
Variation in Fatty Acid Synthase, Ki67 and p53 Esophageal Mucosa Expressions in Barrett’s Esophagus Patients Treated for One Year with Two Esomeprazole Different Regimens

Abstract
:1. Background
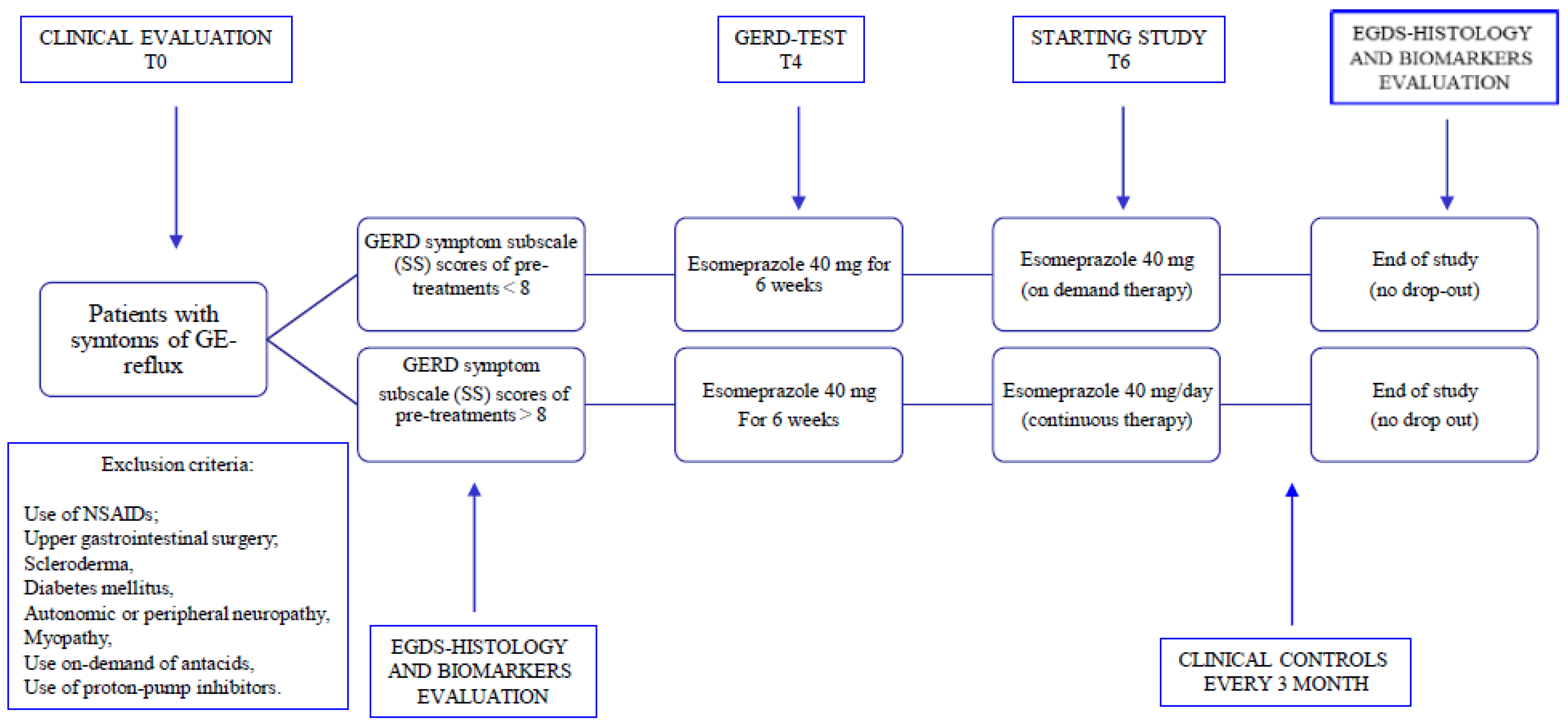
2. Patients and Methods
2.1. Patients
2.2. Endoscopy
2.3. Histology
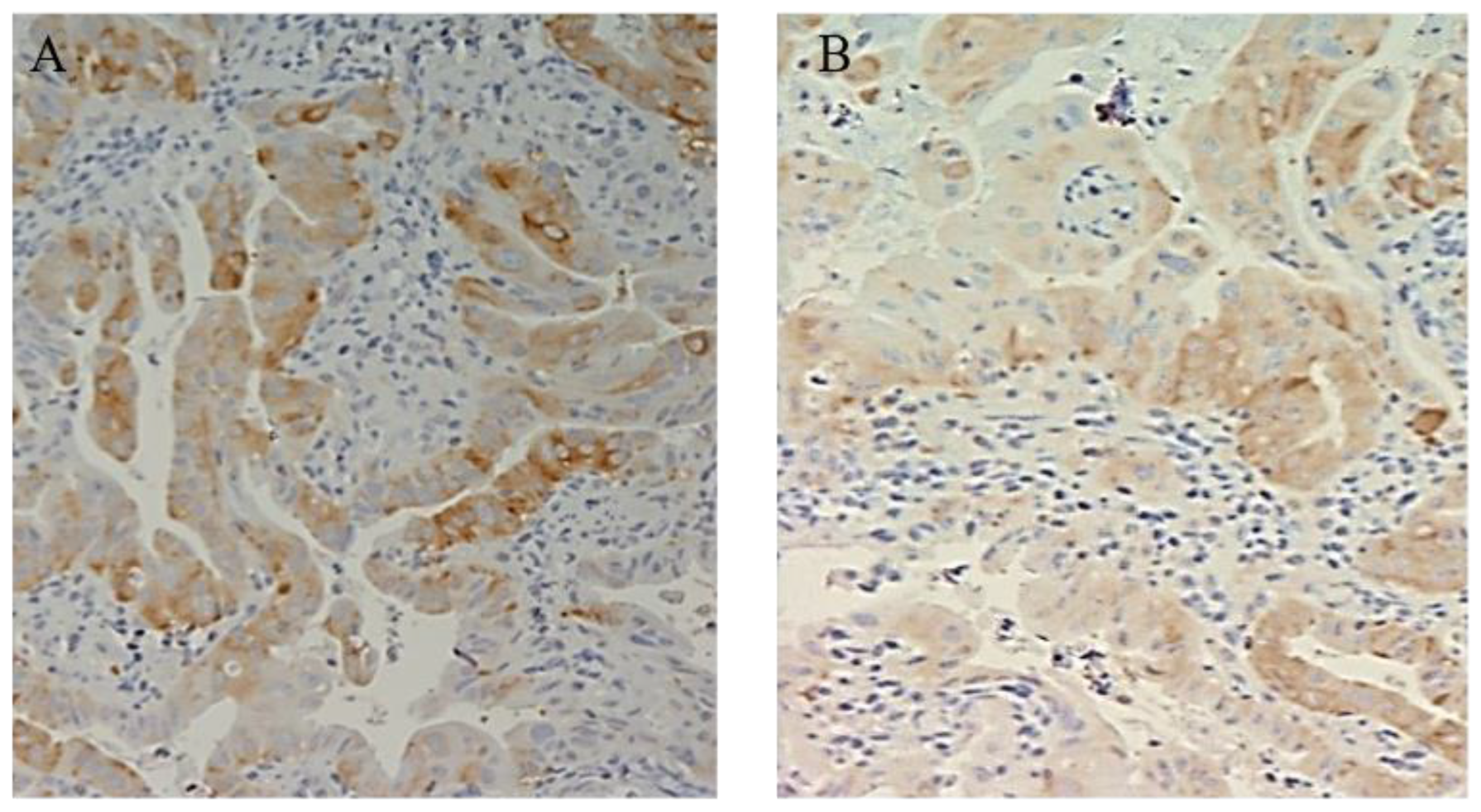
2.4. Determination of FAS Expression
2.5. Determination of Ki67 Expression
2.6. Determination of p53 Expression
2.7. Determination and Evaluation of the Degree of p53, Ki67, and FAS Expression
2.8. Statistical Analysis
3. Results
3.1. Patient’s Characteristics
3.2. Immunohistochemical Evaluation
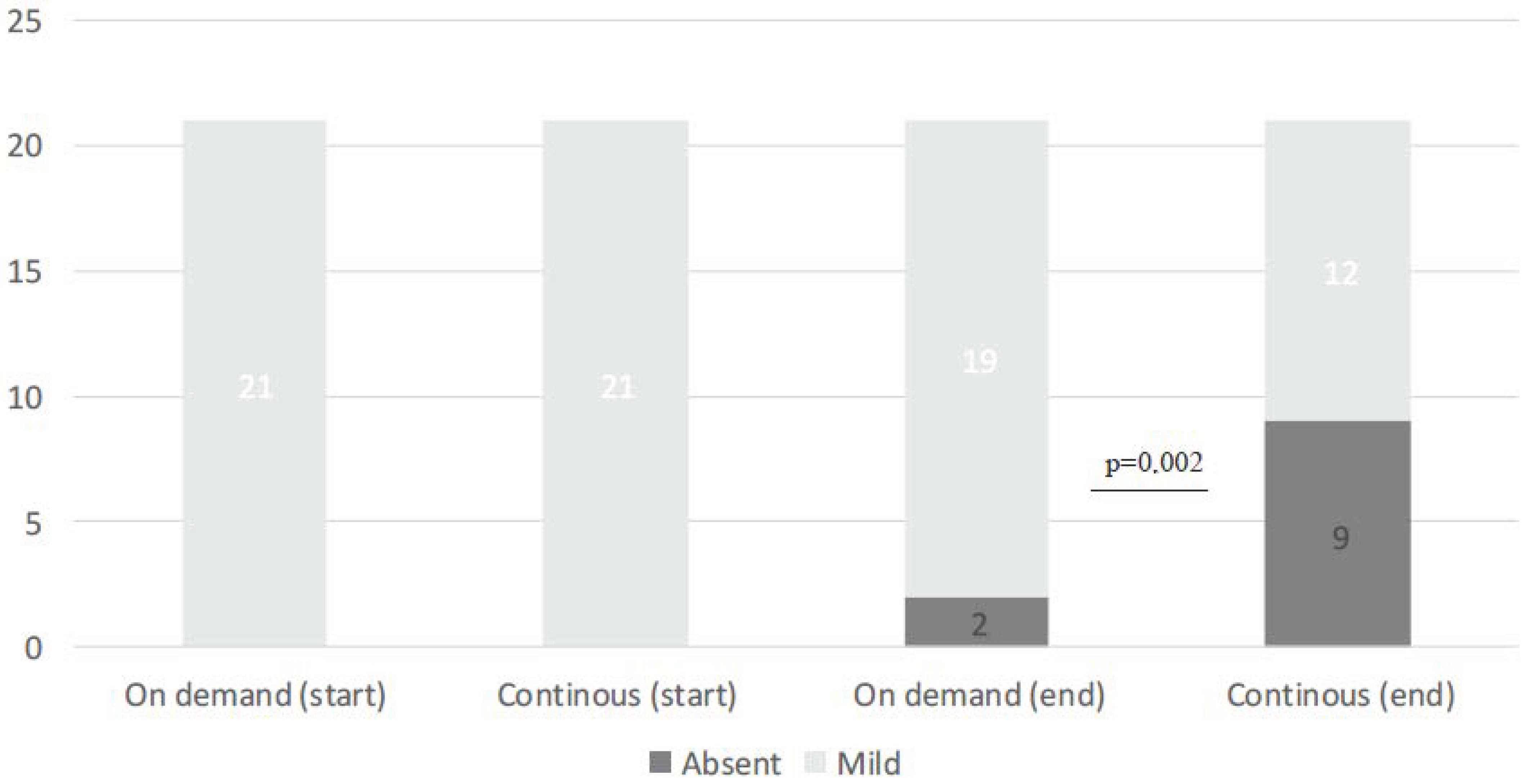
3.2.1. FAS
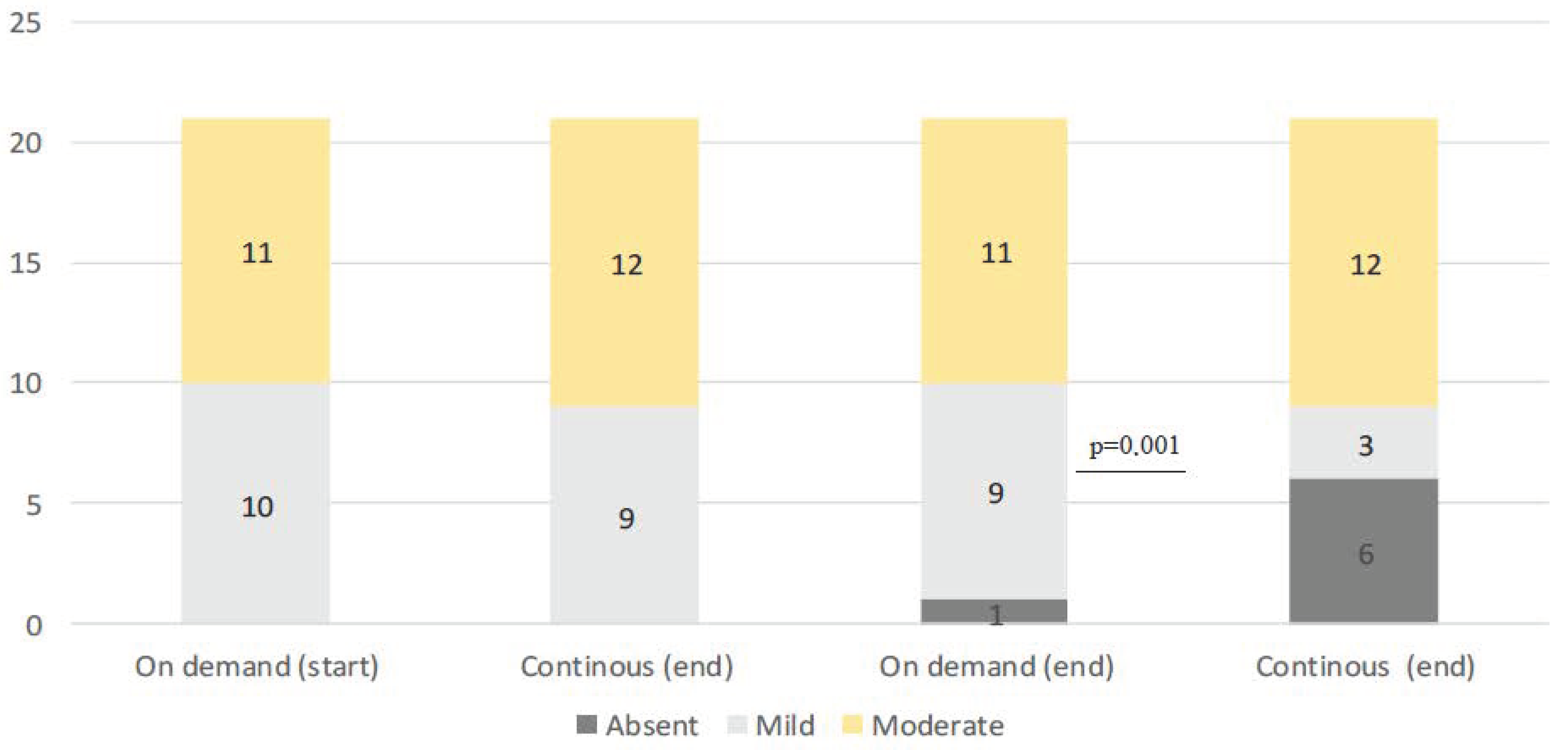
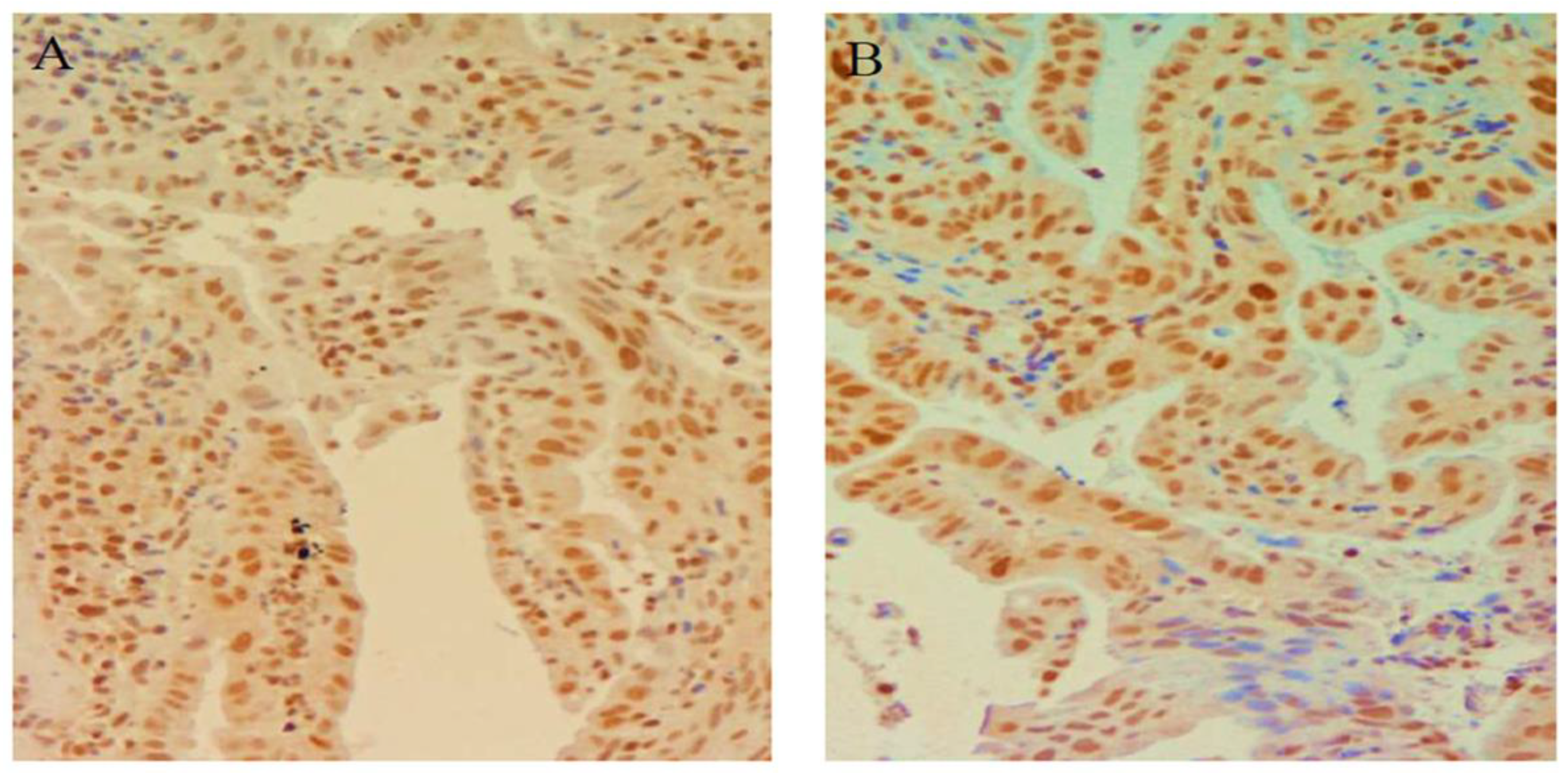
3.2.2. Ki67
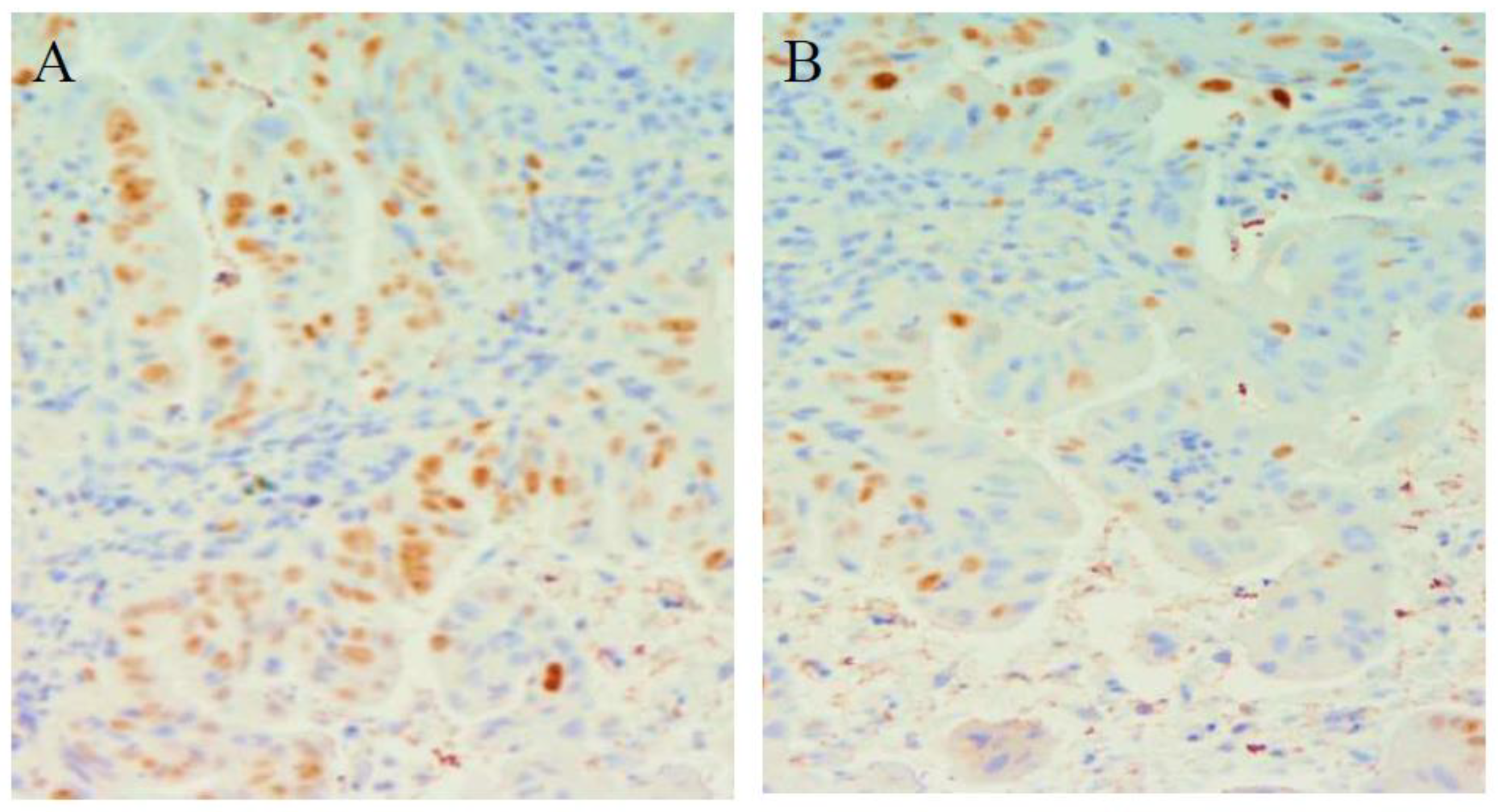
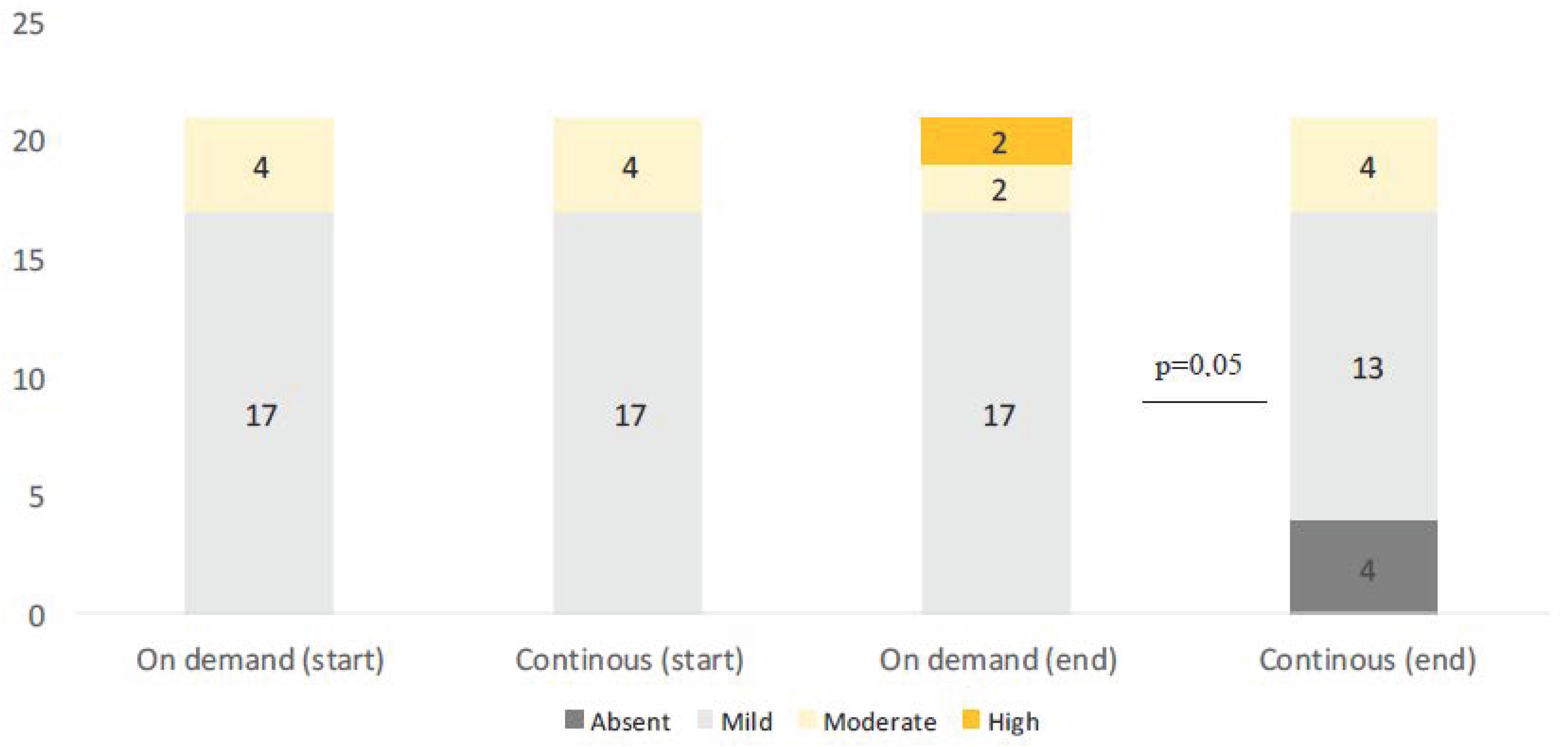
3.2.3. p53
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shaheen, N.J.; Falk, G.W.; Iyer, P.G.; Souza, R.F.; Yadlapati, R.H.; Sauer, B.G.; Wani, S. Diagnosis and Management of Barrett’s Esophagus: An Updated ACG Guideline. Am. J. Gastroenterol. 2022, 117, 559–587. [Google Scholar] [CrossRef] [PubMed]
- Qumseya, B.J.; Bukannan, A.; Gendy, S.; Ahemd, Y.; Sultan, S.; Bain, P.; Gross, S.A.; Iyer, P.; Wani, S. Systematic review and meta-analysis of prevalence and risk factors for Barrett’s esophagus. Gastrointest. Endosc. 2019, 90, 707–717. [Google Scholar] [CrossRef]
- Thrift, A.P.; El-Serag, H.B.; Kanwal, F. Global burden and epidemiology of Barrett esophagus and oesophageal cancer. Nat. Rev. Gastroenterol. Hepatol. 2021, 14, 122–132. [Google Scholar] [CrossRef]
- Codipilly, D.C.; Chandar, A.K.; Singh, S.; Wani, S.; Shaheen, N.J.; Inadomi, J.M.; Chak, A.; Iyer, P.G. The effect of endoscopic surveillance in patients with Barrett’s esophagus: A systematic review and meta-analysis. Gastroenterology 2018, 154, 2068–2086.e5. [Google Scholar] [CrossRef]
- Tan, M.C.; Mansour, N.; White, D.L.; Sisson, A.; El-Serag, H.B.; Thrift, A.P. Systematic review with meta-analysis: Prevalence of prior and concurrent Barrett’s oesophagus in oesophageal adenocarcinoma patients. Aliment. Pharmacol. Ther. 2020, 52, 20–36. [Google Scholar] [CrossRef] [PubMed]
- Iyer, P.G.; Kaul, V. Barrett Esophagus. Mayo Clin. Proc. 2019, 94, 1888–1901. [Google Scholar] [CrossRef] [PubMed]
- Riddell, R.H.; Goldman, H.; Ransohoff, D.F.; Appelman, H.D.; Fenoglio, C.M.; Haggitt, R.C.; Ahren, C.; Correa, P.; Hamilton, S.R.; Morson, B.C.; et al. Dysplasia in inflammatory bowel disease: Standardized classification with provisional clinical applications. Hum. Pathol. 1983, 14, 931–968. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.B.; Corley, D.A.; Murray, L.J.; Liao, L.M.; Kamangar, F.; Ye, W.; Gammon, M.D.; Risch, H.A.; Casson, A.G.; Freedman, N.D.; et al. Gastroesophageal reflux in relation to adenocarcinomas of the esophagus: A pooled analysis from the Barrett’s and Esophageal Adenocarcinoma Consortium (BEACON). PLoS ONE 2014, 9, e103508. [Google Scholar] [CrossRef] [PubMed]
