
The Effectiveness of Sensory Integration Interventions on Motor and Sensory Functions in Infants with Cortical Vision Impairment and Cerebral Palsy: A Single Blind Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
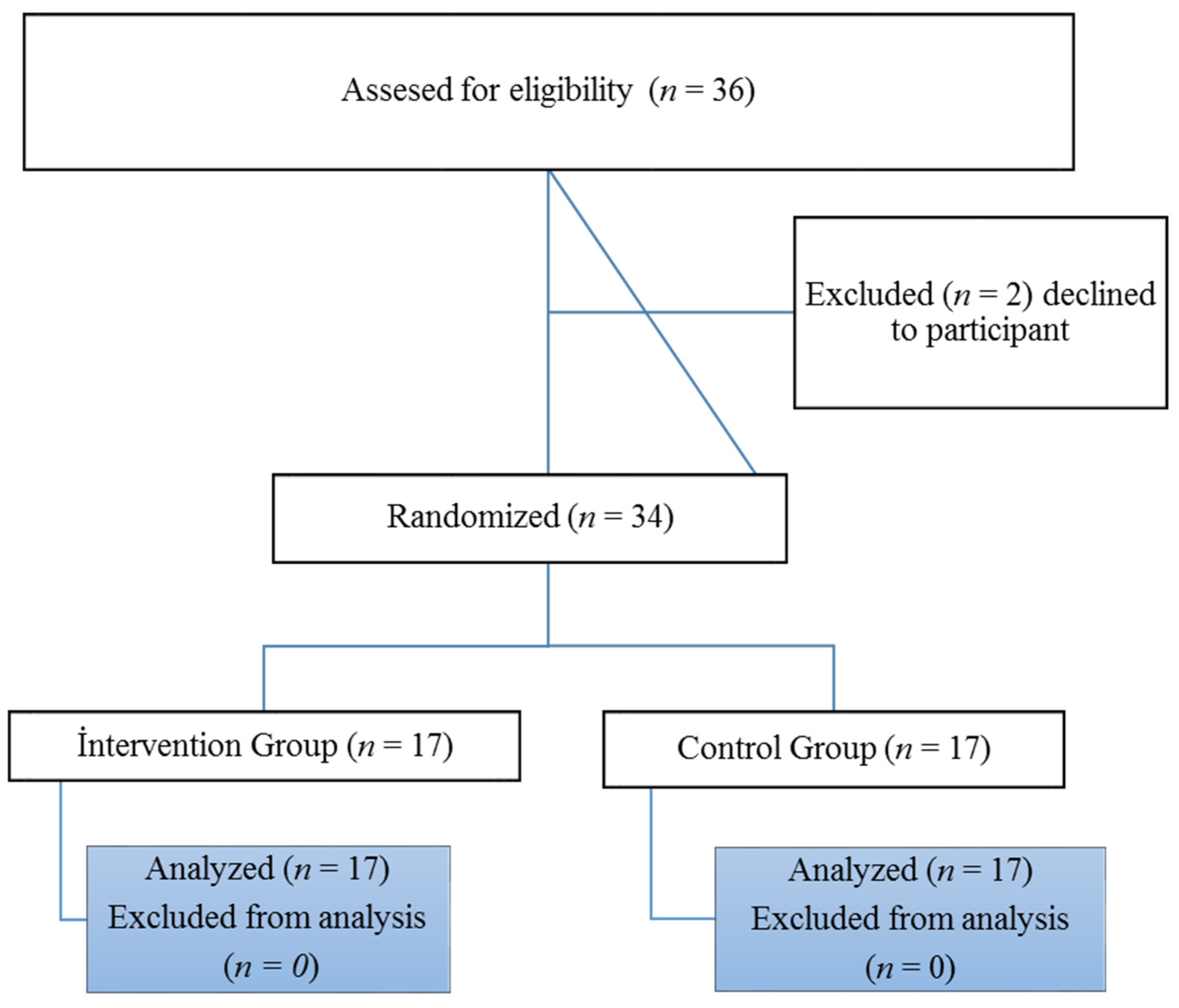
2.1. Participants
2.2. Instruments
2.2.1. Test of Sensory Functions in Infants (TSFI)
2.2.2. Alberta Infant Motor Scale (AIMS)
2.3. Intervention
2.4. Data Analysis
3. Results
4. Discussion
4.1. Sensory Processing
4.2. Motor Development
5. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blackstone, S.W.; Luo, F.; Canchola, J.; Wilkinson, K.M.; Roman-Lantzy, C. Children with cortical visual impairment and complex communication needs: Identifying gaps between needs and current practice. Lang. Speech Hear. Serv. Sch. 2021, 52, 612–629. [Google Scholar] [CrossRef] [PubMed]
- Philip, S.S.; Dutton, G.N. Identifying and characterising cerebral visual impairment in children: A review. Clin. Exp. Optom. 2014, 97, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Chorna, O.D.; Guzzetta, A.; Maitre, N.L. Vision assessments and interventions for infants 0–2 years at high risk for cerebral palsy: A systematic review. Pediatric Neurol. 2017, 76, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Philip, S.S.; Guzzetta, A.; Chorna, O.; Gole, G.; Boyd, R.N. Relationship between brain structure and cerebral visual impairment in children with cerebral palsy: A systematic review. Res. Dev. Disabil. 2020, 99, 103580. [Google Scholar] [CrossRef] [PubMed]
- Lehman, S.S. Cortical Visual Impairment in the Child with Cerebral Palsy. In Cerebral Palsy; Springer: Berlin/Heildeberg, Germany, 2020; pp. 1049–1055. [Google Scholar]
- Pavão, S.L.; Rocha, N.A.C.F. Sensory processing disorders in children with cerebral palsy. Infant Behav. Dev. 2017, 46, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Shams, A.A.; Holizas, M. Effect of sensory integration therapy on gross motor function in children with cerebral palsy. Iran. J. Child Neurol. 2009, 3, 43–48. [Google Scholar]
- Olfatian, Y.; Hemayattalab, R.; Bagherzadeh, F. Examine the effectiveness of sensory integration therapy approach on fine motor skills in children with spastic cerebral palsy. J. Mot. Learn. Mov. 2021. [Google Scholar] [CrossRef]
- Seyam, M.; Sherief, A.; Waly, M.I.; Kashoo, F.Z.; Elfakharany, M.S. Effect of sensory integration on gait for children with mild hemiplegic cerebral palsy. Egypt. J. Phys. Ther. 2021, 7, 1–6. [Google Scholar] [CrossRef]
- Abd El-Maksoud, G.M.; Gharib, N.M.M.; Hussein, R. Visual-based training program for motor functions in cerebral palsied children with cortical visual impairment. Int. J. Ther. Rehabil. Res. 2016, 5, 265–277. [Google Scholar]
- Edmond, J.C.; Foroozan, R. Cortical visual impairment in children. Curr. Opin. Ophthalmol. 2006, 17, 509–512. [Google Scholar] [CrossRef]
- Morse, M.T. Cortical Visual Impairment in Young Children with Multiple Disabilities. J. Vis. Impair. Blind. 1990, 84, 200–203. [Google Scholar] [CrossRef]
