Reference Values of Thromboelastometry Parameters in Healthy Term Neonates Using NATEM in Cord Blood Samples

 , ,
, , 
Abstract
:1. Introduction
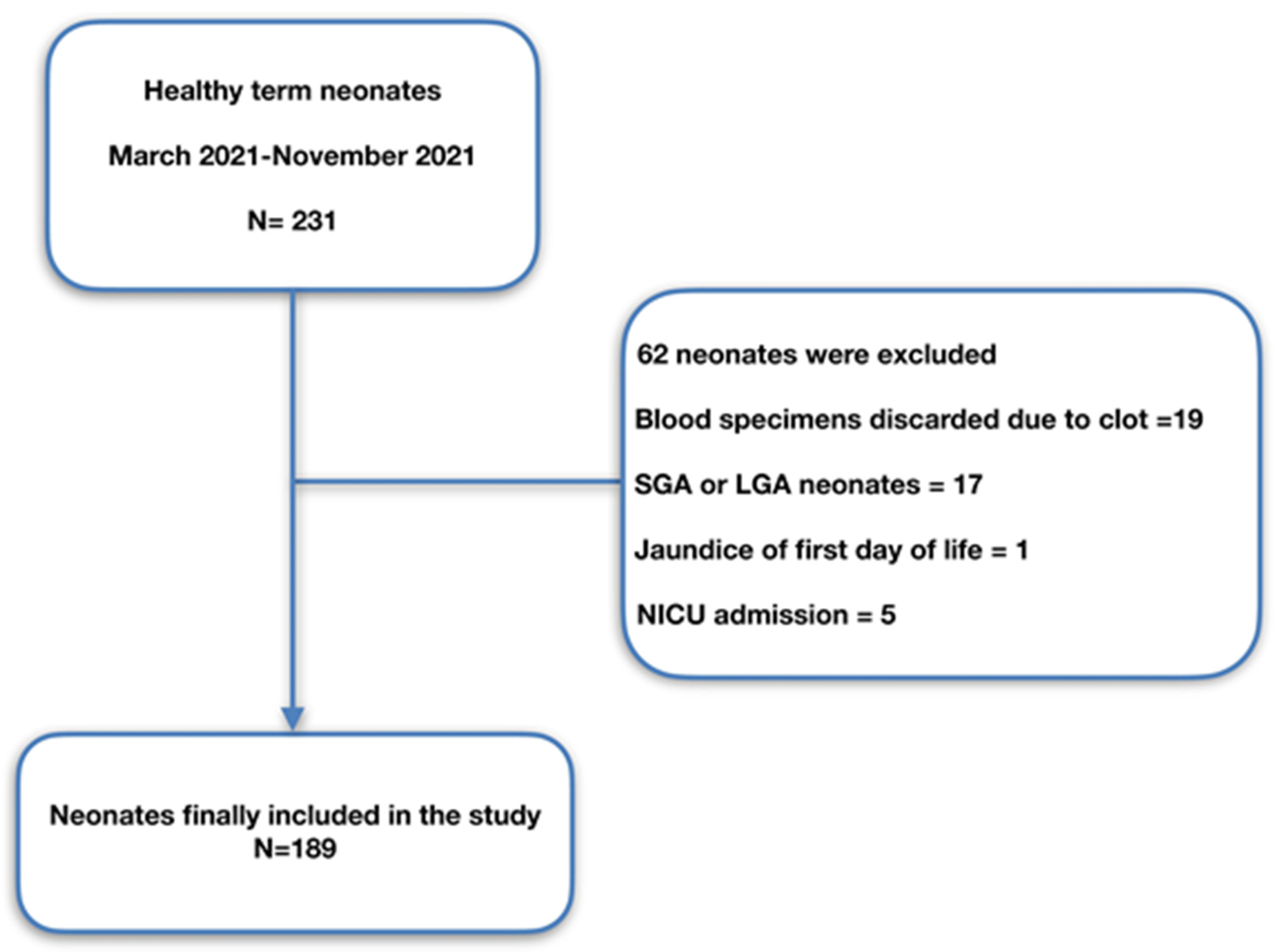
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrew, M.; Paes, B.; Milner, R.; Johnston, M.; Mitchell, L.; Tollefsen, D.M.; Powers, P. Development of the Human Coagulation System in the Full-Term Infant. Blood 1987, 70, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Ignjatovic, V.; Mertyn, E.; Monagle, P. The Coagulation System in Children: Developmental and Pathophysiological Considerations. Semin. Thromb. Hemost. 2011, 37, 723–729. [Google Scholar] [CrossRef]
- Saxonhouse, M.A.; Manco-Johnson, M.J. The Evaluation and Management of Neonatal Coagulation Disorders. Semin. Perinatol. 2009, 33, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, A.; Chantarangkul, V.; Mannucci, P.M. Acquired Coagulation Disorders: Revisited Using Global Coagulation/Anticoagulation Testing. Br. J. Haematol. 2009, 147, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Motta, M.; Guaragni, B.; Pezzotti, E.; Rodriguez-Perez, C.; Chirico, G. Reference Intervals of Citrated-Native Whole Blood Thromboelastography in Premature Neonates. Early Hum. Dev. 2017, 115, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Reverdiau-Moalic, P.; Delahousse, B.; Body, G.; Bardos, P.; Leroy, J.; Gruel, Y. Evolution of Blood Coagulation Activators and Inhibitors in the Healthy Human Fetus. Blood 1996, 88, 900–906. [Google Scholar] [CrossRef] [Green Version]
- Monagle, P.; Ignjatovic, V.; Savoia, H. Hemostasis in Neonates and Children: Pitfalls and Dilemmas. Blood Rev. 2010, 24, 63–68. [Google Scholar] [CrossRef]
- Weinstein, M.J.; Blanchard, R.; Moake, J.L.; Vosburgh, E.; Moise, K. Fetal and Neonatal von Willebrand Factor (VWF) Is Unusually Large and Similar to the VWF in Patients with Thrombotic Thrombocytopenic Purpura. Br. J. Haematol. 1989, 72, 68–72. [Google Scholar] [CrossRef]
- Cannata, G.; Mariotti Zani, E.; Argentiero, A.; Caminiti, C.; Perrone, S.; Esposito, S. TEG® and ROTEM® Traces: Clinical Applications of Viscoelastic Coagulation Monitoring in Neonatal Intensive Care Unit. Diagnostics 2021, 11, 1642. [Google Scholar] [CrossRef]
- Katsaras, G.N.; Sokou, R.; Tsantes, A.G.; Piovani, D.; Bonovas, S.; Konstantinidi, A.; Ioakeimidis, G.; Parastatidou, S.; Gialamprinou, D.; Makrogianni, A.; et al. The Use of Thromboelastography (TEG) and Rotational Thromboelastometry (ROTEM) in Neonates: A Systematic Review. Eur. J. Pediatr. 2021, 180, 3455–3470. [Google Scholar] [CrossRef] [PubMed]
- Mauch, J.; Spielmann, N.; Hartnack, S.; Madjdpour, C.; Kutter, A.P.; Bettschart-Wolfensberger, R.; Weiss, M.; Haas, T. Intrarater and Interrater Variability of Point of Care Coagulation Testing Using the ROTEM Delta. Blood Coagul. Fibrinolysis 2011, 22, 662–666. [Google Scholar] [CrossRef]
