An Updated Systematic and Comprehensive Review of Cytoreductive Prostatectomy for Metastatic Prostate Cancer

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
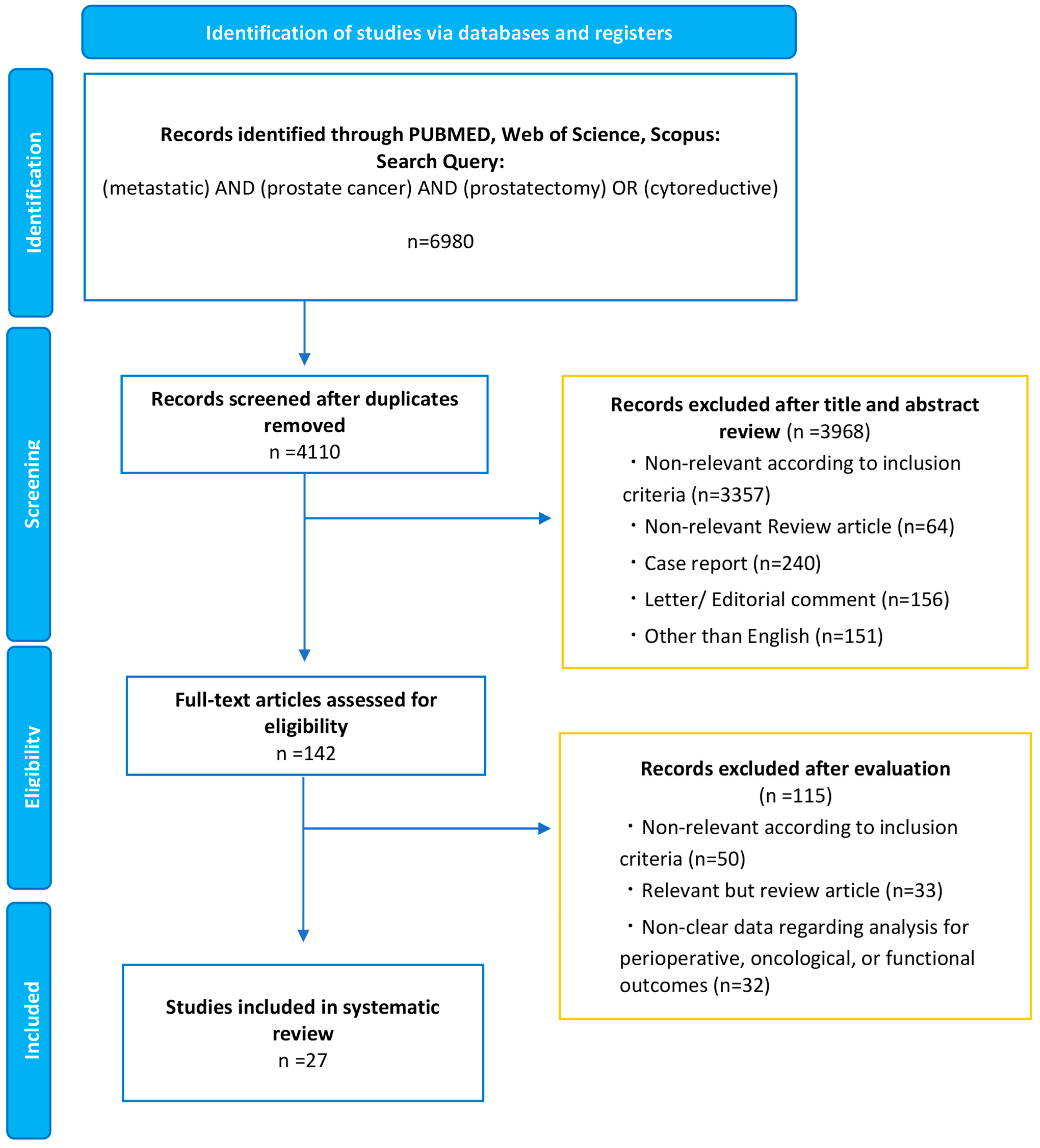
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk-of-Bias Assessment
3. Results
3.1. Study Selection and Characteristics
3.2. Oncologic Outcomes
3.2.1. Population-Based Studies
cRP vs. NLT
cRP vs. RT
3.2.2. Case-Control Studies
cRP vs. NLT
cRP vs. RT
3.2.3. RCT
3.3. Perioperative Outcomes
3.3.1. Complications
3.3.2. Pathologic Outcomes
3.4. Functional Outcomes
3.4.1. Urinary Function
Obstructive Voiding Dysfunction in NLT Patients
Incontinence after cRP
3.4.2. Erectile Function
3.4.3. Quality of Life
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.J.; Azad, A.A.; Iguchi, T.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Alcaraz, A.; Alekseev, B.; Shore, N.D.; et al. Improved Survival with Enzalutamide in Patients with Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. 2022, 40, 1616–1622. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.N.; Chowdhury, S.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez, A.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide in Patients with Metastatic Castration-Sensitive Prostate Cancer: Final Survival Analysis of the Randomized, Double-Blind, Phase III TITAN Study. J. Clin. Oncol. 2021, 39, 2294–2303. [Google Scholar] [CrossRef]
- Fizazi, K.; Foulon, S.; Carles, J.; Roubaud, G.; McDermott, R.; Fléchon, A.; Tombal, B.; Supiot, S.; Berthold, D.; Ronchin, P.; et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet 2022, 399, 1695–1707. [Google Scholar] [CrossRef]
- Smith, M.R.; Hussain, M.; Saad, F.; Fizazi, K.; Sternberg, C.N.; Crawford, E.D.; Kopyltsov, E.; Park, C.H.; Alekseev, B.; Montesa-Pino, Á.; et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2022, 386, 1132–1142. [Google Scholar] [CrossRef]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): Final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019, 20, 686–700. [Google Scholar] [CrossRef]
- Clarke, N.W.; Ali, A.; Ingleby, F.C.; Hoyle, A.; Amos, C.L.; Attard, G.; Brawley, C.D.; Calvert, J.; Chowdhury, S.; Cook, A.; et al. Addition of docetaxel to hormonal therapy in low-and high-burden metastatic hormone sensitive prostate cancer: Long-term survival results from the STAMPEDE trial. Ann. Oncol. 2019, 30, 1992–2003. [Google Scholar] [CrossRef] [PubMed]
- Davis, I.D.; Martin, A.J.; Zielinski, R.R.; Thomson, A.; Tan, T.H.; Sandhu, S.; Reaume, M.N.; Pook, D.W.; Parnis, F.; North, S.A.; et al. Updated overall survival outcomes in ENZAMET (ANZUP 1304), an international, cooperative group trial of enzalutamide in metastatic hormone-sensitive prostate cancer (mHSPC). J. Clin. Oncol. 2022, 40 (Suppl. S17), LBA5004. [Google Scholar] [CrossRef]
- Gravis, G.; Fizazi, K.; Joly, F.; Oudard, S.; Priou, F.; Esterni, B.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): A randomised, open-label, phase 3 trial. Lancet. Oncol. 2013, 14, 149–158. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.E.; Chen, Y.H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J. Clin. Oncol. 2018, 36, 1080–1087. [Google Scholar] [CrossRef] [Green Version]
- Yanagisawa, T.; Rajwa, P.; Thibault, C.; Gandaglia, G.; Mori, K.; Kawada, T.; Fukuokaya, W.; Shim, S.R.; Mostafaei, H.; Motlagh, R.S.; et al. Androgen Receptor Signaling Inhibitors in Addition to Docetaxel with Androgen Deprivation Therapy for Metastatic Hormone-sensitive Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2022, 82, 584–598. [Google Scholar] [CrossRef] [PubMed]
- von Deimling, M.; Rajwa, P.; Tilki, D.; Heidenreich, A.; Pallauf, M.; Bianchi, A.; Yanagisawa, T.; Kawada, T.; Karakiewicz, P.I.; Gontero, P.; et al. The current role of precision surgery in oligometastatic prostate cancer. ESMO Open. 2022, 7, 100597. [Google Scholar] [CrossRef] [PubMed]
- Parker, C.C.; James, N.D.; Brawley, C.D.; Clarke, N.W.; Hoyle, A.P.; Ali, A.; Ritchie, A.W.S.; Attard, G.; Chowdhury, S.; Cross, W.; et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomised controlled phase 3 trial. Lancet 2018, 392, 2353–2366. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qin, Z.; Wang, Y.; Chen, C.; Wang, Y.; Meng, X.; Song, N. The role of radical prostatectomy for the treatment of metastatic prostate cancer: A systematic review and meta-analysis. Biosci. Rep. 2018, 38, BSR20171379. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Hu, M.; Yang, G.; Gao, E.; Xu, W. Cytoreductive prostatectomy improves survival outcomes in patients with oligometastases: A systematic meta-analysis. World J. Surg. Oncol. 2022, 20, 255. [Google Scholar] [CrossRef]
