
Complications and Recurrence of Patellar Instability after Medial Patellofemoral Ligament Reconstruction in Children and Adolescents: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Eligibility Criteria
2.2. Study Design
2.3. Participants
2.4. Interventions
2.5. Types of Outcome Measures
2.6. Information Sources and Search
2.7. Data Collection and Analysis
Study Selection
2.8. Data Collection Process
2.9. Levels of Evidence
2.10. Evaluation of Study Quality
2.11. Statistical Analysis
3. Results
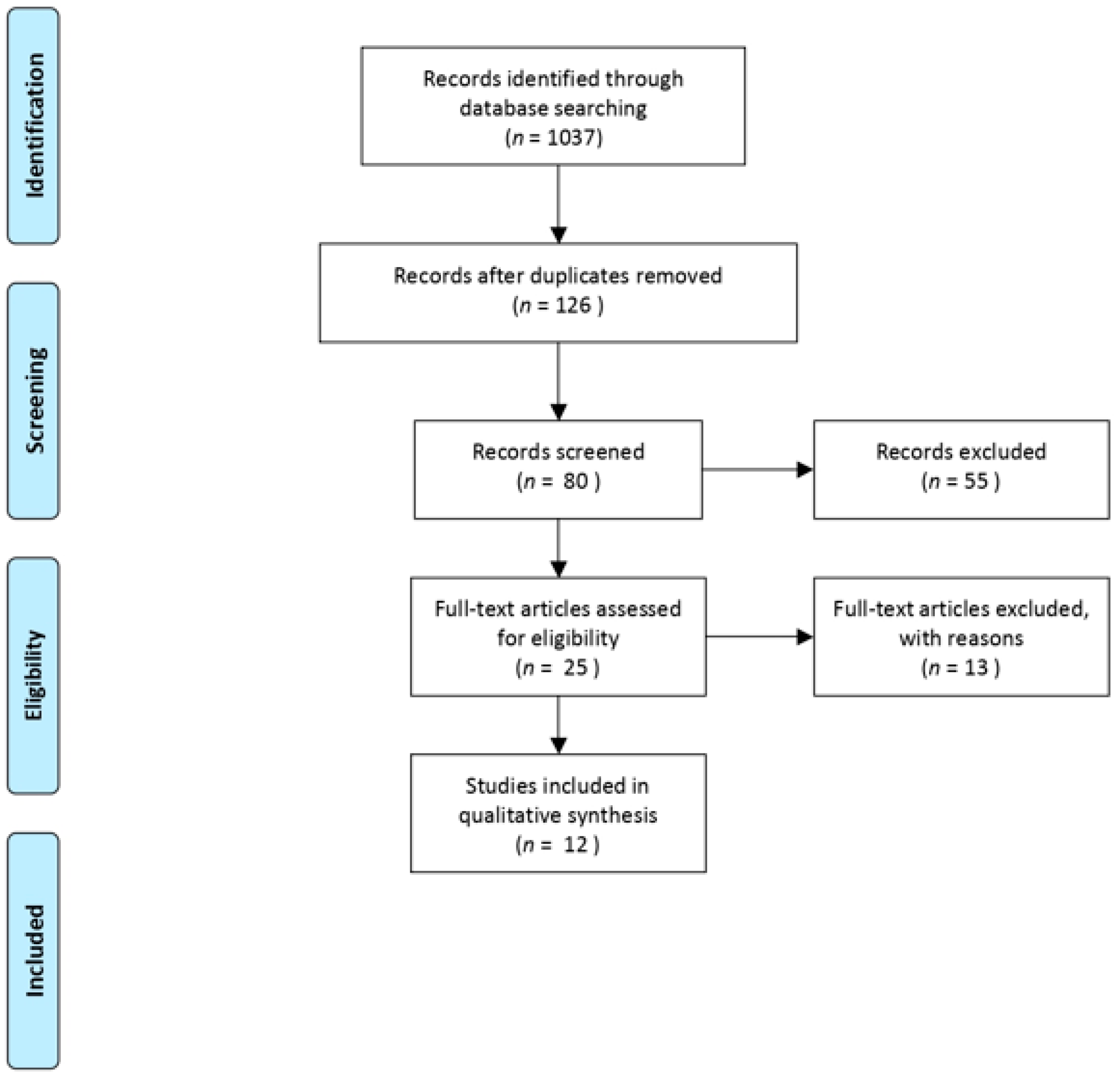
3.1. Search Results
3.2. Patient Demographic
3.3. Outcomes of Interest
3.4. Methodological Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Jaquith, B.P.; Parikh, S.N. Predictors of Recurrent Patellar Instability in Children and Adolescents After First-time Dislocation. J. Pediatr. Orthop. 2017, 37, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Reagan, J.; Kullar, R.; Burks, R. MPFL reconstruction: Technique and results. Orthop. Clin. 2015, 46, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Sappey-Marinier, E.; Sonnery-Cottet, B.; O’Loughlin, P.; Ouanezar, H.; Reina Fernandes, L.; Kouevidjin, B.; Thaunat, M. Clinical Outcomes and Predictive Factors for Failure With Isolated MPFL Reconstruction for Recurrent Patellar Instability: A Series of 211 Reconstructions With a Minimum Follow-up of 3 Years. Am. J. Sports Med. 2019, 47, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.; Metcalfe, A.; Wogan, C.; Mandalia, V.; Eldridge, J. Adolescent patellar instability: Current concepts review. Bone Joint J. 2017, 99, 159–170. [Google Scholar] [CrossRef]
- Smith, M.K.; Werner, B.C.; Diduch, D.R. Avoiding Complications with MPFL Reconstruction. Curr. Rev. Musculoskelet Med. 2018, 11, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 21, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, R.G.; Wilson, S.M.; Swiontkowski, M.F. Updating the assignment of levels of evidence. J. Bone Joint Surg. 2015, 97, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Uppstrom, T.J.; Price, M.; Black, S.; Gausden, E.; Haskel, J.; Green, D.W. Medial patellofemoral ligament (MPFL) reconstruction technique using an epiphyseal femoral socket with fluoroscopic guidance helps avoid physeal injury in skeletally immature patients. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3536–3542. [Google Scholar] [CrossRef]
- Saper, M.G.; Fantozzi, P.; Bompadre, V.; Racicot, M.; Schmale, G.A. Return-to-Sport Testing After Medial Patellofemoral Ligament Reconstruction in Adolescent Athletes. Orthop. J. Sports Med. 2019, 7, 2325967119828953. [Google Scholar] [CrossRef] [Green Version]
- Fabricant, P.D.; Ladenhauf, H.N.; Salvati, E.A.; Green, D.W. Medial patellofemoral ligament (MPFL) reconstruction improves radiographic measures of patella alta in children. Knee 2014, 21, 1180–1184. [Google Scholar] [CrossRef] [PubMed]
