
Type 2 Diabetes and Impaired Physical Function: A Growing Problem


NIHR Leicester Biomedical Research Centre, University Hospitals of Leicester NHS Trust and the University of Leicester, Leicester LE5 4PW, UK
*
Author to whom correspondence should be addressed.
Diabetology 2022, 3(1), 30-45; https://doi.org/10.3390/diabetology3010003
Submission received: 15 November 2021
/
Revised: 5 January 2022
/
Accepted: 6 January 2022
/
Published: 11 January 2022
Abstract
:The focus in diabetes care has traditionally been around the optimisation of the glycaemic control and prevention of complications. However, the prevention of frailty and improvement in physical function have now emerged as new targets of diabetes management. This is mainly driven by the significant adverse impact that early onset frailty and decline in physical function have on health outcomes, functional independence, and quality of life in people with type 2 diabetes (T2D). There is an increasing emphasis in the expert consensus and management algorithms to improve physical function in people with T2D, predominantly through lifestyle interventions, including exercise and the control of modifiable risk factors. Trials of novel glucose-lowering therapies (GLTs) also now regularly assess the impact of these novel agents on measures of physical function within their secondary outcomes to understand the impact that these agents have on physical function. However, challenges remain as there is no consensus on the best method of assessing physical function in clinical practice, and the recognition of impaired physical function remains low. In this review, we present the burden of a reduced physical function in people with T2D, outline methods of assessment used in healthcare and research settings, and discuss strategies for improvement in physical function in people with T2D.
1. Physical Function and Frailty
Physical function is the ability to perform basic activities of daily living (ADL) and instrumental activities of daily living (IADL) that are essential to independent living and have a major impact on quality of life [1,2]. Examples include sitting down and standing up out of a chair, dressing oneself, climbing stairs, taking a shower, and using the toilet. The ability to perform all these activities depends on the complex but co-ordinated functioning of multiple physiological systems, including the musculoskeletal and cardiorespiratory systems [2]. Disruption in this interplay of physiological systems could lead to impaired physical function and, ultimately, frailty.
Frailty is defined as a state of increased vulnerability to physical or psychological stressors because of a reduced physiological reserve in multiple organ systems that causes a limited capacity to maintain homeostasis [3], leading to a reduced capacity to function independently. The presence of three or more of the following five criteria, (i) unintentional weight loss, (ii) low energy-expenditure, (iii) exhaustion (iv), slowness, and (v) weakness, is commonly used to recognise frailty [4].
A concept closely related to impaired physical function is physical disability, which is defined as difficulty in carrying out activities essential to independent living, including tasks needed for self-care and which are considered important for a good quality of life [5]. Whilst distinct, an impairment in physical function may often be predictive of a future physical disability [6].
2. The Phenotype of Frailty in Type 2 Diabetes
When the term frailty is mentioned, the first concept that usually comes to mind is a thin elderly person using a frame or a stick for mobility and who is at an increased risk of recurrent falls, infection, illness, and hospitalisation. However, conversely, the frailty phenotype in type 2 diabetes (T2D) can coexist in younger persons with underlying obesity and multiple comorbidities.
This is a rapidly emerging pattern in people with T2D due to an increase in the incidence of early onset T2D (<40 years) with obesity, particularly in certain minority ethnic groups and is co-associated with reduced physical fitness and functional muscle mass [7]. T2D as a chronic condition is associated with a state of accelerated metabolic ageing, often leading to a cluster of physical problems typical of the elderly population, including functional decline, physical disability, falls and fractures [8]; thus, predisposed to adverse health outcomes and impaired quality of life.
Given its links to functional independence and quality of life, improvement in physical function may often be very high on the treatment agenda for someone with T2D. In an exploratory study of self-reported goals of care in people with T2D aged 65 or above, it was discovered that maintaining functionality and independence with ADLs (71%) was more important than the optimisation of blood glucose control (3.5%), weight loss (14%), or avoidance of symptoms (3.5%) [9]. Thus, improvement in physical function in people with T2D should be both a clinical and research priority.
3. Wider Recognition of Impaired Physical Function form Health Experts
There is an increasing recognition of poor physical function in people with T2D by health authorities and experts. The National Institute for Health and Care Excellence (NICE) recommended several indicators taking account of frailty in people with diabetes that were added to the 2018/19 quality and outcomes framework (QOF) for diabetes and, furthermore, coding of the frailty status for people with diabetes were also included in the latest General Medical Services contract [10,11]. Algorithms for diabetes management, especially T2D, within which the frailty status is prominent in decision making/goal-setting, have also been proposed [12,13,14,15]. However, what these guidelines and consensus recommendations often fail to highlight is that frailty and reduced physical function in diabetes is not necessarily coupled to senescence. In fact, this can occur at a much younger age and needs wider recognition with integration into the holistic model of diabetes care.
4. Assessment of Physical Function
Assessments of physical function that are fit-for-purpose may differ between clinical practice (where there is a need for quick but reliable tools) and clinical research (where more comprehensive, validated methods that are sensitive to small changes with interventions may be preferred). This section outlines commonly used methods within each of these settings.
4.1. Assessment of Physical Function in Clinical Practice
A functional assessment should be a part of the routine diabetes care, especially in older individuals [16], and should ideally be a multidimensional and multidisciplinary approach [17]. However, there is no consensus on the gold-standard measurement of physical function in clinical practice and, therefore, several different methods are used, ranging from self-reported questionnaires to more detailed functional tools [1].
In the UK, primary care clinicians are generally encouraged to identify frailty using an electronic Frailty Index (eFI), which is a composite score based on pre-existing conditions, for all people aged 65 or over. This enables primary care software such as SystmOne© to automatically calculate a frailty score without the need for a physical assessment, using already stored pre-existing information [18,19,20]. It looks at the number of deficits across different clinical conditions and then divides it by 36 to produce a score to describe the degree of frailty.
However, in an outpatient secondary care setting, with often limited access to primary care data, simple but reliable methods can be used to assess physical function. One can simply look at mobility aids such as sticks or ask simple questions to gauge the functional independence of their patients when they first walk into the clinic or by performing a quick but reliable and valid test for quantifying functional mobility such as a 4-metre gait speed evaluation (which can be used as a standalone tool or as a component of the Short Physical Performance Battery [SPPB]) [21] or a “timed up and go” test (which assesses the time required for an individual to stand up from a standard chair with an armrest, walk 3 m, turn around, walk back to the chair, and sit down again) [22,23,24].
A thorough medical history (including social history) and physical examination (particularly for the presence of neuropathy), which all form part of routine diabetes care, could also help in the overall assessment of physical function.
Simply asking people to score their habitual walking pace as slow, steady/average, or brisk is also highly predictive of all-cause or cardiovascular mortality, with slow walking associated with a shorter life expectancy [25,26,27,28]. The use of technology, such as built-in mobile pedometers, can be used effectively to gauge physical activity in clinics. For individuals less familiar with such technology, they can be encouraged and supported to become acquainted with such digital tools to not only improve their physical fitness, but also lower cardiometabolic risk factors such as systolic blood pressure [29].
For those interested in formal assessments and documentation, easy to use and rapid screening tests have been validated to recognise frail individuals in clinical practice, including the Rockwood Clinical Frailty Scale (CFS) [30]. This does not assess physical function directly, but can give you an estimate of physical impairment and overt frailty [31].