- Haas, T.; Spielmann, N.; Mauch, J.; Speer, O.; Schmugge, M.; Weiss, M. Reproducibility of Thrombelastometry (ROTEM®): Point-of-Care versus Hospital Laboratory Performance. Scand. J. Clin. Lab. Investig. 2012, 72, 313–317. [Google Scholar] [CrossRef]
- Oswald, E.; Stalzer, B.; Heitz, E.; Weiss, M.; Schmugge, M.; Strasak, A.; Innerhofer, P.; Haas, T. Thromboelastometry (ROTEM®) in Children: Age-Related Reference Ranges and Correlations with Standard Coagulation Tests. Br. J. Anaesth. 2010, 105, 827–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravn, H.B.; Andreasen, J.B.; Hvas, A.M. Does Whole Blood Coagulation Analysis Reflect Developmental Haemostasis? Blood Coagul. Fibrinolysis 2017, 28, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Romlin, B.S.; Wåhlander, H.; Berggren, H.; Synnergren, M.; Baghaei, F.; Nilsson, K.; Jeppsson, A. Intraoperative Thromboelastometry Is Associated with Reduced Transfusion Prevalence in Pediatric Cardiac Surgery. Anesth. Analg. 2011, 112, 30–36. [Google Scholar] [CrossRef]
- Romlin, B.S.; Wåhlander, H.; Synnergren, M.; Baghaei, F.; Jeppsson, A. Earlier Detection of Coagulopathy with Thromboelastometry during Pediatric Cardiac Surgery: A Prospective Observational Study. Pediatr. Anesth. 2013, 23, 222–227. [Google Scholar] [CrossRef]
- Strauss, T.; Levy-Shraga, Y.; Ravid, B.; Schushan-Eisen, I.; Maayan-Metzger, A.; Kuint, J.; Kenet, G. Clot Formation of Neonates Tested by Thromboelastography Correlates with Gestational Age. Thromb. Haemost. 2010, 103, 344–350. [Google Scholar] [CrossRef]
- Phillips, R.C.; Shahi, N.; Leopold, D.; Levek, C.; Shirek, G.; Hilton, S.; Hyslop, R.; Gien, J.; Kinsella, J.P.; Buckvold, S.; et al. Thromboelastography-Guided Management of Coagulopathy in Neonates with Congenital Diaphragmatic Hernia Supported by Extracorporeal Membrane Oxygenation. Pediatr. Surg. Int. 2020, 36, 1027–1033. [Google Scholar] [CrossRef] [PubMed]
- Forman, K.R.; Wong, E.; Gallagher, M.; McCarter, R.; Luban, N.L.; Massaro, A.N. Effect of Temperature on Thromboelastography and Implications for Clinical Use in Newborns Undergoing Therapeutic Hypothermia. Pediatr. Res. 2014, 75, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.P.; Niebler, R.A.; Stuth, E.A.E.; Newman, D.K.; Tweddell, J.S.; Bercovitz, R.S.; Benson, D.W.; Cole, R.; Simpson, P.M.; Yan, K.; et al. Rotational Thromboelastometry Rapidly Predicts Thrombocytopenia and Hypofibrinogenemia during Neonatal Cardiopulmonary Bypass. World J. Pediatr. Congenit. Heart Surg. 2018, 9, 424–433. [Google Scholar] [CrossRef]
