
Photocrosslinking of Adventitial Collagen in the Porcine Abdominal Aorta: A Preliminary Approach to a Strategy for Prevention of Aneurysmal Rupture


1
Queensland Eye Institute, South Brisbane, QLD 4101, Australia
2
School of Chemistry & Physics, Queensland University of Technology, Brisbane, QLD 4001, Australia
3
Australian Institute of Bioengineering & Nanotechnology, University of Queensland, St. Lucia, QLD 4072, Australia
4
Faculty of Medicine, University of Queensland, Herston, QLD 4006, Australia
5
School of Molecular Science, University of Western Australia, Crawley, WA 6009, Australia
6
Faculty of Medicine, George E. Palade University of Medicine, Pharmacy, Science & Technology, Târgu Mureş 540139, Romania
*
Author to whom correspondence should be addressed.
Designs 2022, 6(1), 5; https://doi.org/10.3390/designs6010005
Submission received: 25 November 2021
/
Revised: 11 January 2022
/
Accepted: 12 January 2022
/
Published: 12 January 2022
(This article belongs to the Section Bioengineering Design)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:This study was aimed at generating data for designing a potential method to prevent the rupture of the abdominal aortic aneurysm (AAA). We found that the mechanical strength and stiffness of blood vessel walls was enhanced by the crosslinking of adventitial collagen through a photochemical process promoted by ultraviolet-A (UV-A) radiation. The experiments were carried out on samples isolated from 25 normal porcine aortas. The adventitial layer was separated from the other layers and exposed to UV radiation of 365-nm wavelength, in the presence of a riboflavin compound as the photosensitizer. Mechanical testing of 30 specimens, prior to and after exposure, indicated an increase in both strength (ultimate stress) and stiffness (Young’s modulus) of the adventitial specimens following irradiation. The crosslinking process also led to an enhanced resistance to experimental collagenolysis, as determined on six specimens. At this phase of conceptual design, we suggest that by applying this method to an aneurysmal dilated wall region, the stabilization of tunica adventitia may delay or prevent the rupture of the aneurysm and, with further investigation and refinement, can become a therapeutic strategy for arresting the progression of AAA.
1. Introduction
In spite of an impressive volume of experimental research, extensive published literature on its pathophysiology and therapeutic strategies, and a significant number of related clinical trials, the abdominal aortic aneurysm (AAA) remains a pathological condition associated with high morbidity and mortality rates. An aortic aneurysm is commonly described as the localized degenerative weakening of the aortic wall, leading to the formation of an irreversibly progressing dilatation (bulge) that exceeds the diameter of the normal aorta by at least 1.5 times, i.e., to ≥3 cm in diameter. The wall’s regional spontaneous rupture at the level of the bulge can trigger massive bleeding into the retroperitoneal or abdominal cavities, with fatal consequences for the patients, unless an effective medical intervention is immediately available.
Currently, repair surgery is the only treatment for AAAs, applicable preventively for aneurysms larger than 5 to 5.5 cm in diameter, and to ruptured aneurysms in emergency settings. There are two types of the procedure, the traditional open surgical repair (OSR) and the newer endovascular aneurysm repair (EVAR) surgery, which both are associated with satisfactory perioperative mortality rates, although some postoperative complications and the occasional need for re-interventions are still present [1,2,3,4,5]. Intensive research has been dedicated lately to a more in-depth understanding of the pathogenesis of AAA, and to develop non-surgical treatment approaches, such as pharmacologic or cellular therapies [3,4,6,7,8], and is anticipated that novel strategies for treating AAA will emerge in the near future.
There is no therapeutic option available now for the patients having small aneurysms (<5 cm in women, <5.5 cm in men) and for those deemed unfit for surgical intervention. As there is no benefit of early repair surgery of small AAAs, the current guidelines for these patients recommend [4] surveillance with size monitoring through ultrasonographic imaging techniques to be carried out repeatedly at various intervals that are selected in accordance with the size attained by the aneurysm. However, screening as such will not reduce aneurysmal degeneration, and it has been associated with certain detrimental outcomes [9,10]. It is becoming evident that an ideal therapeutic strategy for such cases, which would preferably be applicable to larger AAAs too, should be a procedure that is able to arrest the aneurysmal progression, ideally with minimal surgical invasiveness.
Based strictly on mechanical considerations, an AAA can alternatively be defined as the failure of the aortic wall material to withstand the dynamic forces associated with relentless exposure to the pulsatile flow of arterial blood. Ultimately, the aneurysmal rupture is a mechanical event.
The two structural proteins that determine mechanical characteristics of blood vessel walls are elastin and collagen, and their contribution to mechanical performance is evaluated in terms of elasticity, stiffness, and strength. In the mammalian connective tissues, collagen is approximately 1000 times stiffer and 6000 times stronger than elastin, while elastin is 10 times more extensible than collagen [11]. It is therefore commonly assumed [11,12] that the elastin fibres provide high extensibility (strain) and efficient elastic-strain storage properties (resilience, compliance), which are the source of stretchiness and recoil characteristics. The strength and stiffness (rigidity) are provided by the collagen fibres.
We report here the development of a method aimed at mechanically reinforcing the aortic adventitial collagen through its chemical crosslinking induced by ultraviolet-A (UV-A) radiation (wavelength 365 nm) in the presence of riboflavin 5′-phosphate monosodium salt (as a photosensitizer). In principle, mechanical reinforcement can prevent a wall’s rupture. It is also expected that the crosslinking process will stabilize the collagen against enzymatic degradation. The procedure was inspired by the photochemical crosslinking of the eye’s corneal collagen [13,14,15,16], currently a safe primary treatment for keratoconus, an ophthalmic pathological condition of unknown mechanism that leads to severe visual impairment. While the collagen crosslinking cannot cure the condition, it is able to arrest its progression, and it has become a routine procedure in ophthalmology. In an attempt to extend the method to treating other segments of the eye, we have previously demonstrated [17,18] in ex-vivo animal (ovine) tissue that the UV-A-induced crosslinking of tarsal collagen led to increased mechanical strength and stiffening of the tissue and could become a suitable treatment for floppy eyelid syndrome and other cases of eyelid laxity. Further research on rodent tarsal tissue [19] and cadaveric human tarsal tissue [20,21] has confirmed the radiation-induced stiffening effect.
Exposure to electromagnetic radiation has been investigated previously as a therapy for certain vascular conditions. Photodynamic therapy (PDT) with visible and near-infrared laser radiation (wavelengths, 500–850 nm) in the presence of photosensitizers such as methylene blue, indocyanine green (ICG) or phthalocyanines has been proposed for inhibiting intimal hyperplasia leading to restenosis [22,23,24]; it was suggested that PDT can generate collagen crosslinks that may induce resistance to enzymes and fibroplasia [25]. Laser soldering with 830-nm radiation in the presence of ICG enhanced the strength of arterial segments in rats after exposure to elastase [26]. The only PDT experiments to date (660-nm wavelength, methylene blue as photosensitizer) involving an aneurysm animal model have revealed the lack of wall mechanical strengthening in the aneurysmal aorta [27]. The effect of irradiation with the UV-B region of ultraviolet radiation (280–320 nm, no photosensitizer) has been investigated in the mouse angiotensin-II model [28], suggesting a decreased incidence of aneurysmal rupture, which was explained by the expansion of regulatory T cells leading to reduction of an inflammatory process. Low-level laser therapy (LLLT) was another method investigated for arresting the progression of AAA. This is based on the so-called “photobiomodulation”, a controversial treatment applied mostly to blood or skin using laser-delivered visible (600–650 nm) and near-infrared (over 700 nm) radiation in the absence of photosensitizers. Applying 780-nm radiation at low irradiance in animal tissue or angiotensin-II models, researchers at The Hebrew University in Jerusalem have noticed a reinforcement of the aortic wall potentially leading to prevention of aneurysmal rupture, which was explained by enhancement of the biosynthetic activity of smooth muscle cells resulting in increased production of elastin and collagen, and by attenuating the deterioration of mitochondrial membrane potential [29,30,31,32,33].
The present study is different in that it makes use of the irradiation with UV-A light for the in situ strengthening of adventitial collagen as a potential method to attenuate the aneurysmal growth by preventing or delaying the rupture of a weakened aortic wall, thus essentially arresting the progression of the aneurysm. Our proposed process is purposely and entirely based on the photochemical crosslinking of collagen.
2. Materials and Methods
2.1. Materials
Riboflavin 5′-phosphate monosodium salt (henceforth, RF) was supplied by Cayman Chemicals (Ann Arbor, MI, USA), and its solution in saline (0.1% w/v) was used as a photosensitizer. Collagenase type I (255 U/mg), and neutral buffered formalin (10% w/w, ~3.5–4% w/w formaldehyde) were purchased from Thermo Fisher Scientific (Rockford, IL, USA). All other chemicals and reagents were supplied by MilliporeSigma (St Louis, MO, USA) and local suppliers (Australian Biostain P/L, ProSciTech, POCD; all in Australia). High-purity water (Milli-Q or equivalent) was used in all experiments.
The porcine aortas were procured from Highchester Meats Pty. Ltd. (Gleneagle, QLD, Australia), an abattoir unit that operates under the Australian Code of Practice of Animal Welfare Standards for Livestock Processing Establishments, having been harvested from cadavers of 20-week old pigs (of the variety “beacon pigs”) on the day of collection. It is to be mentioned that the animals had been sacrificed for commercial purposes, and the aortas would have been discarded if not used in this study.
