
Consensus on the Best Practice Guidelines for Psychomotor Intervention in Preschool Children with Autism Spectrum Disorder
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Selection and Recruitment of Participants
- (a)
- Have at least a bachelor’s degree in Psychomotor Therapy.
- (b)
- Be a psychomotor therapist with more than three years of experience in psychomotor intervention in different contexts in Portugal, working either individually or in groups (using therapeutic or educational approaches).
- (c)
- Be a researcher or university professor with scientific/professional expertise in preschool children with ASD, in psychomotor intervention.
2.2. Procedures
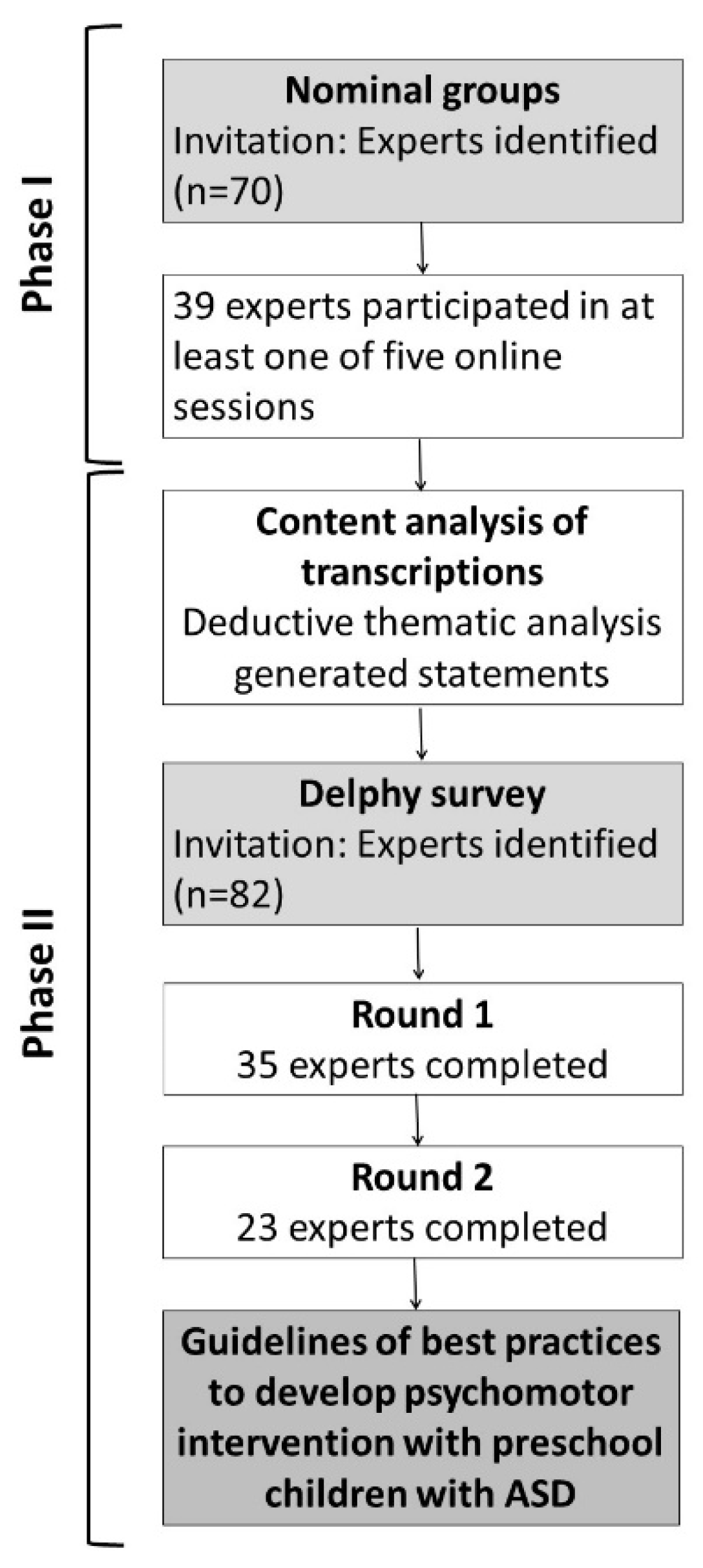
2.2.1. Phase I: Nominal Group Technique (NGT)
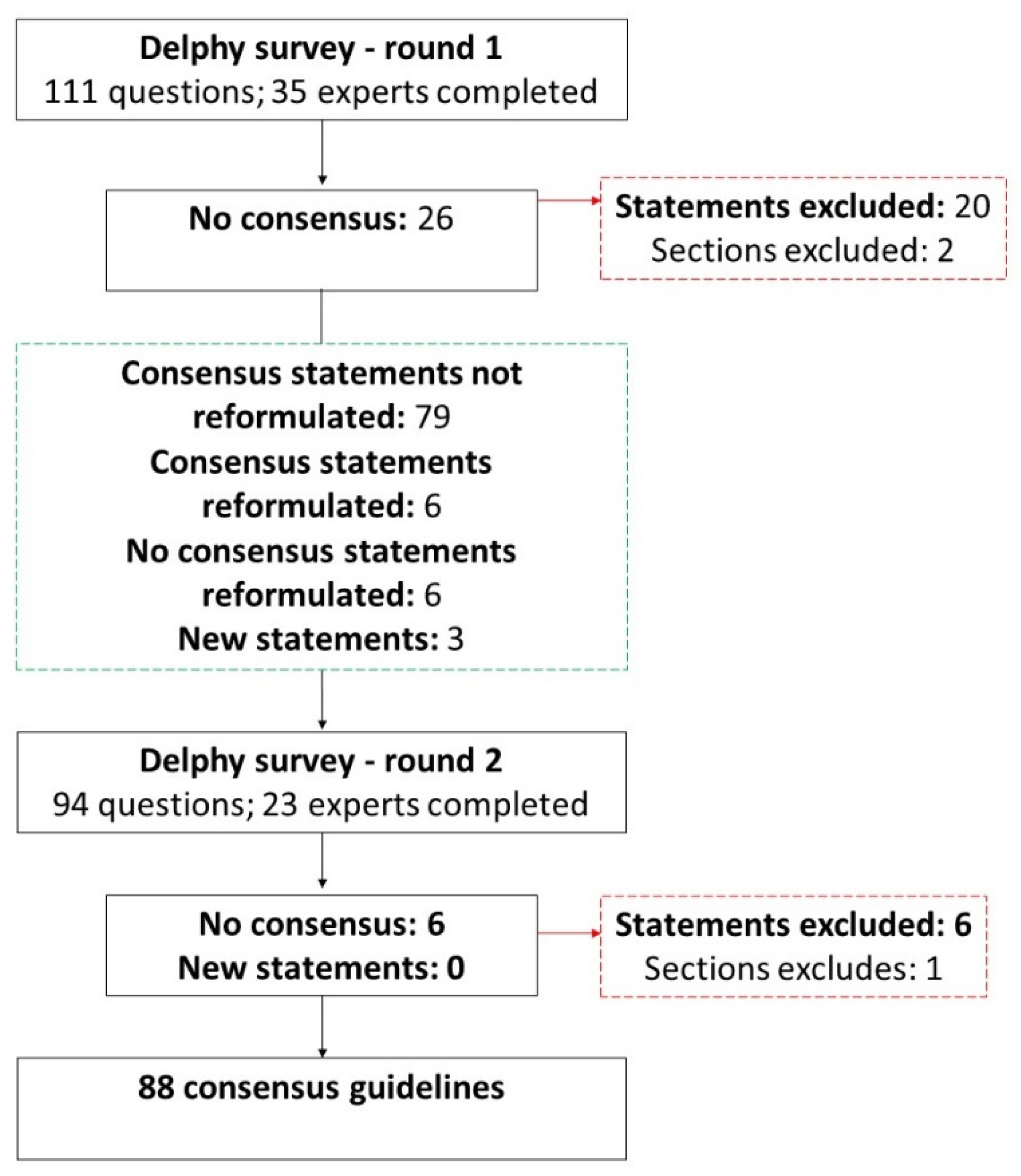
2.2.2. Delphi Technique
2.3. Data Management and Analysis
2.3.1. Phase I
2.3.2. Phase II
3. Results
3.1. Phase I
3.2. Phase II
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Questions Intended to Get Participants to Think about; One Initial Question per Topic | |
|---|---|
| Meeting 1 Trial question Topic: Question: | From your experience what are the primary needs of children with ASD (3–6 years old) that psychomotor intervention may improve? Objectives and primary results What are the aims of psychomotor intervention for children with ASD (3–6 years old)? |
| Meeting 2 Topic: Question: | Theories and models What theories or models support psychomotor intervention with children with ASD (3–6 years)? |
| Meeting 3 Topic: Question: | Methods What types of activities (individual and/or group) are carried out in psychomotor intervention with children with ASD (3–6 years)? (Experts are invited to give two examples of activities in the clarification stage) |
| Meeting 4 Topic: Question: | Environmental arrangements How are the sessions structured (individual and/or group)? Please select three of these aspects on which you would like to give your ideas:
|
| Meeting 5 Topic: Question: | Strategies What are the strategies you use most (in individual and/or group intervention)? Select three of these types of strategies about which you want to give your ideas:
|
References
- Probst, M.; Knapen, J.; Poot, G.; Vancampfort, D. Psychomotor Therapy and Psychiatry: What’s in a Name? Open Complement. Med. J. 2010, 2, 105–113. [Google Scholar] [CrossRef]
- European Forum of Psychomotricity. Statutes of the European Forum of Psychomotricity. 2015. Available online: https://psychomot.org/ (accessed on 20 September 2022).
