
A Retinal Oct-Angiography and Cardiovascular STAtus (RASTA) Dataset of Swept-Source Microvascular Imaging for Cardiovascular Risk Assessment

 , , ,
, , ,  and
and
Abstract
:1. Summary
2. Ethics Approval
3. Data Description
3.1. Data Composition
- Low cardiovascular risk—CHA2DS2-VASc = [0; 1];
- Intermediate cardiovascular risk—CHA2DS2-VASc = [2; 3];
- High cardiovascular risk—CHA2DS2-VASc = [3; 9].
- «sup» for superficial plexus or «deep» for deep plexus or «cc» for choriocapillaris plexus
- «OD» for right eye or «OS» for left eye
- «AnomAlies Rétiniennes précoces au cours du Diabète de type 1» (AwARD; Early Retinal Anomalies in Type 1 Diabetes) [26]: to specify early retinal microvascular abnormalities by measuring the area of the central retinal avascular zone on SS OCT-A images of patients with type 1 diabetes without diabetic retinopathy (ID-RCB: 2017-A02724-49);95 eyes of 95 patients, from 02/23/2018 to 02/28/2020.
- RETINORM: control group of the AwARD study;137 eyes of 75 volunteers, from 04/12/2021 to 11/25/2021.
- «Retinal Microvascular Changes in Familial Hypercholesterolemia: Analysis with Swept-Source Optical Coherence Tomography Angiography» (FAMILIPO) [27]: to analyze the association between retinal vascular density and the presence of atherosclerosis assessed with the Coronary Artery Calcium score and compare SS OCT-A quantitative parameters between patients with familial hypercholesterolemia (FH) and healthy volunteers from the AwARD study without a history of FH;162 eyes of 81 patients with FH, from 10/21/2020 to 10/27/2021.
- «Obstructive sleep apnea and Retinal vascular NETwork» (ORNET): to describe retinal microvascular characteristics with SS OCT-A in a population with obstructive sleep apnea syndrome (OSAS) and to compare these patients with healthy volunteers (ID-RCB: 2018-A02204-51);159 eyes of 79 patients with OSAS and 62 eyes of 33 volunteers without OSAS, from 07/01/2020 to 02/14/2023.
- «Réseau Microvasculaire Rétinien et Chirurgie Cardiaque de revascularisation coronarienne» (MRCC; Retinal Microvascular Network and Coronary Revascularization Cardiac Surgery): to study, in patients scheduled for coronary revascularization cardiac surgery with extracorporeal circulation, the discriminative capacity of the retinal vascular density to predict the occurrence of acute renal failure defined by the KDIGO criterion [28] within 7 days of surgery (ID-RCB: 2021-A02895-36);33 eyes of 33 patients, from 06/07/2022 to 03/06/2023.
- «Giant cell arteritis study» (GIANT): to describe retinal microvasculature on SS OCT-A in patients with giant cell arteritis without ophthalmological symptoms;56 eyes of 40 patients, from 11/21/2017 to 10/18/2022.
- «Evaluation intelligente de la Rétinopathie diabétique» (EviRed; Intelligent Assessment of Diabetic Retinopathy): to propose SS OCT-A analysis to better predict the risk of diabetic retinopathy than the current classification of diabetic retinopathy mainly based on fundus photography (ANR: 18-RHUS-0008);118 eyes of 63 patients without diabetic retinopathy, from 06/01/2021 to 01/19/2022.
- -
- ID: participant’s anonymous identity code.
- -
- Age: age in years at inclusion.
- -
- Sex: 0 if male gender, 1 if female gender.
- -
- Congestive heart failure: presence of heart failure/moderate–severe cardiac dysfunction with left ventricular ejection fraction ≤ 40%.
- -
- Hypertension: presence of hypertension confirmed by ambulatory blood pressure measurement with a systolic blood pressure ≥ 135 mmHg and/or diastolic blood pressure ≥ 85 mmHg.
- -
- Diabetes mellitus: presence of diabetes mellitus confirmed by a single blood glucose sample ≥ 2 g/L or confirmed by a second blood glucose sample ≥ 1.26 g/L when the first one was ≥1.26 g/L and <2 g/L.
- -
- Stroke: prior stroke or transient ischemic attack or thromboembolism.