- Maret-Ouda, J.; Markar, S.R.; Lagergren, J. Gastroesophageal Reflux Disease: A Review. JAMA 2020, 324, 2536–2547. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, M.; Green, C.; Faybush, E.M.; Esquivel, R.F.; Fass, R. The extent of oesophageal acid exposure overlap among the different gastro- oesophageal reflux disease group. Aliment. Pharmacol. Ther. 2006, 23, 321–329. [Google Scholar] [CrossRef]
- Martinez, S.D.; Malagon, I.B.; Garewal, H.S.; Cui, H.; Fass, R. Non-erosive reflux disease (NERD)-acid reflux and symptoms pattern. Aliment. Pharmacol. Ther. 2003, 17, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Champion, G.; Richter, J.E.; Vaezi, M.F.; Singh, S.; Alexander, R. Duodenogastroesophageal reflux: Relationship to pH and importance in Barrett’s esophagus. Gastroenterology 1994, 107, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Vaezi, M.F.; Richter, J.E. Role of acid and duodenogastroesophageal reflux in gastroesophageal reflux disease. Gastroenterology 1996, 111, 1192–1199. [Google Scholar] [CrossRef]
- Bhat, A.A.; Lu, H.; Soutto, M.; Capobianco, A.; Rai, P.; Zaika, A.; El-Rifai, W. Exposure of Barrett’s and esophageal adenocarcinoma cells to bile acids activates EGFR-STAT3 signaling axis via induction of APE1. Oncogene 2018, 37, 6011–6024. [Google Scholar] [CrossRef] [PubMed]
- Lagergreen, J.; Bergstrom, R.; Lindgren, A.; Nyren, O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N. Eng. J. Med. 1999, 340, 825–831. [Google Scholar] [CrossRef]
- Moayyedi, P.; Armstrong, D.; Hunt, R.H.; Lei, Y.; Bukoski, M.; White, R.J. The gain in quality-adjusted life months by switching to esomeprazole in those with continued reflux symptoms in primary care: EncomPASS—A cluster-randomized trial. Am. J. Gastroenterol. 2010, 105, 2341–2346. [Google Scholar] [CrossRef]
- Falk, G.W.; Buttar, N.S.; Foster, N.R.; Ziegler, K.L.; Demars, C.J.; Romero, Y.; Marcon, N.E.; Schnell, T.; Corley, D.A.; Sharma, P.; et al. A combination of esomeprazole and aspirin reduces tissue concentrations of prostaglandin E (2) in patients with Barrett’s esophagus. Gastroenterology 2012, 143, 917–926. [Google Scholar] [CrossRef]
- Ouatu-Lascar, R.; Fitzgerald, R.C.; Triadafilopoulos, G. Differentiation and proliferation in Barrett’s esophagus and the effects of acid suppression. Gastroenterology 1999, 117, 327–335. [Google Scholar] [CrossRef]
