

A Multicenter Study Evaluating the Discontinuation of Eculizumab Therapy in Children with Atypical Hemolytic Uremic Syndrome
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Gene Mutation and Relapse
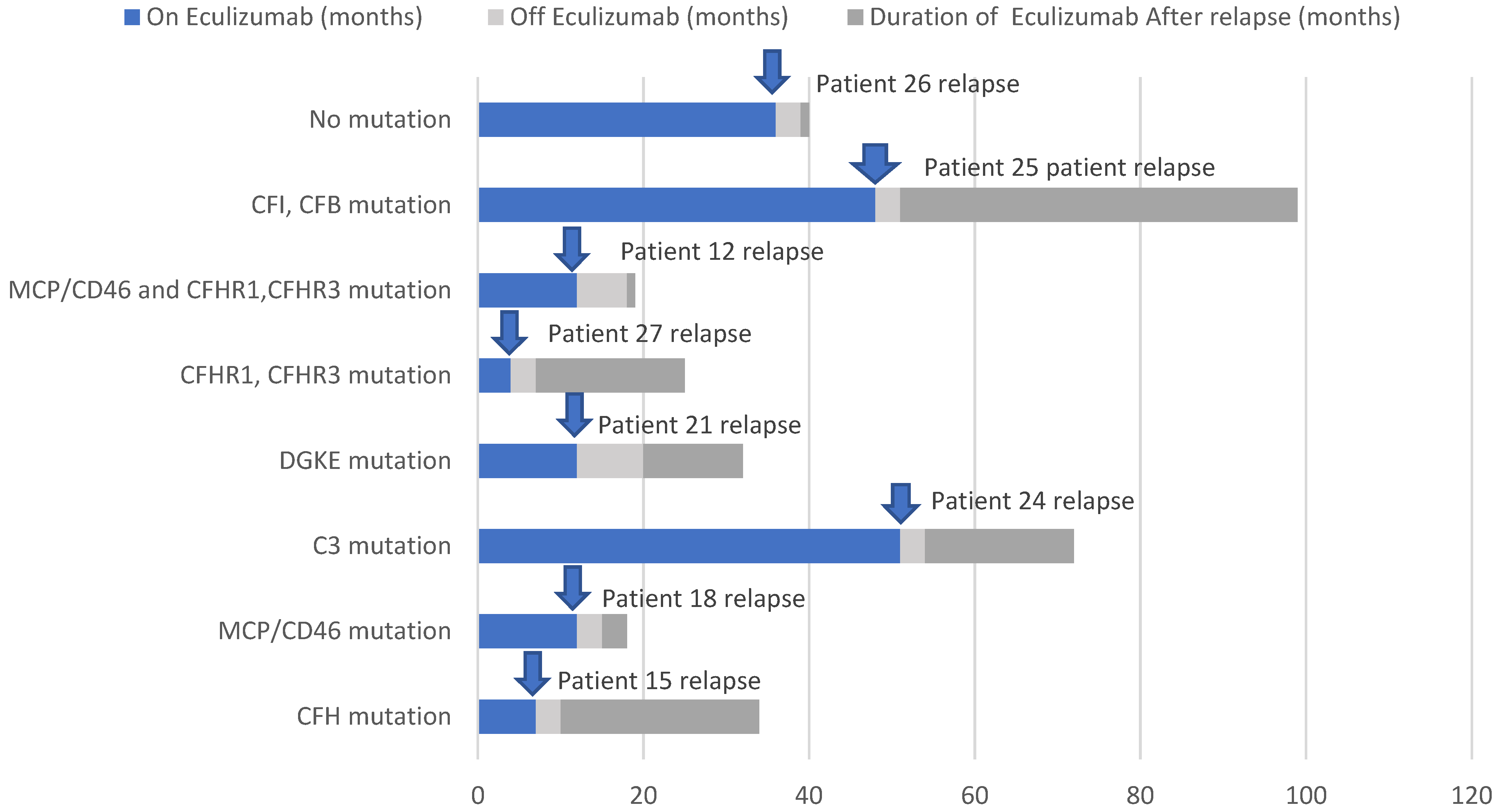
3.3. Relapse of aHUS
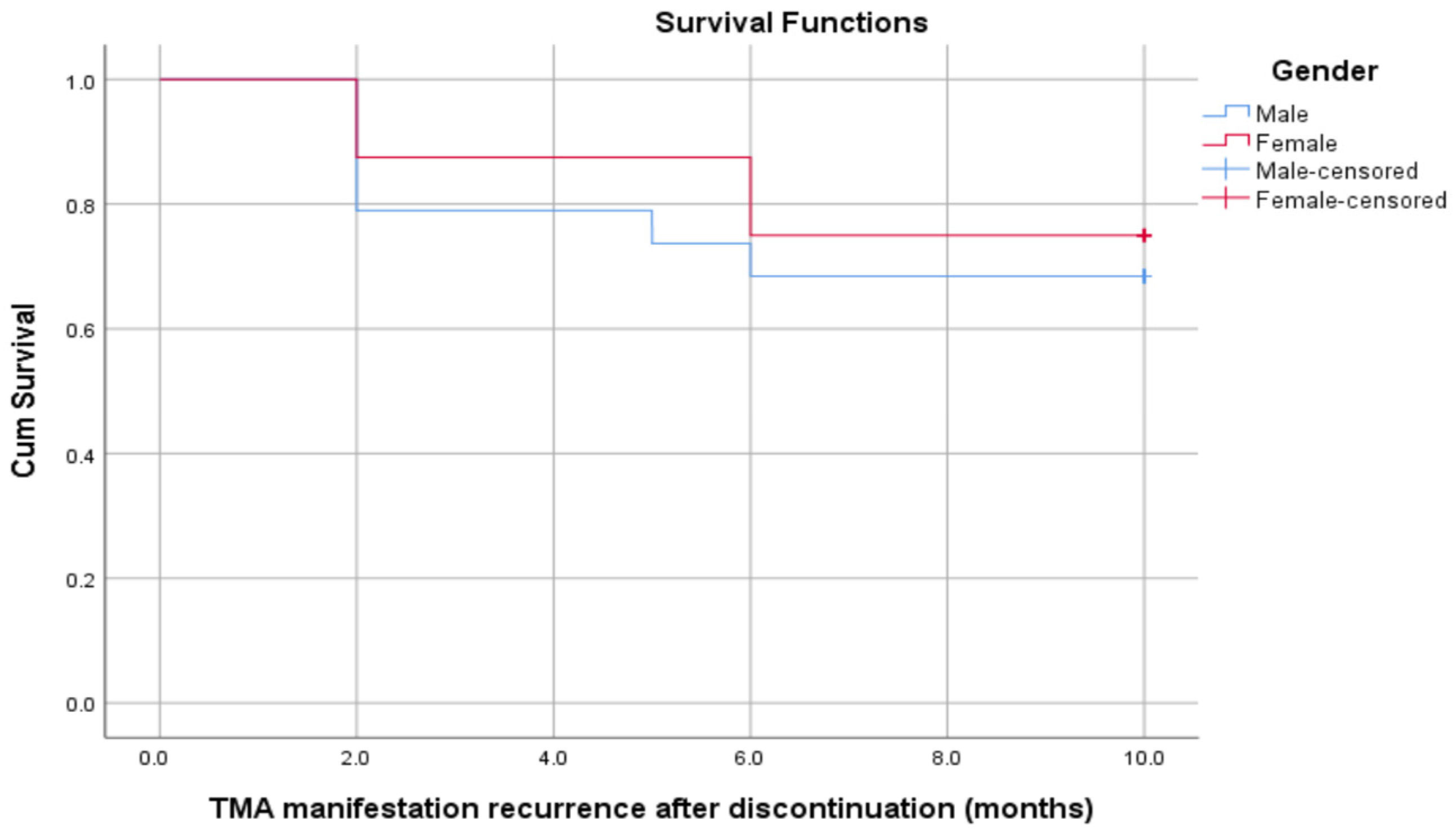
3.4. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ardissino, G.; Testa, S.; Possenti, I.; Tel, F.; Paglialonga, F.; Salardi, S.; Tedeschi, S.; Belingheri, M.; Cugno, M. Discontinuation of Eculizumab Maintenance Treatment for Atypical Hemolytic Uremic Syndrome: A Report of 10 Cases. Am. J. Kidney Dis. 2014, 64, 633–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, Y.; Kato, H.; Ikeda, Y.; Nangaku, M. Pathogenesis of Atypical Hemolytic Uremic Syndrome. J. Atheroscler. Thromb. 2019, 26, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijnsma, K.L.; Duineveld, C.; Volokhina, E.B.; Heuvel, L.P.V.D.; Kar, N.C.A.J.V.D.; Wetzels, J.F.M. Safety and effectiveness of restrictive eculizumab treatment in atypical haemolytic uremic syndrome. Nephrol. Dial. Transplant. 2017, 33, 635–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Kang, E.; Kang, H.G.; Kim, Y.H.; Kim, J.S.; Kim, H.-J.; Moon, K.C.; Ban, T.H.; Oh, S.W.; Jo, S.K.; et al. Consensus regarding diagnosis and management of atypical hemolytic uremic syndrome. Korean J. Intern. Med. 2020, 35, 25–40. [Google Scholar] [CrossRef] [Green Version]
- Raina, R.; Krishnappa, V.; Blaha, T.; Kann, T.; Hein, W.; Burke, L.; Bagga, A. Atypical Hemolytic-Uremic Syndrome: An Update on Pathophysiology, Diagnosis, and Treatment. Ther. Apher. Dial. 2018, 23, 4–21. [Google Scholar] [CrossRef] [Green Version]
- Menne, J.; Delmas, Y.; Fakhouri, F.; Licht, C.; Lommelé, Å.; Minetti, E.E.; Provôt, F.; Rondeau, E.; Sheerin, N.S.; Wang, J.; et al. Outcomes in patients with atypical hemolytic uremic syndrome treated with eculizumab in a long-term observational study. BMC Nephrol. 2019, 20, 125. [Google Scholar] [CrossRef] [Green Version]
