Two-Dimensional Shear Wave Elastography versus Transient Elastography: A Non-Invasive Comparison for the Assessment of Liver Fibrosis in Patients with Chronic Hepatitis C

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
- -
- age ≥18 years
- -
- history of chronic HCV infection treated with Direct-acting antivirals (DAAs)
- -
- undetectable HCV RNA for at least 6 months after DAA treatment completion
- -
- annual TE starting from at least 6 months after DAA treatment completion
- -
- at least 3 evaluations of liver stiffness by TE
- -
- liver stiffness by TE showing stable fibrosis stage over the last 36 months
- -
- active HCV infection
- -
- alanine transaminases (ALT) and/or aspartate transaminases (AST) and or gamma-glutamyltransferase (GGT) > 100 U/L over the last 36 months
- -
- presence of ascites, jaundice or hepatocellular carcinoma
- -
- hepatitis B virus (HBV) or human immunodeficiency virus (HIV) coinfection
- -
- liver steatosis at the basic US examination
- -
- daily alcohol intake ≥ 30 g in men and ≥ 20 g in women
- -
- congestive heart failure
- -
- BMI > 30 Kg/m2
- -
- concomitant autoimmune liver disease or storage diseases
- -
- diagnosis of drug-induced liver injury (DILI) in the last 36 months.
- -
- B-mode abdominal US
- -
- liver stiffness evaluation by TE (Fibroscan)
- -
- liver stiffness evaluation by 2D-SWE (ElastQ)
2.2. Abdominal Ultrasonography, Transient Elastography, and Two-Dimensional Shear Wave Elastography
- -
- at least 10 valid measurements
- -
- a success rate (the ratio of valid measurements to the total number of valid and invalid measurements) above 60%
- -
- IQR less than 30% of the median value.
2.3. Clinical and Laboratory Assessment
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristic of Patients
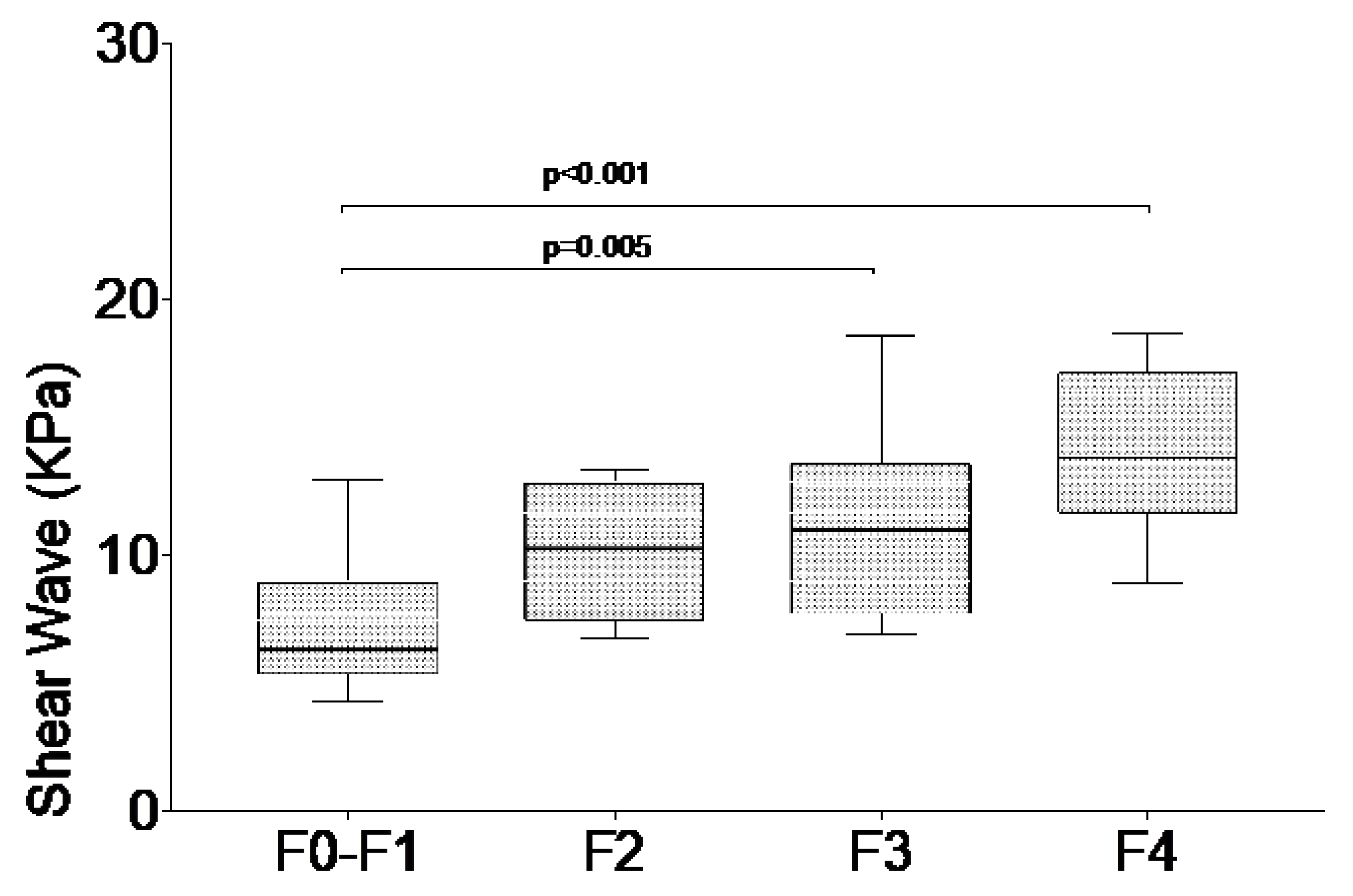
3.2. Liver Stiffness in Patients with Chronic Hepatitis C
3.3. Accuracy of 2D-SWE in Differentiating Different Degrees of Fibrosis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Hepatitis C. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 1 March 2020).
- Han, R.; Zhou, J.; Francois, C.; Toumi, M. Prevalence of hepatitis C infection among the general population and high-risk groups in the EU/EEA: A systematic review update. BMC Infect. Dis. 2019, 19, 655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westbrook, R.H.; Dusheiko, G. Natural history of hepatitis C. J. Hepatol. 2014, 61, S58–S68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, M.J.; el-Farra, N.S.; Reikes, A.R.; Co, R.L. Clinical outcomes after transfusion-associated hepatitis C. N. Engl. J. Med. 1995, 332, 1463–1466. [Google Scholar] [CrossRef] [PubMed]
