
Effect of Prebiotics and Synbiotics Carried by Food over Irritable Bowel Syndrome Symptoms: A Systematic Review

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
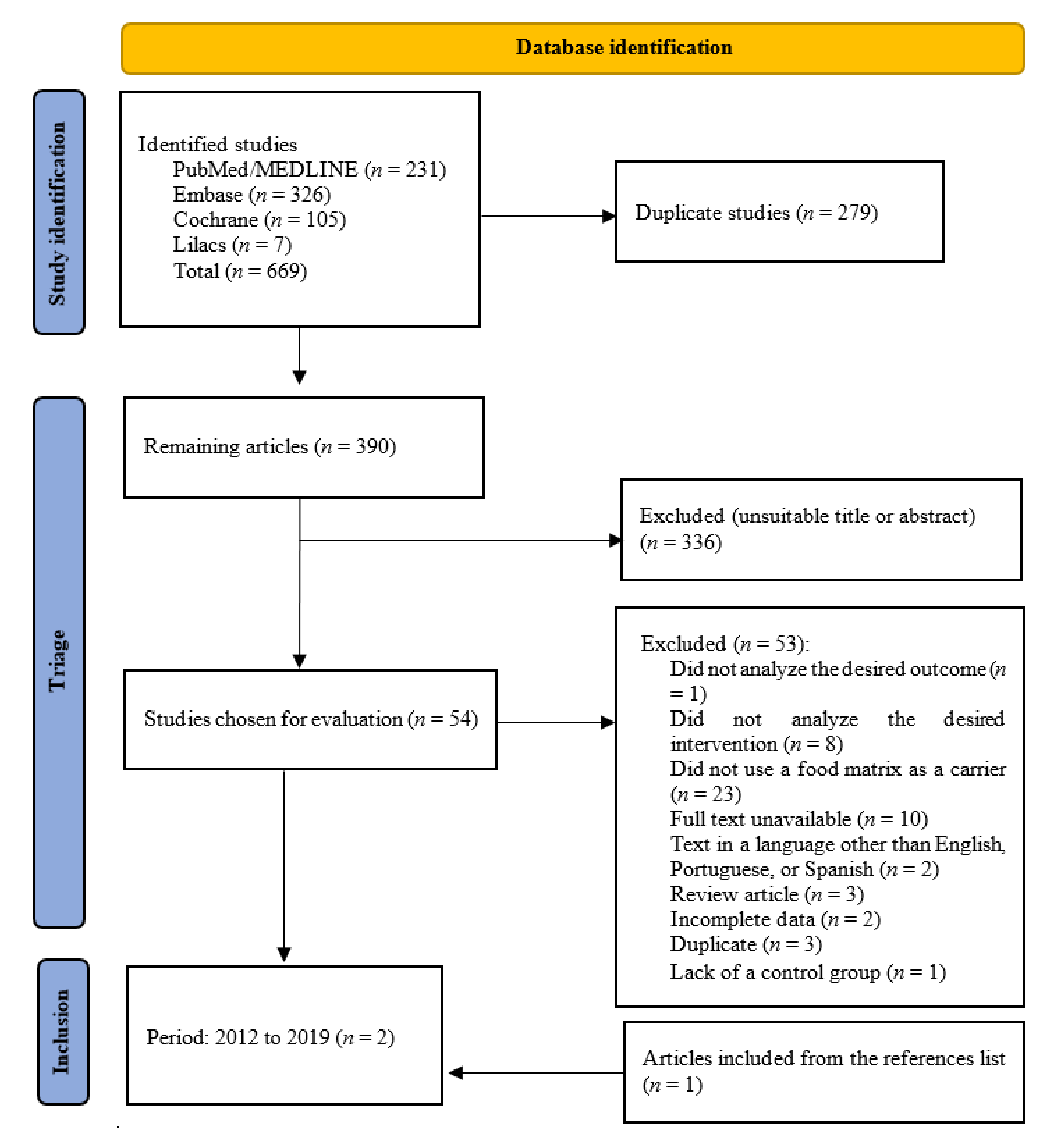
3.1. Study Selection
3.2. Characteristics of the Studies
3.3. Risk of Bias
3.4. Individual Analysis of the Studies
3.4.1. Gastrointestinal Symptoms in IBS-C Patients
3.4.2. Gastrointestinal Symptoms in Patients Suffering from IBS-D
3.4.3. Gastrointestinal Symptoms for Patients Suffering from IBS-M
3.4.4. Gastrointestinal Symptoms in All Patients
3.4.5. Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
| Summary of Review Findings | Studies That Contribute to the Review Finding | CERQual Assessment of Confidence in the Evidence | Explanation of the CERQual Assessment |
|---|---|---|---|
| When IBS subtypes were individually evaluated, individuals receiving the same intervention had different results regarding the analyzed outcomes. Because of that, specific intestinal modulation strategies should be developed for each subtype of IBS. | [21] | Moderate confidence | Moderate concerns about adequacy. |
| Patients who received interventions with the bifidobacterium genus had significant improvements in the overall symptoms of the syndrome. | [21] | Low confidence | Moderate concerns about consistency and serious concerns about adequacy because of the low amount of data contributing to the finding. |
| The use of synbiotics has the potential to reduce overall IBS symptoms and improve the patients’ satisfaction with their bowel habits. | [21,22] | Low confidence | Moderate concerns about methodological limitations and serious concerns about adequacy because of the low amount of data contributing to the finding. |
| Summary of Review Findings | Studies That Contribute to the Review Finding | Methodological Limitations Component | Coherence Component | Adequacy Component | Relevance Component | CERQual Assessment of Confidence in the Evidence | Explanation of the CERQual Assessment |
|---|---|---|---|---|---|---|---|
| When IBS subtypes were individually evaluated, individuals receiving the same intervention had different results regarding the analyzed outcomes. Because of that, specific bowel modulation strategies should be developed for each subtype of IBS. | [21] | Minor concerns about methodological limitations, which are unlikely to reduce confidence in the review finding. | Minor concerns about methodological limitations, which are unlikely to reduce confidence in the review finding. | Moderate concerns about adequacy that will likely reduce confidence in the review finding (only one study contributed to this finding, but this is a topic that has already been discussed by other studies and is a suggestion for further studies). | No concern regarding the relevance of the finding, and that will hardly reduce confidence in the review finding. | Moderate confidence | Moderate concern about adequacy. |