- -
- Vascular disease: presence of vascular disease (e.g., peripheral artery disease, myocardial infarction, aortic plaque) confirmed by Doppler ultrasonography, coronary angiography/cardiac magnetic resonance imaging (MRI)/myocardial perfusion scintigraphy, or computed tomography angiography.
- -
- Body mass index: body mass divided by the square of height, in kg/m2.
- -
- CHA2DS2-VASc: cardiovascular score prediction.
- -
- Obstructive sleep apnea syndrome: presence of obstructive sleep apnea syndrome confirmed by respiratory polygraphy or polysomnography.
- -
- Smoking: previous or active smoking.
- -
- Dyslipidemia: presence of dyslipidemia confirmed by two blood samples with HDL-c < 0.35 g/L or LDL-c > 1.30 g/L and/or TG > 1.5 g/L for patients with cardiovascular risk and two blood samples with HDL-c < 0.35 g/L or LDL-c > 1.60 g/L and/or TG > 1.5 g/L for patients without cardiovascular risk.
- -
- OD: oculus dexter (right eye).
- -
- OS: oculus sinister (left eye).
- -
- Fovea Avascular Zone (FAZ) in superficial plexus:
- ○
- FAZ_RL: raw length (perimeter) of the FAZ in mm;
- ○
- FAZ_Ci: circularity index of the FAZ ranging from 0 (most irregular circular shape) to 1 (perfect circular shape);
- ○
- FAZ_RS: raw size (area) of the FAZ in mm2.
- -
- Vessel density (VD): total length of perfused vasculature per unit area in a region of measurement in units of mm−1. It consists of untangling the entire vasculature in the retina, measuring its length, and then dividing it by the area it originally occupied, ranging from a minimum of 0 (no vessels) to an unbounded maximum.
- ○
- Dens_Ave_Sup: VD average in the superficial plexus;
- ○
- Dens_Circle3mm_Sup: VD in a circle of 3 mm diameter in the superficial plexus;
- ○
- Dens_Circle6mm_Sup: VD in a circle of 6 mm diameter in the superficial plexus;
- ○
- Dens_Ave_Deep: VD average in the deep plexus;
- ○
- Dens_Circle3mm_Deep: VD in a circle of 3 mm diameter in the deep plexus;
- ○
- Dens_Circle6mm_Deep: VD in a circle of 6 mm diameter in the deep plexus.
- -
- Perfusion density (PD): total area of perfused vasculature per unit area in a region of measurement ranging from 0 (no perfusion) to 1 (fully perfused).
- ○
- Perf_Ave_Sup: PD average in the superficial plexus;
- ○
- Perf_Circle3mm_Sup: PD in a circle of 3 mm diameter in the superficial plexus;
- ○
- Perf_Circle6mm_Sup: PD in a circle of 6 mm diameter in the superficial plexus;
- ○
- Perf_Ave_Deep: PD average in the deep plexus;
- ○
- Perf_Circle3mm_Deep: PD in a circle of 3 mm diameter in the deep plexus;
- ○
- Perf_Circle6mm_Deep: PD in a circle of 6 mm diameter in the deep plexus.