- Snyder, P.; Dunbar, K.; Cipher, D.J.; Souza, R.F.; Spechler, S.J.; Konda, V.J.A. Aberrant p53 Immunostaining in Barrett’s Esophagus Predicts Neoplastic Progression: Systematic Review and Meta-Analyses. Dig. Dis. Sci. 2019, 64, 1089–1097. [Google Scholar] [CrossRef]
- Kim, R.; Clarke, M.R.; Melhem, M.F.; Young, M.A.; Vanbibber, M.M.; Safatle-Ribeiro, A.V.; Ribeiro, U., Jr.; Reynolds, J.C. Expression of p53, PCNA, and C-erbB-2 in Barrett’s metaplasia and adenocarcinoma. Dig. Dis. Sci. 1997, 42, 2453–2462. [Google Scholar]
- Kuhajda, F.P.; Jenner, K.; Wood, F.D.; Hennigar, R.A.; Jacobs, L.B.; Dick, J.D.; Pasternack, G.R. Fatty acid synthesis: A potential selective target for antineoplastic therapy. Proc. Natl. Acad. Sci. USA 1994, 91, 6379–6383. [Google Scholar] [CrossRef]
- Schroeder, B.; Vander Steen, T.; Espinoza, I.; Venkatapoorna, C.M.K.; Hu, Z.; Silva, F.M.; Regan, K.; Cuyàs, E.; Meng, X.W.; Verdura, S.; et al. Fatty acid synthase (FASN) regulates the mitochondrial priming of cancer cells. Cell Death Dis. 2021, 12, 977. [Google Scholar] [CrossRef] [PubMed]
- Wakil, S.J. Fatty acid synthase, a proficient multifunctional enzyme. Biochemistry 1989, 28, 4523–4530. [Google Scholar] [CrossRef] [PubMed]
- Fhu, C.W.; Ali, A. Fatty Acid Synthase: An Emerging Target in Cancer. Molecules 2020, 25, 3935. [Google Scholar] [CrossRef]
- Crispino, P.; Alò, P.L.; Rivera, M.; Barillà, D.; Nardi, F.; Mariotti, M.; Giancarlo, Z.; Botti, C.; Pica, R.; Cassieri, C.; et al. Evaluation of fatty acid synthase expression in oesophageal mucosa of patients with oesophagitis, Barrett’s oesophagus and adenocarcinoma. J. Cancer Res. Clin. Oncol. 2009, 135, 1533–1541. [Google Scholar] [CrossRef]
- Maslyonkina, K.S.; Konyukova, A.K.; Alexeeva, D.Y.; Sinelnikov, M.Y.; Mikhaleva, L.M. Barrett’s esophagus: The pathomorphological and molecular genetic keystones of neoplastic progression. Cancer Med. 2022, 11, 447–478. [Google Scholar] [CrossRef] [PubMed]
- Going, J.J.; Keith, W.N.; Neilson, L.; Stoeber, K.; Stuart, R.C.; Williams, G.H. Aberrant expression of minichromosome maintenance proteins 2 and 5, and Ki-67 in dysplastic squamous oesophageal epithelium and Barrett’s mucosa. Gut 2002, 50, 373–377. [Google Scholar] [CrossRef]
- Younes, M.; Ertan, A.; Lechago, L.V.; Somoano, J.R.; Lechago, J. p53 protein accumulation is a specific marker of malignant potential in Barrett’s metaplasia. Dig. Dis. Sci. 1997, 42, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Wu, M.; Zhu, G.; Xu, Y. Emerging Roles of the Tumor Suppressor p53 in Metabolism. Front. Cell. Dev. Biol. 2022, 9, 762742. [Google Scholar] [CrossRef] [PubMed]
- Weston, A.P.; Banerjee, S.K.; Sharma, P.; Tran, T.M.; Richards, R.; Cherian, R. p53 protein overexpression in low grade dysplasia (LGD) in Barrett’s esophagus: Immunohistochemical marker predictive of progression. Am. J. Gastroenterol. 2001, 96, 1355–1362. [Google Scholar] [CrossRef] [PubMed]