- Wiese, M.; Berr, F.; Lafrenz, M.; Porst, H.; Oesen, U. Low frequency of cirrhosis in a hepatitis C (genotype 1b) single-source outbreak in germany: A 20-year multicenter study. Hepatology 2000, 32, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Lefton, H.B.; Rosa, A.; Cohen, M. Diagnosis and epidemiology of cirrhosis. Med. Clin. N. Am. 2009, 93, 787–799. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, E.; de Ledinghen, V.; Cassinotto, C.; Chu, W.C.; Leung, V.Y.; Ferraioli, G.; Filice, C.; Castera, L.; Vilgrain, V.; Ronot, M.; et al. Assessment of biopsy-proven liver fibrosis by two-dimensional shear wave elastography: An individual patient data-based meta-analysis. Hepatology 2018, 67, 260–272. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [Green Version]
- Regev, A.; Berho, M.; Jeffers, L.J.; Milikowski, C.; Molina, E.G.; Pyrsopoulos, N.T.; Feng, Z.Z.; Reddy, K.R.; Schiff, E.R. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. Am. J. Gastroenterol. 2002, 97, 2614–2618. [Google Scholar] [CrossRef]
- Bedossa, P.; Dargere, D.; Paradis, V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology 2003, 38, 1449–1457. [Google Scholar] [CrossRef]
- Castera, L.; Negre, I.; Samii, K.; Buffet, C. Pain experienced during percutaneous liver biopsy. Hepatology 1999, 30, 1529–1530. [Google Scholar] [CrossRef]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver biopsy. N. Engl. J. Med. 2001, 344, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Serra, C.; Grasso, V.; Conti, F.; Felicani, C.; Mazzotta, E.; Lenzi, M.; Verucchi, G.; D’Errico, A.; Andreone, P. A New Two-Dimensional Shear Wave Elastography for Noninvasive Assessment of Liver Fibrosis in Healthy Subjects and in Patients with Chronic Liver Disease. Ultraschall Med. 2018, 39, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Arena, U.; Vizzutti, F.; Abraldes, J.G.; Corti, G.; Stasi, C.; Moscarella, S.; Milani, S.; Lorefice, E.; Petrarca, A.; Romanelli, R.G.; et al. Reliability of transient elastography for the diagnosis of advanced fibrosis in chronic hepatitis C. Gut 2008, 57, 1288–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, M.; Gennisson, J.L.; Deffieux, T.; Tanter, M.; Fink, M. Quantitative viscoelasticity mapping of human liver using supersonic shear imaging: Preliminary in vivo feasibility study. Ultrasound Med. Biol 2009, 35, 219–229. [Google Scholar] [CrossRef]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef]