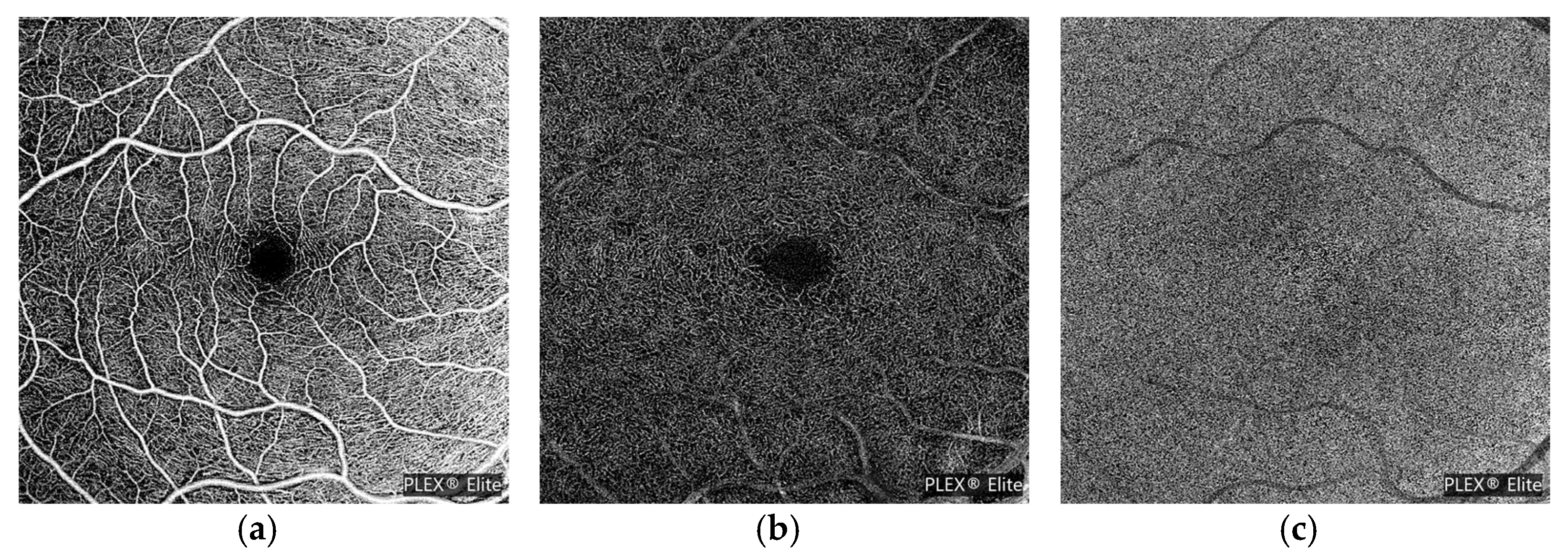
3.2. Swept-Source OCT-A Acquisitions
3.3. Quantitative OCT-A Vascular Features
- -
- Superficial and deep slabs (angio and structure);
- -
- Vessel and perfusion traces for superficial and deep slabs;
- -
- Superficial and deep vessel and perfusion density maps, color overlay images;
- -
- FAZ superficial segmentation;
- -
- Density and FAZ quantification results.
3.4. Cardiovascular Data
4. Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. World Health Organization Reveals Leading Causes of Death and Disability Worldwide: 2000–2019. Available online: https://www.who.int/news/item/09-12-2020-who-reveals-leading-causes-of-death-and-disability-worldwide-2000-2019 (accessed on 26 September 2023).
- Crea, F.; Camici, P.G.; Bairey Merz, C.N. Coronary microvascular dysfunction: An update. Eur. Heart J. 2014, 35, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Yang, H.; Chan-Ling, T. Vascularization of the Human Fetal Retina: Roles of Vasculogenesis and Angiogenesis. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1217–1228. [Google Scholar]
- Arnould, L.; Binquet, C.; Guenancia, C.; Alassane, S.; Kawasaki, R.; Daien, V.; Tzourio, C.; Kawasaki, Y.; Bourredjem, A.; Bron, A.; et al. Association between the retinal vascular network with Singapore “I” Vessel Assessment (SIVA) software, cardiovascular history and risk factors in the elderly: The Montrachet study, population-based study. PLoS ONE 2018, 13, e0194694. [Google Scholar] [CrossRef] [PubMed]
- Seidelmann, S.B.; Claggett, B.; Bravo, P.E.; Gupta, A.; Farhad, H.; Klein, B.E.; Klein, R.; Carli, M.D.; Solomon, S.D. Retinal Vessel Calibers in Predicting Long-Term Cardiovascular Outcomes. Circulation 2016, 134, 1328–1338. [Google Scholar] [CrossRef] [PubMed]
- Arnould, L.; Guenancia, C.; Azemar, A.; Alan, G.; Pitois, S.; Bichat, F.; Zeller, M.; Gabrielle, P.-H.; Bron, A.M.; Creuzot-Garcher, C.; et al. The EYE-MI Pilot Study: A Prospective Acute Coronary Syndrome Cohort Evaluated with Retinal Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4299–4306. [Google Scholar] [CrossRef]
- Jiang, S.; Fang, C.; Xu, X.; Xing, L.; Sun, S.; Peng, C.; Yin, Y.; Lei, F.; Wang, Y.; Li, L.; et al. Identification of High-Risk Coronary Lesions by 3-Vessel Optical Coherence Tomography. J. Am. Coll. Cardiol. 2023, 81, 1217–1230. [Google Scholar] [CrossRef]
- Anderson, K.M.; Wilson, P.W.; Odell, P.M.; Kannel, W.B. An updated coronary risk profile: A statement for health professionals. Circulation 1991, 83, 356–362. [Google Scholar] [CrossRef]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B., Sr.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2935–2959. [Google Scholar] [CrossRef]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S49–S73. [Google Scholar] [CrossRef]
