
Clinical Manifestations of Neonatal Hyperbilirubinemia Are Related to Alterations in the Gut Microbiota


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. 16S rRNA Gene Sequencing
2.3. Gut Microbiota Analysis
3. Results
3.1. Participant Information and Composition
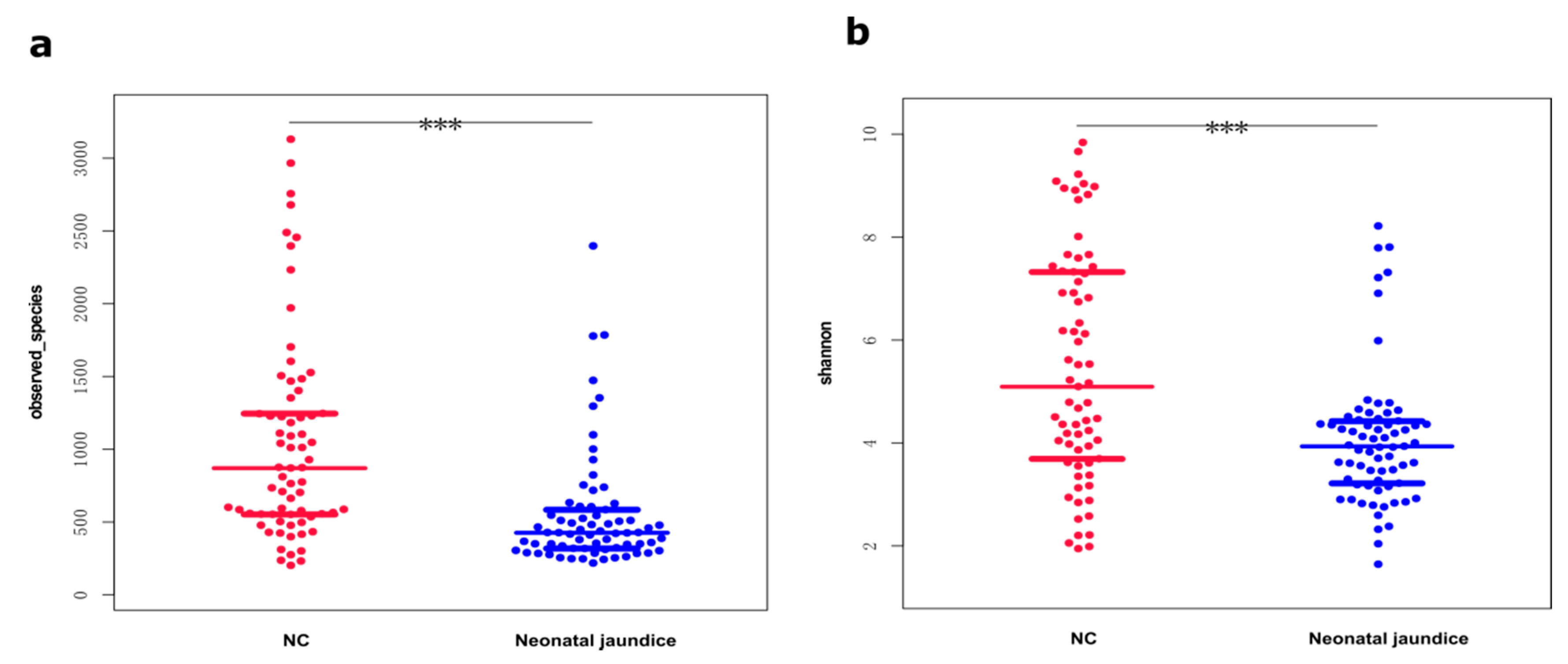
3.2. Shannon Diversity Indices Were Significantly Lower in the Gut Microbiotas of Neonates with Hyperbilirubinemia
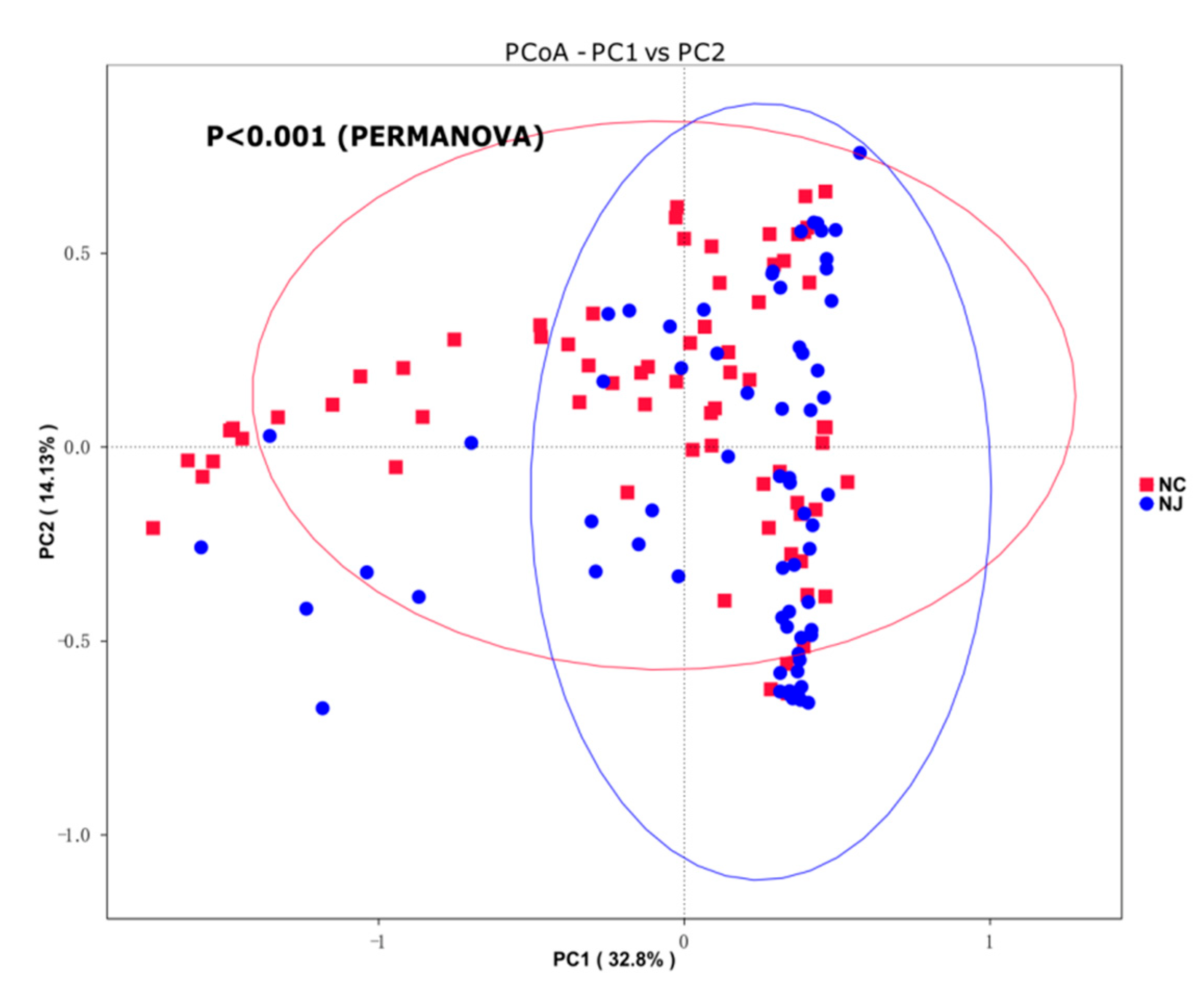
3.3. Species Compositions of Gut Microbiota Partially Distinguished Neonatal Hyperbilirubinemia
3.4. Significant Differences in Gut Microbiota Compositions between Groups
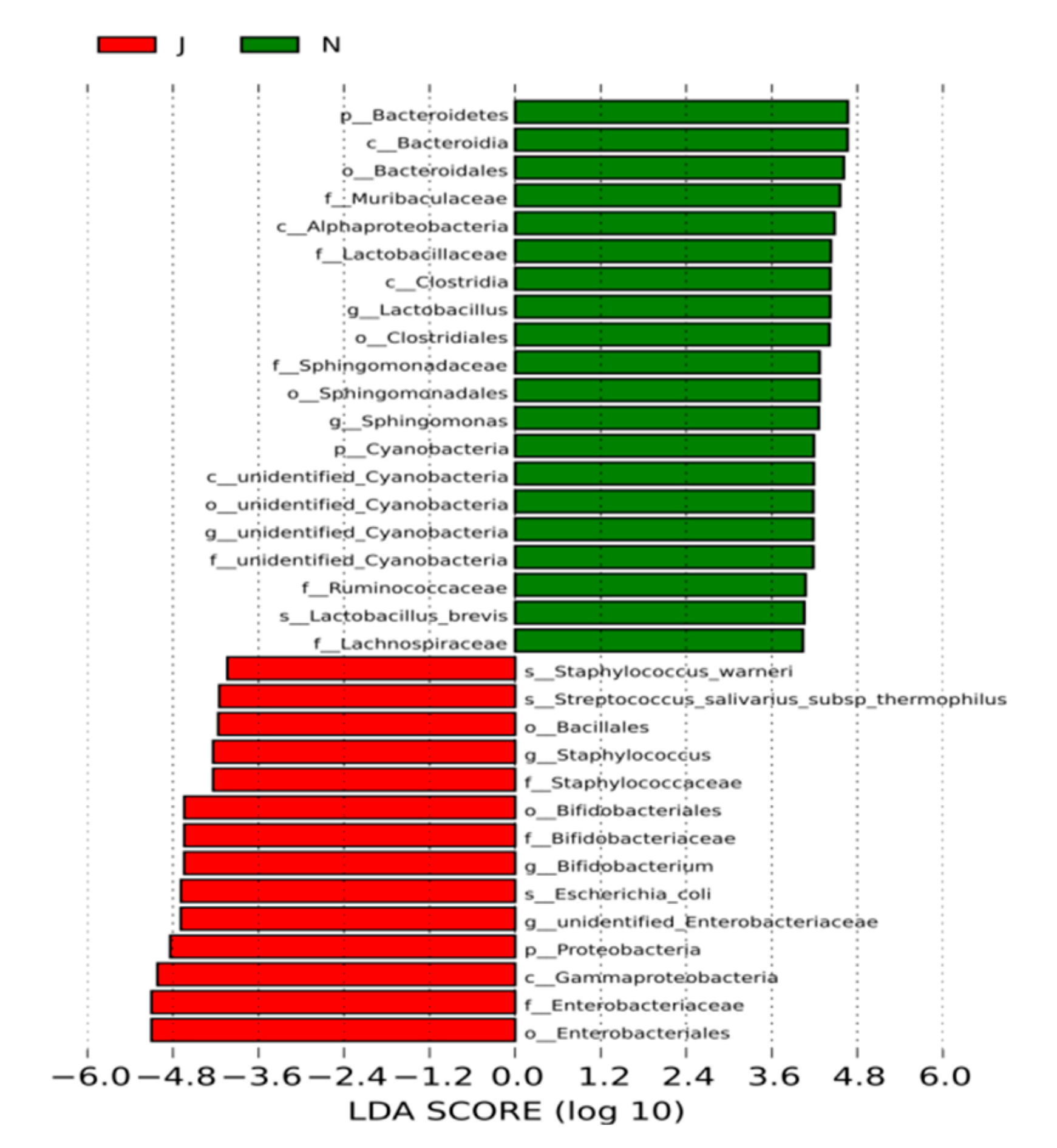
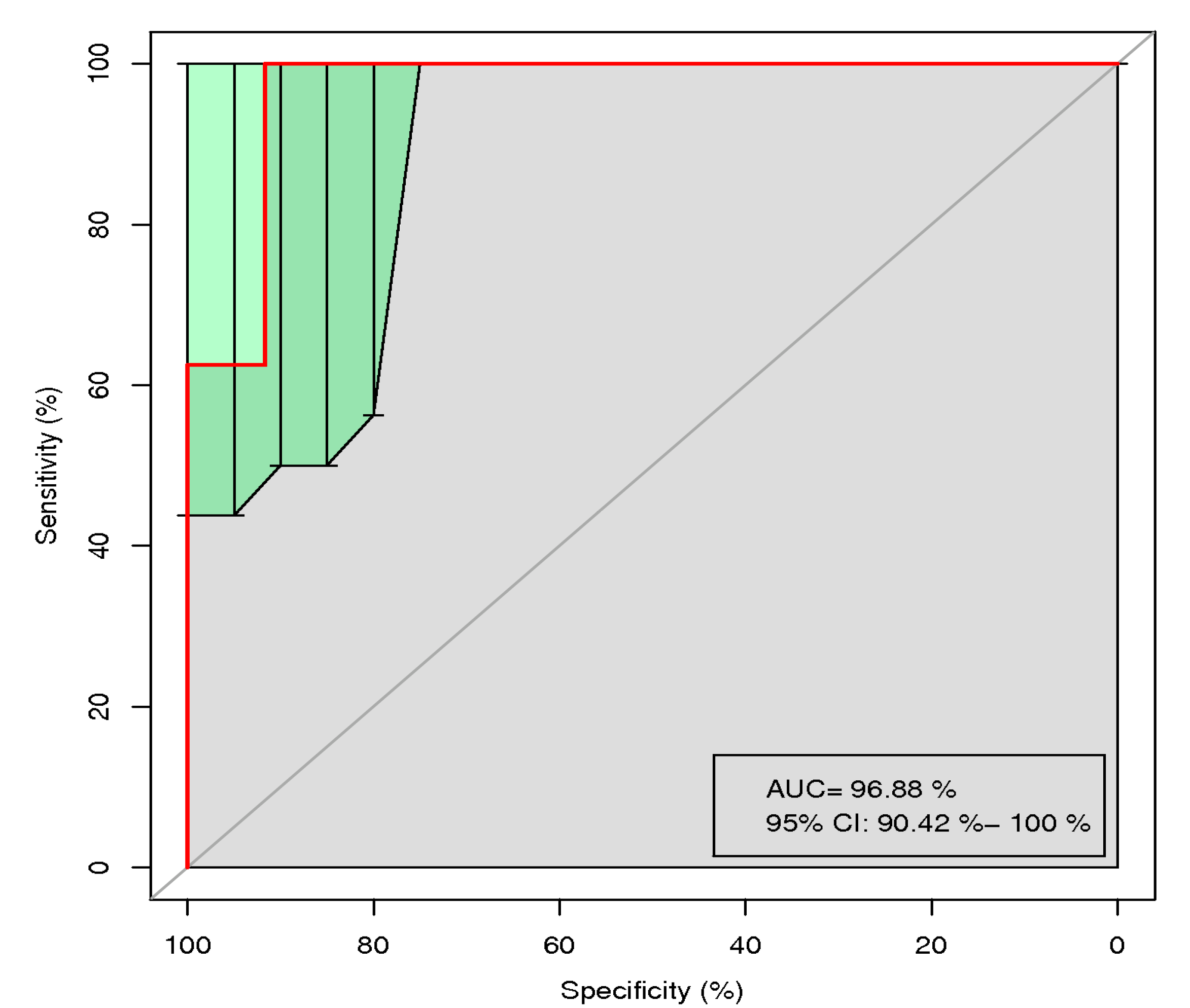
3.5. Potential Biomarkers for Diagnosing Neonatal Hyperbilirubinemia
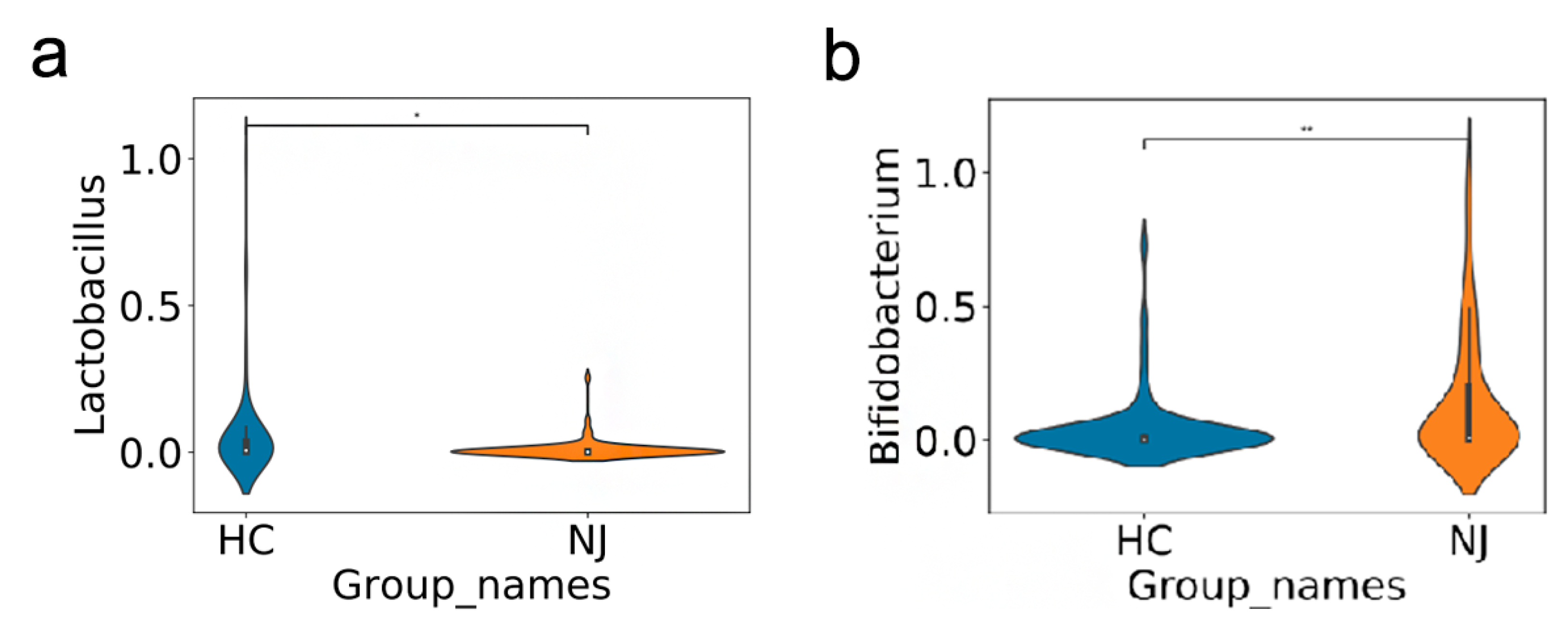
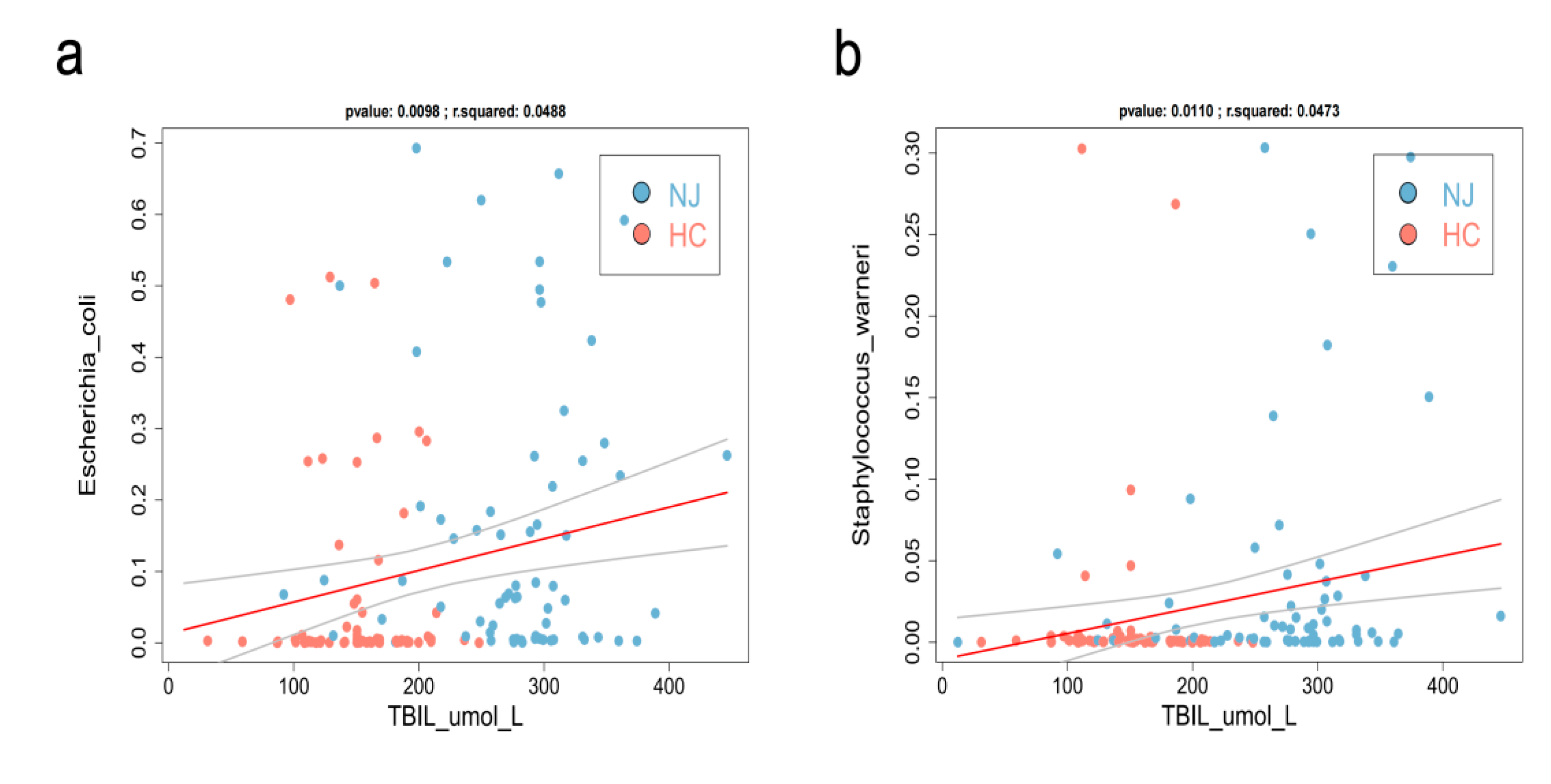