- Kuhajda, P.F. Fatty acid synthase and human cancer: New perspectives on its role in tumor biology. Nutrition 2000, 16, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Pizer, E.S.; Jackisch, C.; Wood, F.D.; Pasternack, G.R.; Davidson, N.E.; Kuhajda, F.P. Inibition of fatty acid synthasis induces programmed cell death in human breast cancer cells. Cancer Res. 1996, 56, 2745–2747. [Google Scholar] [PubMed]
- Alò, P.L.; Visca, P.; Marci, A.; Mangoni, A.; Botti, C.; Di Tondo, U. Expression of fatty acid synthase (FAS) as a predictor of recurrence in stage I breast carcinoma patients. Cancer 1996, 77, 474–482. [Google Scholar] [CrossRef]
- Epstein, J.I.; Carmichael, M.; Partin, A.W. OA-159 (fatty acid synthase) as an independent predictor in pathological stage in adenocarcinoma of the prostate. Urology 1995, 45, 81–86. [Google Scholar] [CrossRef]
- Rashid, A.; Pizer, E.S.; Moga, M.; Milgraum, L.Z.; Zahurak, M.; Pasternack, G.R.; Kuhajda, F.P.; Hamilton, S.R. Elevated expression of fatty acid synthase and fatty acid synthetic activity in colorectal neoplasia. Am. J. Pathol. 1997, 150, 201–208. [Google Scholar]
- Visca, P.; Sebastiani, V.; Botti, C.; Diodoro, M.G.; Lasagni, R.P.; Romagnoli, F.; Brenna, A.; De Joannon, B.C.; Donnorso, R.P.; Lombardi, G.; et al. Fatty acid synthase (FAS) is a marker of increased risk of recurrence in lung carcinoma. Anticancer Res. 2004, 24, 4169–4173. [Google Scholar]
- Kusakabe, T.; Nashimoto, A.; Honna, K.; Suzuki, T. Fatty acid synthase is highly expressed in carcinoma, adenoma, and in the regenerative epithelium and intestinal metaplasia of the stomach. Histopathology 2002, 40, 71–79. [Google Scholar] [CrossRef]
- Sebastiani, V.; Visca, P.; Botti, C.; Santeusanio, G.; Galati, G.M.; Piccini, V.; Capezzone de Joannon, B.; Di Tondo, U.; Alo, P.L. Fatty acid synthase is a marker of increased risk of recurrence in endometrial carcinoma. Gynecol. Oncol. 2004, 92, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, T.; Terashima, S.; Kogure, M.; Hoshino, Y.; Kusakabe, T.; Suzuki, T.; Gotoh, M. Overexpression of fatty acid synthase in esophageal squamous cell dysplasia and carcinoma. Pathobiology 2001, 69, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Giordano, M.; Ciarambino, T.; Castellino, P.; Malatino, L.; Di Somma, S.; Biolo, G.; Paolisso, G.; Adinolfi, L.E. Diseases associated with electrolyte imbalance in the ED: Age-related differences. Am. J. Emerg. Med. 2016, 34, 1923–1926. [Google Scholar] [CrossRef]
- Nakada, K.; Matsuhashi, N.; Iwakiri, K.; Oshio, A.; Joh, T.; Higuchi, K.; Haruma, K. Development and validation of a simple and multifaceted instrument, GERD-TEST, for the clinical evaluation of gastresophageal reflux and dyspeptic symptoms. World J. Gastroenterol. 2017, 23, 5216–5228. [Google Scholar] [CrossRef] [PubMed]
