Intensive Follow-Up Program and Oncological Outcomes of Biliary Tract Cancer Patients after Curative-Intent Surgery: A Twenty-Year Experience in a Single Tertiary Medical Center

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
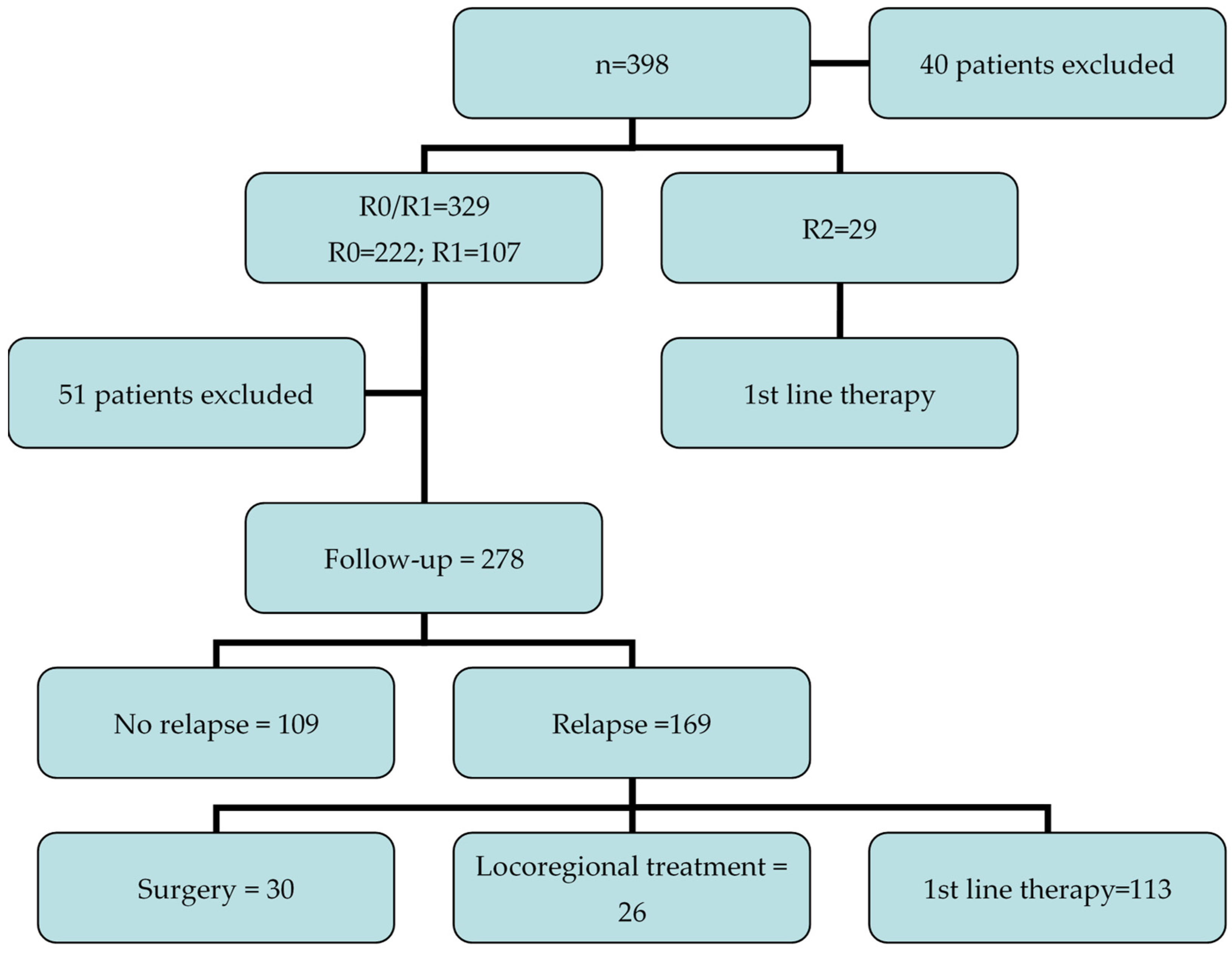
2.1. Patients
2.2. Inclusion Criteria
- -
- More than 18 years of age;
- -
- Surgical resection for primary BTC (iCCA, eCCA, and GBC);
- -
- Pathologically verified R0 or R1 resection.
2.3. Exclusion Criteria
- -
- R2 resection;
- -
- Known metastases;
- -
- Synchronous cancer;
- -
- Concurrent participation in other studies that affect the frequency and content of the follow-up program.
