
Biodetection Techniques for Quantification of Chemokines
by
 , , and
, , and
Esther Sánchez-Tirado
 ,
,
Lourdes Agüí
,
Araceli González-Cortés
,
Paloma Yáñez-Sedeño
* and
José M. Pingarrón

Analytical Chemistry, Faculty of Chemistry, Universidad Complutense de Madrid, 28040 Madrid, Spain
*
Author to whom correspondence should be addressed.
Chemosensors 2022, 10(8), 294; https://doi.org/10.3390/chemosensors10080294
Submission received: 27 June 2022
/
Revised: 23 July 2022
/
Accepted: 24 July 2022
/
Published: 27 July 2022
(This article belongs to the Special Issue Chemical Sensors and Biosensors for Biomedical and Environmental Application: Recent Advances and Future Perspectives)
Abstract
:Chemokines are a class of cytokine whose special properties, together with their involvement and relevant role in various diseases, make them a restricted group of biomarkers suitable for diagnosis and monitoring. Despite their importance, biodetection techniques dedicated to the selective determination of one or more chemokines are very scarce. For some years now, the critical diagnosis of inflammatory diseases by detecting both cytokine and chemokine biomarkers, has had a strong impact on the development of multiple detection platforms. However, it would be desirable to implement methodologies with a higher degree of selectivity for chemokines, in order to provide more precise information. In addition, better development of biosensor technology applied to this specific field would make it possible to address the main challenges of detection methods for several diseases with a high incidence in the population, avoiding high costs and low sensitivity. Taking this into account, this review aims to present the state of the art of chemokine biodetection techniques and emphasize the role of these systems in the prevention, monitoring and treatment of various diseases associated with chemokines as a starting point for future developments that are also analyzed throughout the article.
1. Introduction
Chemokines or chemotactic cytokines constitute a large group of low-molecular-weight proteins (8–12 kDa) with 70–90 amino acids which play decisive roles in angiogenesis and viral infection processes by inducing the migration of immune cells in specific tissues and organs through chemotaxis [1] with cell differentiation and development, and/or cancer metastasis [2]. These proinflammatory proteins attract leukocytes and other cell types via binding with their corresponding receptors [3,4]. The first chemokine was identified in 1977, when platelet factor 4 (PF4/CXCL4) was purified [5]. Later, chemotactic activity for neutrophils by interleukin-8 (IL-8/CXCL8) was shown [6] and, more recently, it was discovered certain chemokines contribute to the HIV suppressive effect in vitro [7,8]. Currently, it has become apparent that chemokines are involved in virtually all pathologies that present an inflammatory component including neurodegenerative diseases [9].
Although they belong to the cytokine family (Figure 1A), chemokines are considered as a specific group due to their importance. Nowadays, these proteins constitute a separate category of selective biomarkers for the diagnosis and monitoring of disorders derived from inflammatory autoimmune and neurological processes. It is known that chemotactic cytokines are produced in inflamed tissue by a wide variety of cell types in response to exogenous or endogenous factors such as lipopolysaccharides, viruses, autoantigens, and inflammatory cytokines [10,11,12]. Once secreted by cells they bind and activate G protein–coupled receptors; these proteins act as inflammatory mediators and immunological modulators by creating an extracellular concentration gradient that is specifically recognized by cells and promotes their movement. Thus, chemokines regulate leukocyte migration in response to extracellular gradients of diffusible chemicals through chemokine receptors [13,14]. This enables the response to inflammation of the immune system by movement of cells responsible for surveillance and antigen uptake. In a second step, subsequent altered expression of chemokine receptors in the cells enables them to exit towards lymphoid organs where specific antigen immunity is initiated. In this way, chemokines fulfil functions such as directing the traffic of various cells to mediate the immune response (i.e., in the case of an infection), as well as promoting homeostasis and development at the cellular level [15].
The expression and production of chemotactic cytokines are induced by a variety of factors in vivo in order to recruit immune cells to inflamed tissue, while the secreted chemokines bind to membrane-bound proteoglycans creating chemotactic gradients that guide the migration of immune cells [17,18]. Quantification of the levels of chemokine secretion by cells, in parallel with the study of their interactions with receptors, are of great interest to understand the regulation and function of chemokines. These objectives justify the creation of new biosensing systems for these proteins in complex samples.
2. Classification of Chemokines
Chemotactic cytokines are characterized by the presence of three or four cysteine residues whose relative position in the amino acid backbone may be used for classifying them into four families: CC, CXC, C, CX3C, where C is a cysteine and X stands for any amino acid residue (Figure 1B) [3,19,20]. More than 50 chemokines and approximately 20 chemokine receptors have been described, with CC (CCL1 through CCL28) and CXC (CXCL1 to CXCL17) forming the two major groups [1,3,10,11,12,20]. The CXC chemokine branch can be further subdivided by structure and function into proteins containing or lacking the amino acid motif ELR (Glu-Leu-Arg) terminal to CXC. Particularly, the C–X–C family is characterized by the separation of the two N-terminal cysteines by one variable amino acid residue while in the C–C subfamily the cysteine residues are adjacent to each other [21]. More than forty different chemokines have been identified in humans [22]. Importantly, structural distinctions of the different branches of chemokines have been shown to parallel differences in their biological activities with some few exceptions [23]. As examples, the CC group is chemotactic primarily for T lymphocytes, monocytes and macrophages, natural killer (NK) cells, basophils, and eosinophils, whereas CXC chemokines are chemotactic mainly for neutrophils, whose adherence to endothelial cells is also promoted [1,4,10,19,24].
3. Chemokine Biomarkers and Related Diseases
The critical role that chemokine–chemokine receptor interactions play in the development, function and homeostasis of the immune system, as well as in the pathogenesis of numerous diseases including viral infection [25], cancer [26], neurological disorders [27] and autoimmune diseases [28] has already been discussed. Table 1 summarizes various chemokines whose expression in biological matrices are useful as biomarkers for detection and monitoring of respective diseases [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43].
In the following, the two most important groups of diseases in which these proteins are involved, cancer and autoimmune diseases, and the role of several chemokines for diagnosis and monitoring of related disorders, are discussed.
3.1. Cancer
Chemokines, which play a crucial role in inflammation and immunity, are also key cancer mediators. They are present at the tumor site in pre-existing chronic inflammatory conditions and are also targeted by oncogenic pathways. Their altered expression in malignant neoplasms drives leukocyte recruitment and activation, as well as angiogenesis, cancer cell proliferation and metastasis at all stages of disease [44]. The amount of evidence and research in this field describing pro-cancer properties of chemokines and their receptors, as well as the possibilities for their use in anti-cancer therapies is enormous, and has been reviewed in various articles [45,46,47]. Therefore, in this section, representative examples have been selected to illustrate the role of chemokines in cancer, with the criterion of choosing the most recent articles in which methods dedicated to the determination of specific chemokines involving different techniques were developed.
Due to its tumorigenic and proangiogenic properties, interleukin-8 (IL-8, CXCL8) is one of the most investigated chemokines in relation to cancer [37,48]. It plays an important role in the process of glioma stem-like cell vascularization, being expressed and secreted in human gliomas at levels associated with their histological grade [49]. Upregulated CXCL8 is also found in breast cancer and its involvement is reported in progression and metastases in HER2-positive cancers [50]. This chemokine has also been used as a biomarker of bladder cancer (BCa) where urothelial carcinomas constitute the majority of all cases [51]. It has been seen that the determination of CXCL8 (and several cytokines) in urine can provide adequate tools for the diagnosis and therapeutic planning of patients with BCa, since this body fluid maintains close contact with tumor cells and the adjacent inflamed urothelium. [52]. Indeed, urinary concentrations of this chemokine appear significantly elevated in BCa patients with both muscle-invasive bladder cancer (MIBC) and non-muscle-invasive bladder cancer (NMIBC), compared to healthy individuals and those with hematuria.
Secreted chemokines act as mediators of cell communication by binding to membrane-bound receptors and triggering intracellular signaling. Among them, CXCL12 is a prototype chemokine. Also known as a stromal-derived factor, it binds to the CXCR4 receptor, resulting in a very useful biomarker for monitoring various types of cancer [53]. The role of the CXCL12–CXCR4 axis in tumour growth and metastasis, and in cancer cell-tumour microenvironment interaction and angiogenesis was reviewed [54]. The tumor promoting activity of CXCL12–CXCR4 in various cancers affecting organs such as kidney, lung or pancreas was established [55]. Increased hepatocyte CXCL12 expression is also associated with melanoma [56] and with the process of tumorigenesis and metastasis in colorectal cancer (CRC) [57].
Specifically taking into account chemokine receptors, the recent studies demonstrating their role in processes of metastasis, including those related to squamous cell carcinoma of the head and neck (HNSCC), should be highlighted [58]. Particular expressions of the paired chemokine–receptor are developed by metastatic tumor cells from cancers affecting breast, liver, prostate or stomach, which significantly correlate with the produced chemokines within distant organs and lymphatic sites to which such cells metastasize. It is known that a wide variety of cell types, mainly leukocytes, express chemokines binding to transmembrane G protein–coupled receptors (GPCRs). This provokes conformational changes in trimeric G proteins that trigger the intracellular signaling pathways required for cell movement and activation. Furthermore, it has been observed that chemokine GPCRs are involved in the initiation and progression of cancers affecting multiple organs [59], suggesting that expression of chemokine GPCRs detecting ligands as growth signals may be the driving force that allows invasion and metastasis in many cancer cells. Among them, one of the most frequently identified chemokine GPCRs in cancer is CXCR4, which has been implicated in more than 23 human cancers.
One of the most common malignancies worldwide is lung cancer, with non-small cell lung cancer (NSCLC) being the most frequent [60]. Importantly, levels of the CXCL10/IP10 chemokine detected in NSCLC tumors are significantly higher than those in adjacent normal lung tissue, which evidences the role of this chemokine in the regulation of NSCLC-induced angiogenesis, as well as in tumor growth and metastasis. In addition to CXCL10, the CXCR4/CXCR7/CXCL12 chemokine axis actively participates in the migration of tumor cells during cancer development by modulating metastasis to specific distant sites including lymph nodes. In this context, it is important to note that high expression of CXCR4 in primary sites and CXCL12 in metastatic lymph nodes have been associated with poor overall survival [61]. Moreover, another chemokine, CCL17/TARC, has been also considered as a highly promising blood biomarker for classic Hodgkin lymphoma (cHL), for its use in early diagnosis, monitoring of treatment response, and relapse detection [62].
3.2. Autoimmune Diseases
Frequently, autoimmune diseases manifest clinically as the consequence of a strong immune response to a particular self-antigen, which leads to significant activation/accumulation of leukocytes in the tissue of the target organ and the subsequent pathology [28]. Chemokines are involved in these processes, since they provide the population of leukocytes necessary to participate in the inflammatory response. Particularly, several chemokines and chemokine receptors, whose role in rheumatoid arthritis (RA) has been recently reviewed [63], are abundant in the peripheral blood and in the local inflamed joints of RA. Expression of CXCL4 and CXCL7 chemokines in patients with early RA may be used to predict progression of early-stage synovitis [64]. Indeed, increased levels of both chemokines were observed in the synovium of these patients compared to those with a resolving disease course. In RA, cells of the immune system including neutrophils, macrophages, B cells, natural killer (NK) cells and T cells migrate to the synovial membrane and, after accumulation in the synovial fluid, they lead to the release of chemokines. Among them, CCL2 (monocyte chemoattractant protein-1, MCP-1) plays an important role in various events related to RA pathogenesis, including migration of effector T cells to the RA synovium tissue and angiogenesis [65]. A significant increase in CCL2 in the synovium of patients with RA is observed, the disease activity score being associated with CCL2 levels, which suggest this chemokine be considered a suitable biomarker of RA [66]. CX3C Ligand 1 chemokine (CX3CL1), also named fractalkine, also participates in monocyte chemotaxis and angiogenesis in RA disease. Increased MMP-2 production from synovial fibroblasts upon CX3CL1 stimulation in vitro was observed, which suggests a pro-inflammatory activity [67].
Multiple sclerosis (MS) is a chronic autoimmune and demyelinating neurodegenerative disorder of the central nervous system (CNS) [68]. This disease is characterized by the attack of abnormally infiltrated immune cells, mainly T-cells, B-cells, and macrophages, that provoke damage to the myelin sheath and oligodendrocytes of the CNS. This action results in demyelination and axonal degeneration to varying degrees, that give rise to dense scar-like tissue, a hallmark of MS. The clinical manifestations of MS can range from relatively mild neurological symptoms to highly debilitating disease. CXCL13 is a validated biomarker for MS [69], playing a role in B-cell recruitment to the CNS during inflammation. It is also considered as a disease activity biomarker present at increased concentrations in patients with active disease which suffer relapsing–remitting and progressive disease courses. Cui et al. recently reviewed the role of chemokine and chemokine receptors in MS [70]. Several CCL-type chemokines are involved in MS disease. For example, CCL5 (RANTES, regulated on activation of normal T cell expressed and secreted) induce the recruitment of immune cells to the CNS via interaction with its receptor CCR5. Thus, it could in principle also regulate synaptic transmission and brain plasticity, [71] in addition to acting in inflammatory regulation. Indeed, an increase in the central levels of CCL5 is associated with the inflammatory process typical of MS which in turn causes significant changes in synaptic excitability of central neurons. Other chemokines proposed as MS biomarkers are CCL11, associated with disease duration and progression, and CCL20 which is related to disease severity. Immunoassay proteomic research has also allowed identification of up-regulated CCL3 (MIP-1a) and CXCL10 in cerebrospinal fluid (CSF) of patients with MS, and a higher expression of both chemokines in active lesions [72].
The correlation existing between chemokines and thyroid autoimmunity has been demonstrated in various studies. This is evidenced by the results obtained in the investigation of patients with Graves’ disease (GD), where the presence of CXCL10 in thyroid follicular cells [73] or the high level of CCL2 (MCP-1) in cultured human thyrocytes [74], and the increased expression of CXCL12 (SDF-1) and CXCL1 (Gro1) in thyroid tissues [75] were reported. Circulating levels of these chemokines are associated with the active phase of GD [76], autoimmune thyroiditis, and other diseases. For example, patients with Hashimoto’s thyroiditis exhibited increased expression of CXCR3 and of CCR2 and CCR5 receptors for CCL5 and CCL2, respectively [77]. Importantly, the wide variability in chemokine expression was related to disease duration. Thus, increased CXCL10 expression was found in the thyroid of recent-onset patients compared with long-standing patients [78]. These results agree with those of Armengol et al., showing increased expression of CXCL12, CXCL13, CCL21, and CCL22 in HT thyroid glands [79,80]. Furthermore, Kemp et al. detected CXCL10, as well as CCL2, CCL3, CCL4, and CCL5 in thyroid tissue from patients with HT [81].
