Hypotensive Effect of Nanomicellar Formulation of Melatonin and Agomelatine in a Rat Model: Significance for Glaucoma Therapy

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Experimental Model of Hypertensive Eyes
2.2. Preparation of Eye Drops
2.3. Administration of Eye Drops and Measurement of Intraocular Pressure
2.4. Statistical Analysis
3. Results
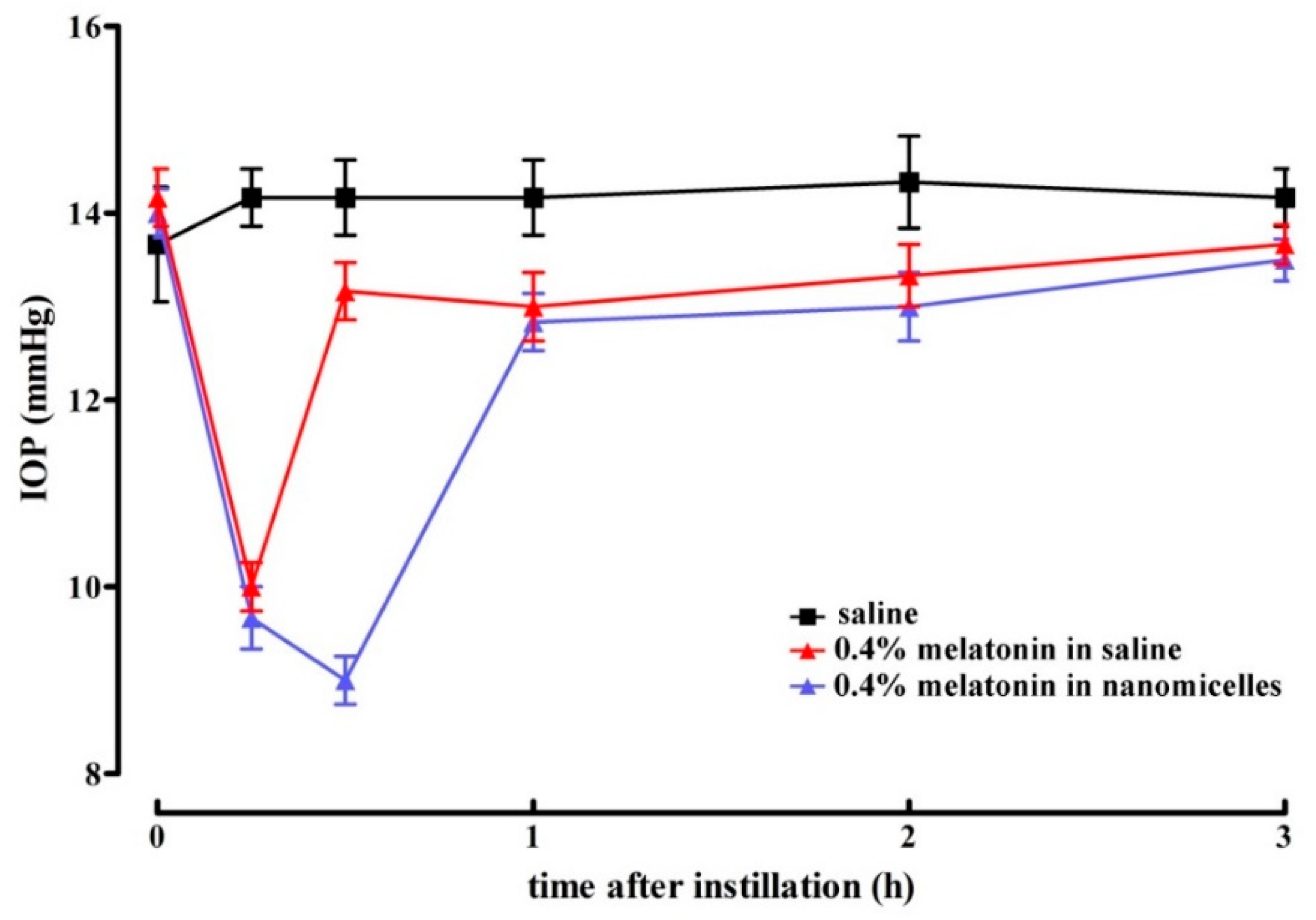
3.1. Normotensive IOP: Effect of Melatonin in Saline vs. Melatonin in Nanomicellar Formulation
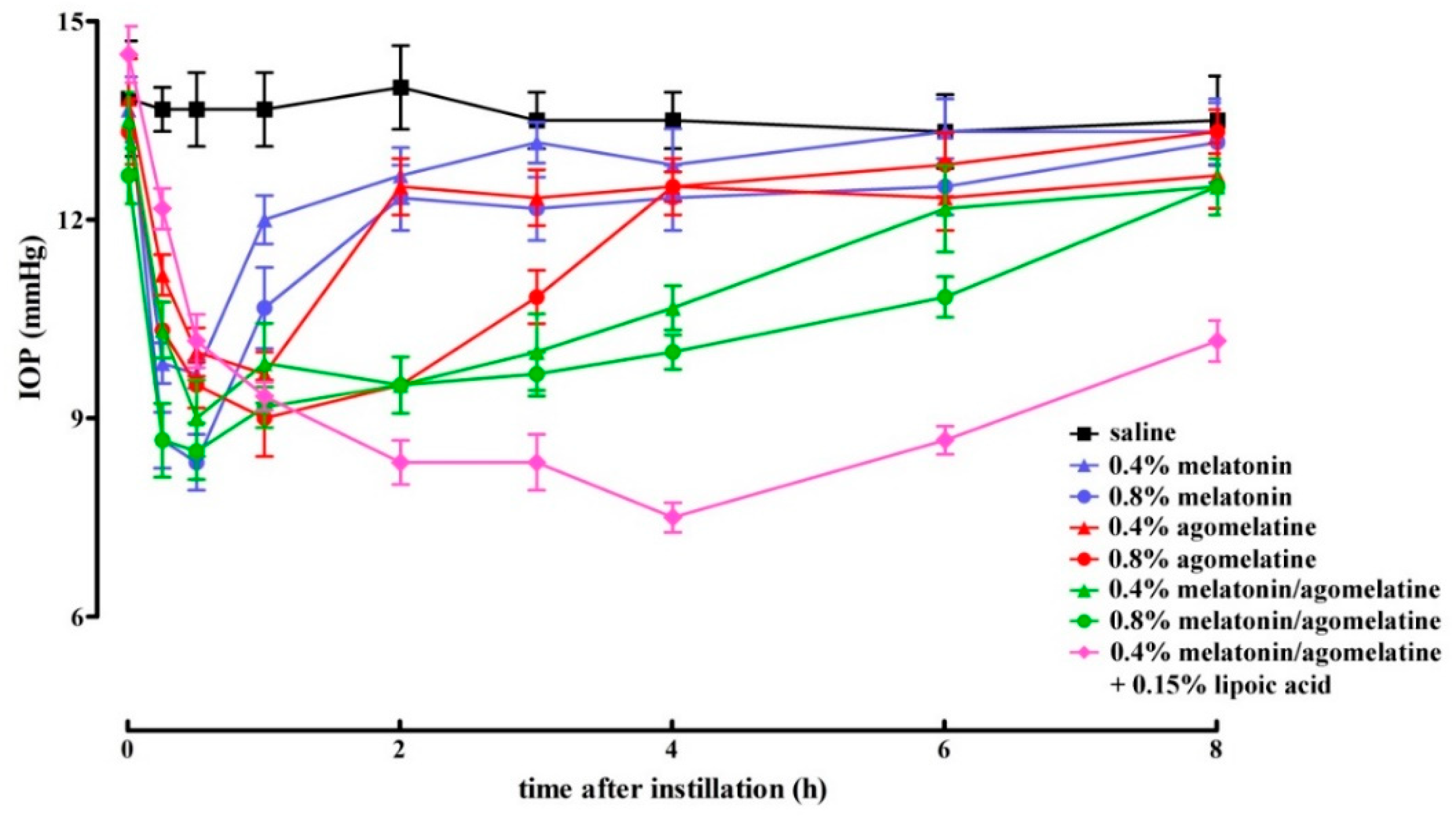
3.2. Normotensive IOP: Effect of Melatonin and Agomelatine Formulated in Nanomicelles either Alone or in Combination, without or with Lipoic Acid
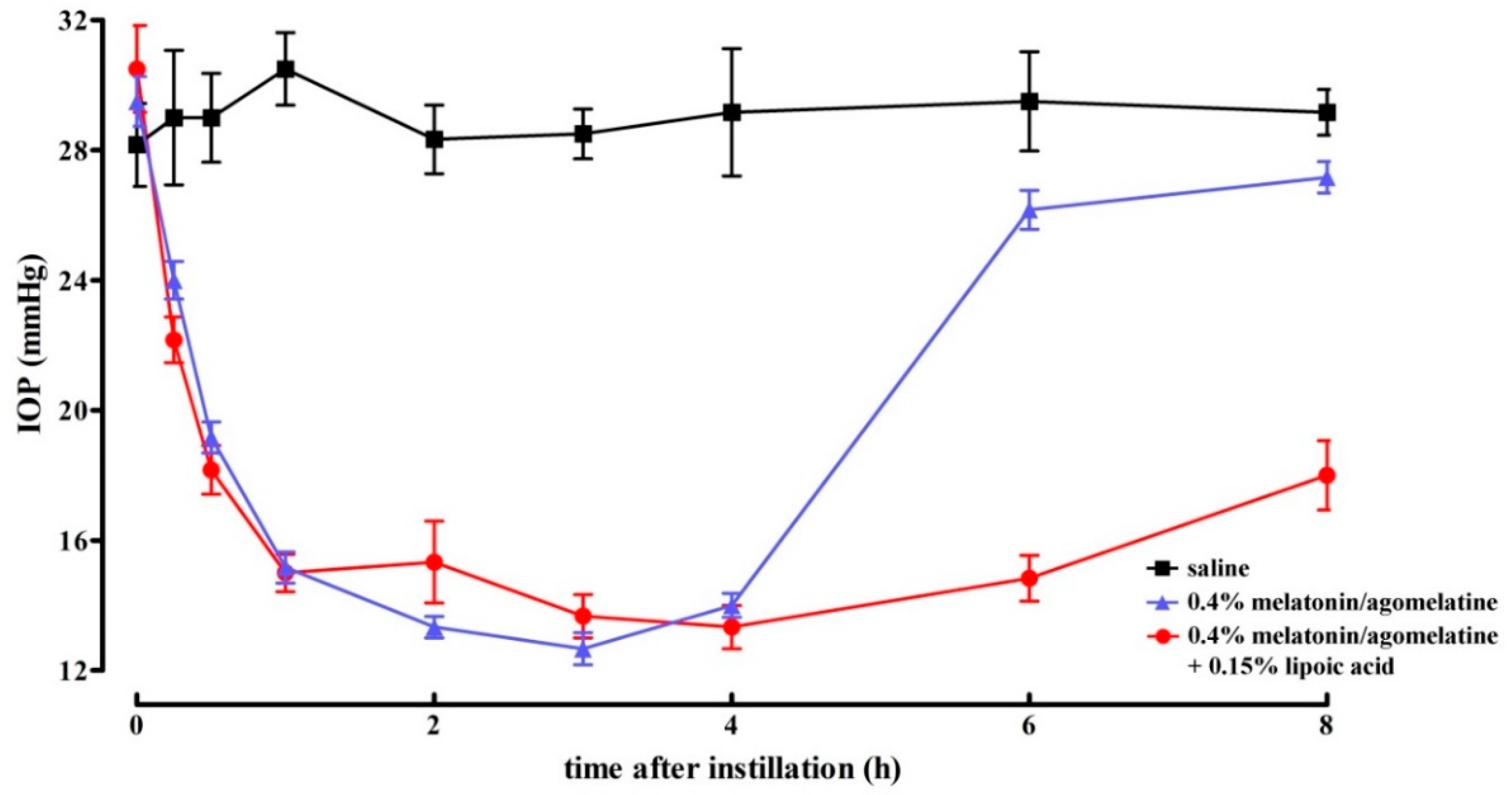
3.3. Hypertensive IOP: Effect of Nanomicellar Formulations with Combined Melatonin and Agomelatine, without or with Lipoic Acid
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alkozi, H.A.; Navarro, G.; Franco, R.; Pintor, J. Melatonin and the control of intraocular pressure. Prog. Retin. Eye Res. 2019. [Google Scholar] [CrossRef]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Kastner, A.; King, A.J. Advanced glaucoma at diagnosis: Current perspectives. Eye (London) 2020, 34, 116–128. [Google Scholar] [CrossRef]
- Asiedu, K.; Abu, S.L. The impact of topical intraocular pressure lowering medications on the ocular surface of glaucoma patients: A review. J. Curr. Ophthalmol. 2018, 31, 8–15. [Google Scholar] [CrossRef]
- Quigley, H.A. Glaucoma. Lancet 2011, 377, 1367–1377. [Google Scholar] [CrossRef]
- Guglielmi, P.; Carradori, S.; Campestre, C.; Poce, G. Novel therapies for glaucoma: A patent review (2013–2019). Expert. Opin. Ther. Pat. 2019, 29, 769–780. [Google Scholar] [CrossRef]
- Gauthier, A.C.; Liu, J. Neurodegeneration and Neuroprotection in Glaucoma. Yale J. Biol. Med. 2016, 89, 73–79. [Google Scholar]