| Patients who received interventions with the bifidobacterium genus had significant improvements in the overall symptoms of the syndrome. | [21] | Minor concerns about methodological limitations, which are unlikely to reduce confidence in the review finding (failure to report treatment allocation method). | Moderate concerns about coherence likely to reduce confidence in the review finding. | Serious concerns regarding the adequacy of the studies since only one study contributed to this finding, and more studies would need to be carried out to be sure of the claim). | No concern regarding the relevance of the finding, and that will hardly reduce confidence in the review finding. | Low confidence | Moderate concerns about consistency and serious concern about adequacy because of the low amount of data contributing to the finding. |
| The use of synbiotics has the potential to reduce overall IBS symptoms and improve the patients’ satisfaction with their bowel habits. | [21,22] | Moderate concerns about methodological limitations, which are likely to reduce confidence in the review finding. One of the studies does not intend to analyze the numerical results (possibility of selection of results). The two studies did not report the treatment allocation method. | Minor concerns about consistency may reduce the confidence of the review finding (although these data are based on data found in the studies, there was variation between symptoms of different subtypes of IBS). | Serious concerns about the adequacy of studies that reduce confidence in the finding. Only one study contributes to the finding of improvement in global IBS symptoms and, in relation to improved satisfaction with bowel habits, one of the studies has moderate informational capacity. | No concern regarding the relevance of the finding, and that will hardly reduce confidence in the review finding. | Low confidence | Moderate concerns for methodological limitations and serious for adequacy because of the low amount of data contributing to the finding. |
References
- Lovel, R.M.; Ford, A.C. Global Prevalence of and Risk Factors for Irritable Bowel Syndrome: A meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721. [Google Scholar] [CrossRef]
- Mearin, F.; Lacy, B.E.; Chang, L.; Chey, W.D.; Lembro, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef] [Green Version]
- Chang, F. Irritable bowel syndrome: The evolution of multi-dimensional looking and multidisciplinary treatments. World J. Gastroenterol. 2014, 20, 2499–2514. [Google Scholar] [CrossRef]
- Enck, P.; Aziz, Q.; Barbara, G.; Farmer, A.D.; Fukudo, S.; Mayer, E.A.; Niesler, B.; Quigley, E.M.M.; Rajilić-Stojanović, M.; Schemann, M.; et al. Irritable bowel syndrome. Nat. Rev. Dis. Primers 2016, 2, 16014. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.C.; Sperber, A.D.; Corsetti, M.; Camilleri, M. Irritable bowel syndrome. Lancet 2020, 396, 1675–1688. [Google Scholar] [CrossRef]