4.2. Assessment of Physical Function in Clinical Trials
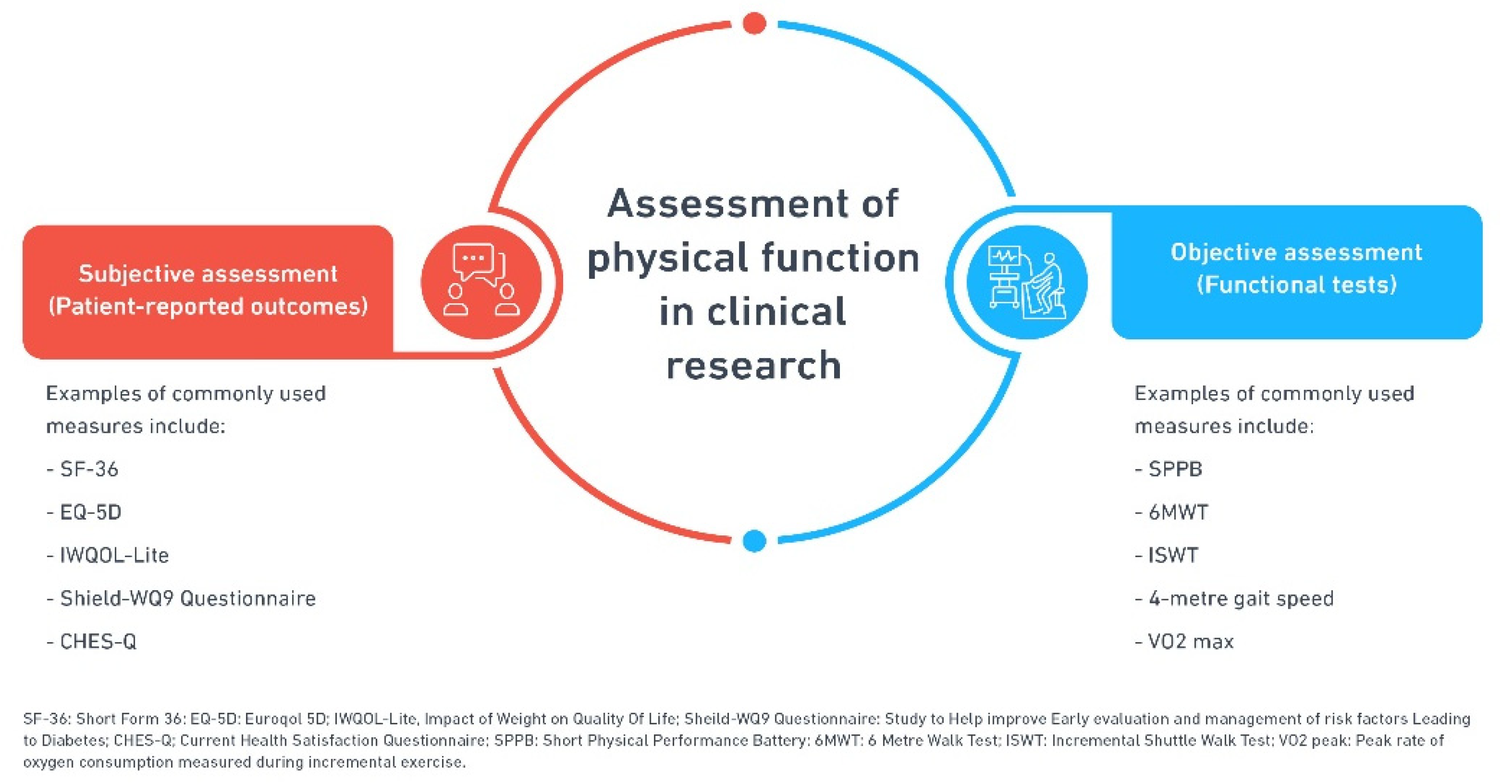
Diverse tools have been employed in clinical research to measure physical function either directly or indirectly, from the use of subjective, but validated, questionnaires and patient-reported outcomes (PRO), e.g., the 36-Item Short Form Survey (SF36) [32], EuroQol-5D (EQ-5D) [33], Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes (SHIELD-WQ9) [34], 14-item Current Health Satisfaction Questionnaire (CHES-Q) [35], and Impact of Weight on Quality of Life-Lite (IWQOL-Lite) [36], to physical laboratory-based assessments that can test an individual’s capacity to perform basic ADL and IADL. Some of these assess gross motor function such as the modified physical performance test (mPPT) [37] and the short physical performance battery (SPPB) [21,38]. Others, such as the 6 min walk test (6MWT) [39] and incremental shuttle walk test (ISWT) [40], assess walking speeds and functional fitness, in the lower limbs mainly. VO2 max, which measures the maximal oxygen consumption during exercise, provides an adequate indication of overall cardiovascular fitness and aerobic endurance [41,42].
Figure 1 shows some of the common measures of physical function in clinical research involving T2D.
Walking tests are primarily more widely used as objective measures of physical function in research settings, including rehabilitation research, as these tend to provide a more accurate assessment of improvement in functional capacity. On the other hand, subjective assessments, especially PROs, mostly assess physical function as one component of overall health, with different tools analysing physical and mental health domains separately, e.g., SF-36 [32,43].
Most of these objective and subjective tools are validated for different chronic conditions and are not diabetes specific, so deciding on the best method to assess physical function in T2D remains largely undecided.
5. The Importance of Physical Function in People with T2D
There are a number of reasons why the assessment and management of poor physical function should be a key priority in T2D management, as outlined below.
5.1. High Prevalence of Impaired Physical Function across All Age Groups
With an increasing diabetes prevalence, frailty and physical disability are now emerging as the third major category of complications in people with diabetes after the traditionally acknowledged micro- and macro- vascular complications [44]. The frailty prevalence of 32% to 48% in people with diabetes older than 65 is much higher than the 5% to 10% seen in the general population [45]. Overall, diabetes ranks amongst the top five chronic conditions associated with frailty, as demonstrated in analyses using the UK Biobank cohort (aged 37–73) [46].
As outlined above, frailty in diabetes, in contrast to many other chronic conditions, also often occurs at a younger age [47]. A cross-sectional analysis of data from 99,357 respondents ≥18 years of age, utilising a self-reported degree of difficulty with nine physical tasks, found that, across all age groups, a higher proportion of people with diabetes had some physical limitation compared to those without diabetes [48], as shown in Table 1.
This physical impairment is distributed across different functional tasks of daily living. In a study from the USA, looking at 6097 participants with a mean age of approximately 70 years, the disability in people with diabetes across various physical functional tasks was distributed as follows (Table 2) [49].
Other observational studies in different populations have also shown that people with diabetes are more likely to report difficulty in performing daily tasks compared to those without diabetes. A cross-sectional analysis of 5035 participants showed an impairment of physical function across four distinct functional domains, with the greatest diabetes-related burden in ADL followed by IADL, lower extremity mobility, and general physical activities [50]. In a Mexican longitudinal study (n = 785), deficits in ADL and IADL were ~2.5 and 3 times more common, respectively, in people with diabetes than in people without [51], whilst a 2013 meta-analysis found that diabetes increased the risk of disability in performing both IADL and ADL by approximately 65–82% (odds ratio (OR) 1.65 (95% Confidence Interval (CI) 1.55, 1.74) and 1.82 (95% CI 1.63, 2.04), respectively). In an ongoing cross-sectional study by our group, the “Chronotype of Patients with Type 2 Diabetes and Effect on Glycaemic Control (CODEC)” study, we assessed physical function using SPPB in people with T2D across the East Midlands, UK. In the analyses of the first ~650 participants, 29% scored < 10 on the SPPB, suggesting impaired physical function [52]. A Chinese study, using a 32-item frailty index, found a higher prevalence and incidence of frailty, not only in people with diabetes, but also in people with pre-diabetes [53]. Overall, we now know that people with diabetes are up to five times more likely to be frail than those without diabetes [45].
Impaired physical function is common in both men and women with diabetes. Among those with diabetes ≥ 60 years of age, 32% of women and 15% of men report an inability to walk one quarter of a mile, climb stairs, or do housework, compared with 14% of women and 8% of men without diabetes [38]. A prospective cohort looking at 8344 women aged 65 or above with diabetes revealed that the yearly incidence of any functional disability was 9.8% among women with diabetes compared to only 4.8% among women without diabetes [54]. In a study using the physical function component of the SF-36 questionnaire, the men with T2D were 2.7 times more likely to have poor physical function than those with a normal glucose tolerance [55]. These data confirm the high prevalence of impaired physical function across different age groups in people with T2D, irrespective of gender and geographic location.
5.2. Physical Function Is a Dynamic Process
It is important to remember that, unlike natural ageing or senescence, which is irreversible, frailty and physical function are dynamic and potentially reversible processes [56,57]. Hence, by addressing modifiable risk factors linked to poor physical function in people with T2D, such as poor glycaemic control, a raised body mass index (BMI), elevated blood pressure, and cholesterol profile, it is possible that significant inroads can be established to improving functional outcomes for people with diabetes. However, such as with many other chronic conditions, early recognition and intervention are key to successful outcomes, because if left unrecognised, could lead to accelerated aging and an increased risk of physical disability.
5.3. Adverse Health Outcomes Associated with Decline in Physical Function
Frailty increases the risk of adverse health outcomes, including an increased risk of hospitalization and death in people with diabetes compared to non-frail counterparts [58]. In a study on predicting the risk of physical disability in old age using modifiable mid-life risk factors, it was found that a young 45-year-old man or woman with the combined risk factors of obesity, diabetes, and smoking has a similar likelihood of surviving free of disability to a 65-year-old person without any of the same risk factors [59]. As a result of this increased propensity to early onset disability, the estimated loss of life expectancy associated with diabetes at a young age of 50 years is approximately 3.2 years for men and 3.1 years for women, compared with their counterparts without diabetes [60].
The International Diabetes Federation (IDF) acknowledges that frailty reduces the ability to cope with stressors and leads to increased risks of falls and hospitalisation [12]. Frailty is now emerging as a strong predictor of adverse outcomes, including institutionalization and mortality [16]. For these reasons, the assessment of frailty and physical function in patients with T2D should be part of the routine clinical care.