- Barr, R.G.; Ferraioli, G.; Palmeri, M.L.; Goodman, Z.D.; Garcia-Tsao, G.; Rubin, J.; Garra, B.; Myers, R.P.; Wilson, S.R.; Rubens, D.; et al. Elastography Assessment of Liver Fibrosis: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology 2015, 276, 845–861. [Google Scholar] [CrossRef] [Green Version]
- Yun, M.H.; Seo, Y.S.; Kang, H.S.; Lee, K.G.; Kim, J.H.; An, H.; Yim, H.J.; Keum, B.; Jeen, Y.T.; Lee, H.S.; et al. The effect of the respiratory cycle on liver stiffness values as measured by transient elastography. J. Viral Hepat. 2011, 18, 631–636. [Google Scholar] [CrossRef]
- Horster, S.; Mandel, P.; Zachoval, R.; Clevert, D.A. Comparing acoustic radiation force impulse imaging to transient elastography to assess liver stiffness in healthy volunteers with and without valsalva manoeuvre. Clin. Hemorheol. Microcirc. 2010, 46, 159–168. [Google Scholar] [CrossRef]
- Castera, L.; Forns, X.; Alberti, A. Non-invasive evaluation of liver fibrosis using transient elastography. J. Hepatol. 2008, 48, 835–847. [Google Scholar] [CrossRef]
- Ferraioli, G. Review of Liver Elastography Guidelines. J. Ultrasound Med. 2019, 38, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Ferraioli, G.; Wong, V.W.; Castera, L.; Berzigotti, A.; Sporea, I.; Dietrich, C.F.; Choi, B.I.; Wilson, S.R.; Kudo, M.; Barr, R.G. Liver Ultrasound Elastography: An Update to the World Federation for Ultrasound in Medicine and Biology Guidelines and Recommendations. Ultrasound Med. Biol. 2018, 44, 2419–2440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abe, T.; Kuroda, H.; Fujiwara, Y.; Yoshida, Y.; Miyasaka, A.; Kamiyama, N.; Takikawa, Y. Accuracy of 2D shear wave elastography in the diagnosis of liver fibrosis in patients with chronic hepatitis C. J. Clin. Ultrasound 2018, 46, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Matos, J.; Paparo, F.; Bacigalupo, L.; Cenderello, G.; Mussetto, I.; De Cesari, M.; Bernardi, S.P.; Cevasco, L.; Forni, G.L.; Cassola, G.; et al. Noninvasive liver fibrosis assessment in chronic viral hepatitis C: Agreement among 1D transient elastography, 2D shear wave elastography, and magnetic resonance elastography. Abdom. Radiol. (NY) 2019, 44, 4011–4021. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, G.; Maiocchi, L.; Lissandrin, R.; Tinelli, C.; De Silvestri, A.; Filice, C. Liver Fibrosis Study Group, Accuracy of the ElastPQ Technique for the Assessment of Liver Fibrosis in Patients with Chronic Hepatitis C: A “Real Life” Single Center Study. J. Gastrointestin. Liver Dis. 2016, 25, 331–335. [Google Scholar] [CrossRef]