- Hohn, E.; Pandya, N.K. Does the Utilization of Allograft Tissue in Medial Patellofemoral Ligament Reconstruction in Pediatric and Adolescent Patients Restore Patellar Stability? Clin. Orthop. Relat. Res. 2017, 475, 1563–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lind, M.; Enderlein, D.; Nielsen, T.; Christiansen, S.E.; Faunø, P. Clinical outcome after reconstruction of the medial patellofemoral ligament in paediatric patients with recurrent patella instability. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Malecki, K.; Fabis, J.; Flont, P.; Lipczyk, Z.; Niedzielski, K. Preliminary results of two surgical techniques in the treatment of recurrent patellar dislocation: Medial patellofemoral ligament reconstruction versus combined technique of vastus medialis advancement, capsular plasty and Roux-Goldthwait procedure in treatment of recurrent patellar dislocation. Int. Orthop. 2016, 9, 1869–1874. [Google Scholar] [CrossRef]
- Matuszewski, Ł.; Tramś, M.; Ciszewski, A.; Wilczyński, M.; Tramś, E.; Jakubowski, P.; Matuszewska, A.; John, K. Medial patellofemoral ligament reconstruction in children: A comparative randomized short-term study of fascia lata allograft and gracilis tendon autograft reconstruction. Medicine 2018, 97, e13605. [Google Scholar] [CrossRef] [PubMed]
- Nelitz, M.; Dreyhaupt, J.; Reichel, H.; Woelfle, J.; Lippacher, S. Anatomic reconstruction of the medial patellofemoral ligament in children and adolescents with open growth plates: Surgical technique and clinical outcome. Am. J. Sports Med. 2013, 1, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Nelitz, M.; Dreyhaupt, J.; Williams, S.R.M. Anatomic reconstruction of the medial patellofemoral ligament in children and adolescents using a pedicled quadriceps tendon graft shows favourable results at a minimum of 2-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1210–1215. [Google Scholar] [CrossRef] [PubMed]
- Pesenti, S.; Ollivier, M.; Escudier, J.C.; Cermolacce, M.; Baud, A.; Launay, F.; Jouve, J.L.; Choufani, E. Medial patellofemoral ligament reconstruction in children: Do osseous abnormalities matter? Int. Orthop. 2018, 42, 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- Roger, J.; Viste, A.; Cievet-Bonfils, M.; Pracros, J.P.; Raux, S.; Chotel, F. Axial patellar engagement index and patellar tilt after medial patello-femoral ligament reconstruction in children and adolescents. Orthop. Traumatol. Surg. Res. 2019, 105, 133–138. [Google Scholar] [CrossRef]
- Spang, R.C.; Tepolt, F.A.; Paschos, N.K.; Redler, L.H.; Davis, E.A.; Kocher, M.S. Combined Reconstruction of the Medial Patellofemoral Ligament (MPFL) and Medial Quadriceps Tendon-Femoral Ligament (MQTFL) for Patellar Instability in Children and Adolescents: Surgical Technique and Outcomes. J Pediatr. Orthop. 2019, 39, e54–e61. [Google Scholar] [CrossRef]
- Migliorini, F.; Trivellas, A.; Driessen, A.; Quack, V.; Tingart, M.; Eschweiler, J. Graft choice for isolated MPFL reconstruction: Gracilis versus semitendinosus. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 763–770. [Google Scholar] [CrossRef]