2.4. The Follow-Up Program
2.5. Statistical Analysis
3. Results
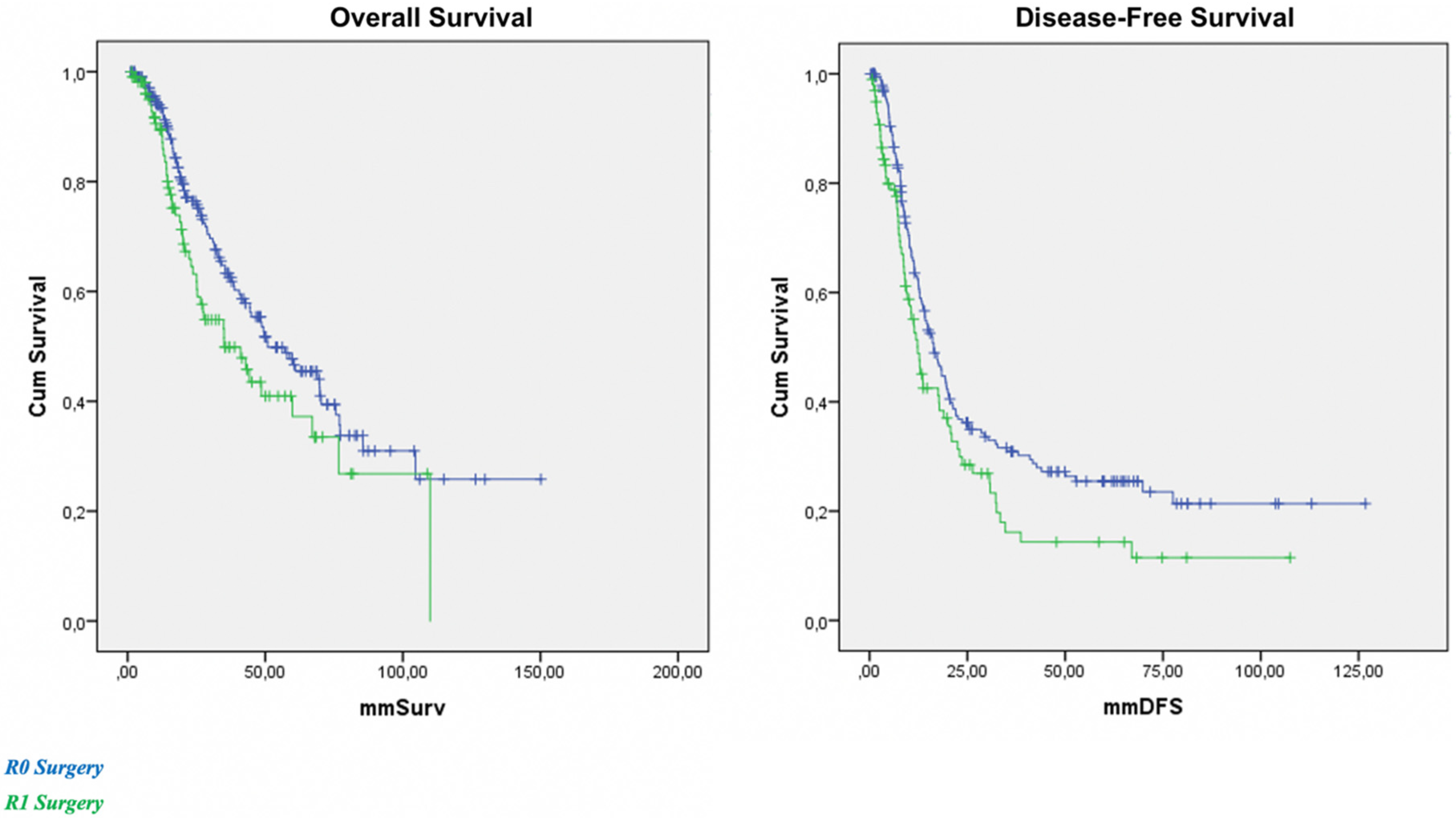
Overall Survival and Disease-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rizvi, S.; Gores, G.J. Pathogenesis, diagnosis, and management of cholangiocarcinoma. Gastroenterology 2013, 145, 1215–1229. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forner, A.; Vidili, G.; Rengo, M.; Bujanda, L.; Ponz-Sarvisé, M.; Lamarca, A. Clinical presentation, diagnosis and staging of cholangiocarcinoma. Liver Int. 2019, 39 (Suppl. S1), 98–107. [Google Scholar] [CrossRef] [Green Version]
- Nooijen, L.E.; Banales, J.M.; de Boer, M.T.; Braconi, C.; Folseraas, T.; Forner, A.; Holowko, W.; Hoogwater, F.J.H.; Klümpen, H.J.; Groot Koerkamp, B.; et al. Impact of Positive Lymph Nodes and Resection Margin Status on the Overall Survival of Patients with Resected Perihilar Cholangiocarcinoma: The ENSCCA Registry. Cancers 2022, 14, 2389. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Bridgewater, J.A.; Goodman, K.A.; Kalyan, A.; Mulcahy, M.F. Biliary Tract Cancer: Epidemiology, Radiotherapy, and Molecular Profiling. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e194–e203. [Google Scholar] [CrossRef] [PubMed]
- DeOliveira, M.L.; Cunningham, S.C.; Cameron, J.L.; Kamangar, F.; Winter, J.M.; Lillemoe, K.D.; Choti, M.A.; Yeo, C.J.; Schulick, R.D. Cholangiocarcinoma: Thirty-one-year experience with 564 patients at a single institution. Ann. Surg. 2007, 245, 755–762. [Google Scholar] [CrossRef]
- Schweitzer, N.; Fischer, M.; Kirstein, M.M.; Berhane, S.; Kottas, M.; Sinn, M.; Gonzalez-Carmona, M.A.; Balta, Z.; Weismüller, T.J.; Strassburg, C.P.; et al. Risk estimation for biliary tract cancer: Development and validation of a prognostic score. Liver Int. 2017, 37, 1852–1860. [Google Scholar] [CrossRef]
- Rizzo, A.; Brandi, G. Pitfalls, challenges, and updates in adjuvant systemic treatment for resected biliary tract cancer. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 547–554. [Google Scholar] [CrossRef]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Brandi, G. BILCAP trial and adjuvant capecitabine in resectable biliary tract cancer: Reflections on a standard of care. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 483–485. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Zhu, A.X.; Fuchs, C.S.; Brooks, G.A. Forty-year trends in cholangiocarcinoma incidence in the US: Intrahepatic disease on the rise. Oncologist 2016, 21, 594–599. [Google Scholar] [CrossRef] [Green Version]