- Oh, D.J.; Chen, J.L.; Vajaranant, T.S.; Dikopf, M.S. Brimonidine tartrate for the treatment of glaucoma. Expert. Opin. Pharmacother. 2019, 20, 115–122. [Google Scholar] [CrossRef]
- Saylor, M.; McLoon, L.K.; Harrison, A.R.; Lee, M.S. Experimental and clinical evidence for brimonidine as an optic nerve and retinal neuroprotective agent: An evidence-based review. Arch. Ophthalmol. 2009, 127, 402–406. [Google Scholar] [CrossRef] [Green Version]
- Krupin, T.; Liebmann, J.M.; Greenfield, D.S.; Ritch, R.; Gardiner, S.; Low-Pressure Glaucoma Study Group. A randomized trial of brimonidine vs. timolol in preserving visual function: Results from the Low-Pressure Glaucoma Treatment Study. Am. J. Ophthalmol. 2011, 151, 671–681. [Google Scholar] [CrossRef]
- Norman, T.R.; Olver, J.S. Agomelatine for depression: Expanding the horizons? Expert. Opin. Pharmacother. 2019, 20, 647–656. [Google Scholar] [CrossRef]
- Martínez-Águila, A.; Fonseca, B.; Pérez de Lara, M.J.; Pintor, J. Effect of Melatonin and 5-Methoxycarbonylamino-N-Acetyltryptamine on the Intraocular Pressure of Normal and Glaucomatous Mice. J. Pharmacol. Exp. Ther. 2016, 357, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Crooke, A.; Huete-Toral, F.; Martínez-Águila, A.; Martín-Gil, A.; Pintor, J. Melatonin and its analog 5-methoxycarbonylamino-N-acetyltryptamine potentiate adrenergic receptor-mediated ocular hypotensive effects in rabbits: Significance for combination therapy in glaucoma. J. Pharmacol. Exp. Ther. 2013, 346, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Águila, A.; Fonseca, B.; Bergua, A.; Pintor, J. Melatonin analogue agomelatine reduces rabbit’s intraocular pressure in normotensive and hypertensive conditions. Eur. J. Pharmacol. 2013, 701, 213–217. [Google Scholar] [CrossRef]