- Shemshaki, H.; Al-Mamari, S.A.; Geelani, I.A.; Kumar, S. Cytoreductive radical prostatectomy versus systemic therapy and radiation therapy in metastatic prostate cancer: A systematic review and meta-analysis. Urologia 2022, 89, 16–30. [Google Scholar] [CrossRef]
- Christ, S.M.; Pohl, K.; Muehlematter, U.J.; Heesen, P.; Kühnis, A.; Willmann, J.; Ahmadsei, M.; Badra, E.V.; Kroeze, S.G.C.; Mayinger, M.; et al. Imaging-Based Prevalence of Oligometastatic Disease: A Single-Center Cross-Sectional Study. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 596–602. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Antwi, S.; Everson, T.M. Prognostic impact of definitive local therapy of the primary tumor in men with metastatic prostate cancer at diagnosis: A population-based, propensity score analysis. Cancer Epidemiol. 2014, 38, 435–441. [Google Scholar] [CrossRef]
- Culp, S.H.; Schellhammer, P.F.; Williams, M.B. Might men diagnosed with metastatic prostate cancer benefit from definitive treatment of the primary tumor? A SEER-based study. Eur. Urol. 2014, 65, 1058–1066. [Google Scholar] [CrossRef]
- Gratzke, C.; Engel, J.; Stief, C.G. Role of radical prostatectomy in metastatic prostate cancer: Data from the Munich Cancer Registry. Eur. Urol. 2014, 66, 602–603. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Xia, H.; Su, X.; Hou, H.; Zhong, Q.; Wang, J. Comparing the Survival Outcomes of Radical Prostatectomy Versus Radiotherapy for Patients with De Novo Metastasis Prostate Cancer: A Population-Based Study. Front. Oncol. 2021, 11, 797462. [Google Scholar] [CrossRef] [PubMed]
- Jin, K.; Qiu, S.; Jin, H.; Zheng, X.; Zhou, X.; Jin, D.; Li, J.; Yang, L.; Wei, Q. Survival Outcomes for Metastatic Prostate Cancer Patients Treated with Radical Prostatectomy or Radiation Therapy: A SEER-based Study. Clin. Genitourin. Cancer 2020, 18, e705–e722. [Google Scholar] [CrossRef]
- Jin, S.; Wei, J.; Wang, J.; Wang, B.; Wu, J.; Gan, H.; Dai, B.; Qin, X.; Lin, G.; Wei, Y.; et al. Prognostic Value of Local Treatment in Prostate Cancer Patients with Different Metastatic Sites: A Population Based Retrospective Study. Front. Oncol. 2020, 10, 527952. [Google Scholar] [CrossRef] [PubMed]
- Parikh, R.R.; Byun, J.; Goyal, S.; Kim, I.Y. Local Therapy Improves Overall Survival in Patients with Newly Diagnosed Metastatic Prostate Cancer. Prostate 2017, 77, 559–572. [Google Scholar] [CrossRef]
- Satkunasivam, R.; Kim, A.E.; Desai, M.; Nguyen, M.M.; Quinn, D.I.; Ballas, L.; Lewinger, J.P.; Stern, M.C.; Hamilton, A.S.; Aron, M.; et al. Radical Prostatectomy or External Beam Radiation Therapy vs No Local Therapy for Survival Benefit in Metastatic Prostate Cancer: A SEER-Medicare Analysis. J. Urol. 2015, 194, 378–385. [Google Scholar] [CrossRef]
- Stolzenbach, L.F.; Deuker, M.; Collà-Ruvolo, C.; Nocera, L.; Tian, Z.; Maurer, T.; Steuber, T.; Tilki, D.; Briganti, A.; Saad, F.; et al. Radical prostatectomy improves survival in selected metastatic prostate cancer patients: A North American population-based study. Int. J. Urol. 2021, 28, 834–839. [Google Scholar] [CrossRef]
- Babst, C.; Amiel, T.; Maurer, T.; Knipper, S.; Lunger, L.; Tauber, R.; Retz, M.; Herkommer, K.; Eiber, M.; von Amsberg, G.; et al. Cytoreductive radical prostatectomy after chemohormonal therapy in patients with primary metastatic prostate cancer. Asian J. Urol. 2022, 9, 69–74. [Google Scholar] [CrossRef]
- Buelens, S.; Poelaert, F.; Claeys, T.; De Bleser, E.; Dhondt, B.; Verla, W.; Ost, P.; Rappe, B.; De Troyer, B.; Verbaeys, C.; et al. Multicentre, prospective study on local treatment of metastatic prostate cancer (LoMP study). BJU Int. 2022, 129, 699–707. [Google Scholar] [CrossRef]
- Chaloupka, M.; Stoermer, L.; Apfelbeck, M.; Buchner, A.; Wenter, V.; Stief, C.G.; Westhofen, T.; Kretschmer, A. Health-Related Quality of Life following Cytoreductive Radical Prostatectomy in Patients with De-Novo Oligometastatic Prostate Cancer. Cancers 2021, 13, 5636. [Google Scholar] [CrossRef]
- Dai, B.; Zhang, S.; Wan, F.N.; Wang, H.K.; Zhang, J.Y.; Wang, Q.F.; Kong, Y.Y.; Ma, X.J.; Mo, M.; Zhu, Y.; et al. Combination of Androgen Deprivation Therapy with Radical Local Therapy Versus Androgen Deprivation Therapy Alone for Newly Diagnosed Oligometastatic Prostate Cancer: A Phase II Randomized Controlled Trial. Eur. Urol. Oncol. 2022, 5, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, A.; Fossati, N.; Pfister, D.; Suardi, N.; Montorsi, F.; Shariat, S.; Grubmüller, B.; Gandaglia, G.; Briganti, A.; Karnes, R.J. Cytoreductive Radical Prostatectomy in Men with Prostate Cancer and Skeletal Metastases. Eur. Urol. Oncol. 2018, 1, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, A.; Pfister, D.; Porres, D. Cytoreductive radical prostatectomy in patients with prostate cancer and low volume skeletal metastases: Results of a feasibility and case-control study. J. Urol. 2015, 193, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.Y.; Mitrofanova, A.; Panja, S.; Sterling, J.; Srivastava, A.; Kim, J.; Kim, S.; Singer, E.A.; Jang, T.L.; Ghodoussipour, S.; et al. Genomic analysis and long-term outcomes of a phase 1 clinical trial on cytoreductive radical prostatectomy. Prostate Int. 2022, 10, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Knipper, S.; Beyer, B.; Mandel, P.; Tennstedt, P.; Tilki, D.; Steuber, T.; Graefen, M. Outcome of patients with newly diagnosed prostate cancer with low metastatic burden treated with radical prostatectomy: A comparison to STAMPEDE arm H. World J. Urol. 2020, 38, 1459–1464. [Google Scholar] [CrossRef]
