F.; Marchetti, S.; Cortese, N.; Qehajaj, D.; Pistillo, D.; et al. Correlation of metabolic information on FDG-PET with tissue expression of immune markers in patients with non-small cell lung cancer (NSCLC) who are candidates for upfront surgery. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, K.G.; Amini, B.; Wang, Y.; Carter, B.W.; Godoy, M.C.B.; Parra, E.R.; Behrens, C.; Villalobos, P.; Reuben, A.; Lee, J.J.; et al. 18F-fluorodeoxyglucose positron emission tomography correlates with tumor immunometabolic phenotypes in resected lung cancer. Cancer Immunol. Immunother 2020, 69, 1519–1534. [Google Scholar] [CrossRef] [PubMed]
- Faubert, B.; Li, K.Y.; Cai, L.; Hensley, C.T.; Kim, J.; Zacharias, L.G.; Yang, C.; Do, Q.N.; Doucette, S.; Burguete, D.; et al. Lactate metabolism in human lung tumors. Cell 2017, 171, 358–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landwehr, P.; Schulte, O.; Lackner, K. MR imaging of the chest: Mediastinum and chest wall. Eur. Radiol. 1999, 9, 1737–1744. [Google Scholar] [CrossRef]
- Beiderwellen, K.; Huebner, M.; Heusch, P.; Grueneisen, J.; Ruhlmann, V.; Nensa, F.; Kuehl, H.; Umutlu, L.; Rosenbaum-Krumme, S.; Lauenstein, T.C. Whole-body [18F] FDG PET/MRI vs. PET/CT in the assessment of bone lesions in oncological patients: Initial results. Eur. Radiol. 2014, 24, 2023–2030. [Google Scholar] [CrossRef]
- Gatidis, S.; Schmidt, H.; Claussen, C.D.; Schwenzer, N.F. Multiparametrische Bildgebung mittels simultaner MR/PET. Radiology 2013, 53, 669–675. [Google Scholar] [CrossRef]
- Schmidt, H.; Brendle, C.; Schraml, C.; Martirosian, P.; Bezrukov, I.; Hetzel, J.; Müller, M.; Sauter, A.; Claussen, C.D.; Pfannenberg, C.; et al. Correlation of simultaneously acquired diffusion-weighted imaging and 2-Deoxy-[18F] fluoro-2-D-glucose positron emission tomography of pulmonary lesions in a dedicated whole-body magnetic resonance/positron emission tomography system. Investig. Radiol. 2013, 48, 247–255. [Google Scholar] [CrossRef]
- Kirchner, J.; Sawicki, L.M.; Nensa, F.; Schaarschmidt, B.M.; Reis, H.; Ingenwerth, M.; Bogner, S.; Aigner, C.; Buchbender, C.; Umutlu, L.; et al. Prospective comparison of 18 F-FDG PET/MRI and 18 F-FDG PET/CT for thoracic staging of non-small cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 437–445. [Google Scholar] [CrossRef]