4. Biodetection Methods for Determination of Chemokines
Methods to determine chemokine levels are mostly based on immunoassays such as ELISA. At present, commercially available ELISA kits make it possible to measure several cytokines and chemokines in biological samples and cell culture supernatants [82]. Western blotting analysis has also been used to investigate the expression of various chemokines in biological fluids [83]. However, methods involving such techniques have limited sensitivity for detecting very small amounts of the target compounds such as concentrations below pg/mL that appear as cut-off levels for individuals suspected of suffering from some diseases, or to determine mis-expressed proteins [84]. In the case of immunoassays, most require long assay times, taking up to five hours, and do not allow investigation of the secretion of chemokines in real time [85], also relying on the availability of specific and sensitive immuno-reagents. Nevertheless, there are a lot of kits for the determination of individual chemokines which are commonly used as reference methods for validation of results obtained in sample analysis using other methodologies, mainly biosensors.
As will be seen in what follows, the development of biosensors for the determination of chemokines is still scarce. However, it should be emphasized that these devices have ideal analytical characteristics for the diagnosis, prognosis and monitoring of diseases such as cancer or autoimmune disorders, since they allow real-time measurements and can detect minimal amounts of biomarkers (in some cases at the fg/mL level) in very small volumes—below microliter units—of physiological samples, based on antibodies, peptides, nucleic acids, receptors or other types of biomolecules capable of interacting with the chemokine of interest. Table 2 summarizes the methods and analytical characteristics of some recent biosensors using different detection techniques, which have been applied to clinical samples [37,38,62,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109]. In the following sections we discuss the relevant aspects of some selected designs. For better understanding, several sub-sections for the different instrumental techniques used were also considered.
4.1. Electrochemical Techniques
A variety of electrochemical biosensors have been proposed for the determination of CXCL8 (IL-8) alone or together with various cytokines. This is probably due to the implication of this chemokine in important inflammatory diseases and cancer [20]. Torrente et al. [100] prepared a dual biosensing platform for the simultaneous determination of CXCL8 and its associated messenger RNA oligonucleotide, which involved the use of carboxyl- and streptavidin-functionalized magnetic microparticles (MBs), respectively, as supports for immobilization of the capture anti-CXCL8 antibody to implement a sandwich-type immunoassay, as well as binding of BHCpCXCL8 for subsequent hybridization with the biotinylated target DNA, which were finally labelled with Strept-HRP. The resulting method, involving amperometric detection at disposable SPCEs, allowed limits of detection of 0.21 nM and 72.4 pg/mL for the respective targets, and it was successfully applied to the determination of CXCL8 in undiluted human saliva. More recently, a label-free impedimetric immunosensor for CXCL8 was also prepared using anti-fouling zwitterionic hydrogel polycarboxybetaine methacrylate (pCBMA) to immobilize polyclonal anti-CXCL8 antibody. The charge transfer resistance (Rct) changes were used as the analytical signal to determine CXCL8 in a wide range of detection, from 55 fM to 55 nM, with a limit of detection (LOD) value of 10 fM. Interestingly, the immunosensor was successfully applied to determine CXCL8 in samples of nasal epithelial lining fluid (NELF) of asthma patients and healthy individuals [99].
Because of the low levels of chemokines existing in biological fluids, ranging between pg/mL to low ng/mL, one of the main objectives in the construction of an electrochemical biosensor for these biomarkers is obtaining high sensitivity. To achieve this, widely used strategies are those involving the employment of nanomaterials capable of amplifying the response due to their high conductivity while enabling stable immobilization of bioreagents. In this context, an interesting article of Aydin et al. [92] reported the preparation of a composite consisting of Super P© carbon black, polyvinylidene fluoride (PVDF) and star shaped poly(glycidylmethacrylate) (PGMA) as a useful modifier of a disposable ITO electrode for the construction of a label-free impedimetric CXCL8/IL-8 biosensor. Figure 2 illustrates the steps of composite preparation and fabrication of the electrode by a spin coating process. As can also be seen, specific anti-CXCL8/IL-8 capture antibodies were bound covalently to epoxy groups of the star polymer. Under optimum conditions, measurements of the charge transfer resistance (ΔRct) provided a wide linear 0.01–3 pg/mL range and a low detection limit of 3.3 fg/mL. The applicability of the proposed immunosensor to determine CXCL8 in saliva and serum samples was also investigated.
Another label-free biosensor for CXCL8/IL-8 using electrochemical impedance spectroscopy (EIS) with a detection limit of 90 fg/mL in full serum, was developed by Sharma et al. [98]. A self-assembled monolayer (SAM) was prepared using monothiol-alkane-PEG-acid which has anti-fouling properties and also prevents non-specific adsorption onto gold electrodes. Synthetic antibody mimetic proteins with high affinity to the human chemokine were selected via phage display and covalently immobilized on the carboxyl groups. On the resulting electrode surface, binding of biomarkers to the capture reagents resulted in a variation in the local environment of the SAM leading to changes in monolayer defects and in the electrochemical impedance, which can be measured as a change in the phase Δθ(f). Hence, such electrodes are sensitive to the variation of CXCL8 concentrations in the range of 9 fg/mL to 900 ng/mL.
It has been found that CXCL5 also plays important roles in tumorigenesis and cancer progression; studies suggest that this chemokine promotes cell metastasis through tumor angiogenesis in colorectal cancer (CRC). Therefore, the detection of this chemokine could serve as a potential prognostic biomarker for cancer patients [110] However, despite its importance, the number of methods developed for biodetection of CXCL5 are very scarce [111]. As an example, a biosensor for detection of CXCL5 in the CRC cell line was developed by Chung et al. [87]. It was based on the immobilization of CXCR2 onto a glassy carbon electrode modified with gold nanoparticles (AuNPs) and an electro-polymerized 2,2′:5′,2″-terthiophene-3′ (p-benzoic acid) (TBA) nanocomposite film. Interestingly, a chemokine receptor, CXCR2, for which the target has natural affinity, was used for biosensor development. Amperometric detection provided a method with a calibration range between 0.1 and 10 ng/mL CXCL5. The LOD value was 0.078 ± 0.004 ng/mL. The proposed biosensor was successfully applied to determine clinically relevant concentrations of this chemokine in human serum and CRC cells, with high sensitivity and selectivity. Regarding the latter samples, HT-29 cells which are known to secrete CXCL5 extracellularly, were analyzed for recovery studies after spiking with the chemokine in autoclaved PBS solution containing 105 cells/mL.
Also related to cancer detection, it is worth highlighting the development of an electrochemical affinity biosensor for CCL17/TARC (thymus- and activation-regulated chemokine) as a tool for rapid triage and monitoring of classical Hodgkin lymphoma (cHL) [62]. Indeed, this chemokine is secreted by cHL tumor cells and has recently emerged as blood biomarker for this disease [112]. The amperometric immunosensor proposed by Rinaldi et al., involved a thiolated heterobifunctional cross-linker, sulfo-LC-SPDP, chemisorbed onto gold electrodes for immobilization of the specific capture antibody and preparation of a sandwich design with biotinylated CCL17 secondary antibody conjugated with streptavidin-HRP. The resulting bioelectrode showed excellent analytical performance using 3,3′,5,5′-tetramethylbenzidine (TMB) and hydrogen peroxide for the electrochemical measurements, covering a linear range of 387 to 50,000 pg/mL CCL17 with a LOD value of 194 pg/mL. An important achievement in this work was to demonstrate the ability of the immunosensor to differentiate healthy individuals from 42 diagnosed cHL patients by analyzing blood serum, and to discriminate between samples of patients collected prior to treatment and during chemotherapy on the basis of the decrease in chemokine level.
Multiplexed biosensors for the simultaneous determination of chemokines have also been described. These configurations are of great interest for the diagnosis and monitoring of diseases in which quantification of chemokines, often present in biological samples together with various other cytokines, are essential for a better understanding of the disorder’s evolution. As an example, Tanak et al. [101], prepared a multiplexed biosensor involving host immune response for rapid sepsis stratification and endotyping. Sepsis is an intricate condition characterized by a dysfunctional immune response which often is misdiagnosed with serious health consequences [113]. For the purpose of being used as a near-patient point-of-care sensor to detect sepsis, the same team [114] developed the first multi-biosensing platform consisting of five functionalized working electrodes to measure individual biomarkers, with only one chemokine, CXCL10/IP-10, among them. It should be noted that the detection of this chemokine has high importance since it allows identification of the source of the pathogen-triggered immune response. Indeed, viral infection seems to be reflected by an increase in this chemokine [103]. More recently, in this new configuration, CXCL8/IL-8 and CXCL10/IP-10 chemokines were determined, together with three cytokines (IL-6, IL-10 and TRAIL) and two well-established inflammatory biomarkers (PCT and CRP). The multi-assay device, named Direct Electrochemical Technique Targeting (DETecT), consisted of an array of seven electrodes for simultaneous detection of the biomarkers by EIS using a palm-sized, form-factor electronic reader. The sensor surface was modified with dithiobis (succinimidyl propionate) (DSP) to immobilize the specific capture antibodies. It detected all biomarkers in a small plasma sample volume (<40 μL) and the results correlated well with the reference standard method, Luminex, during clinical evaluation of 124 sepsis patient samples. Among other advantages, the method allows stratification of patient samples by measuring a panel of seven host immune response biomarkers on a single platform, providing results in less than 5 min.
Related to the multiplexed electrochemical device described above, fabrication of a wearable biosensor for noninvasive tracking of host immune response biomarkers in sweat was also reported by Jagannah et al. [41,103]. The developed design, named Sweatsenser, allowed the simultaneous and continuous detection of CXCL10/IP-10 and/or CXCL8/IL-8 chemokines together with inflammatory cytokines and C-reactive protein (CRP) for infection monitoring, with limits of detection of 1 pg/mL (IP-10 and TRAIL), and 0.2 ng/mL (CRP) with wide dynamic ranges. The platform (Figure 3) is based on an electrochemical biosensor strip functionalized with capture antibodies via a cross-linker on zinc oxide nanofilm. It allows measurements to be performed with real-time transduction and continuous reporting of targets in sweat. As can also be seen, the sensor strip is comprised of multiple fluid transport sites that have been carefully designed by means of an absorbent layer interfacing with the skin, to ensure effective capture of sweat, and sweat diffusion through the porous sieve.
Elevated expression of the CXCL7/NAP-2 chemokine has been shown in synovial fluid and serum of patients with rheumatoid arthritis (RA) during the first weeks of the disease but appearing at lower levels in RA with a longer duration. This difference in chemokine concentration is very useful to reflect local pathological changes in the clinical status of patients [115]. Two electrochemical immunosensors were developed by our group for application in the determination of CXCL7 in serum of healthy individuals and patients diagnosed with RA. In a first approach, an original method for immobilization of anti-CXCL7 capture antibodies was developed. It involved a copper (I) catalyzed azide–alkyne cycloaddition reaction (click chemistry) to prepare an integrated disposable immune-platform involving screen printed carbon electrodes modified with azide-modified-multi-walled carbon nanotubes which react with alkynylated IgG by the Cu(I)-catalyzed click reaction followed by the efficient conjugation with antibodies (Figure 4A). A sandwich-type immunoassay was then implemented for the electrochemical detection by differential pulse voltammetry (DPV) using alkaline phosphatase (AP) and 1-naphthyl phosphate (1-NPP) as the enzyme substrate. The immunosensor was successfully employed to determine CXCL7 in human sera with no need for sample treatment except dilution [88].
The second approach [89] (Figure 4B), was designed with the goal of achieving a better assessment of the disease state and treatment success by the simultaneous determination of the CXCL7 chemokine and matrix metalloproteinase-3 (MMP3), an enzyme involved in the degradation of various extracellular matrix components and in the destruction of cartilage and bone in RA [116]. In this configuration, an immunoplatform was prepared using carboxylated magnetic microbeads as substrates for the preparation of the immunoconjugates. The resulting methods, involving amperometric detection with the HRP/H2O2/hydroquinone (HQ) system, provided good results in the determination of biomarkers when applied to serum samples of RA patients and healthy individuals. When comparing the methodologies implemented for CXCL7 (Table 2), it can be seen that the one based on electrode modification by click chemistry provided the highest sensitivity, with a LOD value of 0.1 pg/mL vs. 0.8 ng/mL obtained with the magnetic assisted immunoplatform. This may be due to the different configurations prepared for the bioassays and also to the different enzymes, redox probes and electrochemical technique used for detection. However, both configurations were suitable for detecting chemokine overexpression with respect to normal levels of CXCL7 in human serum samples of healthy individuals, which are around 850 ng/mL [117].
CCL2 chemokine, also named monocyte chemotactic protein-1 (MCP-1), has relevant roles in pathogeneses of several diseases related to heart and circulatory system, and actively participates in progression of autoimmune diseases. It is considered an initiating factor and biomarker of atherosclerosis and is also involved in several events related to rheumatoid arthritis. Therefore, a there is great interest in the development of sensitive biosensors for detecting CCL2 in different types of clinical samples. Among the electrochemical biosensors proposed for this chemokine, a sensitive electrochemical design based on conductive wires orderly oriented was reported by Li et al. [105]. Such wires were prepared with gold nanoparticles joined to Au@Pt core–shell microspheres via a cysteamine (CA) crosslinker and grafting to the gold electrode to immobilize anti-CCL2 antibodies. After incubation in the presence of the chemokine using only 6 μL of sample, differential pulse voltammetry with Fe(CN)63−/4− as the redox probe, provided decreasing changes in the signal response related to the increase in antigen concentration, which reduces the peak current by hindering the spread of redox probe to the electrode surface. A high sensitivity with a calibration interval ranging between 0.09 and 360 pg/mL CCL2, and a LOD value of 0.03 pg/mL was achieved.
CXCL10/IP-10 is an interferon (IFN) inducible chemokine associated with poor prognosis in many types of cancer, showing greater affinity for the CXCR3 receptor. The CXCR3/IFN chemokine axis plays a significant role in cancer progression. To detect this chemokine, Bonham et al. [102] reported an electrochemical DNA biosensor which was prepared by immobilizing a DNA strand with a distal methylene blue redox reporter attached via SAM-AuE. The method involved the grafting of a 21-residue polypeptide binding element derived from CXCR3 receptor onto a peptide–nucleic-acid strand, and hybridization to the AuE-attached methylene blue-modified DNA strand via a terminal thiol group. The binding of CXCL10 to this recognition element reduces current from methylene blue related to the target concentration, which can be measured by square wave voltammetry (SWV). Figure 5 shows the fundamentals of this biosensor, that allows determination of the chemokine in a concentration range between 1 nM to 2 μM.
Regarding chemokine receptors, CCR4 has aroused considerable interest as a biomarker of prostate cancer. For its quantitation, an impedimetric immunosensor was prepared using an ITO electrode modified with an acid-substituted polypyrrole (p(Pyr-Pac) containing several carboxyl groups for covalent immobilization of the specific capture anti-CCR4 antibody [109]. As in other research works from Aydin´s group, the implementation of a label-free immunosensor achieves a high sensitivity, with a detection limit of 6.4 fg/mL and a wide linear range extending from 0.02 to 8 pg/mL, which is suitable for application of the developed method to analyze clinical samples.