- Lumen, N.; De Bleser, E.; Buelens, S.; Verla, W.; Poelaert, F.; Claeys, W.; Fonteyne, V.; Verbeke, S.; Villeirs, G.; De Man, K.; et al. The Role of Cytoreductive Radical Prostatectomy in the Treatment of Newly Diagnosed Low-volume Metastatic Prostate Cancer. Results from the Local Treatment of Metastatic Prostate Cancer (LoMP) Registry. Eur. Urol. Open Sci. 2021, 29, 68–76. [Google Scholar] [CrossRef]
- Mandel, P.C.; Huland, H.; Tiebel, A.; Haese, A.; Salomon, G.; Budäus, L.; Tilki, D.; Chun, F.; Heinzer, H.; Graefen, M.; et al. Enumeration and Changes in Circulating Tumor Cells and Their Prognostic Value in Patients Undergoing Cytoreductive Radical Prostatectomy for Oligometastatic Prostate Cancer-Translational Research Results from the Prospective ProMPT trial. Eur. Urol. Focus. 2021, 7, 55–62. [Google Scholar] [CrossRef]
- Mistretta, F.A.; Luzzago, S.; Conti, A.; Verri, E.; Marvaso, G.; Collà Ruvolo, C.; Catellani, M.; Di Trapani, E.; Cozzi, G.; Bianchi, R.; et al. Oligometastatic Prostate Cancer: A Comparison between Multimodality Treatment vs. Androgen Deprivation Therapy Alone. Cancers 2022, 14, 2313. [Google Scholar] [CrossRef]
- Moschini, M.; Morlacco, A.; Kwon, E.; Rangel, L.J.; Karnes, R.J. Treatment of M1a/M1b prostate cancer with or with out radical prostatectomy at diagnosis. Prostate Cancer Prostatic Dis. 2017, 20, 117–121. [Google Scholar] [CrossRef]
- Poelaert, F.; Verbaeys, C.; Rappe, B.; Kimpe, B.; Billiet, I.; Plancke, H.; Decaestecker, K.; Fonteyne, V.; Buelens, S.; Lumen, N. Cytoreductive Prostatectomy for Metastatic Prostate Cancer: First Lessons Learned from the Multicentric Prospective Local Treatment of Metastatic Prostate Cancer (LoMP) Trial. Urology 2017, 106, 146–152. [Google Scholar] [CrossRef]
- Sooriakumaran, P.; Wilson, C.; Rombach, I.; Hassanali, N.; Aning, J.; D Lamb, A.; Cathcart, P.; Eden, C.; Ahmad, I.; Rajan, P.; et al. Feasibility and safety of radical prostatectomy for oligo-metastatic prostate cancer: The Testing Radical prostatectomy in men with prostate cancer and oligo-Metastases to the bone (TRoMbone) trial. BJU Int. 2022, 130, 43–53. [Google Scholar] [CrossRef]
- Steuber, T.; Berg, K.D.; Røder, M.A.; Brasso, K.; Iversen, P.; Huland, H.; Tiebel, A.; Schlomm, T.; Haese, A.; Salomon, G.; et al. Does Cytoreductive Prostatectomy Really Have an Impact on Prognosis in Prostate Cancer Patients with Low-volume Bone Metastasis? Results from a Prospective Case-Control Study. Eur. Urol. Focus. 2017, 3, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K.; Kawase, M.; Kato, D.; Kawase, K.; Takai, M.; Iinuma, K.; Nakane, K.; Hagiwara, N.; Yamada, T.; Tomioka, M.; et al. Robot-Assisted Radical Prostatectomy for Potential Cancer Control in Patients with Metastatic Prostate Cancer. Curr. Oncol. 2022, 29, 2864–2870. [Google Scholar] [CrossRef] [PubMed]
- Xue, P.; Wu, Z.; Wang, K.; Gao, G.; Zhuang, M.; Yan, M. Oncological Outcome of Combining Cytoreductive Prostatectomy and Metastasis-Directed Radiotherapy in Patients with Prostate Cancer and Bone Oligometastases: A Retrospective Cohort Study. Cancer Manag. Res. 2020, 12, 8867–8873. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Fossati, N.; Stabile, A.; Bandini, M.; Rigatti, P.; Montorsi, F.; Briganti, A. Radical Prostatectomy in Men with Oligometastatic Prostate Cancer: Results of a Single-institution Series with Long-term Follow-up. Eur. Urol. 2017, 72, 289–292. [Google Scholar] [CrossRef]
- Mazzone, E.; Mistretta, F.A.; Knipper, S.; Tian, Z.; Larcher, A.; Widmer, H.; Zorn, K.; Capitanio, U.; Graefen, M.; Montorsi, F.; et al. Contemporary National Assessment of Robot-Assisted Surgery Rates and Total Hospital Charges for Major Surgical Uro-Oncological Procedures in the United States. J. Endourol. 2019, 33, 438–447. [Google Scholar] [CrossRef]
- Ploussard, G.; Grabia, A.; Beauval, J.B.; Barret, E.; Brureau, L.; Dariane, C.; Fiard, G.; Fromont, G.; Gauthé, M.; Mathieu, R.; et al. A 5-Year Contemporary Nationwide Evolution of the Radical Prostatectomy Landscape. Eur. Urol. Open Sci. 2021, 34, 1–4. [Google Scholar] [CrossRef]