6. Mechanisms Underlying Reduced Physical Function in T2D
6.1. Multimorbidity in T2D
Decline in physical function in T2D is multifactorial. Poor glycaemic control, diabetes duration, concurrent cardiometabolic co-morbidities (e.g., obesity and renal disease), hormonal imbalances (e.g., thyroid disorders and hypogonadism), cognitive decline, diabetes-related complications (both microvascular and macrovascular), nutritional deficiencies, polypharmacy, hypoglycaemia associated with certain medications (e.g., insulin and sulphonylureas), and chronic underlying inflammation have all been postulated to contribute to impaired physical function in people with T2D [61,62,63,64,65,66,67,68]. Multimorbidity, in general, increases the frailty risk [69] and the presence of multiple comorbidities with functional impairments having been found to be a more important predictor of a reduced life expectancy in people with T2D than age alone [70]. However, it is difficult to be exactly certain of the contribution from comorbidities and other factors in terms of the decline in physical function in people with T2D, and studies have shown some varying results with regard to the contribution of individual factors towards impaired physical function and disability in people with T2D.
Koye et al. analysed data from individuals aged 60 years or above 12 years after the baseline study of AusDiab (with the vast majority comprising of people with T2D) to examine the association between diabetes and disability in older Australians and identify factors underpinning this association [71]. They adjusted for different factors, including baseline demographics, lifestyle, and cardiometabolic factors, to determine which of these variables could explain the association between diabetes and risk of disability at 12 years. They found that, among men, baseline BMI and other cardiometabolic factors individually were responsible for 68% and 23% increased odds of disability at 12 years, respectively. Similarly, in women, baseline BMI and other cardiometabolic factors explained 48% and 37% of the odds of disability after 12 years, respectively. They concluded that baseline BMI was the most important contributor to disability in people with diabetes, explaining 50–70% of the excess odds of disability in this group. Cardio-metabolic factors (hypertension, cardiovascular, and renal disease, all together) explained another 25–35% of the excess odds of disability. However, there was no baseline data on the functional status and loss to follow-up because of severe disability possibly having affected the results.
Data from an Italian study looking at physical disability using a physical performance test (PPT) among people with diabetes also showed that after adjusting for various factors among both men and women, an increased BMI was the most important condition explaining the increased risk of impairment in physical functioning (8% and 16%, respectively) [72]. Combining all conditions, including the BMI and cardiometabolic comorbidities, explained 16% of the excess risk of physical disability in men and 38% in women.
Greg et al. analysed data from 6588 community-dwelling men and women, adjusting for various factors, including age, ethnicity, diabetes duration, BMI, and comorbidities to explain the association between diabetes and the risk of physical disability [38]. They also confirmed that, in people with diabetes, especially in women, BMI and coronary heart disease (CHD) were more important than other comorbidities in explaining the increased risk of impaired physical function and disability. An interesting observation they determined was that even after controlling for all of the above factors, including BMI and CHD, women and men with diabetes still had 50% and 46% increased odds of disability, respectively, versus people without diabetes.
A population-based case–control study looked at physical function in 403 individuals with diabetes compared to 403 matched controls [73]. The study assessed physical function using validated tools, including the Barthel index, Nottingham Extended Activities of Daily Living Scale, and SF-36 questionnaire. The study showed a significant impairment of physical function in people with diabetes compared to their matched controls without diabetes. They attributed this to the increased prevalence of comorbidities, particularly cardiovascular comorbidities, complications such as peripheral neuropathy and polypharmacy.
These studies confirm the detrimental impact of cardiometabolic comorbidities, particularly a raised BMI, on physical function in people with diabetes and just having a poor glycaemic control is not responsible for the decline in physical function. This was also endorsed by results from the National Health and Nutrition Examination Survey (NHANES), 1999–2006, which confirmed that comorbidities, mostly cardiovascular disease and obesity, and poor glycaemic control (HbA1c ≥ 8%), together explained up to 85% of the excess odds of disability associated with diabetes, whereas poor glycaemic control alone explained only 10% of the excess odds [49].
6.2. Sarcopenia and T2D
A crucial concept in understanding physical function in people with T2D is sarcopenic obesity. Sarcopenia and frailty are intricately linked by the shared core reduction in physical function, which ultimately leads to an increased risk of disability [74]. Sarcopenia is generally characterised by a low muscle mass and strength, which play an important role in functional decline [75,76]. In sarcopenic obesity seen in T2D, however, this occurs alongside excess adiposity and often a low muscle quality and functional capacity despite a large muscle volume [75,77].
The underlying pathophysiology in sarcopenia is progressive muscle atrophy with the loss of muscle fibres, both type I and type II, and replacement by fat and other non-contractile connective tissue [78,79], alongside changes in muscle metabolism [80]. There is a strong association between diabetes and sarcopenia [81], as both share common etiological pathways [75,77,82,83]. In diabetes, metabolic disturbances, including insulin resistance, lead to increased oxidative stress, endothelial dysfunction, and an altered mitochondrial function, ultimately causing the accelerated loss of muscle mass, strength, and contractile efficiency [82,84,85]. We now know that skeletal muscle mitochondria in people with T2D and those with obesity are smaller in size (~30%) and less functional compared to lean age-matched controls without diabetes [86,87]. An improvement in insulin sensitivity through exercise has been shown to normalise this mitochondrial dysfunction [88].
It is widely believed that sarcopenia is in fact an intermediate step between diabetes and frailty [8]. This can be attributed not only to the imbalance in the factors highlighted above, but also because obesity and physical inactivity is common in people with T2D, which contributes to muscle wasting and decline in physical function (Figure 2).
The association of T2D and sarcopenia is further established in prospective studies. A study using a dual-energy X-ray absorptiometry (DEXA) scan to measure the body composition and a computerised tomography (CT) scan to assess the thigh muscle cross sectional area (CSA) over 6 years showed an excessive loss of appendicular lean mass in people with either diagnosed or previously undiagnosed T2D, compared with individuals without diabetes [83]. They concluded that the excessive loss of muscle mass in older adults with T2D may result in poor muscle strength, functional limitations, and physical disability.
Another study assessing functional capacity and pedometer-measured physical activity in 100 people with T2D (median of 6429 steps per day) found that, after adjusting for age and sex, lower muscle strength and the presence of neuropathy were responsible for a reduction of 1782 and 1967 steps per day, respectively [62]. Each 1 kg/m2 increase in BMI was responsible for a reduction of 210 steps per day.
7. Interventions to Improve Physical Function
7.1. Role of Exercise
Of the interventions known to improve physical function, exercise training is considered to be most effective, including in people with T2D [89,90,91,92]. In particular, a combination of resistance and endurance training has been shown to have greatest benefits [14]. Exercise counteracts many of the factors responsible for impaired physical function and improves blood supply and nutrient delivery to working tissues [85,93]. Fielding reported in 1995 that an increase in fat mass and decline in skeletal muscle mass contribute to functional dependence in elderly individuals, and that strength training interventions could be employed as a powerful tool in the prevention of this loss of muscle mass [94].
In a systematic review of interventions to prevent disability in frail elderly, whilst no evidence was found for the effect of nutritional interventions on improving disability, exercise (especially multicomponent exercise programmes) showed beneficial effects on improving the ability to perform both ADL and IADL [95].
In T2D specifically, a recent meta-analysis also demonstrated that resistance training not only reduced HbA1c (~0.50%), but also increased muscular strength by 38% in elderly people with T2D [96]. A similar study looked at the effects of long-term resistance training in people with diabetes and showed ~33% increased strength for all muscle groups after 6 months of training [97].
Exercise training, even without an overall body weight loss, improves insulin sensitivity and fasting glycaemia and decreases abdominal fat in older people with T2D [98]. Two main mechanisms underlying this beneficial effect of exercise on insulin sensitivity are the loss of visceral adipose tissue [99] and increase in muscle mass, which provides an increased storage area for glucose; thus, reducing blood glucose [100,101,102,103].
Exercise also confers cardiovascular benefits and can be used as a strong tool to improve physical fitness, especially in the management of frailty [91,99]. A study in obese people with T2D showed that exercise increases oxygen utilisation as measured by VO2 max by 41%, improves insulin sensitivity by 46%, reduces visceral adipose tissue by 48%, and leads to an 18% loss of subcutaneous fat without any significant effect on body weight [99].
Combining different lifestyle interventions (e.g., dietary interventions) with structured exercise programmes can have added benefit. For example, the combination of a resistance exercise programme alongside structured diabetes and nutritional support in functionally impaired people with T2D led to a mean SPPB score 0.85 times higher than those of the usual care group at the end of 12 months (95% CI 0.44, 1.26, p < 0.001) [104], indicating better physical function in the intervention group compared to the control group.