- Carracedo-Rodríguez, G.; Martínez-Águila, A.; Rodriguez-Pomar, C.; Bodas-Romero, J.; Sanchez-Naves, J.; Pintor, J. Effect of nutritional supplement based on melatonin on the intraocular pressure in normotensive subjects. Int. Ophthalmol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Ismail, S.A.; Mowafi, H.A. Melatonin provides anxiolysis, enhances analgesia, decreases intraocular pressure, and promotes better operating conditions during cataract surgery under topical anesthesia. Anesth. Analg. 2009, 108, 1146–1151. [Google Scholar] [CrossRef]
- Pescosolido, N.; Gatto, V.; Stefanucci, A.; Rusciano, D. Oral treatment with the melatonin agonist agomelatine lowers the intraocular pressure of glaucoma patients. Ophthalmic. Physiol. Opt. 2015, 35, 201–205. [Google Scholar] [CrossRef]
- Del Valle Bessone, C.; Fajreldines, H.D.; de Barboza, G.E.D.; Tolosa de Talamoni, N.G.; Allemandi, D.A.; Carpentieri, A.R.; Quinteros, D.A. Protective role of melatonin on retinal ganglionar cell: In vitro an in vivo evidences. Life Sci. 2019, 218, 233–240. [Google Scholar] [CrossRef]
- Scuderi, L.; Davinelli, S.; Iodice, C.M.; Scuderi, L.; Davinelli, S.; Iodice, C.M.; Bartollino, S.; Scapagnini, G.; Costagliola, C.; Scuderi, G. Melatonin: Implications for Ocular Disease and Therapeutic Potential. Curr. Pharm. Des. 2019, 25, 4185–4191. [Google Scholar] [CrossRef]
- Dehdashtian, E.; Mehrzadi, S.; Yousefi, B.; Hosseinzadeh, A.; Reiter, R.J.; Safa, M.; Ghaznavi, H.; Naseripour, M. Diabetic retinopathy pathogenesis and the ameliorating effects of melatonin; involvement of autophagy, inflammation and oxidative stress. Life Sci. 2018, 193, 20–33. [Google Scholar] [CrossRef]