3.6. Gut Microbiota—Bilirubin Association Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lai, N.M.; Gerard, J.P.; Ngim, C.F.; Kamar, A.A.; Chen, K.H. The Association between Serum Bilirubin and Kernicterus Spectrum Disorder: A Systematic Review and Meta-Analysis. Neonatology 2021, 118, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Lauer, B.J.; Spector, N.D. Hyperbilirubinemia in the newborn. Pediatr. Rev. 2011, 32, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, M.; Irmak, E.; Aslan, Y.; Kader, Ş. Effects of Lactobacillus rhamnosus GG as a probiotic on neonatal hyperbilirubinemia. Turk. J. Pediatr. 2018, 60, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Tapia, E.; Sebastiani, G.; Sailer, S.; Toledano, L.A.; Serra-Delgado, M.; García-Algar, Ó.; Andreu-Fernández, V. Probiotic Supplementation during the Perinatal and Infant Period: Effects on Gut Dysbiosis and Disease. Nutrients 2020, 12, 2243. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Wang, Z.; He, F.; Qiu, H.; Wang, Y.; Wang, H.; Zhou, J.; Zhou, J.; Cheng, G.; Zhou, W.; et al. Association of serum bilirubin in newborns affected by jaundice with gut microbiota dysbiosis. J. Nutr. Biochem. 2019, 63, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Maisels, M.J.; Bhutani, V.K.; Bogen, D.; Newman, T.B.; Stark, A.R.; Watchko, J.F. Hyperbilirubinemia in the newborn infant > or =35 weeks’ gestation: An update with clarifications. Pediatrics 2009, 124, 1193–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, R.; Wu, B.; Liang, J.; He, F.; Gu, W.; Li, K.; Luo, Y.; Chen, J.; Gao, Y.; Wu, Z.; et al. Altered gut microbiota and mucosal immunity in patients with schizophrenia. Brain Behav. Immun. 