
The Most Common Vitamin D Receptor Polymorphisms (ApaI,FokI, TaqI, BsmI, and BglI) in Children with Dental Caries: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Literature Search
2.2. Eligibility Criteria and Study Selection
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
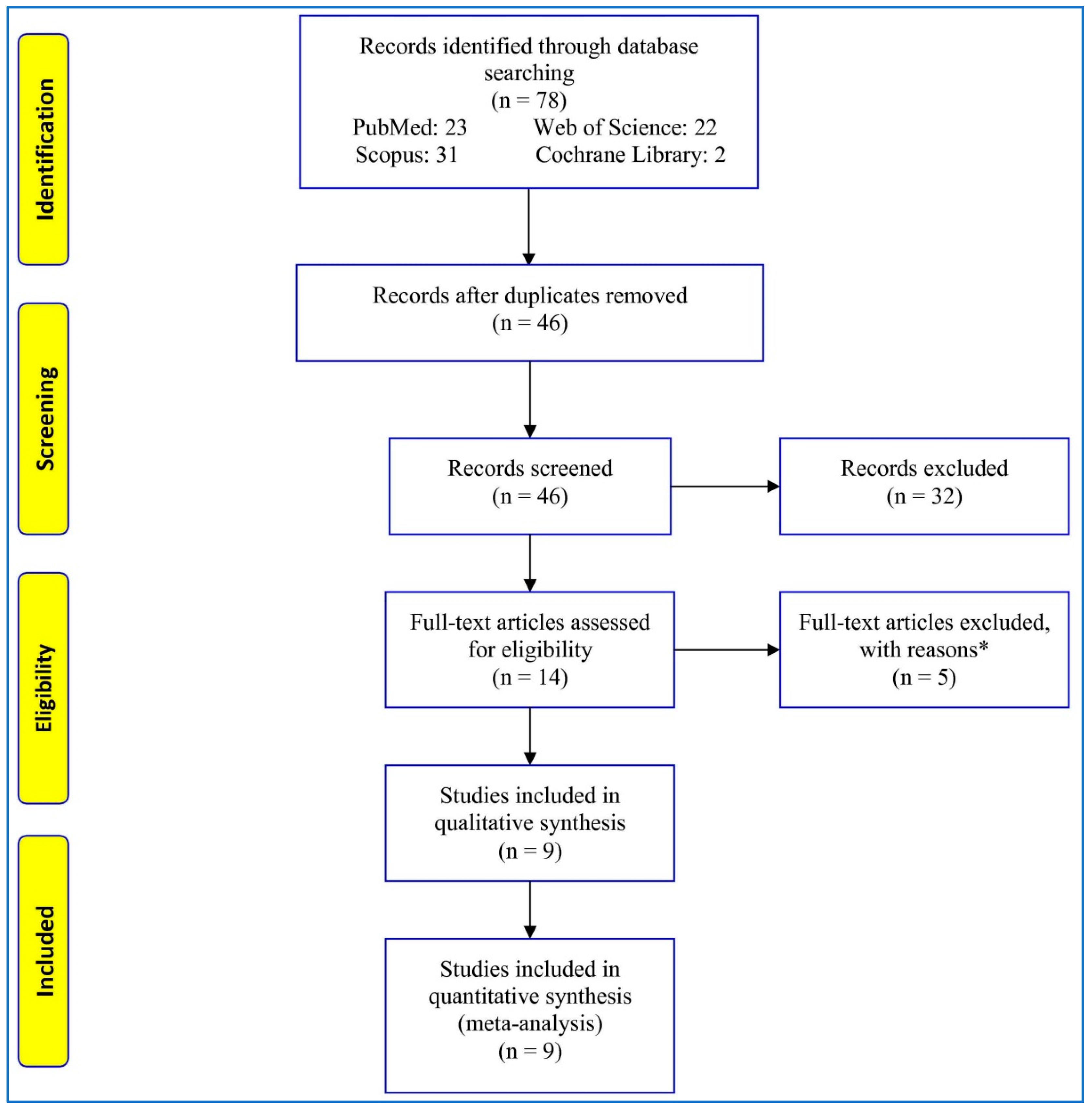
3.1. Study Selection
3.2. Quality Assessment
3.3. Characteristics of Studies
3.4. Meta-Analysis
3.5. Subgroup Analysis
3.6. Sensitivity Analysis
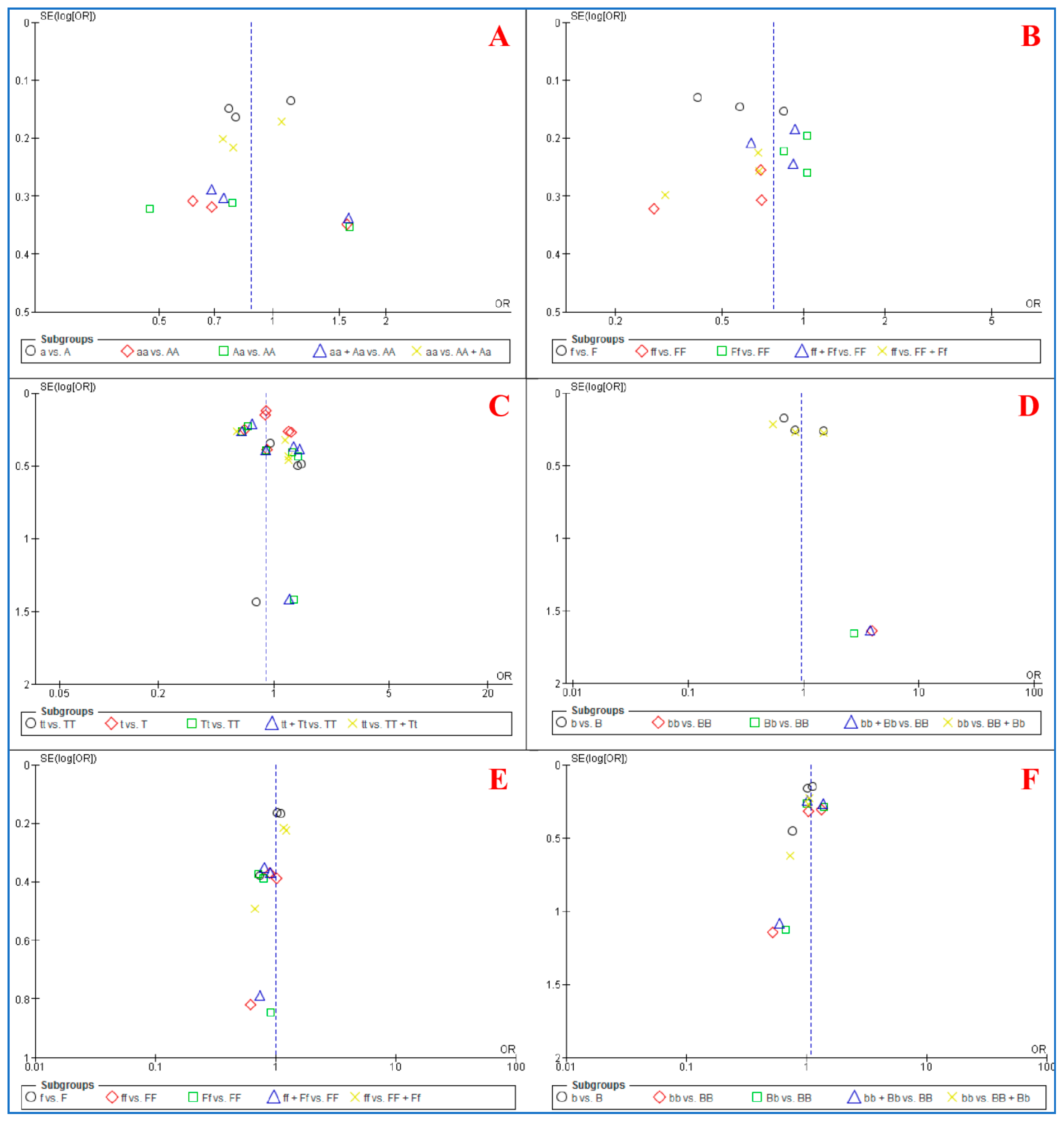
3.7. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Selwitz, R.; Ismail, A.; Pitts, N. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Collaborators, G.O.D.; Bernabe, E.; Marcenes, W.; Hernandez, C.; Bailey, J.; Abreu, L.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: A systematic analysis for the global burden of disease 2017 study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Modesto, A.; Marazita, M.L. Caries: Review of human genetics research. Caries Res. 2014, 48, 491–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haworth, S.; Shungin, D.; Van Der Tas, J.T.; Vucic, S.; Medina-Gomez, C.; Yakimov, V.; Feenstra, B.; Shaffer, J.R.; Lee, M.K.; Standl, M. Consortium-based genome-wide meta-analysis for childhood dental caries traits. Hum. Mol. Genet. 2018, 27, 3113–3127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, J.; Wang, X.; Feingold, E.; Lee, M.; Begum, F.; Weeks, D.; Cuenco, K.; Barmada, M.; Wendell, S.; Crosslin, D. Genome-wide association scan for childhood caries implicates novel genes. J. Dent. Res. 2011, 90, 1457–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapple, I.L.; Bouchard, P.; Cagetti, M.G.; Campus, G.; Carra, M.C.; Cocco, F.; Nibali, L.; Hujoel, P.; Laine, M.L.; Lingström, P. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: Consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, S39–S51. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Shaffer, J.; Weyant, R.; Cuenco, K.; DeSensi, R.; Crout, R.; McNeil, D.; Marazita, M. Genes and their effects on dental caries may differ between primary and permanent dentitions. Caries Res. 2010, 44, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Wendell, S.; Wang, X.; Brown, M.; Cooper, M.; DeSensi, R.; Weyant, R.; Crout, R.; McNeil, D.; Marazita, M. Taste genes associated with dental caries. J. Dent. Res. 2010, 89, 1198–1202. [Google Scholar] [CrossRef]
- Randev, S.; Kumar, P.; Guglani, V. Vitamin D supplementation in childhood—A review of guidelines. Indian J. Pediatrics 2018, 85, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Chhonkar, A.; Gupta, A.; Arya, V. Comparison of vitamin D level of children with severe early childhood caries and children with no caries. Int. J. Clin. Pediatric Dent. 2018, 11, 199. [Google Scholar] [CrossRef]
- Deane, S.; Schroth, R.J.; Sharma, A.; Rodd, C. Combined deficiencies of 25-hydroxyvitamin D and anemia in preschool children with severe early childhood caries: A case–control study. Paediatr. Child Health 2018, 23, e40–e45. [Google Scholar] [CrossRef] [PubMed]
- Gyll, J.; Ridell, K.; Öhlund, I.; Åkeson, P.K.; Johansson, I.; Holgerson, P.L. Vitamin D status and dental caries in healthy Swedish children. Nutr. J. 2018, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.-J.; Lee, H.-S.; Ju, H.-J.; Na, J.-Y.; Oh, H.-W. A cross-sectional study on the association between vitamin D levels and caries in the permanent dentition of Korean children. BMC Oral Health 2018, 18, 1–6. [Google Scholar] [CrossRef]
- Sutton, A.L.; MacDonald, P.N. Vitamin D: More than a “bone-a-fide” hormone. Mol. Endocrinol. 2003, 17, 777–791. [Google Scholar] [CrossRef]
- Valdivielso, J.M.; Fernandez, E. Vitamin D receptor polymorphisms and diseases. Clin. Chim. Acta 2006, 371, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Uitterlinden, A.G.; Fang, Y.; Van Meurs, J.B.; Pols, H.A.; Van Leeuwen, J.P. Genetics and biology of vitamin D receptor polymorphisms. Gene 2004, 338, 143–156. [Google Scholar] [CrossRef] [Green Version]
- Uitterlinden, A.G.; Fang, Y.; van Meurs, J.B.; van Leeuwen, H.; Pols, H.A. Vitamin D receptor gene polymorphisms in relation to Vitamin D related disease states. J. Steroid Biochem. Mol. Biol. 2004, 89, 187–193. [Google Scholar] [CrossRef]