- Malkowicz, D.E.; Myers, G.; Leisman, G. Rehabilitation of cortical visual impairment in children. Int. J. Neurosci. 2006, 116, 1015–1033. [Google Scholar]
- Zhao, Z. Effects of visual impairment on sensory integration and new opportunities for inclusive e-learning managing. Int. J. Disabil. Dev. Educ. 2021, 68, 1–15. [Google Scholar] [CrossRef]
- Van Balen, L.C.; Dijkstra, L.J.; Dirks, T.; Bos, A.F.; Hadders-Algra, M. Early intervention and postural adjustments during reaching in infants at risk of cerebral palsy. Pediatric Phys. Ther. 2019, 31, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Ward, R.; Hennessey, N.; Barty, E.; Elliott, C.; Valentine, J.; Cantle Moore, R. Clinical utilisation of the Infant Monitor of vocal Production (IMP) for early identification of communication impairment in young infants at-risk of cerebral palsy: A prospective cohort study. Dev. Neurorehabilit. 2022, 25, 101–114. [Google Scholar] [CrossRef]
- Hielkema, T.; Hamer, E.G.; Boxum, A.G.; La Bastide-Van Gemert, S.; Dirks, T.; Reinders-Messelink, H.A.; Maathuis, C.G.; Verheijden, J.; Geertzen, J.H.; Hadders-Algra, M.; et al. Learn2move 0–2 years, a randomized early intervention trial for infants at very high risk of cerebral palsy: Neuromotor, cognitive, and behavioral outcome. Disabil. Rehabil. 2020, 42, 3752–3761. [Google Scholar] [CrossRef] [PubMed]
- Maitre, N.L.; Jeanvoine, A.; Yoder, P.J.; Key, A.P.; Slaughter, J.C.; Carey, H.; Needham, A.; Murray, M.M.; Heathcock, J. Kinematic and somatosensory gains in infants with cerebral palsy after a multi-component upper-extremity intervention: A randomized controlled trial. Brain Topogr. 2020, 33, 751–766. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Choi, Y.I. A systematic review and meta-analysis of sensory integration intervention studies in children with cerebral palsy. J. Digit. Converg. 2013, 11, 383–389. [Google Scholar]
- Chorna, O.; Heathcock, J.; Key, A.; Noritz, G.; Carey, H.; Hamm, E.; Nelin, M.A.; Murray, M.; Needham, A.; Slaughter, J.C.; et al. Early childhood constraint therapy for sensory/motor impairment in cerebral palsy: A randomised clinical trial protocol. BMJ J. 2015, 5, e010212. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Fergusson, D. CONSORT 2010 changes and testing blindness in RCTs. Lancet 2010, 375, 1144–1146. [Google Scholar] [CrossRef]
- DeGangi, G.A.; Greenspan, S.I. Test of Sensory Functions in Infants (TSFI); Western Psychological Services: Los Angeles, CA, USA, 1989. [Google Scholar]
- Arıcıkül, A. Adaptation of Sensory Function Test for Infants. Master’s Thesis, Marmara University Institute of Educational Sciences, Department of Special Education, İstanbul, Turkey, 2014. [Google Scholar]
- Amiel-Tison, C. Update of the Amiel-Tison neurologic assessment for the term neonate or at 40 weeks corrected age. Pediatric Neurol. 2002, 27, 196–212. [Google Scholar] [CrossRef]
- Piper, M.C.; Pinnell, L.E.; Darrah, J.; Maguire, T.; Byrne, P.J. Construction and validation of the Alberta Infant Motor Scale (AIMS). Can. J. Public Health Rev. Can. De Sante Publique 1992, 83, 46–50. [Google Scholar]