- Isshi, K.; Matsuhashi, N.; Joh, T.; Higuchi, K.; Iwakiri, K.; Kamiya, T.; Manabe, N.; Ogawa, M.; Arihiro, S.; Haruma, K. Proton pump inhibitor monotherapy is effective to attenuate dyspepsia symptoms associated with gastresophageal reflux disease: A multicenter prospective observational study. J. Gastroenterol. 2019, 54, 492–500, reprinted in J. Gastroenterol. 2019, 54, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Lundell, L.; Dent, J.; Bennett, J.; Blum, A.L.; Armstrong, D.; Galmiche, J.P.; Johnson, F.; Hongo, M.; Richter, J.E.; Spechler, S.J. Endoscopic assessment of esophagitis: Clinical and functional correlates and further validation of the Los Angeles Classification. Gut 1999, 45, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Alvarez Herrero, L.; Curvers, W.L.; van Vilsteren, F.G.; Wolfsen, H.; Ragunath, K.; Wong Kee Song, L.M.; Mallant-Hent, R.C.; van Oijen, A.; Scholten, P.; Schoon, E.J. Validation of the classification of Barrett’s esophagus in clinical practice. Endoscopy 2013, 45, 876–882. [Google Scholar] [CrossRef]
- Levine, D.S.; Haggitt, R.C.; Blount, P.L.; Rabinovitch, P.S.; Rusch, V.W.; Reid, B.J. An endoscopic biopsy protocol can differentiate high-grade dysplasia from early adenocarcinoma in Barrett’s esophagus. Gastroenterology 1993, 105, 40–50. [Google Scholar] [CrossRef]
- Richardson, J.D.; Kuhns, J.G.; Richardson, R.L.; Polk, H.C. Properly conducted fundoplication reverses histologic evidence of esophagitis. Ann. Surg. 1083, 197, 763–770. [Google Scholar] [CrossRef]
- Geboes, K.; Van Eyken, P. The diagnosis of dysplasia and malignancy in Barrett’s esophagus. Histopathology 2000, 37, 99–107. [Google Scholar] [CrossRef]
- Januszewicz, W.; Pilonis, N.D.; Sawas, T.; Phillips, R.; O’Donovan, M.; Miremadi, A.; Malhotra, S.; Tripathi, M.; Blasko, A.; Katzka, D.A.; et al. The utility of P53 immunohistochemistry in the diagnosis of Barrett’s oesophagus with indefinite for dysplasia. Histopathology 2022, 80, 1081–1090. [Google Scholar] [CrossRef]
- Mittal, S.K.; Abdo, J.; Adrien, M.P.; Bayu, B.A.; Kline, J.R.; Sullivan, M.M.; Agrawal, D.K. Current state of prognostication, therapy and prospective innovations for Barrett’s-related esophageal adenocarcinoma: A literature review. J. Gastrointest. Oncol. 2021, 12, 1197–1214. [Google Scholar] [CrossRef]
- Weston, A.P.; Badr, A.S.; Hassanein, R.S. Prospective multivariate analysis of clinical, endoscopic, and histological factors predictive of the development of Barrett’s multifocal high-grade dysplasia or adenocarcinoma. Am. J. Gastroenterol. 1999, 94, 3413–3419. [Google Scholar] [CrossRef]