- Hujoel, P.P. Vitamin D and dental caries in controlled clinical trials: Systematic review and meta-analysis. Nutr. Rev. 2013, 71, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.-Y.; Zheng, J.-M.; Zhang, W.-J.; Jiang, Q.-Z.; Yang, X.-C.; Yu, M.; Zeng, S.-J. The relationship between vitamin D receptor gene polymorphism and deciduous tooth decay in Chinese children. BMC Oral Health 2017, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Patir, A.; Seymen, F.; Yildirim, M.; Deeley, K.; Cooper, M.; Marazita, M.; Vieira, A. Enamel formation genes are associated with high caries experience in Turkish children. Caries Res. 2008, 42, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Sharifi, R.; Jahedi, S.; Mozaffari, H.R.; Imani, M.M.; Sadeghi, M.; Golshah, A.; Moradpoor, H.; Safaei, M. Association of LTF, ENAM, and AMELX polymorphisms with dental caries susceptibility: A meta-analysis. BMC Oral Health 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Triantos, C.; Aggeletopoulou, I.; Kalafateli, M.; Spantidea, P.I.; Vourli, G.; Diamantopoulou, G.; Tapratzi, D.; Michalaki, M.; Manolakopoulos, S.; Gogos, C. Prognostic significance of vitamin D receptor (VDR) gene polymorphisms in liver cirrhosis. Sci. Rep. 2018, 8, 1–14. [Google Scholar] [CrossRef]
- Zhang, P.; Li, Q.; Qi, J.; Lv, Q.; Zheng, X.; Wu, X.; Gu, J. Association between vitamin D receptor gene polymorphism and ankylosing spondylitis in Han Chinese. Int. J. Rheum. Dis. 2017, 20, 1510–1516. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Machiela, M.J.; Chanock, S.J. LDlink: A web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants. Bioinformatics 2015, 31, 3555–3557. [Google Scholar] [CrossRef] [PubMed]
- Aribam, V.G.; Aswath, N.; Ramanathan, A. Single-nucleotide polymorphism in Vitamin D receptor gene and its association with dental caries in children. J. Indian Soc. Pedod. Prev. Dent. 2020, 38, 8. [Google Scholar]
- Barbosa, M.C.; Lima, D.C.; Reis, C.L.; Reis, A.L.; Rigo, D., Jr.; Segato, R.A.; Storrer, C.L.; Küchler, E.C.; de Oliveira, D.S. Vitamin D receptor FokI and BglI genetic polymorphisms, dental caries, and gingivitis. Int. J. Paediatr. Dent. 2020, 30, 642–649. [Google Scholar] [CrossRef]
- Cogulu, D.; Onay, H.; Ozdemir, Y.; Aslan, G.I.; Ozkinay, F.; Eronat, C. The role of vitamin D receptor polymorphisms on dental caries. J. Clin. Pediatric Dent. 2016, 40, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Fatturi, A.L.; Menoncin, B.L.; Reyes, M.T.; Meger, M.; Scariot, R.; Brancher, J.A.; Küchler, E.C.; Feltrin-Souza, J. The relationship between molar incisor hypomineralization, dental caries, socioeconomic factors, and polymorphisms in the vitamin D receptor gene: A population-based study. Clin. Oral Investig. 2020, 24, 3971–3980. [Google Scholar] [CrossRef]
- Holla, L.I.; Linhartova, P.B.; Kastovsky, J.; Bartosova, M.; Musilova, K.; Kukla, L.; Kukletova, M. Vitamin D receptor TaqI gene polymorphism and dental caries in Czech children. Caries Res. 2017, 51, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Madalena, I.R.; Xavier, T.A.; Cruz, G.V.; Brancher, J.A.; da Silva, L.A.B.; Paza, A.O.; Segato, R.A.B.; Küchler, E.C. Evaluation of vitamin D receptor genetic polymorphisms with dental caries and developmental defects of enamel in Brazilian children. Pediatric Dent. J. 2020, 30, 161–166. [Google Scholar] [CrossRef]
- Qin, X.; Shao, L.; Zhang, L.; Ma, L.; Xiong, S. Investigation of Interaction between Vitamin D Receptor Gene Polymorphisms and Environmental Factors in Early Childhood Caries in Chinese Children. Biomed Res. Int. 2019, 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, M.; Jiang, Q.-Z.; Sun, Z.-Y.; Kong, Y.-Y.; Chen, Z. Association between single nucleotide polymorphisms in vitamin D receptor gene polymorphisms and permanent tooth caries susceptibility to permanent tooth caries in Chinese adolescent. Biomed Res. Int. 2017, 2017. [Google Scholar] [CrossRef] [Green Version]