- Novara, G.; Ficarra, V.; Rosen, R.C.; Artibani, W.; Costello, A.; Eastham, J.A.; Graefen, M.; Guazzoni, G.; Shariat, S.F.; Stolzenburg, J.U.; et al. Systematic review and meta-analysis of perioperative outcomes and complications after robot-assisted radical prostatectomy. Eur. Urol. 2012, 62, 431–452. [Google Scholar] [CrossRef]
- Won, A.C.; Gurney, H.; Marx, G.; De Souza, P.; Patel, M.I. Primary treatment of the prostate improves local palliation in men who ultimately develop castrate-resistant prostate cancer. BJU Int. 2013, 112, E250–E255. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Comparisons | No. of Patients | Recruitment Year | Inclusion Criteria | Confounders for Matching | Follow-Up | Cancer-Specific Mortality | Overall Mortality | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Culp et al. [20] (SEER) | 2014 | NLT | 7811 | 2004–2010 | ·Stage IV (M1a-c) PCa (adenocarcinoma) at diagnosis identified using SEER and divided on the basis of definitive treatment of the RP or BT or NLT | ND | Median: 16 mo. (IQR: 7–31) | 5-yearCSS: 48.7% | 5-year OS: 22.5% (95% CI: 21.1–23.9) | ||
| cRP | 245 | 5-yearCSS: 75.8% | 5-year OS: 67.4% (95% CI: 58.7–74.7) | ||||||||
| BT | 129 | 5-yearCSS: 61.3% | 5-year OS: 52.6% (95% CI: 39.8–63.9) | ||||||||
| Gratzke et al. [21] (Munich Cancer Registry) | 2014 | NLT | 1075 | 1998–2010 | ND | ND | ND | ND | 5-year OS: 21% | ||
| cRP | 74 | 5-year OS: 55% | |||||||||
| RT | 389 | ND | |||||||||
| Antwi et al. [19] (SEER) | 2014 | NLT | 7516 | 2004–2010 | ·Stage IV (M1a-c) PCa (adenocarcinoma) at diagnosis identified using SEER and divided on the basis of definitive treatment of the RP or BT or NLT | Age, race, marital status, tumor grade, PSA level, and cancer registry | ND | ND | Reference | ND | Reference |
| cRP | 222 | Adjusted HR: 0.28 (95% CI: 0.20–0.39) | Adjusted HR: 0.27 (95% CI: 0.20–0.38) | ||||||||
| BT | 120 | Adjusted HR: 0.46 (95% CI: 0.33–0.64) | Adjusted HR: 0.43 (95% CI: 0.31–0.59) | ||||||||
| Satkunasivam et al. [26] (SEER) | 2015 | NLT | 3827 | 2004–2009 | ·Stage IV (M1a-c) PCa (adenocarcinoma) at diagnosis identified using SEER and divided on the basis of definitive treatment of the RP or IMRT or CRT or NLT ·Included only patients > age 65 years | Age at diagnosis, diagnosis year, race, marital status, pretreatment PSA (categorical variable), clinical tumor stage and grade, CCI, ADT, and bone radiation within 6 months of diagnosis | Median: 20 mo. (IQR: 10–36) | 3-year CSS: 46% | Reference | 3-year OS: 34% | Reference |
| cRP | 47 | 3-year CSS: 79% | Adjusted HR: 0.48 (95% CI: 0.27–0.85) | 3-year OS: 73% | Adjusted HR: 0.43 (95% CI: 0.26–0.70) | ||||||
| IMRT | 88 | 3-year CSS: 82% | Adjusted HR: 0.38 (95% CI: 0.24–0.61) | 3-year OS: 72% | Adjusted HR: 0.45 (95% CI: 0.31–0.65) | ||||||
| CRT | 107 | 3-year CSS: 49% | Adjusted HR: 0.85 (95% CI: 0.64–1.14) | 3-year OS: 37% | ND | ||||||
| Parikh et al. [25] (NCDB) | 2017 | NLT | 5224 | 2004–2013 | ·Stage IV (M1a-c) PCa (adenocarcinoma) at diagnosis identified using NCDB and divided on the basis of definitive treatment of the RP or IMRT or CRT or NLT | Race, age, CCI score, T-stage, N-stage, insurance status, income quartile, facility type, and use of ADT | Median: 22 mo. | ND | ND | 5-year OS: 17.1% | Reference |
| cRP | 622 | 5-year OS: 51.4% | Adjusted HR: 0.51 (95% CI: 0.45–0.59) | ||||||||
| CRT | 153 | 5-year OS: 26.8% | Adjusted HR: 1.04 (95% CI: 0.86–1.27) | ||||||||
| IMRT | 52 | Adjusted HR: 0.47 (95% CI: 0.31–0.72) | |||||||||
| Jin S et al. [24] (SEER) | 2020 | NLT | 5628 | 2010–2014 | ·Stage IV (M1a-c) PCa (adenocarcinoma) at diagnosis identified using SEER and divided on the basis of definitive treatment of the RP or BT or NLT | ND | ND | ND | Reference | ND | Reference |
| cRP | 159 | Adjusted HR: 0.56 (95% CI: 0.37–0.86) | Adjusted HR: 0.60 (95% CI: 0.42–0.87) | ||||||||
| BT | 62 | Adjusted HR: 0.71 (95% CI: 0.43–1.18) | Adjusted HR: 0.72 (95% CI: 0.46–1.14) | ||||||||
| Jin K et al. [23] (SEER) | 2020 | NLT | 18,857 | 2004–2015 | ·Stage IV (M1a-c) PCa (adenocarcinoma) at diagnosis identified using SEER and divided on the basis of definitive treatment of the RP or RT or NLT ·Patients who received EBRT with unknown region were excluded | marital status, race, age, clinical TNM stages, GS, and PSA level | ND | Reference | NA | Reference | NA |
| cRP | 435 | Adjusted HR (Cox regression): 0.39 (95% CI: 0.34–0.45) Adjusted HR (PSM): 0.50 (95% CI: 0.41–0.60) Adjusted HR (Covariate adjustment PS): 0.57 (95% CI:0.49–0.66) | Adjusted HR (Cox regression): 0.61 (95% CI: 0.42–0.91) Adjusted HR (PSM): 0.49 (95% CI: 0.32–0.73) | Adjusted HR (Cox regression): 0.39 (95% CI: 0.35–0.44) Adjusted HR (PSM): 0.51 (95% CI: 0.44–0.60) Adjusted HR (Covariate adjustment PS): 0.57 (95% CI: 0.50–0.65) | Adjusted HR (Cox regression): 0.60 (95% CI: 0.43–0.83) Adjusted HR (PSM): 0.45 (95% CI: 0.32–0.65) | ||||||