- Sokou, R.; Piovani, D.; Konstantinidi, A.; Tsantes, A.G.; Parastatidou, S.; Lampridou, M.; Ioakeimidis, G.; Gounaris, A.; Iacovidou, N.; Kriebardis, A.G.; et al. A Risk Score for Predicting the Incidence of Hemorrhage in Critically Ill Neonates: Development and Validation Study. Thromb. Haemost. 2021, 121, 131–139. [Google Scholar] [CrossRef]
- Konstantinidi, A.; Sokou, R.; Parastatidou, S.; Lampropoulou, K.; Katsaras, G.; Boutsikou, T.; Gounaris, A.K.; Tsantes, A.E.; Iacovidou, N. Clinical Application of Thromboelastography/Thromboelastometry (TEG/TEM) in the Neonatal Population: A Narrative Review. Semin. Thrombos. Hemostasis 2019, 45, 449–457. [Google Scholar] [CrossRef]
- Liu, Q.; Xu, C.; Chen, X.; Wang, J.; Ke, Z.; Hu, H. Establishing a Reference Range for Thromboelastograph Parameters in the Neonatal Period. Int. J. Lab. Hematol. 2019, 41, 530–535. [Google Scholar] [CrossRef] [Green Version]
- Sokou, R.; Foudoulaki-Paparizos, L.; Lytras, T.; Konstantinidi, A.; Theodoraki, M.; Lambadaridis, I.; Gounaris, A.; Valsami, S.; Politou, M.; Gialeraki, A.; et al. Reference Ranges of Thromboelastometry in Healthy Full-Term and Pre-Term Neonates. Clin. Chem. Lab. Med. 2017, 28, 1592–1597. [Google Scholar] [CrossRef]
- Durila, M. Nonactivated Thromboelastometry Able to Detect Fibrinolysis in Contrast to Activated Methods (EXTEM, INTEM) in a Bleeding Patient. Blood Coagul. Fibrinolysis 2016, 27, 828–830. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, E.; Moore, E.E.; Moore, H.B. Management of Trauma-Induced Coagulopathy with Thrombelastography. Crit. Care Clin. 2017, 33, 119–134. [Google Scholar] [CrossRef] [Green Version]
- Sidlik, R.; Strauss, T.; Morag, I.; Shenkman, B.; Tamarin, I.; Lubetsky, A.; Livnat, T.; Kenet, G. Assessment of Functional Fibrinolysis in Cord Blood Using Modified Thromboelastography: Assessment of Functional Fibrinolysis in Cord Blood. Pediatr. Blood Cancer 2016, 63, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Theodoraki, M.; Sokou, R.; Valsami, S.; Iliodromiti, Z.; Pouliakis, A.; Parastatidou, S.; Karavana, G.; Ioakeimidis, G.; Georgiadou, P.; Iacovidou, N.; et al. Reference Values of Thrombolastometry Parameters in Healthy Term Neonates. Children 2020, 7, 259. [Google Scholar] [CrossRef] [PubMed]
- Scarpelini, S.; Rhind, S.G.; Nascimento, B.; Tien, H.; Shek, P.N.; Peng, H.T.; Huang, H.; Pinto, R.; Speers, V.; Reis, M.; et al. Normal Range Values for Thromboelastography in Healthy Adult Volunteers. Braz. J. Med. Biol. Res. 2009, 42, 1210–1217. [Google Scholar] [CrossRef]
- Ahammad, J.; Kurien, A.; Shastry, S.; Shah, H.H.; Nayak, D.; Kamath, A.; Badagabettu, S. Age- and Gender-related Reference Ranges for Thromboelastography from a Healthy Indian Population. Int. J. Lab. Hematol. 2020, 42, 180–189. [Google Scholar] [CrossRef]