In the Look AHEAD trial, a multisite randomized controlled trial of 5145 overweight and obese people, the lifestyle intervention group had a relative reduction of 48% in the risk of loss of mobility, as compared with the diabetes support and education group (OR 0.52; 95% CI 0.44, 0.63; p < 0.001) [105]. In this study, the participants in the lifestyle intervention group reported better physical function as assessed by SF-36 than the diabetes support and education group throughout the first 8 years (mean difference = 0.93; p < 0.001).
Even light-intensity physical activity is associated with improvement in self-rated physical and psychological health [106] and, thus, it is important to encourage physical activity in all adults with diabetes to improve physical functioning.
Despite all this evidence, incorporating and prescribing tailored exercise programmes in clinical practice remains a challenge. There is now an emerging recognition of resistance and endurance exercises in management algorithms to address frailty [13]. The Erasmus Vivifrail Project focuses on providing training for Healthcare Professionals (HCPs) and social care providers to promote and prescribe exercise programmes in older individuals [107]. However, it is vital to remember that tailoring exercise programmes to individual needs and capacity is crucial to support continued adherence and improve the likelihood of successful outcomes [104]. In the follow-up of the LIFE study, 1-year after the cessation of exercise intervention, the improvement in physical function between the intervention group and control, as determined by SPPB, was lost [108]; thus, supporting the argument for flexible and preferably supervised exercise programmes for sustained benefits.
7.2. Controlling the Risk Factors
In addition to lifestyle interventions, namely, diet and exercise, addressing modifiable risk factors should be part of the multimodal approach to improving physical function in people with T2D. This includes improving glycaemic control, the management of co-morbidities (particularly a raised BMI and cardiovascular co-morbidities), optimising lipid and blood pressure control, correction of hormonal imbalances and nutritional deficiencies, and review of medications; thus, avoiding polypharmacy as part of a comprehensive management plan [109]. A collective position statement from the International Association of Gerontology and Geriatrics (IAGG), the European Diabetes Working Party for Older People (EDWPOP), and the International Task Force of Experts in Diabetes, which recognises progressive functional loss as a significant risk to patient safety, also recommends the regular assessment of both physical and cognitive function, the avoidance of polypharmacy, and encourages the use of simplified treatment regimens to achieve realistic glucose targets [110].
7.3. Physical Function and Novel Glucose Lowering Agents
Until recently, the assessment of physical function in clinical trials of glucose-lowering therapies (GLTs) was not universally considered. However, with the advent of modern agents, particularly sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonist (GLP-1RA), which are associated with clinically meaningful weight loss and cardio-renal benefits, this is transforming, and the assessment of physical function is becoming an important secondary outcome in many large randomised–controlled trials (RCTs) of these agents [111]. This is mainly driven by the observation from large cardiovascular outcome trials, that not only do these agents improve glycaemic control, but also confer additional cardiometabolic benefits, similar to exercise and induce weight loss, all of which could lead to meaningful improvements in physical function. There is also evidence that these novel agents have anti-inflammatory potential and beneficial effects on blood pressure, endothelial function, and lipid profile [112,113], which could improve cellular metabolism in people with T2D. However, dedicated randomised clinical trials assessing physical function as a primary outcome are urgently needed to understand the exact impact of these novel agents on physical function, functional independence, and quality of life to increase our arsenal against poor physical function in people with T2D in addition to existing lifestyle interventions.
7.4. Interplay between Exercise and Novel GLTs
There is a paucity of evidence investigating precisely how exercise training interacts with GLTs, especially the newer agents such as SGLT2i and GLP-1RAs and their combined impact on physical function [114].
Previous evidence suggests that the interaction between metformin, the most commonly prescribed agent, and exercise has not proven very beneficial and blunts each other’s individual beneficial effects on insulin sensitivity, cardiovascular risk factors (including blood pressure and inflammation), aerobic capacity, and postprandial glucose levels [115,116,117,118,119,120].
Evidence around the impact of the combination therapy of exercise and either SGLT2i or GLP-1RA on physical function is limited. A recent 12-week RCT looked at the impact of endurance exercise when combined with either dapagliflozin, an SGLT2i, or placebo [121]. Although the study failed to demonstrate any synergistic effects of the combination of dapagliflozin and endurance exercise compared to the placebo plus endurance exercise on body mass and cardiorespiratory fitness, dapagliflozin did not attenuate these either. Another study explored the impact of liraglutide, a GLP-1RA, alone or in combination with exercise therapy (150 min per week) on physical function assessed using time to ascend/descend an 11-step stairway twice and cardiorespiratory fitness using peak oxygen consumption [122]. Again, adding liraglutide did not negatively impact the improvement in physical fitness with exercise, but the results were not encouraging either. Thus, so far, the available evidence on combining exercise with novel agents is not very convincing. Additionally, it will be worth considering the impact these combination therapies might have on other aspects of diabetes care, particularly the risk of hypoglycaemia, dehydration, and euglycaemic diabetic ketoacidosis, especially when combining exercise with SGLT2 inhibitor therapy.
In summary, how structured exercise can be effectively combined with novel GLTs to improve physical function and cardiometabolic fitness through routine care in people with T2D remains largely unanswered, and there is an unmet research and clinical need to elucidate the exact impact of these combined therapies (structured exercise and novel GLTs) on physical function [114].
8. Conclusions
People with T2D are at an increased risk of frailty and impaired physical function. The decline in physical function in people with T2D is multifactorial, including sarcopenic obesity. Despite a high prevalence, poor physical function remains largely unrecognised in clinical practice. Structured but flexible exercise programmes could be utilised as an effective tool to improve physical function. Additionally, there is a need to better understand the impact of novel agents on physical function alone and in combination with exercise in people with T2D through the use of dedicated trials.
Author Contributions
Conceptualization, M.J.D., D.R.W., and E.A.; writing—original draft preparation, E.A.; writing—review and editing, M.J.D., D.R.W., T.Y., J.A.S., and E.A.; visualization, M.J.D., T.Y., J.A.S., and E.A.; supervision, M.J.D., D.R.W., T.Y., and J.A.S. All authors have read and agreed to the published version of the manuscript.
Funding
J.A.S. received a grant in support of an investigator-initiated trial from AstraZeneca. T.Y. is supported by the NIHR Leicester BRC and received funding from Astra Zeneca for an investigator-initiated project. D.R.W. received honoraria as a speaker for AstraZeneca, Sanofi-Aventis, and Lilly, and received research funding support from Novo Nordisk. M.J.D. acted as a consultant, advisory board member, and speaker for Novo Nordisk, Sanofi, Lilly, and Boehringer Ingelheim, an advisory board member and speaker for AstraZeneca, an advisory board member for Janssen, Lexicon, Pfizer, Servier, and Gilead Sciences Ltd., and as a speaker for Napp Pharmaceuticals, Mitsubishi Tanabe Pharma Corporation, and Takeda Pharmaceuticals International Inc. She has received grants in support of investigator and investigator-initiated trials from Novo Nordisk, Sanofi-Aventis, Lilly, Boehringer Ingelheim, AstraZeneca, and Janssen.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
This study was supported by the National Institute for Health Research (NIHR) Leicester Biomedical Research Centre (BRC) and the NIHR Leicester Clinical Research Facility (CRF). The views expressed are those of the authors and not necessarily those of the National Health Service, the National Institute for Health Research, or the Department of Health.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Painter, P.; Stewart, A.L.; Carey, S. Physical Functioning: Definitions, Measurement, and Expectations. Adv. Ren. Replace. Ther. 1999, 6, 110–123. [Google Scholar] [CrossRef]
- Garber, C.E.; Greaney, M.L.; Riebe, D.; Nigg, C.R.; Burbank, P.A.; Clark, P.G. Physical and mental health-related correlates of physical function in community dwelling older adults: A cross sectional study. BMC Geriatr. 2010, 10, 6–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, H.; Ferrucci, L.; Guralnik, J.; Hogan, D.; Hummel, S.; Karunananthan, S.; Wolfson, C. Frailty: An Emerging Research and Clinical Paradigm—Issues and Controversies. J. Gerontol. Ser. A 2007, 62, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M255–M263. [Google Scholar] [CrossRef] [Green Version]
- Chalé-Rush, A.; Guralnik, J.M.; Walkup, M.P.; Miller, M.E.; Rejeski, W.J.; Katula, J.A.; King, A.C.; Glynn, N.W.; Manini, T.M.; Blair, S.N.; et al. Relationship Between Physical Functioning and Physical Activity in the Lifestyle Interventions and Independence for Elders Pilot. J. Am. Geriatr. Soc. 2010, 58, 1918–1924. [Google Scholar] [CrossRef] [Green Version]
- Magliano, D.J.; Sacre, J.W.; Harding, J.L.; Gregg, E.W.; Zimmet, P.Z.; Shaw, J.E. Young-onset type 2 diabetes mellitus—Implications for morbidity and mortality. Nat. Rev. Endocrinol. 2020, 16, 321–331. [Google Scholar] [CrossRef]
- Volpato, S.; Maraldi, C.; Fellin, R. Type 2 diabetes and risk for functional decline and disability in older persons. Curr. Diabetes Rev. 2010, 6, 134–143. [Google Scholar] [CrossRef]
- Huang, E.S.; Gorawara-Bhat, R.; Chin, M.H. Self-Reported Goals of Older Patients with Type 2 Diabetes Mellitus. J. Am. Geriatr. Soc. 2005, 53, 306–311. [Google Scholar] [CrossRef] [Green Version]
- NICE. New QOF Indicators Added to Menu by NICE. 2018. Available online: https://diabetestimes.co.uk/new-qof-indicators-added-to-menu-by-nice/ (accessed on 21 June 2021).