- Siedlecki, A.M.; Isbel, N.; Walle, J.V.; Eggleston, J.J.; Cohen, D.J.; Licht, C.; Frémeaux-Bacchi, V.; Ariceta, G.; Ardissino, G.; Fakhouri, F.; et al. Eculizumab Use for Kidney Transplantation in Patients with a Diagnosis of Atypical Hemolytic Uremic Syndrome. Kidney Int. Rep. 2018, 4, 434–446. [Google Scholar] [CrossRef] [Green Version]
- Merrill, S.A.; Brittingham, Z.D.; Yuan, X.; Moliterno, A.R.; Sperati, C.J.; Brodsky, R.A. Eculizumab cessation in atypical hemolytic uremic syndrome. Blood 2017, 130, 368–372. [Google Scholar] [CrossRef] [Green Version]
- Loirat, C.; HUS International; Fakhouri, F.; Ariceta, G.; Besbas, N.; Bitzan, M.; Bjerre, A.; Coppo, R.; Emma, F.; Johnson, S.; et al. An international consensus approach to the management of atypical hemolytic uremic syndrome in children. Pediatr. Nephrol. 2015, 31, 15–39. [Google Scholar] [CrossRef]
- Fakhouri, F.; Fila, M.; Hummel, A.; Ribes, D.; Sellier-Leclerc, A.-L.; Ville, S.; Pouteil-Noble, C.; Coindre, J.-P.; Le Quintrec, M.; Rondeau, E.; et al. Eculizumab discontinuation in children and adults with atypical hemolytic-uremic syndrome: A prospective multicenter study. Blood 2021, 137, 2438–2449. [Google Scholar] [CrossRef]
- Olson, S.R.; Lu, E.; Sulpizio, E.; Shatzel, J.J.; Rueda, J.F.; Deloughery, T.G. When to Stop Eculizumab in Complement-Mediated Thrombotic Microangiopathies. Am. J. Nephrol. 2018, 48, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Bamhraz, A.A.; Rahim, K.A.; Faqeehi, H.Y.; Alanazi, A. Improved Renal Recovery with Eculizumab Therapy among Children with High Prevalence of Mutation-Associated Atypical Hemolytic Uremic Syndrome: A Retrospective Cohort Study. Kidney Blood Press. Res. 2020, 45, 939–954. [Google Scholar] [CrossRef]
- Macia, M.; Moreno, F.D.A.; Dutt, T.; Fehrman, I.; Hadaya, K.; Gasteyger, C.; Heyne, N. Current evidence on the discontinuation of eculizumab in patients with atypical haemolytic uraemic syndrome. Clin. Kidney J. 2016, 10, 310–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzabli, S.M.; Al Anazi, A.; Rahman, M.A.U.; Rahim, K.A. Complete Renal Recovery Following Delayed Therapy with Eculizumab in Atypical Hemolytic Uremic Syndrome. Asian J. Pediatr. Nephrol. 2019, 2, 25–30. Available online: www.ajpn-online.org (accessed on 15 July 2018).