- Sivrikaya, A.; Baran, H.; Abusoglu, S.; Öztürk, B.; Vatansev, H.; Unlu, A. Effect of Gender and Age on the Prothrombin Time (PT), Activated Partial Thromboplastin Time (aPTT) Levels and International Normalized Ratio (INR). Int. J. Mevlana Med. Sci. 2013, 1, 27–29. [Google Scholar]
- Schott, N.J.; Emery, S.P.; Garbee, C.; Waters, J. Thromboelastography in Term Neonates. J. Matern.-Fetal Neonatal Med. 2018, 31, 2599–2604. [Google Scholar] [CrossRef]
- Christensen, R.D.; Baer, V.L.; Lambert, D.K.; Henry, E.; Ilstrup, S.J.; Bennett, S.T. Reference Intervals for Common Coagulation Tests of Preterm Infants (CME): Coagulation Studies of Preterm Neonates. Transfusion 2014, 54, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Neary, E.; McCallion, N.; Kevane, B.; Cotter, M.; Egan, K.; Regan, I.; Kirkham, C.; Mooney, C.; Coulter-Smith, S.; Ní Áinle, F. Coagulation Indices in Very Preterm Infants from Cord Blood and Postnatal Samples. J. Thromb. Haemost. 2015, 13, 2021–2030. [Google Scholar] [CrossRef]
- Carroll, P.D.; Christensen, R.D. New and Underutilized Uses of Umbilical Cord Blood in Neonatal Care. Matern. Health Neonatol. Perinatol. 2015, 1, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | n | Value * | |
|---|---|---|---|
| Newborns’ data | GA (weeks) Median (Q1–Q3) | 189 | 39 (38–40) |
| BW (g) Median (Q1–Q3) | 189 | 3330 (3140–3530) | |
| Gender (females) | 189 | 86 (45.5%) | |
| Apgar score 1 min | 189 | 9 (9–9) | |
| Apgar score 5 min | 189 | 10 (10–10) | |
| pH (umbilical cord) | 185 | 7.36 (7.33–7.38) | |
| Newborns’ laboratory data | Blood group | 183 | A (62/33.88%) B (35/19.13%) AB (8/4.37%) O (78/42.62%) |
| Rhesus | 183 | Positive (166/90.7%) Negative (17/9.3%) | |
| Maternal data | Thrombophilic history | 189 | 11 (5.82%) |
| Anticoagulation treatment | 189 | 36 (19.05%) | |
| Pregnancy and delivery | Delivery mode | 189 | CS 116 (61.38%) VD 61 (32.28%) FD 12 (6.35%) |
| Parameter | Median (Q1–Q3) | 2.5 Pctl | 97.5 Pctl |
|---|---|---|---|
| CT | 322 (250–391) | 182 | 499 |
| A5 | 41 (36–45.5) | 28 | 52 |
| A10 | 51 (47–55) | 37 | 61 |
| A20 | 57 (53–61) | 42 | 66 |
| CFT | 97 (80–127) | 63 | 176 |
| MCF | 58 (54–61) | 43 | 67 |
| α-angle | 71 (65–74) | 58 | 78 |
| LI30 | 100 (99–100) | 97 | 100 |
| LI60 | 93 (91–95) | 87 | 98 |
| MCE | 136.5 (118–158.5) | 75 | 203 |
| Parameter | Gender | p-Value | |
|---|---|---|---|
| Males (n = 103) Median (Q1–Q3) | Females (n = 86) Median (Q1–Q3) | ||
| CT | 333 (280–413) | 299.5 (245–370) | 0.016 |
| A5 | 40 (35–45) | 42 (38–46) | 0.105 |
| A10 | 50 (46–55) | 52 (49–55) | 0.079 |
| A20 | 56 (52–60) | 58 (55–61) | 0.035 |
| CFT | 103 (82–137) | 92.5 (78–121) | 0.071 |
| MCF | 57 (53–61) | 59 (56–61) | 0.032 |
| α-angle | 70 (64–74) | 71 (67–74) | 0.094 |
| LI30 | 100 (99–100) | 100 (99–100) | 0.952 |
| LI60 | 93 (90–95) | 93 (91–95) | 0.915 |