- Simrén, M.; Barbara, G.; Flint, H.J.; Spigel, B.M.R.; Spiller, R.C.; Vanner, S.; Verdu, E.F.; Whorwell, P.J.; Zoetendal, E.G. Intestinal microbiota in functional bowel disorders: A Rome foundation report. Gut 2013, 62, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Moreli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Grastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The international scientific association for probiotics and prebiotics (isapp) consensus statement on the definition and scope of prebiotics. Nat. Rev. Grastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, K.S.; Gibson, G.R.; Hutkins, R.; Reimer, R.A.; Reid, G.; Verbeke, K.; Scott, K.P.; Holscher, H.D.; Azad, M.B.; Delzenn, N.M.; et al. The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of synbiotics. Nat. Rev. Grastroenterol. Hepatol. 2020, 17, 687–701. [Google Scholar] [CrossRef]
- Ford, A.C.; Harris, L.A.; Lacy, B.E.; Quigley, E.M.M.; Moayyedi, P. Systematic review with meta-analysis: The efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment. Pharmacol. Ther. 2018, 48, 1044–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbara, G.; Feinle-Bisset, C.; Ghoshal, U.C.; Quigley, E.M.; Santos, J.; Vanner, S.; Vergnolle, N.; Zoetendal, E.G. The Intestinal Microenvironment and Functional Gastrointestinal Disorders. Gastroenterology 2016, 150, 1305–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranadheera, R.D.C.S.; Evans, C.A.; Adams, M.C.; Baines, S.K. In vitro analysis of gastrointestinal tolerance and intestinal cell adhesion of probiotics in goat’s milk ice cream and yogurt. Food Res. Int. 2012, 49, 619–625. [Google Scholar] [CrossRef]
- Vrese, M.; Schrezenmeir, J. Probiotics, prebiotics and synbiotics. Adv. Biochem. Eng. Biotechnol. 2008, 111, 1–66 101007/10_2008_097. [Google Scholar] [PubMed]
- Ranadheera, R.D.C.S.; Baines, S.K.; Adams, M.C. Importance of food in probiotic efficacy. Food Res. Int. 2010, 43, 1–7. [Google Scholar] [CrossRef]
- FAO; WHO. Probiotics in Food, Health and Nutritional Properties and Guidelines for Evaluation; FAO: Rome, Italy, 2006; Available online: https://www.fao.org/3/a0512e/a0512e.pdf (accessed on 6 January 2022).
- Asha, M.Z.; Khalil, S.F.H. Efficacy and Safety of Probiotics, Prebiotics and Synbiotics in the Treatment of Irritable Bowel Syn-drome: A systematic review and meta-analysis. Sultan Qaboos Univ. Med. J. 2020, 20, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chlebicz-Wójcik, A.; Ślizewska, K. Probiotics, Prebiotics, and Synbiotics in the Irritable Bowel Syndrome Treatment: A review. Biomolecules 2021, 11, 1154. [Google Scholar] [CrossRef]
- Ford, A.C.; Quigley, E.M.M.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.R.; Moayyedi, P. Efficacy of Prebiotics, preobiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: Systematic review aand meta-analysis. Am. J. Gastroenterol. 2014, 109, 1547–1561. [Google Scholar] [CrossRef] [PubMed]
- Canto, G.L. Revisões Sistemáticas da Literatura, Guia Prático; Brazil Publishing: Curitiba, Brazil, 2020; p. 186. [Google Scholar]
- CERQual—Confidence in the Evidence from Reviews of Qualitative Research. Available online: http://cerqual.org/whatisthecerqualapproach (accessed on 4 December 2021).