- Morales, C.P.; Souza, R.F.; Spechler, S.J. Hallmarks of cancer progression in Barrett’s esophagus. Lancet 2002, 360, 1587–1589. [Google Scholar] [CrossRef] [PubMed]
- Que, J.; Garman, K.S.; Souza, R.F.; Spechler, S.J. Pathogenesis and Cells of Origin of Barrett’s Esophagus. Gastroenterology 2019, 157, 349–364.e1. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Zhang, C. The Oxidative Damage and Inflammation Mechanisms in GERD-Induced Barrett’s Esophagus. Front. Cell Dev. Biol. 2022, 10, 885537. [Google Scholar] [CrossRef] [PubMed]
- Sugano, K.; Spechler, S.J.; El-Omar, E.M.; McColl, K.E.L.; Takubo, K.; Gotoda, T.; Fujishiro, M.; Iijima, K.; Inoue, H.; Kawai, T.; et al. Kyoto international consensus report on anatomy, pathophysiology and clinical significance of the gastroesophageal junction. Gut 2022, 71, 1488–1514. [Google Scholar] [CrossRef]
- Frei, N.F.; Stachler, M.D.; Bergman, J.J.G.H.M. Risk stratification in Barrett’s esophagus patients with diagnoses of indefinite for dysplasia: The definite silver bullet has not (yet) been found. Gastrointest. Endosc. 2020, 91, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Grewal, U.S.; Randhawa, M.S.; Mehta, A. Role of Mitochondrial Markers in Improved Detection and Risk-Stratification in Barrett’s Esophagus Patients. Yale J. Biol. Med. 2019, 92, 533–539. [Google Scholar]
- Sihvo, E.I.T.; Salminen, J.T.; Rantanen, T.K.; Rämö, O.J.; Ahotupa, M.; Färkkilä, M.; Auvinen, M.I.; Salo, J.A. Oxidative stress has a role in a malignant transformation in Barret’s esophagus. Int. J. Cancer 2002, 102, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.Y.; Lee, J.S.; Ahn, B.O.; Cho, H.; Kim, W.B.; Kim, Y.B.; Surh, Y.J.; Cho, S.W.; Hahm, K.B. Oxidative damage are critical in pathogenesis of reflux esophagitis: Implication of antioxidant in its treatment. Radic. Biol. Med. 2001, 30, 905–915. [Google Scholar] [CrossRef]
- Baggetto, L.G. Deviant energetic metabolism of glycolytic cancer cells. Biochimie 1992, 74, 959–974. [Google Scholar] [CrossRef]
- Newsholme, E.A.; Board, M. Application of metabolic-control logic to fuel utilization and its significance in tumor cells. Adv. Enzyme Regul. 1991, 31, 225–246. [Google Scholar] [CrossRef]
- Umansky, M.; Yasui, W.; Hallak, A.; Brill, S.; Shapira, I.; Halpern, Z.; Hibshoosh, H.; Rattan, J.; Meltzer, S.; Tahara, E.; et al. Proton pump inhibitors reduce cell cycle anomalies in Barrett’s esophagus. Oncogene 2001, 20, 7987–7991. [Google Scholar] [CrossRef]
- Zhang, L.; Sun, B.; Zhou, X.; Wei, Q.; Liang, S.; Luo, G.; Li, T.; Lv, M. Barrett’s Esophagus and Intestinal Metaplasia. Front. Oncol. 2021, 11, 630837. [Google Scholar] [CrossRef]