- Group PCSaNC. 2019/20 General Medical Services (GMS) contract Quality and Outcomes Framework (QOF) Guidance for GMS contract 2019/20 in Englan. BMA 2019. Available online: https://www.england.nhs.uk/wp-content/uploads/2019/05/gms-contract-qof-guidance-april-2019.pdf (accessed on 22 June 2021).
- Dunning, T.; Sinclair, A.; Colagiuri, S. New IDF Guideline for managing type 2 diabetes in older people. Diabetes Res. Clin. Pract. 2014, 103, 538–540. [Google Scholar] [CrossRef]
- Sinclair, A.J.; Abdelhafiz, A.; Dunning, T.; Izquierdo, M.; Manas, L.R.; Bourdel-Marchasson, I.; Morley, J.E.; Munshi, M.; Woo, J.; Vellas, B. An international position statement on the management of frailty in diabetes mellitus: Summary of recommendations 2017. J. Frailty Aging 2018, 7, 1–11. [Google Scholar] [CrossRef]
- Sinclair, A.; Gallaher, A. Managing Frailty and Associated Comorbidities in Older Adults with Diabetes: Position Statement on behalf of the Association of British Clinical Diabetologists (ABCD). Available online: https://abcd.care/sites/abcd.care/files/site_uploads/Resources/Position-Papers/ABCD-Position-Paper-Frailty.pdf. (accessed on 22 June 2021).
- Strain, W.D.; Down, S.; Brown, P.; Puttanna, A.; Sinclair, A. Diabetes and Frailty: An Expert Consensus Statement on the Management of Older Adults with Type 2 Diabetes. Diabetes Ther. 2021, 12, 1227–1247. [Google Scholar] [CrossRef]
- Castro-Rodríguez, M.; Carnicero, J.A.; Garcia-Garcia, F.J.; Walter, S.; Morley, J.E.; Rodríguez-Artalejo, F.; Sinclair, A.J.; Rodríguez-Mañas, L. Frailty as a Major Factor in the Increased Risk of Death and Disability in Older People with Diabetes. J. Am. Med. Dir. Assoc. 2016, 17, 949–955. [Google Scholar] [CrossRef]
- Sinclair, A.; Dunning, T.; Rodríguez-Mañas, L. Diabetes in older people: New insights and remaining challenges. Lancet Diabetes Endocrinol. 2015, 3, 275–285. [Google Scholar] [CrossRef]
- Strain, W.D.; Hope, S.; Green, A.; Kar, P.; Valabhji, J.; Sinclair, A.J. Type 2 diabetes mellitus in older people: A brief statement of key principles of modern day management including the assessment of frailty. A national collaborative stakeholder initiative. Diabet. Med. 2018, 35, 838–845. [Google Scholar] [CrossRef] [Green Version]
- NHS Electronic Frailty Index. Available online: https://www.england.nhs.uk/ourwork/clinical-policy/older-people/frailty/efi/. (accessed on 22 June 2021).
- Sinclair, A. (September 2019) Key Learning Points: Diabetes in Older People with Frailty. Available online: https://www.guidelinesinpractice.co.uk/diabetes/key-learning-points-diabetes-in-older-people-with-frailty/454910.article (accessed on 22 June 2021).
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.; Ceda, G.P.; Ticinesi, A.; De Vita, F.; Gelmini, G.; Costantino, C.; Meschi, T.; Kressig, R.W.; Cesari, M.; Fabi, M.; et al. Instrumental and Non-Instrumental Evaluation of 4-Meter Walking Speed in Older Individuals. PLoS ONE 2016, 11, e0153583. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: A systematic review and meta- analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Nicolini-Panisson, R.D.; Donadio, M. Timed “Up & Go” test in children and adolescents. Rev. Paul. Pediatr. 2013, 31, 377–383. [Google Scholar] [CrossRef]
- Yates, T.; Zaccardi, F.; Dhalwani, N.; Davies, M.; Bakrania, K.; Celis-Morales, C.A.; Gill, J.M.R.; Franks, P.; Khunti, K. Association of walking pace and handgrip strength with all-cause, cardiovascular, and cancer mortality: A UK Biobank observational study. Eur. Heart J. 2017, 38, 3232–3240. [Google Scholar] [CrossRef]
- Timmins, I.R.; Zaccardi, F.; Nelson, C.P.; Franks, P.W.; Yates, T.; Dudbridge, F. Genome-wide association study of self-reported walking pace suggests beneficial effects of brisk walking on health and survival. Commun. Biol. 2020, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Argyridou, S.; Zaccardi, F.; Davies, M.; Khunti, K.; Yates, T. Walking pace improves all-cause and cardiovascular mortality risk prediction: A UK Biobank prognostic study. Eur. J. Prev. Cardiol. 2020, 27, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Zaccardi, F.; Davies, M.; Khunti, K.; Yates, T. Comparative Relevance of Physical Fitness and Adiposity on Life Expectancy: A UK Biobank Observational Study. Mayo Clin. Proc. 2019, 94, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R. Using Pedometers to Increase Physical Activity and Improve Health: A systematic review. J. Am. Med. Assoc. 2007, 298, 2296–2304. [Google Scholar] [CrossRef]
- Van Kan, G.A.; Rolland, Y.; Bergman, H.; Morley, J.E.; Kritchevsky, S.B.; Vellas, B. The I.A.N.A. task force on frailty assessment of older people in clinical practice. J. Nutr. Health Aging 2008, 12, 29–37. [Google Scholar] [CrossRef]
- Morley, J.E.; Vellas, B.; Van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.; Doehner, W.; Evans, J.; et al. Frailty Consensus: A Call to Action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Lins, L.; Carvalho, F. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Balestroni, G.; Bertolotti, G. EuroQol-5D (EQ-5D): An instrument for measuring quality of life. Monaldi Arch. Chest Dis. 2012, 78, 155–159. [Google Scholar] [CrossRef]
- Grandy, S.; Fox, K.M.; Bazata, D.D.; for the SHIELD Study Group. Health-related quality of life association with weight change in type 2 diabetes mellitus: Perception vs. reality. Int. J. Clin. Pract. 2013, 67, 455–461. [Google Scholar] [CrossRef]
- Traina, S.B.; Colwell, H.H.; Crosby, R.D.; Mathias, S.D. Pragmatic measurement of health satisfaction in people with type 2 diabetes mellitus using the Current Health Satisfaction Questionnaire. Patient Relat. Outcome Meas. 2015, 6, 103–115. [Google Scholar] [CrossRef] [Green Version]
- Kolotkin, R.L.; Williams, V.S.L.; Ervin, C.M.; Williams, N.; Meincke, H.H.; Qin, S.; Smith, L.V.H.; Fehnel, S. Validation of a new measure of quality of life in obesity trials: Impact of Weight on Quality of Life-Lite Clinical Trials Version. Clin. Obes. 2019, 9, e12310. [Google Scholar] [CrossRef]
- Villareal, D.T.; Chode, S.; Parimi, N.; Sinacore, D.R.; Hilton, T.; Armamento-Villareal, R.; Napoli, N.; Qualls, C.; Shah, K. Weight Loss, Exercise, or Both and Physical Function in Obese Older Adults. N. Engl. J. Med. 2011, 364, 1218–1229. [Google Scholar] [CrossRef] [Green Version]
- Gregg, E.W.; Beckles, G.L.; Williamson, D.F.; Leveille, S.G.; Langlois, J.A.; Engelgau, M.M.; Narayan, K.M. Diabetes and physical disability among older U.S. adults. Diabetes Care 2000, 23, 1272–1277. [Google Scholar] [CrossRef] [Green Version]
- Enright, P.L. The six-minute walk test. Respir Care 2003, 48, 783–785. [Google Scholar]
- Costa, I.P.; Corso, S.D.; Borghi-Silva, A.; Peixoto, F.; Stirbulov, R.; Arena, R.; Cahalin, L.P.; Sampaio, L.M.M. Reliability of the Shuttle Walk Test with Controlled Incremental Velocity in Patients with Difficult-to-Control Asthma. J. Cardiopulm. Rehabil. Prev. 2018, 38, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Betik, A.C.; Hepple, R.T. Determinants ofVO2 maxdecline with aging: An integrated perspective. Appl. Physiol. Nutr. Metab. 2008, 33, 130–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitchett, M.A. Predictability of VO2 max from submaximal cycle ergometer and bench stepping tests. Br. J. Sports Med. 1985, 19, 85–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laucis, N.C.; Hays, R.D.; Bhattacharyya, T. Scoring the SF-36 in Orthopaedics: A Brief Guide. J. Bone Jt. Surg. 2015, 97, 1628–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, E.; Backholer, K.; Gearon, E.; Harding, J.; Freak-Poli, R.; Stevenson, C.; Peeters, A. Diabetes and risk of physical disability in adults: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2013, 1, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Malmstrom, T.K.; Rodríguez-Mañas, L.; Sinclair, A.J. Frailty, Sarcopenia and Diabetes. J. Am. Med. Dir. Assoc. 2014, 15, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, e323. [Google Scholar] [CrossRef]