- Mukherjee, R.; Banerjee, S.; Joshi, N.; Singh, P.K.; Baxi, D.; Ramachandran, A.V. A combination of melatonin and alpha lipoic acid has greater cardioprotective effect than either of them singly against cadmium-induced oxidative damage. Cardiovasc. Toxicol. 2011, 11, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Inman, D.M.; Lambert, W.S.; Calkins, D.J.; Horner, P.J. α-Lipoic acid antioxidant treatment limits glaucoma-related retinal ganglion cell death and dysfunction. PLoS ONE 2013, 8, e65389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.D.; Cai, F.Y. Development of experimental chronic intraocular hypertension in the rabbit. Aust. N. Z. J. Ophthalmol. 1992, 20, 225–234. [Google Scholar] [CrossRef]
- Dey, A.; Manthey, A.L.; Chiu, K.; Do, C.W. Methods to Induce Chronic Ocular Hypertension: Reliable Rodent Models as a Platform for Cell Transplantation and Other Therapies. Cell. Transplant. 2018, 27, 213–229. [Google Scholar] [CrossRef] [Green Version]
- Alarma-Estrany, P.; Guzman-Aranguez, A.; Huete, F.; Peral, A.; Plourde, R., Jr.; Pelaez, T.; Yerxa, B.; Pintor, J. Design of novel melatonin analogs for the reduction of intraocular pressure in normotensive rabbits. J. Pharmacol. Exp. Ther. 2011, 337, 703–709. [Google Scholar] [CrossRef] [Green Version]
- Rusciano, D.; Pezzino, S.; Mutolo, M.G.; Giannotti, R.; Librando, A.; Pescosolido, N. Neuroprotection in Glaucoma: Old and New Promising Treatments. Adv. Pharmacol. Sci. 2017, 2017, 4320408. [Google Scholar] [CrossRef]
- Mandal, A.; Cholkar, K.; Khurana, V.; Shah, A.; Agrahari, V.; Bisht, R.; Pal, D.; Mitra, A.K. Topical Formulation of Self-Assembled Antiviral Prodrug Nanomicelles for Targeted Retinal Delivery. Mol. Pharm. 2017, 14, 2056–2069. [Google Scholar] [CrossRef]
- Quinteros, D.; Vicario-de-la-Torre, M.; Andrés-Guerrero, V.; Palma, S.; Allemandi, D.; Herrero-Vanrell, R.; Molina-Martínez, I.T. Hybrid formulations of liposomes and bioadhesive polymers improve the hypotensive effect of the melatonin analogue 5-MCA-NAT in rabbit eyes. PLoS ONE 2014, 9, e110344. [Google Scholar] [CrossRef]