- Hiemstra, L.A.; Kerslake, S.; Lafave, M.; Mohtadi, N.G. Concurrent Validation of the Banff Patella Instability Instrument to the Norwich Patellar Instability Score and the Kujala Score in Patients With Patellofemoral Instability. Orthop. J. Sports Med. 2016, 4, 2325967116646085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiemstra, L.A.; Kerslake, S.; Lafave, M.R. Quality-of-Life Outcomes of Patients following Patellofemoral Stabilization Surgery: The Influence of Trochlear Dysplasia. J. Knee Surg. 2017, 30, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Hiemstra, L.A.; Kerslake, S.; Lafave, M.R.; Tucker, A. Patella alta is reduced following MPFL reconstruction but has no effect on quality-of-life outcomes in patients with patellofemoral instability. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Saadat, A.A.; Lall, A.C.; Battaglia, M.R.; Mohr, M.R.; Maldonado, D.R.; Domb, B.G. Prevalence of Generalized Ligamentous Laxity in Patients Undergoing Hip Arthroscopy: A Prospective Study of Patients’ Clinical Presentation, Physical Examination, Intraoperative Findings, and Surgical Procedures. Am. J. Sports Med. 2019, 47, 885–893. [Google Scholar] [CrossRef]
- Pfeiffer, T.R.; Kanakamedala, A.C.; Herbst, E.; Nagai, K.; Murphy, C.; Burnham, J.M.; Popchak, A.; Debski, R.E.; Musahl, V. Female sex is associated with greater rotatory knee laxity in collegiate athletes. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1319–1325. [Google Scholar] [CrossRef]
- Flanigan, D.C.; Shemory, S.; Lundy, N.; Stitgen, M.; Long, J.M.; Magnussen, R.A. Medial patellofemoral ligament reconstruction with allograft versus autograft tissue results in similar recurrent dislocation risk and patient-reported outcomes. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2099–2104. [Google Scholar] [CrossRef]
- McNeilan, R.J.; Everhart, J.S.; Mescher, P.K.; Abouljoud, M.; Magnussen, R.A.; Flanigan, D.C. Graft Choice in Isolated Medial Patellofemoral Ligament Reconstruction: A Systematic Review With Meta-analysis of Rates of Recurrent Instability and Patient-Reported Outcomes for Autograft, Allograft, and Synthetic Options. Arthroscopy 2018, 34, 1340–1354. [Google Scholar] [CrossRef]
- Koenen, P.; Shafizadeh, S.; Pfeiffer, T.R.; Wafaisade, A.; Bouillon, B.; Kanakamedala, A.C.; Jaecker, V. Intraoperative fluoroscopy during MPFL reconstruction improves the accuracy of the femoral tunnel position. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3547–3552. [Google Scholar] [CrossRef]
- Chen, J.; Han, K.; Jiang, J.; Huangfu, X.; Zhao, S.; Zhao, J.; Xie, G. Radiographic Reference Points Do Not Ensure Anatomic Femoral Fixation Sites in Medial Patellofemoral Ligament Reconstruction: A Quantified Anatomic Localization Method Based on the Saddle Sulcus. Am. J. Sports Med. 2021, 49, 435–441. [Google Scholar] [CrossRef]