- Ryan, J.W.; Anderson, P.H.; Morris, H.A. Pleiotropic activities of vitamin D receptors–adequate activation for multiple health outcomes. Clin. Biochem. Rev. 2015, 36, 53. [Google Scholar]
- Dusso, A.S.; Brown, A.J. Mechanism of vitamin D action and its regulation. Am. J. Kidney Dis. 1998, 32, S13–S24. [Google Scholar] [CrossRef]
- Amano, Y.; Komiyama, K.; Makishima, M. Vitamin D and periodontal disease. J. Oral Sci. 2009, 51, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Demay, M.B. Mechanism of vitamin D receptor action. Ann. N. Y. Acad. Sci. 2006, 1068, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.S.; Umbach, D.M. Are vitamin D receptor polymorphisms associated with bone mineral density? A meta-analysis. J. Bone Miner. Res. 1996, 11, 1841–1849. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.L.; Peacock, J.L.; Rees, J.R.; Bostick, R.M.; Robertson, D.J.; Bresalier, R.S.; Baron, J.A. Vitamin D receptor genotype, vitamin D3 supplementation, and risk of colorectal adenomas: A randomized clinical trial. JAMA Oncol. 2017, 3, 628–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karasneh, J.A.; Ababneh, K.T.; Taha, A.H.; Al-Abbadi, M.S.; Marzouka, N.A.d.S.; Jaradat, S.M.; Thornhill, M.H. Association of vitamin D receptor gene polymorphisms with chronic and aggressive periodontitis in Jordanian patients. Eur. J. Oral Sci. 2013, 121, 551–558. [Google Scholar] [CrossRef]
- Sarkissyan, M.; Wu, Y.; Chen, Z.; Mishra, D.K.; Sarkissyan, S.; Giannikopoulos, I.; Vadgama, J.V. Vitamin D receptor FokI gene polymorphisms may be associated with colorectal cancer among African American and Hispanic participants. Cancer 2014, 120, 1387–1393. [Google Scholar] [CrossRef] [Green Version]
- Vanessa, O.; Asani, F.F.; Jeffery, T.J.; Saccone, D.S.; Bornman, L. Vitamin D receptor gene expression and function in a South African population: Ethnicity, vitamin D and Fok I. PLoS ONE 2013, 8, e67663. [Google Scholar]
- Nelson, D.; Vord, P.V.; Wooley, P. Polymorphism in the vitamin D receptor gene and bone mass in African-American and white mothers and children: A preliminary report. Ann. Rheum. Dis. 2000, 59, 626–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, K.; Miyake, Y.; Hanioka, T.; Arakawa, M. VDR gene polymorphisms, interaction with smoking and risk of periodontal disease in Japanese women: The Kyushu Okinawa maternal and child health study. Scand. J. Immunol. 2013, 78, 371–377. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Database | Search |
|---|---|
| PubMed | (“Vit D”[Title/Abstract] OR “Vitamin D” [Title/Abstract] OR “calciferol”[Title/Abstract] OR “VDR” [Title/Abstract]) AND (“dental caries” [Title/Abstract] OR “caries”[Title/Abstract] OR “decay”[Title/Abstract]) AND (“gene”[Title/Abstract] OR “polymorphism*”[Title/Abstract] OR “variant*”[Title/Abstract] OR “allele*”[Title/Abstract] OR “genetic*”[Title/Abstract]) |
| Cochrane Library | (“Vit D”:ti,ab,kw OR “Vitamin D”:ti,ab,kw OR “calciferol”:ti,ab,kw OR “VDR”:ti,ab,kw) AND (“dental caries”:ti,ab,kw OR “caries”:ti,ab,kw OR “decay”:ti,ab,kw) AND (“polymorphism*”:ti,ab,kw OR “variant*”:ti,ab,kw OR “genotype*”) |
| Web of Science | TS = (“Vit D” OR “Vitamin D” OR “calciferol” OR “VDR”) AND TS = (“dental caries” OR “caries” OR “decay”) AND TS = (“ polymorphism*” OR “variant*” OR “allele*” OR “genotype*”) |
| Scopus | (TITLE-ABS-KEY (“Vit D”) OR TITLE-ABS-KEY (“Vitamin D”) OR TITLE-ABS-KEY (“calciferol”) OR TITLE-ABS-KEY (“VDR”)) AND (TITLE-ABS-KEY (“dental caries”) OR TITLE-ABS-KEY (“caries”) OR TITLE-ABS-KEY (“decay”)) AND (TITLE-ABS-KEY (“polymorphism*”) OR TITLE-ABS-KEY (“variant*”) OR TITLE-ABS-KEY (“allele*”) OR TITLE-ABS-KEY (“genotype*”)) |
| Criteria | Score |
|---|---|
| 1. Representativeness of cases | |
| Consecutive/randomly selected from case population with clearly defined sampling frame | 2 |
| Consecutive/randomly selected from case population without clearly defined sampling frame or with extensive inclusion/exclusion criteria | 1 |
| Not described | 0 |
| 2. Source of controls | |
| Population- or community-based | 2 |
| Hospital-based | 1 |
| Not described | 0 |
| 3. Ascertainment of dental caries | |
| Clinical examination | 2 |
| Diagnosis of caries by patient medical record | 1 |