4.2. Optical Techniques
Although electrochemical techniques comprise the majority for biosensor applications, other forms of transduction such as fluorimetry, have also been used. Figure 6 shows a schematic of the method developed by Verbarg et al. [93] for the detection of CXCL8 using a magnetic modulation biosensing system (MMB) which combines fluorescence measurements with the use of superparamagnetic beads on which capture anti-CXCL8 antibodies were immobilized. As can be seen, a sandwich-type immunoassay was implemented with biotinylated detection antibodies and streptavidin phyco-erythrin (SA-PE) fluorescent dye. In the laser system developed (Figure 6b), the fluorophores in the sample were excited and the emitted response was collected and detected by a photomultiplier tube (PMT). The resulting method allowed determination of CXCL8 through a 6-log dynamic range, being capable of detecting 0.08 ng/L of the chemokine in blood plasma. Important advantages of the MMB system are the ability to measure very low concentrations of analyte such as those from the calibration plot obtained in this method (up to 50 ng/L CXCL8) in a short time (after a 15-min incubation time) and the discrimination between the signal and the background noise due to unbound fluorescent molecules without requiring washing or separation steps.
Using a very different methodology but also involving fluorescence measurements, Zhang et al. [37] developed a microfluidic biosensor with dual function and based on rolling circle amplification (RCA) for on-line detection of CXCL8/IL-8. The analytical concept of on-line detection in this method derives from the configuration depicted in Figure 7. As can be seen, a microfluidic chip was constructed with two passages connected by the vertical channels, where the specific capture antibody was immobilized onto one channel, and the other was used for investigating cell culture. Affinity bioassays to determine CXCL8 were performed by a sandwich-type configuration involving antibodies and aptamers. As Figure 7A shows, once the target is sandwiched, the biotinylated RCA primer template complexes are linked to aptamers followed by isothermal amplification with Phi29 DNA polymerase. Finally, addition of DNA probes complementary to the amplified sequence provides multiple fluorescent probes to generate enhanced signals observed by a fluorescent microscope. This assay allowed quantitative determination of the chemokine to be performed within a linear range between 7.5 and 120 pg/mL CXCL8. Furthermore, the system was also applied to study the expression of CXCL8 tumor-derived and human umbilical vein endothelial cells (TDEC and HUVEC, respectively) under hypoxic conditions.
A surface-enhanced Raman scattering (SERS) immunoassay for the determination of CXCL8/IL-8 was also reported [90], which involves diatom biosilica with immobilized antibodies and integrated gold nanoparticles (AuNPs) using 5,5′-dithiobis(2-nitrobenzoic acid (DTNB) as a Raman reporter molecule. As Figure 8 shows, the immune reaction was performed in a sandwich-type configuration using silica-rich frustules from diatom species (Pseudostaurosira trainorii) where anti-CXCL8 capture antibodies were covalently bound. In the presence of the target chemokine, an intense SERS spectrum of DTNB bonded with the detection antibody was obtained, which was suitable for the development of an analytical method for quantitative determination by measuring the peak intensity of the average SERS response. A linear increase in these signals with the CXCL8 concentration in human blood plasma up to 30 ng/mL, and a limit of detection of 6.2 pg/mL were reported.
A sensitive real-time biosensing approach to quantify secretion and receptor binding of native chemokines in live cells was developed by White et al. [85]. CRISPR/Cas9 genome editing was used to tag the chemokine CXCL12 with the nanoluciferase fragment HiBiT and subsequent monitoring and determination by luminescence output. Binding of CXCL12-HiBiT to Alexa-Fluor488-tagged CXCR4 chemokine receptors was analyzed using BRET (bioluminescence resonance energy transfer) in a range between 1 fM and 1 nM. This live cell biomonitoring combines the sensitivity of nanoluciferase with CRISPR/Cas9 genome editing, to detect and quantify binding of low levels of native secreted proteins in real time.
Surface plasmon resonance (SPR) measurements can be used to study interactions between biomolecules immobilized onto metal surfaces and those present in liquid samples. Indeed, SPR biosensors have demonstrated their usefulness as diagnostic tools in a wide variety of biomedical applications [118]. As an example, an SPR biosensor was fabricated by Vega et al. [86] for real-time detection of CXCL12 chemokine in urine samples of RA patients. The developed configuration involved the use of lentiviral particles which bear the chemokine receptor CXCR4 in its native plasma membrane. In fact, CXCL12 chemokine, also named stromal cell-derived factor 1 (SDF-1), is one of the most relevant biomarkers for RA [119]. It is expressed by synovial endothelial cells binding to proteoglycans and participates in bone erosion and progression of the disease. The SPR method showed linear responses to CXCL12 concentration in the 5–40 nM range with good reproducibility and stability of the sensor responses for more than 150 measurements. Furthermore, its application to analyze urine samples demonstrated the high expression of this chemokine in RA patients with respect to healthy individuals, suggesting value of this biomarker for diagnosis of the autoimmune disease.
5. Advantages and Disadvantages of Electrochemical and Optical Biosensors
As discussed above, electrochemical and optical biosensors have been applied to the determination of chemokines. Although all of them are highly sensitive and selective, both have pros and cons. Regarding electrochemical biosensors, they show advantageous properties that, in general, can be summarized as providing wide linear dynamic ranges and low LODs, as well as the ability to be miniaturized and having lower experimental cost compared to optical biosensors. Moreover, they are not affected by interference of the light source and can be used for analyzing turbid samples. However, the electrode surface easily deteriorates, thus explaining why disposable electrodes are more frequently used, with the subsequent increase in the cost of analysis. In addition, and also in general, optical biosensors involving luminescence or absorbance measurements, require more complex instrumentation than that used in electrochemical transduction, and are more susceptible to physical damage and environmental interferences.
Furthermore, amperometric detection is easy to implement and use. The involvement of nanomaterials as electrode surface modifiers to improve the electrochemical responses [88] or as carrier tags for current amplification [104] allow for a high sensitivity. As has been pointed out, an important advantage of these biosensors is the possibility of carrying out the simultaneous detection of several biomarkers, as has been demonstrated with the bioplatforms magnetically assisted with MBs, for the immobilization of the bioreagents [89,100]. In addition, label-free detection involving the EIS technique allows the highly sensitive determination of CXCL8 [94,97] and the CCR4 receptor [108,109]. Regarding optical biosensors, the high sensitivity achieved with sensors using luminescent detection [85] and their suitability for detection in cells [37], as well as the wide dynamic range of calibrations [95] should be highlighted. Also noteworthy is the use of fluorometric detection in microfluidic systems [37] and the one-pot approach using Förster resonance energy transfer (FRET) detection [96]. In this area, the advantages of nanomaterials have been exploited to build SPR-based biosensors that allow real-time monitoring without the need for labels [86], or SERS immunoassay using Raman-reporter-labelled gold nanoparticles for signal enhancement [90].
6. Conclusions and Future Perspectives
In this review, the importance of the determination of different chemokines in clinical samples due to their involvement in diseases of high severity and incidence in the population has been highlighted. The selected examples have demonstrated the need for highly sensitive detection techniques to reach the low concentration levels in which these proteins are usually expressed, but also selective enough to be used directly in the analysis of complex samples without the need for previous treatment. In this context, electrochemical biosensors can offer a wide range of possibilities using different bioassay configurations, by detection with different techniques, and employing nanomaterials and signal amplification strategies.
Assuming that biosensors improve many of the characteristics of conventional methodologies for chemokine determination, it is necessary to pose new challenges that make more efficient detection in the early stages of the disease possible, when the probability of cure is higher, but also during its course by applying accurate methodologies for monitoring capable of detecting selected biomarkers from biological samples obtained by non-invasive collection.
As has been seen, some biosensors are validated by applying them to spiked samples instead of real clinical samples from patients, this being one of the many challenges that still lie ahead when evaluating the clinical utility of biosensors for chemokine detection. On the other hand, there are still only a few examples of multiple biosensing that enable the simultaneous detection of several chemokines and their receptors, to provide more information on the course of the disease. In this context, the use of label-free detection devices should be emphasized, which in the field of electrochemical biosensors has a predominant role in the impedance spectroscopy (EIS) technique.
Additionally, the dissemination of the utility of these devices must be carried out intensively so that the implemented methodologies reach users in clinical laboratories and patients, for point-of-care and self-application. This objective will be easier to achieve if the biosensors are prepared with the additional criteria of ease-of-use and low cost using simple protocols and cheap instrumentation, as well as working with miniaturized systems that allow the patient to monitor parameters of medical interest in spaces that do not necessarily qualify as laboratories or hospitals.
Author Contributions
Writing—review and editing, funding acquisition E.S.-T., L.A., A.G.-C., P.Y.-S. and J.M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Ministerio de Ciencia, Innovación y Universidades, research project RTI2018-096135-B-I00 and Comunidad de Madrid TRANSNANOAVANSENS-CM Program, Grant S2018/NMT-4349.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The financial support of RTI2018-096135-B-I00 (Spanish Ministerio de Ciencia, Innovacion y Universidades), and the TRANSNANOAVANSENS-CM Program from the Comunidad de Madrid (Grant S2018/NMT-4349) are gratefully acknowledged.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the writing of the manuscript.
References
- Zlotnik, A.; Yoshie, O. The chemokine superfamily revisited. Immunity 2012, 36, 705–716. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.E.; Nibbs, R.J.B. A guide to chemokines and their receptors. FEBS 2018, 285, 2944–2971. [Google Scholar] [CrossRef]
- Bacon, K.B.; Harrison, J.K. Chemokines and their receptors in neurobiology: Perspectives in physiology and homeostasis. J. Neuroimmun. 2000, 104, 92–97. [Google Scholar] [CrossRef]
- Charo, I.F.; Ransohoff, R.M. The many roles of chemokines and chemokine receptors in inflammation. N. Eng. J. Med. 2006, 354, 610–621. [Google Scholar] [CrossRef]
- Walz, D.A.; Wu, V.Y.; de Lamo, R.; Dene, H.; McCoy, L.E. Primary structure of human platelet factor 4. Thrombosis Res. 1977, 11, 893–898. [Google Scholar] [CrossRef]
- Yoshimura, T.; Matsushima, K.; Tanaka, S.; Robinson, E.A.; Appella, E.; Oppenheim, J.J.; Leonard, E.J. Purification of a human monocyte-derived neutrophil chemotactic factor that has peptide sequence similarity to other host defense cytokines. Proc. Natl. Acad. Sci. USA 1987, 84, 9233–9237. [Google Scholar] [CrossRef] [Green Version]
- Cocchi, F.; DeVico, A.L.; Garzino-Demo, A.; Arya, S.K.; Gallo, R.C.; Lusso, P. Identification of RANTES, MIP-1 alpha, and MIP-1 beta as the major HIV-suppressive factors produced by CD8+T cells. Science 1995, 270, 1811–1815. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; Broder, C.C.; Kennedy, P.E.; Berger, E.A. HIV-1 entry cofactor: Functional cDNA cloning of a seven-transmembrane, G protein-coupled receptor. Science 1996, 272, 872–877. [Google Scholar] [CrossRef]
- Callewaare, C.; Banisadr, G.; Rostène, W.; Parsadaniantz, S.M. Chemokines and chemokine receptors in the brain: Implication in neuroendocrine regulation. J. Mol. Edocrinol. 2007, 38, 355–363. [Google Scholar] [CrossRef]
- Moser, B.; Wolf, M.; Walz, A.; Loetscher, P. Chemokines: Multiple levels of leukocyte control. Trends Immunol. 2004, 25, 75–84. [Google Scholar] [CrossRef]
- Kimura, Y.N.; Watari, K.; Fotovati, A.; Hosoi, F.; Yasumoto, K.; Izumi, H.; Kohno, K.; Umezawa, K.; Iguchi, H.; Shirouzu, K.; et al. Inflammatory stimuli from macrophages and cancer cells synergistically promote tumor growth and angiogenesis. Cancer Sci. 2007, 98, 2009–2018. [Google Scholar] [CrossRef]
- Rotondi, M.; Chiovato, L.; Romagnani, S.; Serio, M.; Romagnani, P. Role of chemokines in endocrine autoimmune diseases. Endocrine Rev. 2007, 28, 492–520. [Google Scholar] [CrossRef] [Green Version]
- Cameron, M.J.; Kelvin, D.J. Cytokines, chemokines and their receptors. In Madame Curie Bioscience Dataabase [Internet]; Landes Bioscience: Austin, TX, USA, 2000–2013. Available online: https://www.ncbi.nlm.nih.gov/books/NBK6294/ (accessed on 27 June 2022).