2.2. Sample Preparation
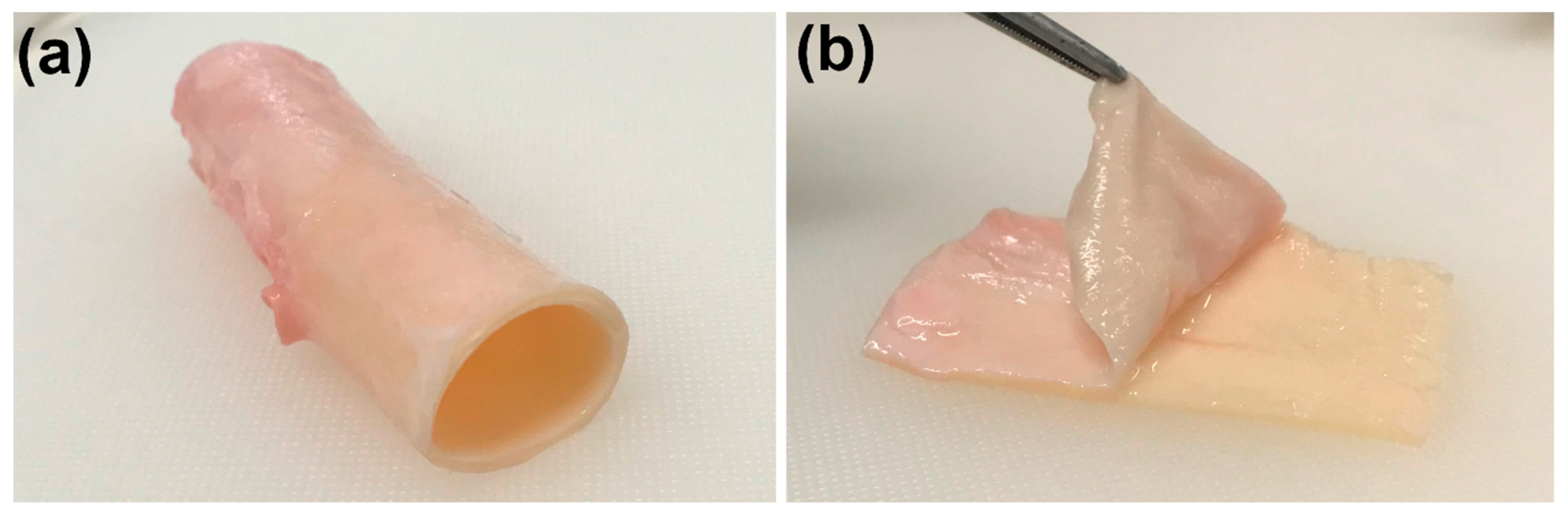
Twenty-five aortas from the abdominal region were used in this study. For the mechanical testing, the samples were maintained fresh. For the other evaluations, the aortas were stored in a freezer and thawed when necessary. The aorta specimens were processed by first removing the extraneous adipose and loose connective tissue debris from the external surface using surgical scissors. One cut was then performed along the longitudinal axis of each aortic tube, in order to obtain flat rectangular sheets. A surgical scalpel was used to make an initial cornerwise-interstitial incision between adventitia and media layers, and the adventitial layer was carefully dissected and peeled off by hand. Following additional removal of medial tissue residues adhering to the internal surface, the specimens were stored for no longer than 30 min in saline at room temperature prior to irradiation.
2.3. Treatment with Formalin
The samples were treated with neutral buffered formalin (10%) for 20 h at room temperature for two purposes: (a) For fixation prior to histological processing, the treated samples were then washed and stored in phosphate buffered saline (PBS) at 4 °C; (b) For the collagenolytic degradation experiments and also for mechanical testing, each treated sample was washed in 100 mL water for 24 h, with gentle shaking and 5 water exchanges throughout, and then used in experiments.
2.4. Histology
The formalin-fixed specimens, both full-thickness aortic wall and the isolated layers, were placed in plastic tissue processing cassettes and processed for a duration of 9 h in the Tissue-Tek® VIP® 6 Tissue Processor (Sakura Finetek, Torrance, CA, USA). The processed samples were embedded in paraffin with the region of interest facing down. Sections (4-μm thick) were cut with a Leica RM2234 microtome (Leica Biosystems, Nussloch, Germany) and collected onto labelled SuperFrost Plus slides (Menzel-Gläser, Braunschweig, Germany). The slides were stained with haematoxylin and eosin (H&E) in a Tissue-Tek Prisma® autostainer (Sakura Finetek, Torrance, CA, USA), and coverslipped on the attached automated coverslipper. The slides were then imaged using an Olympus VS120 Slide Scanner (Olympus, Sydney, Australia) using the Olympus OlyVIA™ software. Except for the initial fixation in formalin, the histological processing and imaging were carried out at the Histology & Microscopy Core Facility of the Translational Research Institute, Brisbane, Australia.
2.5. Irradiation Procedure
Rectangular strips of the adventitia of about 7 cm × 3 cm were soaked in RF solution for 30 min at room temperature. Each specimen was then irradiated with UV-A radiation of 365-nm wavelength produced by the UV Curing System OmniCure 1500 (Excelitas Technologies Corp., Waltham, MA, USA). The irradiance at the exposure site was monitored with the radiometer Dymax ACCU-CAL 50 (Dymax Corp., Torrington, CT, USA). The required irradiance was achieved by adjusting the distance between the radiation source and target. Each side of the specimen was exposed to an irradiance of 45 mW/cm2 for 10 min.
2.6. Mechanical Testing
An Instron Materials Testing System Model #5943 (Instron, Norwood, MA, USA), equipped with a 50-N load cell, was used to measure uniaxially the tensile properties of isolated adventitia specimens (n = 30), prior to and after irradiation. Before measurements, each specimen was soaked in phosphate-buffered saline (PBS) for at least 1 h at room temperature. Strips (1 cm × 3 cm) were cut, and their thickness and width were measured with a digital calliper (Digimax Global Inc., Toronto, ON, Canada). Thirty measurements for each set of samples (non-irradiated and irradiated) were carried out along the longitudinal direction at a set gauge distance of 16 mm and a speed of 10 mm/min. The values for Young’s moduli were computed from the recorded stress-strain plots in the linear region. All mechanical tests were performed by only one researcher.
2.7. Experimental Collagenolysis
Non-irradiated and irradiated adventitial samples, 6 specimens of each, were rinsed 3 times in 100 mL water for 1 h with gentle shaking, and then each placed in a 2-mL Eppendorf tube, and lyophilized in a freeze drier/vacuum concentrator (Alpha 1–2 LDplus, Martin Chris GmbH, Osterode, Germany). Washed formalin-treated treated specimens (n = 6) were processed in the same manner. The weight of the resulting solid material was recorded in all cases. A solution containing 20 U/mL (~0.08 mg/mL) collagenase was prepared in Tris buffer (0.05 M, pH 7.4) containing calcium chloride (10 mM) and sodium azide (0.02%), and 1 mL of this solution was added to each tube. The tubes were mounted on an orbital shaker and shaken at 240 rpm for 48 h at 37 °C and then centrifuged at 10,000 rpm for 10 min at 4 °C. The solid deposits in each tube were rinsed 3 times in water (1 mL) with gentle shaking for 10 min, followed by centrifugation after each rinsing. After lyophilization, the measured weight values of the deposits were used to estimate the percentage of weight loss due to enzymatic degradation.
2.8. Statistical Processing
When applicable, the results were expressed as mean values ± standard error of the mean. For their statistical comparisons, the GraphPad® Prism software (Version 6.0) was used to carry out the unpaired 2-tailed t-test (mechanical evaluation, 30 samples), or the unpaired Mann–Whitney 2-tailed nonparametric test (enzymatic degradation, 6 samples).
3. Results
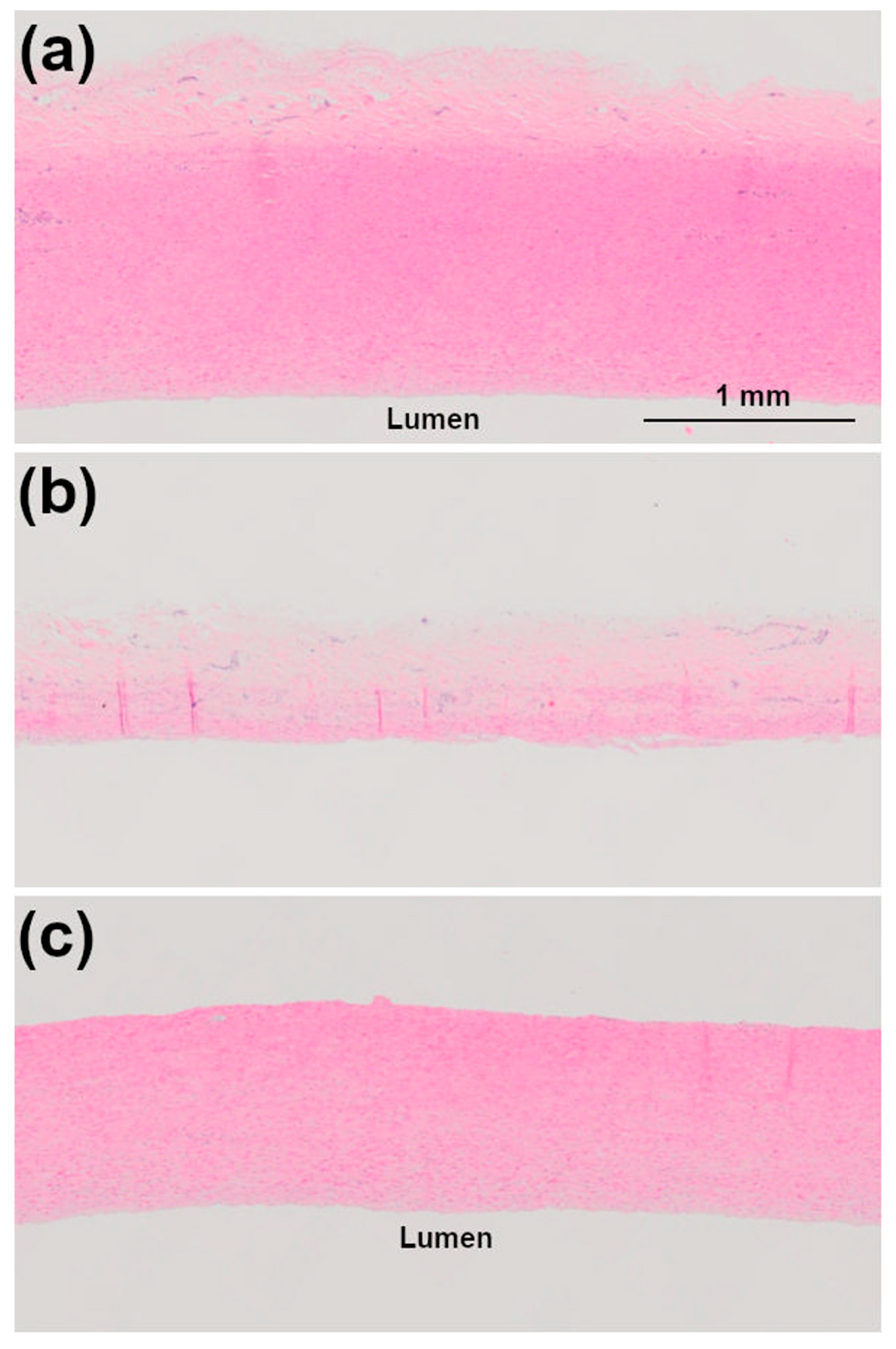
Tunica media was easy to distinguish and could be conveniently separated from the adventitia (Figure 1), as noted also by other investigators [34]. Gross histological analysis (Figure 2) indicated that the isolated adventitia was completely separated from the media, however, residual patches of medial tissue could still be noticed on the medial side of it.
