
The In Vitro Impact of Two Scaffold-Type Structure Dental Ceramics on the Viability, Morphology, and Cellular Migration of Pharyngeal Cancer Cells

 , , , ,
, , , ,  , and
, and 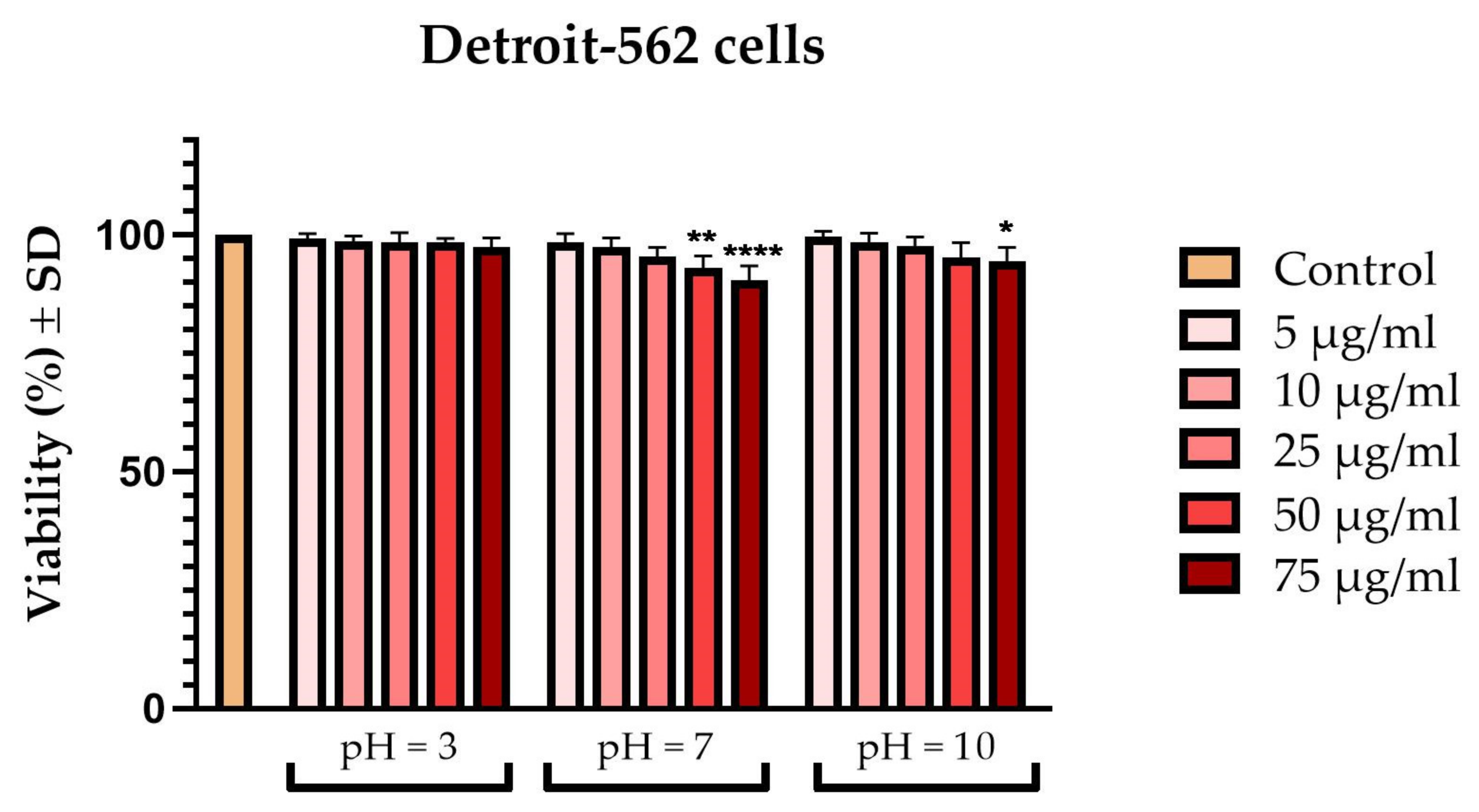{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Preparation of the Artificial Saliva
2.3. Storage Period of Samples in Artificial Saliva
2.4. Cell Culture
2.5. Cellular Viability Assessment
2.6. Cellular Morphology
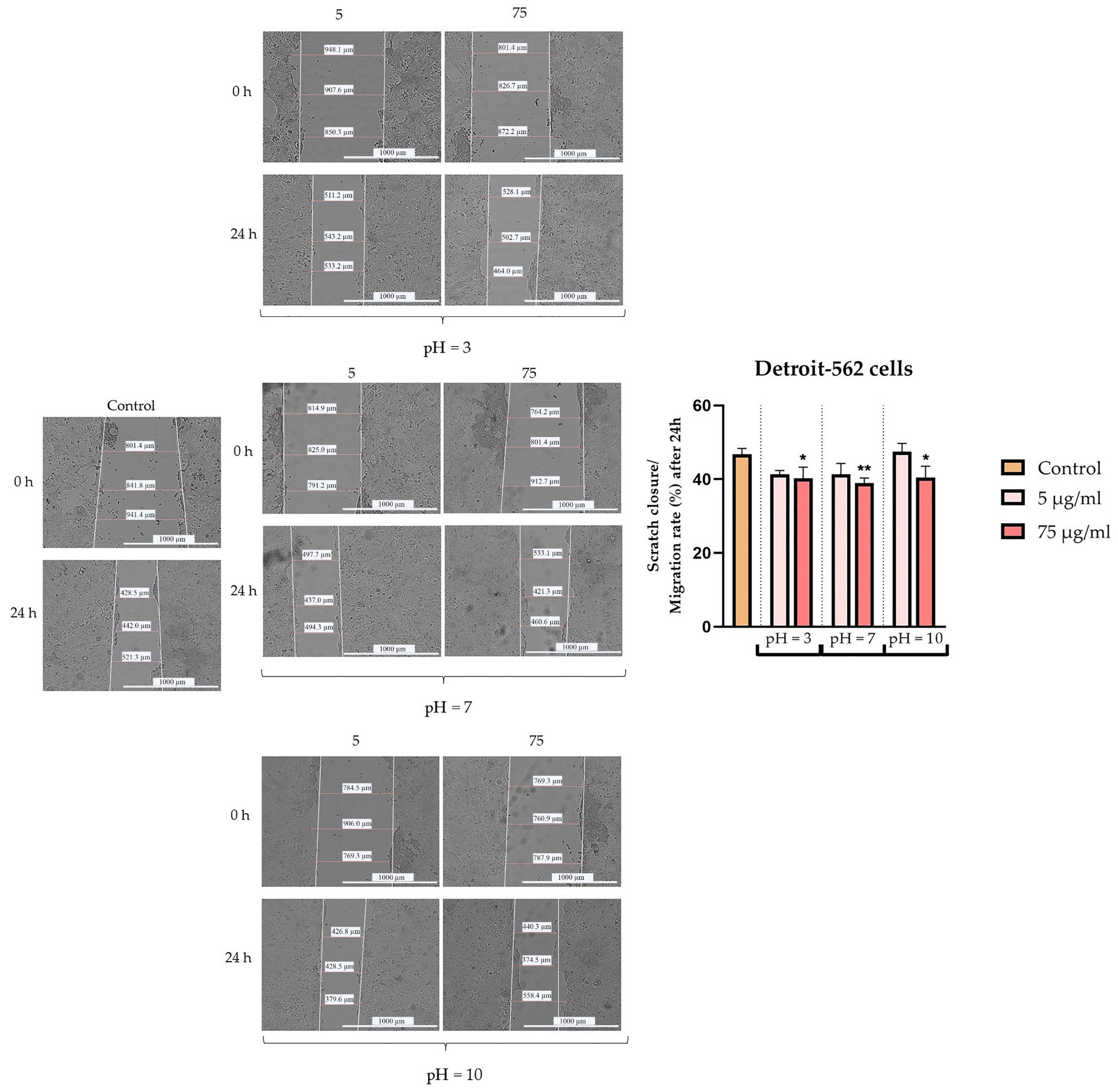
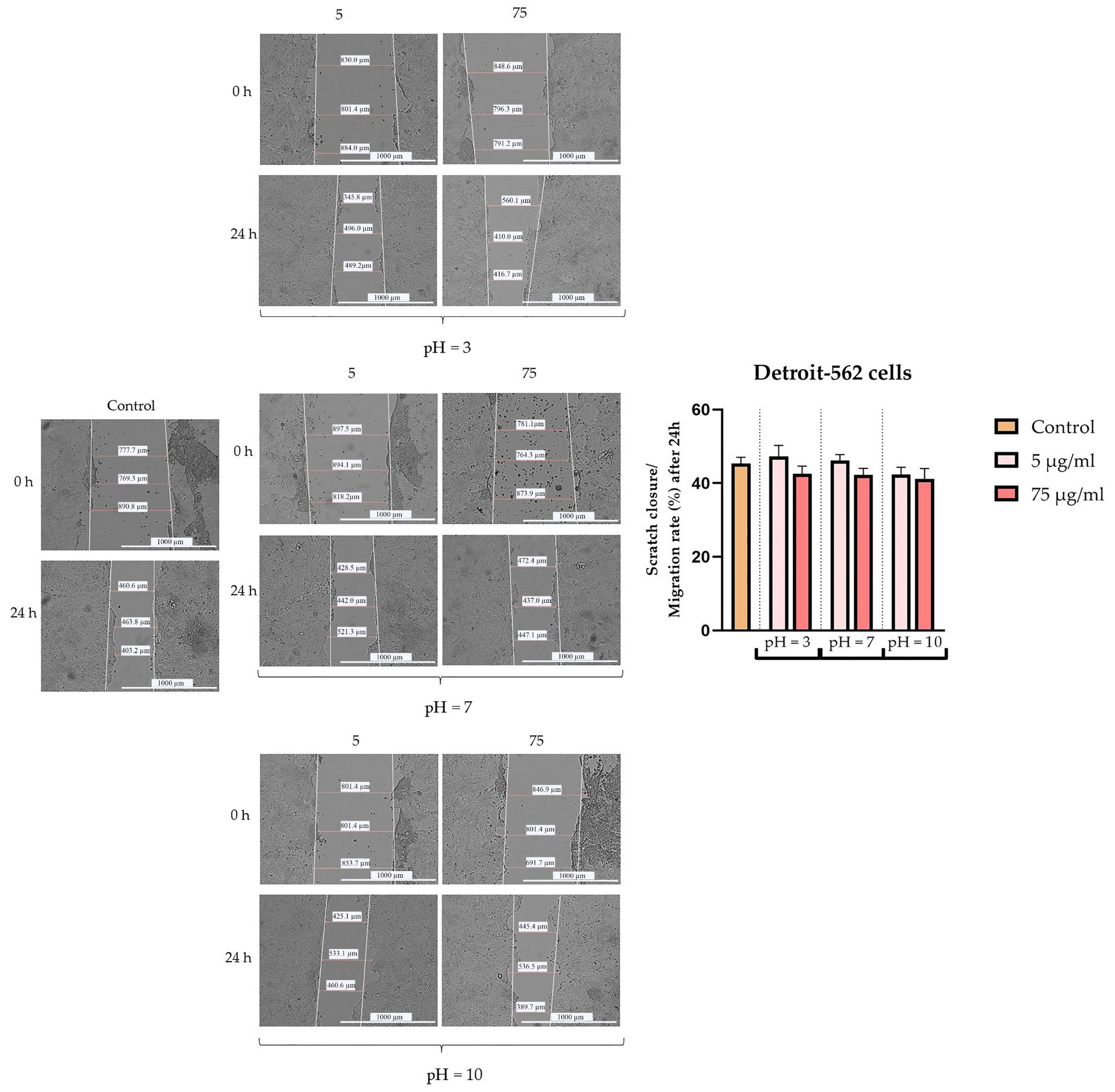
2.7. Wound-Healing Assay
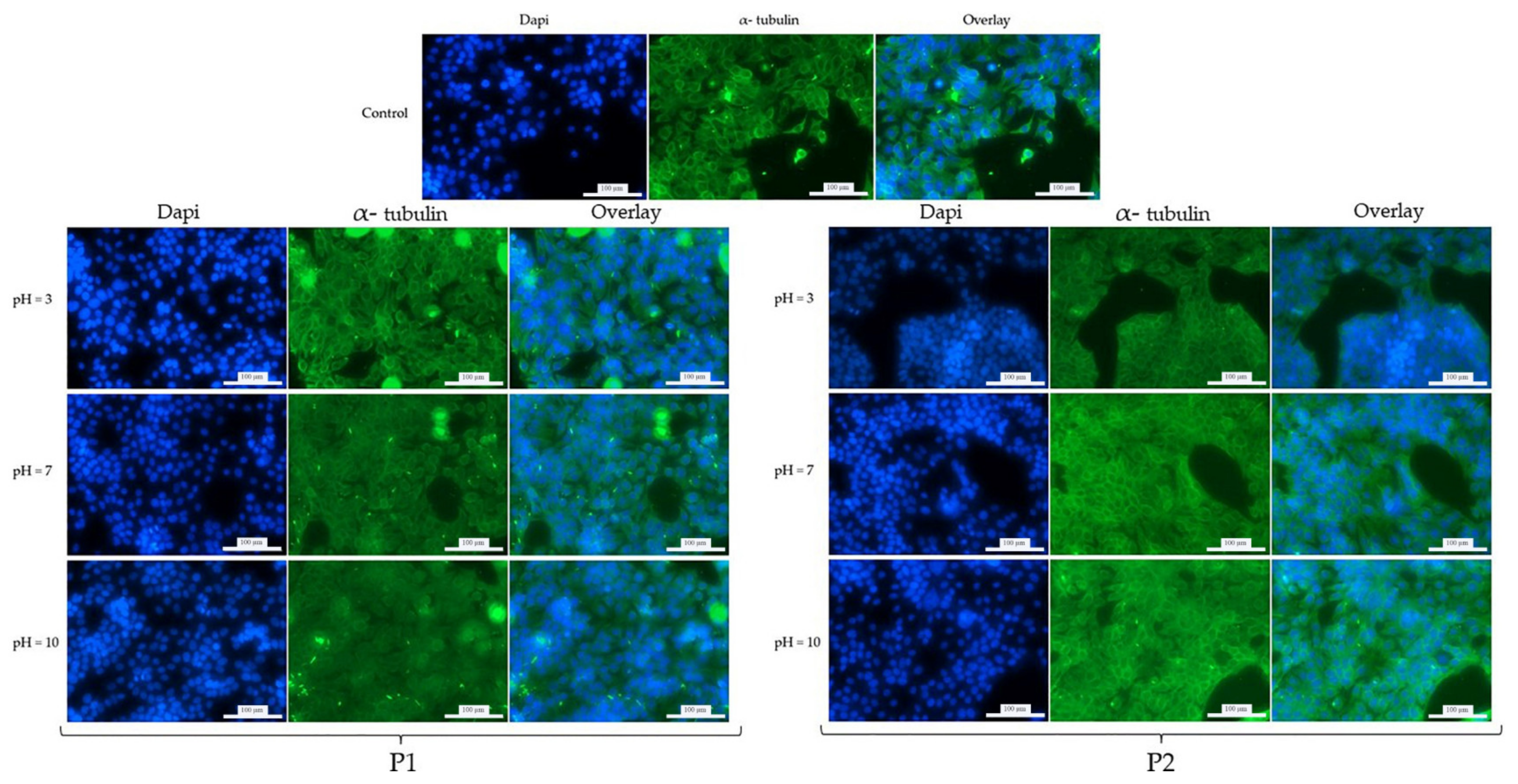
2.8. Fluorescence Immunocytochemistry
2.9. Statistical Analysis
3. Results
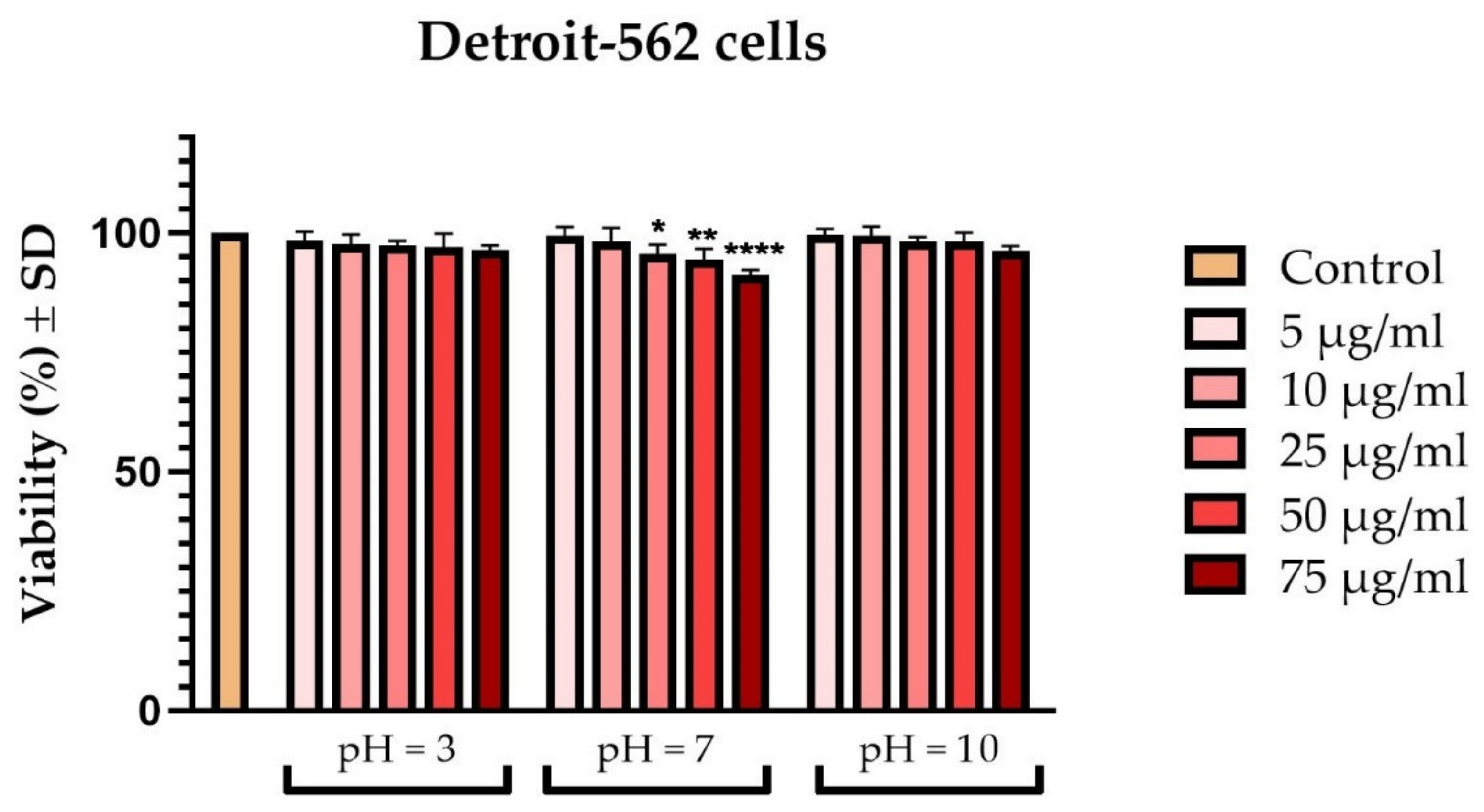
3.1. Cellular Viability Assessment
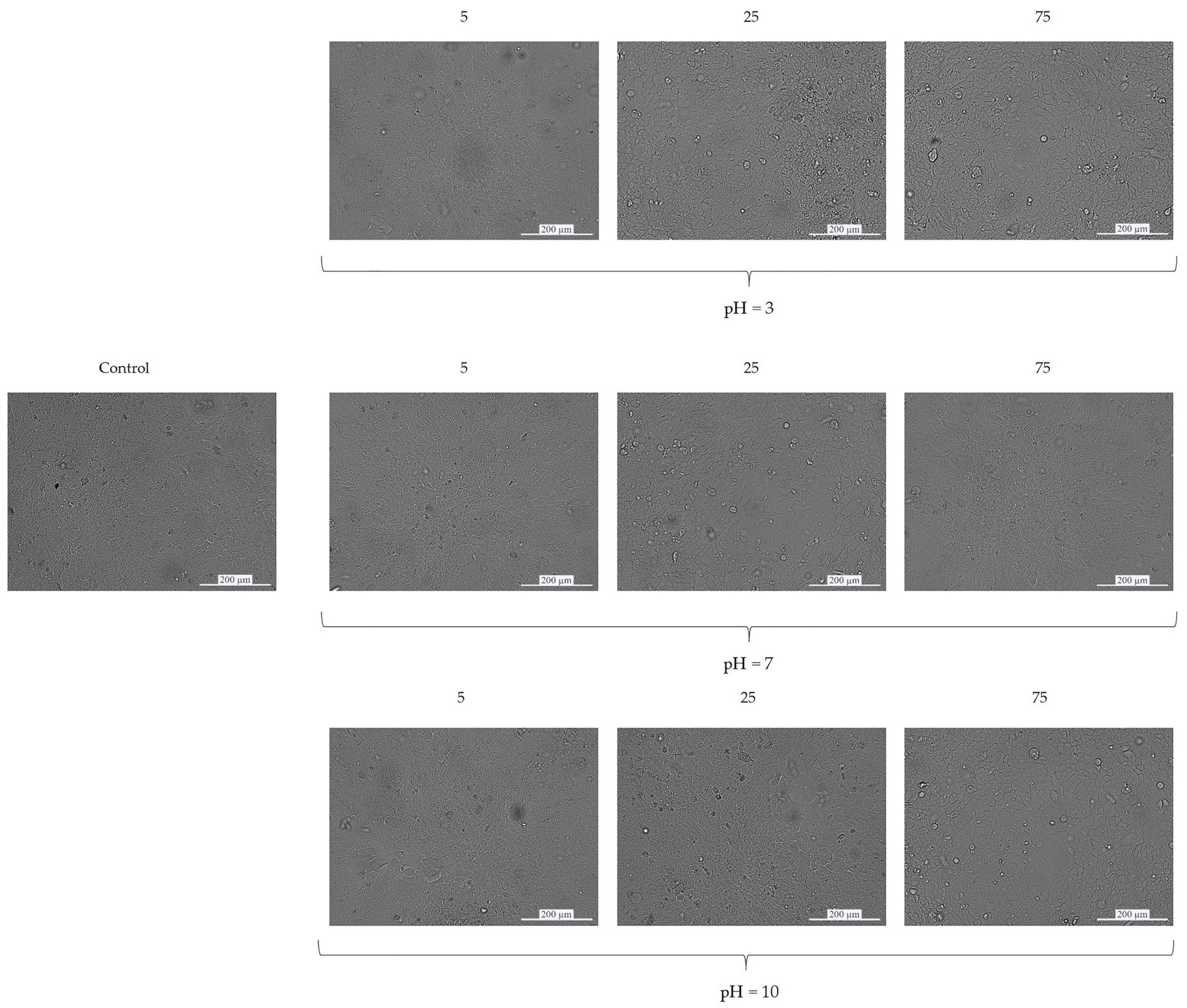
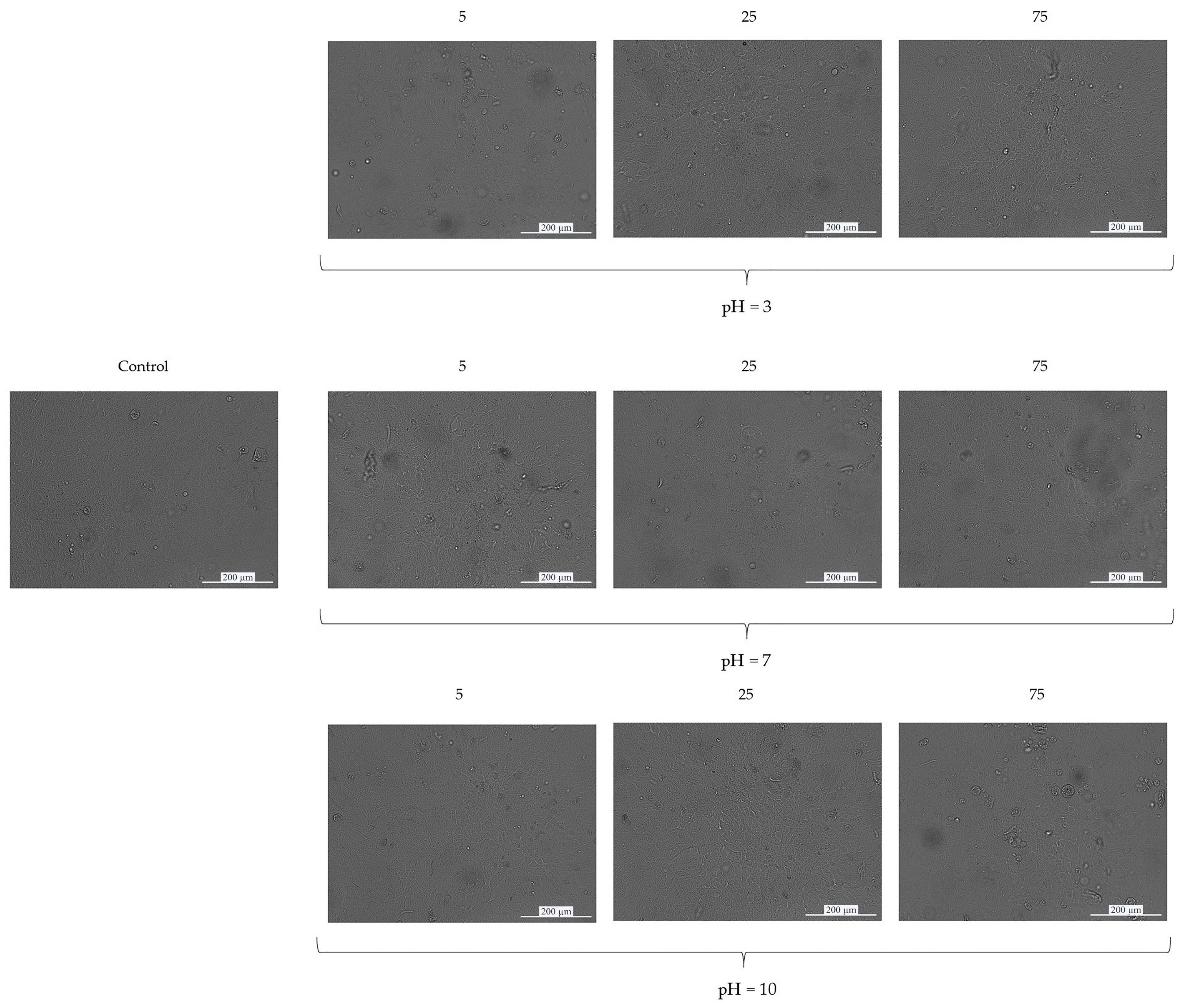
3.2. Cellular Morphology
3.3. Wound-Healing Assay
3.4. Fluorescence Immunocytochemistry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bajraktarova Valjakova, E.; Lj, G.; Korunoska-Stevkovska, V.; Gigovski, N.; Kapusevska, B.; Mijoska, A.; Bajevska, J.; Bajraktarova Misevska, C.; Grozdanov, A. Dental Ceramic Materials, Part I: Technological Development of All-Ceramic Dental Materials. Macedonian Stomatological Review. 2018, 41, 30–34. [Google Scholar]
- Zarone, F.; Russo, S.; Sorrentino, R. From Porcelain-Fused-to-Metal to Zirconia: Clinical and Experimental Considerations. Dent. Mater. 2011, 27, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Sharma, S.; Thapa, S.; Bhagat, M.; Kumar, V.; Sharma, V. Nanohydroxyapatite-, Gelatin-, and Acrylic Acid-Based Novel Dental Restorative Material. ACS Omega 2020, 5, 27886–27895. [Google Scholar] [CrossRef]