- Pekçetin, S.; Akı, E.; Üstünyurt, Z.; Kayıhan, H. The efficiency of sensory integration interventions in preterm infants. Percept. Mot. Ski. 2016, 123, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Parham, L.D.; Roley, S.S.; May-Benson, T.A.; Koomar, J.; Brett-Green, B.; Burke, J.P.; Cohn, E.S.; Mailloux, Z.; Miller, L.J.; Schaaf, R.C. Development of a fidelity measure for research on the effectiveness of the Ayres Sensory Integration® intervention. Am. J. Occup. Ther. 2011, 65, 133–142. [Google Scholar] [PubMed] [Green Version]
- Yakut, Y.; Özalp, Ö.; Habibzadeh, A.; Gürşen, C.; Yagci, G. Better presentation of the intervention: The Template for Intervention Description and Replication (TIDieR) checklist and guide. J. Exerc. Ther. Rehabil. 2020, 7, 302–320. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- Kashoo, F.Z.; Ahmad, M. Effect of sensory integration on attention span among children with infantile hemiplegia. Int. J. Health Sci. 2019, 13, 29. [Google Scholar]
- Ju, J.O.; Lee, H.R.; Kim, K.M. The effects of sensory integrative intervention on the self-regulation capacities of children with cerebral palsy: Single-subject research design. J. Korean Acad. Sens. Integr. 2011, 9, 15–28. [Google Scholar]
- Hsieh, H.Y.; Chen, L.Y.; Ko, K.L.; Liu, H.H.; Chou, W.J.; Chou, M.C.; Tsai, C.S.; Wang, L.J. Adjunctive sensory integration therapy for children with developmental disabilities in a family-based early intervention program. Taiwan J. Psychiatry 2020, 34, 121. [Google Scholar]
- Lecuona, E.; Van Jaarsveld, A.; van Jaarsveld, J.; Van Heerden, R. Sensory integration intervention and the development of the premature infant: A controlled trial. South Afr. Med. J. 2017, 107, 976–982. [Google Scholar]
- Kayihan, H.; Bumin, G. Effectiveness of two different sensory-integration programmes for children with spastic diplegic cerebral palsy. Disabil. Rehabil. 2001, 23, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Papadelis, C.; Ahtam, B.; Nazarova, M.; Nimec, D.; Snyder, B.; Grant, P.E.; Okada, Y. Cortical somatosensory reorganization in children with spastic cerebral palsy: A multimodal neuroimaging study. Front. Hum. Neurosci. 2014, 8, 725. [Google Scholar] [PubMed]
- Auld, M.L.; Ware, R.S.; Boyd, R.N.; Moseley, G.L.; Johnston, L.M. Reproducibility of tactile assessments for children with unilateral cerebral palsy. Phys. Occup. Ther. Pediatrics 2012, 32, 151–166. [Google Scholar]
- Sanger, T.D.; Kukke, S.N. Abnormalities of tactile sensory function in children with dystonic and diplegic cerebral palsy. J. Child Neurol. 2007, 22, 289–293. [Google Scholar] [CrossRef]
- Auld, M.L.; Ware, R.S.; Boyd, R.N.; Moseley, G.L.; Johnston, L.M. Tactile assessment in children with cerebral palsy: A clinimetric review. Phys. Occup. Ther. Pediatrics 2011, 31, 413–439. [Google Scholar] [CrossRef]
- Cumurcu, T.; Cumurcu, H.B.; Erkorkmaz, Ü.; Yardim, H. Ocular findings in children with cerebral palsy. Fırat J. Med. 2007, 12, 48–52. [Google Scholar]