| Not described | 0 |
| 4. Sample size | |
| >1000 | 2 |
| 200–1000 | 1 |
| <200 | 0 |
| 5. Age and sex were matched between cases and controls | |
| Yes | 1 |
| No/Not described | 0 |
| 6. Quality control of genotyping methods | |
| Repetition of partial/total tested samples | 1 |
| Not described | 0 |
| 7. Hardy–Weinberg equilibrium in control subjects | |
| Hardy–Weinberg equilibrium | 1 |
| Hardy–Weinberg disequilibrium | 0 |
| First Author, Publication Year | Country | Ethnicity | Source of Control | Genotyping Method | Quality Score |
|---|---|---|---|---|---|
| Cogulu, 2016 [32] | Turkey | Caucasian | Population-based | PCR-RFLP | 7 |
| Holla, 2017 [34] | Czech Republic | Caucasian | Population-based | TaqMan | 9 |
| Kong, 2017 [21] | China | Asian | School-based | PCR | 8 |
| Yu, 2017 [37] | China | Asian | School-based | PCR-RFLP | 10 |
| Qin, 2019 [36] | China | Asian | Population-based | TaqMan | 10 |
| Aribam, 2020 [30] | India | Caucasian | Population-based | PCR | 9 |
| Barbosa, 2020 [31] | Brazil | Mixed | School-based | Real-Time PCR | 8 |
| Fatturi, 2020 [33] | Brazil | Mixed | School-based | Real-Time PCR | 10 |
| Madalena, 2020 [35] | Brazil | Mixed | School-based | Real-Time PCR | 9 |
| First Author, Publication Year | Groups (N) | ApaI (rs7975232) | FokI (rs10735810) | TaqI (rs731236) | BsmI (rs1544410) | p-Value of HWE | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AA | Aa | aa | FF | Ff | ff | TT | Tt | Tt | BB | Bb | bb | |||
| Cogulu, 2016 [32] | Case (112) | - | - | - | - | - | - | 35 | 46 | 31 | - | - | - | 0.132 |
| Control (38) | - | - | - | - | - | - | 15 | 14 | 9 | - | - | - | ||
| Holla, 2017 [34] | Case (235) | - | - | - | - | - | - | 95 | 110 | 30 | - | - | - | 0.037 |
| Control (153) | - | - | - | - | - | - | 51 | 85 | 17 | - | - | - | ||
| Kong, 2017 [21] | Case (249) | 44 | 87 | 118 | 69 | 132 | 48 | 230 | 19 | 0 | 0 | 152 | 97 | 0.011, 0.662, 0.615, and <0.001 |
| Control (131) | 18 | 43 | 70 | 34 | 63 | 34 | 120 | 11 | 0 | 0 | 60 | 71 | ||
| Yu, 2017 [37] | Case (200) | 33 | 85 | 82 | 86 | 96 | 18 | 171 | 29 | 0 | 0 | 36 | 164 | 0.210, 0.057, 0.097, and 0.399 |
| Control (200) | 24 | 79 | 97 | 65 | 86 | 49 | 158 | 42 | 0 | 0 | 31 | 169 | ||
| Qin, 2019 [36] | Case (304) | 17 | 129 | 158 | 98 | 160 | 46 | 1 | 274 | 29 | 0 | 28 | 276 | 0.895, 0.764, <0.001, and 0.909 |
| Control (245) | 21 | 100 | 124 | 75 | 119 | 51 | 1 | 207 | 37 | 1 | 31 | 213 | ||
| Aribam, 2020 [30] | Case (60) | - | - | - | - | - | - | 22 | 25 | 13 | - | - | - | 0.158 |
| Control (60) | - | - | - | - | - | - | 26 | 23 | 11 | - | - | - | ||
| First Author, Publication Year | Groups (N) | FokI (rs2228570) | BglI (rs739837) | p-Value of HWE | ||||||||||
| FF | Ff | Ff | BB | Bb | bb | |||||||||
| Barbosa, 2020 [31] | Case (164 and 163) | 19 | 64 | 81 | 29 | 82 | 52 | 0.691 and 0.347 | ||||||
| Control (179 and 188) | 17 | 80 | 82 | 43 | 87 | 58 | ||||||||
| Fatturi, 2020 [33] | Case (204 and 213) | 22 | 85 | 97 | 63 | 101 | 49 | 0.435 and 0.692 | ||||||
| Control (132 and 121) | 13 | 63 | 56 | 36 | 58 | 27 | ||||||||
| Madalena, 2020 [35] | Case (138 and 99) | 19 | 60 | 59 | 13 | 52 | 34 | 0.649 and 0.665 | ||||||
| Control (19 and 12) | 2 | 7 | 10 | 1 | 6 | 5 | ||||||||
| Genetic Model | First Author, Publication Year | Case | Control | Weight | Odds Ratio | ||
|---|---|---|---|---|---|---|---|
| Events | Total | Events | Total | M-H, Random, 95%CI | |||
| a vs. A | Kong, 2017 [21] | 323 | 498 | 183 | 262 | 30.3% | 0.80 [0.58, 1.10] |
| Yu, 2017 [37] | 249 | 400 | 273 | 400 | 33.4% | 0.77 [0.57, 1.03] | |
| Qin, 2019 [36] | 445 | 608 | 348 | 490 | 36.4% | 1.11 [0.85, 1.45] | |
| Subtotal (95%CI) | 1506 | 1152 | 100.0% | 0.89 [0.70, 1.13] | |||
| Total events | 1017 | 804 | |||||
| Heterogeneity: Tau² = 0.02; Chi² = 4.19, df = 2 (P = 0.12); I² = 52%; Test for overall effect: Z = 0.95 (p = 0.34) | |||||||
| aa vs. AA | Kong, 2017 [21] | 118 | 162 | 70 | 88 | 33.9% | 0.69 [0.37, 1.29] |
| Yu, 2017 [37] | 82 | 115 | 97 | 121 | 34.8% | 0.61 [0.34, 1.12] | |
| Qin, 2019 [36] | 158 | 175 | 124 | 145 | 31.3% | 1.57 [0.80, 3.11] | |