- Bajraktarova-Valjakova, E.; Korunoska-Stevkovska, V.; Kapusevska, B.; Gigovski, N.; Bajraktarova-Misevska, C.; Grozdanov, A. Contemporary Dental Ceramic Materials, A Review: Chemical Composition, Physical and Mechanical Properties, Indications for Use. Open Access Maced. J. Med. Sci. 2018, 6, 1742–1755. [Google Scholar] [CrossRef]
- Da Silva, L.H.; de Lima, E.; de Miranda, R.B.P.; Favero, S.S.; Lohbauer, U.; Cesar, P.F. Dental Ceramics: A Review of New Materials and Processing Methods. Braz. Oral Res. 2017, 31, e58. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.G.K.; Oh, J.-H. Recent Advances in Dental Implants. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 33. [Google Scholar] [CrossRef] [PubMed]
- Jané-Salas, E.; López-López, J.; Roselló-Llabrés, X.; Rodríguez-Argueta, O.-F.; Chimenos-Küstner, E. Relationship between Oral Cancer and Implants: Clinical Cases and Systematic Literature Review. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e23–e28. [Google Scholar] [CrossRef] [PubMed]
- Osman, R.B.; Swain, M.V. A Critical Review of Dental Implant Materials with an Emphasis on Titanium versus Zirconia. Materials 2015, 8, 932–958. [Google Scholar] [CrossRef] [PubMed]
- Ghassemi, T.; Shahroodi, A.; Ebrahimzadeh, M.H.; Mousavian, A.; Movaffagh, J.; Moradi, A. Current Concepts in Scaffolding for Bone Tissue Engineering. Arch. Bone Jt. Surg. 2018, 6, 90–99. [Google Scholar] [PubMed]
- Rodriguez-archilla, A.; Luna-berral, M. Oral Cancers Adjacent to Dental Implants: A Descriptive Study. Sci. Repos. 2019, 2, 1–7. [Google Scholar] [CrossRef]
- Irani, S. New Insights into Oral Cancer-Risk Factors and Prevention: A Review of Literature. Int. J. Prev. Med. 2020, 11, 202. [Google Scholar] [CrossRef]
- Alikhasi, M.; Kazemi, M.; Nokar, S.; Khojasteh, A.; Sheikhzadeh, S. Step-by-Step Full Mouth Rehabilitation of a Nasopharyngeal Carcinoma Patient with Tooth and Implant-Supported Prostheses: A Clinical Report. Contemp. Clin. Dent. 2011, 2, 256–260. [Google Scholar] [CrossRef]