- Fakhouri, F.; Fila, M.; Provôt, F.; Delmas, Y.; Barbet, C.; Châtelet, V.; Rafat, C.; Cailliez, M.; Hogan, J.; Servais, A.; et al. Pathogenic Variants in Complement Genes and Risk of Atypical Hemolytic Uremic Syndrome Relapse after Eculizumab Discontinuation. Clin. J. Am. Soc. Nephrol. 2016, 12, 50–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noris, M.; Caprioli, J.; Bresin, E.; Mossali, C.; Pianetti, G.; Gamba, S.; Daina, E.; Fenili, C.; Castelletti, F.; Sorosina, A.; et al. Relative Role of Genetic Complement Abnormalities in Sporadic and Familial aHUS and Their Impact on Clinical Phenotype. Clin. J. Am. Soc. Nephrol. 2010, 5, 1844–1859. [Google Scholar] [CrossRef] [Green Version]
- Ariceta, G.; Fakhouri, F.; Sartz, L.; Miller, B.; Nikolaou, V.; Cohen, D.; Siedlecki, A.M.; Ardissino, G. Eculizumab discontinuation in atypical haemolytic uraemic syndrome: TMA recurrence risk and renal outcomes. Clin. Kidney J. 2021, 14, 2075–2084. [Google Scholar] [CrossRef]
- Khedraki, R.; Noor, Z.; Rick, J. The Most Expensive Drug in the World: To Continue or Discontinue, That Is the Question. Fed. Pract. 2016, 33, 22. [Google Scholar]
- Rodriguez, E.; Barrios, C.; Soler, M.J. Should eculizumab be discontinued in patients with atypical hemolytic uremic syndrome? Clin. Kidney J. 2017, 10, 320–322. [Google Scholar] [CrossRef] [Green Version]
- Vilalta, R.; Lara, E.; Madrid, A.; Chocron, S.; Muñoz, M.; Casquero, A.; Nieto, J. Long-term eculizumab improves clinical outcomes in atypical hemolytic uremic syndrome. Pediatr. Nephrol. 2012, 27, 2323–2326. [Google Scholar] [CrossRef] [Green Version]
- Licht, C.; Ardissino, G.; Ariceta, G. Characteristics of 521 adult and pediatric patients in the Global aHUS Registry. In Proceedings of the American Society of Nephrology (ASN) Kidney Week 2014 Annual Meeting, Philadelphia, PA, USA, 11–16 November 2014. [Google Scholar]