- Peters, F.T.; Ganesh, S.; Kuipers, E.J.; Sluiter, W.J.; Klinkenberg-Knol, E.C.; Lamers, C.B.; Kleibeuker, J.H. Endoscopic regression of Barrett’s oesophagus during omeprazole treatment; a randomised double blind study. Gut 1999, 45, 489–494, reprinted in Gut 2000, 47, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Peters, F.T.M.; Ganesh, S.; Kuipers, E.J.; Sluiter, W.J.; Karrenbeld, A.; de Jager-Krikken, A.; Klinkenberg-Knol, E.C.; Lamers, C.B.; Kleibeuker, J.H. Effect of elimination of acid reflux on epithelial cell proliferative activity of Barrett oesophagus. Scand. J. Gastroenterol. 2000, 12, 1239–1244. [Google Scholar]
- Alkhayyat, M.; Kumar, P.; Sanaka, K.O.; Thota, P.N. Chemoprevention in Barrett’s esophagus and esophageal adenocarcinoma. Therap. Adv. Gastroenterol. 2021, 14, 17562848211033730. [Google Scholar] [CrossRef]
- Panda, A.; Shin, M.R.; Cheng, C.; Bajpai, M. Barrett’s Epithelium to Esophageal Adenocarcinoma: Is There a “Point of No Return”? Front. Genet. 2021, 12, 706706. [Google Scholar] [CrossRef]
- Hillman, L.C.; Chiragakis, L.; Shadbolt, B.; Kaye, G.L.; Clarke, A.C. Effect of proton pump inhibitors on markers of risk for high-grade dysplasia and oesophageal cancer in Barrett’s oesophagus. Aliment. Pharmacol. Ther. 2008, 27, 321–326. [Google Scholar] [CrossRef]
- Stolte, M.; Vieth, M.; Schmitz, J.M.; Alexandridis, T.; Seifert, E. Effects of long-term treatment with proton pump inhibitors in gastroesophageal reflux disease on the histological findings in the lower oesophagus. Scand. J. Gastroenterol. 2000, 35, 1125–1130. [Google Scholar] [PubMed]
- Baldaque-Silva, F.; Vieth, M.; Debel, M.; Håkanson, B.; Thorell, A.; Lunet, N.; Song, H.; Mascarenhas-Saraiva, M.; Pereira, G.; Lundell, L.; et al. Impact of gastresophageal reflux control through tailored proton pump inhibition therapy or fundoplication in patients with Barrett’s esophagus. World J. Gastroenterol. 2017, 23, 3174–3183. [Google Scholar] [CrossRef]
- Feagins, L.A.; Zhang, H.Y.; Hormi-Carver, K.; Quinones, M.H.; Thomas, D.; Zhang, X.; Terada, L.S.; Spechler, S.J.; Ramirez, R.D.; Souza, R.F. Acid has antiproliferative effects in nonneoplastic Barrett’s epithelial cells. Am. J. Gastroenterol. 2007, 102, 10–20. [Google Scholar] [CrossRef]
- Zhang, H.Y.; Zhang, X.; Hormi-Carver, K.; Feagins, L.A.; Spechler, S.J.; Souza, R.F. In non-neoplastic Barrett’s epithelial cells, acid exerts antiproliferative effects through activation of the Chk2 pathway. Cancer Res. 2007, 67, 8580–8587. [Google Scholar] [CrossRef] [PubMed]
- Leedham, S.; Jankowski, J. The evidence-based of proton pump inhibitor chemopreventative agents in Barrett’s esophagus—The good, the bad, and the flawed. Am. J. Gastroenterol. 2007, 102, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Koltai, T.; Reshkin, S.J.; Harguindey, S. (Eds.) Chapter 2—Cancer metabolism. In An Innovative Approach to Understanding and Treating Cancer: Targeting pH; Academic Press: Cambridge, MA, USA, 2020; pp. 15–52. ISBN 9780128190593. [Google Scholar] [CrossRef]