- Jacobsen, C.; Kruse, A.; Lübbers, H.-T.; Zwahlen, R.; Studer, S.; Zemann, W.; Seifert, B.; Grätz, K.-W. Is Mandibular Reconstruction Using Vascularized Fibula Flaps and Dental Implants a Reasonable Treatment? Clin. Implant Dent. Relat. Res. 2014, 16, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Toneatti, D.J.; Graf, R.R.; Burkhard, J.P.; Schaller, B. Survival of Dental Implants and Occurrence of Osteoradionecrosis in Irradiated Head and Neck Cancer Patients: A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2021, 25, 5579–5593. [Google Scholar] [CrossRef] [PubMed]
- Asa’ad, F.; Pagni, G.; Pilipchuk, S.P.; Giannì, A.B.; Giannobile, W.V.; Rasperini, G. 3D-Printed Scaffolds and Biomaterials: Review of Alveolar Bone Augmentation and Periodontal Regeneration Applications. Int. J. Dent. 2016, 2016, 1239842. [Google Scholar] [CrossRef] [PubMed]
- McDermott, N.E.; Chuang, S.-K.; Woo, V.V.; Dodson, T.B. Complications of Dental Implants: Identification, Frequency, and Associated Risk Factors. Int. J. Oral Maxillofac. Implants 2003, 18, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.R.; Passi, D.; Singh, P.; Atri, M.; Mohan, S.; Sharma, A. Risks and Complications Associated with Dental Implant Failure: Critical Update. Natl. J. Maxillofac. Surg. 2020, 11, 14–19. [Google Scholar] [CrossRef]
- Thrivikraman, G.; Madras, G.; Basu, B. In Vitro/In Vivo Assessment and Mechanisms of Toxicity of Bioceramic Materials and Its Wear Particulates. RSC Adv. 2014, 4, 12763–12781. [Google Scholar] [CrossRef]