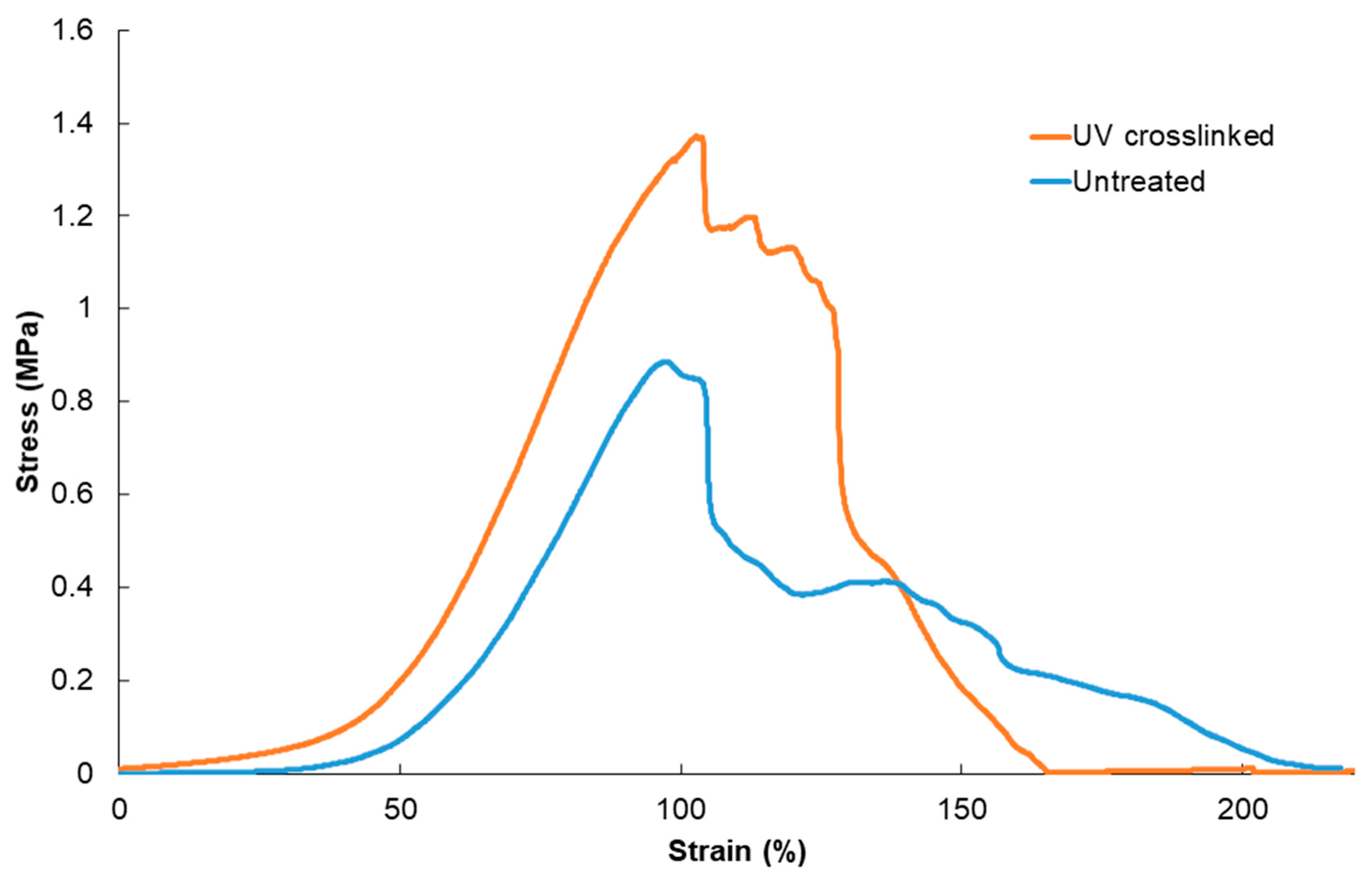
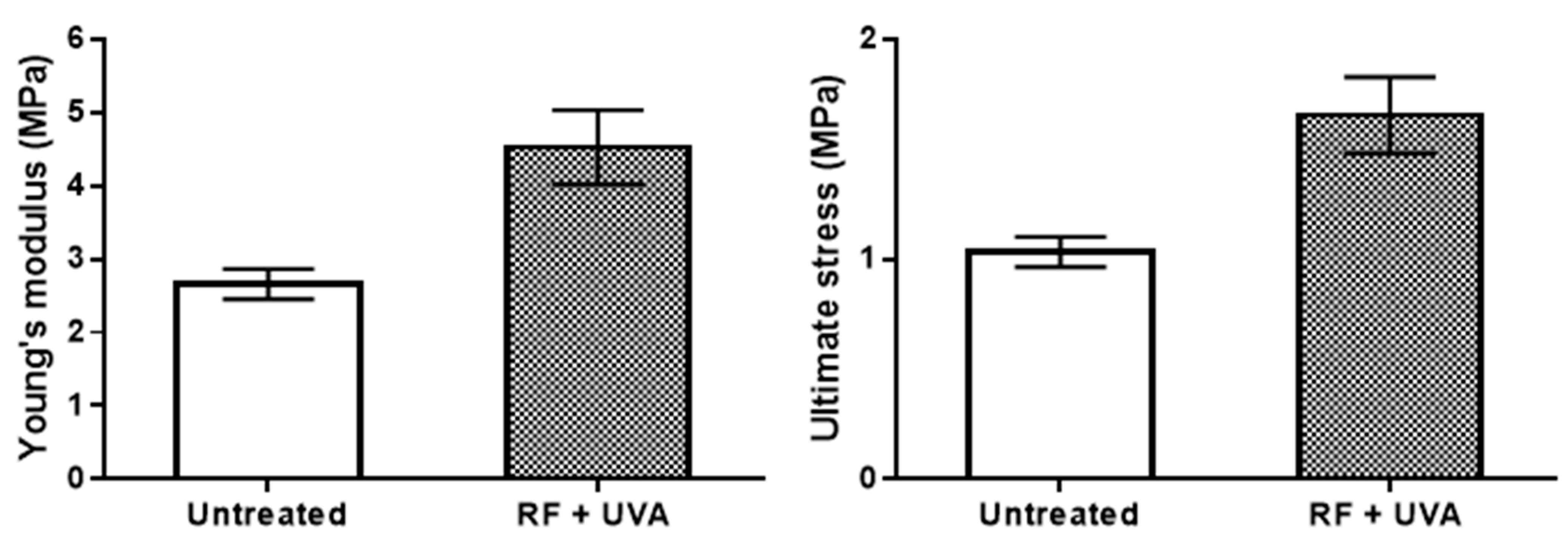
A typical individual stress-strain plot recorded by the mechanical tester indicates unequivocally an irradiation-induced strengthening effect (Figure 3). The tensile measurements involving a larger number of samples (n = 30) showed a difference between irradiated and non-irradiated adventitial specimens concerning both stiffening (Young’s modulus) and strengthening (ultimate stress, i.e., the maximum load at the time of rupture) (Figure 4). This suggests that a structural reinforcing due to the crosslinking of adventitial collagen can delay the mechanical failure of the irradiated wall, as compared to a non-irradiated one. Noticeably, the values measured in this study for the tensile strength are in the range reported for the human aortic wall [35]. In a separate mechanical assessment, the ultimate tensile stress of adventitial samples treated with formaldehyde (as a formalin solution) was found to be ~2.6 times higher than that of untreated specimens, but only ~1.6 higher than that of UV-irradiated specimens. In spite of the more extensive effect of chemical crosslinking, crosslinking with formaldehyde is fundamentally different from photocrosslinking, regarding both chemistry and reaction conditions.