- SCORE2 Working Group; ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar] [CrossRef]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Welles, C.C.; Whooley, M.A.; Na, B.; Ganz, P.; Schiller, N.B.; Turakhia, M.P. The CHADS2 score predicts ischemic stroke in the absence of atrial fibrillation among subjects with coronary heart disease: Data from the Heart and Soul Study. Am. Heart J. 2011, 162, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Taşolar, H.; Çetin, M.; Ballı, M.; Bayramoğlu, A.; Otlu, Y.; Türkmen, S.; Aktürk, E. CHA2DS2-VASc-HS score in non-ST elevation acute coronary syndrome patients: Assessment of coronary artery disease severity and complexity and comparison to other scoring systems in the prediction of in-hospital major adverse cardiovascular events. Anatol. J. Cardiol. 2016, 16, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Kang, I.S.; Pyun, W.B.; Shin, G.J. Predictive value of CHADS2 score for cardiovascular events in patients with acute coronary syndrome and documented coronary artery disease. Korean J. Intern. Med. 2016, 31, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Satilmisoglu, M.H.; Gul, M.; Yildiz, G.; Akgul, O.; Kaya, M.; Cakmak, H.A.; Akkaya, E.; Aslan, S.; Ameri, M.T.; Ozyilmaz, S.O.; et al. Prognostic value of CHA2DS2-VASc score in patients with ST-segment elevation myocardial infarction who underwent primary percutaneous coronary intervention. Acta Cardiol. 2016, 71, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Satılmış, S.; Durmuş, G. Predictive accuracy of CHA(2)DS(2)-VASc score in determining the high thrombus burden in patients with non-ST-elevation myocardial infarction. Acta Cardiol. 2021, 76, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.C.; Su, H.M.; Lee, W.H.; Chiu, C.A.; Chi, N.Y.; Tsai, W.C.; Lin, T.H.; Voon, W.C.; Lai, W.T.; Sheu, S.H.; et al. CHA(2)DS(2)-VASc Score and Risk of New-Onset Peripheral Arterial Occlusive Disease in Patients without Atrial Fibrillation. Acta Cardiol. Sin. 2021, 37, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Kurtul, A.; Acikgoz, S.K. Validation of the CHA2DS2-VASc Score in Predicting Coronary Atherosclerotic Burden and In-Hospital Mortality in Patients With Acute Coronary Syndrome. Am. J. Cardiol. 2017, 120, 8–14. [Google Scholar] [CrossRef]
- Decencière, E.; Zhang, X.; Cazuguel, G.; Laÿ, B.; Cochener, B.; Trone, C.; Gain, P.; Ordóñez-Varela, J.-R.; Massin, P.; Erginay, A.; et al. Feedback on a publicly distributed image database: The Messidor database. Image Anal. Stereol. 2014, 33, 231–234. [Google Scholar] [CrossRef]
- Staal, J.; Abràmoff, M.D.; Niemeijer, M.; Viergever, M.A.; van Ginneken, B. Ridge-based vessel segmentation in color images of the retina. IEEE Trans. Med. Imaging 2004, 23, 501–509. [Google Scholar] [CrossRef]
- Hoover, A.; Kouznetsova, V.; Goldbaum, M. Locating blood vessels in retinal images by piecewise threshold probing of a matched filter response. IEEE Trans. Med. Imaging 2000, 19, 203–210. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and Validation of a Deep Learning Algorithm for Detection of Diabetic Retinopathy in Retinal Fundus Photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Decencière, E.; Cazuguel, G.; Zhang, X.; Thibault, G.; Klein, J.-C.; Meyer, F.; Marcotegui, B.; Quellec, G.; Lamard, M.; Danno, R.; et al. TeleOphta: Machine learning and image processing methods for teleophthalmology. Innov. Res. BioMed. Eng. 2013, 34, 196–203. [Google Scholar] [CrossRef]