- Kis, A.M.; Macasoi, I.; Paul, C.; Radulescu, M.; Buzatu, R.; Watz, C.G.; Cheveresan, A.; Berceanu, D.; Pinzaru, I.; Dinu, S.; et al. Methotrexate and Cetuximab—Biological Impact on Non-Tumorigenic Models: In Vitro and In Ovo Assessments. Medicina 2022, 58, 167. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Jackson, L.; Epstein, J.B.; Migliorati, C.A.; Murphy, B.A. Dental Demineralization and Caries in Patients with Head and Neck Cancer. Oral Oncol. 2015, 51, 824–831. [Google Scholar] [CrossRef]
- In ‘t Veld, M.; Schulten, E.A.J.M.; Leusink, F.K.J. Immediate Dental Implant Placement and Restoration in the Edentulous Mandible in Head and Neck Cancer Patients: A Systematic Review and Meta-Analysis. Curr. Opin. Otolaryngol. Head Neck Surg. 2021, 29, 126. [Google Scholar] [CrossRef] [PubMed]
- Navalón, C.; Ros-Tárraga, P.; Murciano, A.; Velasquez, P.; Mazón, P.; Piedad, N. Easy Manufacturing of 3D Ceramic Scaffolds by the Foam Replica Technique Combined with Sol-Gel or Ceramic Slurry. Ceram. Int. 2019, 45, 18338–18346. [Google Scholar] [CrossRef]
- Qin, W.; Kolooshani, A.; Kolahdooz, A.; Saber-Samandari, S.; Khazaei, S.; Khandan, A.; Ren, F.; Toghraie, D. Coating the Magnesium Implants with Reinforced Nanocomposite Nanoparticles for Use in Orthopedic Applications. Colloids Surfaces A Physicochem. Eng. Asp. 2021, 621, 126581. [Google Scholar] [CrossRef]
- Li, X.; Saeed, S.-S.; Beni, M.H.; Morovvati, M.R.; Angili, S.N.; Toghraie, D.; Khandan, A.; Khan, A. Experimental Measurement and Simulation of Mechanical Strength and Biological Behavior of Porous Bony Scaffold Coated with Alginate-Hydroxyapatite for Femoral Applications. Compos. Sci. Technol. 2021, 214, 108973. [Google Scholar] [CrossRef]
- Khandan, A.; Abdellahi, M.; Ozada, N.; Ghayour, H. Study of the Bioactivity, Wettability and Hardness Behaviour of the Bovine Hydroxyapatite-Diopside Bio-Nanocomposite Coating. J. Taiwan Inst. Chem. Eng. 2016, 60, 538–546. [Google Scholar] [CrossRef]