- Zhao, L.; Sanyal, S. p53 Isoforms as Cancer Biomarkers and Therapeutic Targets. Cancers 2022, 14, 3145. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Group A | Group B |
|---|---|---|---|
| Sex | 18 females and 24 males | ||
| Age | 50.44 ± 10.16 | 51.21 ± 6.6 | 49.23 ± 4.4 |
| Length of BE at entry | 2.8 ± 0.6 | 2.9 ± 0.2 | 2.7 ± 0.8 |
| Length of BE at exit | 2.55 ± 0.4 | 2.5 ± 0.7 | 2.6 ± 0.1 |
| Smokers | 16/42 | 7/42 | 9/21 |
| Alcohol consumers | 7/42 | 3/21 | 4/21 |
| Heartburn | 8/42 | 5/21 | 3/21 |
| Regurgitation | 5/42 | 4/21 | 4/21 |
| Heartburn and regurgitation | 29/42 | 19/21 | 10/21 |
| Nightly symptoms | 36/42 | 17/21 | 15/21 |
| Number of episodes/week < 7 | 21/42 | 11/10 | 10/10 |
| Number of episodes/week > 8 | 21/42 | 12/21 | 9/21 |
| Long-Term PPIs | On-Demand PPIs. | |
|---|---|---|
| p53 | ||
| Mild | 17 (80%) | 17 (80%) |
| Intense | 4 (20%) | 4 (20%) |
| Ki67 | ||
| Mild | 9 (43%) | 10 (48%) |
| Moderate | 12 (57%) | 11(52%) |
| FAS | ||
| Mild | 21 (100%) | 21 (100%) |
| Intense | 0 | 0 |
| Long-Term PPIs | On-Demand PPIs | |
|---|---|---|
| p53 | ||
| Absent Mild | 4 (19%) 13 (62%) | 0 17 (82%) |
| Moderate Intense | 4 (19%) | 2 (9%) 2 (9%) |
| Pearson chi-square: 15.00; df: 1; p = 0.05; | ||
| FAS | ||
| Absent | 9 (43%) | 2 (10%) |
| Mild | 11 (56%) | 19 (90%) |
| Intense | 0 | 0 |
| Pearson chi-square: 16.16; df: 2; p = 0.002; | ||
| i67 | ||
| Absent | 6 (28%) | 1 (5%) |
| Mild | 3 (14%) | 9 (43%) |
| Moderate | 12 (58%) | 11 (52%) |
| Pearson chi-square: 8.8; fd: 1; p = 0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crispino, P.; Ciarambino, T.; Giordano, M. Variation in Fatty Acid Synthase, Ki67 and p53 Esophageal Mucosa Expressions in Barrett’s Esophagus Patients Treated for One Year with Two Esomeprazole Different Regimens. Curr. Issues Mol. Biol. 2023, 45, 4701-4715. https://doi.org/10.3390/cimb45060299
Crispino P, Ciarambino T, Giordano M. Variation in Fatty Acid Synthase, Ki67 and p53 Esophageal Mucosa Expressions in Barrett’s Esophagus Patients Treated for One Year with Two Esomeprazole Different Regimens. Current Issues in Molecular Biology. 2023; 45(6):4701-4715. https://doi.org/10.3390/cimb45060299
Chicago/Turabian StyleCrispino, Pietro, Tiziana Ciarambino, and Mauro Giordano. 2023. "Variation in Fatty Acid Synthase, Ki67 and p53 Esophageal Mucosa Expressions in Barrett’s Esophagus Patients Treated for One Year with Two Esomeprazole Different Regimens" Current Issues in Molecular Biology 45, no. 6: 4701-4715. https://doi.org/10.3390/cimb45060299