- McCarthy, M.; Ridley, T.J.; Bollier, M.; Wolf, B.; Albright, J.; Amendola, A. Femoral tunnel placement in medial patellofemoral ligament reconstruction. Iowa Orthop. J. 2013, 33, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Carnesecchi, O.; Neri, T.; Di Iorio, A.; Farizon, F.; Philippot, R. Results of anatomic gracilis MPFL reconstruction with precise tensioning. Knee 2015, 22, 580–584. [Google Scholar] [CrossRef]
- Stephen, J.M.; Kaider, D.; Lumpaopong, P.; Deehan, D.J.; Amis, A.A. The effect of femoral tunnel position and graft tension on patellar contact mechanics and kinematics after medial patellofemoral ligament reconstruction. Am. J. Sports Med. 2014, 42, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Shamrock, A.G.; Day, M.A.; Duchman, K.R.; Glass, N.; Westermann, R.W. Medial Patellofemoral Ligament Reconstruction in Skeletally Immature Patients: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2019, 7, 2325967119855023. [Google Scholar] [CrossRef] [PubMed]
- Sidharthan, S.; Wang, G.; Schlichte, L.M.; Fulkerson, J.P.; Green, D.W. Medial Patellofemoral Ligament Reconstruction in Skeletally Immature Patients. JBJS Essent. Surg. Tech. 2020, 10, e0110.1-3. [Google Scholar] [CrossRef]
- Popkin, C.A.; Bayomy, A.F.; Trupia, E.P.; Chan, C.M.; Redler, L.H. Patellar Instability in the Skeletally Immature. Curr. Rev. Musculoskelet Med. 2018, 11, 172–181. [Google Scholar] [CrossRef]


{kind=link}
| Author | Journal | Level of Evidence | Number of Patients | Mean Age (Years) | Graft Used for MPFL Reconstruction | Mean Follow-Up (Months) | Complications | Recurrence Instability |
|---|---|---|---|---|---|---|---|---|
| Uppstrom et al. (2019) [9] | KSSTA | IV—Case Series | 49 patients—54 knees (30 F–19 M) | 13.3 ± 1.6 | 54 Gracilis | 28.8 (6–96) | None | 5 |
| Saper et al. (2019) [10] | Orthop J Sport Med | IV—Case Series | 28 patients (20 F–8 M) | 14.9 (12–16) | 17 Hamstring11 Not specified | 7.4 | None | None |
| Fabricant et al. (2014) [11] | The Knee | IV—Case Series | 27 patients (22 F–5 M) | 14.9 | 27 Hamstring | 3 | None | None |
| Hohn et al. (2016) [12] | CORR | IV—Case Series | 22 patients—25 knees (18 F–7 M) | 16 ± 2.0 | 25 Gracilis | 24 (12–44) | 1 patella fracture1 1 screw removal due to inflammation | 2 |
| Lind et al. (2014) [13] | KSSTA | III—Case Control | 20 patients—24 knees (11 F–9 M) | 12.5 | 24 Gracilis | 39 (17–72) | 5 subluxation | 4 |
| Malecki et al. (2016) [14] | Int. Orthop. | III—Case Control | 28 patients (32 knees) | 14 (6–18) | 32 Adductor Magnus | 67.2 (36–180) | none | 3 |
| Matuszewski et al. (2018) [15] | Medicine | I—Randomized clinical trial | 44 patients (27 F–17 M) | 15 (13–17) | 22 Fascia Lata Allograft 22 Gracilis | 24 | 1 infection | 1 |
| Nelitz et al. (2013) [16] | AJSM | IV—Case Series | 21 patients (6 F–15 M) | 15 (14.4–16.4) | 21 Gracilis | 33.6 (24–43.2) | 1 post-operative stiffness | None |
| Nelitz et al. (2017) [17] | KSSTA | III—Prospective Study | 25 patients (16 F–9 M) | 12.8 (9.5–14.7) | 25 Pedicle Quadriceps Tendon | 31.2 (24–40.8) | 1 post-operative stiffness | None |
