Rapid Large-Scale COVID-19 Testing during Shortages

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Portal Description
2.2. Sample Collection and Storage
2.3. RNA Extraction
2.4. RT-PCR and Result Evaluation
2.5. Tested Individuals
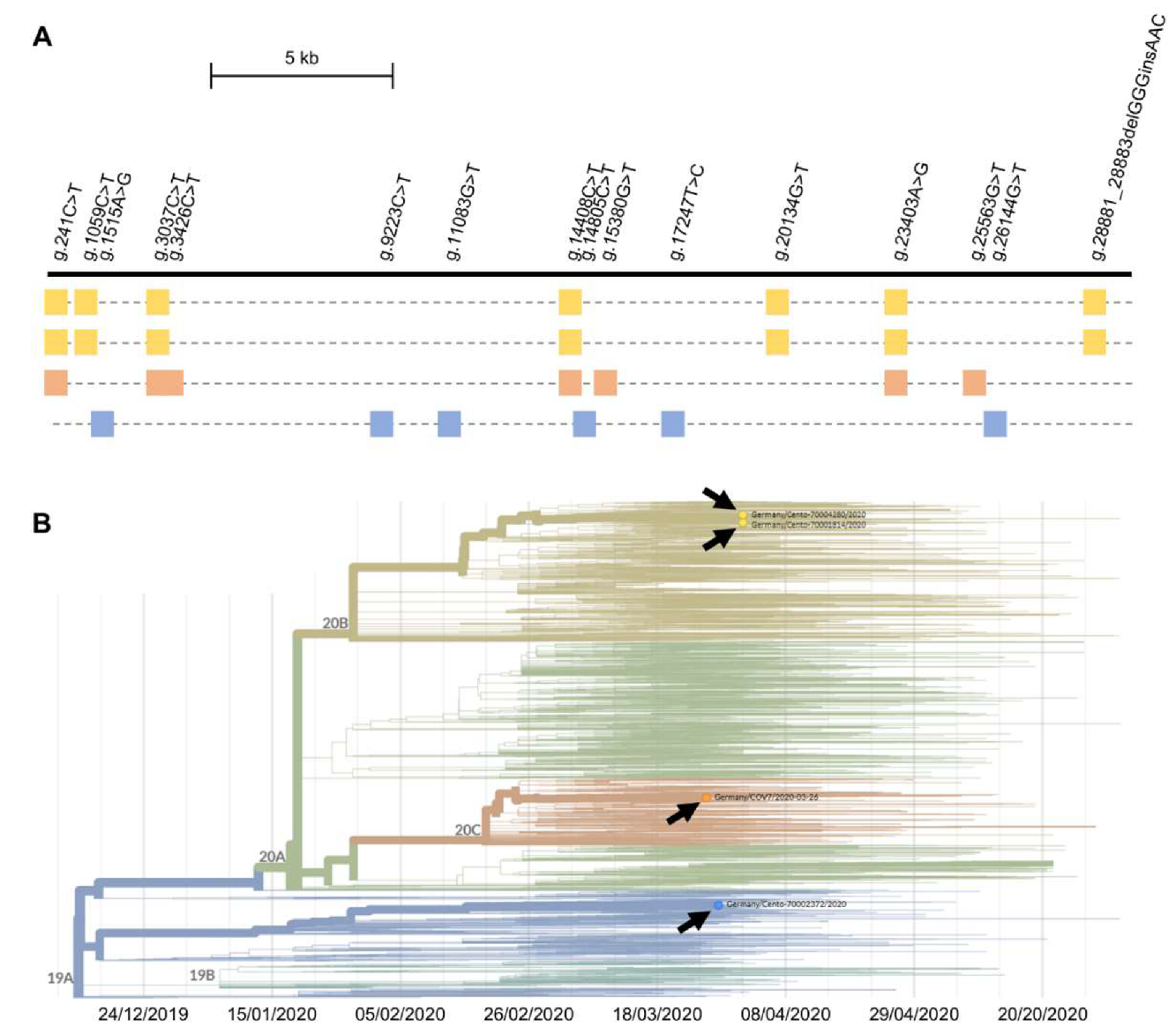
2.6. Virus Genome Sequencing and Analysis
3. Results
3.1. Corona Test Portal
3.2. General Validation of the Virus Detection Approach
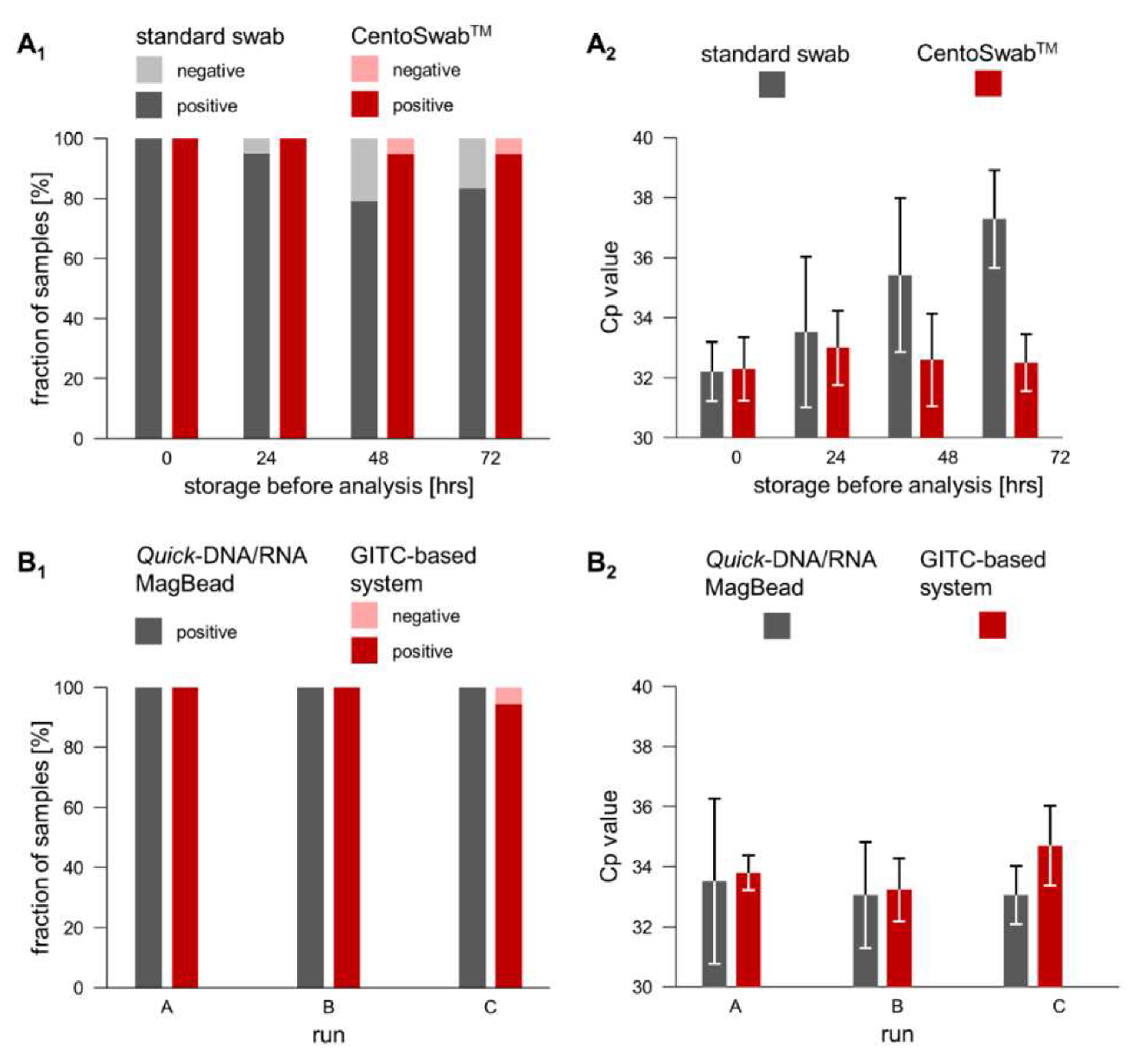
3.3. Validation of an Alternative Sample Collection Swab and of an Alternative RNA Extraction Approach
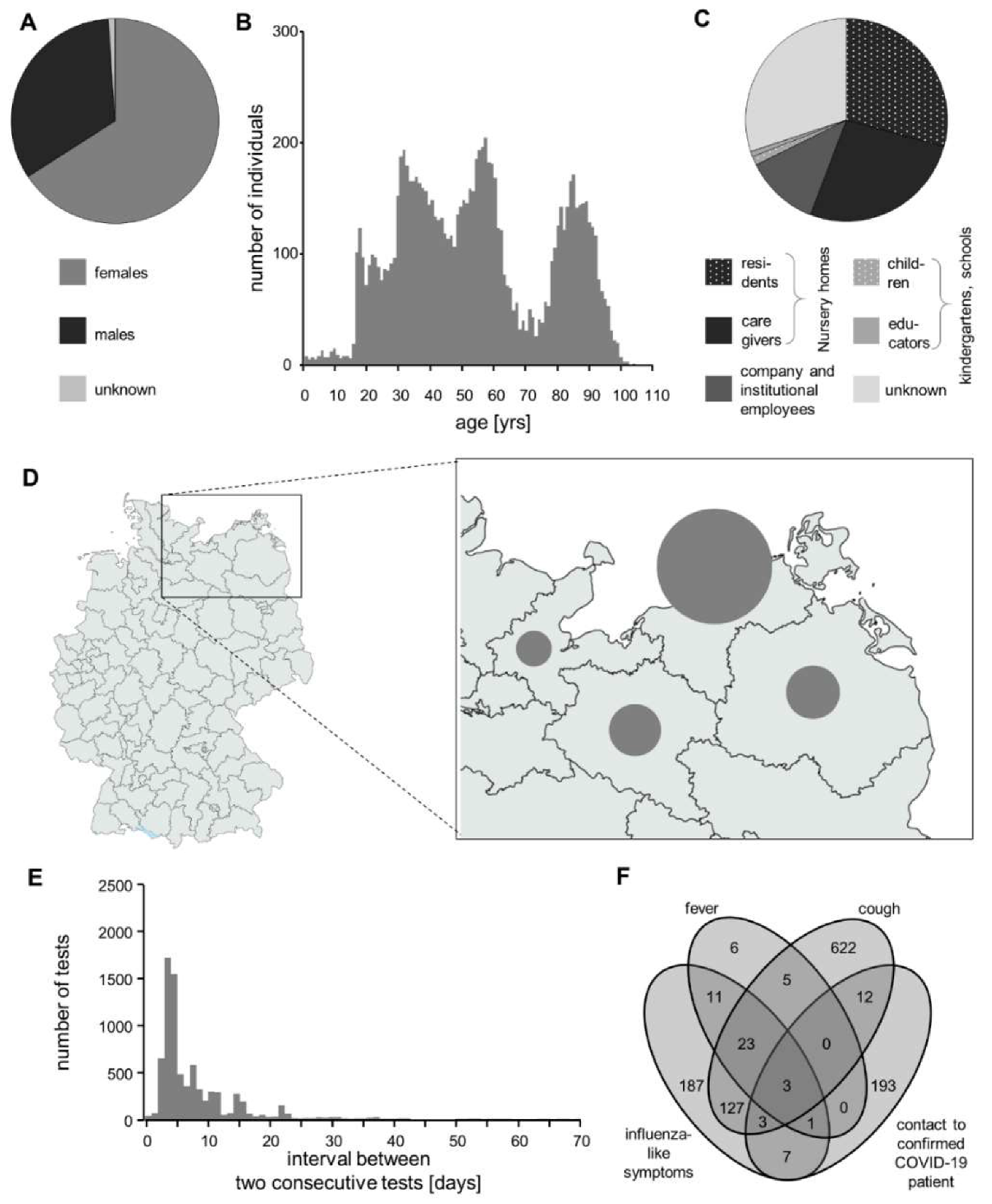
3.4. Description of the Tested Cohort
3.5. Positively Tested Individuals
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Zitek, T. The Appropriate Use of Testing for COVID-19. West. J. Emerg. Med. 2020, 21, 470–472. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.; Zhang, A.J.; Yuan, S.; Poon, V.K.; Chan, C.C.; Lee, A.C.; Chan, W.M.; Fan, Z.; Tsoi, H.W.; Wen, L.; et al. Simulation of the clinical and pathological manifestations of Coronavirus Disease 2019 (COVID-19) in golden Syrian hamster model: Implications for disease pathogenesis and transmissibility. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Muller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petruzzi, G.; De Virgilio, A.; Pichi, B.; Mazzola, F.; Zocchi, J.; Mercante, G.; Spriano, G.; Pellini, R. COVID-19: Nasal and oropharyngeal swab. Head Neck 2020, 42, 1303–1304. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, H.; Mio, M.; Murase, T.; Egawa, K.; Kokumai, Y.; Uchida, T.; Morimoto, N.; Otsuka, F.; Shiota, S. Is wet swab superior to dry swab as an intranasal screening test? J. Intensive Care 2013, 1, 10. [Google Scholar] [CrossRef] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wee, S.K.; Sivalingam, S.P.; Yap, E.P.H. Rapid Direct Nucleic Acid Amplification Test without RNA Extraction for SARS-CoV-2 Using a Portable PCR Thermocycler. Genes 2020, 11, 664. [Google Scholar] [CrossRef]
- Nalla, A.K.; Casto, A.M.; Huang, M.W.; Perchetti, G.A.; Sampoleo, R.; Shrestha, L.; Wei, Y.; Zhu, H.; Jerome, K.R.; Greninger, A.L. Comparative Performance of SARS-CoV-2 Detection Assays Using Seven Different Primer-Probe Sets and One Assay Kit. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [Green Version]
- Fomsgaard, A.S.; Rosenstierne, M.W. An alternative workflow for molecular detection of SARS-CoV-2-escape from the NA extraction kit-shortage, Copenhagen, Denmark, March 2020. Euro Surveill. 2020, 25, 2000398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Kasteren, P.B.; van der Veer, B.; van den Brink, S.; Wijsman, L.; de Jonge, J.; van den Brandt, A.; Molenkamp, R.; Reusken, C.; Meijer, A. Comparison of seven commercial RT-PCR diagnostic kits for COVID-19. J. Clin. Virol. 2020, 128, 104412. [Google Scholar] [CrossRef] [PubMed]
- Pere, H.; Podglajen, I.; Wack, M.; Flamarion, E.; Mirault, T.; Goudot, G.; Hauw-Berlemont, C.; Le, L.; Caudron, E.; Carrabin, S.; et al. Nasal Swab Sampling for SARS-CoV-2: A Convenient Alternative in Times of Nasopharyngeal Swab Shortage. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Scientist. Available online: https://www.the-scientist.com/news-opinion/rna-extraction-kits-for-covid-19-tests-are-in-short-supply-in-us-67250 (accessed on 22 June 2020).
- Coronavirus Disease 2019 (COVID-19) Specimen Collection. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 22 June 2020).
- Chomczynski, P.; Sacchi, N. The single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction: Twenty-something years on. Nat. Protoc. 2006, 1, 581–585. [Google Scholar] [CrossRef]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef] [Green Version]
- Illumina® Informatics Blog. Available online: https://blog.software.illumina.com/2020/04/14/illumina-cov-2-ngs-data-toolkit/ (accessed on 22 June 2020).
- Nextstrain – Real-Time Tracking of Pathogen Evolution. Available online: https://github.com/nextstrain/ncov (accessed on 22 June 2020).