- Sheerin, N.S.; Kavanagh, D.; Goodship, T.H.J.; Johnson, S. A national specialized service in England for atypical haemolytic uraemic syndrome-the first year’s experience. QJM 2016, 109, 27–33. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pt # | Sex | Age at Onset | Familial Consanguinity | Family history of aHUS | Hemoglobin on Presentation g/dL | Platelets on Presentation 109/L | LDH on Presentation (U/L) | Creatinine on Presentation µm/L | GFR mL/min/1.73 m2 on Presentation | C3 Level on Presentation | Hypertensive | Timing of Eculizumab (After Presentation) | Acute Dialysis on Presentation | Duration While on Eculizumab (Months) before Discontinuation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 54 m | No | Negative | 7.00 | 86,000 | 3539 | 174 | 45 | Normal | No | 1 day | Yes | 2 27 |
| 2 | F | 6 m | No | Sibling | 7.60 | 86,000 | 3616 | 278 | 35 | Normal | Yes | 2 days | Yes | 3 |
| 3 | M | 6 y | Yes | Cousin | 10.00 | 73,000 | 2008 | 191 | 40 | Low | Yes | 1 day | No | 3 |
| 4 | M | 6 y | Yes | Cousin | 8.90 | 50,000 | 3370 | 282 | 20 | Low | Yes | 1 day | Yes | 6 |
| 5 | M | 4 y | Yes | Cousin | 7.80 | 35,000 | 2182 | 169 | 25 | Low | No | 2 days | Yes | 2 |
| 6 | F | 6 y | Yes | Negative | 10.00 | 71,000 | 1780 | 38 | 100 | Normal | No | 1 day | No | 10 |
| 7 | F | 20 m | Yes | Negative | 6.20 | 46,000 | 2621 | 441 | 20 | Normal | No | 1 day | No | 26 |
| 8 | M | 7 y | Yes | Negative | 8.00 | 41,000 | 2991 | 207 | 35 | Normal | Yes | 30 days | Yes | 12 |
| 9 | F | 2 y | Yes | Negative | 7.80 | 77,000 | 2336 | 275 | 20 | Normal | No | 2 days | Yes | 6 |
| 10 | M | 14 m | No | Negative | 5.00 | 11,000 | 3531 | 137 | 22 | Low | No | 1 day | Yes | 19 |
| 11 | M | 9 m | Yes | Negative | 8.10 | 167,000 | 551 | 97 | 95 | Normal | Yes | NA | No | 2 |
| 12 | F | 3 y | No | Negative | 10.60 | 44,000 | 2242 | 164 | 27 | Low | No | 3 days | No | 12 |
| 13 | M | 3 m | Yes | Cousin | 5.20 | 53,000 | 1840 | 300 | 18 | Normal | Yes | 9 years | Yes | 15 |
| 14 | F | 3 m | Yes | Cousin | 8.60 | 92,000 | 1760 | 300 | 19 | Normal | Yes | 5 years | Yes | 15 |
| 15 | M | 10 m | Yes | Negative | 7.50 | 200,000 | 400 | 252 | 20 | Normal | Yes | 5 days | No | 7 |
| 16 | M | 5 y | Yes | Negative | 12.00 | 282,000 | 379 | 160 | 25 | Low | Yes | 3 months | Yes | 12 |