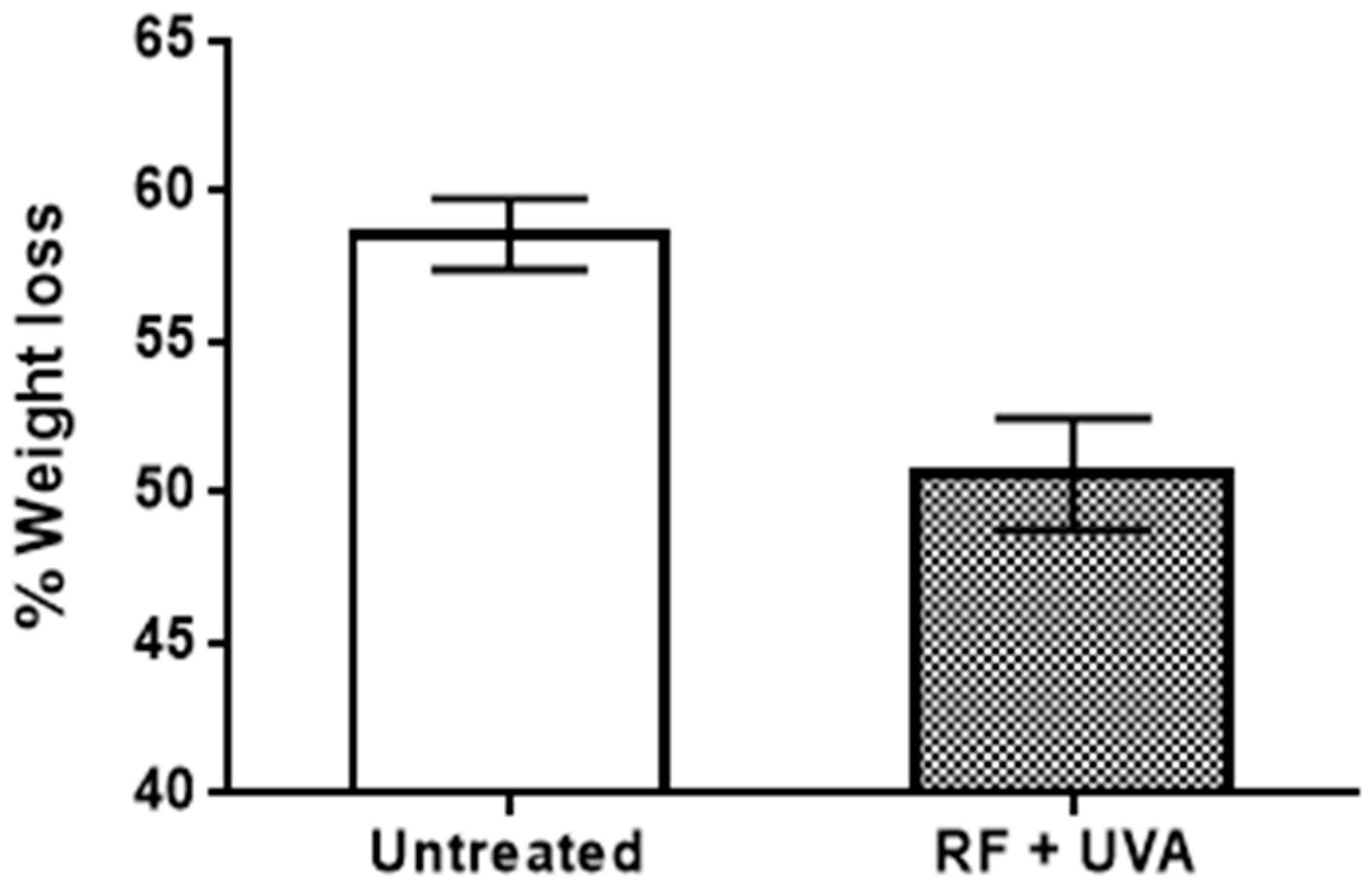
The effect of the crosslinking process was further assessed by measuring quantitatively the weight loss caused by the in-vitro collagenolytic degradation in the untreated samples, and in the UV-irradiated samples. As seen in Figure 5, the exposure to UV-A radiation was able to stabilize the adventitial tissue against enzymatic degradation. In a separate experiment, chemical crosslinking with formaldehyde resulted also in the enhancement of proteolytic resistance, the weight loss being ~3 times less than that recorded for UV-irradiated samples. This can be regarded as an indication that a crosslinking process is a common denominator underlying the effects observed both upon exposure to UV-A radiation and after formaldehyde treatment.
4. Discussion
According to the current knowledge of the pathophysiology of AAA [1,2,3,4,5], the dominant characteristics of the disease include inflammatory cell infiltration, degradation and impaired remodelling of the extracellular matrix (ECM), and depletion of medial smooth muscle cells (SMCs). Associated events or contributing factors may include neovascularization of the tunica media, endothelial dysfunction, atherosclerosis, thrombus formation, wall calcification, oxidative stress, altered blood flow dynamics, genetic predisposition, environmental agents, and patient-related factors.
Of significant relevance to our study is the issue of degradation and alteration of elastin and collagen as the ECM components in media and adventitia induced by elevated proteolytic activity of enzymes, such as elastases, matrix metalloproteinases (MMPs), cysteine and serine proteases, and cathepsins. Based on seminal publications [1,36,37,38,39,40,41,42,43,44], the following simplified scenario can be conceptualized. The normal aortic tunica media is composed of concentric layers of SMCs, an intricate network of elastic fine fibres and fenestrated lamellae interspersed with collagen fibrils and a proteoglycan matrix, and bundles of collagen. In the healthy wall, media is a major contributor to its mechanical properties. The normal tunica adventitia consists of collagen fibrils interspersed with elastic lamellae, blood vessels, nerves, and certain cell populations. Following the massive loss of medial elastin and a partial loss of collagen due to aneurysmal degeneration, collagen from medial outer regions and adventitia is recruited in order to take over the load generated by the pulsatile blood flow. Because this process becomes gradually inefficient, an enhanced turnover of fibrillary “repair” collagen commences as a compensatory deposition of remodelled collagen, leading to the reinforcement and thickening of the adventitia. At this stage, the wall’s collagen content would indicate at any given time the net effect of ongoing turnover vs. ongoing degradation. While both elastolytic dissipation of elastin (reflected in a significant drop of the elastin-to-collagen ratio) and depletion of SMCs advance steadily within the medial layers, the degradation of adventitial collagen is largely balanced by its repair. A point in time comes, however, when the capacity of collagen for neosynthesis and remodelling is overwhelmed by the degradation processes, and the altered collagen fibres no longer can contribute efficiently to maintaining the strength of the aneurysmal wall, leading to its sudden and catastrophic rupture. We may therefore conclude that the mechanical failure of the aneurysmal wall is the result of the mechanical failure of adventitial collagen. Indeed, it has been asserted [41,45] that the loss of elastin in the media does not actually affect the wall integrity, and the mechanical support for the aneurysmal wall is confined to the adventitia.
The prominent role played by the adventitial collagen was fundamental to the development of our proposed strategy. To enhance the strength of remaining collagen prior to mechanical failure appears as a rational approach for delaying or preventing the rupture. Additional premises may substantiate the validity of such strategy and justify the choice of adventitia as a target, as itemized in the paragraphs below.
- (a)
- The level of crosslinking of the collagen in aneurysmal wall tissues was shown to be elevated [46,47,48], which suggests that the remodelled repair collagen itself is in a crosslinked state. This natural, enzyme-controlled crosslinking process of the remodelled adventitial collagen could be aimed at providing the mechanical reinforcement needed to withstand the excessive pressure load induced by the loss of elastin and SMCs in the media. In fact, the terminal failure of the aneurysmal wall is believed to be a consequence of changes in the microarchitecture of the collagen network [49], rather than being caused by an ineffective natural crosslinking.
- (b)
- In diabetic experimental animals and post-mortem diabetic human tissue, it was found that arterial stiffness and remodelling were related to the non-enzymatic crosslinking of collagen through a natural process based on the advanced glycation end products (AGEs). The level of glycation-induced crosslinking of collagen was significantly higher in the aortic collagen when compared to other regions of the body, and it was associated with the stiffening of the vessel’s wall [50,51,52,53,54,55,56]. At the same time, a statistically significant negative association between diabetes and AAA has been demonstrated in a number of studies [57,58,59,60]. A legitimate conclusion would be that the stiffening of the aortic wall in diabetic patients due to crosslinking of collagen is one of the reasons for a delayed rupture of their aneurysms. This is another supporting premise for our proposed strategy.
- (c)
- An additional justification for selecting adventitia as the primary target in the method we report here comes from vascular surgery. Eversion endarterectomy consists of the debridement and removal of the intima and the media (or part of it) in order to treat lesions (e.g., atheromatous plaques or blockages) inside arteries and reduce their recurrence. Although it was mainly adventitia left onto the lumen side, the extant studies [61,62,63,64] have shown that no “false” aneurysms were formed postoperatively, and the strength level of endarterectomized walls was similar to that of full walls or even enhanced. The observed increased collagen content after endarterectomy suggests a deposition process of repair collagen. These findings may confirm an important contributory role of the adventitia to the mechanical performance of the aortic wall. While the knowledge of AAA is being continually re-evaluated and enriched, the prominent role of adventitial collagen in the evolution of the disease appears to be a safe presupposition underlying our investigation.