- Fabricky, M.M.C.; Gabor, A.-G.; Milutinovici, R.A.; Watz, C.G.; Avram, Ș.; Drăghici, G.; Mihali, C.V.; Moacă, E.-A.; Dehelean, C.A.; Galuscan, A.; et al. Scaffold-Type Structure Dental Ceramics with Different Compositions Evaluated through Physicochemical Characteristics and Biosecurity Profiles. Materials 2021, 14, 2266. [Google Scholar] [CrossRef] [PubMed]
- ISO—ISO 10993-5:2009—Biological Evaluation of Medical Devices—Part 5: Tests for in Vitro Cytotoxicity. Available online: https://www.iso.org/standard/36406.html (accessed on 4 July 2022).
- Pytko-Polonczyk, J.; Jakubik, A.; Przeklasa-Bierowiec, A.; Muszynska, B. Artificial Saliva and Its Use in Biological Experiments. J. Physiol. Pharmacol. 2017, 68, 807–813. [Google Scholar]
- Romonti, D.E.; Gomez Sanchez, A.V.; Milošev, I.; Demetrescu, I.; Ceré, S. Effect of Anodization on the Surface Characteristics and Electrochemical Behaviour of Zirconium in Artificial Saliva. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 62, 458–466. [Google Scholar] [CrossRef]
- Lameira, D.P.; Buarque e Silva, W.A.; Andrade e Silva, F.; De Souza, G.M. Fracture Strength of Aged Monolithic and Bilayer Zirconia-Based Crowns. Biomed Res. Int. 2015, 2015, 418641. [Google Scholar] [CrossRef] [PubMed]
- DA Silva, M.A.B.; Vitti, R.P.; Sinhoreti, M.A.C.; Consani, R.L.X.; da Silva-Júnior, J.G.; Tonholo, J. Effect of Alcoholic Beverages on Surface Roughness and Microhardness of Dental Composites. Dent. Mater. J. 2016, 35, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Alshali, R.Z.; Salim, N.A.; Satterthwaite, J.D.; Silikas, N. Long-Term Sorption and Solubility of Bulk-Fill and Conventional Resin-Composites in Water and Artificial Saliva. J. Dent. 2015, 43, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Pulikkottil, V.J.; Chidambaram, S.; Bejoy, P.U.; Femin, P.K.; Paul, P.; Rishad, M. Corrosion