- Unver, N.; Esendagli, G.; Yilmaz, G.; Guc, D. CXCL7-induced macrophage infiltration in lung tumor is independent of CXCR2 expression: CXCL7-induced macrophage chemotaxis in LLC tumors. Cytokine 2015, 75, 330–337. [Google Scholar] [CrossRef]
- Jin, T.; Xu, X.; Hereld, D. Chemotaxis, chemokine receptors and human disease. Cytokine 2008, 44, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.-D.; Song, X.-Y.; Yang, P.-F.; Ai, Q.-D.; Wang, Y.-Y.; Feng, X.-Y.; He, X.; Chen, N.-H. Progress in pharmacological research of chemokine like factor 1 (CKLF1). Cytokine 2018, 102, 41–50. [Google Scholar] [CrossRef]
- Proudfoot, A.E.I.; Johnson, Z.; Bonvin, P.; Handel, T.M. Glycosaminoglycan interactions with chemokines add complexity to a complex system. Pharmaceuticals 2017, 10, 70. [Google Scholar] [CrossRef] [Green Version]
- Stone, M.J. Regulation of chemokine-receptor interactions and functions. Int. J. Mol. Sci. 2017, 18, 2415. [Google Scholar] [CrossRef] [Green Version]
- Lindley, I.J.D. 8. Interleukin-8. In Cytokines Handbook of Immunopharmacology; Academic Press: Cambridge, MA, USA, 1998; pp. 125–140. [Google Scholar] [CrossRef]
- Zlotnik, A.; Yoshie, O.; Nomiyama, H. The chemokine and chemokine receptor superfamilies and their molecular evolution. Genome Biol. 2006, 7, 243. [Google Scholar] [CrossRef]
- Turner, M.D.; Nedjai, B.; Hurst, T.; Pennington, D.J. Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochim. Biophys. Acta-Mol. Cell Res. 2014, 1843, 2563–2582. [Google Scholar] [CrossRef] [Green Version]
- Panda, S.; Padhiary, S.K.; Routray, S. Chemokines accentuating protumoral activities in oral cancer microenvironment possess an imperious stratagem for therapeutic resolutions. Oral Oncol. 2016, 60, 8–17. [Google Scholar] [CrossRef]
- Gerszten, R.E.; Mach, F.; Sauty, A.; Rosenzweig, A.; Luster, A.D. Chemokines, leukocytes, and atherosclerosis. J. Lab. Clin. Med. 2000, 136, 87–92. [Google Scholar] [CrossRef]
- Rot, A.; von Andrian, U.H. Chemokines in innate and adaptive host defense: Basic chemokinese grammar for immune cells. Annu. Rev. Immunol. 2004, 22, 891–928. [Google Scholar] [CrossRef]
- Butera, D.; Marukian, S.; Iwamaye, A.E.; Hembrador, E.; Chambers, T.J.; di Bisceglie, A.M.; Charles, E.D.; Talal, A.H.; Jacobson, I.M.; Rice, C.M.; et al. Plasma chemokine levels correlate with the outcome of antiviral therapy in patients with hepatitis C. Blood 2005, 106, 1175–1182. [Google Scholar] [CrossRef] [Green Version]
- Ruffini, P.A.; Morandi, P.; Cabioglu, N.; Altundag, K.; Cristofanilli, M. Manipulating the chemokine-chemokine receptor network to treat cancer. Cancer 2007, 109, 2392–2404. [Google Scholar] [CrossRef]
- Saruhan-Direskeneli, G.; Yentür, S.P.; Akman-Demir, G.; Isik, N.; Serdaroğlu, P. Cytokines and chemokines in neuro-Behçet’s disease compared to multiple sclerosis and other neurological diseases. J. Neuroimmunol. 2003, 145, 127–134. [Google Scholar] [CrossRef]
- Godessart, N.; Kunkel, S.L. Chemokines in autoimmune disease. Curr. Opin. Immunol. 2001, 13, 670–675. [Google Scholar] [CrossRef]
- Collins, P.J.; McCully, M.L.; Martínez-Muñoz, L.; Santiago, C.; Wheeldon, J.; Caucheteux, S.; Thelen, S.; Cecchinato, V.; Laufer, J.M.; Purvanov, V.; et al. Epithelial chemokine CXCL14 synergizes with CXCL12 via allosteric modulation of CXCR4. Faseb J. 2017, 31, 3084–3097. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.T.; Wong, Y.K.; Hsiao, H.Y.; Wang, Y.W.; Chan, M.Y.; Chang, K.W. Evaluation of saliva and plasma cytokine biomarkers in patients with oral squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2018, 47, 699–707. [Google Scholar] [CrossRef]
- Mrugacz, M.; Zelazowska, B.; Bakunowicz-Lazarczyk, A.; Kaczmarski, M.; Wysocka, J. Elevated tear fluid levels of MIP-1alpha in patients with cystic fibrosis. J. Interferon Cytokine Res. 2007, 27, 491–495. [Google Scholar] [CrossRef]
- Gornowicz, A.; Bielawska, A.; Bielawski, K.; Grabowska, S.Z.; Wójcicka, A.; Zalewska, M.; Maciorkowska, E. Pro-inflammatory cytokines in saliva of adolescents with dental caries disease. Ann. Agric. Environ. Med. 2012, 19, 711–716. [Google Scholar]
- Ujhelyi, B.; Gogolak, P.; Erdei, A.; Nagy, V.; Balazs, E.; Rajnavolgyi, E.; Berta, A.; Nagy, E.V. Graves’ Orbitopathy results in profound changes in tear composition: A study of plasminogen activator inhibitor-1 and seven cytokines. Thyroid 2012, 22, 407–414. [Google Scholar] [CrossRef]
- Thorman, R.; Lundahl, J.; Yucel-Lindberg, T.; Hylander, B. Inflammatory cytokines in saliva: Early signs of metabolic disorders in chronic kidney disease. A controlled cross sectional study. Oral Surg. Oral Med. Oral Pathol. Oral Radio 2010, 110, 597–604. [Google Scholar] [CrossRef]
- Kishazi, E.; Dor, M.; Eperon, S.; Oberic, A.; Turck, N.; Hamedani, M. Differential profiling of lacrimal cytokines in patients suffering from thyroid-associated orbitopathy. Sci. Rep. 2018, 8, 10792. [Google Scholar] [CrossRef] [Green Version]
- Robison, H.M.; Chapman, C.A.; Zhou, H.; Erskine, C.L.; Theel, E.; Peikert, T.; Arlehamn, C.S.L.; Sette, A.; Bushell, C.; Welge, M.; et al. Risk assessment of latent tuberculosis infection through a multiplexed cytokine biosensor assay and machine learning feature selection. Sci. Rep. 2021, 11, 20544. [Google Scholar] [CrossRef]
- He, W.Z.Z.; Yi, L.; Mao, S.; Li, H.; Lin, J.-M. A dual-functional microfluidic chip for on-line detection of interleukin-8 based on rolling circle amplification. Biosens. Bioelectron. 2018, 102, 652–660. [Google Scholar] [CrossRef]
- Zhou, W.; Mahshid, S.S.; Wang, W.; Vallée-Bélisle, A.; Zandstra, P.W.; Sargent, E.H.; Kelley, S.O. Steric hindrance assay for secreted factors in stem cell culture. ACS Sens. 2017, 2, 495–500. [Google Scholar] [CrossRef]
- Kramer, J.M.; Klimatcheva, E.; Rothstein, T.L. CXCL13 is elevated in Sjögren’s syndrome in mice and humans and is implicated in disease pathogenesis. J. Leukoc. Biol. 2013, 94, 1079–1089. [Google Scholar] [CrossRef] [Green Version]
- Alosaimi, B.; Hamed, M.E.; Naeem, A.; Alsharef, A.A.; al Qahtani, S.Y.; al Dosari, K.M.; Alamri, A.A.; Al-Eisa, K.; Khojah, T.; Assiri, A.M.; et al. MERS-CoV infection is associated with downregulation of genes encoding Th1 and Th2 cytokines/chemokines and elevated inflammatory innate immune response in the lower respiratory tract. Cytokine 2020, 126, 154895. [Google Scholar] [CrossRef]
- Jagannath, B.; Pali, M.; Lin, K.-C.; Sankhala, D.; Naraghi, P.; Muthukumar, S.; Prasad, S. Novel approach to track the lifecycle of inflammation from chemokine expression to inflammatory proteins in sweat using electrochemical biosensor. Adv. Mater. Technol. 2022, 2101356. [Google Scholar] [CrossRef]
- Hernández-Molina, G.; Michel-Peregrina, M.; Hernández-Ramírez, D.F.; Sánchez-Guerrero, J.; Llorente, L. Chemokine saliva levels in patients with primary Sjögren’s syndrome, associated Sjögren’s syndrome, pre-clinical Sjögren’s syndrome and systemic autoimmune diseases. Rheumatology 2011, 50, 1288–1292. [Google Scholar] [CrossRef] [Green Version]
- Jekarl, D.W.; Kim, J.Y.; Ha, J.H.; Lee, S.; Yoo, J.; Kim, M.; Kim, Y. Diagnosis and prognosis of sepsis based on use of cytokines, chemokines, and growth factors. Dis. Markers 2019, 1089107. [Google Scholar] [CrossRef]
- Poeta, V.M.; Massara, M.; Capucetti, A.; Bonecchi, R. Chemokines and chemokine receptors: New targets for cancer immunotherapy. Front. Immunol. 2019, 10, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karin, N. Chemokines and cancer: New immune checkpoints for cancer therapy. Curr. Op. Immunol. 2018, 51, 140–145. [Google Scholar] [CrossRef]
- Korbecki, J.; Kojder, K.; Simińska, D.; Bohatyrewicz, R.; Gutowska, I.; Chlubek, D.; Baranowska-Bosiacka, I. CC chemokines in a tumor: A review of pro-cancer and anti-cancer properties of the ligands of receptors CCR1, CCR2, CCR3, and CCR4. Int. J. Mol. Sci. 2020, 21, 8412. [Google Scholar] [CrossRef]
- Korbecki, J.; Grochans, S.; Gutowska, I.; Barczak, K.; Baranowska-Bosiacka, I. CC chemokines in a tumor: A review of pro-cancer and anti-cancer properties of receptors CCR5, CCR6, CCR7, CCR8, CCR9, and CCR10 ligands. Int. J. Mol. Sci. 2020, 21, 7619. [Google Scholar] [CrossRef]
- Waugh, D.J.J.; Wilson, C.; Seaton, A.; Maxwell, P.J. Multi-faceted roles for CXC-chemokines in prostate cancer progression. Front. Biosci. 2008, 13, 4595–4604. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Riese, D.J., II; Shen, J. The role of the CXCL12/CXCR4/CXCR7 chemokine axis in cancer. Front. Pharmacol. 2020, 11, 574667. [Google Scholar] [CrossRef]
- Singh, J.K.; Simoes, B.M.; Howell, S.J.; Farnie, G.; Clarke, R.B. Recent advances reveal IL-8 signaling as a potential key to targeting breast cancer stem cells. Breast Cancer Res. 2013, 15, 210. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Gomes-Giacoia, E.; Dai, Y.; Lawton, A.; Miyake, M.; Furuya, H.; Goodison, S.; Rosser, C.J. Validation and clinicopathologic associations of a urine-based bladder cancer biomarker signature. Diagn. Pathol. 2014, 9, 200. [Google Scholar] [CrossRef] [Green Version]
- Margel, D.; Pesvner-Fischer, M.; Baniel, J.; Yossepowitch, O.; Cohen, I.R. Stress proteins and cytokines are urinary biomarkers for diagnosis and staging of bladder cancer. Eur. Urol. 2011, 59, 113–119. [Google Scholar] [CrossRef]
- Samarendra, H.; Jones, K.; Petrinic, T.; Silva, M.A.; Reddy, S.; Soonawalla, Z.; Gordon-Weeks, A. A meta-analysis of CXCL12 expression for cancer prognosis. Br. J. Cancer 2017, 117, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Domanska, U.M.; Kruizinga, R.C.; Nagengast, W.B.; Timmer-Bosscha, H.; Huls, G.; de Vries, E.G.E.; Walenkamp, A.M.E. A review on CXCR4/CXCL12 axis in oncology: No place to hide. Eur. J. Cancer 2013, 49, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Khare, T.; Bissonnette, M.; Khare, S. CXCL12-CXCR4/CXCR7 axis in colorectal cancer: Therapeutic target in preclinical and clinical studies. Int. J. Mol. Sci. 2021, 22, 7371. [Google Scholar] [CrossRef]
- Ieranò, C.; D’Alterio, C.; Giarra, S.; Napolitano, M.; Rea, G.; Portella, L.; Santagata, A.; Trotta, A.M.; Barbieri, A.; Campani, V.; et al. CXCL12 loaded-dermal filler captures CXCR4 expressing melanoma circulating tumor cells. Cell Death Dis. 2019, 10, 562. [Google Scholar] [CrossRef] [PubMed]
- Mortezaee, K. CXCL12/CXCR4 axis in the microenvironment of solid tumors: A critical mediator of metastasis. Life Sci. 2020, 249, 117534. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xi, L.; Gooding, W.; Godfrey, T.E.; Ferrisa, R.L. Chemokine receptors 6 and 7 identify a metastatic expression pattern in squamous cell carcinoma of the head and neck. Adv. Otorhinolaryngol. 2005, 62, 121–133. [Google Scholar] [PubMed]
- Chen, K.; Bao, Z.; Tang, P.; Gong, W.; Yoshimura, T.; Wang, J.M. Chemokines in homeostasis and diseases. Cell. Mol. Immunol. 2018, 15, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, T.; Shetty, V.; Yamaguchi, M. Salivary cytokine panel indicative of non-small cell lung cancer. J. Int. Med. Res. 2018, 46, 3570–3582. [Google Scholar] [CrossRef] [PubMed]
- Katsura, M.; Shoji, F.; Okamoto, T.; Shimamatsu, S.; Hirai, F.; Toyokawa, G.; Morodomi, Y.; Tagawa, T.; Oda, Y.; Maehara, Y. Correlation between CXCR4/ CXCR7/ CXCL12 chemokine axis expression and prognosis in lymph-node-positive lung cancer patients. Cancer Sci. 2018, 109, 154–165. [Google Scholar] [CrossRef] [Green Version]
- Rinaldi, C.; Corrigan, D.K.; Dennany, L.; Jarrett, R.F.; Lake, A.; Baker, M.J. Development of an electrochemical CCL17/TARC biosensor toward rapid triage and monitoring of classic Hodgkin lymphoma. ACS Sens. 2021, 6, 3262–3272. [Google Scholar] [CrossRef] [PubMed]
- Elemam, N.M.; Hannawi, S.; Maghazachi, A.A. Role of chemokines and chemokine receptors in rheumatoid arthritis. Immunotargets Ther. 2020, 9, 43–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, L.; Adlard, N.; Biehl, M.; Juarez, M.; Smallie, T.; Snow, M.; Buckley, C.D.; Raza, K.; Filer, A.; Scheel-Toellner, D. Expression of chemokines CXCL4 and CXCL7 by synovial macrophages defines an early stage of rheumatoid arthritis. Ann. Rheum. Dis. 2016, 75, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Moadab, F.; Khorramdelazad, H.; Abbasifard, M. Role of CCL2/CCR2 axis in the immunopathogenesis of rheumatoid arthritis: Latest evidence and therapeutic approaches. Life Sci. 2021, 269, 119034. [Google Scholar] [CrossRef] [PubMed]
- Liou, L.-B.; Fang, Y.-F.; Tan, C.F.; Lai, J.-H.; Jang, S.-s.; Tsai, P.-H.; Yeh, T.-c. A new laboratory surrogate (Monocyte Chemotactic Protein-1) for Disease Activity Score28: A favourable indicator for remission in rheumatoid arthritis. Sci. Rep. 2020, 10, 8238. [Google Scholar] [CrossRef] [PubMed]
- Blaschke, S.; Koziolek, M.; Schwarz, A.; Benohr, P.; Middel, P.; Schwarz, G.; Hummel, K.M.; Muller, G.A. Proinflammatory role of fractalkine (CX3CL1) in rheumatoid arthritis. J. Rheumatol. 2003, 30, 1918–1927. [Google Scholar]
- Demirdöğen, B.C. A literature review of biosensors for multiple sclerosis: Towards personalized medicine and point-of-care testing. Mult. Scler. Relat. Disord. 2021, 48, 102675. [Google Scholar] [CrossRef]
- Comabella, M.; Montalban, X. Body fluid biomarkers in multiple sclerosis. Lancet Neurol. 2014, 13, 113–126. [Google Scholar] [CrossRef]
- Cui, L.-Y.; Chu, S.-F.; Chen, N.-H. The role of chemokines and chemokine receptors in multiple sclerosis. Int. Immunopharmacol. 2020, 83, 106314. [Google Scholar] [CrossRef]