- Hubbard, R.E.; Andrew, M.K.; Fallah, N.; Rockwood, K. Comparison of the prognostic importance of diagnosed diabetes, co-morbidity and frailty in older people. Diabet. Med. 2010, 27, 603–606. [Google Scholar] [CrossRef] [PubMed]
- Ryerson, B.; Tierney, E.F.; Thompson, T.J.; Engelgau, M.M.; Wang, J.; Gregg, E.W.; Geiss, L.S. Excess physical limitations among adults with diabetes in the U.S. population, 1997–1999. Diabetes Care 2003, 26, 206–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalyani, R.R.; Saudek, C.D.; Brancati, F.L.; Selvin, E. Association of Diabetes, Comorbidities, and A1C With Functional Disability in Older Adults: Results from the National Health and Nutrition Examination Survey (NHANES), 1999–2006. Diabetes Care 2010, 33, 1055–1060. [Google Scholar] [CrossRef] [Green Version]
- Godino, J.G.; Appel, L.J.; Gross, A.L.; Schrack, J.A.; Parrinello, C.M.; Kalyani, R.R.; Windham, B.G.; Pankow, J.S.; Kritchevsky, S.B.; Bandeen-Roche, K.; et al. Diabetes, hyperglycemia, and the burden of functional disability among older adults in a community-based study. J. Diabetes 2017, 9, 76–84. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Saldaña, J.; Morley, J.E.; Reynoso, M.T.; Medina, C.A.; Salazar, P.; Cruz, E.; Torres, A.L.N. Diabetes Mellitus in a Subgroup of Older Mexicans: Prevalence, Association with Cardiovascular Risk Factors, Functional and Cognitive Impairment, and Mortality. J. Am. Geriatr. Soc. 2002, 50, 111–116. [Google Scholar] [CrossRef]
- Mickute, M.; Henson, J.; Rowlands, A.V.; Sargeant, J.A.; Webb, D.; Hall, A.P.; Edwardson, C.L.; Baldry, E.L.; Brady, E.M.; Khunti, K.; et al. Device-measured physical activity and its association with physical function in adults with type 2 diabetes mellitus. Diabet. Med. 2021, 38. [Google Scholar] [CrossRef]
- Chhetri, J.K.; Zheng, Z.; Xu, X.; Ma, C.; Chan, P. The prevalence and incidence of frailty in Pre-diabetic and diabetic community-dwelling older population: Results from Beijing longitudinal study of aging II (BLSA-II). BMC Geriatr. 2017, 17, 47. [Google Scholar] [CrossRef] [Green Version]
- Gregg, E.W.; Mangione, C.M.; Cauley, J.A.; Thompson, T.J.; Schwartz, A.V.; Ensrud, K.E.; Nevitt, M.C.; for the Study of Osteoporotic Fractures Research Group. Diabetes and Incidence of Functional Disability in Older Women. Diabetes Care 2002, 25, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Sayer, A.A.; Dennison, E.M.; Syddall, H.E.; Gilbody, H.J.; Phillips, D.I.; Cooper, C. Type 2 diabetes, muscle strength, and impaired physical function: The tip of the iceberg? Diabetes Care 2005, 28, 2541–2542. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.Y.; Gan, P.; How, C.H. Approach to frailty in the elderly in primary care and the community. Singap. Med. J. 2018, 59, 240–245. [Google Scholar] [CrossRef] [Green Version]
- Radner, H.; Smolen, J.S.; Aletaha, D. Comorbidity affects all domains of physical function and quality of life in patients with rheumatoid arthritis. Rheumatology 2010, 50, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Chao, C.-T.; COhort of GEriatric Nephrology in NTUH (COGENT) Study Group; Wang, J.; Chien, K.-L. Both pre-frailty and frailty increase healthcare utilization and adverse health outcomes in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 130. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.; Stevenson, C.; Backholer, K.; Woodward, M.; Shaw, J.E.; Peeters, A. Predicting the risk of physical disability in old age using modifiable mid-life risk factors. J. Epidemiol. Community Health 2014, 69, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, L.; Shaw, J.E.; Wong, E.; Harding, J.L.; Peeters, A.; Magliano, D.J. Burden of diabetes in Australia: Life expectancy and disability-free life expectancy in adults with diabetes. Diabetologia 2016, 59, 1437–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turnbull, P.J.; Sinclair, A.J. Evaluation of nutritional status and its relationship with functional status in older citizens with diabetes mellitus using the mini nutritional assessment (MNA) tool—A preliminary investigation. J. Nutr. Health Aging 2002, 6, 185–189. [Google Scholar]
- Van Sloten, T.T.; Savelberg, H.H.; Duimel-Peeters, I.G.; Meijer, K.; Henry, R.M.; Stehouwer, C.D.; Schaper, N.C. Peripheral neuropathy, decreased muscle strength and obesity are strongly associated with walking in persons with type 2 diabetes without manifest mobility limitations. Diabetes Res. Clin. Pract. 2011, 91, 32–39. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Garin, N.; Olaya, B.; Ayuso-Mateos, J.L.; Miret, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Leonardi, M.; et al. Diabetes mellitus and its association with central obesity and disability among older adults: A global perspective. Exp. Gerontol. 2015, 64, 70–77. [Google Scholar] [CrossRef]
- Atkinson, H.H.; Rosano, C.; Simonsick, E.M.; Williamson, J.D.; Davis, C.; Ambrosius, W.T.; Rapp, S.R.; Cesari, M.; Newman, A.B.; Harris, T.B.; et al. Cognitive Function, Gait Speed Decline, and Comorbidities: The Health, Aging and Body Composition Study. J. Gerontol. Ser. A 2007, 62, 844–850. [Google Scholar] [CrossRef] [Green Version]
- Kirkman, M.S.; Briscoe, V.J.; Clark, N.; Florez, H.; Haas, L.B.; Halter, J.B.; Huang, E.S.; Korytkowski, M.T.; Munshi, M.N.; Odegard, P.S.; et al. Diabetes in Older Adults. Diabetes Care 2012, 35, 2650–2664. [Google Scholar] [CrossRef] [Green Version]
- Cacciatore, F.; Testa, G.; Galizia, G.; Della-Morte, D.; Mazzella, F.; Langellotto, A.; Pirozzi, G.; Ferro, G.; Gargiulo, G.; Ferrara, N.; et al. Clinical frailty and long-term mortality in elderly subjects with diabetes. Acta Diabetol. 2013, 50, 251–260. [Google Scholar] [CrossRef]
- Gadsby, R.; Hope, S.; Hambling, C.A.C. Frailty, older people and type 2 diabetes. J. Diabetes Nurs. 2017, 21, 138–142. [Google Scholar]
- Helmersson, J.; Vessby, B.; Larsson, A.; Basu, S. Association of Type 2 Diabetes with Cyclooxygenase-Mediated Inflammation and Oxidative Stress in an Elderly Population. Circulation 2004, 109, 1729–1734. [Google Scholar] [CrossRef]
- Szewieczek, J.; Bieniek, J.; Wilczyński, K. Fried frailty phenotype assessment components as applied to geriatric inpatients. Clin. Interv. Aging 2016, 11, 453–459. [Google Scholar] [CrossRef] [Green Version]
- Huang, E.S.; Zhang, Q.; Gandra, N.; Chin, M.H.; Meltzer, D.O. The Effect of Comorbid Illness and Functional Status on the Expected Benefits of Intensive Glucose Control in Older Patients with Type 2 Diabetes: A Decision Analysis. Ann. Intern. Med. 2008, 149, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Koye, D.N.; Shaw, J.E.; Magliano, D. Diabetes and disability in older Australians: The Australian Diabetes, Obesity and Lifestyle (AusDiab) study. Diabetes Res. Clin. Pr. 2017, 126, 60–67. [Google Scholar] [CrossRef]