- Schaarschmidt, B.; Buchbender, C.; Gomez, B.; Rubbert, C.; Hild, F.; Köhler, J.; Grueneisen, J.; Reis, H.; Ruhlmann, V.; Wetter, A.; et al. Thoracic staging of non-small-cell lung cancer using integrated (18)F-FDG PET/MR imaging: Diagnostic value of different MR sequences. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1257–1267. [Google Scholar] [CrossRef]
- Schaarschmidt, B.M.; Grueneisen, J.; Metzenmacher, M.; Gomez, B.; Gauler, T.; Roesel, C.; Heusch, P.; Ruhlmann, V.; Umutlu, L.; Antoch, G.; et al. Thoracic staging with 18F-FDG PET/MR in non-small cell lung cancer–does it change therapeutic decisions in comparison to 18F-FDG PET/CT? Eur. Radiol. 2017, 27, 681–688. [Google Scholar] [CrossRef]
- Gillies, R.; Kinahan, P.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keek, S.; Leijenaar, R.; Jochems, A.; Woodruff, H.C. A review on radiomics and the future of theranostics for patient selection in precision medicine. Br. J. Radiol. 2018, 91, 20170926. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Aiello, M.; Cavaliere, C.; D’Albore, A.; Salvatore, M. The challenges of diagnostic imaging in the era of big data. J. Clin. Med. 2019, 8, 316. [Google Scholar] [CrossRef] [Green Version]
- Kirienko, M.; Cozzi, L.; Antunovic, L.; Lozza, L.; Fogliata, A.; Voulaz, E.; Rossi, A.; Chiti, A.; Sollini, M. Prediction of disease-free survival by the PET/CT radiomic signature in non-small cell lung cancer patients undergoing surgery. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 207–217. [Google Scholar] [CrossRef]
- Bianconi, F.; Fravolini, M.; Palumbo, I.; Palumbo, B. Shape and texture analysis of radiomic data for Computer-assisted Diagnosis and prognostication: An overview. In Proceedings of the International Conference on Design Tools and Methods in Industrial Engineering (ADM), Modena, Italy, 9–10 September 2019; Rizzi, C., Andrisano, A., Leali, F., Gherardini, F., Pini, F., Vergnano, A., Eds.; Lecture Notes in Mechanical Engineering. Springer: Modena, Italy, 2019; pp. 3–14. [Google Scholar]
- Bianconi, F.; Palumbo, I.; Spanu, A.; Nuvoli, S.; Fravolini, M.L.; Palumbo, B. PET/CT Radiomics in Lung Cancer: An Overview. Appl. Sci. 2020, 10, 1718. [Google Scholar] [CrossRef] [Green Version]
- Thawani, R.; McLane, M.; Beig, N.; Ghose, S.; Prasanna, P.; Velcheti, V.; Madabhushi, A. Radiomics and radiogenomics in lung cancer: A review for the clinician. Lung Cancer 2018, 115, 34–41. [Google Scholar] [CrossRef]