- Khan, S.M.; Liu, X.; Nath, S.; Korot, E.; Faes, L.; Wagner, S.K.; Keane, P.A.; Sebire, N.J.; Burton, M.J.; Denniston, A.K. A global review of publicly available datasets for ophthalmological imaging: Barriers to access, usability, and generalisability. Lancet Digit. Health 2021, 3, e51–e66. [Google Scholar] [CrossRef] [PubMed]
- Eid, P.; Creuzot-Garcher, C.; Aho, L.S.; Gabrielle, P.H.; Charpin, E.; Haddad, D.; Steinberg, L.A.; Bron, A.; Verges, B.; Arnould, L. Early Retinal Microvascular Changes Assessed with Swept-Source OCT Angiography in Type 1 Diabetes Patients without Retinopathy. J. Clin. Med. 2023, 12, 2687. [Google Scholar] [CrossRef] [PubMed]
- Eid, P.; Arnould, L.; Gabrielle, P.H.; Aho, L.S.; Farnier, M.; Creuzot-Garcher, C.; Cottin, Y. Retinal Microvascular Changes in Familial Hypercholesterolemia: Analysis with Swept-Source Optical Coherence Tomography Angiography. J. Pers. Med. 2022, 12, 871. [Google Scholar] [CrossRef] [PubMed]
- Summary of Recommendation Statements. Kidney Int. Suppl. 2012, 2, 8–12. [CrossRef]
- Laíns, I.; Wang, J.C.; Cui, Y.; Katz, R.; Vingopoulos, F.; Staurenghi, G.; Vavvas, D.G.; Miller, J.W.; Miller, J.B. Retinal applications of swept source optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA). Prog. Retin. Eye Res. 2021, 84, 100951. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef]
- Ridker, P.M.; Cook, N.R. Statins: New American guidelines for prevention of cardiovascular disease. Lancet 2013, 382, 1762–1765. [Google Scholar] [CrossRef]
- Kuragaichi, T.; Kataoka, Y.; Miyakoshi, C.; Miyamoto, T.; Sato, Y. External validation of pooled cohort equations using systolic blood pressure intervention trial data. BMC Res. Notes 2019, 12, 271. [Google Scholar] [CrossRef]
- Harb, S.C.; Wang, T.K.M.; Nemer, D.; Wu, Y.; Cho, L.; Menon, V.; Wazni, O.; Cremer, P.C.; Jaber, W. CHA(2)DS(2)-VASc score stratifies mortality risk in patients with and without atrial fibrillation. Open Heart 2021, 8, e001794. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.T.; Campbell, B.C.; Meretoja, A.; Churilov, L.; Lees, K.R.; Donnan, G.A.; Davis, S.M. Pre-stroke CHADS2 and CHA2DS2-VASc scores are useful in stratifying three-month outcomes in patients with and without atrial fibrillation. Cerebrovasc. Dis. 2013, 36, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H.; Yiu, K.H.; Lau, K.K.; Yiu, Y.F.; Li, S.W.; Lam, T.H.; Lau, C.P.; Siu, C.W.; Tse, H.F. The CHADS2 and CHA2DS2-VASc scores predict adverse vascular function, ischemic stroke and cardiovascular death in high-risk patients without atrial fibrillation: Role of incorporating PR prolongation. Atherosclerosis 2014, 237, 504–513. [Google Scholar] [CrossRef]
- Chen, Y.L.; Cheng, C.L.; Huang, J.L.; Yang, N.I.; Chang, H.C.; Chang, K.C.; Sung, S.H.; Shyu, K.G.; Wang, C.C.; Yin, W.H.; et al. Mortality prediction using CHADS2/CHA2DS2-VASc/R2CHADS2 scores in systolic heart failure patients with or without atrial fibrillation. Medicine 2017, 96, e8338. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.J.; Wang, G.J.; Shuai, W.; Shen, C.J.; Kong, B.; Huang, H. The Value of the CHADS(2) and CHA(2)DS(2)-VASc Score for Predicting the Prognosis in Lacunar Stroke with or without Atrial Fibrillation Patients. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2019, 28, 104143. [Google Scholar] [CrossRef] [PubMed]