- Maggi, S.; Noale, M.; Gallina, P.; Marzari, C.; Bianchi, D.; Limongi, F.; Crepaldi, G.; For the ILSA Group. Physical disability among older Italians with diabetes. The ILSA Study. Diabetologia 2004, 47, 1957–1962. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, A.J.; Conroy, S.; Bayer, A.J. Impact of Diabetes on Physical Function in Older People. Diabetes Care 2007, 31, 233–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesari, M.; Landi, F.; Vellas, B.; Bernabei, R.; Marzetti, E. Sarcopenia and Physical Frailty: Two Sides of the Same Coin. Front. Aging Neurosci. 2014, 6, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.; de Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Accelerated Loss of Skeletal Muscle Strength in Older Adults with Type 2 Diabetess: The health, aging, and body composition study. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolland, Y.; Czerwinski, S.; Van Kan, G.A.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Onder, G.; Bernabei, R. Sarcopenia and Diabetes: Two Sides of the Same Coin. J. Am. Med. Dir. Assoc. 2013, 14, 540–541. [Google Scholar] [CrossRef] [PubMed]
- McNeil, C.J.; Doherty, T.J.; Stashuk, D.W.; Rice, C.L. Motor unit number estimates in the tibialis anterior muscle of young, old, and very old men. Muscle Nerve 2005, 31, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Giresi, P.G.; Stevenson, E.J.; Theilhaber, J.; Koncarevic, A.; Parkington, J.; Fielding, R.A.; Kandarian, S.C. Identification of a molecular signature of sarcopenia. Physiol. Genom. 2005, 21, 253–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cree-Green, M.; Newcomer, B.R.; Katsanos, C.S.; Sheffield-Moore, M.; Chinkes, D.; Aarsland, A.; Urban, R.; Wolfe, R.R. Intramuscular and Liver Triglycerides Are Increased in the Elderly. J. Clin. Endocrinol. Metab. 2004, 89, 3864–3871. [Google Scholar] [CrossRef]
- Sinclair, A.J.; Abdelhafiz, A.H.; Rodríguez-Mañas, L. Frailty and sarcopenia-newly emerging and high impact complications of diabetes. J. Diabetes Its Complicat. 2017, 31, 1465–1473. [Google Scholar] [CrossRef]
- Sinclair, A.J.; Rodríguez-Mañas, L. Diabetes and Frailty: Two Converging Conditions? Can. J. Diabetes 2016, 40, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Park, S.W.; Goodpaster, B.H.; Lee, J.S.; Kuller, L.H.; Boudreau, R.; de Rekeneire, N.; Harris, T.B.; Kritchevsky, S.; Tylavsky, F.A.; Nevitt, M.; et al. Excessive Loss of Skeletal Muscle Mass in Older Adults with Type 2 Diabetes. Diabetes Care 2009, 32, 1993–1997. [Google Scholar] [CrossRef] [Green Version]
- Kalyani, R.R.; Corriere, M.; Ferrucci, L. Age-related and disease-related muscle loss: The effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2014, 2, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Reusch, J.E.B.; Bridenstine, M.; Regensteiner, J.G. Type 2 diabetes mellitus and exercise impairment. Rev. Endocr. Metab. Disord. 2013, 14, 77–86. [Google Scholar] [CrossRef]
- Kelley, D.E.; He, J.; Menshikova, E.V.; Ritov, V.B. Dysfunction of Mitochondria in Human Skeletal Muscle in Type 2 Diabetes. Diabetes 2002, 51, 2944–2950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, K.F.; Befroy, D.; Dufour, S.; Dziura, J.; Ariyan, C.; Rothman, D.L.; DiPietro, L.; Cline, G.W.; Shulman, G.I. Mitochondrial Dysfunction in the Elderly: Possible Role in Insulin Resistance. Science 2003, 300, 1140–1142. [Google Scholar] [CrossRef] [Green Version]
- Lanza, I.R.; Short, D.K.; Short, K.R.; Raghavakaimal, S.; Basu, R.; Joyner, M.J.; McConnell, J.P.; Nair, K.S. Endurance Exercise as a Countermeasure for Aging. Diabetes 2008, 57, 2933–2942. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Vellas, B.; Hsu, F.-C.; Newman, A.B.; Doss, H.; King, A.C.; Manini, T.M.; Church, T.; Gill, T.; Miller, M.E.; et al. A Physical Activity Intervention to Treat the Frailty Syndrome in Older Persons—Results From the LIFE-P Study. J. Gerontol. Ser. A 2015, 70, 216–222. [Google Scholar] [CrossRef]
- De Vries, N.M.; Staal, J.B.; van der Wees, P.J.; Adang, E.M.M.; Akkermans, R.; Rikkert, M.G.M.O.; der Sanden, M.W.G.N.-V. Patient-centred physical therapy is (cost-) effective in increasing physical activity and reducing frailty in older adults with mobility problems: A randomized controlled trial with 6 months follow-up. J. Cachex-Sarcopenia Muscle 2015, 7, 422–435. [Google Scholar] [CrossRef]
- Theou, O.; Stathokostas, L.; Roland, K.P.; Jakobi, J.M.; Patterson, C.; Vandervoort, A.A.; Jones, G.R. The Effectiveness of Exercise Interventions for the Management of Frailty: A Systematic Review. J. Aging Res. 2011, 2011, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovanec, N.; Sawant, A.; Overend, T.J.; Petrella, R.J.; Vandervoort, A.A. Resistance Training and Older Adults with Type 2 Diabetes Mellitus: Strength of the Evidence. J. Aging Res. 2012, 2012, 284635. [Google Scholar] [CrossRef]
- Fielding, R.A. The role of progressive resistance training and nutrition in the preservation of lean body mass in the elderly. J. Am. Coll. Nutr. 1995, 14, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Daniels, R.; Van Rossum, E.; De Witte, L.; Kempen, G.I.J.M.; Heuvel, W.V.D. Interventions to prevent disability in frail community-dwelling elderly: A systematic review. BMC Health Serv. Res. 2008, 8, 278. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Kim, D.; Kim, C. Resistance Training for Glycemic Control, Muscular Strength, and Lean Body Mass in Old Type 2 Diabetic Patients: A Meta-Analysis. Diabetes Ther. 2017, 8, 459–473. [Google Scholar] [CrossRef] [Green Version]
- Brandon, L.J.; Gaasch, D.A.; Boyette, L.W.; Lloyd, A.M. Effects of Long-Term Resistive Training on Mobility and Strength in Older Adults with Diabetes. J. Gerontol. Ser. A 2003, 58, M740–M745. [Google Scholar] [CrossRef]
- Ibañez, J.; Izquierdo, M.; Argüelles, I.; Forga, L.; Larrión, J.L.; García-Unciti, M.; Idoate, F.; Gorostiaga, E.M. Twice-Weekly Progressive Resistance Training Decreases Abdominal Fat and Improves Insulin Sensitivity in Older Men with Type 2 Diabetes. Diabetes Care 2005, 28, 662–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mourier, A.; Gautier, J.-F.; De Kerviler, E.; Bigard, A.X.; Villette, J.-M.; Garnier, J.-P.; Duvallet, A.; Guezennec, C.Y.; Cathelineau, G. Mobilization of Visceral Adipose Tissue Related to the Improvement in Insulin Sensitivity in Response to Physical Training in NIDDM: Effects of branched-chain amino acid supplements. Diabetes Care 1997, 20, 385–391. [Google Scholar] [CrossRef]
- Eriksson, J.; Taimela, S.; Parviainen, S.; Peltonen, J.; Kujala, U. Resistance Training in the Treatment of Non-Insulin-Dependent Diabetes Mellitus. Int. J. Sports Med. 1997, 18, 242–246. [Google Scholar] [CrossRef]
- Miller, W.J.; Sherman, W.M.; Ivy, J.L. Effect of strength training on glucose tolerance and post-glucose insulin response. Med. Sci. Sports Exerc. 1984, 16, 539–543. [Google Scholar] [CrossRef]
- Poehlman, E.T.; Dvorak, R.V.; DeNino, W.F.; Brochu, M.; Ades, P.A. Effects of Resistance Training and Endurance Training on Insulin Sensitivity in Nonobese, Young Women: A Controlled Randomized Trial1. J. Clin. Endocrinol. Metab. 2000, 85, 2463–2468. [Google Scholar] [CrossRef] [Green Version]