- Mori, F.; Nisticò, R.; Nicoletti, C.G.; Zagaglia, S.; Mandolesi, G.; Piccinin, S.; Martino, G.; Finardi, A.; Rossini, P.M.; Marfia, G.A.; et al. RANTES correlates with inflammatory activity and synaptic excitability in multiple sclerosis. Mult. Sclerosis J. 2016, 22, 1405–1412. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Khademi, M.; Fugger, L.; Lindhe, Ö.; Novakova, L.; Axelsson, M.; Malmeström, C.; Constantinescu, C.; Lyckee, J.; Piehl, F.; et al. Inflammation-related plasma and CSF biomarkers for multiple sclerosis. Proc. Natl. Acad. Sci. USA 2020, 117, 12952–12960. Available online: www.pnas.org/cgi/doi/10.1073/pnas.1912839117 (accessed on 27 June 2022). [CrossRef]
- Weetman, A.P.; Bennett, G.L.; Wong, W.L. Thyroid follicular cells produce interleukin-8. J. Clin. Endocrinol. Metab. 2002, 75, 328–330. [Google Scholar] [CrossRef]
- Kasai, K.; Banba, N.; Motohashi, S.; Hattor, Y.; Manaka, K.; Shimoda, S.I. Expression of monocyte chemoattractant protein-1 mRNA and protein in cultured human thyrocytes. FEBS Lett. 1996, 394, 137–140. [Google Scholar] [CrossRef] [Green Version]
- Aust, G.; Steinert, M.; Boltze, C.; Kieseling, A.; Simchen, C. GRO-a in normal and pathological thyroid tissues and its regulation in thyroid-derived cells. J. Endocrinol. 2001, 170, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, S.M.; Fallahi, P.; Ruffilli, I.; Elia, G.; Ragusa, F.; Benvenga, S.; Antonelli, A. The association of other autoimmune diseases in patients with Graves’ disease (with or without ophthalmopathy): Review of the literature and report of a large series. Autoimmun. Rev. 2019, 18, 287–292. [Google Scholar] [CrossRef]
- Garcia-Lopez, M.A.; Sancho, D.; Sanchez-Madrid, F.; Marazuela, M. Thyrocytes from autoimmune thyroid disorders produce the chemokines IP-10 and Mig and attract CXCR3 lymphocytes. J. Clin. Endocrinol. Metab. 2001, 86, 5008–5016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romagnani, P.; Rotondi, M.; Lazzeri, E.; Lasagni, L.; Francalanci, M.; Buonamano, A.; Milani, S.; Vitti, P.; Chiovato, L.; Tonacchera, M.; et al. Expression of IP-10/CXCL10 and MIG/CXCL9 in the thyroid and increased levels of IP-10/CXCL10 in the serum of patients with recent-onset Graves’ disease. Am. J. Pathol. 2002, 161, 195–206. [Google Scholar] [CrossRef]
- Ferrer-Francesch, X.; Caro, P.; Alcalde, L.; Armengol, M.P.; Ashhab, Y.; Lucas-Martin, A.; Martinez-Caceres, E.M.; Pujol-Borrell, M.J.R. Onetube-PCR technique for CCL2, CCL3, CCL4 and CCL5 applied to fine needle aspiration biopsies shows different profiles in autoimmune and non-autoimmune thyroid disorders. J. Endocrinol. Investig. 2006, 29, 342–349. [Google Scholar] [CrossRef]
- Armengol, M.P.; Juan, M.; Lucas-Martin, A.; Fernandez-Figueras, M.T.; Jaraquemada, D.; Gallart, T.; Pujol-Borrell, R. Thyroid autoimmune disease: Demonstration of thyroid antigenspecifi c B cells and recombination-activating gene expression in chemokine-containing active intrathyroidal germinal centers. Am. J. Pathol. 2001, 159, 861–873. [Google Scholar] [CrossRef]
- Kemp, E.H.; Metcalfe, R.A.; Smith, K.A.; Woodroofe, M.N.; Watson, P.F.; Weetman, A.P. Detection and localization of chemokine gene expression in autoimmune thyroid disease. Clin. Endocrinol. 2003, 59, 207–213. [Google Scholar] [CrossRef]
- Masih, M.; Agarwal, S.; Kaur, R.; Gautam, P.K. Role of chemokines in breast cancer. Cytokine 2022, 155, 155909. [Google Scholar] [CrossRef]
- Chen, X.; Jin, R.C.R.; Huang, Z. The role of CXCL chemokine family in the development and progression of gastric cancer. Int. J. Clin. Exp. Pathol. 2020, 13, 484–492. [Google Scholar] [PubMed]
- McDonough, A.A.; Veiras, L.C.; Minas, J.N.; Ralph, D.L. Considerations when quantitating protein abundance by immunoblot. Am. J. Physiol. Cell. Physiol. 2015, 308, C426–C433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, C.W.; Kilpatrick, L.E.; Pfleger, K.D.G.; Hill, S.J. A nanoluciferase biosensor to investigate endogenous chemokine secretion and receptor binding. iScience 2021, 24, 102011. [Google Scholar] [CrossRef]
- Vega, B.; Calle, A.; Sanchez, A.; Lechuga, L.M.; Ortiz, A.M.; Armelles, G.; Rodríguez-Frade, J.M.; Mellado, M. Real-time detection of the chemokine CXCL12 in urine samples by surface plasmon resonance. Talanta 2013, 109, 209–215. [Google Scholar] [CrossRef]
- Chung, S.; Chandra, P.; Koo, J.P.; Shim, Y.-B. Development of a bifunctional nanobiosensor for screening and detection of chemokine ligand in colorectal cancer cell line. Biosens. Bioelectron. 2018, 100, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, S.; Cadano, D.; Agüí, L.; Barderas, R.; Campuzano, S.; Yañez-Sedeño, P.; Pingarrón, J.M. Click chemistry-assisted antibodies immobilization for immunosensing of CXCL7 chemokine in serum. J. Electroanal. Chem. 2019, 837, 246–253. [Google Scholar] [CrossRef]
- Guerrero, S.; Sánchez-Tirado, E.; Agüí, L.; González-Cortés, A.; Yáñez-Sedeño, P.; Pingarrón, J.M. Simultaneous determination of CXCL7 chemokine and MMP3 metallopro-teinase as biomarkers for rheumatoid arthritis. Talanta 2021, 234, 122705. [Google Scholar] [CrossRef]
- Kamińska, A.; Sprynskyy, M.; Winkler, K.; Szymborski, T. Ultrasensitive SERS immunoassay based on diatom biosilica for detection of interleukins in blood plasma. Anal. Bioanal. Chem. 2017, 409, 6337–6347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydın, E.B.; Sezgintürk, M.K. An impedimetric immunosensor for highly sensitive detection of IL-8 in human serum and saliva samples: A new surface modification method by 6-phosphonohexanoic acid for biosensing applications. Anal. Biochem. 2018, 554, 44–52. [Google Scholar] [CrossRef]
- Aydın, M.; Aydın, E.B.; Sezgintürk, M.K. A highly selective electrochemical immunosensor based on conductive carbon black and star PGMA polymer composite material for IL-8 biomarker detection in human serum and saliva. Biosens. Bioelectron. 2018, 117, 720–728. [Google Scholar] [CrossRef]
- Verbarg, J.; Hadass, O.; Olivo, P.D.; Danielli, A. High sensitivity detection of a protein biomarker interleukin-8 utilizing a magnetic modulation biosensing system. Sens. Actuators B 2017, 241, 614–618. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, R.; Xu, L.; Ning, Y.; Xie, S.; Zhang, G.J. Silicon nanowire biosensor for highly sensitive detection of oral squamous cell carcinoma biomarkers in saliva. Anal. Sci. 2015, 31, 73–78. [Google Scholar] [CrossRef] [Green Version]
- Margulis, M.; Cohen, M.; Burg, S.; Avivi-Mintz, S.; Danielli, A. Optical modulation biosensing system for rapid detection of biological targets at low concentrations. Biomed. Opt. Express 2021, 12, 5338–5350. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Jo, E.-J.; Hong, D.; Oh, H.-K.; Lee, K.J.; Shin, Y.-B.; Kim, M.-G. One-pot, solid-phase immunosensing platform consisting of a nanometer-thick Au/TiO2 photocatalytic film and Cy5/capture antibody/gold nanorod conjugates. ACS Appl. Nano Mater. 2021, 4, 5454–5460. [Google Scholar] [CrossRef]
- Aydın, E.B.; Sezgintürk, M.K. Fabrication of electrochemical immunosensor for detection of interleukin 8 biomarker via layer-by-layer self-assembly process on cost-effective fluorine tin oxide electrode. Electroanalysis 2021, 33, 1596–1605. [Google Scholar] [CrossRef]
- Sharma, R.; Deacon, S.E.; Nowak, D.; George, S.E.; Szymonik, M.P.; Tang, A.A.S.; Tomlinson, D.C.; Davies, A.G.; McPherson, M.J.; Wälti, C. Label-free electrochemical impedance biosensor to detect human interleukin-8 in serum with sub-pg/ml sensitivity. Biosens. Bioelectron. 2016, 80, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan-Nixon, H.A.G.; Singh, N.; Cass, A.E.G. A sensitive impedimetric immuno-sensor for the detection of Interleukin-8 in nasal epithelial lining fluid of asthma patients. Biosens. Bioelectron. X 2022, 10, 100118. [Google Scholar] [CrossRef]
- Torrente-Rodríguez, R.M.; Campuzano, S.; Montiel, V.R.; Gamella, M.; Pingarrón, J.M. Electrochemical bioplatforms for the simultaneous determination of interleukin (IL)-8 mRNA and IL-8 proteinoralcancerbiomarkersinraw saliva. Biosens. Bioelectron. 2016, 77, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Tanak, A.S.; Sardesai, A.; Muthukumar, S.; Krishnan, S.; Striegel, D.A.; Schully, K.L.; Clark, D.V.; Prasad, S. Multiplexed host immune response biosensor for rapid sepsis stratification and endotyping at point-of-care. Biosens. Bioelectron. X 2022, 10, 100144. [Google Scholar] [CrossRef]
- Bonham, A.J.; Paden, N.G.; Ricci, F.; Plaxco, K.W. Detection of IP-10 protein marker in undiluted blood serum via an electrochemical E-DNA scaffold sensor. Analyst 2013, 138, 5580–5583. [Google Scholar] [CrossRef] [Green Version]
- Jagannath, B.; Lin, K.; Pali, M.; Sankhala, D.; Muthukumar, S.; Prasad, S. Temporal profiling of cytokines in passively expressed sweat for detection of infection using wearable device Bioeng. Transl. Med. 2021, 6, e10220. [Google Scholar] [CrossRef]
- Mao, W.; He, J.; Tang, Z.; Zhang, C.; Chen, J.; Li, J.; Yu, C. A sensitive sandwich-type immunosensor for the detection of MCP-1 based on a rGO-TEPA-Thi-Au nanocomposite and novel RuPdPt trimetallic nanoalloy particles. Biosens. Bioelectron. 2019, 131, 67–73. [Google Scholar] [CrossRef]
- Li, Y.; He, J.; Xia, C.; Gao, L.; Yu, C. Ultrasensitive electrochemical immunosensor based on orderly oriented conductive wires for the detection of human monocyte chemotactic protein-1 in serum. Biosens. Bioelectron. 2015, 70, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Valera, E.; Shia, W.W.; Bailey, R.C. Development and validation of an immunosensor for monocyte chemotactic protein 1 using a silicon photonic microring resonator biosensing platform. Clin. Biochem. 2016, 49, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Z.; Liu, X.; Zhang, C.; Tang, Z.; Chen, J.; Yu, C. Electrochemical immunosensor for monocyte chemoattractant protein-1 detection based on Pt nanoparticles functionalized single-walled carbon nanohorns. Int. J. Electrochem. Sci. 2018, 13, 3923–3934. [Google Scholar] [CrossRef]
- Aydın, E.B.; Aydın, M.; Sezgintürk, M.K. Electrochemical immunosensor for detection of CCR4 cancer biomarker in human serum: An alternative strategy for modification of disposable ITO electrode. Mol. Biosci. 2021, 21, 2000267. [Google Scholar] [CrossRef]
- Aydın, E.B.; Aydın, M.; Sezgintürk, M.K. Fabrication of electrochemical immunosensor based on acid-substituted poly(pyrrole) polymer modified disposable ITO electrode for sensitive detection of CCR4 cancer biomarker in human serum. Talanta 2021, 222, 121487. [Google Scholar] [CrossRef]
- Hu, B.; Fan, H.; Lv, X.; Chen, S.; Shao, Z. Prognostic significance of CXCL5 expression in cancer patients: A meta-analysis. Cancer Cell Int. 2018, 18, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinchia, J.; Echeverri, D.; Cruz-Pacheco, A.F.; Maldonado, M.E.; Orozco, J. Electrochemical biosensors for determination of colorectal tumor biomarkers. Micromachines 2020, 11, 411. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Jarrett, R.F.; Hjalgrim, H.; Proietti, C.; Chang, E.T.; Smedby, K.E.; Yu, K.J.; Lake, A.; Troy, S.; McAulay, K.A.; et al. Evaluation of the antibody response to the EBV proteome in EBV-associated classical Hodgkin lymphoma. Int. J. Cancer 2020, 147, 608–618. [Google Scholar] [CrossRef]
- Nedeva, C.; Menassa, J.; Puthalakath, H. Sepsis: Inflammation is a necessary evil. Front. Cell Dev. Biol. 2019, 7, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanak, A.S.; Muthukumar, S.; Krishnan, S.; Schully, K.L.; Clark, D.V.; Prasad, S. Multiplexed cytokine detection using electrochemical point-of-care sensing device towards rapid sepsis endotyping. Biosens. Bioelectron. 2021, 171, 112726. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Aletaha, D.; Koeller, M.; Weisman, M.; Emery, P. New therapies for the treatment of rheumatoid arthritis. Lancet 2007, 370, 1861–1874. [Google Scholar] [CrossRef]
- Ribbens, C.; Porras, M.M.y.; Franchimont, N.; Kaiser, M.-J.; Jaspar, J.-M.; Damas, P.; Houssiau, F.A.; Malaise, M.G. Increased matrix metalloproteinase-3 serum levels in rheumatic diseases: Relationship with synovitis and steroid treatment. Ann. Rheum. Dis. 2002, 61, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Du, Q.; Li, E.; Liu, Y.; Xie, W.; Huang, C.; Song, J.; Zhang, W.; Zheng, Y.; Wang, H.; Wang, Q. CTAPIII/CXCL7: A novel biomarker for early diagnosis of lung cancer. Cancer Med. 2018, 7, 283–535. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.H.; Park, J.; Kang, S.; Kim, M. Surface plasmon resonance: A versatile technique for biosensor applications. Sensors 2015, 15, 10481–10510. [Google Scholar] [CrossRef] [Green Version]
- Szekanecz, Z.; Vegvari, A.; Szabo, Z.; Koch, A.E. Chemokines and chemokine receptors in arthritis. Front. Biosci. 2010, 2, 153–167. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
(A) Cytokines and chemokines. (B) Structures of the chemokine family. Drawn from a schematic of [16].
Figure 1.
(A) Cytokines and chemokines. (B) Structures of the chemokine family. Drawn from a schematic of [16].

Figure 2.
Schematic illustration of the composite preparation procedure and the fabrication process of the label-free CXCL8/IL-8 immunosensor. Adapted from Ref. [92] with permission.
Figure 2.
Schematic illustration of the composite preparation procedure and the fabrication process of the label-free CXCL8/IL-8 immunosensor. Adapted from Ref. [92] with permission.

Figure 3.
(A) Schematics of the layers of the SWEATSENSER strip on contact with skin and (B) Skin–device interface where SWEATSENSER is functionalized with specific antibodies to capture the biomarkers. Adapted from Ref. [103] with permission.
Figure 3.
(A) Schematics of the layers of the SWEATSENSER strip on contact with skin and (B) Skin–device interface where SWEATSENSER is functionalized with specific antibodies to capture the biomarkers. Adapted from Ref. [103] with permission.

Figure 4.