- Wagner, S.K.; Fu, D.J.; Faes, L.; Liu, X.; Huemer, J.; Khalid, H.; Ferraz, D.; Korot, E.; Kelly, C.; Balaskas, K.; et al. Insights into Systemic Disease through Retinal Imaging-Based Oculomics. Transl. Vis. Sci. Technol. 2020, 9, 6. [Google Scholar] [CrossRef]
- Arnould, L.; Meriaudeau, F.; Guenancia, C.; Germanese, C.; Delcourt, C.; Kawasaki, R.; Cheung, C.Y.; Creuzot-Garcher, C.; Grzybowski, A. Using Artificial Intelligence to Analyse the Retinal Vascular Network: The Future of Cardiovascular Risk Assessment Based on Oculomics? A Narrative Review. Ophthalmol. Ther. 2023, 12, 657–674. [Google Scholar] [CrossRef]


{kind=link}
| Subject Area | Biomedical Imaging, Ophthalmology |
| More specific subject area | Retinal OCT-A volumes analysis for cardiovascular risk prediction |
| Type of data | Image, CSV |
| How data were acquired | Swept-source OCT-A Instrument name: PLEX Elite 9000® (Carl Zeiss Meditec Inc., Dublin, OH, USA) |
| Data format | DICOM for volumes, Bitmap for en face images |
| Experimental factors | Pupillary dilatation with tropicamide 0.5% if signal strength < 8/10 |
| Experimental features | Macular angiography 6 × 6-mm |
| Main data source location | University Hospital of Dijon, Dijon 21000, France |
| Data accessibility | https://rasta.u-bourgogne.fr/, accessed on 28 September 2023. |
| ID | Age | Sex | Congestive Heart Failure | Hypertension | Diabetes Mellitus | Stroke | Vascular Disease | Body Mass Index | CHA2DS2-VASc | Obstructive Sleep Apnea Syndrome |
|---|---|---|---|---|---|---|---|---|---|---|
| 7BLCE82 | 39.3 | 1 | 0 | 0 | 1 | 0 | 0 | 27.63 | 2 | 0 |
| 7BODO57 | 63.7 | 0 | 0 | 1 | 1 | 0 | 0 | 39.71 | 2 | 0 |
| Smoking | Dyslipidemia | FAZ_RL_OD | FAZ_Ci_OD | FAZ_RS_OD | FAZ_RL_OS | FAZ_Ci_OS | FAZ_RS_OS | Dens_Ave_Sup_OD | ||
| 0 | 0 | 1.847828 | 0.7151644 | 0.1943207 | 1.870777 | 0.7684844 | 0.2140274 | 17.9124348958329 | ||
| 0 | 1 | 3.164148 | 0.5358088 | 0.4268875 | 1.629538 | 0.7863739 | 0.1661682 | 17.6601562499993 | ||
| Dens_Circle3mm_Sup_OD | Dens_Circle6mm_Sup_OD | Dens_Ave_Sup_OS | Dens_Circle3mm_Sup_OS | Dens_Circle6mm_Sup_OS | ||||||
| 15.7255366682872 | 17.2295695743654 | 20.0175781250004 | 19.2683353754627 | 19.9760718897393 | ||||||
| 14.4667042195168 | 17.5332242119224 | 18.0494791666661 | 18.1161517910436 | 17.8680600309991 | ||||||
| Perf_Ave_Sup_OD | Perf_Circle3mm_Sup_OD | Perf_Circle6mm_Sup_OD | Perf_Ave_Sup_OS | Perf_Circle3mm_Sup_OS | ||||||
| 0.398761749267578 | 0.335599805730937 | 0.380546984640812 | 0.436973571777344 | 0.399284283408211 | ||||||
| 0.380107879638672 | 0.304275197638055 | 0.372604011433318 | 0.409038543701172 | 0.400241226363707 | ||||||
| Perf_Circle6mm_Sup_OS | Dens_Ave_Deep_OD | Dens_Circle3mm_Deep_OD | Dens_Circle6mm_Deep_OD | Dens_Ave_Deep_OS | ||||||