| RT | 320 | Reference | Reference | ||||||||
| Guo et al. [22] (SEER) | 2021 | cRP | 481 (148) * | 2004–2016 | ·Stage IV (M1a-c) PCa (adenocarcinoma) at diagnosis identified using SEER and divided on the basis of definitive treatment of the RP or RT ·Patients with incomplete clinicopathological data, such as T-stage, PSA value, and GS were excluded | Age, year of diagnosis, PSA level, clinical tumor stage, biopsy GS, and the M stage | Median (IQR): 37 mo. (14.0–83.5) | 10-year CSS: 73.8% | Adjusted HR (PSM): 0.77 (95% CI: 0.46–1.30) Adjusted HR (SMRW): 0.83 (95% CI: 0.52–1.32) | 10-year OS: 60.8% | Adjusted HR (PSM): 0.73 (95% CI: 0.48–1.11) Adjusted HR (SMRW): 0.75 (95% CI: 0.52–1.09) |
| RT | 203 (148) * | Median (IQR): 56.5 mo. (18.0–110.0) | 10-year CSS: 66.7% | Reference | 10-year OS: 45.6% | Reference | |||||
| Stolzenbach et al. [27] (SEER) | 2021 | cRP | 954 | 2004–2016 | ·Stage IV (M1a-b) PCa (adenocarcinoma) at diagnosis identified using SEER and divided on the basis of definitive treatment of the RP or RT ·On the basis of the composition of the STAMPEDE trial and on the basis of the definition of low-volume mPCa, M1c patients were excluded | Age at diagnosis, initial PSA, biopsy GGG, and clinical T, N and M1 stages | Median (range): 23 mo. (11–46) | PSM cohort 5-year CSM: 47% (p = 0.003) | Adjusted HR (PSM and CRR): 0.79 (95% CI: 0.68–0.90) | ND | ND |
| RT | 3326 | Median (range): 21 mo. (10–42) | PSM cohort 5-year CSM: 53% (p = 0.003) | Reference | |||||||
| Author | Year | Comparisons | No. of pts. | Recruitment Year | Country (Institution) | Inclusion Criteria | Treatment after cRP | Follow-Up Duration | Progression-Free | Time to CRPC/CRPC-Free Survival | Cancer-Specific Survival | Overall Survival |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparative studies between cRP and no cRP | ||||||||||||
| Heidenreich et al. [33] | 2015 | cRP | 23 | ND | Germany | Patients with biopsy-proven PCa, minimal bone metastases (3 or fewer hot spots on bone scan), absence of visceral or extensive LN metastases and PSA decrease to less than 1.0 ng/mL after neoadjuvant ADT | No treatment: 9 (39) ADT only: 5 (21): ABI: 5 (21) DOC: 2 (21) | Median (range): 34.5 mo. (7–75) | Median (range): 38.6 mo. (12–52) | Median (range): 40 mo. (9–65) | Median: 47 mo. (range: 9–71) 95.6% | 91.3% |
| No cRP | 38 | Patients with mPCa treated with ADT without LT served as the control group | Median (range): 37.0 mo. (28–96) | Median (range): 26.5 mo. (12–48) | Median (range): 29 mo. (16–54) | Median: 40.5 mo. (range: 19–75) 84.2% | 78.9% | |||||
| Poelaert et al. [40] (LoMP trial) | 2017 | cRP | 17 | 2014- | Multicenter | RP was performed in asymptomatic patients with a resectable tumor and who were fit to undergo surgery (group A, n = 17) | No treatment: 4 (24) ADT: 13 (76) | Mean ± SD: 13 ± 8 mo. | ND | No patients develop CRPC | 2-yr: 100% | 2-yr: 100% |
| No cRP | 29 | Only SOC was administered to patients with mPCa ineligible or unwilling to undergo cRP (group B, n = 29) | Mean ± SD: 16 ± 10 mo. | Median (range): 14 mo. (2–26) | 2-yr: 61% | 2-yr: 55% | ||||||
| Moschini et al. [39] | 2017 | cRP | 31 | 2007–2014 | USA (Mayo) | 31 (66%) underwent cRP with or without adjuvant therapies and 16 (34%) underwent ADT only | M1a: minimum 6 mo. ADT M1b: minimum 6 mo. ADT + MDT | Median: 38.8 mo. | ND | ND | 1-yr: 100% 3-yr: 91.3% 5-yr: 61.9% | ND |
| No cRP | 16 | NA | 1-yr: 93.8% 3-yr: 76.9% 5-yr: 46.2% | |||||||||
| Steuber et al. [42] | 2017 | cRP | 43 | 2000–2011 | Germany (Martini-Klinik Prostate Cancer Center) | Patients with low-volume bone metastases (1–3 lesions) undergoing cRP | All patients received ADT or CAB | Median: 32.7 mo. | ND | No significant differences in CRPC-free survival: p = 0.92 | ND | No significant differences in overall survival: p = 0.92 |
| No cRP | 40 | Patients receiving best systemic therapy | Median: 82.2 mo. | |||||||||
| Buelens et al. [29] (LoMP trial) | 2022 | cRP | 40 | 2014–2018 | Multicenter | Asymptomatic patients: cRP was offered to all fit patients with resectable tumors, resulting in 40 patients; standard of care was administered to 40 patients who were ineligible or unwilling to undergo surgery | All patients received ADT ± DOC/ABI | Median (IQR): 38 (32–50) mo. | ND | Median CRPC-free survival: 53 mo. (95% CI: 14–92) 3-yr: 59% (95% CI: 43–74) | ND | ND |
| No cRP | 40 | Median (IQR): 31 (15–46) mo. | Median CRPC-free survival: 21 mo. (95% CI: 15–27) 3-yr: 40% (95% CI: 25–55) | |||||||||
| Mistretta et al. [38] | 2022 | cRP | 40 | 2010–2018 | Italy | Patients affected by cM1a-b oligometastatic PCa (defined as <5 metastatic lesions at diagnosis involving M1a and/or bone (M1b), with locally resectable cT1-T3 tumors) | Adjuvant ADT at least 12 mo. | Median: 55 mo. | radiological progression: 83.1% | mCRPC rate: 24.0% | CSM: 5.9% | ND |