Similarly to the lysyl oxidase (LOX)-promoted physiologic crosslinking of collagen that occurs naturally in the vertebrate organisms, the purposeful extraneous crosslinking of collagen by chemical or physical means, either in vitro or ex vivo [17,18,19,20,21,65,66,67,68,69,70,71,72,73,74,75,76], also can stabilize its network by enhancing the mechanical characteristics and the resistance to proteolytic degradation. It is a process frequently used in tissue engineering and regenerative medicine research. Photochemical crosslinking implies the use of electromagnetic radiation of a specific wavelength to induce crosslinking reactions in collagen after its irradiation in situ, and it can be applied for therapeutic purposes. The presence of either a photosensitizer or a photoinitiator is essential in the crosslinking system: upon being excited energetically by radiation, it triggers a chain of free-radical-based reactions resulting in the formation of covalent crosslinks within the collagen molecular matrix. A commonly employed radiation is the region A of the ultraviolet (UV-A) radiation with wavelengths between 320 and 400 nm, although the more energetic regions UV-B and UV-C have been also experimented with in some applications. As mentioned earlier, the only approved therapeutic procedure based on UV-A-induced crosslinking belongs to ophthalmology and refers to a treatment for keratoconus [13,14,15,16]. Our present study shows that the UV-A-induced crosslinking of adventitial collagen promoted by a suitable photosensitizer can lead both to an increase in strength and stiffness and to a reduction of the collagenolytic degradative effects.
The fate of elastin, the other essential protein in the vessel wall structure, following the UV irradiation of the adventitia is also relevant. Elastin is inherently a highly crosslinked biopolymer as a result of natural elastogenesis involving the LOX-mediated crosslinking of the precursor tropoelastin [77,78,79]. In fact, the lack of an elastin’s turnover and its half-life of over 70 years in vertebrates are attributed to remarkably stable natural crosslinks [79]. Although the formation of further crosslinks in elastin is unlikely, UV-A radiation may still cause scission of the existing natural crosslinks (mainly desmosine and isodesmosine structures) [80,81]. However, at the time of applying the irradiation to an aneurysmal wall, elastin would be significantly depleted in both media and adventitia. Besides, there is little likelihood that the low irradiance and short time of exposure to UV-A radiation will cause additional damage to the elastin macromolecules.
Aortic elastin has been a strategic target in the development of a non-surgical, pharmacological approach to arresting the progression of aneurysmal degeneration. The proposed treatment was based on the remarkable biological properties of natural polyphenols, in particular of pentagalloylglucose (PGG) [82,83], and it was initiated by investigators at Clemson University, SC, USA [70,84,85,86,87]. It is known that the hydrolyzable vegetable tannins display a specific tendency to associate non-covalently with proteins [88,89,90], in a process that is particularly effective in proline-rich proteins such as collagen and elastin. It is assumed, albeit not entirely correctly, that the process is a “crosslinking” reaction accomplished through complexation, rather than through covalent linkages. It was reported that aortic elastin can be stabilized against elastolysis by treatment with tannins such as tannic acid [84], PGG [70,83,85,86,87], and epigallocatechin gallate [91], presumably due to blockage by complexation of the elastin’s hydrophobic sites that are the target for enzymatic attack. More recently, research has been focused on establishing strategies for delivering PGG to the aorta [92,93,94], and on assessing its therapeutic potential in animal AAA models [95,96,97,98,99,100].
In our experiments, the enhancement of mechanical characteristics of the adventitial layer was associated with a satisfactory level of statistical significance (p < 0.002). This was in spite of (a) potential effects of absorption, scattering, reflections and refraction of radiation caused by both chemistry and morphology of the adventitial tissue components; and (b) the fact that not all chemical reactions triggered by the irradiation are necessarily conducive to crosslinking of collagen. In our early experiments that involved irradiation of the whole vessel wall, mechanical enhancement was hardly noticeable upon evaluation in the mechanical tester (results not included), an indication that the structural complexity of peri-adventitial tissues and medial layers could have contributed to the decay of radiation preventing its penetration farther than adventitia. The results for enzymatic degradation had also an acceptable level of statistical significance in our present study (p < 0.005). However, the weight loss after experimental collagenolysis is still substantial in the irradiated samples. As the conditions of the experiments are likely different from the in vivo conditions, a comparison with what actually happens in aneurysmal adventitia is not conclusive based on these preliminary data.
Our results were compared in this study to those provided by treating the adventitial specimens with formaldehyde, a known effective crosslinking agent for proteins [66]. It reacts with the ε-amino groups of lysine and hydroxylysine residues, leading to imine intermediates that form crosslinks with tyrosine, asparagine and glutamine residues. Being a more efficient process than the photochemically induced crosslinking, the chemical crosslinking with formaldehyde resulted in stronger effects on both mechanical strength and proteolytic resistance of the adventitial tissue. Due to the toxicity of formaldehyde and the most crosslinking agents in use, and because of the long reaction times required, the chemical treatment is not an option for in situ applications directed at the blood vessel walls. Here, we have used this comparison only to confirm that the crosslinking of collagen can indeed generate such effects on the mechanical properties and the resistance to enzymatic degradation.
A beneficial outcome in the long term of the proposed strategy requires further developmental work, such as finding a type of radiation that might be a more effective penetrant than UV-A radiation. We are currently investigating the crosslinking effect of the visible radiation (400–700 nm) on adventitial tissue in the presence of low-cytotoxicity photosensitizers including RF (maximum absorption at ~447 nm), rose bengal (~546 nm), azure B (~650 nm), or methylene blue (~668 nm). Another important issue is the method of radiation delivery with minimally invasive surgical intervention. The laparoscopic fibre optics technology can offer a valid option for delivering the radiation beam to the patient’s aortic wall, preceded by laparoscopic administration of the photosensitizer solution onto the targeted surface. An alternative worth considering would be delivery by lasers that emit in the visible region, such as helium-neon lasers (543.5 nm and other wavelengths), argon ion lasers (488 nm, 514.5 nm), krypton ion lasers (530.9 nm, 647.1 nm), ruby laser (694.3 nm), Nd:YAG laser (frequency-doubled, 532 nm), and many others. Considering the large surface area of the vessel wall that must be covered by irradiation, the delivery technique through lasers will have to incorporate the raster scanning of the beam across the target area.
5. Conclusions
The exposure of aortic tunica adventitia to UV-A radiation increases its mechanical strength and stiffness, based on a photochemical crosslinking process involving the tissue collagenous components. Application of this technique to an aneurysmal dilated region of the abdominal aorta should be considered as a potential strategy aimed at delaying or preventing the rupture of the aneurysmal bulge. With further developmental designing and refinements, the method can make a genuine contribution to the AAA therapeutic armamentarium.
Author Contributions
T.V.C. conceptualized the project, and both authors contributed to the design of the study. T.V.C. coordinated the research, carried out the literature search, and wrote the manuscript. S.S. performed the experimental work and prepared the graphic material for publication. Both authors contributed to the analysis and interpretation of results. S.S. revised the final draft of the manuscript and approved its version for submission. Both authors agree to be personally accountable for their contributions. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public or commercial sector.
Institutional Review Board Statement
Not applicable. No animal or human experimentation or trials were associated with this study.
Informed Consent Statement
Not applicable.
Data Availability Statement
Authors can confirm that all relevant data are included in this published article.
Acknowledgments
The authors acknowledge the ongoing support from the Queensland Eye Institute Foundation (Brisbane, Australia) through the Viertel’s Vision Program. This organisation was not involved in the design and conclusions of the study, interpretation of results, or in the process of writing the manuscript. The authors thank Justin Large and Andy Wu (Translational Research Institute, Brisbane, Australia) for the histologic processing. The input of Tai M. Smith on the initial stages of the project, and creative discussions with Idriss Blakey (University of Queensland, Brisbane, Australia) are gratefully acknowledged. One of the authors (TVC) dedicates this work to the memory of Ioan Crăciun (Romania), a victim of aneurysm.
Conflicts of Interest
The authors have no conflict of interest or any financial interests to declare that are relevant to the content of this article.