- Clayton, K.; Fleming, J.M.; Copley, J. Behavioral responses to tactile stimuli in children with cerebral palsy. Phys. Occup. Ther. Pediatrics 2003, 23, 43–62. [Google Scholar] [CrossRef]
- Dusing, S.C.; Harbourne, R.T.; Lobo, M.A.; Westcott-McCoy, S.; Bovaird, J.A.; Kane, A.E.; Syed, G.; Marcinowski, E.C.; Koziol, N.A.; Brown, S.E. A physical therapy intervention to advance cognitive and motor skills: A single subject study of a young child with cerebral palsy. Pediatric Phys. Ther. 2019, 31, 347–352. [Google Scholar] [CrossRef]
- Park, E.Y.; Kim, W.H. Effect of neurodevelopmental treatment-based physical therapy on the change of muscle strength, spasticity, and gross motor function in children with spastic cerebral palsy. J. Phys. Ther. Sci. 2017, 29, 966–969. [Google Scholar]
- Velasco, M.A.; Raya, R.; Muzzioli, L.; Morelli, D.; Otero, A.; Iosa, M.; Cincotti, F.; Rocon, E. Evaluation of cervical posture improvement of children with cerebral palsy after physical therapy based on head movements and serious games. Biomed. Eng. Online 2017, 16, 74. [Google Scholar] [CrossRef] [Green Version]
- Das, S.P.; Ganesh, G.S. Evidence-based approach to physical therapy in cerebral palsy. Indian J. Orthop. 2019, 53, 20. [Google Scholar] [CrossRef] [PubMed]
- Bumin, G.; Kavak, S.T. An investigation of the factors affecting handwriting performance in children with hemiplegic cerebral palsy. Disabil. Rehabil. 2008, 30, 1374–1385. [Google Scholar] [CrossRef] [PubMed]
- Shams, A.A. Comparison between the effect of neurodevelopmental treatment and sensory integration therapy on gross motor function in children with cerebral palsy. Iran. J. Child Neurol. 2010, 4, 31–38. [Google Scholar]
- Mahaseth, P.K.; Choudhary, A. Sensory Integration Therapy Verses Conventional Physical Therapy Among Children with Cerebral Palsy on Gross Motor Function—A Comparative Randomized Controlled Trial. Ann. Rom. Soc. Cell Biol. 2021, 25, 17315–17334. [Google Scholar]
- Arslan, C.; Ünsal, E.; Sezer, K.Ş.; Tarakci, D. Investigation of the Effect of Structured Neurodevelopmental Therapy and Sensory Integration Approaches on Sitting Balance in Children with Cerebral Palsy. Haliç Univ. J. Health Sci. 2020, 3, 107–116. [Google Scholar]


{kind=link}
| Intervention Group | Control Group | p | ||||
|---|---|---|---|---|---|---|
| n = 17 | % | n = 17 | % | |||
| Gender | Female | 5 | 29.4% | 11 | 64.7% | 0.7154 |
| Male | 12 | 70.6% | 6 | 35.3% | ||
| Gestational week | Less than 37 weeks | 9 | 52.9% | 10 | 58.8% | 0.730 |
| 37 weeks and later | 8 | 47.1% | 7 | 41.2% | ||
| Diagnosis | Spastic CP | 0 | 0% | 3 | 17.7% | 0.147 |
| Dystonic CP | 4 | 30.7% | 5 | 29.4% | ||
| Hypotonic CP | 13 | 69.3% | 9 | 52.9% | ||
| Intervention Group (n = 17) | Control Group (n = 17) | p | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Response to tactile deep pressure | 2.94 ± 1.08 | 2.94 ± 0.96 | 0.986 |
| Adaptive motor functions | 3.52 ± 1.37 | 3.82 ± 1.23 | 0.423 |
| Visual–tactile integration | 3.47 ± 1.37 | 2.94 ± 1.08 | 0.296 |