- Guo, L.; Sun, X.; Wang, X.; Liang, C.; Jiang, H.; Gao, Q.; Dai, M.; Qu, B.; Fang, S.; Mao, Y.; et al. SARS-CoV-2 detection with CRISPR diagnostics. Cell Discov. 2020, 6, 34. [Google Scholar] [CrossRef]
- Lu, R.; Wu, X.; Wan, Z.; Li, Y.; Jin, X.; Zhang, C. A Novel Reverse Transcription Loop-Mediated Isothermal Amplification Method for Rapid Detection of SARS-CoV-2. Int. J. Mol. Sci. 2020, 21, 2826. [Google Scholar] [CrossRef] [Green Version]
- Reusken, C.; Broberg, E.K.; Haagmans, B.; Meijer, A.; Corman, V.M.; Papa, A.; Charrel, R.; Drosten, C.; Koopmans, M.; Leitmeyer, K.; et al. Laboratory readiness and response for novel coronavirus (2019-nCoV) in expert laboratories in 30 EU/EEA countries, January 2020. Euro Surveill. 2020, 25, 2000082. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.; Yip, C.C.; To, K.K.; Tang, T.H.; Wong, S.C.; Leung, K.H.; Fung, A.Y.; Ng, A.C.; Zou, Z.; Tsoi, H.W.; et al. Improved Molecular Diagnosis of COVID-19 by the Novel, Highly Sensitive and Specific COVID-19-RdRp/Hel Real-Time Reverse Transcription-PCR Assay Validated In Vitro and with Clinical Specimens. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.fda.gov/medical-devices/emergency-situations-medical-devices/faqs-testing-sars-cov-2#validation (accessed on 22 June 2020).