| Pesenti et al. (2018) [18] | Int. Orthop. | IV—Case Series | 25 patients—27 knees (19–6 M) | 13.8 ± 2.5 | 19 Gracilis 8 Semitendinosus | 41.1 ± 13.5 | 5 wound complications | 1 |
| Roger et al. (2018) [19] | OTSR | II—Non-randomized prospective observational study | 18 patients—20 knees (11 F–7 M) | 14.6 (8–17) | 20 Gracilis | 38.7 (24–63) | None | None |
| Spang et al. (2019) [20] | J Ped Orthop | IV—Case Series | 25 patients (15 F–10 M) | 15.0 ± 2.2 | 25 Gracilis allograft | 24 ± 6 | 1 subluxation | 2 |
| Author | A Clearly Stated aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint | Follow-up Period Appropriate to the Aim of the Study | Loss to Follow up Less Than 5% | Prospective Calculation of the Study Size | An Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Additional criteria in the case of comparative study | |||||||||||||
| Uppstrom et al. (2019) [9] | ** | * | * | ** | ** | ** | n.a. | n.a. | n.a. | n.a. | 10 | ||
| Saper et al. (2019) [10] | ** | * | * | ** | * | ** | n.a. | n.a. | n.a. | n.a. | 9 | ||
| Fabricant et al. (2014) [11] | ** | * | * | * | ** | n.a. | n.a. | n.a. | n.a. | 7 | |||
| Hohn et al. (2016) [12] | * | * | * | * | ** | ** | n.a. | n.a. | n.a. | n.a. | 8 | ||
| Lind et al. (2014) [13] | * | * | * | * | * | ** | n.a. | n.a. | n.a. | n.a. | 7 | ||
| Malecki et al. (2016) [14] | ** | * | ** | ** | * | ** | ** | ** | ** | * | 17 | ||
| Matuszewski et al. (2018) [15] | ** | * | ** | ** | ** | ** | ** | ** | * | * | 16 | ||
| Nelitz et al. (2013) [16] | ** | ** | ** | ** | ** | ** | n.a. | n.a. | n.a. | n.a. | 12 | ||
| Nelitz et al. (2017) [17] | ** | ** | ** | ** | ** | ** | n.a. | n.a. | n.a. | n.a. | 12 | ||
| Pesenti et al. (2018) [18] | ** | * | * | ** | * | ** | n.a. | n.a. | n.a. | n.a. | 9 | ||
| Roger et al. (2018) [19] | ** | ** | ** | ** | * | ** | n.a. | n.a. | n.a. | n.a. | 11 | ||
| Spang et al. (2019) [20] | ** | * | * | ** | ** | ** | n.a. | n.a. | n.a. | n.a. | 11 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Ambrosi, R.; Corona, K.; Capitani, P.; Coccioli, G.; Ursino, N.; Peretti, G.M. Complications and Recurrence of Patellar Instability after Medial Patellofemoral Ligament Reconstruction in Children and Adolescents: A Systematic Review. Children 2021, 8, 434. https://doi.org/10.3390/children8060434
D’Ambrosi R, Corona K, Capitani P, Coccioli G, Ursino N, Peretti GM. Complications and Recurrence of Patellar Instability after Medial Patellofemoral Ligament Reconstruction in Children and Adolescents: A Systematic Review. Children. 2021; 8(6):434. https://doi.org/10.3390/children8060434
Chicago/Turabian StyleD’Ambrosi, Riccardo, Katia Corona, Paolo Capitani, Gianluca Coccioli, Nicola Ursino, and Giuseppe Maria Peretti. 2021. "Complications and Recurrence of Patellar Instability after Medial Patellofemoral Ligament Reconstruction in Children and Adolescents: A Systematic Review" Children 8, no. 6: 434. https://doi.org/10.3390/children8060434