References
- Thompson, R.W.; Geraghty, P.J.; Lee, J.K. Abdominal aortic aneurysms: Basic mechanisms and clinical implications. Curr. Probl. Surg. 2002, 39, 110–230. [Google Scholar] [CrossRef]
- Chaikof, E.L.; Brewster, D.C.; Dalman, R.L.; Makaroun, M.S.; Illig, K.A.; Sicard, G.A.; Timaran, C.H.; Upchurch, G.R., Jr.; Veith, F.J. The care of patients with an abdominal aortic aneurysm: The Society for Vascular Surgery practice guidelines. J. Vasc. Surg. 2009, 50, S2–S49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuivaniemi, H.; Ryer, E.J.; Elmore, J.R.; Tromp, G. Understanding the pathogenesis of abdominal aortic aneurysms. Expert Rev. Cardiovasc. Ther. 2015, 13, 975–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golledge, J. Abdominal aortic aneurysm: Update on pathogenesis and medical treatments. Nat. Rev. Cardiol. 2019, 16, 225–242. [Google Scholar] [CrossRef] [PubMed]
- Kent, K.C. Abdominal aortic aneurysms. N. Engl. J. Med. 2014, 371, 2101–2108. [Google Scholar] [CrossRef]
- Nordon, I.M. Abdominal aortic aneurysms: Fundamental concepts. In Oxford Textbook of Vascular Surgery; Thompson, M., Ed.; Oxford University Press: Oxford, UK, 2016; pp. 469–484. [Google Scholar]
- Golledge, J.; Norman, P.E.; Murphy, M.P.; Dalman, R.L. Challenges and opportunities in limiting abdominal aortic aneurysm growth. J. Vasc. Surg. 2017, 65, 225–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, F.M.; Daugherty, A.; Lu, H.S. Updates of recent aortic aneurysm research. Arterioscler. Thromb. Vasc. Biol. 2019, 39, e83–e90. [Google Scholar] [CrossRef]
- Guirguis-Blake, J.M.; Beil, T.L.; Senger, C.A.; Coppola, E.L. Primary care screening for abdominal aortic aneurysm: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2019, 322, 2219–2238. [Google Scholar] [CrossRef] [Green Version]
- Bains, P.; Oliffe, J.L.; Mackay, M.H.; Kelly, M.T. Screening older adult men for abdominal aortic aneurysm: A scoping review. Am. J. Mens. Health 2021, 15, 15579883211001204. [Google Scholar] [CrossRef]
- Gosline, J.; Lillie, M.; Carrington, E.; Guerette, P.; Ortlepp, C.; Savage, K. Elastic proteins: Biological and mechanical properties. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2002, 357, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Montes, G.S. Structural biology of the fibres of the collagenous and elastic systems. Cell Biol. Int. 1996, 20, 15–27. [Google Scholar] [CrossRef]
- Sorkin, N.; Varssano, D. Corneal collagen crosslinking: A systematic review. Ophthalmologica 2014, 332, 10–27. [Google Scholar] [CrossRef]
- Randleman, J.B.; Khandelwal, S.S.; Hafezi, F. Corneal cross-linking. Surv. Ophthalmol. 2015, 60, 509–523. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.; Lim, E.W.L. A review of corneal collagen cross-linking—current trends in practice applications. Open Ophthalmol. J. 2018, 12 (Suppl. 1), 181–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feizi, S.; Karimian, F.; Esfandiari, H. Corneal crosslinking for the treatment of infectious keratitis: A review. Expert Rev. Ophthalmol. 2021, 16, 287–295. [Google Scholar] [CrossRef]
- Smith, T.M.; Suzuki, S.; Cronin, B.G.; Haghighatpanah, M.; Petcu, E.B.; Philippa, C.J.; Chirila, T.V. Photochemically induced crosslinking of tarsal collagen as a treatment for eyelid laxity: Assessing potentiality in animal tissue. Ophthal. Plast. Reconstr. Surg. 2018, 34, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.M.; Suzuki, S.; Sabat, N.; Rayner, C.L.; Harkin, D.G.; Chirila, T.V. Further investigations on the crosslinking of tarsal collagen as a treatment for eyelid laxity: Optimizing the procedure in animal tissue. Ophthal. Plast. Reconstr. Surg. 2019, 35, 600–603. [Google Scholar] [CrossRef] [PubMed]
- Akella, S.S.; Liu, J.; Miao, Y.; Chuck, R.S.; Barmettler, A.; Zhang, C. Collagen structural changes in rat tarsus after crosslinking. Transl. Vis. Sci. Technol. 2021, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Ugradar, S.; Le, A.; Lesgart, M.; Goldberg, R.A.; Rootman, D.; Demer, J.L. Biomechanical and morphologic effects of collagen cross-linking in human tarsus. Transl. Vis. Sci. Technol. 2019, 8, 25. [Google Scholar] [CrossRef] [Green Version]
- Ugradar, S.; Karlin, J.; Le, A.; Park, J.; Goldberg, R.A. Photochemical collagen cross-linking reverses elastase-induced mechanical degradation of upper eyelid tarsus. Ophthal. Plast. Reconstr. Surg. 2020, 36, 562–565. [Google Scholar] [CrossRef]
- LaMuraglia, G.M.; ChandraSekar, N.R.; Flotte, T.J.; Abbott, W.M.; Michaud, N.; Hasan, T. Photodynamic therapy inhibition of experimental intimal hyperplasia: Acute and chronic effects. J. Vasc. Surg. 1994, 19, 321–331. [Google Scholar] [CrossRef] [Green Version]
- LaMuraglia, G.M.; Schiereck, J.; Heckenkamp, J.; Nigri, G.; Waterman, P.; Leszczynski, D.; Kossodo, S. Photodynamic therapy induces apoptosis in intimal hyperplastic arteries. Am. J. Pathol. 2000, 157, 867–875. [Google Scholar] [CrossRef] [Green Version]
- Overhaus, M.; Heckenkamp, J.; Kossodo, S.; Leszczynski, D.; LaMuraglia, G.M. Photodynamic therapy generates a matrix barrier to invasive vascular cell migration. Circ. Res. 2000, 86, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Waterman, P.R.; Overhaus, M.; Heckenkamp, J.; Nigri, G.R.; Fungaloi, P.F.C.; Landis, M.E.; Kossodo, S.C.; LaMuraglia, G.M. Mechanisms of reduced human vascular cell migration after photodynamic therapy. Photochem. Photobiol. 2002, 75, 46–50. [Google Scholar] [CrossRef]
- Oskoui, P.; Stadler, I.; Lanzafame, R.J. A preliminary study of laser tissue soldering as arterial wall reinforcement in an acute experimental aneurysm model. Lasers Surg. Med. 2003, 32, 346–348. [Google Scholar] [CrossRef] [PubMed]
- Heckenkamp, J.; Luebke, T.; Theis, T.; Schumacher, L.; Gawenda, M.; Thul, R.; Fries, J.W.U.; Brunkwall, J. Effects of vascular photodynamic therapy in a newly adapted experimental rat aortic aneurysm model. Interact. CardioVasc. Thorac. Surg. 2012, 15, 69–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, T.; Sasaki, N.; Yamashita, T.; Mizoguchi, T.; Emoto, T.; Amin, Z.A.; Yodoi, K.; Matsumoto, T.; Kasahara, K.; Yoshida, N.; et al. Ultraviolet B exposure inhibits angiotensin II–induced abdominal aortic aneurysm formation in mice by expanding CD4+Foxp3+ regulatory T cells. J. Am. Heart Assoc. 2017, 6, e007024. [Google Scholar] [CrossRef] [PubMed]
- Gavish, L.; Rubinstein, C.; Bulut, A.; Berlatzky, Y.; Beeri, R.; Gilon, D.; Gavish, L.; Harlev, M.; Reissman, P.; Gertz, S.D. Low-level laser irradiation inhibits abdominal aortic aneurysm progression in apolipoprotein E-deficient mice. Cardiovasc. Res. 2009, 83, 785–792. [Google Scholar] [CrossRef] [Green Version]
- Gavish, L.; Rubinstein, C.; Berlatzky, Y.; Gavish, L.Y.; Beeri, R.; Gilon, D.; Bulut, A.; Harlev, M.; Reissman, P.; Gertz, S.D. Low level laser arrests abdominal aortic aneurysm by collagen matrix reinforcement in apolipoprotein E-deficient mice. Lasers Surg. Med. 2012, 44, 664–674. [Google Scholar] [CrossRef]
- Gavish, L.; Beeri, R.; Gilon, D.; Rubinstein, C.; Berlatzky, Y.; Bulut, A.; Reissman, P.; Gavish, L.Y.; Gertz, S.D. Arrest of progression of pre-induced abdominal aortic aneurysm in apolipoprotein E-deficient mice by low level laser phototherapy. Lasers Surg. Med. 2014, 46, 781–790. [Google Scholar] [CrossRef]
- Gavish, L.; Beeri, R.; Gilon, D.; Rubinstein, C.; Berlatzky, Y.; Gavish, L.Y.; Bulut, A.; Harlev, M.; Reissman, P.; Gertz, S.D. Inadequate reinforcement of transmedial disruptions at branch points subtends aortic aneurysm formation in apolipoprotein-E-deficient mice. Cardiovasc. Pathol. 2014, 23, 152–159. [Google Scholar] [CrossRef]
- Gavish, L.; Gilon, D.; Beeri, R.; Zuckerman, A.; Nachman, D.; Gertz, S.D. Photobiomodulation and estrogen stabilize mitochondrial membrane potential in angiotensin-II challenged porcine aortic muscle cells. J. Biophotonics 2021, 14, e202000329. [Google Scholar] [CrossRef] [PubMed]
- Sommer, G.; Gasser, T.C.; Regitnig, P.; Auer, M.; Holzapfel, G.A. Dissection properties of the human aortic media: An experimental study. J. Biomech. Eng. 2008, 130, 021007. [Google Scholar] [CrossRef]
- Tavares Monteiro, J.A.; da Silva, E.S.; Raghavan, M.L.; Puech-Leão, P.; de Lourdes Higuchi, M.; Pinhata Otoch, J. Histologic, histochemical, and biomechanical properties of fragments isolated from the anterior wall of abdominal aortic aneurysms. J. Vasc. Surg. 2014, 59, 1393–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrin, P.B.; Baker, W.H.; Gley, W.C. Elastolytic and collagenolytic studies of arteries. Arch. Surg. 1984, 119, 405–409. [Google Scholar] [CrossRef]