- Ferré, G.; Dueñas, J.M.; Camps, C. Differences between the dynamic and normative psychomotricity in child development. Rev. Int. Med. Ciencias Act. Físi. Deporte 2021, 2, 47–62. [Google Scholar] [CrossRef]
- Moreira, M.S.; Almeida, G.N.; Marinho, S.M. Efectos de un programa de Psicomotricidad Educativa en niños en edad preescolar. Sportis 2016, 2, 326–342. [Google Scholar] [CrossRef] [Green Version]
- Vetter, M.; Sandmeier, A. Psychomotricity: Effects of psychomotor interventions from the perspective of teachers. Eur. Psychomot. J. 2020, 12, 30–42. [Google Scholar]
- Fotiadou, E.G.; Neofotistou, K.H.; Giagazoglou, P.F.; Tsimaras, V.K. The effect of a psychomotor education program on the static balance of children with intellectual disability. J. Strength Cond. Res. 2017, 31, 1702–1708. [Google Scholar] [CrossRef] [PubMed]
- Moschos, G.; Pollatou, E. The effect of a psychomotor intervention program in children 3–10 years of age: A systematic review. Body Mov. Danc. Psychother. 2022, 294–309. [Google Scholar] [CrossRef]
- Caliendo, M.; Di Sessa, A.; D’Alterio, E.; Frolli, A.; Verde, D.; Iacono, D.; Romano, P.; Vetri, L.; Carotenuto, M. Efficacy of Neuro-Psychomotor Approach in Children Affected by Autism Spectrum Disorders: A Multicenter Study in Italian Pediatric Population. Brain Sci. 2021, 11, 1210. [Google Scholar] [CrossRef] [PubMed]
- Emck, C. Double trouble? Movement behaviour and psychiatric conditions in children: An opportunity for treatment and development. Arts Psychother. 2014, 41, 214–222. [Google Scholar] [CrossRef]
- Frazão, A.; Santos, S.; Lebre, P. Psychomotor Intervention Practices for Children with Autism Spectrum Disorder: A Scoping Review. Rev. J. Autism Dev. Disord. 2021. [Google Scholar] [CrossRef]
- Bhat, A.N. Is Motor Impairment in Autism Spectrum Disorder Distinct from Developmental Coordination Disorder A Report from the SPARK Study. Phys. Ther. 2020, 100, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Paquet, A.; Olliac, B.; Golse, B.; Vaivre-Douret, L. Nature of motor impairments in autism spectrum disorder: A comparison with developmental coordination disorder. J. Clin. Exp. Neuropsychol. 2019, 41, 1–14. [Google Scholar] [CrossRef]
- Bhat, A.N. Motor Impairment Increases in Children with Autism Spectrum Disorder as a Function of Social Communication, Cognitive and Functional Impairment, Repetitive Behavior Severity, and Comorbid Diagnoses: A SPARK Study Report. Autism Res. 2021, 14, 202–219. [Google Scholar] [CrossRef]
- Leonard, H.C.; Hill, E.L. Review: The impact of motor development on typical and atypical social cognition and language: A systematic review. Child Adolesc. Ment. Health. 2014, 19, 163–170. [Google Scholar] [CrossRef]
- Hume, K.; Steinbrenner, J.R.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Szendrey, S.; McIntyre, N.S.; Yücesoy-Özkan, S.; Savage, M.N. Evidence-based practices for children, youth, and young adults with Autism: Third Generation Review. J. Autism Dev. Disord. 2021, 51, 4013–4032. [Google Scholar] [CrossRef] [PubMed]
- Steinbrenner, J.R.; Hume, K.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Szendrey, S.; McIntyre, N.S.; Yücesoy-Özkan, S.; Savage, M.N. Evidence-Based Practices for Children, Youth, and Young Adults with Autism Spectrum Disorder; The University of North Carolina at Chapel Hill: Chapel Hill, NC, USA; Frank Porter Graham Child Development Institute: Chapel Hill, NC, USA; National Clearinghouse on Autism Evidence and Practice Review Team: Chapel Hill, NC, USA, 2020. [Google Scholar]