Schematic displays of the different steps involved in the preparation of (A) the immunosensor for CXCL7 by click chemistry assisted synthesis of IgG−alkyne−azide−MWCNTs and modification of SPCE (1); blocking step with casein and immobilization of anti-CXCL7 (2); sandwich assay with CXCL7 and biotin-anti−CXCL7 (3); incubation with AP−Strept (4); addition of 1-NPP and DP voltammetric monitoring of the 1-NP oxidation (5). (B) the dual CXCL7 and MMP3 immunoplatform involving carboxylated magnetic microbeads as substrates for preparation of the immunoconjugates. Reproduced from Refs. [88,89] with permission.
Figure 4.
Schematic displays of the different steps involved in the preparation of (A) the immunosensor for CXCL7 by click chemistry assisted synthesis of IgG−alkyne−azide−MWCNTs and modification of SPCE (1); blocking step with casein and immobilization of anti-CXCL7 (2); sandwich assay with CXCL7 and biotin-anti−CXCL7 (3); incubation with AP−Strept (4); addition of 1-NPP and DP voltammetric monitoring of the 1-NP oxidation (5). (B) the dual CXCL7 and MMP3 immunoplatform involving carboxylated magnetic microbeads as substrates for preparation of the immunoconjugates. Reproduced from Refs. [88,89] with permission.

Figure 5.
Scheme of the fundamentals of the electrochemical DNA biosensor for the determination of CXCL10/IP-10. (a) DNA anchor strand (purple) with a distal methylene blue reporter (blue hexagon) attached via thiol to AuE; (b) hybridization to a DNA recognition strand (green) linked to a CXCL10/IP−10 binding peptide; (c) SWV current reduction upon chemokine binding. Reproduced from Ref. [102] with permission.
Figure 5.
Scheme of the fundamentals of the electrochemical DNA biosensor for the determination of CXCL10/IP-10. (a) DNA anchor strand (purple) with a distal methylene blue reporter (blue hexagon) attached via thiol to AuE; (b) hybridization to a DNA recognition strand (green) linked to a CXCL10/IP−10 binding peptide; (c) SWV current reduction upon chemokine binding. Reproduced from Ref. [102] with permission.

Figure 6.