- Dobrin, P.B.; Schwartz, T.H.; Baker, W.H. Mechanisms of arterial and aneurysmal tortuosity. Surgery 1988, 104, 568–571. [Google Scholar]
- Dobrin, P.B. Pathophysiology and pathogenesis of aortic aneurysms. Current concepts. Surg. Clin. N. Am. 1989, 69, 687–703. [Google Scholar] [CrossRef]
- White, J.V.; Haas, K.; Phillips, S.; Comerota, A.J. Adventitial elastolysis is a primary event in aneurysm formation. J. Vasc. Surg. 1993, 17, 371–381. [Google Scholar] [CrossRef] [Green Version]
- White, J.V. Aneurysm formation in vivo by the topical degradation of adventitial elastin. J. Vasc. Surg. 1994, 20, 153–155. [Google Scholar] [CrossRef]
- White, J.V.; Mazzacco, S.L. Formation and growth of aortic aneurysms induced by adventitial elastolysis. Ann. N. Y. Acad. Sci. 1996, 800, 97–120. [Google Scholar] [CrossRef]
- Choke, E.; Cockerill, G.; Wilson, W.R.W.; Sayed, S.; Dawson, J.; Loftus, I.; Thompson, M.M. A review of biological factors implicated in abdominal aortic aneurysm rupture. Eur. J. Vasc. Endovasc. Surg. 2005, 30, 227–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vorp, D.A. Biomechanics of abdominal aortic aneurysm. J. Biomech. 2007, 40, 1887–1902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghavan, M.L.; da Silva, E.S. Mechanical properties of AAA tissue. Stud. Mechanobiol. Tissue Eng. Biomater. 2011, 7, 139–162. [Google Scholar]
- Sumner, D.S.; Hokanson, D.E.; Strandness, D.E., Jr. Stress-strain characteristics and collagen-elastin content of abdominal aortic aneurysms. Surg. Gynecol. Obstret. 1970, 130, 459–466. [Google Scholar]
- Sobolewski, K.; Wolańska, M.; Bańkowski, E.; Gacko, M.; Głowiński, S. Collagen, elastin and glycosaminoglycans in aortic aneurysms. Acta Biochim. Pol. 1995, 42, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Carmo, M.; Colombo, L.; Bruno, A.; Corsi, F.R.M.; Roncoroni, L.; Cuttin, M.S.; Radice, F.; Mussini, E.; Settembrini, P.G. Alteration of elastin, collagen and their cross-links in abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2002, 23, 543–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villard, C.; Eriksson, P.; Hanemaaijer, R.; Lindeman, J.H.; Hultgren, R. The composition of collagen in the aneurysm wall of men and women. J. Vasc. Surg. 2017, 66, 579–585. [Google Scholar] [CrossRef]
- Lindeman, J.H.N.; Ashcroft, B.A.; Beenakker, J.-V.M.; van Es, M.; Koekkoek, N.B.R.; Prins, F.A.; Tielemans, J.F.; Abdul-Hussien, H.; Bank, R.A.; Oosterkamp, T.H. Distinct defects in collagen microarchitecture underlie vessel-wall failure in advanced abdominal aneurysms and aneurysms in Marfan syndrome. Proc. Natl. Acad. Sci. USA 2010, 107, 862–865. [Google Scholar] [CrossRef] [Green Version]
- Mikšik, I.; Deyl, Z. Change in the amount of ε-hexosyllisine, UV absorbance, and fluorescence of collagen with age in different animal species. J. Gerontol. 1991, 46, B111–B116. [Google Scholar] [CrossRef] [PubMed]
- Sell, D.R.; Nagaraj, R.H.; Grandhee, S.K.; Odetti, P.; Lapolla, A.; Fogarty, J.; Monnier, V.M. Pentosidine: A molecular marker for the cumulative damage to proteins in diabetes, aging, and uremia. Diabetes Metab. Rev. 1991, 7, 239–251. [Google Scholar] [CrossRef]
- Takahashi, M.; Ohishi, T.; Aoshima, H.; Kawana, K.; Kushida, K.; Inoue, T.; Horiuchi, K. The Maillard protein cross-link pentosidine in urine from diabetic patients. Diabetologia 1993, 36, 664–667. [Google Scholar] [CrossRef] [Green Version]
- Hoshino, H.; Takahashi, M.; Kushida, K.; Ohishi, T.; Kawana, K.; Inoue, T. Quantitation of the crosslinks, pyridinoline, deoxypyridinoline, and pentosidine, in human aorta with dystrophic calcification. Atherosclerosis 1995, 112, 39–46. [Google Scholar] [CrossRef]
- Sims, T.J.; Rasmussen, L.M.; Oxlund, H.; Bailey, A.J. The role of glycation cross-links in diabetic vascular stiffening. Diabetologia 1996, 39, 946–951. [Google Scholar] [CrossRef]
- Reddy, K.C. AGE-related cross-linking of collagen is associated with aortic wall matrix stiffness in the pathogenesis of drug-induced diabetes in rats. Microvasc. Res. 2004, 68, 132–142. [Google Scholar] [CrossRef]
- Schram, M.T.; Henry, R.M.A.; van Dijk, R.A.J.M.; Kostense, P.J.; Dekker, J.M.; Nijpels, G.; Heine, R.J.; Bouter, L.M.; Westerhof, N.; Stehouwer, C.D.A. Increased central artery stiffness in impaired glucose metabolism and type 2 diabetes. Hypertension 2004, 43, 176–181. [Google Scholar] [CrossRef]
- Åstrand, H.; Rydén-Ahlgren, Å.; Sundkvist, G.; Sandgren, T.; Länne, T. Reduced aortic wall stress in diabetes mellitus. Eur. J. Vasc. Endovasc. Surg. 2007, 33, 592–598. [Google Scholar] [CrossRef] [Green Version]
- Le, M.T.Q.; Jamrozik, K.; Davis, T.M.E.; Norman, P.E. Negative association between infra-renal aortic diameter and glycaemia: The Health in Men Study. Eur. J. Vasc. Endovasc. Surg. 2007, 33, 599–604. [Google Scholar] [CrossRef]
- Norman, P.E.; Davis, T.M.E.; Le, M.T.Q.; Golledge, J. Matrix biology of abdominal aortic aneurysms in diabetes: Mechanisms underlying the negative association. Connect. Tissue Res. 2007, 48, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; Karan, M.; Moran, C.S.; Muller, J.; Clancy, P.; Dear, A.E.; Norman, P.E. Reduced expansion rate of abdominal aortic aneurysms in patients with diabetes may be related to aberrant monocyte-matrix interactions. Eur. Heart J. 2008, 29, 665–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butcher, H.R., Jr. The elastic properties of human aortic intima, media and adventitia: The initial effect of thromboendarterectomy. Ann. Surg. 1960, 151, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, D.E.; Smith, R.F.; Whitney, D.G. The durability of aorto-iliac endarteriectomy: A roentgenographic and pathologic study of late recurrence. Arch. Surg. 1964, 89, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Sumner, D.S.; Hokanson, D.E.; Strandness, D.E., Jr. Arterial wall before and after endarterectomy. Stress-strain characteristics and collagen-elastin content. Arch. Surg. 1969, 99, 606–611. [Google Scholar] [CrossRef]
- Inahara, T. Eversion endarterectomy for aortoiliofemoral occlusive disease: A 16 year experience. Am. J. Surg. 1979, 138, 196–204. [Google Scholar] [CrossRef]
- Khor, E. Methods for the treatment of collagenous tissues for bioprostheses. Biomaterials 1996, 18, 95–105. [Google Scholar] [CrossRef]
- Friess, W. Collagen—biomaterial for drug delivery. Eur. J. Pharmac. Biopharmac. 1998, 45, 113–136. [Google Scholar] [CrossRef]
- Chan, B.P.; So, K.-F. Photochemical crosslinking improves the physicochemical properties of collagen scaffolds. J. Biomed. Mater. Res. 2005, 75, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Isenburg, J.C.; Simionescu, D.T.; Vyavahare, N.R. Tannic acid treatment enhances biostability and reduces calcification of glutaraldehyde fixed aortic wall. Biomaterials 2005, 26, 1237–1245. [Google Scholar] [CrossRef]
- Mercuri, J.J.; Lovekamp, J.J.; Simionescu, D.T.; Vyavahare, N.R. Glycosaminoglycan-targeted fixation for improved bioprosthetic heart valve stabilization. Biomaterials 2007, 28, 496–503. [Google Scholar] [CrossRef]
- Tedder, M.E.; Liao, J.; Weed, B.; Stabler, C.; Zhang, H.; Simionescu, A.; Simionescu, D.T. Stabilized collagen scaffolds for heart valve tissue engineering. Tissue Eng. A 2009, 15, 1257–1268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeugolis, D.I.; Paul, G.R.; Attenburrow, G. Cross-linking of extruded collagen fibers–A biomimetic three-dimensional scaffold for tissue engineering application. J. Biomed. Mater. Res. 2009, 89, 895–908. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Mao, X.; Schwend, T.; Littlechild, S.; Conrad, G.W. Resistance of corneal RFUVA–Cross-linked collagens and small leucine-rich proteoglycans to degradation by matrix metalloproteinases. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1014–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rich, H.; Odlyha, M.; Cheema, U.; Mudera, V.; Bozec, L. Effects of photochemical riboflavin-mediated crosslinks on the physical properties of collagen constructs and fibrils. J. Mater. Sci. Mater. Med. 2014, 25, 11–21. [Google Scholar] [CrossRef]
- Deborde, C.; Simionescu, D.T.; Wright, C.; Liao, J.; Sierad, L.N.; Simionescu, A. Stabilized collagen and elastin-based scaffolds for mitral valve tissue engineering. Tissue Eng. A 2016, 22, 1241–1251. [Google Scholar] [CrossRef] [Green Version]
- Tam, H.; Zhang, W.; Infante, D.; Parchment, N.; Sacks, M.; Vyavahare, N.R. Fixation of bovine pericardium-based tissue biomaterial with irreversible chemistry improves biochemical and biomechanical properties. J. Cardiovasc. Trans. Res. 2017, 10, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Krasselt, K.; Frommelt, C.; Brunner, R.; Rauscher, F.G.; Francke, M.; Körber, N. Various cross-linking methods inhibit the collagenase I degradation of rabbit scleral tissue. BMC Ophthalmol. 2020, 20, 488. [Google Scholar] [CrossRef]