- Sanoyan, D.A.; McNamara, M.G.; Lamarca, A.; Valle, J.W. Adjuvant chemotherapy in biliary tract cancer: State of the art and future perspectives. Curr. Opin. Oncol. 2020, 32, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Kim, R. Adjuvant therapy for resected extrahepatic cholangiocarcinoma: A review of the literature and future directions. Cancer Treat. Rev. 2009, 35, 322–327. [Google Scholar] [CrossRef]
- Lamarca, A.; Edeline, J.; Mcnamara, M.; Hubner, R.A.; Nagino, M.; Bridgewater, J.; Primrose, J.; Valle, J.W. Current standards and future perspectives in adjuvant treatment for biliary tract cancers. Cancer Treat. Rev. 2020, 84, 101936. [Google Scholar] [CrossRef]
- Brindley, P.J.; Bachini, M.; Ilyas, S.I.; Khan, S.A.; Loukas, A.; Sirica, A.E.; Teh, B.T.; Wongkham, S.; Gores, G.J. Cholangiocarcinoma. Nat. Rev. Dis. Prim. 2021, 7, 65. [Google Scholar] [CrossRef]
- Khan, A.S.; Dageforde, L.A. Cholangiocarcinoma. Surg. Clin. N. Am. 2019, 99, 315–335. [Google Scholar] [CrossRef]
- Rizzo, A.; Brandi, G. First-line Chemotherapy in Advanced Biliary Tract Cancer Ten Years After the ABC-02 Trial: “And Yet It Moves!”. Cancer Treat. Res. Commun. 2021, 27, 100335. [Google Scholar] [CrossRef]
- Kendall, T.; Verheij, J.; Gaudio, E.; Evert, M.; Guido, M.; Goeppert, B.; Carpino, G. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019, 39 (Suppl. S1), 7–18. [Google Scholar] [CrossRef] [Green Version]
- Waseem, D.; Tushar, P. Intrahepatic, Perihilar and Distal Cholangiocarcinoma: Management and Outcomes. Ann. Hepatol. 2017, 16, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Kim, Y.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; et al. Management and Outcomes of Patients with Recurrent Intrahepatic Cholangiocarcinoma Following Previous Curative-Intent Surgical Resection. Ann. Surg. Oncol. 2016, 23, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Langella, S.; Russolillo, N.; Ossola, P.; Luzzi, A.-P.; Casella, M.; Tesoriere, R.L.; Ferrero, A. Recurrence after Curative Resection for Intrahepatic Cholangiocarcinoma: How to Predict the Chance of Repeat Hepatectomy? J. Clin. Med. 2021, 10, 2820. [Google Scholar] [CrossRef] [PubMed]
- Andreou, A.; Brouquet, A.; Abdalla, E.K.; Aloia, T.A.; Curley, S.A.; Vauthey, J.-N. Repeat hepatectomy for recurrent colorectal liver metastases is associated with a high survival rate. HPB 2011, 13, 774–782. [Google Scholar] [CrossRef] [Green Version]