- McMichael, G.L.; Gibson, C.S.; O’Callaghan, M.E.; Goldwater, P.N.; Dekker, G.A.; Haan, E.A.; MacLennan, A.H.; South Australian Cerebral Palsy Research, G. DNA from buccal swabs suitable for high-throughput SNP multiplex analysis. J. Biomol. Tech. 2009, 20, 232–235. [Google Scholar]
- Scallan, M.F.; Dempsey, C.; MacSharry, J.; O’Callaghan, I.; O’Connor, P.M.; Horgan, C.P.; Durack, E.; Cotter, P.D.; Hudson, S.; Moynihan, H.A.; et al. Validation of a Lysis Buffer Containing 4 M Guanidinium Thiocyanate (GITC)/ Triton X-100 for Extraction of SARS-CoV-2 RNA for COVID-19 Testing: Comparison of Formulated Lysis Buffers Containing 4 to 6 M GITC, Roche External Lysis Buffer and Qiagen RTL Lysis Buffer. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Team, C.N.I.R.S. COVID-19, Australia: Epidemiology Report 17 (Fortnightly reporting period ending 24 May 2020). Commun. Dis. Intell. 2020, 44. [Google Scholar] [CrossRef]
- Carvalho, A.; Cezarotti Filho, M.L.; Azevedo, P.C.P.; Silveira Filho, R.N.; Barbosa, F.T.; Rocha, T.J.M.; Sousa-Rodrigues, C.F.; Ramos, F. Epidemiology, diagnosis, treatment, and future perspectives concerning SARS-COV-2: A review article. Rev. Assoc. Med. Bras. 2020, 66, 370–374. [Google Scholar] [CrossRef]
- Watson, J.; Whiting, P.F.; Brush, J.E. Interpreting a covid-19 test result. BMJ 2020, 369, m1808. [Google Scholar] [PubMed]
- FAQs on testing for SARS-CoV-2. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Fallzahlen.html (accessed on 22 June 2020).
- Tabata, S.; Imai, K.; Kawano, S.; Ikeda, M.; Kodama, T.; Miyoshi, K.; Obinata, H.; Mimura, S.; Kodera, T.; Kitagaki, M.; et al. Clinical characteristics of COVID-19 in 104 people with SARS-CoV-2 infection on the Diamond Princess cruise ship: A retrospective analysis. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Benvenuto, D.; Giovanetti, M.; Salemi, M.; Prosperi, M.; De Flora, C.; Junior Alcantara, L.C.; Angeletti, S.; Ciccozzi, M. The global spread of 2019-nCoV: A molecular evolutionary analysis. Pathog. Glob. Health 2020, 114, 64–67. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Specificity | Sensitivity | Precision | ||
|---|---|---|---|---|
| Intrarun | Interrun | |||
| E gene | 65/65 (=100%) | 49/50 (=98%) | 1.8% | 1.9% |
| RdRP gene | n.d. | n.d. | 2.6% | 2.4% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beetz, C.; Skrahina, V.; Förster, T.M.; Gaber, H.; Paul, J.J.; Curado, F.; Rolfs, A.; Bauer, P.; Schäfer, S.; Weckesser, V.; et al. Rapid Large-Scale COVID-19 Testing during Shortages. Diagnostics 2020, 10, 464. https://doi.org/10.3390/diagnostics10070464
Beetz C, Skrahina V, Förster TM, Gaber H, Paul JJ, Curado F, Rolfs A, Bauer P, Schäfer S, Weckesser V, et al. Rapid Large-Scale COVID-19 Testing during Shortages. Diagnostics. 2020; 10(7):464. https://doi.org/10.3390/diagnostics10070464
Chicago/Turabian StyleBeetz, Christian, Volha Skrahina, Toni M. Förster, Hanaa Gaber, Jefri J. Paul, Filipa Curado, Arndt Rolfs, Peter Bauer, Stephan Schäfer, Volkmar Weckesser, and et al. 2020. "Rapid Large-Scale COVID-19 Testing during Shortages" Diagnostics 10, no. 7: 464. https://doi.org/10.3390/diagnostics10070464