- Reiser, K.; McCormick, R.J.; Rucker, R.B. Enzymatic and non-enzymatic cross-linking of collagen and elastin. FASEB J. 1992, 6, 2439–2449. [Google Scholar] [CrossRef] [PubMed]
- Vrhovski, B.; Weiss, A.S. Biochemistry of tropoelastin. Eur. J. Biochem. 1998, 258, 1–18. [Google Scholar] [CrossRef]
- Heinz, A. Elastases and elastokines: Elastin degradation and its significance in health and disease. Crit. Rev. Biochem. Mol. Biol. 2020, 55, 252–273. [Google Scholar] [CrossRef]
- Baurain, R.; Larochelle, J.F.; Lamy, F. Photolysis of desmosine and isodesmosine by ultraviolet light. Eur. J. Biochem. 1976, 67, 155–164. [Google Scholar] [CrossRef]
- Dhital, B.; Durlik, P.; Rathod, P.; Gul-E-Noor, F.; Wang, Z.; Sun, C.; Chang, E.J.; Itin, B.; Boutis, G.S. Ultraviolet radiation reduces desmosine cross-links in elastin. Biochem. Biophys. Rep. 2017, 10, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, L.; Kim, S.-H.; Hagerman, A.E.; Lü, J. Anti-cancer, anti-diabetic and other pharmacologic and biological activities of penta-galloyl-glucose. Pharmac. Res. 2009, 26, 2066–2080. [Google Scholar] [CrossRef] [Green Version]
- Patnaik, S.S.; Piskin, S.; Pillalamarri, N.R.; Romero, G.; Escobar, G.P.; Sprague, E.; Finol, E.A. Biomechanical restoration potential of pentagalloyl glucose after arterial extracellular matrix degeneration. Bioengineering 2019, 6, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isenburg, J.C.; Simionescu, D.T.; Vyavahare, N.R. Elastin stabilization in cardiovascular implants: Improved resistance to enzymatic degradation by treatment with tannic acid. Biomaterials 2004, 25, 3293–3302. [Google Scholar] [CrossRef]
- Isenburg, J.C.; Karamchandani, N.V.; Simionescu, D.T.; Vyavahare, N.R. Structural requirements for stabilization of vascular elastin by polyphenolic tannins. Biomaterials 2006, 27, 3645–3651. [Google Scholar] [CrossRef] [PubMed]
- Vyavahare, N.R.; Isenburg, J.C.; Simionescu, D.T. Elastin Stabilization of Connective Tissue. U.S. Patent 8435553, 24 January 2012. [Google Scholar]
- Isenburg, J.C.; Simionescu, D.T.; Starcher, B.C.; Vyavahare, N.R. Elastin stabilization for treatment of abdominal aortic aneurysms. Circulation 2007, 115, 1729–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagerman, A.E.; Butler, L.G. The specificity of proanthocyanidin-protein interactions. J. Biol. Chem. 1981, 256, 4494–4497. [Google Scholar] [CrossRef]
- Spencer, C.M.; Cai, Y.; Martin, R.; Gaffney, S.H.; Goulding, P.N.; Magnolato, D.; Lilley, T.H.; Haslam, E. Polyphenol complexation―some thoughts and observations. Phytochemistry 1988, 27, 2397–2409. [Google Scholar] [CrossRef]
- Haslam, E. Natural polyphenols (vegetable tannins) as drugs: Possible modes of action. J. Nat. Prod. 1996, 59, 205–215. [Google Scholar] [CrossRef]
- Sinha, A.; Nosoudi, N.; Vyavahare, N. Elasto-regenerative properties of polyphenols. Biochem. Biophys. Res. Commun. 2014, 444, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Sinha, A.; Shaporev, A.; Nosoudi, N.; Lei, Y.; Vertegel, A.; Lessner, S.; Vyavahare, N. Nanoparticle targeting to diseased vasculature for imaging and therapy. Nanomed. Nanotechnol. Biol. Med. 2014, 10, 1003–1012. [Google Scholar] [CrossRef] [Green Version]
- Nosoudi, N.; Chowdhury, A.; Siclari, S.; Parasaram, V.; Karamched, S.; Vyavahare, N. Systemic delivery of nanoparticles loaded with pentagalloyl glucose protects elastic lamina and prevents abdominal aortic aneurysm in rats. J. Cardiovasc. Trans. Res. 2016, 9, 445–455. [Google Scholar] [CrossRef]
- Patnaik, S.S.; Simionescu, D.T.; Goergen, C.J.; Hoyt, K.; Sirsi, S.; Finol, E.A. Pentagalloyl glucose and its functional role in vascular health: Biomechanics and drug-delivery characteristics. Ann. Biomed. Eng. 2019, 47, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Thirugnanasambandam, M.; Simionescu, D.T.; Escobar, P.G.; Sprague, E.; Goins, B.; Clarke, G.D.; Han, H.-C.; Amezcua, K.L.; Adeyinka, O.R.; Goergen, C.J.; et al. The effect of pentagalloyl glucose on the wall mechanics and inflammatory activity of rat abdominal aortic aneurysms. J. Biomech. Eng. 2018, 140, 084502. [Google Scholar] [CrossRef]
- Simionescu, D.; Casco, M.; Turner, J.; Rierson, N.; Yue, J.; Ning, K. Chemical stabilization of the extracellular matrix attenuates growth of experimentally induced abdominal aorta aneurysms in a large animal model. JVS Vasc. Sci. 2020, 1, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Dhital, S.; Vyavahare, N.R. Nanoparticle-based targeted delivery of pentagalloyl glucose reverses elastase-induced abdominal aortic aneurysm and restores aorta to the healthy state in mice. PLoS ONE 2020, 15, e0227165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schack, A.S.; Stubbe, J.; Steffensen, L.B.; Mahmoud, H.; Laursen, M.S.; Lindholt, J.S. Intraluminal infusion of penta-galloyl glucose reduces abdominal aortic aneurysm development in the elastase rat model. PLoS ONE 2020, 15, e0234409. [Google Scholar] [CrossRef]
- Anderson, J.L.; Niedert, E.E.; Patnaik, S.S.; Tang, R.; Holloway, R.L.; Osteguin, V.; Finol, E.A.; Goergen, C.J. Animal model dependent response to pentagalloyl glucose in murine abdominal aortic injury. J. Clin. Med. 2021, 10, 219. [Google Scholar] [CrossRef]
- Golledge, J.; Thanigaimani, S.; Phie, J. A systematic review and meta-analysis of the effect of pentagalloyl glucose administration on aortic expansion in animal models. Biomedicines 2021, 9, 1442. [Google Scholar] [CrossRef]
Figure 1.
(a) A debrided segment of porcine abdominal aorta; (b) Stripping tunica adventitia off the outer side of tunica media.
Figure 1.
(a) A debrided segment of porcine abdominal aorta; (b) Stripping tunica adventitia off the outer side of tunica media.

Figure 2.
Gross histology of porcine abdominal aorta: (a) aortic wall; (b) isolated adventitia; (c) the remaining layers. H&E staining.
Figure 2.
Gross histology of porcine abdominal aorta: (a) aortic wall; (b) isolated adventitia; (c) the remaining layers. H&E staining.

Figure 3.
Representative stress versus strain plot of porcine adventitial specimens subjected to uniaxial tensile deformation in an Instron-type mechanical tester. The treated specimen was exposed to UV-A (365 nm) radiation for 10 min at an irradiance of 45 mW/cm2 prior to testing.
Figure 3.
Representative stress versus strain plot of porcine adventitial specimens subjected to uniaxial tensile deformation in an Instron-type mechanical tester. The treated specimen was exposed to UV-A (365 nm) radiation for 10 min at an irradiance of 45 mW/cm2 prior to testing.

Figure 4.
Mechanical properties of isolated porcine aortic adventitia. The differences between UV-treated (365 nm, 45 mW/cm2, 10 min) and untreated specimens were significant at a level of less than 0.15% (p = 0.0012 for modulus, p = 0.0015 for stress), for n = 30.
Figure 4.
Mechanical properties of isolated porcine aortic adventitia. The differences between UV-treated (365 nm, 45 mW/cm2, 10 min) and untreated specimens were significant at a level of less than 0.15% (p = 0.0012 for modulus, p = 0.0015 for stress), for n = 30.

Figure 5.
In-Vitro enzymatic degradation was evaluated by the weight loss of isolated porcine aortic adventitia treated with 20 U/mL collagenases (37 °C, 48 h). The differences between UV-treated (365 nm, 45 mW/cm2, 10 min) and untreated specimens were significant at a level of 0.5% (p < 0.005) for n = 6.
Figure 5.
In-Vitro enzymatic degradation was evaluated by the weight loss of isolated porcine aortic adventitia treated with 20 U/mL collagenases (37 °C, 48 h). The differences between UV-treated (365 nm, 45 mW/cm2, 10 min) and untreated specimens were significant at a level of 0.5% (p < 0.005) for n = 6.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chirila, T.V.; Suzuki, S. Photocrosslinking of Adventitial Collagen in the Porcine Abdominal Aorta: A Preliminary Approach to a Strategy for Prevention of Aneurysmal Rupture. Designs 2022, 6, 5. https://doi.org/10.3390/designs6010005
AMA Style
Chirila TV, Suzuki S. Photocrosslinking of Adventitial Collagen in the Porcine Abdominal Aorta: A Preliminary Approach to a Strategy for Prevention of Aneurysmal Rupture. Designs. 2022; 6(1):5. https://doi.org/10.3390/designs6010005
Chicago/Turabian StyleChirila, Traian V., and Shuko Suzuki. 2022. "Photocrosslinking of Adventitial Collagen in the Porcine Abdominal Aorta: A Preliminary Approach to a Strategy for Prevention of Aneurysmal Rupture" Designs 6, no. 1: 5. https://doi.org/10.3390/designs6010005