- Osborne, N.N. Serotonin and melatonin in the iris/ciliary processes and their involvement in intraocular pressure. Acta Neurobiol. Exp. (Wars) 1994, 54, S57–S64. [Google Scholar]
- Conway, S.; Canning, S.J.; Howell, H.E.; Mowat, E.S.; Barrett, P.; Drew, J.E.; Delagrange, P.; Lesieur, D.; Morgan, P.J. Characterisation of human melatonin mt(1) and MT(2) receptors by CRE-luciferase reporter assay. Eur. J. Pharmacol. 2000, 390, 15–24. [Google Scholar] [CrossRef]
- Rochette, L.; Ghibu, S.; Richard, C.; Zeller, M.; Cottin, Y.; Vergely, C. Direct and indirect antioxidant properties of α-lipoic acid and therapeutic potential. Mol. Nutr. Food Res. 2013, 57, 114–125. [Google Scholar] [CrossRef]
- Arivazhagan, P.; Shila, S.; Kumaran, S.; Panneerselvam, C. Effect of dl-alpha-lipoic acid on the status of lipid peroxidation and antioxidant enzymes in various brain regions of aged rats. Exp. Gerontol. 2002, 37, 803–811. [Google Scholar] [CrossRef]
- Pescosolido, N.; (Department of Clinical Internal, Anesthesiological and Cardiovascular Sciences, Sapienza University of Rome, Rome, Italy). Personal communication. 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | 0.4% Melatonin in Saline | 0.4% Melatonin in Nanomicelles |
|---|---|---|
| 0 | 3.7% | 2.4% |
| 15 min | −29.4% 1 | −31.8% 1 |
| 30 min | −7.1% | −36.4% 1,2 |
| 1 h | −8.3% | −9.5% |
| 2 h | −6.9% | −9.3% |
| 3 h | −3.5% | −4.7% |
| 4 h | −3.5% | −7.1% |
| 6 h | 3.7% | 2.4% |
| 8 h | 3.7% | 1.3% |
| Time | 0.4% Melatonin | 0.4% Agomelatine | 0.4% Melatonin/Agomelatine | 0.8% Melatonin | 0.8% Agomelatine | 0.8% Melatonin/Agomelatine | 0.4% Melatonin/Agomelatine + 0.15% Lipoic Acid |
|---|---|---|---|---|---|---|---|
| 0 | −1.2% | 0 | −2.4% | 0 | −3.6% | −8.4% | 4.8% |
| 15 min | −28.9% 1 | −19.2% 2 | −25.3% 1 | −37.3% 1 | −25.3% 1 | −37.3% 1 | −11.0% 2 |
| 30 min | −30.1% 1 | −27.7% 1 | −34.9% 1 | −39.1% 1 | −30.5% 1 | −37.8% 1 | −25.6% 1 |