- Ferraioli, G.; Tinelli, C.; Dal Bello, B.; Zicchetti, M.; Filice, G.; Filice, C.; Liver Fibrosis Study, G. Accuracy of real-time shear wave elastography for assessing liver fibrosis in chronic hepatitis C: A pilot study. Hepatology 2012, 56, 2125–2133. [Google Scholar] [CrossRef]
- Friedrich-Rust, M.; Ong, M.F.; Martens, S.; Sarrazin, C.; Bojunga, J.; Zeuzem, S.; Herrmann, E. Performance of transient elastography for the staging of liver fibrosis: A meta-analysis. Gastroenterology 2008, 134, 960–974. [Google Scholar] [CrossRef] [Green Version]
- Tsochatzis, E.A.; Gurusamy, K.S.; Ntaoula, S.; Cholongitas, E.; Davidson, B.R.; Burroughs, A.K. Elastography for the diagnosis of severity of fibrosis in chronic liver disease: A meta-analysis of diagnostic accuracy. J. Hepatol. 2011, 54, 650–659. [Google Scholar] [CrossRef]
- Bavu, E.; Gennisson, J.L.; Couade, M.; Bercoff, J.; Mallet, V.; Fink, M.; Badel, A.; Vallet-Pichard, A.; Nalpas, B.; Tanter, M.; et al. Noninvasive in vivo liver fibrosis evaluation using supersonic shear imaging: A clinical study on 113 hepatitis C virus patients. Ultrasound Med. Biol. 2011, 37, 1361–1373. [Google Scholar] [CrossRef]
- Popescu, A.; Sporea, I.; Sirli, R.; Bota, S.; Focsa, M.; Danila, M.; Nicolita, D.; Martie, A.; Sendroiu, M.; Juchis, A. The mean values of liver stiffness assessed by Acoustic Radiation Force Impulse elastography in normal subjects. Med. Ultrason. 2011, 13, 33–37. [Google Scholar]
- Poynard, T.; Lenaour, G.; Vaillant, J.C.; Capron, F.; Munteanu, M.; Eyraud, D.; Ngo, Y.; M’Kada, H.; Ratziu, V.; Hannoun, L.; et al. Liver biopsy analysis has a low level of performance for diagnosis of intermediate stages of fibrosis. Clin. Gastroenterol. Hepatol. 2012, 10, 657–663. [Google Scholar] [CrossRef]


{kind=link}
| All Patients N = 178 | F0-F1 Group N = 44 | F2 Group N = 32 | F3 Group N = 43 | F4 Group N = 59 |
|---|---|---|---|---|
| Age (years) | 64.2 ± 13 | 63.7 ± 13 | 64.1 ± 12.7 | 64.5 ± 13 |
| Gender (M/F) | 30/14 | 19/13 | 22/21 | 36/23 |
| BMI kg/m2 | 24.1 ± 4.3 | 23.1 ± 3.7 | 24.5 ± 4.1 | 23.8 ± 2.9 |
| Aspartate transaminases (AST) (U/L) | 32.4 ± 16.8 | 38.2 ± 23.3 | 29.9 ± 17.3 | 26.2 ± 24.1 |
| Alanine transaminases (ALT) (U/L) | 19.2 ± 11.3 | 31.3 ± 26.8 | 39.4 ± 13.8 | 38.6 ± 19.8 |
| Gamma-glutamyltransferase (GGT) (U/L) | 22.3 ± 19.7 | 31.1 ± 18.6 | 36.8 ± 21.3 | 37.2 ± 9.9 |
| Liver Stiffness (ElastQ) | F0–F1 Group | F2 Group | F3 Group | F4 Group |
|---|---|---|---|---|
| Overall Population (N = 178) | ||||
| Median (KPa) | 6.31 | 10.28 | 11.03 | 13.83 |
| 25% Percentile | 5.36 | 7.47 | 7.76 | 11.72 |
| 75% Percentile | 8.94 | 12.81 | 13.6 | 17.15 |
| Female (N = 71) | ||||
| Median (KPa) | 6.17 | 10.23 | 11.52 | 14.40 |