| Oculomotor control | 0.70 ± 0.58 | 0.41 ± 0.50 | 0.141 |
| Response to vestibular stimuli | 3.41 ± 1.22 | 3.52 ± 1.,12 | 0.886 |
| TSFI total score | 14.05 ± 4.22 | 13.64 ± 3.49 | 0.809 |
| AIMS | 19.64 ± 8.14 | 13.76 ± 7.20 | 0.054 |
| Intervention Group | Control Group | Between-Group Comparison | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline Assessment Mean ± SD | Final Assessment Mean ± SD | p | Cohen’s d | Baseline Assessment Mean ± SD | Final Assessment Mean ± SD | p | Cohen’s d | F | p | d | |
| Response to tactile deep pressure | 2.94 ± 1.08 | 6.35 ± 1.41 | <0.001 | 3.139 | 2.94 ± 0.96 | 3.94 ± 0.96 | <0.001 | 1.877 | 81.48 | <0.001 * | 0.691 |
| Adaptive motor functions | 3.52 ± 1.37 | 7.82 ± 2.78 | <0.001 | 2.464 | 3.82 ± 1.23 | 4.70 ± 1.26 | <0.001 | 2.383 | 67.52 | <0.001 * | 0.595 |
| Visual–tactile integration | 3.47 ± 1.37 | 6.64 ± 1.36 | <0.001 | 2.959 | 2.94 ± 1.08 | 3.52 ± 1.17 | <0.001 | 0.902 | 107.21 | <0.001 * | 0.734 |
| Oculomotor control | 0.7 ± 0.58 | 1.52 ± 0.51 | <0.001 | 2.238 | 0.41 ± 0.5 | 1.41 ± 0.71 | <0.001 | 2.351 | 1.50 | 0.228 | 0.039 |
| Response to vestibular stimuli | 3.41 ± 1.22 | 6.94 ± 1.81 | <0.001 | 3.521 | 3.52 ± 1.12 | 4.35 ± 1.45 | <0.001 | 0.913 | 62.77 | <0.001 * | 0.670 |
| TSFI total score | 14.05 ± 4.22 | 29.29 ± 6.84 | <0.001 | 4.654 | 13.64 ± 3.49 | 17.94 ± 3.49 | <0.001 | 2.138 | 199.53 | <0.001 * | 0.759 |
| AIMS | 19.64 ± 8.14 | 20.94 ± 8.79 | <0.001 | 1.213 | 13.76 ± 7.20 | 14.94 ± 8 | <0.001 | 1.226 | 1.22 | 0.276 | 0.003 |
| Variable | Intervention Group (n = 17) | Control Group (n = 17) | p |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Response to tactile deep pressure | 6.35 ± 1.41 | 3.94 ± 0.96 | <0.001 * |
| Adaptive motor functions | 7.82 ± 2.78 | 4.70 ± 1.26 | <0.001 * |
| Visual–tactile integration | 6.64 ± 1.36 | 3.52 ± 1.17 | <0.001 * |
| Oculomotor control | 1.52 ± 0.51 | 1.41 ± 0.71 | 0.755 |
| Response to vestibular stimuli | 6.94 ± 1.81 | 4.35 ± 1.45 | <0.001 * |
| TSFI total score | 29.29 ± 6.84 | 17.94 ± 3.49 | <0.001 * |
| AIMS | 20.94 ± 8.79 | 14.94 ± 8 | 0.078 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cemali, M.; Pekçetin, S.; Akı, E. The Effectiveness of Sensory Integration Interventions on Motor and Sensory Functions in Infants with Cortical Vision Impairment and Cerebral Palsy: A Single Blind Randomized Controlled Trial. Children 2022, 9, 1123. https://doi.org/10.3390/children9081123
Cemali M, Pekçetin S, Akı E. The Effectiveness of Sensory Integration Interventions on Motor and Sensory Functions in Infants with Cortical Vision Impairment and Cerebral Palsy: A Single Blind Randomized Controlled Trial. Children. 2022; 9(8):1123. https://doi.org/10.3390/children9081123
Chicago/Turabian StyleCemali, Mustafa, Serkan Pekçetin, and Esra Akı. 2022. "The Effectiveness of Sensory Integration Interventions on Motor and Sensory Functions in Infants with Cortical Vision Impairment and Cerebral Palsy: A Single Blind Randomized Controlled Trial" Children 9, no. 8: 1123. https://doi.org/10.3390/children9081123