Resistance of Stainless Steel, Nickel-Titanium, Titanium Molybdenum Alloy, and Ion-Implanted Titanium Molybdenum Alloy Archwires in Acidic Fluoride-Containing Artificial Saliva: An in Vitro Study. J. Pharm. Bioallied Sci. 2016, 8, S96–S99. [Google Scholar] [CrossRef]
- Yan, M.; Wei, C.-K.; Lin, Y.-Y.; Hu, S.-W.; Ding, S.-J. Impact Behavior of Three Notched All-Ceramic Restorations after Soaking in Artificial Saliva. Materials 2015, 8, 4479–4490. [Google Scholar] [CrossRef] [PubMed]
- Milleding, P.; Haraldsson, C.; Karlsson, S. Ion Leaching from Dental Ceramics during Static in Vitro Corrosion Testing. J. Biomed. Mater. Res. Off. J. Soc. Biomater. Japanese Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2002, 61, 541–550. [Google Scholar]
- Esquivel-Upshaw, J.F.; Dieng, F.Y.; Clark, A.E.; Neal, D.; Anusavice, K.J. Surface Degradation of Dental Ceramics as a Function of Environmental PH. J. Dent. Res. 2013, 92, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Tomozawa, M.; Oka, Y.; Wahl, J.M. Glass Surface Cracks Caused by Alkaline Solution Containing an Alkaline—Earth Element. J. Am. Ceram. Soc. 1981, 64, C-32. [Google Scholar] [CrossRef]
- Pinto, M.M.; Cesar, P.F.; Rosa, V.; Yoshimura, H.N. Influence of PH on Slow Crack Growth of Dental Porcelains. Dent. Mater. 2008, 24, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, N.Z.; El Guindy, J.; Zamzam, M. Effect of Artificial Saliva Storage on Microhardness and Fracture Toughness of a Hydrothermal Glass-Ceramic. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2009, 18, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Lakhloufi, S.; Labjar, H.; El Hamdouni, Y.; Bouhouche, I.; Dahrouch, A.; Serghini-Idriissi, M.; Lotfi, E.M.; El Mahi, M.; El Yamani, A.; El Hajjaji, S.; et al. Electrochemical Behavior and Surface Characterization of Dental Materials in Artificial Salivary. Mater. Today Proc. 2020, 31, S141–S148. [Google Scholar] [CrossRef]