- Gaster, M.; Vach, W.; Beck-Nielsen, H.; Schrøder, H.D. GLUT4 expression at the plasma membrane is related to fibre volume in human skeletal muscle fibres. APMIS 2002, 110, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Mañas, L.; Laosa, O.; Vellas, B.; Paolisso, G.; Topinkova, E.; Oliva-Moreno, J.; Bourdel-Marchasson, I.; Izquierdo, M.; Hood, K.; Zeyfang, A.; et al. Effectiveness of a multimodal intervention in functionally impaired older people with type 2 diabetes mellitus. J. Cachex-Sarcopenia Muscle 2019, 10, 721–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rejeski, W.J.; Ip, E.H.; Bertoni, A.; Bray, G.A.; Evans, G.; Gregg, E.; Zhang, Q. Lifestyle Change and Mobility in Obese Adults with Type 2 Diabetes. N. Engl. J. Med. 2012, 366, 1209–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buman, M.P.; Hekler, E.B.; Haskell, W.L.; Pruitt, L.; Conway, T.L.; Cain, K.L.; Sallis, J.F.; Saelens, B.E.; Frank, L.D.; King, A.C. Objective Light-Intensity Physical Activity Associations with Rated Health in Older Adults. Am. J. Epidemiol. 2010, 172, 1155–1165. [Google Scholar] [CrossRef] [Green Version]
- Izquierdo, M.; Vivifrail Investigators Group; Rodriguez-Mañas, L.; Sinclair, A.J. What is new in exercise regimes for frail older people—How does the Erasmus Vivifrail Project take us forward? J. Nutr. Health Aging 2016, 20, 736–737. [Google Scholar] [CrossRef] [PubMed]
- Henderson, R.M.; Miller, M.E.; Fielding, R.A.; Gill, T.; Glynn, N.W.; Guralnik, J.M.; King, A.; Newman, A.B.; Manini, T.M.; Marsh, A.P.; et al. Maintenance of Physical Function 1 Year After Exercise Intervention in At-Risk Older Adults: Follow-up from the LIFE Study. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2018, 73, 688–694. [Google Scholar] [CrossRef]
- Morley, J.E.; Von Haehling, S.; Anker, S.D.; Vellas, B. From sarcopenia to frailty: A road less traveled. J. Cachex- Sarcopenia Muscle 2014, 5, 5–8. [Google Scholar] [CrossRef]
- Sinclair, A.; Morley, J.E.; Rodriguez-Mañas, L.; Paolisso, G.; Bayer, T.; Zeyfang, A.; Bourdel-Marchasson, I.; Vischer, U.; Woo, J.; Chapman, I.; et al. Diabetes Mellitus in Older People: Position Statement on behalf of the International Association of Gerontology and Geriatrics (IAGG), the European Diabetes Working Party for Older People (EDWPOP), and the International Task Force of Experts in Diabetes. J. Am. Med. Dir. Assoc. 2012, 13, 497–502. [Google Scholar] [CrossRef]
- Reaney, M.; Elash, C.A.; Litcher-Kelly, L. Patient Reported Outcomes (PROs) used in recent Phase 3 trials for Type 2 Diabetes: A review of concepts assessed by these PROs and factors to consider when choosing a PRO for future trials. Diabetes Res. Clin. Pract. 2016, 116, 54–67. [Google Scholar] [CrossRef]
- Tentolouris, A.; Vlachakis, P.; Tzeravini, E.; Eleftheriadou, I.; Tentolouris, N. SGLT2 Inhibitors: A Review of Their Antidiabetic and Cardioprotective Effects. Int. J. Environ. Res. Public Health 2019, 16, 2965. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-S.; Jun, H.-S. Anti-Inflammatory Effects of GLP-1-Based Therapies beyond Glucose Control. Mediat. Inflamm. 2016, 2016, 3094642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yates, T.; Henson, J.; Sargeant, J.; King, J.A.; Ahmad, E.; Zaccardi, F.; Davies, M.J. Exercise, Pharmaceutical Therapies and Type 2 Diabetes: Looking beyond Glycemic Control to Whole Body Health and Function. Transl. Med. Exerc. Prescr. 2021, 33–42. [Google Scholar] [CrossRef]
- Boulé, N.G.; Robert, C.; Bell, G.J.; Johnson, S.T.; Bell, R.C.; Lewanczuk, R.Z.; Gabr, R.Q.; Brocks, D.R. Metformin and Exercise in Type 2 Diabetes. Diabetes Care 2011, 34, 1469–1474. [Google Scholar] [CrossRef] [Green Version]
- Braun, B.; Eze, P.; Stephens, B.R.; Hagobian, T.A.; Sharoff, C.G.; Chipkin, S.; Goldstein, B. Impact of metformin on peak aerobic capacity. Appl. Physiol. Nutr. Metab. 2008, 33, 61–67. [Google Scholar] [CrossRef]
- Linden, M.A.; Fletcher, J.A.; Morris, E.M.; Meers, G.M.; Kearney, M.L.; Crissey, J.M.; Laughlin, M.H.; Booth, F.W.; Sowers, J.R.; Ibdah, J.A.; et al. Combining metformin and aerobic exercise training in the treatment of type 2 diabetes and NAFLD in OLETF rats. Am. J. Physiol. Metab. 2014, 306, E300–E310. [Google Scholar] [CrossRef] [Green Version]
- Malin, S.K.; Nightingale, J.; Choi, S.-E.; Chipkin, S.R.; Braun, B. Metformin modifies the exercise training effects on risk factors for cardiovascular disease in impaired glucose tolerant adults. Obesity 2013, 21, 93–100. [Google Scholar] [CrossRef]
- Myette-Côté, E.; Terada, T.; Boulé, N.G. The Effect of Exercise with or Without Metformin on Glucose Profiles in Type 2 Diabetes: A Pilot Study. Can. J. Diabetes 2016, 40, 173–177. [Google Scholar] [CrossRef]
- Sharoff, C.G.; Hagobian, T.A.; Malin, S.; Chipkin, S.; Yu, H.; Hirshman, M.F.; Goodyear, L.J.; Braun, B. Combining short-term metformin treatment and one bout of exercise does not increase insulin action in insulin-resistant individuals. Am. J. Physiol. Metab. 2010, 298, E815–E823. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.A.; Grimm, N.C.; Wilburn, J.R.; Schoenberg, H.M.; Trikha, S.R.; Luckasen, G.J.; Biela, L.M.; Melby, C.L.; Bell, C.; Wilburn, J.R. Influence of Sodium Glucose Cotransporter 2 Inhibition on Physiological Adaptation to Endurance Exercise Training. J. Clin. Endocrinol. Metab. 2019, 104, 1953–1966. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.; Janus, C.; Lundgren, J.R.; Juhl, C.R.; Blond, M.B.; Stallknecht, B.; Holst, J.J.; Madsbad, S.; Torekov, S.S. 686-P: Exercise Alone and in Combination with Liraglutide Exert Clinically Relevant Improvements in Cardiorespiratory Fitness during 1-Year Weight Loss Maintenance: The S-LITE Randomized Trial. Diabetes 2020, 69, 686. [Google Scholar] [CrossRef]
Figure 1.
Examples of physical function assessments used in clinical research.

Figure 2.
Mechanisms underpinning impaired physical function in T2D.


{kind=link}
{kind=link}
Table 1.
Percentage limitation in physical activity by age groups- diabetes vs. non diabetes.
| Age Groups | Percentage with Some Physical Limitation | |
|---|---|---|
| With Diabetes | Without Diabetes | |
| 18–44 | 46 | 18 |
| 45–64 | 63 | 35 |
| 65–74 | 74 | 53 |
| ≥75 | 85 | 70 |
Adopted from Reference [48].
Table 2.
Disability in various physical functional tasks.
| Physical Function Category | Percentage (%) | 95% Confidence Interval (95% CI) |
|---|---|---|
| General physical activities | 73.6 | 70.2–76.9 |
| Lower extremity mobility | 52.2 | 48.5–55.9 |
| IADL | 43.6 | 40.1–47.2 |
| ADL | 37.2 | 33.1–41.3 |
| Leisure and social activities | 33.8 | 30.8–36.9 |
Adapted from Reference [49]. (ADL, Activities of Daily Living; IADL, Instrumental Activities of Daily Living; CI, Confidence Interval).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ahmad, E.; Sargeant, J.A.; Yates, T.; Webb, D.R.; Davies, M.J. Type 2 Diabetes and Impaired Physical Function: A Growing Problem. Diabetology 2022, 3, 30-45. https://doi.org/10.3390/diabetology3010003
AMA Style
Ahmad E, Sargeant JA, Yates T, Webb DR, Davies MJ. Type 2 Diabetes and Impaired Physical Function: A Growing Problem. Diabetology. 2022; 3(1):30-45. https://doi.org/10.3390/diabetology3010003
Chicago/Turabian StyleAhmad, Ehtasham, Jack A. Sargeant, Tom Yates, David R. Webb, and Melanie J. Davies. 2022. "Type 2 Diabetes and Impaired Physical Function: A Growing Problem" Diabetology 3, no. 1: 30-45. https://doi.org/10.3390/diabetology3010003