| Subtotal (95%CI) | 452 | 354 | 100.0% | 0.86 [0.49, 1.50] | |||
| Total events | 358 | 291 | |||||
| Heterogeneity: Tau² = 0.14; Chi² = 4.68, df = 2 (P = 0.10); I² = 57%; Test for overall effect: Z = 0.54 (p = 0.59) | |||||||
| Aa vs. AA | Kong, 2017 [21] | 87 | 164 | 43 | 61 | 33.7% | 0.47 [0.25, 0.89] |
| Yu, 2017 [37] | 85 | 118 | 79 | 103 | 34.4% | 0.78 [0.43, 1.44] | |
| Qin, 2019 [36] | 129 | 146 | 100 | 121 | 31.8% | 1.59 [0.80, 3.18] | |
| Subtotal (95% CI) | 428 | 285 | 100.0% | 0.83 [0.42, 1.62] | |||
| Total events | 301 | 222 | |||||
| Heterogeneity: Tau² = 0.24; Chi² = 6.50, df = 2 (P = 0.04); I² = 69%; Test for overall effect: Z = 0.55 (p = 0.58) | |||||||
| aa + Aa vs. AA | Kong, 2017 [21] | 205 | 249 | 113 | 131 | 34.0% | 0.74 [0.41, 1.34] |
| Yu, 2017 [37] | 167 | 200 | 176 | 200 | 35.6% | 0.69 [0.39, 1.22] | |
| Qin, 2019 [36] | 287 | 304 | 224 | 245 | 30.4% | 1.58 [0.82, 3.07] | |
| Subtotal (95%CI) | 753 | 576 | 100.0% | 0.91 [0.55, 1.50] | |||
| Total events | 659 | 513 | |||||
| Heterogeneity: Tau² = 0.10; Chi² = 4.03, df = 2 (P = 0.13); I² = 50%; Test for overall effect: Z = 0.37 (p = 0.71) | |||||||
| aa vs. AA + Aa | Kong, 2017 [21] | 118 | 249 | 70 | 131 | 28.2% | 0.78 [0.51, 1.20] |
| Yu, 2017 [37] | 82 | 200 | 97 | 200 | 33.4% | 0.74 [0.50, 1.10] | |
| Qin, 2019 [36] | 158 | 304 | 124 | 245 | 38.5% | 1.06 [0.75, 1.48] | |
| Subtotal (95%CI) | 753 | 576 | 100.0% | 0.87 [0.69, 1.10] | |||
| Total events | 358 | 291 | |||||
| Heterogeneity: Chi² = 2.16, df = 2 (P = 0.34); I² = 8%; Test for overall effect: Z = 1.18 (p = 0.24) | |||||||
| Genetic Model | First Author, Publication Year | Case | Control | Weight | Odds Ratio | ||
|---|---|---|---|---|---|---|---|
| Events | Total | Events | Total | M-H, Random, 95%CI | |||
| f vs. F | Kong, 2017 [21] | 228 | 498 | 131 | 262 | 32.7% | 0.84 [0.63, 1.14] |
| Yu, 2017 [37] | 132 | 400 | 184 | 400 | 33.1% | 0.58 [0.43, 0.77] | |
| Qin, 2019 [36] | 152 | 608 | 221 | 490 | 34.2% | 0.41 [0.31, 0.52] | |
| Subtotal (95%CI) | 1506 | 1152 | 100.0% | 0.58 [0.38, 0.88] | |||
| Total events | 512 | 536 | |||||
| Heterogeneity: Tau² = 0.12; Chi² = 13.37, df = 2 (P = 0.001); I² = 85%; Test for overall effect: Z = 2.56 (p = 0.01) | |||||||
| ff vs. FF | Kong, 2017 [21] | 48 | 117 | 34 | 68 | 32.3% | 0.70 [0.38, 1.27] |
| Yu, 2017 [37] | 18 | 104 | 49 | 114 | 31.3% | 0.28 [0.15, 0.52] | |
| Qin, 2019 [36] | 46 | 144 | 51 | 126 | 36.4% | 0.69 [0.42, 1.14] | |
| Subtotal (95%CI) | 365 | 308 | 100.0% | 0.52 [0.29, 0.92] | |||
| Total events | 112 | 134 | |||||
| Heterogeneity: Tau² = 0.17; Chi² = 5.91, df = 2 (P = 0.05); I² = 66%; Test for overall effect: Z = 2.24 (p = 0.02) | |||||||
| Ff vs. FF | Kong, 2017 [21] | 132 | 201 | 63 | 97 | 23.3% | 1.03 [0.62, 1.72] |
| Yu, 2017 [37] | 96 | 182 | 86 | 151 | 35.5% | 0.84 [0.55, 1.30] | |
| Qin, 2019 [36] | 160 | 258 | 119 | 194 | 41.2% | 1.03 [0.70, 1.51] | |
| Subtotal (95% CI) | 641 | 442 | 100.0% | 0.96 [0.75, 1.24] | |||
| Total events | 388 | 268 | |||||
| Heterogeneity: Chi² = 0.54, df = 2 (P = 0.76); I² = 0; Test for overall effect: Z = 0.29 (p = 0.77) | |||||||
| ff + Aa vs. FF | Kong, 2017 [21] | 180 | 249 | 97 | 131 | 22.9% | 0.91 [0.57, 1.48] |
| Yu, 2017 [37] | 114 | 200 | 135 | 200 | 37.7% | 0.64 [0.42, 0.96] | |
| Qin, 2019 [36] | 206 | 304 | 170 | 245 | 39.4% | 0.93 [0.65, 1.33] | |
| Subtotal (95%CI) | 753 | 576 | 100.0% | 0.82 [0.64, 1.04] | |||
| Total events | 500 | 402 | |||||
| Heterogeneity: Chi² = 2.09, df = 2 (P = 0.35); I² = 4%; Test for overall effect: Z = 1.66 (p = 0.10) | |||||||
| ff vs. FF + Ff | Kong, 2017 [21] | 48 | 249 | 34 | 131 | 33.6% | 0.68 [0.41, 1.13] |
| Yu, 2017 [37] | 18 | 200 | 49 | 200 | 29.9% | 0.30 [0.17, 0.55] | |
| Qin, 2019 [36] | 46 | 304 | 51 | 245 | 36.6% | 0.68 [0.44, 1.05] | |
| Subtotal (95%CI) | 753 | 576 | 100.0% | 0.53 [0.33, 0.87] | |||
| Total events | 753 | 576 | 100.0% | 0.53 [0.33, 0.87] | |||
| Heterogeneity: Tau² = 0.12; Chi² = 5.53, df = 2 (P = 0.06); I² = 64%; Test for overall effect: Z = 2.53 (p = 0.01) | |||||||
| Genetic Model | First Author, Publication Year | Case | Control | Weight | Odds Ratio | ||
|---|---|---|---|---|---|---|---|