- Min, Y.W.; Park, S.U.; Jang, Y.S.; Kim, Y.; Rhee, P.; Ko, S.H.; Joo, N.; Kim, S.I.; Kim, C.H.; Chang, D.K. Effect of composite yogurt enriched with acacia fiber and Bifidobacterium lactis. World J. Gastroenterol. 2012, 18, 4563. [Google Scholar] [CrossRef] [PubMed]
- Bahrudin, M.F.; Rani, R.A.; Tamil, A.M.; Mokhtar, N.M.; Ali, R.A.R. Effectiveness of Sterilized Synbiotic Drink Containing Lactobacillus helveticus Comparable to Probiotic Alone in Patients with Constipation-Predominant Irritable Bowel Syndrome. Dig. Dis. Sci. 2019, 65, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Guarrigues, V.; Gálvez, C.; Ortiz, V.; Ponce, M.; Nos, P.; Ponce, J. Prevalence of constipation: Agreement among several criteria and evaluation of the diagnostic accuracy of qualifying symptoms and self-reported definition in a population-based survey in Spain. Am. J. Epidemiol. 2004, 159, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Meydan, C.; Afshinnekoo, E.; Rickard, N.; Daniels, G.; Kunces, L.; Hardy, T.; Lili, L.; Pesce, S.; Jacobson, P.; Mason, C.E.; et al. Improved gastrointestinal health for irritable bowel syndrome with metagenome-guided interventions. Precis. Clin. Med. 2020, 3, 136–146. [Google Scholar] [CrossRef]
- Cherbut, C.; Michel, C.; Raison, V.; Kravtchenko, T.; Severine, M. Acacia Gum is a Bifidogenic Dietary Fibre with High Di-gestive Tolerance in Healthy Humans. Microb. Ecol. Health Dis. 2003, 15, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Carmo, M.M.R.; Walker, J.C.L.; Novello, D.; Caselato, V.M.; Sgarbieri, V.C.; Ouwehand, A.C.; Andreollo, N.A.; Hiane, P.A.; Santos, E.F. Polydextrose: Physiological function, and effects on health. Nutrients 2016, 8, 553. [Google Scholar] [CrossRef]
- World Health Organization. Handbook for Good Clinical Research Practice (GCP): Guidance for Implementation; WHO: Geneva, Switzerland, 2002; Available online: https://www.who.int/medicines/areas/quality_safety/safety_efficacy/gcp1.pdf (accessed on 5 September 2021).
- FAO; WHO. Working Group Report on Drafting Guidelines for the Evaluation of Probiotics in Food. London, Ontario, Canada, 2002. Available online: https://www.who.int/foodsafety/fs_management/en/probiotic_guidelines.pdf (accessed on 5 September 2021).
- Nobaek, S.; Johansson, M.L.; Molin, G.; Ahrné, S.; Jeppsson, B. Alteration of intestinal microflora is associated with reduction in abdominal bloating and pain in patients with irritable bowel syndrome. Am. J. Gastroenterol. 2000, 95, 1231–1238. [Google Scholar] [CrossRef]
- Noorbakhsh, H.; Yavarmanesh, M.; Mortazavi, S.A.; Adibi, P.; Moazzami, A.A. Metabolomics analysis revealed metabolic changes in patients with diarrhea-predominant irritable bowel syndrome and metabolic responses to a synbiotic yogurt intervention. Eur. J. Nutr. 2019, 58, 3109–3119. [Google Scholar] [CrossRef]
- FDA. Guidance for Industry: Meta-Analyses of Randomized Controlled Clinical Trials to Evaluate the Safety of Human Drugs or Biological Products Fishers Lane; U. S. Department of Health and Human Services Food and Drug Administration: Rockville, MD, USA, 2018. Available online: https://www.fda.gov/media/117976/download (accessed on 5 September 2021).