| 17 | 5 y | No | Negative | 9.10 | 96,000 | 391 | 203 | 28 | Low | Yes | 7 days | No | 11 | |
| 18 | M | 7 y | Yes | Negative | 8.20 | 13,000 | 4020 | 195 | 24 | Low | Yes | 7 days | Yes | 12 |
| 19 | M | 2 y | No | Negative | 8.70 | 6000 | 4848 | 393 | 20 | Normal | No | 5 days | Yes | 5 |
| 20 | F | 4 y | Yes | Negative | 9.30 | 121,000 | 631 | 291 | 16 | Low | No | 1 week | No | 4 |
| 21 | M | 1 m | Yes | Sibling | 6.20 | 32,000 | 1118 | 709 | 12 | Low | Yes | 7 days | No | 12 |
| 22 | M | 9 y | Yes | Negative | 5.80 | 81,000 | 776 | 511 | 16 | Low | No | 3 days | Yes | 20 |
| 23 | M | 11 y | No | Sibling | 12.10 | 59,000 | 3274 | 504 | 17 | Low | Yes | 72 h | Yes | 48 |
| 24 | M | 9 m | Yes | Sibling | 7.50 | 47,000 | 1023 | 80 | 16 | Normal | Yes | 7 days | Yes | 51 |
| 25 | M | 20 m | Yes | Cousin | 7.70 | 321,000 | 433 | 165 | 24 | Low | Yes | 4 months | No | 48 |
| 26 | M | 10 m | Yes | Sibling | 6.10 | 70,000 | 519 | 101 | 29 | Low | Yes | 4 days | Yes | 36 |
| 27 | F | 4 y | No | Negative | 8.60 | 23,000 | 1896 | 182 | 20 | Low | Yes | 4 days | Yes | 4 |
| 28 | F | 2 m | Yes | Negative | 7.70 | 104,000 | 4904 | 80 | 23 | Normal | No | 59 days | Yes | 5 |
| Pt # | Genetic Testing Result | Variant Nomenclature | Zygosity | Variant Classification | Relapse | Outcome |
|---|---|---|---|---|---|---|
| 1 | No mutation | NA | NA | NA | No | In remission |
| 2 | No mutation | NA | NA | NA | No | In remission |
| 3 | MCP/CD46 CFHR1, CFHR3 mutation | c.736T > A; p.Phe246Ile Whole genes deletion | Homozygous Homozygous | VOUS VOUS | No | In remission |
| 4 | CFHR1, CFHR3 mutation | Whole genes deletion | Homozygous | VOUS | No | In remission |
| 5 | No mutation | NA | NA | NA | No | In remission |
| 6 | No mutation | NA | NA | NA | No | In remission |
| 7 | No mutation | NA | NA | NA | No | In remission |
| 8 | No mutation | NA | NA | NA | No | In remission |
| 9 | Not done | NA | NA | NA | No | In remission |
| 10 | CFH mutation | c.2195C > T; p.Thr732Met | Heterozygous | VOUS | No | In remission |
| 11 | CFHR1, CFHR3 mutation | Whole genes deletion | Homozygous | VOUS | No | In remission |