Schemes of (a) the magnetic immunoconjugate for the determination of CXCL8/IL8 with a superparamagnetic bead coated with the capture antibody, the antigen, the biotinylated detection antibody, and a fluorophore conjugated to avidin; (b) the MMB system (see the text for more information). Reprinted from Ref. [93] with permission.
Figure 6.
Schemes of (a) the magnetic immunoconjugate for the determination of CXCL8/IL8 with a superparamagnetic bead coated with the capture antibody, the antigen, the biotinylated detection antibody, and a fluorophore conjugated to avidin; (b) the MMB system (see the text for more information). Reprinted from Ref. [93] with permission.

Figure 7.
(A) Scheme of the steps for CXCL8/IL-8 determination by RCA and a fluorescent probe. (B) The design of a dual function microfluidic chip. (C) Hypoxia signalling pathway in TDECs and HUVECs. Adapted from Ref. [37] with permission.
Figure 7.
(A) Scheme of the steps for CXCL8/IL-8 determination by RCA and a fluorescent probe. (B) The design of a dual function microfluidic chip. (C) Hypoxia signalling pathway in TDECs and HUVECs. Adapted from Ref. [37] with permission.

Figure 8.
Scheme of the SERS immunosensor for CXCL8 detection (a) the glass slide modified with diatom frustules; (b) SEM image of a portion of the modified slide; (c) the sandwich-type configuration; (d) the bonding of the antibody. Reprinted from Ref. [90] with permission.
Figure 8.
Scheme of the SERS immunosensor for CXCL8 detection (a) the glass slide modified with diatom frustules; (b) SEM image of a portion of the modified slide; (c) the sandwich-type configuration; (d) the bonding of the antibody. Reprinted from Ref. [90] with permission.


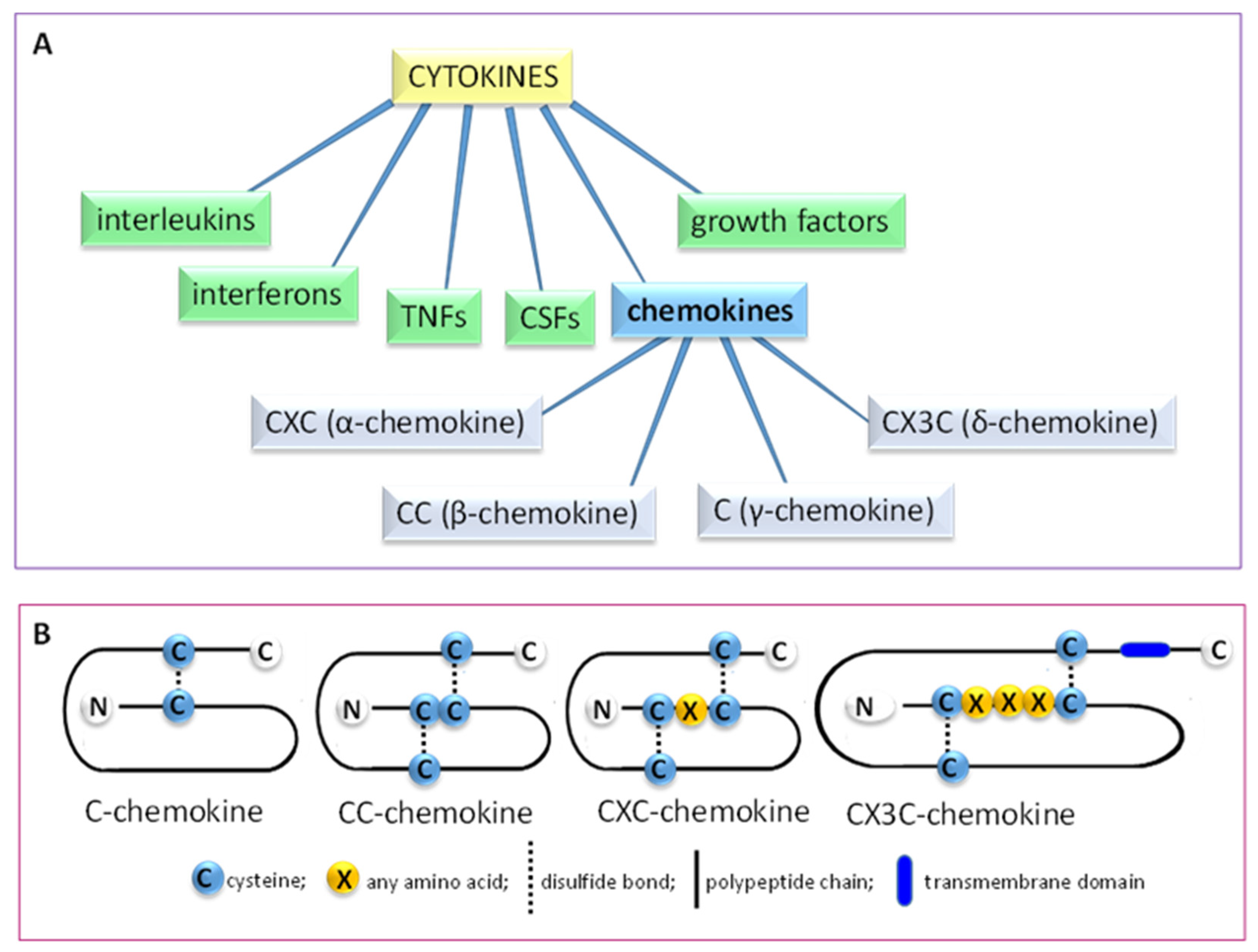{kind=link}
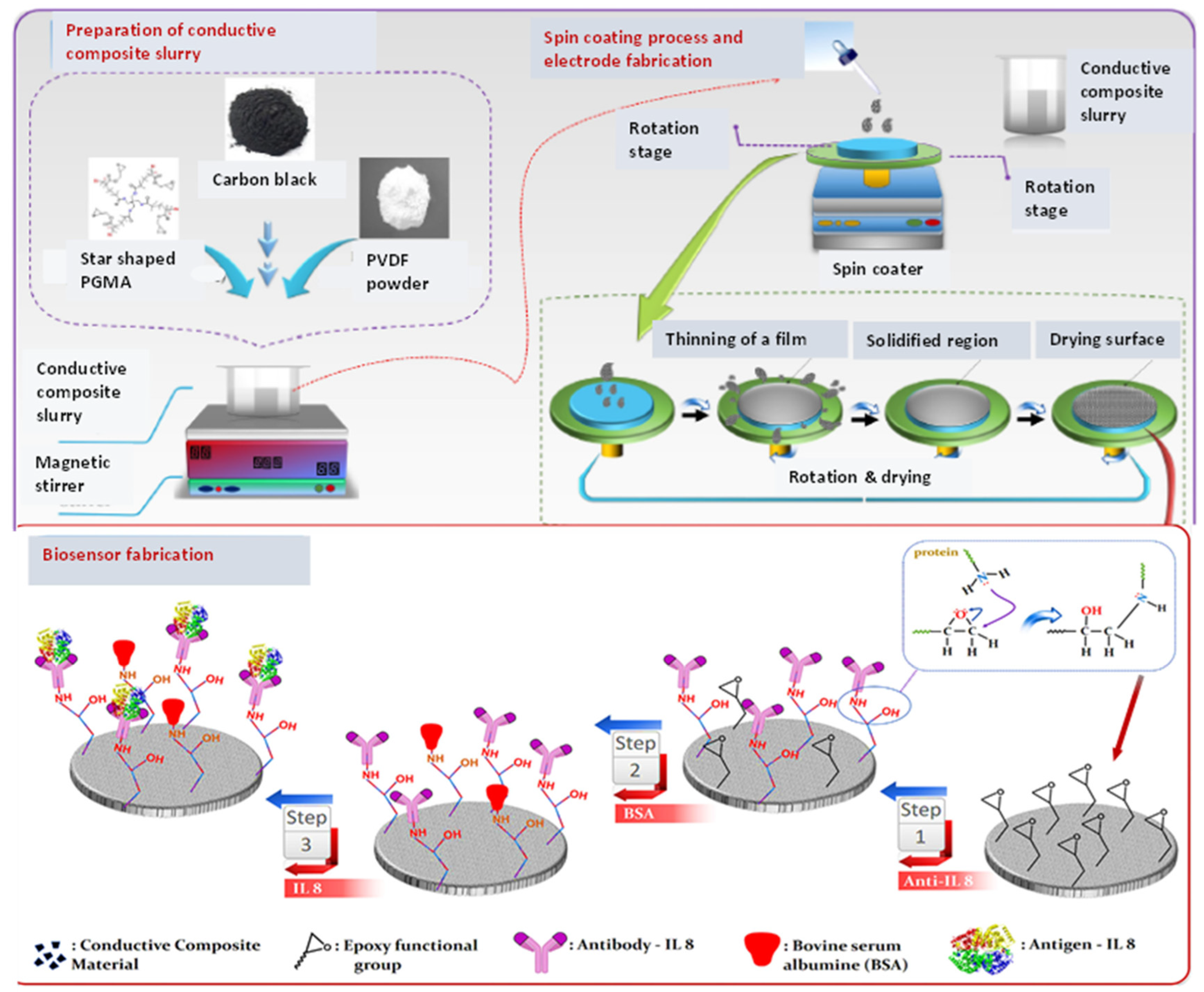{kind=link}
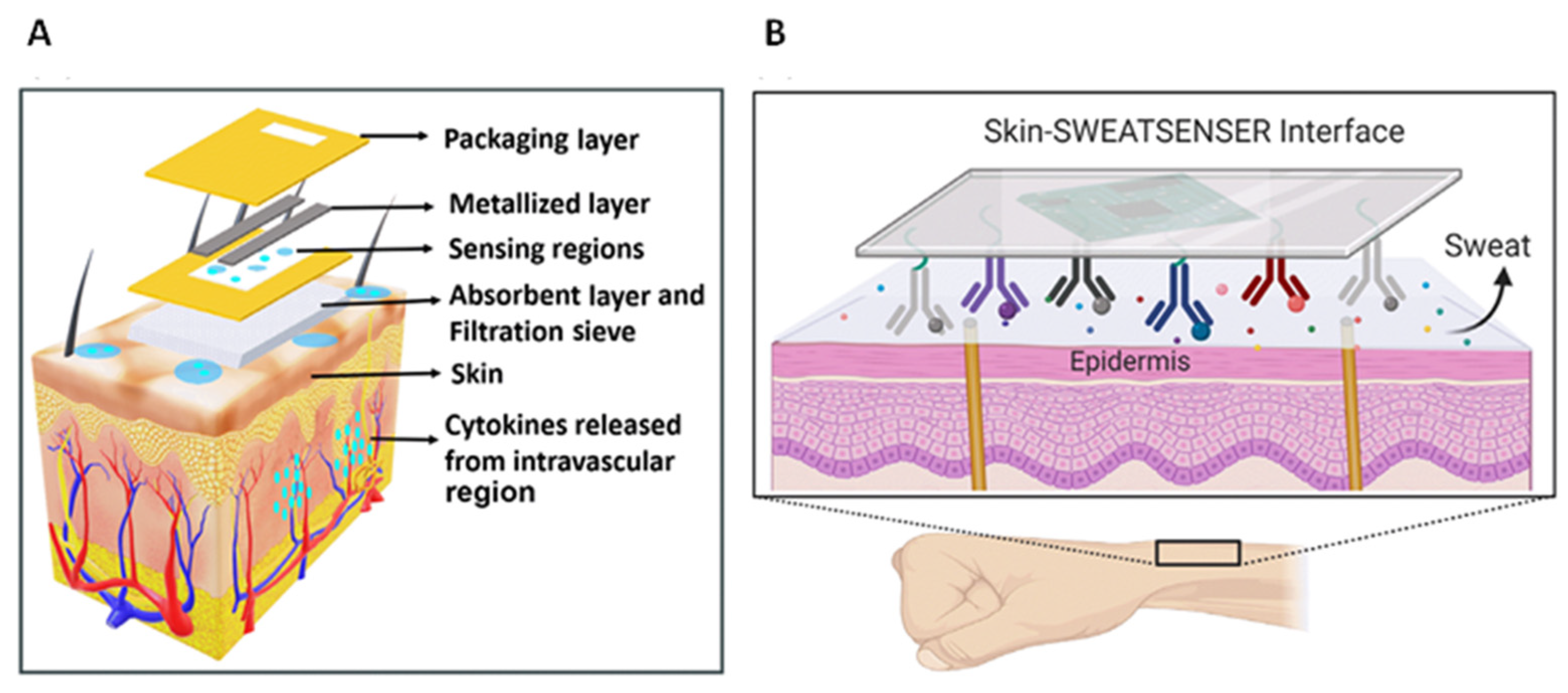{kind=link}
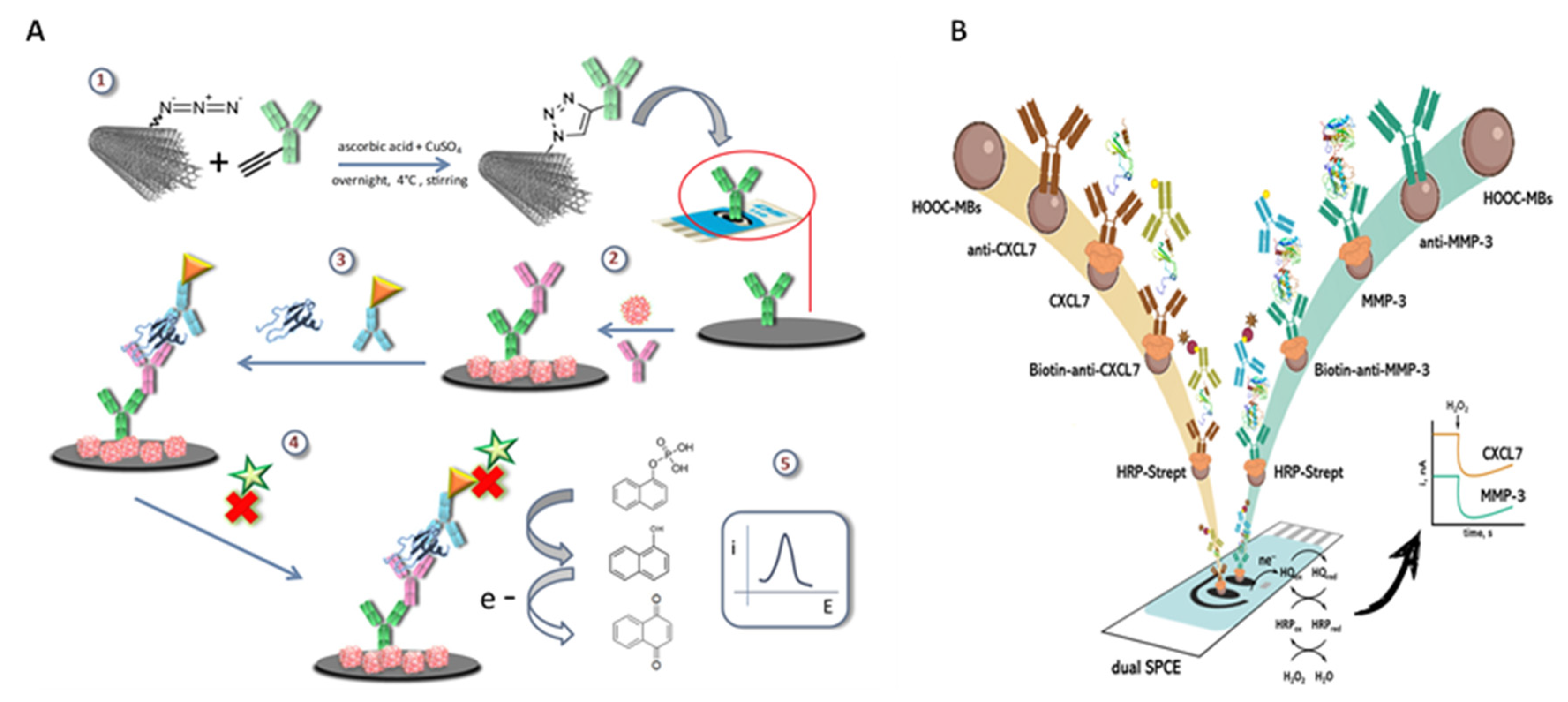{kind=link}
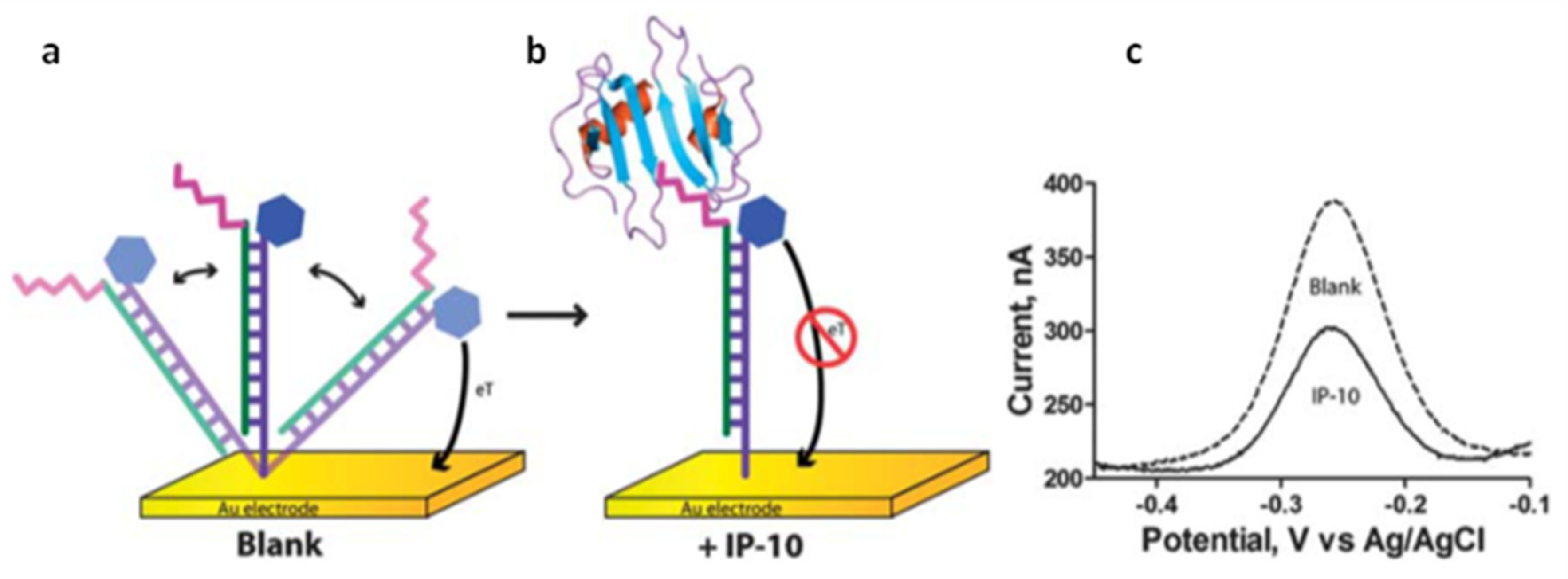{kind=link}
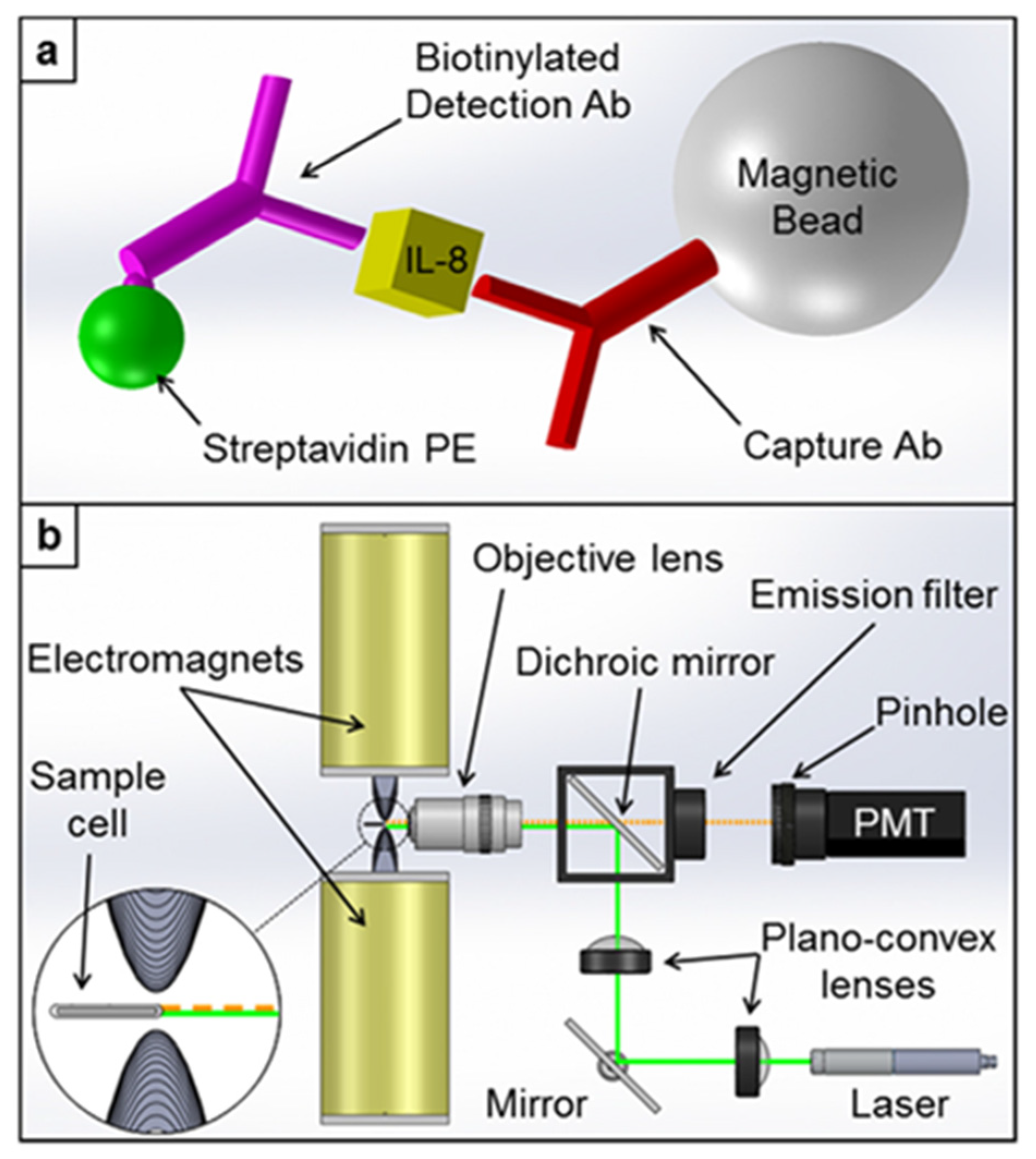{kind=link}
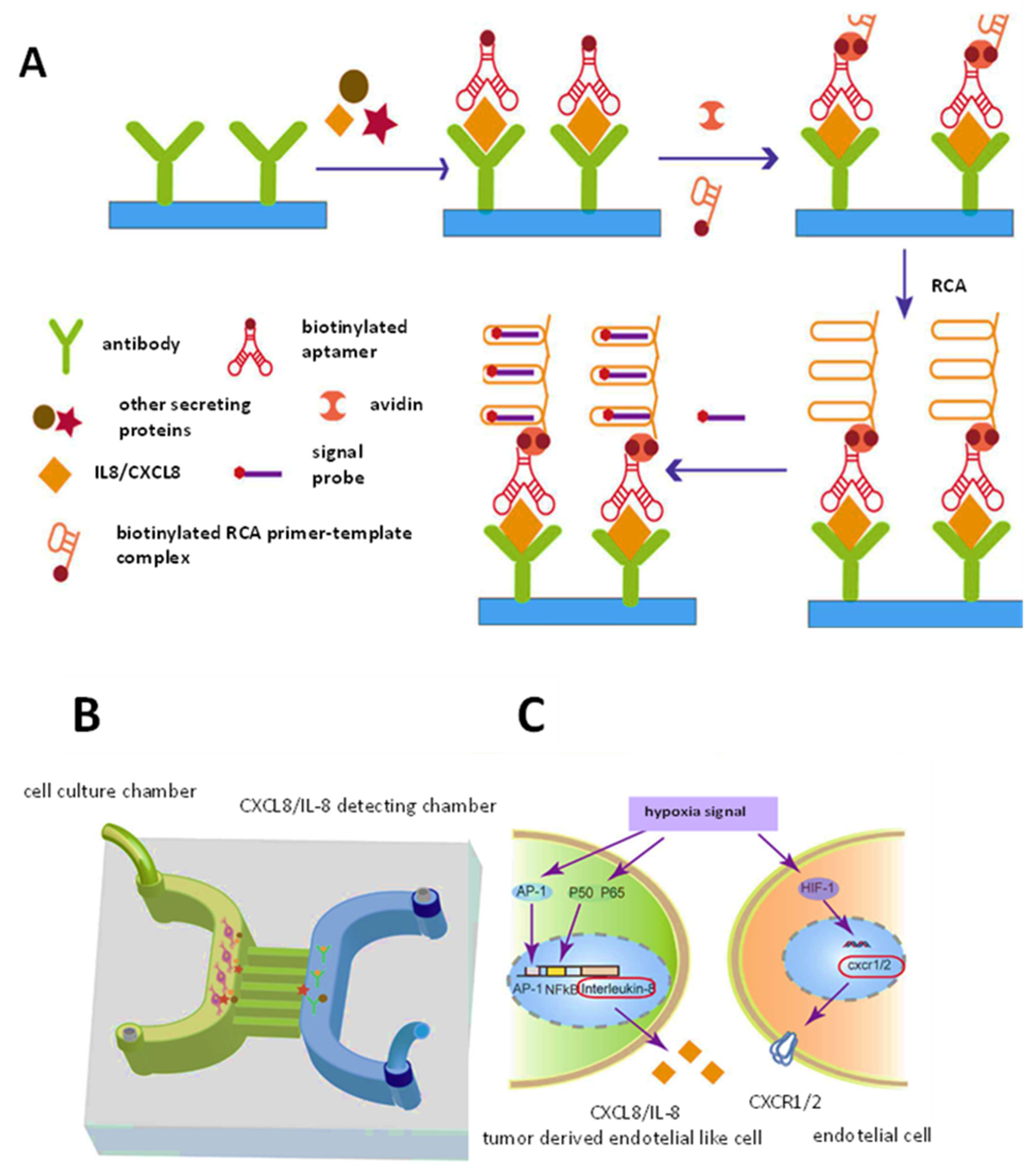{kind=link}
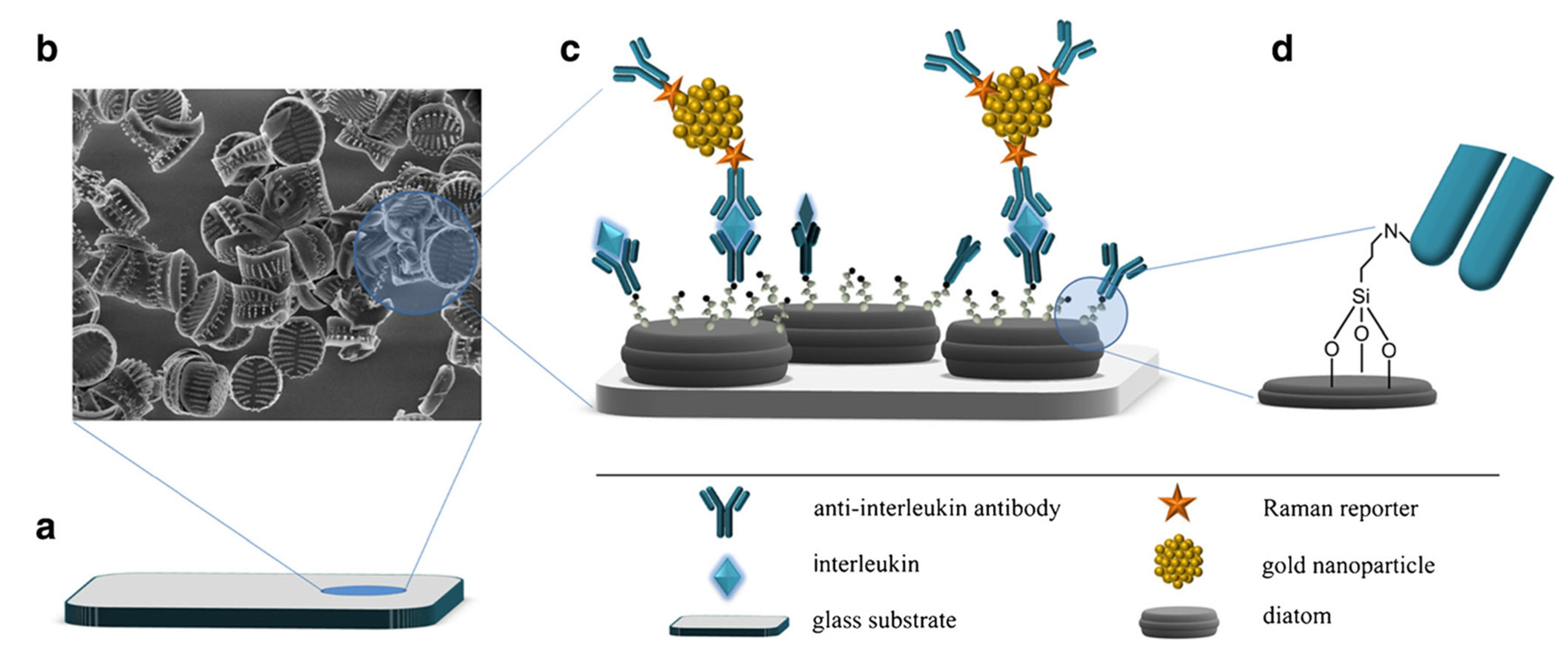{kind=link}
Table 1.