- Lewis, S.J.; Heaton, K.W. Bristol Stool Form Scale as a Useful Guide to Intestinal Transit Time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Bengtsson, M.; Ohlsson, B.; Ulander, K. Development and psychometric testing of the Visual Analogue Scale for Irritable Bowel Syndrome (VAS-IBS). BMC Gastroenterol. 2007, 7, 16. [Google Scholar] [CrossRef]
- Mani-López, E.; Palou, E.; López-Malo, A. Probiotic viability and storage stability of yogurts and fermented milks prepared with several mixtures of lactic acid bacteria. J. Dairy Sci. 2014, 97, 2578–2590. [Google Scholar] [CrossRef] [Green Version]
- Cancaveric, I.; Rehman, M.; Iskander, B.; Lalani, S.; Malik, B.H. Is There a Correlation Between Irritable Bowel Syndrome and Lactose Intolerance? Cureus 2020, 12, 6–13. [Google Scholar] [CrossRef] [Green Version]

| PICOT | Inclusion and Exclusion Criteria |
|---|---|
| Patient | Patients suffering from any type of irritable bowel syndrome, diagnosed by a physician according to Rome Criteria I, II, III, or IV. No restrictions for age, sex, ethnic group, or geographic location. |
| Intervention | Prebiotic or synbiotic foods for patients suffering from irritable bowel syndrome. |
| Control | Non-intervention or placebo. |
| Outcome | Evaluation of the intervention’s effects over the patient’s irritable bowel syndrome symptoms. |
| Type of study | Controlled randomized clinical trial. |
| Study (Year) | Country | Methodology | Diagnosis Criteria | Age Range/Sex | IBS Subtype | Intervention—Daily Dose | Control Group—Daily Dose | Intervention Period (Weeks) | Symptom Evaluation Criteria | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| Min et al. [21] | South Korea | RCT | Rome III | 18–70, males and females | 35% IBS-C; 29.9% IBS-D; 8.5% IBS-M; 26.5% IBS-U | 300 mL of yogurt. Bifidobacterium animalis (≥ufc/serving) + Bifidobacterium booster + acacia fiber + starter culture (n = 58) | 300 mL of yogurt. Bifidobacterium animalis (≥ufc/serving) starter culture (n = 59) | 8 | VAS; Frequency measurement, and BSS | Abdominal symptoms and bowel habits. |
| Bahrudin et al. [22] | Malaysia | RCT | Rome III | >18, males and females | IBS -C | 350 mL of milk-based drink. Lactobacillus helveticus + Polydextrose (1.5 g/100 mL) (n = 79) | 350 mL of milk-based drink. Lactobacillus helveticus (n = 84) | 1 | Garrigues Constipation Questionaries | Stool hardness; Strain; Incomplete evacuation; Bowel blockage; Need to press onto perineum; Defecation time > 10 min; Improvement on constipation. |
| Study (Year) | Bias Arising from the Randomization Process | Bias Due to Deviations from Intended Intervention | Bias Due to Missing Outcome Data | Bias in Measurement of the Outcome | Bias in Selection of the Reported Result | Global Risk |
|---|---|---|---|---|---|---|
| Bahrudin et al. [22] | Some concerns | Low risk | Low risk | Low risk | Some concerns | Some concerns |
| Min et al. [21] | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns |
| Study (Year) | Evluated Symptom | Test Group c—Start | Test Group c—End | Control Group b—Start | Control Group b—End | p-Value between Groups |
|---|---|---|---|---|---|---|
| Min et al. [21] | Strain | 94.70% | 57.9% (p = 0.016) | 81.8% | 54.5% (p = 0.146) | 0.321 |
| Incomplete evacuation | 78.90% | 36.80% (p = 0.021) | 72.70% | 40.90% (p = 0.016) | 0.776 | |
| Satisfaction with bowel habits | - | 26.32 (p = 0) | - | 17.05 (p = 0.004) | 0.21 | |