| 12 | CD46 CFHR1-CFHR3 mutation | c.350_351dup;p.Glu118Thrfs17 Whole genes deletion | Homozygous Homozygous | Likely pathogenic VOUS | Yes | In remission |
| 13 | DGKE mutation | No | CKD | |||
| 14 | DGKE mutation | No | CKD | |||
| 15 | CFH mutation | c.3545G > T; p.Arg118Met | Heterozygous | VOUS | Yes | Transplant |
| 16 | CFHR1, CFHR3 mutation | Whole genes deletion | Heterozygous | VOUS | No | In remission |
| 17 | No mutation | NA | NA | NA | No | CKD |
| 18 | MCP/CD46 mutation | c.608T > C; p.Ile203Thr | Homozygous | VOUS | Yes | In remission |
| 19 | CFHR1, CFHR3 mutation | Whole genes deletion | Homozygous | VOUS | No | In remission |
| 20 | CFHR1, CFHR3 mutation | Whole genes deletion | Heterozygous | VOUS | No | In remission |
| 21 | DGKE | c.413 G > A (p.Cys138Tyr) | Homozygous | Likely pathogenic | Yes | CKD |
| 22 | No mutation | NA | NA | NA | No | In remission |
| 23 | MCP/CD46 CFI | c.736T > A (p.Phe246Ile) c.540 A > G (p.Glu180Glu) | Homozygous Heterozygous | VOUS VOUS | No | In remission |
| 24 | C3 mutation | c.3326 T > G (P.leu1109 Arg) | Homozygous | Likely pathogenic | Yes | In remission |
| 25 | C3 CFB CFI | c.3326T > G (p. Leu1109Arg) c.1697A > C (p. Glu566Ala) c.1246A > C (p. Ile416 Leu) | Heterozygous Heterozygous Homozygous | VOUS Likely pathogenic Pathogenic | Yes | In remission |
| 26 | No mutation | NA | NA | NA | Yes | In remission |
| 27 | CFHR1, CFHR3 mutation | Whole genes deletion | Homozygous | VOUS | Yes | In remission |
| 28 | CFHR1, CFHR3 mutation | Whole genes deletion | Homozygous | VOUS | No | In remission |
| Factor | With Relapse | No Relapse | p-Value |
|---|---|---|---|
| N (%) | N (%) | ||
| (n = 8) | (n = 20) | ||
| Age at onset HUS | |||
| 04 (50.0%) | 04 (20.0%) | 0.505 |
| 02 (25.0%) | 04 (20.0%) | |
| 01 (12.5%) | 05 (25.0%) | |
| 01 (12.5%) | 03 (15.0%) | |
| 0 | 04 (20.0%) | |
| Creatinine at presentation, micromole/L (mean ± SD) | 231.0 ± 200.4 | 251.6 ± 133.1 | 0.753 |
| C3 Level at the presentation | |||
| 05 (62.5%) | 09 (45.0%) | 0.678 |
| 03 (37.5%) | 11 (55.0%) | |
| Timing of eculizumab after the presentation | |||