- Inas Mohammed, D.Z.N.A. An Evaluation of the Effect of Artificial Saliva with Different PH on Shear Bond Strength of Veneering Ceramic to Metal and World Journal of Pharmaceutical Research an Evaluation of the Effect of Artificial Saliva with Different PH on Shear Bond Strength. World J. Pharm. Res. 2019, 6, 30–44. [Google Scholar] [CrossRef]
- Kim, R.H.-K.; Yang, P.; Sung, E.C. Managing Intraoral Lesions in Oral Cancer Patients in a General Dental Practice: An Overview. J. Calif. Dent. Assoc. 2016, 44, 85–92. [Google Scholar] [PubMed]
- Moore, S.R.; Johnson, N.W.; Pierce, A.M.; Wilson, D.F. The Epidemiology of Tongue Cancer: A Review of Global Incidence. Oral Dis. 2000, 6, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Anusavice, K.J. Degradability of Dental Ceramics. Adv. Dent. Res. 1992, 6, 82–89. [Google Scholar] [CrossRef]
- Wang, X.; Xia, Y.; Liu, L.; Liu, M.; Gu, N.; Guang, H.; Zhang, F. Comparison of MTT Assay, Flow Cytometry, and RT—PCR in the Evaluation of Cytotoxicity of Five Prosthodontic Materials. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 95, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Sjögren, G.; Sletten, G.; Dahl, J.E. Cytotoxicity of Dental Alloys, Metals, and Ceramics Assessed by Millipore Filter, Agar Overlay, and MTT Tests. J. Prosthet. Dent. 2000, 84, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Messer, R.L.W.; Lockwood, P.E.; Wataha, J.C.; Lewis, J.B.; Norris, S.; Bouillaguet, S. In Vitro Cytotoxicity of Traditional versus Contemporary Dental Ceramics. J. Prosthet. Dent. 2003, 90, 452–458. [Google Scholar] [CrossRef]