- Zampella, C.J.; Wang, L.A.L.; Haley, M.; Hutchinson, A.G.; de Marchena, A. Motor Skill Differences in Autism Spectrum Disorder: A Clinically Focused Review. Curr. Psychiatry Rep. 2021, 23, 10. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, K.V.V.; Lima, S.A. Intervenção psicomotora no desenvolvimento infantil: Uma revisão integrativa. Rev. Bras. Promoção Saúde 2019, 32, 1–10. [Google Scholar] [CrossRef]
- Blease, C.R.; Lilienfeld, S.O.; Kelley, J.M. Evidence-Based Practice and Psychological Treatments: The Imperatives of Informed Consent. Front Psychol. 2016, 7, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Cook, S.C.; Schwartz, A.C.; Kaslow, N.J. Evidence-Based Psychotherapy: Advantages and Challenges. Neurotherapeutics 2017, 14, 537–545. [Google Scholar] [CrossRef] [Green Version]
- Fuentes, J.; Hervás, A.; Howlin, P. ESCAP practice guidance for autism: A summary of evidence-based recommendations for diagnosis and treatment. Eur. Child Adolesc. Psychiatry 2021, 30, 6961–6984. [Google Scholar] [CrossRef]
- Weissman, L. Autism Spectrum Disorder in Children and Adolescents: Overview of Management. In UpToDate; Augustyn, M., Patterson, M., Eds.; UpToDate: Waltham, MA, USA, 2021. [Google Scholar]
- Weissman, L. Autism Spectrum Disorder in Children and Adolescents: Behavioral and Educational Interventions. In UpToDate; Augustyn, M., Patterson, M., Eds.; UpToDate: Waltham, MA, USA, 2021. [Google Scholar]
- National Institute for Health and Care Excellence. Autism Spectrum Disorder in under 19s: Support and Management. 2021. Available online: https://www.nice.org.uk/guidance/cg170 (accessed on 11 January 2022).
- Direção-Geral da Saúde. Norma no 002/2019-Abordagem Diagnóstica e Intervenção na Perturbação do Espetro do Autismo em Idade Pediátrica e no Adulto. 2019. Available online: https://normas.dgs.min-saude.pt/wp-content/uploads/2019/09/Abordagem-Diagnostica-e-Intervencao-na-Perturbacao-do-Espetro-do-Autismo-em-Idade-Pediatrica-e-no-Adulto_2019.pdf (accessed on 29 September 2022).
- Yiulin, W.; Fan, L.; Yuting, D.; Zhaoxiang, B.; Chi, Z.; Yaolong, C. CONSORT-SPI 2018 explanation and elaboration: Guidance for reporting social and psychological intervention trials. Chin. J. Evid. Based Med. 2020, 20, 1458–1470. [Google Scholar] [CrossRef]
- Manera, K.; Hanson, C.S.; Gutman, T.; Tong, A. Consensus Methods: Nominal Group Technique. In Handbook of Research Methods in Health Social Sciences; Liamputtong, P., Ed.; Springer: Singapore, 2019; pp. 737–750. [Google Scholar]
- World Health Organization. WHO Handbook for Guideline Development, 2nd. ed.; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Van de, A.H.; Delbecq, A.L. The Effectiveness of Nominal, Delphi, and Interacting Group Decision Making Processes. Acad. Manag. J. 1974, 17, 605–621. [Google Scholar] [CrossRef]
- Niederberger, M.; Spranger, J. Delphi Technique in Health Sciences: A Map. Front. Public Health 2020, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Skela-Savič, B.; MacRae, R.; Lillo-Crespo, M.; Rooney, K.D. The Development of a Consensus Definition for Healthcare Improvement Science (HIS) in Seven European Countries: A consensus methods approach. Zdr. Varst. 2017, 56, 82–90. [Google Scholar] [CrossRef] [Green Version]
- McMillan, S.S.; Kelly, F.; Sav, A.L.; Kendall, E.; King, M.A.; Whitty, J.A.; Wheeler, A.J. Using the Nominal Group Technique: How to analyse across multiple groups. Health Serv. Outcomes Res. Methodol. 2014, 14, 92–108. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Developing NICE Guidelines: The Manual. NICE. 2014. Available online: http://www.nice.org.uk/article/pmg20 (accessed on 12 February 2022).