Some chemokines and chemokine receptors associated with various diseases.
| Chemokines, Receptors | Disease | Sample | Observations | Ref. |
|---|---|---|---|---|
| CXCL12, CXCL14, CXCR4 | HIV-1 | Peripheral blood mononuclear cells (PBMCs) | CXCL14 synergizes with CXCL12 via allosteric modulation of CXCR4; CXCL14 bound to CXCR4 with high affinity, induced redistribution of cell-surface CXCR4, and enhanced HIV-1 infection by >3-fold | [29] |
| CXCL8, CXCL10 (and pro-inflammatory cytokines) | Oral squamous cell carcinoma | Saliva, plasma | The levels of CXCL8 and CXCL10 were higher in the OSCC patients than in the controls | [30] |
| CCL3, MIP-1α | Cystic fibrosis (CF) | Tears | Patients with severe CF have significantly increased levels of MIP-1 α which correlate negatively with clinical status | [31] |
| CXCL8 (and IL-6, TNF-α) | Dental caries | Saliva | CXCL8 levels significantly higher in dental caries patients | [32] |
| CXCL8, CCL5/ RANTES (IL-1β, IL-6, IL-13, IL-17A, TNF-α) | Graves’ orbitopathy (GO) | Tears | Higher release of CCL5 (RANTES) and cytokines in GO patients | [33] |
| MCP-1, CXCL8 (and IL-6, IL-1β, TNF-α, γ-INF) | CKD (chronic kidney disease) | Saliva | MCP-1 and CXCL8 levels decrease in patients with CKD | [34] |
| CXCL8 (and various cytokines) | Thyroid-associated orbitopathy (TAO) | Tears | CXCL8 levels increase in patients of TAO | [35] |
| CCL2, CCL3, CCL8, CXCL10 (and IL-2, IL-6, IL-15, TNF-α, γ-INF) | Latent tuberculosis infection (LTBI) | Peripheral blood mononuclear cells (PBMCs) | Relevant role of CCL2 relevant for revealing subjects at higher risk of reactivation LTBI | [36] |
| CXCL8 | Glioblastomas | TDECs and UVECs | CXCL8 plays an important role in the process of glioma stem-like cell vascularization | [37] |
| CCL5/RANTES, MDC (and TGF-β1) | HSC expansion | Stem cell cultures | CCL5, MDC, TGF-β1: secreted factors deleterious to HSC expansion. Significant modulators in stem cell cultures. | [38] |
| CXCL13 | Sjögren’s syndrome (SS) | Serum, saliva | Elevated serum or salivary CXCL13 levels in patients with primary SS or SS | [39] |
| CXCL8 (and IL1α, IL 1β) | MERS-CoV | Sputum, tracheal aspirate | High expression of CXCL8 in the lower respiratory tract of MERS-CoV infected patients | [40] |
| CXCL8 (and IL-6, IL-10, TNF-α) | infection/ inflammation | Eccrine sweat | CXCL8 levels in sweat can be correlated to that in serum | [41] |
| CXCL13, CXCL10, CCL2, CCL3, CXCL12, CCL5 | Sjögren’s syndrome (SS) | Saliva | Higher levels of CXCL10 and CCL2 in primary SS | [42] |
| 28 cytokines, eight chemokines, and nine growth factors | Sepsis | Serum | Increased levels of CCL2, CCL3, CCL4, CCL5/RANTES, CCL11, CXCL10, CXCL12 in sepsis patients | [43] |
Table 2.
Some recent biosensors for chemokines and chemokine receptors.
| Type of Biosensor | Technique | Target(s) | Biodetection Principle | Dynamic Range | LOD | Sample | Ref. |
|---|---|---|---|---|---|---|---|
| Chemokine tagging with nanoluciferase fragment HiBiT and to Alexa-Fluor488-tagged CXCR4 | Luminescence (BRET) | CXCL12 | CRISPR/Cas9 genome editing used to tag the chemokine. CXCL12 secretion monitored in live cells | 1 fM–1 nM | - | live cells | [85] |
| Lentiviral particles with CXCR4 immobilized on MUA SAM onto Au chip | SPR | CXCL12 | Specific CXCL12 binding to LVPX4-coated chip in the biosensor | 5–50 nM | - | urine of RA patients | [86] |
| CXCR2-AuNPs/2,2′:5′,2″-tert-thiophene-3′(p-benzoic acid) | Amperometry | CXCL5 | Selection of the ligand for CXCR2 receptor by EIS | 0.1–10 ng/mL | 0.078 ng/mL | human serum CRC cells | [87] |
| Chip-based gold nanostructured micro-electrode with immobilized thiolated DNA | SWV | CCL5/RANTES CCL22/MDC | Amplified steric hindrance hybridization combining DNA and antibodies signaled by methylene blue | 10 pg/mL–10 ng/mL | 10 pg/mL | stem cell culture | [38] |
| Electrochemical sandwich-type immunosensor with immobilized anti-CXCL7 on IgG-MWCNTs/SPCE | Amperometry | CXCL7 | Electrode modification by click chemistry | 0.5–600 pg/mL | 0.1 pg/mL | human serum form patients with RA | [88] |
| Sandwich-type electrochemical dual immunosensing platform | Amperometry | CXCL7 | Simultaneous determination of CXCL7 and MMP3 with COOH-MBs on SPdCE | 1–75 ng/mL CXCL7 2.0–2000 ng/mL MMP3 | 0.3 ng/mL 0.8 pg/mL | +/− RA human serum | [89] |
| Sandwich-type with cAb immobilized on diatom biosilica/AuNPs/DTNB | SERS | CXCL8/IL-8 | cAb/AuNPs-DTNB as the Raman reporter | up to 30 ng/mL | 6.2 pg/mL | plasma | [90] |
| Dual-function microfluidic chip. Sandwich-type with Abs and aptamers | Fluorescence | CXCL8/IL-8 | Rolling circle amplification | 7.5–120 pg/mL | 0.84 pg/mL | TDEC and HUVEC | [37] |
| Label-free immunosensor with anti-CXCL8 immobilized on 6-phospho-hexanoic acid/ITO | EIS (charge transfer resistance, ΔRct) | CXCL8/IL-8 | Phosphonic acid covalently bound to hydroxylated ITO. EDC/NHS activation of carboxyl groups for Ab immobilization | 0.02–3 pg/mL | 6 fg/mL | human serum and saliva | [91] |
| Label-free immunosensor with anti-CXCL8 immobilized on SuperP© carbon black/Star polymer/ITO | EIS (charge transfer resistance, ΔRct) | CXCL8/IL-8 | The high conductivity of carbonaceous material enhances electron transfer | 0.01–3 pg/mL | 3.3 fg/mL | human serum and saliva | [92] |
| Sandwich-type fluorometric immunoassay with fluorophore-Avidin-Biotin-CXCL8-cAb-MBs | Fluorescence | CXCL8/IL-8 | Laser excitation of sample fluorophores | up to 5000 ng/L | 0.19 ng/mL | spiked human plasma | [93] |
| SiNMW FET biosensor with Abs immobilized onto APTES and GA modified surface | ΔR in I/V curves | CXCL8/IL-8 | Multiplexed determination of CXCL8 and TNF-α. Current/Resistance increase or decrease depending on pI of proteins | 10 fg/mL–1 ng/mL | 10 fg/mL | saliva | [94] |
| Optical modulation biosensing (OMB) | Fluorescence | CXCL8/IL-8 | SA-PE-Biotin-Ab2-CXCL8-Ab1-MBs | 0.05–10,000 ng/mL | 0.02 ng/L | - | [95] |
| Fluorometric immunosensor with H2O2 generating Au/TiO2 photocatalytic film and Cy5/cAb/GNR MEF probes | Fluorescence | CXCL8/IL-8 | One-pot, wash-free immunoassay. H2O2 induced chloro-1-naphthol precipitation quench Cy5 fluorescence via FRET | 1–1000 pg/mL | 0.612 pg/mL | serum | [96] |
| Label-free electrochemical immunosensor | EIS (Rct) | CXCL8/IL-8 | Anti-CXCL8 immobilized onto FTO-OH/IPTES platform. | 0.04–2 pg/mL | 11.9 fg/mL | human serum, saliva | [97] |
| Label-free synthetic Ab-mimetic protein-monothiol-alkane-PEG SAM-AuE | EIS (change in phase, Δθ(f)) | CXCL8/IL-8 | Ab-mimetic protein selected via phage display. Capture protein coding region subcloned in top ET11 | 900 fg/mL–900 ng/mL | 90 fg/mL | spiked serum | [98] |
| Label-free immunosensor with cAb immobilized onto pCBMA/AuE | EIS (Rct) | CXCL8/IL-8 | AuE modified by cysteamine adsorption, covalent linking of CB and photo-polymerization. | 55 fM–55 nM | 10 fM | nasal epithelial lining fluid | [99] |
| Electrochemical dual biosensing platform with anti-CXCL8 antibody and specific hairpin DNA sequence | Amperometry | CXCL8/IL-8 CXCL8 mRNA | Simultaneous determination of CXCL8 and CXCL8 mRNA involving COOH-MBs, Strept-MBs and dual SPCEs | 87.9–5000 pg/mL CXCL8; 0.32–7.5 nM CXCL8 mRNA | 72.4 pg/mL 0.21 nM | spiked human saliva | [100] |
| Array of nanofilm ZnO/metal electrodes functionalized with specific Abs | EIS | CXCL8/IL-8 CXCL10/IP-10 | Simultaneous determination of CXCL8 CXCL10, IL-6, IL-10 and TRAIL | 0.1–5000 pg/mL CXCL8 1–2000 pg/mL CXCL10 | ~1 pg/mL | sepsis patients´ serum | [101] |
| Electrochemical DNA biosensor. Immobilized DNA strand with a distal methylene blue reporter on SAM-AuE. | Amperometry | CXCL10 /IP-10 | Hybridization to recognition strand with target binding peptide. Current decrease as increase target concentration | 1–2000 nM | ~60 pM | serum | [102] |
| DTSSP/Abs solutions immobilized onto ZnO electrodes | EIS | CXCL10/IP-10 | Simultaneous determination of CXCL10, TRAIL and CRP | up to 500 pg/mL | <2 pg/mL | human sweat | [103] |
| Sulfo-LC-SPDP/Ab solution immobilized onto AuE. Sandwich-type electrochemical immunoassay. | Amperometry | CCL17/TARC | HRP-Strept-Biotin-Ab2 conjugates for TMB/H2O2 detection | 387–50,000 pg/mL | 194 pg/mL | serum from patients with cHL | [62] |
| Sandwich-type electrochemical immunosensor with cAb immobilized on rGO-(rGO-TEPAThi-Au)/GCE | Amperometry | CCL2/MCP1 | Signal amplification with Ab2-RuPdPt | 20 fg/mL–1000 pg/mL | 8.9 fg/mL | spiked serum | [104] |
| Label-free electrochemical immuno-sensor with cAb immobilized on Au @Pt-CA-AuE | DPV | CCL2/MCP1 | Decrease in peak current of Fe(CN)63−/4− as increased CCL2 concentration | 0.09–360 pg/mL | 0.03 pg/mL | spiked serum | [105] |
| Sandwich-type immunosensor with cAb immobilized onto a silicon photonic micro ring resonator. | Res λ shift | CCL2/MCP1 | Shifts in resonance wavelength are related to the target concentration | 84.3–1582.1 pg/mL | 0.5 pg/mL | spiked serum | [106] |
| Label-free electrochemical immunosensor with cAb immobilized on PtNPs/SWCNHs | Amperometry | CCL2/MCP1 | Reduction current of H2O2 decrease as increased CCL2 concentration | 0.06–450 pg/mL | 0.02 pg/mL | serum | [107] |
| Label-free anti-CCR4-PPyr-CSsg-ITO immunosensor | EIS | CCR4 | Amino groups of anti-CCR4 antibodies bound covalently to succinimide groups of PPyr-CSsg polymer | 0.024–12 pg/mL | 7.3 fg/mL | human serum | [108] |
| Label-free anti-CCR4-P(Pyr-Pac)-ITO | EIS | CCR4 | Amino groups of anti-CCR4 antibodies bound covalently to carboxyl groups of P(Pyr-Pac) polymer | 0.02–8 pg/mL | 6.4 fg/mL | human serum | [109] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sánchez-Tirado, E.; Agüí, L.; González-Cortés, A.; Yáñez-Sedeño, P.; Pingarrón, J.M. Biodetection Techniques for Quantification of Chemokines. Chemosensors 2022, 10, 294. https://doi.org/10.3390/chemosensors10080294
AMA Style
Sánchez-Tirado E, Agüí L, González-Cortés A, Yáñez-Sedeño P, Pingarrón JM. Biodetection Techniques for Quantification of Chemokines. Chemosensors. 2022; 10(8):294. https://doi.org/10.3390/chemosensors10080294
Chicago/Turabian StyleSánchez-Tirado, Esther, Lourdes Agüí, Araceli González-Cortés, Paloma Yáñez-Sedeño, and José M. Pingarrón. 2022. "Biodetection Techniques for Quantification of Chemokines" Chemosensors 10, no. 8: 294. https://doi.org/10.3390/chemosensors10080294
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.