- Battula, N.; Tsapralis, D.; Mayer, D.; Isaac, J.; Muiesan, P.; Sutcliffe, R.P.; Bramhall, S.; Mirza, D.; Marudanayagam, R. Repeat liver resection for recurrent colorectal metastases: A single-centre, 13-year experience. HPB 2014, 16, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Midorikawa, Y.; Takayama, T.; Moriguchi, M.; Yagi, R.; Yamagishi, S.; Nakayama, H.; Aramaki, O.; Yamazaki, S.; Tsuji, S.; Higaki, T. Liver Resection Versus Embolization for Recurrent Hepatocellular Carcinoma. World J. Surg. 2020, 44, 232–240. [Google Scholar] [CrossRef]
- Sirica, A.E.; Gores, G.J.; Groopman, J.D.; Selaru, F.M.; Strazzabosco, M.; Wang, X.W.; Zhu, A.X. Intrahepatic Cholangiocarcinoma: Continuing Challenges and Translational Advances. Hepatology 2019, 69, 1803–1815. [Google Scholar] [CrossRef]
- Mukkamalla, S.K.R.; Naseri, H.M.; Kim, B.M.; Katz, S.C.; Armenio, V.A. Trends in Incidence and Factors Affecting Survival of Patients with Cholangiocarcinoma in the United States. J. Natl. Compr. Cancer Netw. 2018, 16, 370–376. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients | (n = 278) |
| Sex | |
| Male | 108 (38.9%) |
| Female | 170 (61.1%) |
| Median age | |
| 63 years, range 37–85 | |
| Primary tumor site | |
| iCCA | 116 (41.7%) |
| eCCA | 126 (45.4%) |
| GBC | 36 (12.9%) |
| Grading | |
| G1 | 24 (8.6%) |
| G2 | 136 (48.9%) |
| G3 | 102 (36.8%) |
| Not available | 16 (5.7%) |
| Vascular infiltration | |
| Yes | 96 (24.8%) |
| No | 39 (14.0%) |
| Not available | 143 (51.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, A.; Carloni, R.; Frega, G.; Palloni, A.; Di Federico, A.; Ricci, A.D.; De Luca, R.; Tavolari, S.; Brandi, G. Intensive Follow-Up Program and Oncological Outcomes of Biliary Tract Cancer Patients after Curative-Intent Surgery: A Twenty-Year Experience in a Single Tertiary Medical Center. Curr. Oncol. 2022, 29, 5084-5090. https://doi.org/10.3390/curroncol29070402
Rizzo A, Carloni R, Frega G, Palloni A, Di Federico A, Ricci AD, De Luca R, Tavolari S, Brandi G. Intensive Follow-Up Program and Oncological Outcomes of Biliary Tract Cancer Patients after Curative-Intent Surgery: A Twenty-Year Experience in a Single Tertiary Medical Center. Current Oncology. 2022; 29(7):5084-5090. https://doi.org/10.3390/curroncol29070402
Chicago/Turabian StyleRizzo, Alessandro, Riccardo Carloni, Giorgio Frega, Andrea Palloni, Alessandro Di Federico, Angela Dalia Ricci, Raffaele De Luca, Simona Tavolari, and Giovanni Brandi. 2022. "Intensive Follow-Up Program and Oncological Outcomes of Biliary Tract Cancer Patients after Curative-Intent Surgery: A Twenty-Year Experience in a Single Tertiary Medical Center" Current Oncology 29, no. 7: 5084-5090. https://doi.org/10.3390/curroncol29070402