- Borek, A.J.; Abraham, C.; Smith, J.R.; Greaves, C.J.; Tarrant, M. A checklist to improve reporting of group-based behaviour-change interventions. BMC Public Health 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the Delphi method for selecting healthcare quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Loebach, J.; Cox, A. Tool for observing play outdoors (Topo): A new typology for capturing children’s play behaviors in outdoor environments. Int. J. Environ. Res. Public Health 2020, 17, 5611. [Google Scholar] [CrossRef]
- Foth, T.; Efstathiou, N.; Vanderspank-Wright, B.; Ufholz, L.A.; Dütthorn, N.; Zimansky, M.; Humphrey-Murto, S. The use of Delphi and Nominal Group Technique in nursing education: A review. Int. J. Nurs. Stud. 2016, 60, 112–120. [Google Scholar] [CrossRef]
- Humphrey-murto, S.; Varpio, L.; Gonsalves, C.; Wood, T.J. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med. Teacher 2016, 39, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Verwoerd, M.; Wittink, H.; Maissan, F.; Smeets, R. Consensus of potential modifiable prognostic factors for persistent pain after a first episode of nonspecific idiopathic, non-traumatic neck pain: Results of nominal group and Delphi technique approach. BMC Musculoskelet. Disord. 2020, 21, 656. [Google Scholar] [CrossRef] [PubMed]
- Platz, T. Methods for the Development of Healthcare Practice Recommendations Using Systematic Reviews and Meta-Analyses. Front. Neurol. 2021, 12, 699968. [Google Scholar] [CrossRef]
- Nasa, P.; Jain, R.; Juneja, D. Delphi methodology in healthcare research: How to decide its appropriateness. World J. Methodol. 2021, 11, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Beiderbeck, D.; Frevel, N.; Von Der Gracht, H.A.; Schmidt, S.L.; Schweitzer, V.M. Preparing, conducting, and analyzing Delphi surveys: Cross-disciplinary practices, new directions, and advancements. MethodsX 2021, 8, 01401. [Google Scholar] [CrossRef] [PubMed]


| NGT Process | Delphi Survey–Round One | |
|---|---|---|
| Age | M | M [min, max] |
| Years | 37 [26, 67] | 37 [26, 68] |
| Gender | n | n |
| Female | 38 | 5 |
| Male | 1 | 0 |
| Current profession | n | n |
| Psychomotor therapist | 35 | 34 |
| Professor/researcher | 4 | 1 |
| Working experience | M [min, max] | M [min, max] |
| Years of experience | 13 [5, 45] | 15 [5, 45] |
| Number of children with ASD accompanied (last 2 years) | 8 [0, 30] | 9 [0, 30] |
| Number of children accompanied in group settings with or without ASD (last 2 years) | 7 [0, 25] | 3 [0, 25] |
| Context of intervention (predominantly) | ||
| Clinic | 18 | 18 |
| Home | 8 | 8 |
| Community teams/association | 3 | 2 |
| School | 3 | 2 |
| Hospital | 3 | 2 |
| Others | 4 | 2 |
| Intervention Design | Intervention Content |
|---|---|
|
|
| Participants | Facilitators |
|
|
| Sections |
|
4. Psychomotor intervention can occur individually or in groups, where individual interventions allow the strengthening of the therapeutic relationship and the reinforcement of skills with individualized strategies. |
|
|
14. The child’s motivations (interests) are the starting point for developing competencies. 15. Playfulness promotes active, interactive, and pleasurable learning. 16. The therapeutic relationship should be guided by active listening, empathy, authenticity, and trust. 17. Safety is provided by a structured space and time, and by a welcoming and affectionate climate. 18. Sensorimotor experiences promote sensory information processing and processing related to planning, learning and control. 20. The movement of the body produces physiological and emotional responses that are regulated according to the interaction with the social and physical environment, and is systematized in the implicit memory responsible for the pleasure in action and the relationship with the other. 21. Body (and self) awareness influences the ability to feel and understand the emotional state of the other and, therefore, influences interpersonal relationships. 23. The use of expression-oriented activities/strategies and action-oriented activities/strategies provides a comprehensive and integrated response to a child’s development. |