| Events | Total | Events | Total | M-H, Random, 95%CI | |||
| t vs. T | Cogulu, 2016 [32] | 108 | 224 | 32 | 76 | 7.3% | 1.28 [0.76, 2.16] |
| Holla, 2017 [34] | 170 | 470 | 119 | 306 | 27.3% | 0.89 [0.66, 1.20] | |
| Kong, 2017 [21] | 19 | 498 | 11 | 262 | 4.1% | 0.91 [0.42, 1.93] | |
| Yu, 2017 [37] | 29 | 400 | 42 | 400 | 11.6% | 0.67 [0.41, 1.09] | |
| Qin, 2019 [36] | 332 | 608 | 281 | 490 | 42.0% | 0.89 [0.70, 1.14] | |
| Aribam, 2020 [30] | 51 | 120 | 45 | 120 | 7.7% | 1.23 [0.73, 2.07] | |
| Subtotal (95%CI) | 2320 | 1654 | 100.0% | 0.92 [0.79, 1.08] | |||
| Total events | 709 | 530 | |||||
| Heterogeneity: Chi² = 4.47, df = 5 (P = 0.48); I² = 0%; Test for overall effect: Z = 1.03 (p = 0.30) | |||||||
| tt vs. TT | Cogulu, 2016 [32] | 31 | 66 | 9 | 24 | 22.2% | 1.48 [0.57, 3.85] |
| Holla, 2017 [34] | 30 | 125 | 17 | 68 | 53.1% | 0.95 [0.48, 1.88] | |
| Kong, 2017 [21] | 0 | 230 | 0 | 120 | Not estimable | ||
| Yu, 2017 [37] | 0 | 171 | 0 | 158 | Not estimable | ||
| Qin, 2019 [36] | 29 | 30 | 37 | 38 | 3.4% | 0.78 [0.05, 13.07] | |
| Aribam, 2020 [30] | 13 | 35 | 11 | 37 | 21.3% | 1.40 [0.52, 3.73] | |
| Subtotal (95%CI) | 657 | 445 | 100.0% | 1.15 [0.72, 1.86] | |||
| Total events | 103 | 74 | |||||
| Heterogeneity: Chi² = 0.79, df = 3 (P = 0.85); I² = 0%; Test for overall effect: Z = 0.58 (p = 0.56) | |||||||
| Tt vs. TT | Cogulu, 2016 [32] | 46 | 81 | 14 | 29 | 7.6% | 1.41 [0.60, 3.30] |
| Holla, 2017 [34] | 110 | 205 | 85 | 136 | 40.5% | 0.69 [0.45, 1.08] | |
| Kong, 2017 [21] | 19 | 249 | 11 | 131 | 11.4% | 0.90 [0.42, 1.96] | |
| Yu, 2017 [37] | 29 | 200 | 42 | 200 | 30.7% | 0.64 [0.38, 1.07] | |
| Qin, 2019 [36] | 274 | 275 | 207 | 208 | 0.7% | 1.32 [0.08, 21.29] | |
| Aribam, 2020 [30] | 25 | 47 | 23 | 49 | 9.0% | 1.28 [0.58, 2.86] | |
| Subtotal (95% CI) | 1057 | 753 | 100.0% | 0.81 [0.62, 1.07] | |||
| Total events | 503 | 382 | |||||
| Heterogeneity: Chi² = 4.36, df = 5 (P = 0.50); I² = 0%; Test for overall effect: Z = 1.49 (p = 0.14) | |||||||
| tt + Tt vs. TT | Cogulu, 2016 [32] | 77 | 112 | 23 | 38 | 8.7% | 1.43 [0.67, 3.08] |
| Holla, 2017 [34] | 140 | 235 | 102 | 153 | 40.5% | 0.74 [0.48, 1.13] | |
| Kong, 2017 [21] | 19 | 249 | 11 | 131 | 10.8% | 0.90 [0.42, 1.96] | |
| Yu, 2017 [37] | 29 | 200 | 42 | 200 | 29.1% | 0.64 [0.38, 1.07] | |
| Qin, 2019 [36] | 303 | 304 | 244 | 245 | 0.7% | 1.24 [0.08, 19.96] | |
| Aribam, 2020 [30] | 38 | 60 | 34 | 60 | 10.1% | 1.32 [0.63, 2.75] | |
| Subtotal (95%CI) | 1160 | 827 | 100.0% | 0.85 [0.66, 1.11] | |||
| Total events | 606 | 456 | |||||
| Heterogeneity: Chi² = 4.89, df = 5 (P = 0.43); I² = 0%; Test for overall effect: Z = 1.21 p = 0.23) | |||||||
| tt vs. TT + Tt | Cogulu, 2016 [32] | 31 | 112 | 9 | 38 | 13.2% | 1.23 [0.52, 2.90] |
| Holla, 2017 [34] | 30 | 235 | 17 | 153 | 24.5% | 1.17 [0.62, 2.21] | |
| Kong, 2017 [21] | 0 | 249 | 0 | 131 | Not estimable | ||
| Yu, 2017 [37] | 0 | 200 | 0 | 200 | Not estimable | ||
| Qin, 2019 [36] | 29 | 304 | 37 | 245 | 50.5% | 0.59 [0.35, 1.00] | |
| Aribam, 2020 [30] | 13 | 60 | 11 | 60 | 11.7% | 1.23 [0.50, 3.02] | |
| Subtotal (95%CI) | 1160 | 827 | 100.0% | 0.93 [0.62, 1.40] | |||
| Total events | 103 | 74 | |||||
| Heterogeneity: Chi² = 4.14, df = 3 (P = 0.25); I² = 28; Test for overall effect: Z = 0.72 (p = 0.35) | |||||||
| Genetic Model | First Author, Publication Year | Case | Control | Weight | Odds ratio | ||
|---|---|---|---|---|---|---|---|
| Events | Total | Events | Total | M-H, Random, 95%CI | |||
| b vs. B | Kong, 2017 [21] | 346 | 498 | 202 | 262 | 38.6% | 0.68 [0.48, 0.96] |
| Yu, 2017 [37] | 364 | 400 | 369 | 400 | 31.1% | 0.85 [0.51, 1.40] | |
| Qin, 2019 [36] | 580 | 608 | 457 | 490 | 30.3% | 1.50 [0.89, 2.51] | |
| Subtotal (95%CI) | 1506 | 1152 | 100.0% | 0.92 [0.58, 1.46] | |||
| Total events | 1290 | 1028 | |||||
| Heterogeneity: Tau² = 0.11; Chi² = 6.24, df = 2 (P = 0.04); I² = 68%; Test for overall effect: Z = 0.34 (p = 0.73) | |||||||
| bb vs. BB | Kong, 2017 [21] | 97 | 97 | 71 | 71 | Not estimable | |
| Yu, 2017 [37] | 164 | 164 | 169 | 169 | Not estimable | ||
| Qin, 2019 [36] | 276 | 276 | 213 | 214 | 100.0% | 3.89 [0.16, 95.85] | |