| 25% Percentile | 5.40 | 7.06 | 7.96 | 10.91 |
| 75% Percentile | 9.83 | 12.39 | 12.2 | 15.90 |
| Male (N = 107) | ||||
| Median (KPa) | 6.39 | 9.1 | 11.47 | 13.58 |
| 25% Percentile | 5.35 | 6.8 | 9.55 | 12 |
| 75% Percentile | 7.51 | 10.4 | 18.56 | 18.22 |
| ≥65 years (N = 97) | ||||
| Median (KPa) | 7.22 | 10.06 | 10.55 | 15.07 |
| 25% Percentile | 5.38 | 6.8 | 8.01 | 12.57 |
| 75% Percentile | 9.2 | 13.39 | 12.47 | 17.52 |
| Fibrosis Stage | Cut-off Value (KPa) | AUROC (95% CI) | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | LR+ | LR− |
|---|---|---|---|---|---|---|---|---|
| F = 4 | 12.65 | 0.899 (0.824–0.973) | 73.3 (44.9–92.2) | 88.5 (76.6–95.7) | 69.5 (54.2–89.7) | 90.9 (82.3–99.7) | 6.373 | 0.301 |
| F ≥ 3 | 10.31 | 0.900 (0.834–0.967) | 77.1 (59.9–89.6) | 85.4 (70.8–94.4) | 77.7 (61.6–97.3) | 90.2 (80.7–99.9) | 5.280 | 0.268 |
| F ≥ 2 | 8.15 | 0.899 (0.829–0.969) | 87.1 (70.2–96.4) | 73 (55.9–86.2) | 87.3 (70.4–99.9) | 70.2 (58.3–96.9) | 3.223 | 0.176 |
| Fibrosis Stage | Cut–off Value (KPa) | AUROC (95% CI) | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | LR+ | LR− |
|---|---|---|---|---|---|---|---|---|
| F = 4 | 13.00 | 0.900 (0.781–1.000) | 71.4 (39–96.3) | 93.3 (77.9–99.2) | 73.6 (48–99.8) | 94.3 (84.4–99.9) | 10.7 | 0.116 |
| F ≥ 3 | 11.29 | 0.847 (0.722–0.973) | 64.3 (35.2–87.2) | 91.3 (72–98.9) | 81.8 (61.6–100) | 80.8 (64.7–96.9) | 7.39 | 0.183 |
| F ≥ 2 | 10.47 | 0.862 (0.744–0.979) | 70.6 (44.1–89.7) | 95 (75.1–99.9) | 92.3 (77.8–100) | 79.2 (63–95.4) | 14.2 | 0.071 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villani, R.; Cavallone, F.; Romano, A.D.; Bellanti, F.; Serviddio, G. Two-Dimensional Shear Wave Elastography versus Transient Elastography: A Non-Invasive Comparison for the Assessment of Liver Fibrosis in Patients with Chronic Hepatitis C. Diagnostics 2020, 10, 313. https://doi.org/10.3390/diagnostics10050313
Villani R, Cavallone F, Romano AD, Bellanti F, Serviddio G. Two-Dimensional Shear Wave Elastography versus Transient Elastography: A Non-Invasive Comparison for the Assessment of Liver Fibrosis in Patients with Chronic Hepatitis C. Diagnostics. 2020; 10(5):313. https://doi.org/10.3390/diagnostics10050313
Chicago/Turabian StyleVillani, Rosanna, Francesco Cavallone, Antonino Davide Romano, Francesco Bellanti, and Gaetano Serviddio. 2020. "Two-Dimensional Shear Wave Elastography versus Transient Elastography: A Non-Invasive Comparison for the Assessment of Liver Fibrosis in Patients with Chronic Hepatitis C" Diagnostics 10, no. 5: 313. https://doi.org/10.3390/diagnostics10050313