| 0 | 07 (35.0%) | 0.252 |
| 03 (37.5%) | 04 (20.0%) | |
| 04 (50.0%) | 06 (30.0%) | |
| 01 (12.5%) | 03 (15.0%) | |
| Acute dialysis before eculizumab | |||
| 06 (75.0%) | 12 (60.0%) | 0.669 |
| 02 (25.0%) | 08 (40.0%) | |
| Duration while on eculizumab (months) | |||
| 0 | 04 (20.0%) | 0.23 |
| 01 (12.5%) | 05 (25.0%) | |
| 02 (25.0%) | 02 (10.0%) | |
| 01 (12.5%) | 06 (30.0%) | |
| 03 (37.5%) | 3 (5.0%) | |
| 01 (12.5%) | 0 | |
| Complement gene variants | |||
| 01 (12.5%) | 01 (05.0%) | 0.497 |
| 01 (12.5%) | 01 (05.0%) | 0.497 |
| 01 (12.5%) | 0 | 0.286 |
| 01 (12.5%) | 02 (10.0%) | 1.000 |
| 01 (12.5%) | 04 (20.0%) | 1.000 |
| 01 (12.5%) | 01 (05.0%) | 0.497 |
| 01 (12.5%) | 0 | 0.286 |
| 01 (12.5%) | 10 (50.0%) | 0.088 |
| Creatinine at time discontinuation of eculizumab | 63.7 ± 76.6 | 43.2 ± 19.9 | 0.267 |
| GFR at time of discontinuation of eculizumab (mean ± SD) | 101.9 ± 32.1 | 109.1 ± 16.5 | 0.700 |
| Protein/creatinine ratio (g/mmol) at time of discontinuation of eculizumab (median (min–max)) (mean ± SD) | 0.45 (0.01–1.90) | 0.50 (0.01–15) | 0.439 |
| Durations of eculizumab treatment in months, median (min–max) | 12.0 (4.0–51.0) | 10.5 (2.0–48.0) | 0.165 |
| GFR (mL/min/1.73 m2) at the last visit after discontinuation | |||
| 06 (75.0%) | 16 (80.0%) | |
| 01 (12.5%) | 02 (10.0%) | 1000 |
| 01 (12.5%) | 02 (10.0%) |
| Gene Mutations | Rate of Relapse | p-Value * | ||
|---|---|---|---|---|
| One N (%) | Two N (%) | Three N (%) | ||
| CFH mutation | 01 (20.0%) | 0 | 0 | 1.000 |
| MCP/CD46 mutation | 0 | 0 | 01 (100%) | 0.125 |
| C3 mutation | 01 (20.0%) | 0 | 0 | 1.000 |
| DGKE mutation | 0 | 01 (50.0%) | 0 | 0.375 |
| CFHR1, CFHR3 mutation | 01 (20.0%) | 0 | 0 | 1.000 |
| MCP/CD46 and CFHR1, CFHR3 mutation | 01 (20.0%) | 0 | 0 | 1.000 |
| CFI, CFB mutation | 0 | 01 (50.0%) | 0 | 0.375 |
| No mutation | 01 (20.0%) | 0 | 0 | 1.000 |
| Patient | Age at Initial Eculizumab Treatment (Years) | Mutation | Reason for Discontinuation Time | Time of Eculizumab before Discontinuation | Time of Relapse | Restarted Eculizumab | Outcome | Duration of Follow Up Months |
|---|---|---|---|---|---|---|---|---|