- Chalkidou, A.; O’Doherty, M.; Marsden, P. False discovery rates in PET and CT studies with texture features: A systematic review. PLoS ONE 2015, 10, e0124165. [Google Scholar] [CrossRef] [Green Version]
- Ninatti, G.; Kirienko, M.; Neri, E.; Sollini, M.; Chiti, A. Imaging-Based Prediction of Molecular Therapy Targets in NSCLC by Radiogenomics and AI Approaches: A Systematic Review. Diagnostics 2020, 30, 359. [Google Scholar] [CrossRef]
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-Small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar]
- Shi, Y.; Au, J.S.K.; Thongprasert, S.; Srinivasan, S.; Tsai, C.-M.; Khoa, M.T.; Heeroma, K.; Itoh, Y.; Cornelio, G.; Yang, P.-C. Prospective, Molecular Epidemiology Study of EGFR Mutations in Asian Patients with Advanced Non–Small-Cell Lung Cancer of Adenocarcinoma Histology (PIONEER). J. Thorac. Oncol. 2014, 9, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dearden, S.; Stevens, J.; Wu, Y.; Blowers, D. Mutation incidence and coincidence in non-small-cell lung cancer: Meta-analyses by ethnicity and histology (mutMap). Ann. Oncol. 2013, 24, 2371–2376. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhao, X.; Zhao, Y.; Zhang, J.; Zhang, Z.; Wang, J.; Wang, Y.; Dai, M.; Han, J. Value of pre-therapy 18F-FDG PET/CT radiomics in predicting EGFR mutation status in patients with non-small cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogan, S.; Shen, R.; Ang, D.C.; Johnson, M.L.; D’Angelo, S.P.; Paik, P.K.; Brzostowski, E.B.; Riely, G.J.; Kris, M.G.; Zakowski, M.F.; et al. Molecular Epidemiology of EGFR and KRAS Mutations in 3026 Lung Adenocarcinomas: Higher Susceptibility of Women to Smoking-Related KRAS-Mutant Cancers. Clin. Cancer Res. 2012, 18, 6169–6177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
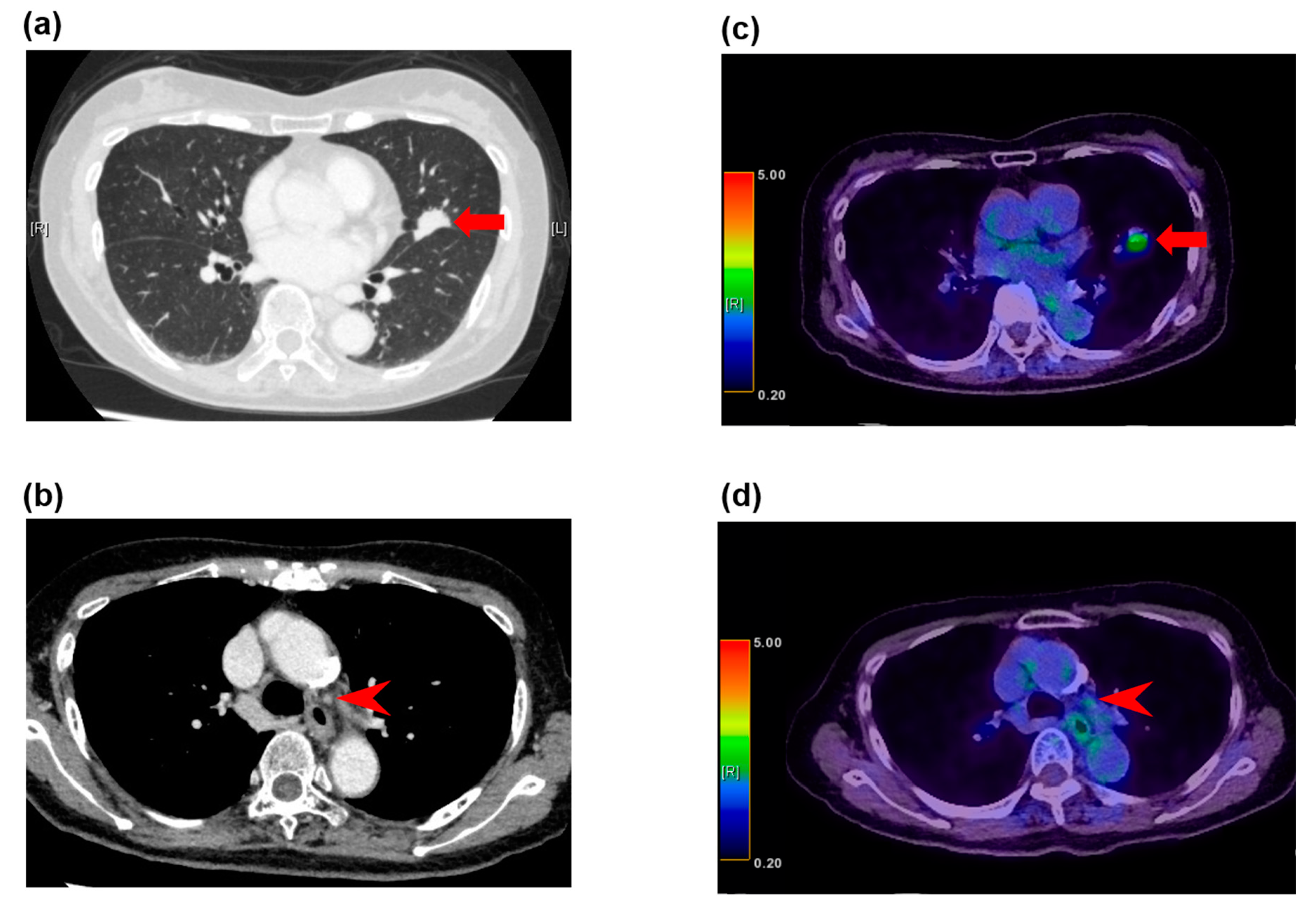
False negative fluorodeoxyglucose F 18 positron emission tomography (FDG-PET) findings in normal-sized lymph nodes in a 79-year-old woman with adenocarcinoma. (a) The computed tomography (CT) image shows a left upper lobe tumor (arrow), (b) and nonenlarged station 5 lymph nodes (arrowhead). (c) The FDG-PET/CT image shows FDG accumulation with a maximum standardized uptake value (SUV) of 3.3 (arrow) in the adenocarcinoma in the left upper lobe, (d) and no FDG accumulation in the normal-sized station 5 lymph nodes (arrowhead). These lymph nodes demonstrated metastatic disease at histopathologic examination of the specimen from surgical biopsy.
Figure 1.