| Subtotal (95%CI) | 537 | 454 | 100.0% | 3.89 [0.16, 95.85] | |||
| Total events | 537 | 453 | |||||
| Heterogeneity: Not applicable; Test for overall effect: Z = 0.83 (p = 0.41) | |||||||
| Bb vs. BB | Kong, 2017 [21] | 152 | 152 | 60 | 60 | Not estimable | |
| Yu, 2017 [37] | 36 | 36 | 31 | 31 | Not estimable | ||
| Qin, 2019 [36] | 28 | 28 | 31 | 32 | 100.0% | 2.71 [0.11, 69.34] | |
| Subtotal (95% CI) | 216 | 123 | 100.0% | 2.71 [0.11, 69.34] | |||
| Total events | 216 | 122 | |||||
| Heterogeneity: Not applicable; Test for overall effect: Z = 0.60 (p = 0.55) | |||||||
| bb + Bb vs. BB | Kong, 2017 [21] | 249 | 249 | 131 | 131 | Not estimable | |
| Yu, 2017 [37] | 200 | 200 | 200 | 200 | Not estimable | ||
| Qin, 2019 [36] | 304 | 304 | 244 | 245 | 100.0% | 3.74 [0.15, 92.12] | |
| Subtotal (95%CI) | 753 | 576 | 100.0% | 3.74 [0.15, 92.12] | |||
| Total events | 753 | 575 | |||||
| Heterogeneity: Not applicable; Test for overall effect: Z = 0.81 (p = 0.42) | |||||||
| bb vs. BB + Bb | Kong, 2017 [21] | 97 | 249 | 71 | 131 | 35.6% | 0.54 [0.35, 0.83] |
| Yu, 2017 [37] | 164 | 200 | 169 | 200 | 32.4% | 0.84 [0.49, 1.41] | |
| Qin, 2019 [36] | 276 | 304 | 213 | 245 | 32.0% | 1.48 [0.86, 2.54] | |
| Subtotal (95%CI) | 753 | 576 | 100.0% | 0.86 [0.48, 1.54] | |||
| Total events | 537 | 453 | |||||
| Heterogeneity: Tau² = 0.20; Chi² = 8.32, df = 2 (P = 0.02); I² = 76%; Test for overall effect: Z = 0.51 (p = 0.61) | |||||||
| Genetic Model | First Author, Publication Year | Case | Control | Weight | Odds Ratio | ||
|---|---|---|---|---|---|---|---|
| Events | Total | Events | Total | M-H, Random, 95%CI | |||
| f vs. F | Barbosa, 2020 [31] | 226 | 328 | 244 | 358 | 46.3% | 1.04 [0.75, 1.43] |
| Fatturi, 2020 [33] | 279 | 408 | 175 | 264 | 42.9% | 1.10 [0.79, 1.53] | |
| Madalena, 2020 [35] | 178 | 276 | 27 | 38 | 10.8% | 0.74 [0.35, 1.56] | |
| Subtotal (95%CI) | 1012 | 660 | 100.0% | 1.03 [0.83, 1.28] | |||
| Total events | 683 | 446 | |||||
| Heterogeneity: Chi² = 0.91, df = 2 (P = 0.63); I² = 0%; Test for overall effect: Z = 0.29 (p = 0.77) | |||||||
| ff vs. FF | Barbosa, 2020 [31] | 81 | 100 | 82 | 99 | 47.5% | 0.88 [0.43, 1.82] |
| Fatturi, 2020 [33] | 97 | 119 | 56 | 69 | 39.7% | 1.02 [0.48, 2.19] | |
| Madalena, 2020 [35] | 59 | 78 | 10 | 12 | 12.8% | 0.62 [0.12, 3.09] | |
| Subtotal (95%CI) | 297 | 180 | 100.0% | 0.91 [0.55, 1.50] | |||
| Total events | 237 | 148 | |||||
| Heterogeneity: Chi² = 0.32, df = 2 (P = 0.85); I² = 0%; Test for overall effect: Z = 0.37 (p = 0.71) | |||||||
| Ff vs. FF | Barbosa, 2020 [31] | 64 | 83 | 80 | 97 | 48.2% | 0.72 [0.34, 1.49] |
| Fatturi, 2020 [33] | 85 | 107 | 63 | 76 | 43.2% | 0.80 [0.37, 1.70] | |
| Madalena, 2020 [35] | 60 | 79 | 7 | 9 | 8.6% | 0.90 [0.17, 4.72] | |
| Subtotal (95% CI) | 269 | 182 | 100.0% | 0.77 [0.46, 1.27] | |||
| Total events | 209 | 150 | |||||
| Heterogeneity: Chi² = 0.08, df = 2 (P = 0.96); I² = 0%; Test for overall effect: Z = 1.04 (p = 0.30) | |||||||
| ff + Ff vs. FF | Barbosa, 2020 [31] | 145 | 164 | 162 | 179 | 47.7% | 0.80 [0.40, 1.60] |
| Fatturi, 2020 [33] | 182 | 204 | 119 | 132 | 41.4% | 0.90 [0.44, 1.86] | |
| Madalena, 2020 [35] | 119 | 138 | 17 | 19 | 10.9% | 0.74 [0.16, 3.45] | |
| Subtotal (95%CI) | 506 | 330 | 100.0% | 0.84 [0.52, 1.35] | |||
| Total events | 446 | 298 | |||||
| Heterogeneity: Chi² = 0.09, df = 2 (P = 0.96); I² = 0%; Test for overall effect: Z = 0.73 (p = 0.46) | |||||||
| ff vs. FF + Ff | Barbosa, 2020 [31] | 81 | 164 | 82 | 179 | 46.5% | 1.15 [0.76, 1.76] |
| Fatturi, 2020 [33] | 97 | 204 | 56 | 132 | 41.8% | 1.23 [0.79, 1.91] | |
| Madalena, 2020 [35] | 59 | 138 | 10 | 19 | 11.8% | 0.67 [0.26, 1.76] | |
| Subtotal (95%CI) | 506 | 330 | 100.0% | 1.13 [0.84, 1.51] | |||
| Total events | 237 | 148 | |||||
| Heterogeneity: Chi² = 1.27, df = 2 (P = 0.53); I² = 0%; Test for overall effect: Z = 0.82 (p = 0.41) | |||||||
| Genetic Model | First Author, Publication Year | Case | Control | Weight | Odds Ratio | ||
|---|---|---|---|---|---|---|---|
| Events | Total | Events | Total | M-H, Random, 95%CI | |||
| b vs. B | Barbosa, 2020 [31] | 186 | 326 | 203 | 376 | 48.1% | 1.13 [0.84, 1.53] |