| No cRP | 34 | NA | Median: 50 mo. | radiological progression: 62.5% | mCRPC rate: 62.5% | CSM: 37.1% | ||||||
| RCT (Phase1/2) for cRP vs. No cRP | ||||||||||||
| Sooriakumaran et al. [41] (TRoMbone) | 2022 | cRP | 25 | ND | UK (multicenter) | Patients diagnosed with oligometastatic PCa (defined as one to three skeletal lesions on bone imaging, no visceral metastases); locally resectable tumor (clinical/radiological stage T1–T3; ECOG-PS 01); and suitable for RP within 3 months of starting SOC All patients received SOC systemic therapy of ADT + DOC | All patients received ADT ± DOC | ND | ND | |||
| No cRP | 25 | ND | ||||||||||
| Comparative studies between cRP and RT | ||||||||||||
| Knipper et al. [35] | 2020 | cRP | 78 | 2008–2018 | Germany (Martini-Klinik Prostate Cancer Center) | Patients with newly diagnosed mPCa with low-volume (<4 bone metastases) and no visceral metastases according to STAMPEDE definition), confirmed on bone scan and CT/MRI, who underwent RP with PLND | All patients received ADT | Median (IQR): 36 (15–48) mo. | 3-yr metastatic PFS: 63% | ND | 3-yr CSS: 92% | 3-yr OS: 91% |
| STAMPEDE arm H (low volume with RT) | 410 | NA | NA | ND | 3-yr metastatic PFS: 67% | 3-yr CSS: 86% | 3-yr OS: 81% | |||||
| RCT (Phase2) assessing LT (including 85% of cRP) vs. NLT | ||||||||||||
| Dai et al. [31] | 2022 | LT | 100 (85) * | 2015–2019 | China | Patients with newly diagnosed oligometastasis PCa defined as five or fewer bone or extrapelvic LN metastases and no visceral metastases | All patients received ADT (94% received CAB) | Median (IQR): 48 (43–50) mo. | Median rPFS: not reached 3-yr rPFS: 79% HR: 0.43, 95% CI: 0.27–0.70 | ND | ND | 3-yr OS: 88% HR: 0.44, 95% CI: 0.24–0.81 |
| NLT | 100 | Median rPFS: 40 mo. 3-yr rPFS: 56% | 3-yr OS: 70% | |||||||||
| Comparative studies between cRP, RT, and NLT | ||||||||||||
| Lumen et al. [36] (LoMP trial) | 2021 | cRP | 48 | 2014- | Multicenter | RP was performed in asymptomatic patients with a resectable tumor and who were fit to undergo surgery; only SOC was administered to patients with metastatic prostate cancer ineligible or unwilling to undergo cRP For this study, patients with high-volume disease were excluded, leaving only patients with low-volume disease for evaluation | All patients received SOC (ADT ± ARSI or DOC) | Median (IQR): 42 (24–57) mo. | ND | ND | 2-yr CSS: 93% (vs. NLT: HR 0.36, 95% CI:0.14–0.94) | 2-yr OS: 93% (vs. NLT: HR 0.28, 95% CI:0.11–0.71) |
| RT | 26 | Median (IQR): 26 (14–51) mo. | 2-yr CSS: 100% (vs. NLT: HR 0.33, 95% CI: 0.09–1.20) | 2-yr OS: 100% (vs. NLT: HR 0.26, 95% CI: 0.07–0.91) | ||||||||
| NLT | 35 | Median (IQR): 24 (12–44) mo. | 2-yr CSS: 75% | 2-yr OS: 69% | ||||||||
| Comparative studies between cRP and RP for localized PCa | ||||||||||||
| Chaloupka et al. [30] | 2021 | cRP | 79 | 2012–2020 | Germany (Ludwig-Maximilians University) | cRP was performed in patients with oligometastasis, defined as <5 bone lesions in the preoperative staging; biopsy-proven PCa, history of RP at one tertiary center and completed follow-up; patients with preoperative ADT and pre-RP RT of the prostate were excluded from further analysis Of 1268 pts., matched cohort of 411 patients were retained after PSM | ND | ND | ND | ND | 5-yr CSS: 61% | 5-yr OS: 38% |
| RP for localized PCa | 332 | 5-yr CSS: 81% | 5-yr OS: 57% | |||||||||
| Single arm or only including cRP cohort | ||||||||||||
| Gandaglia et al. [45] | 2017 | cRP | 11 | 2006–2011 | Italy | Patients with oligometastatic PCa | Adjuvant ADT: 10 (91) | Median (IQR): 63 mo. (48–77) | 7-yr cPFS: 45% | ND | 7-yr CSS: 82% | ND |
| Heidenreich et al. [32] | 2018 | cRP | 113 | ND | Multicenter | Biopsy-proven mPCa who fulfilled the following selection criteria: (1) completely resectable PCa; (2) osseous metastases; (3) absence of gross retroperitoneal LN metastases; (4) absence of bulky pelvic LN metastases >3 cm; (5) no or minimal visceral metastases; (6) ECOG-PS of 0–1; and (7) written informed consent | Neoadjuvant ADT:80 (71), adjuvant ADT: 91 (87) | Median (range): 45.7 mo. (13–96) | Median(range): 72.3 mo. (8–96) 65 pts. remain clinical progression-free at 5yr | ND | ND | 3-yr OS: 89.3% 5-yr OS: 80.5% |
| Xue et al. [44] | 2020 | cRP + MDT | 26 | 2012–2016 | Multicenter (China) | (1) Biopsy-confirmed diagnosis of prostate adenocarcinoma; (2) M1b disease with the presence of 1–5 visible bone metastases (by Tc-99m MDP BS, CT, or MRI); (3) not received RT and chemotherapy in hormone-sensitive phase; (4) adequate organ function; (5) ECOG performance status 0.1; (6) pretreatment total testosterone > 200 ng/dL; and (7) written informed consent | All patients received ADT | Median (range): 43.1 mo. (15–61) | ND | 3-yr CRPC-free survival: 75.9% RP + MDT had better CRPC-free survival (HR: 0.41, 95% CI: 0.18–0.95) | 3-yr CSS: 91.4% No significant differences between two groups (HR: 0.59, 95% CI: 0.12–2.95) | ND |