2020, 85, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Butel, M.J.; Waligora-Dupriet, A.J.; Wydau-Dematteis, S. The developing gut microbiota and its consequences for health. J. Dev. Orig. Health Dis. 2018, 9, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Casaburi, G.; Duar, R.M.; Brown, H.; Mitchell, R.D.; Kazi, S. Metagenomic insights of the infant microbiome community structure and function across multiple sites in the United States. Sci. Rep. 2021, 11, 1472, Erratum in: Sci. Rep. 2021, 11, 11050. [Google Scholar] [CrossRef] [PubMed]
- Weiss, G.A.; Hennet, T. Mechanisms and consequences of intestinal dysbiosis. Cell. Mol. Life Sci. 2017, 74, 2959–2977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heeney, D.D.; Gareau, M.G.; Marco, M.L. Intestinal Lactobacillus in health and disease, a driver or just along for the ride? Curr. Opin. Biotechnol. 2018, 49, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Qin, H.; Zhang, M.; Shen, T.; Chen, H.; Ma, Y.; Chu, Z.; Zhang, P.; Liu, Z. Lactobacillus plantarum inhibits intestinal epithelial barrier dysfunction induced by unconjugated bilirubin. Br. J. Nutr. 2010, 104, 390–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.K.; Qin, H.L.; Zhang, M.; Shen, T.Y.; Chen, H.Q.; Ma, Y.L.; Chu, Z.X.; Zhang, P.; Liu, Z.H. Effects of Lactobacillus plantarum on gut barrier function in experimental obstructive jaundice. World J. Gastroenterol. 2012, 18, 3977–3991. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhang, L.; Zeng, L.; Yang, X.; Jiang, L.; Gui, G.; Zhang, Z. Probiotics Supplementation Therapy for Pathological Neonatal Jaundice: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2017, 8, 432. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, J.; Deshmukh, M.; Patole, S. Probiotics for the management of neonatal hyperbilirubinemia: A systematic review of randomized controlled trials. J. Matern. Fetal Neonatal Med. 2019, 32, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, B.; Ruiz, L.; de los Reyes-Gavilan, C.G.; Margolles, A. Proteomics of stress response in Bifidobacterium. Front. Biosci. 2008, 13, 6905–6919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, B.; Chen, Y.; Stanton, C.; Ross, R.P.; Lee, Y.K.; Zhao, J.; Zhang, H.; Chen, W. Bifidobacterium and Lactobacillus Composition at Species Level and Gut Microbiota Diversity in Infants before 6 Weeks. Int. J. Mol. Sci. 2019, 20, 3306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaper, J.B. Pathogenic Escherichia coli. Int. J. Med. Microbiol. 2005, 295, 355–356. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Zeng, S.; Cheng, G.; He, L.; Chen, M.; Wang, M.; Zhou, W.; Qiu, H.; Wang, Z. Clinical Manifestations of Neonatal Hyperbilirubinemia Are Related to Alterations in the Gut Microbiota. Children 2022, 9, 764. https://doi.org/10.3390/children9050764
Zhang X, Zeng S, Cheng G, He L, Chen M, Wang M, Zhou W, Qiu H, Wang Z. Clinical Manifestations of Neonatal Hyperbilirubinemia Are Related to Alterations in the Gut Microbiota. Children. 2022; 9(5):764. https://doi.org/10.3390/children9050764
Chicago/Turabian StyleZhang, Xueli, Shujuan Zeng, Guoqiang Cheng, Liufang He, Mingqiu Chen, Mingbang Wang, Wenhao Zhou, Huixian Qiu, and Zhangxing Wang. 2022. "Clinical Manifestations of Neonatal Hyperbilirubinemia Are Related to Alterations in the Gut Microbiota" Children 9, no. 5: 764. https://doi.org/10.3390/children9050764