| Fatturi, 2020 [33] | 199 | 426 | 112 | 242 | 45.2% | 1.02 [0.74, 1.40] | |
| Madalena, 2020 [35] | 120 | 198 | 16 | 24 | 6.7% | 0.77 [0.31, 1.88] | |
| Subtotal (95%CI) | 950 | 642 | 100.0% | 1.06 [0.86, 1.31] | |||
| Total events | 505 | 331 | |||||
| Heterogeneity: Chi² = 0.74, df = 2 (P = 0.69); I² = 0%; Test for overall effect: Z = 0.51 (p = 0.61) | |||||||
| bb vs. BB | Barbosa, 2020 [31] | 52 | 81 | 58 | 101 | 45.8% | 1.33 [0.73, 2.43] |
| Fatturi, 2020 [33] | 49 | 112 | 27 | 63 | 48.1% | 1.04 [0.56, 1.93] | |
| Madalena, 2020 [35] | 34 | 47 | 5 | 6 | 6.1% | 0.52 [0.06, 4.91] | |
| Subtotal (95%CI) | 240 | 170 | 100.0% | 1.15 [0.75, 1.75] | |||
| Total events | 135 | 90 | |||||
| Heterogeneity: Chi² = 0.80, df = 2 (P = 0.67); I² = 0%; Test for overall effect: Z = 0.63 (p = 0.53) | |||||||
| Bb vs. BB | Barbosa, 2020 [31] | 82 | 111 | 87 | 130 | 40.7% | 1.40 [0.80, 2.44] |
| Fatturi, 2020 [33] | 101 | 164 | 58 | 94 | 55.1% | 1.00 [0.59, 1.68] | |
| Madalena, 2020 [35] | 52 | 65 | 6 | 7 | 4.2% | 0.67 [0.07, 6.03] | |
| Subtotal (95% CI) | 340 | 231 | 100.0% | 1.15 [0.79, 1.67] | |||
| Total events | 235 | 151 | |||||
| Heterogeneity: Chi² = 1.00, df = 2 (P = 0.61); I² = 0%; Test for overall effect: Z = 0.71 (p = 0.48) | |||||||
| bb + Bb vs. BB | Barbosa, 2020 [31] | 134 | 163 | 145 | 188 | 40.9% | 1.37 [0.81, 2.32] |
| Fatturi, 2020 [33] | 150 | 213 | 85 | 121 | 54.7% | 1.01 [0.62, 1.64] | |
| Madalena, 2020 [35] | 86 | 99 | 11 | 12 | 4.4% | 0.60 [0.07, 5.05] | |
| Subtotal (95%CI) | 475 | 321 | 100.0% | 1.14 [0.80, 1.62] | |||
| Total events | 370 | 241 | |||||
| Heterogeneity: Chi² = 1.06, df = 2 (P = 0.59); I² = 0%; Test for overall effect: Z = 0.73 (p = 0.46) | |||||||
| bb vs. BB + Bb | Barbosa, 2020 [31] | 52 | 163 | 58 | 188 | 53.1% | 1.05 [0.67, 1.65] |
| Fatturi, 2020 [33] | 49 | 213 | 27 | 121 | 38.4% | 1.04 [0.61, 1.77] | |
| Madalena, 2020 [35] | 34 | 99 | 5 | 12 | 8.5% | 0.73 [0.22, 2.48] | |
| Subtotal (95%CI) | 475 | 321 | 100.0% | 1.02 [0.73, 1.42] | |||
| Total events | 135 | 90 | |||||
| Heterogeneity: Chi² = 0.30, df = 2 (P = 0.86); I² = 0%; Test for overall effect: Z = 0.11 (p = 0.91) | |||||||
| Variable (N) | t vs. T | tt vs. TT | Tt vs. TT | tt + Tt vs. TT | tt vs. TT + Tt |
|---|---|---|---|---|---|
| OR (95%CI), p, I2 | OR (95%CI), p, I2 | OR (95%CI), p, I2 | OR (95%CI), p, I2 | OR (95%CI), p, I2 | |
| Ethnicity | |||||
| Caucasian (3) | 1.02 (0.81, 1.29), 0.86, 2% | 1.17 (0.72, 1.89), 0.53, 0% | 0.96 (0.59, 1.56), 0.87, 36% | 1.02 (0.64, 1.61), 0.94, 39% | 1.20 (0.77, 1.87), 0.42, 0% |
| Asian (3) | 0.85 (0.69, 1.05), 0.13, 0% | 0.75 (0.05, 13.07), 0.87 | 0.72 (0.47, 1.10), 0.13, 0% | 0.72 (0.47, 1.10), 0.13, 0% | 0.59 (0.35, 1.00), 0.05 |
| Genotyping method | |||||
| PCR (4) | 0.99 (0.71, 1.37), 0.95, 27% | 1.44 (0.72, 2.85), 0.30, 0% | 0.91 (0.62, 1.33), 0.63, 14% | 0.96 (0.64, 1.43), 0.83, 28% | 1.23 (0.66, 2.29), 0.51, 0% |
| TaqMan (2) | 0.89 (0.74, 1.08), 0.23, 0% | 0.94 (0.48, 1.82), 0.85, 0% | 0.71 (0.46, 1.09), 0.12, 0% | 0.75 (0.49, 1.14), 0.17, 0% | 0.81 (0.42, 1.58), 0.54, 62% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadeghi, M.; Golshah, A.; Godiny, M.; Sharifi, R.; Khavid, A.; Nikkerdar, N.; Tadakamadla, S.K. The Most Common Vitamin D Receptor Polymorphisms (ApaI,FokI, TaqI, BsmI, and BglI) in Children with Dental Caries: A Systematic Review and Meta-Analysis. Children 2021, 8, 302. https://doi.org/10.3390/children8040302
Sadeghi M, Golshah A, Godiny M, Sharifi R, Khavid A, Nikkerdar N, Tadakamadla SK. The Most Common Vitamin D Receptor Polymorphisms (ApaI,FokI, TaqI, BsmI, and BglI) in Children with Dental Caries: A Systematic Review and Meta-Analysis. Children. 2021; 8(4):302. https://doi.org/10.3390/children8040302
Chicago/Turabian StyleSadeghi, Masoud, Amin Golshah, Mostafa Godiny, Roohollah Sharifi, Atefeh Khavid, Nafiseh Nikkerdar, and Santosh Kumar Tadakamadla. 2021. "The Most Common Vitamin D Receptor Polymorphisms (ApaI,FokI, TaqI, BsmI, and BglI) in Children with Dental Caries: A Systematic Review and Meta-Analysis" Children 8, no. 4: 302. https://doi.org/10.3390/children8040302