| cRP only | 32 | Median (range): 47.6 mo. (18–65) | ||||||||||
| Mandel et al. [37] (ProMPT trial) | 2021 | cRP (assessing CTC as prognostic value) | 33 | 2014–2015 | Germany (Martini-Klinik Prostate Cancer Center) | (1) Newly diagnosed PCa, with 1–3 bone metastases (positive BS and confirmed by CT or MRI; no PETCT was used) at the time of diagnosis; (2) asymptomatic patient; (3) absence of visceral metastases; (4) locally resectable tumor (<cT3); (5) PSA at diagnosis <150 mg/dl; and (6) no prior radiation of bone metastases; in addition to cRP, the best systemic therapy (only ADT) was recommended to all patients | All patients were recommended ADT | Median: 39.4 mo. | ND | 3-yr CRPC-free survival: 65.6% | ND | 3-yr OS: 87.9% |
| Babst et al. [28] | 2021 | cRP (assessing the impact of upfront DOC-based doublet therapy) | 38 | 2015–2018 | Germany (two centers) | Patients with mHSPC underwent cRP after primary chemohormonal therapy (DOC +ADT) | All patients received ADT continuously | Median (range): 22.6 mo. (5.7–48.6) | ND | Median time to CRPC: 35.9 mo. | ND | ND |
| Kim et al. [34] | 2022 | cRP | 32 | ND | Multicenter (USA, South Korea, Japan) | The major inclusion criterion was biopsy-proven N1M0 or NxM1a/b PCa | All patients received ADT | Median (IQR): 46 (32–53) mo. | ND | ND | ND | 5-yr OS: 67% (All patients) 69% (M1 patients) |
| Takagi et al. [43] | 2022 | cRP (assessing the feasibility of RARP) | 12 | 2017–2021 | Japan (two centers) | Patients with mPCa who had undergone neoadjuvant therapy followed by RARP | Adjuvant ADT: 5 (25) | ND | BCR-free survival: 1-yr: 83.3%/2-yr: 66.7% MFS: 1-yr: 90%/2-yr: 90% | ND | ND | ND |
| Author | Year | Comparisons | No. of Pts. | Approach of CRP, n (%) | Nerve Sparing | LND, n (%) | LN Removed, n | LN Involvement, n (%) | Estimated Blood Loss, mL | Operation Time, Min | Catheterization, Days | LOS, Days | Postoperative Complication (All), n (%) | Postoperative Complication (CD > 3), n(%) | Rectal Injury, n (%) | PSM, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Heidenreich et al. [33] | 2015 | cRP | 23 | Open RP | ND | All ePLND | ND | 13 (57) | Mean (range): 335 (250–600) | Mean (range): 127 (115–145) | Mean (range): 5.6 days (5–12) | Mean (range): 7.8 (6–13) | 9 (39) | 3 (13) | ND | 4 (17) |
| Poelaert et al. [40] (LoMP trial) | 2017 | cRP | 17 | Open: 1 RARP: 16 | None | All ePLND | Median (range): 20 (9–47) | 12 (71) | Median (range): 250 (100–900) | Median (range): 215 (150–290) | ND | ND | 7 (41) | 0 | 0 | 14 (82) |
| Moschini et al. [39] | 2017 | cRP | 31 | Open RP | ND | All ePLND | Median (IQR): 19 (13–31) | 20 (64) | Median (IQR): 400 (250–500) | ND | ND | Median (IQR): 3 (3–5) | 30 days: 9 (29) 90 days: 4 (13) | 30 days: 2( 6.5) 90 days: 2 (6.5) | 0 | 8 (26) |
| Steuber et al. [42] | 2017 | cRP | 43 | ND | None: 74% Unilateral: 16% Bilateral: 9.3% | ND | Median (IQR): 21 (12–27) | 67% | ND | ND | ND | ND | ND | ND | ND | 67% |
| Buelens et al. [29] (LoMP trial) | 2022 | cRP | 40 | Open: 2 RARP: 38 | None | All ePLND | Median (IQR): 17 (11–21) | 31 (78) | Median (IQR): 250 (150–325) | Median (IQR): 205 (165–220) | ND | ND | 90 days 20 (50) | 2 (5) | 0 | 32 (80) |
| Sooriakumaran et al. [41] (TRoMbone) | 2022 | cRP | 25 | RARP | ND | All ePLND | 11 (7–14) | 11 (46) | ND | Median (IQR): 185 (165–217) | 14 (10–14) | Median (IQR): 1 (1–2) | 3 (12.5) | ND | ND | 10 (42) |
| Knipper et al. [35] | 2020 | cRP | 78 | Open RP | ND | ND | ND | ND | ND | ND | ND | ND | 34 (44) | 16 (21) | ND | ND |
| Dai et al. [31] | 2022 | cRP | 85 | Open RP: 68 (80) RARP: 17 (20) | ND | ND | ND | 26 (31) | ND | ND | ND | ND | 24 (28) | 7 (8.2) | 1 (1.2) | 36 (42) |
| Chaloupka et al. [30] | 2021 | cRP | 79 | Open: 69 (87) RARP:10 (13) | 13 (17) | ND | Median (IQR): 10 (6–13) | 41 (52) | ND | ND | ND | ND | ND | ND | ND | 59 (75) |
| RP for localized PCa | 332 | Open: 116 (35) RARP: 216 (65) | 183 (55) | Median (IQR): 11 (6–18) | 112 (34) | 165 (50) | ||||||||||
| Gandaglia et al. [41] | 2017 | cRP | 11 | Open | ND | All ePLND | Median (IQR): 27 (23–42) | 10 (91) | Median (IQR): 750 (600–850) | Median (IQR): 170 (160–380) | ND | Median (IQR): 13 (7–19) | 6 (54) | 2 (18) | 0 | 8 (73) |
| Heidenreich et al. [32] | 2018 | cRP | 113 | Open: 104 (92) RARP: 9 (8) | ND | None: 1.8% Limited: 8.8% Extended: 89.4% | Median (range): 15.3 (0–57) | 70 (62) | ND | Median (range): 145 (95–380) | ND | Median (range): 6.5 (3–21) | 38 (34) | 11 (9.7) | 0 | 42 (37) |
| Xue et al. [44] | 2020 | cRP + MDT | 26 | Open/LRP | ND | All | ND | 10 (39) | ND | ND | ND | ND | ND | ND | ND | 3 (12) |