| MCE | 132.5 (114–157) | 146 (127–159) | 0.032 |
| Parameter | VD (n = 61) Median (Q1–Q3) | CS (n = 116) Median (Q1–Q3) | FD (n = 12) Median (Q1–Q3) | p-Value |
|---|---|---|---|---|
| CT | 322 (232–377) | 272.5 (321–401.5) | 283.5 (236–378) | 0.429 |
| A5 | 42 (37.5–46.5) | 36 (40.5–45) | 42.5 (35.5–44) | 0.389 |
| A10 | 52 (47–56) | 46.5 (50–54) | 53 (47.5–54) | 0.428 |
| A20 | 57 (53–62) | 53 (57–60) | 59 (53–60.5) | 0.413 |
| CFT | 88 (78–127) | 81.5 (102.5–128) | 113 (82–130.5) | 0.232 |
| MCF | 59 (54–62) | 54 (57.5–61) | 59.5 (53.5–61.5) | 0.408 |
| α-angle | 72 (65–74) | 65 (70–74) | 68.5 (66–73) | 0.321 |
| LI30 | 100 (99–100) | 99 (100–100) | 100 (99.5–100) | 0.945 |
| LI60 | 93 (91–95) | 90 (93–94) | 92 (91–94.5) | 0.389 |
| MCE | 145 (120–162) | 118 (135–154) | 147 (115.5–161) | 0.377 |
| Parameter | Blood Group ABO | ||||
|---|---|---|---|---|---|
| A (n = 62) Median (Q1–Q3) | B (n = 35) Median (Q1–Q3) | AB (n = 8) Median (Q1–Q3) | O (n = 78) Median (Q1–Q3) | p-Value | |
| CT | 299.5 (246–377) | 342 (255–415) | 375 (303.5–420) | 322.5 (250–385) | 0.472 |
| A5 | 41 (37–47) | 39 (34–44) | 43 (35–45.5) | 42 (37–45) | 0.306 |
| A10 | 51 (48–57) | 49 (45–53) | 53.5 (46–54.5) | 52 (47–54) | 0.294 |
| A20 | 58 (54–62) | 55 (51–60) | 59.5 (53–61) | 57 (54–60) | 0.169 |
| CFT | 92 (77–123) | 109 (82–138) | 102 (83–128.5) | 97 (82–121) | 0.284 |
| MCF | 59 (55–62) | 56 (52–61) | 59.5 (53.5–62.5) | 58 (54–60) | 0.194 |
| α-angle | 71.5 (66–74) | 68 (63–74) | 70 (65–73) | 71 (67–74) | 0.289 |
| LI30 | 100 (100–100) | 100 (99–100) | 100 (99–100) | 100 (99–100) | 0.394 |
| LI60 | 93 (91–95) | 93 (90–94) | 90 (90–92) | 92 (90–94) | 0.046 |
| MCE | 146 (121–166) | 128 (109–157) | 145 (113–162) | 136.5 (120–153) | 0.211 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sulaj, A.; Tsaousi, M.; Karapati, E.; Pouliakis, A.; Iliodromiti, Z.; Boutsikou, T.; Valsami, S.; Iacovidou, N.; Politou, M.; Sokou, R. Reference Values of Thromboelastometry Parameters in Healthy Term Neonates Using NATEM in Cord Blood Samples. Children 2022, 9, 47. https://doi.org/10.3390/children9010047
Sulaj A, Tsaousi M, Karapati E, Pouliakis A, Iliodromiti Z, Boutsikou T, Valsami S, Iacovidou N, Politou M, Sokou R. Reference Values of Thromboelastometry Parameters in Healthy Term Neonates Using NATEM in Cord Blood Samples. Children. 2022; 9(1):47. https://doi.org/10.3390/children9010047
Chicago/Turabian StyleSulaj, Alma, Marina Tsaousi, Eleni Karapati, Abraham Pouliakis, Zoi Iliodromiti, Theodora Boutsikou, Serena Valsami, Nicoletta Iacovidou, Marianna Politou, and Rozeta Sokou. 2022. "Reference Values of Thromboelastometry Parameters in Healthy Term Neonates Using NATEM in Cord Blood Samples" Children 9, no. 1: 47. https://doi.org/10.3390/children9010047