False negative fluorodeoxyglucose F 18 positron emission tomography (FDG-PET) findings in normal-sized lymph nodes in a 79-year-old woman with adenocarcinoma. (a) The computed tomography (CT) image shows a left upper lobe tumor (arrow), (b) and nonenlarged station 5 lymph nodes (arrowhead). (c) The FDG-PET/CT image shows FDG accumulation with a maximum standardized uptake value (SUV) of 3.3 (arrow) in the adenocarcinoma in the left upper lobe, (d) and no FDG accumulation in the normal-sized station 5 lymph nodes (arrowhead). These lymph nodes demonstrated metastatic disease at histopathologic examination of the specimen from surgical biopsy.

Figure 2.
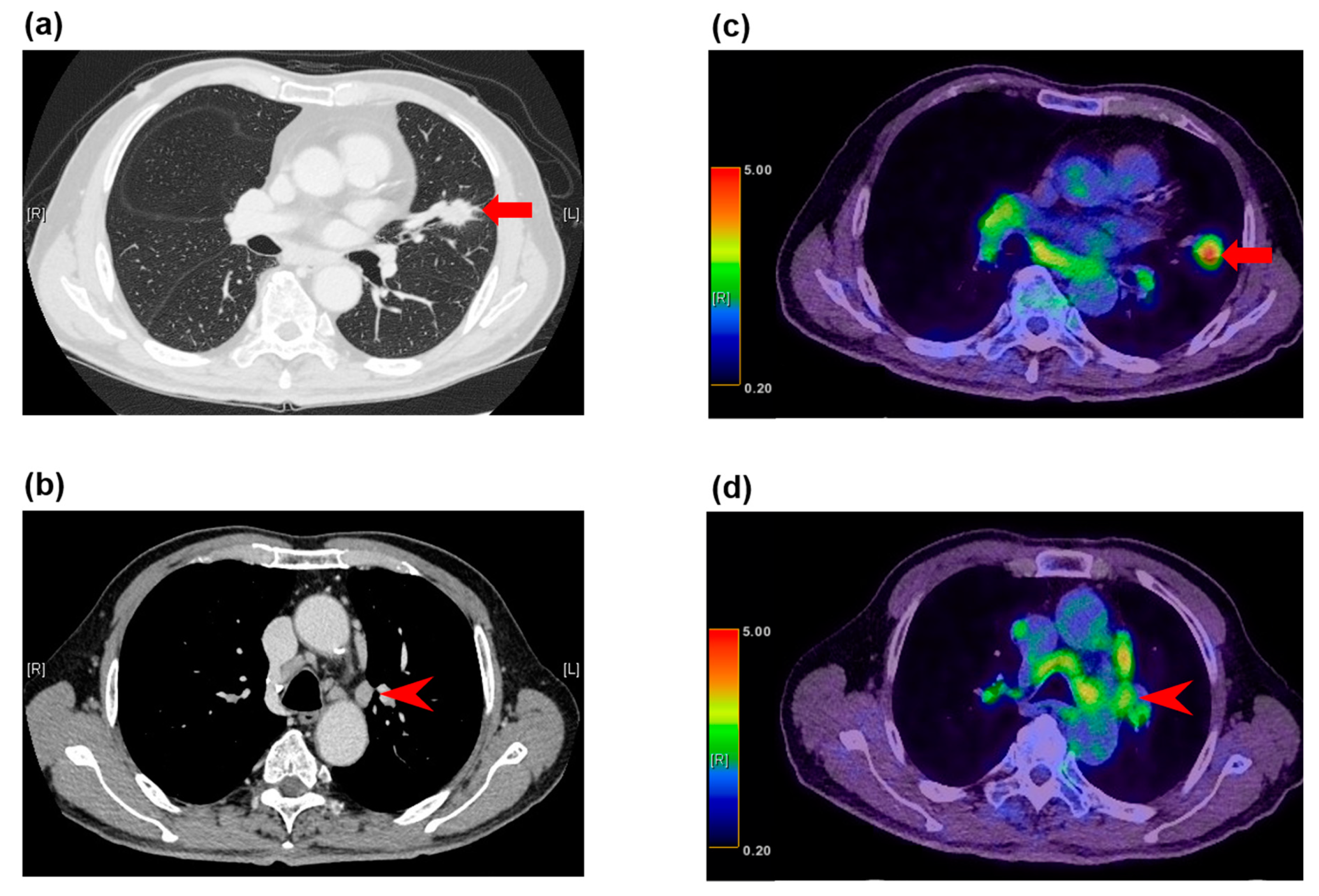
False positive FDG-PET/CT findings in enlarged lymph nodes in a 78-year-old man with squamous cell carcinoma. (a) The CT image shows a left upper lobe tumor (arrow), (b) and enlarged station 5 lymph nodes (arrowhead). (c) The FDG-PET/CT image shows FDG accumulation with a maximum SUV of 6.9 (arrow) in the squamous cell carcinoma in the left upper lobe, (d) and FDG accumulation with a maximum SUV of 3.9 in the enlarged station 5 lymph nodes (arrowhead). These lymph nodes demonstrated granulomatous inflammation at histopathologic examination of the specimen from surgical biopsy.