27. The type of games played in the first intervention sessions should be based on the child’s spontaneity and/or interests. 31. Fine-movement play: drawing, painting, modeling, fine manipulation and writing materials in different planes and spatial dimensions should be facilitated. 32. Movement games, massage and imitation of simple movements involved in a story or song can be used, to provide the perception of the contrast between contraction and relaxation states. 33. Expressive play: different music and rhythms creating sequences of movements, can be used. 34. In expressive play, different types of movements, positions and body postures that vary between states of movement and immobility should be facilitated. 38. Symbolic imaginative play: objects, actions, or ideas that symbolize something should be facilitated. 40. Conventional-rules games, (i.e., playing football): knowledge of rules for “know-how” enables the mobilization of skills of perception, memorization, planning, organization, sequencing and association. 42. Constructive exploration play (i.e., building a tower): construction materials should be available. 43. Sensory exploration play: materials with different sensory properties (visual, auditory, tactile, proprioceptive, vestibular) should be facilitated. 44. Sensory exploration play: experiences of therapeutic/affective touch, breathing, body restraint and passive mobilization using mediation materials, should be facilitated. |
51. The manipulation of involvement through the organization of space, the selection of materials and the positioning of the psychomotor therapist’s body should guide the exploration of the child’s possibilities of action, introducing or removing elements. 52. Verbal instruction should be clear, simple/short and directive, of the type associated with gestures or demonstration. 53. Visual or gestural prompts should be used when there is a need to guide the child’s response to act in accordance with the objective, during instruction or execution of the activity. 60. The total or partial physical and verbal assistance that leads to the achievement of the objective in the activity should evolve from a greater to a lesser intensity. 64. The psychomotor therapist should create challenges between the child and what he wants to do, to promote the child’s interaction/communication when there are situational conditions and a trusting, therapeutic relationship. 65. Anticipating what will happen through planning the session structure with the child and establishing routine moments should happen to help the child manage their emotions and behaviors, through drawing, images, verbalization, repeated actions and definitions of spaces and materials. 66. The description of observable emotions and behaviors of the child should be used whenever there is a need to help the child to self-regulate. 67. The therapist’s tonic receptiveness should induce the child’s emotional safety, interaction, and communication, through the psychomotor therapist’s posture, looking from the child’s eye-level, and being in synchrony with the verbal and non-verbal communication and tone of voice. |
87. The psychomotor therapist should resort to supervision/tutoring and continuous training based on scientific evidence. |
90. The psychomotor therapist should actively observe or participate with the child. 91. The psychomotor therapist’s approach should be directive or non-directive, according to the characteristics of the children and the therapeutic goals. 92. The psychomotor therapist should establish an authentic and safe therapeutic relationship. 93. The limits/rules actively defined by the group should be known to all group elements, whenever necessary. 94. The facilitation of group activities should provide for the participation of all group elements, making the necessary adaptations so that all children can demonstrate their abilities, and welcoming different forms of performance. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frazão, A.; Santos, S.; Rodrigues, A.; Brandão, T.; Simões, C.; Lebre, P. Consensus on the Best Practice Guidelines for Psychomotor Intervention in Preschool Children with Autism Spectrum Disorder. Children 2022, 9, 1778. https://doi.org/10.3390/children9111778
Frazão A, Santos S, Rodrigues A, Brandão T, Simões C, Lebre P. Consensus on the Best Practice Guidelines for Psychomotor Intervention in Preschool Children with Autism Spectrum Disorder. Children. 2022; 9(11):1778. https://doi.org/10.3390/children9111778
Chicago/Turabian StyleFrazão, Adriana, Sofia Santos, Ana Rodrigues, Teresa Brandão, Celeste Simões, and Paula Lebre. 2022. "Consensus on the Best Practice Guidelines for Psychomotor Intervention in Preschool Children with Autism Spectrum Disorder" Children 9, no. 11: 1778. https://doi.org/10.3390/children9111778