| Patient 12 | 6 years | MCP/CD46, CFHR1, CFHR3 mutation | Family preference | 12 months | 3 months | Yes | Stable (in remission) | 15 |
| Patient 15 | 6 years | CFH mutation | Stable patient and complete remission | 7 months | 3 months | Yes | Transplanted | 16 |
| Patient 18 | 7 years | MCP/CD46 mutation | Stable patient and complete remission | 12 months | 15 months | Yes | Stable (in remission) | 48 |
| Patient 21 | 14 months | DGKE mutation | DKGE mutation | 12 months | 12 months | Yes | CKD | 60 |
| Patient 24 | 3 months | C3 mutation | Genetic testing showed DKGE mutation | 51 months | 3 months | Yes | Stable (in remission) | 30 |
| Patient 25 | 3 months | CFI, CFB mutation | Genetic testing showed DKGE mutation | 48 months | 3 months | Yes | Stable (in remission) | 17 |
| Patient 26 | 2 years | No mutation | Insurance coverage | 36 months | 7 weeks | Yes | Stable (in remission) | 24 |
| Patient 27 | 9 months | CFHR1, CFHR3 mutation | Stable patient and complete remission | 4 months | 14 months | Yes | Stable (in remission) | 60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlZabali, S.; AlBatati, S.; Rahim, K.; Faqeehi, H.; Osman, A.; Bamhraz, A.; Saleh, M.A.; Kari, J.A.; Aloufi, M.; Eid, L.; et al. A Multicenter Study Evaluating the Discontinuation of Eculizumab Therapy in Children with Atypical Hemolytic Uremic Syndrome. Children 2022, 9, 1734. https://doi.org/10.3390/children9111734
AlZabali S, AlBatati S, Rahim K, Faqeehi H, Osman A, Bamhraz A, Saleh MA, Kari JA, Aloufi M, Eid L, et al. A Multicenter Study Evaluating the Discontinuation of Eculizumab Therapy in Children with Atypical Hemolytic Uremic Syndrome. Children. 2022; 9(11):1734. https://doi.org/10.3390/children9111734
Chicago/Turabian StyleAlZabali, Saeed, Sawsan AlBatati, Khawla Rahim, Hassan Faqeehi, Abubaker Osman, Abdulaziz Bamhraz, Mohammed A. Saleh, Jameela A. Kari, Majed Aloufi, Loai Eid, and et al. 2022. "A Multicenter Study Evaluating the Discontinuation of Eculizumab Therapy in Children with Atypical Hemolytic Uremic Syndrome" Children 9, no. 11: 1734. https://doi.org/10.3390/children9111734