| Defecation frequency (times per week) | - | 1.79 (p = 0.002) | - | 1.96 (p = 0.032) | 0.872 | |
| Stool consistency | - | 0.789 (p = 0.789) | - | 1.09 (p = 0.001) | 0.386 | |
| Urgency | 21.1% | 21.1% (p = 1) | 13.6% | 27.3% (p = 0.375) | 0.336 | |
| Defecation duration | - | −2.61 (p = 0.106) | - | −4.25 (p < 0.001) | 0.358 | |
| Bahrudin et al. [22] | Strain | 91% | 56% | 77% | 48% | 0.04 |
| Incomplete evacuation | 84% | 56% | 93% | 47% | 0.04 | |
| Stool hardness | 97% | 66% | 90% | 64% | 0.05 | |
| Sensation of blockage | 74% | 47% | 83% | 39% | 0.67 | |
| Need to press onto the perineum | 57% | 37% | 75% | 23% | 0.67 | |
| Defecation lasting more than 10 min | 85% | 69% | 52% | 43% | 0.04 | |
| Constipation relief | 100% | 81% | 100% | 84% | 0.03 |
| Study (Year) | Evaluated Symptom | Variance (1) Test Group | Variance (1) Control Group | p-Value |
|---|---|---|---|---|
| Min et al. [21] | Abdominal pain/discomfort | −19.74 (p = 0.001) | −21.59 (p = 0.001) | 0.8 |
| Frequency of abdominal pain/discomfort | −0.61 (p = 0.032) | −0.6 (p = 0.029) | 0.979 | |
| Bloating | −19.74 (p = 0.007) | −12.5 (p = 0.031) | 0.393 | |
| Flatulence (per week) | 0.08 (p = 0.952) | 0.5 (p = 0.577) | 0.785 | |
| Overall reduction in IBS-C symptoms | 72 ± 18.4 | 50.0 ± 21.8 | <0.001 |
| Study (Year) | Evaluated Symptom | Variance (1) Test Group | Variance (1) Control Group | p-Value |
|---|---|---|---|---|
| Min et al. [21] | Defecation frequency | −1.76 (p = 0.381) | 0 (p = 1) | 0.451 |
| Defecation duration (min) | −0.08 (p = 0.938) | −0.97 (p = 0.3) | 0.52 | |
| Urgency | −2 (p = 0.625) | −1 (p = 1) | 0.867 | |
| Strain | −5 (p = 0.063) | −5 (p = 0.063) | 0.707 | |
| Feeling of incomplete evacuation | −7 (p = 0.039) | −7 (p = 0.016) | 0.826 | |
| Stool consistency | −1.26 (p = 0.001) | −0.63 (p = 0.036) | 0.738 | |
| Satisfaction with bowel habits | 32.9 (p = 0) | 7.81 (p = 0.173) | 0.006 |
| Study (Year) | Evaluated Symptom | Variance (1) Test Group | Variance (1) Control Group | p-Value |
|---|---|---|---|---|
| Min et al. [21] | Abdominal pain/discomfort | −26.68 (p = 0) | −9.38 (p = 0.083) | 0.05 |
| Frequency of abdominal pain/discomfort | −1.82 (p = 0.036) | −0.34 (p = 0.245) | 0.117 | |
| Bloating | −18.42 (p = 0.012) | −6.25 (p = 0.164) | 0.146 | |
| Flatulence (per week) | −0.55 (p = 0.503) | 0.84 (p = 0.255) | 0.212 | |
| Overall reduction in IBS-C symptoms | 61.8 ± 17.4 | 51.6 ± 14.3 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Souza, S.S.; Pierezan, M.D.; de Souza Hassemer, G.; Lima, C.M.G.; De Dea Lindner, J.; Miotto, M.; Verruck, S. Effect of Prebiotics and Synbiotics Carried by Food over Irritable Bowel Syndrome Symptoms: A Systematic Review. Dairy 2022, 3, 148-162. https://doi.org/10.3390/dairy3010012
de Souza SS, Pierezan MD, de Souza Hassemer G, Lima CMG, De Dea Lindner J, Miotto M, Verruck S. Effect of Prebiotics and Synbiotics Carried by Food over Irritable Bowel Syndrome Symptoms: A Systematic Review. Dairy. 2022; 3(1):148-162. https://doi.org/10.3390/dairy3010012
Chicago/Turabian Stylede Souza, Sofia Steinmetz, Milena Dutra Pierezan, Guilherme de Souza Hassemer, Clara Mariana Gonçalves Lima, Juliano De Dea Lindner, Marília Miotto, and Silvani Verruck. 2022. "Effect of Prebiotics and Synbiotics Carried by Food over Irritable Bowel Syndrome Symptoms: A Systematic Review" Dairy 3, no. 1: 148-162. https://doi.org/10.3390/dairy3010012