Figure 2.
False positive FDG-PET/CT findings in enlarged lymph nodes in a 78-year-old man with squamous cell carcinoma. (a) The CT image shows a left upper lobe tumor (arrow), (b) and enlarged station 5 lymph nodes (arrowhead). (c) The FDG-PET/CT image shows FDG accumulation with a maximum SUV of 6.9 (arrow) in the squamous cell carcinoma in the left upper lobe, (d) and FDG accumulation with a maximum SUV of 3.9 in the enlarged station 5 lymph nodes (arrowhead). These lymph nodes demonstrated granulomatous inflammation at histopathologic examination of the specimen from surgical biopsy.


{kind=link}
{kind=link}
Table 1.
Representative studies on the incidence of pathological nodal metastasis in clinical N0 lung cancer.
Table 1.
Representative studies on the incidence of pathological nodal metastasis in clinical N0 lung cancer.
| Author | Year | Histology | cStage | Total Number of Patients | Number of pN1/2 Patients (%) |
|---|---|---|---|---|---|
| Okada M et al. [46] | 2011 | adenocarcinoma | IA | 502 | 38 (7.6) |
| Gomez-Caro A et al. [45] | 2012 | NSCLC | I | 153 | 52 (34.0) |
| Koike T et al. [42] | 2012 | NSCLC | IA | 894 | 67 (7.5) for pN2 |
| Takenaka T et al. [47] | 2012 | NSCLC | IA | 94 | 9 (9.6) |
| Zhang Y et al. [49] | 2012 | NSCLC | IA | 530 | 89 (16.8) for pN2 |
| Cho S et al. [43] | 2013 | NSCLC | I | 770 | 149 (19.4) |
| Miyasaka Y et al. [48] | 2013 | NSCLC | IA-IIIA (N0) | 265 | 51 (20.1) |
| Bao F et al. [51] | 2014 | NSCLC | T1aN0M0 | 315 | 51 (16.2) |
| Shiono S et al. [52] | 2014 | lung cancer | IA | 315 | 20 (6.3) |
| Ye B et al. [53] | 2014 | adenocarcinoma | T1aN0M0 | 273 | 18 (6.6) |
| Tsutani Y et al. [50] | 2015 | squamous cell carcinoma | IA | 100 | 12 (12.0) |
| Wang L et al. [54] | 2015 | peripheral lung cancer | IA | 292 | 28 (9.6) for pN1 |
| Kaseda K et al. [55] | 2016 | NSCLC | I | 246 | 31 (12.6) |
Non-small-cell lung cancer (NSCLC).
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kaseda, K. Recent and Current Advances in FDG-PET Imaging within the Field of Clinical Oncology in NSCLC: A Review of the Literature. Diagnostics 2020, 10, 561. https://doi.org/10.3390/diagnostics10080561
AMA Style
Kaseda K. Recent and Current Advances in FDG-PET Imaging within the Field of Clinical Oncology in NSCLC: A Review of the Literature. Diagnostics. 2020; 10(8):561. https://doi.org/10.3390/diagnostics10080561
Chicago/Turabian StyleKaseda, Kaoru. 2020. "Recent and Current Advances in FDG-PET Imaging within the Field of Clinical Oncology in NSCLC: A Review of the Literature" Diagnostics 10, no. 8: 561. https://doi.org/10.3390/diagnostics10080561
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.