- Aseervatham, J. Cytoskeletal Remodeling in Cancer. Biology 2020, 9, 385. [Google Scholar] [CrossRef] [PubMed]
- Tassin, M.; Bonte, E.; Loison-Robert, L.S.; Nassif, A.; Berbar, T.; Le Goff, S.; Berdal, A.; Sadoun, M.; Fournier, B.P.J. Effects of High-Temperature-Pressure Polymerized Resin-Infiltrated Ceramic Networks on Oral Stem Cells. PLoS ONE 2016, 11, e0155450. [Google Scholar] [CrossRef]
- Martins, C.S.; Ferraz, E.P.; De Castro-Raucci, L.M.S.; Teixeira, L.N.; Maximiano, W.M.A.; Rosa, A.L.; De Oliveira, P.T. Changes in Actin and Tubulin Expression in Osteogenic Cells Cultured on Bioactive Glass-Based Surfaces. Microsc. Res. Tech. 2015, 78, 1046–1053. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabricky, M.M.C.; Racea, R.C.; Macasoi, I.; Pinzaru, I.; Sinescu, C.; Manea, H.C.; Rusu, L.-C.; Stoian, D.; Buzatu, R.; Dinu, S. The In Vitro Impact of Two Scaffold-Type Structure Dental Ceramics on the Viability, Morphology, and Cellular Migration of Pharyngeal Cancer Cells. Coatings 2022, 12, 1212. https://doi.org/10.3390/coatings12081212
Fabricky MMC, Racea RC, Macasoi I, Pinzaru I, Sinescu C, Manea HC, Rusu L-C, Stoian D, Buzatu R, Dinu S. The In Vitro Impact of Two Scaffold-Type Structure Dental Ceramics on the Viability, Morphology, and Cellular Migration of Pharyngeal Cancer Cells. Coatings. 2022; 12(8):1212. https://doi.org/10.3390/coatings12081212
Chicago/Turabian StyleFabricky, Mihai M. C., Robert Cosmin Racea, Ioana Macasoi, Iulia Pinzaru, Cosmin Sinescu, Horatiu Cristian Manea, Laura-Cristina Rusu, Dana Stoian, Roxana Buzatu, and Stefania Dinu. 2022. "The In Vitro Impact of Two Scaffold-Type Structure Dental Ceramics on the Viability, Morphology, and Cellular Migration of Pharyngeal Cancer Cells" Coatings 12, no. 8: 1212. https://doi.org/10.3390/coatings12081212