| 1 h | −12.2% | −29.3% 1 | −28.1% 1,3 | −21.9% 4,5 | −34.2% 1 | −32.9% 1 | −31.7% 1 |
| 2 h | −9.5% | −10.7% | −32.1% 1,6,7 | −11.9% | −32.1% 1,8 | −32.1% 1,9 | −41.0% 1 |
| 3 h | −2.4% | −8.7% | −25.9% 1,6,7 | −9.9% | −19.8% 10 | −28.4% 1,11 | −38.3% 1 |
| 4 h | −5.0% | −7.4% | −21.0% 5,8,11 | −8.7% | −7.4% | −25.9% 1,10,11 | −44.4% 1,11,12 |
| 6 h | 0 | −7.5% | −8.7% | −6.2% | −3.6% | −18.9% 2,10,11,13 | −27.5% 1,14,15 |
| 8 h | −1.3% | −6.1% | −7.4% | −2.4% | −1.3% | −7.4% | −24.7% 1,14,16 |
| Time | 0.4% Melatonin/Agomelatine | 0.4% Melatonin/Agomelatine + 0.15% Lipoic Acid |
|---|---|---|
| 0 | 4.7% | 8.3% |
| 15 min | −17.2% 1 | −23.6% 2 |
| 30 min | −33.9% 2 | −37.3% 2 |
| 1 h | −50.3% 2 | −50.8% 3 |
| 2 h | −52.9% 2 | −45.9% 2 |
| 3 h | −55.5% 2 | −52.0% 2 |
| 4 h | −52.0% 2 | −54.3% 2 |
| 6 h | −26.0% | −49.7% 2,3 |
| 8 h | −6.9% | −38.3% 2,3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dal Monte, M.; Cammalleri, M.; Pezzino, S.; Corsaro, R.; Pescosolido, N.; Bagnoli, P.; Rusciano, D. Hypotensive Effect of Nanomicellar Formulation of Melatonin and Agomelatine in a Rat Model: Significance for Glaucoma Therapy. Diagnostics 2020, 10, 138. https://doi.org/10.3390/diagnostics10030138
Dal Monte M, Cammalleri M, Pezzino S, Corsaro R, Pescosolido N, Bagnoli P, Rusciano D. Hypotensive Effect of Nanomicellar Formulation of Melatonin and Agomelatine in a Rat Model: Significance for Glaucoma Therapy. Diagnostics. 2020; 10(3):138. https://doi.org/10.3390/diagnostics10030138
Chicago/Turabian StyleDal Monte, Massimo, Maurizio Cammalleri, Salvatore Pezzino, Roberta Corsaro, Nicola Pescosolido, Paola Bagnoli, and Dario Rusciano. 2020. "Hypotensive Effect of Nanomicellar Formulation of Melatonin and Agomelatine in a Rat Model: Significance for Glaucoma Therapy" Diagnostics 10, no. 3: 138. https://doi.org/10.3390/diagnostics10030138