| cRP only | 32 | 10 (32) | 4 (13) | |||||||||||||
| Mandel et al. [37] (ProMPT trial) | 2021 | cRP | 33 | Open: 28 (85) RARP: 5 (15) | ND | ND | ND | 24 (73) | ND | ND | ND | ND | ND | ND | ND | 24 (73) |
| Babst et al. [28] | 2021 | cRP | 38 | Open: 35 (92) RARP: 3 (7.9) | ND | All | Median (IQR): 18.5 (12–24) | 34 (89) | ND | Median (IQR): 196 (157–233) | ND | Median (IQR): 9 (6–10) | within 30 days 5 (13) | within 30 days 4 (11) | 0 | 21 (55) |
| Kim et al. [34] | 2022 | cRP | 32 | ND | ND | ND | ND | 20 (62) | Median (IQR): 200 (100–400) | Median (IQR): 225 (198–312) | ND | ND | ND | 6% | ND | 20 (66) |
| Takagi et al. [43] | 2022 | cRP | 12 | RARP | None | None | ND | ND | Median (IQR): 23 (7–45) | Median (IQR): 85 (70–112) * | ND | ND | 0 | 0 | 0 | 1 (8.3) |
| Author | Year | Comparisons | No. of Pts. | Approach of cRP, n (%) | Nerve Sparing | Pre-RP Urinary Function, n (%) | Continence during Follow-Up, n (%) | Pre-cRP Erectile Function, n (%) | Erectile Function at Last Follow-Up, n (%) |
|---|---|---|---|---|---|---|---|---|---|
| Heidenreich et al. [33] | 2015 | cRP | 23 | Open RP | ND | ND | at last follow-up 0 pads/day: 13 (57) 0–1 pads/day: 21 (91) 2–4 pads/day: 2 (8.7) | ND | ND |
| Poelaert et al. [40] (LoMP trial) | 2017 | cRP | 17 | Open: 1 RARP: 16 | None | ND | at 3 mo. Continent and no local symptoms: 12 (71) | ND | ND |
| No cRP | 29 | NA | at 3 mo. Continent and no local symptoms: 13 (45) | ||||||
| Moschini et al. [39] | 2017 | cRP | 31 | Open RP | ND | ND | at 90 days 0 pads/day: 24 (77) 1–2 pads/day: 2 (6.5) >2 pads/day: 5 (16) | ND | ND |
| Buelens et al. [29] (LoMP trial) | 2022 | cRP | 40 | Open: 2 RARP: 38 | None | ND | Continent (0–1 pads/day) at 1 yr: 31 (79) at last follow-up: 35 (88) | ND | ND |
| Sooriakumaran et al. [41] (TRoMbone) | 2022 | cRP | 25 | RARP | ND | Incontinence: 0 | Incontinence at 1 mo.: 9 (37.5%) Incontinence at 3 mo.: 6 (25%) Incontinence at 6 mo.: 4 (17%) | IIEF-5 score (median, IQR): 13.0 (5.5–21.0) | IIEF-5 score at 3 mo. (median, IQR): 5.0 (5.0–6.0) |
| No cRP | 25 | NA | Incontinence: 0 | ND | IIEF-5 score (median, IQR): 18.5 (10.0–21.0) | IIEF-5 score at 3 mo. (median, IQR): 5.0 (5.0–12.0) | |||
| Knipper et al. [35] | 2020 | cRP | 78 | Open RP | ND | ND | at 1 yr 0 pads/day: 20 (53) 0–1 pads/day: 28 (74) 2 pads/day: 2 (5) | ND | ND |
| Dai et al. [31] | 2022 | cRP | 85 | Open RP: 68 (80) RARP: 17 (20) | ND | ND | at 1 yr 0 pads/day: 78 (92) at 2 yrs 0 pads/day: 81 (95) | ND | ND |
| Chaloupka et al. [30] | 2021 | cRP | 79 | Open: 69 (87) RARP:10 (13) | 13 (17) | ICIQ-SF score (mean ± SD): 2.3 ± 4.6 | at 25 mo. ICIQ-SF score (mean ± SD): 6.4 ± 5.7 Daily pad usage (mean ± SD): 1.6 ± 2.5 Continence recovery: 66% | IIEF-5 score (mean ± SD): 8.5 ± 10.2 IIEF-5 score > 18: 26.8% | IIEF-5 score (mean ± SD): 1.3 ± 4.2 IIEF-5 score > 18: 2.0% |
| RP | 332 | Open: 116 (35) RARP: 216 (65) | 183 (55) | ICIQ-SF score (mean ± SD): 1.1 ± 2.6 | at 25 mo. ICIQ-SF score (mean ± SD): 6.4 ± 5.2 Daily pad usage (mean ± SD): 1.2 ± 1.7 Continence recovery: 72% | IIEF-5 score (mean ± SD): 11.3 ± 9.9 IIEF-5 score > 18: 37.2% | IIEF-5 score (mean ± SD): 3.5 ± 6.2 IIEF-5 score > 18: 6.8% | ||
| Gandaglia et al. [45] | 2017 | cRP | 11 | Open | ND | ND | at 90 days 0 pads/day: 3 (27) | ND | ND |
| Heidenreich et al. [32] | 2018 | cRP | 113 | Open: 104 (92) RARP: 9 (8) | ND | ND | at 12 mo. 0 pads/day: 68% 1–2 pads/day: 18% >2 pads/day: 14% | ND | ND |
| Babst et al. [28] | 2021 | cRP | 38 | Open: 35 (92) RARP: 3 (7.9) | ND | ND | 0–1 pads/day at 1 mo.: 87% at 6 mo.: 92% at 12 mo.: 88% | ND | ND |
| Takagi et al. [43] | 2022 | cRP | 12 | RARP | None | ND | at 24 mo.: >2 pads/day: 1 (8.3) | ND | ND |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanagisawa, T.; Rajwa, P.; Kawada, T.; Bekku, K.; Laukhtina, E.; Deimling, M.v.; Majdoub, M.; Chlosta, M.; Karakiewicz, P.I.; Heidenreich, A.; et al. An Updated Systematic and Comprehensive Review of Cytoreductive Prostatectomy for Metastatic Prostate Cancer. Curr. Oncol. 2023, 30, 2194-2216. https://doi.org/10.3390/curroncol30020170
Yanagisawa T, Rajwa P, Kawada T, Bekku K, Laukhtina E, Deimling Mv, Majdoub M, Chlosta M, Karakiewicz PI, Heidenreich A, et al. An Updated Systematic and Comprehensive Review of Cytoreductive Prostatectomy for Metastatic Prostate Cancer. Current Oncology. 2023; 30(2):2194-2216. https://doi.org/10.3390/curroncol30020170
Chicago/Turabian StyleYanagisawa, Takafumi, Pawel Rajwa, Tatsushi Kawada, Kensuke Bekku, Ekaterina Laukhtina, Markus von Deimling, Muhammad Majdoub, Marcin Chlosta, Pierre I. Karakiewicz, Axel Heidenreich, and et al. 2023. "An Updated Systematic and Comprehensive Review of Cytoreductive Prostatectomy for Metastatic Prostate Cancer" Current Oncology 30, no. 2: 2194-2216. https://doi.org/10.3390/curroncol30020170