| 0.431644794054866 | 8.82747395833345 | 5.98949651934599 | 8.44266017287466 | 15.5621744791656 | ||||||
| 0.398799313893654 | 6.07356770833347 | 4.00121723028324 | 5.5699215791659 | 4.33268229166667 | ||||||
| Dens_Circle3mm_Deep_OS | Dens_Circle6mm_Deep_OS | Perf_Ave_Deep_OD | Perf_Circle3mm_Deep_OD | Perf_Circle6mm_Deep_OD | ||||||
| 12.0008038845776 | 15.7933960523881 | 0.174694061279297 | 0.118523555123847 | 0.166902197033784 | ||||||
| 5.46489248566923 | 3.8770957475287 | 0.118579864501953 | 0.0750344774003069 | 0.106823345466983 | ||||||
| Perf_Ave_Deep_OS | Perf_Circle3mm_Deep_OS | Perf_Circle6mm_Deep_OS | ||||||||
| 0.310855865478516 | 0.237508995079448 | 0.315187959522492 | ||||||||
| 0.0877456665039063 | 0.105439265426815 | 0.07639377745169 | ||||||||
| Model | Manufacturer | Technology | Hardware | |||
|---|---|---|---|---|---|---|
| PLEX Elite 9000® | Carl Zeiss Meditec Inc, Dublin, OH, USA | Swept Source Optical Coherence Tomography | Optical Micro AngioGraphy (OMAG) | |||
| FOV | Wave Length | Slew Rate | Axial Scan Depth | Optical Axial Resolution | Optical Transversal Resolution | Number of Images in Dataset |
| 56° | 1040–1060 nm | 100,000 A-scans/sec | 3.0 mm | 6.3 µm | 20 µm | 2005 en face images 814 angiocubes |
| Risk Factor | Score |
|---|---|
| Congestive heart failure/Left ventricular dysfunction | 1 |
| Hypertension | 1 |
| Age ≥ 75 years | 2 |
| Diabetes mellitus | 1 |
| Stroke/TIA/TE | 2 |
| Vascular disease (prior myocardial infarction, peripheral artery disease, or aortic plaque) | 1 |
| Age 65–74 years | 1 |
| Sex category (i.e., female gender) | 1 |
| Risk Scheme | Low Risk [0; 1] | Intermediate Risk [2; 3] | High Risk [4; 9] |
|---|---|---|---|
| RASTA (2023) | One or no combination risk factor | One definitive risk factor and 1 or no combination risk factor, or 2 or 3 combination risk factors | Two definitive risk factors, or 1 definitive risk factor and ≥2 combination risk factors, or ≥4 combination risk factors |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Germanèse, C.; Meriaudeau, F.; Eid, P.; Tadayoni, R.; Ginhac, D.; Anwer, A.; Laure-Anne, S.; Guenancia, C.; Creuzot-Garcher, C.; Gabrielle, P.-H.; et al. A Retinal Oct-Angiography and Cardiovascular STAtus (RASTA) Dataset of Swept-Source Microvascular Imaging for Cardiovascular Risk Assessment. Data 2023, 8, 147. https://doi.org/10.3390/data8100147
Germanèse C, Meriaudeau F, Eid P, Tadayoni R, Ginhac D, Anwer A, Laure-Anne S, Guenancia C, Creuzot-Garcher C, Gabrielle P-H, et al. A Retinal Oct-Angiography and Cardiovascular STAtus (RASTA) Dataset of Swept-Source Microvascular Imaging for Cardiovascular Risk Assessment. Data. 2023; 8(10):147. https://doi.org/10.3390/data8100147
Chicago/Turabian StyleGermanèse, Clément, Fabrice Meriaudeau, Pétra Eid, Ramin Tadayoni, Dominique Ginhac, Atif Anwer, Steinberg Laure-Anne, Charles Guenancia, Catherine Creuzot-Garcher, Pierre-Henry Gabrielle, and et al. 2023. "A Retinal Oct-Angiography and Cardiovascular STAtus (RASTA) Dataset of Swept-Source Microvascular Imaging for Cardiovascular Risk Assessment" Data 8, no. 10: 147. https://doi.org/10.3390/data8100147