BRAF: A Two-Faced Janus
by
 , , and
, , and
Pasquale Pisapia
 ,
,
Francesco Pepe
, 
Antonino Iaccarino
,
Roberta Sgariglia
,
Mariantonia Nacchio
,
Gianluca Russo
 ,
,
Gianluca Gragnano
,
Umberto Malapelle
 and
and
Giancarlo Troncone
*
Department of Public Health, University of Naples Federico II, 80131 Naples, Italy
*
Author to whom correspondence should be addressed.
Cells 2020, 9(12), 2549; https://doi.org/10.3390/cells9122549
Submission received: 4 November 2020
/
Revised: 18 November 2020
/
Accepted: 25 November 2020
/
Published: 27 November 2020
(This article belongs to the Special Issue Identification of Prognostic Markers in Cancer Biology)
Abstract
:Gain-of-function of V-Raf Murine Sarcoma Viral Oncogene Homolog B (BRAF) is one of the most frequent oncogenic mutations in numerous cancers, including thyroid papillary carcinoma, melanoma, colon, and lung carcinomas, and to a lesser extent, ovarian and glioblastoma multiforme. This mutation aberrantly activates the mitogen-activated protein (MAP) kinase extracellular signal-regulated kinase (MEK)/extracellular signal-regulated kinase (ERK) signaling pathway, thereby eliciting metastatic processes. The relevance of BRAF mutations stems from its prognostic value and, equally important, from its relevant therapeutic utility as an actionable target for personalized treatment. Here, we discuss the double facets of BRAF. In particular, we argue the need to implement diagnostic molecular algorithms that are able to detect this biomarker in order to streamline and refine diagnostic and therapeutic decisions.
1. Introduction
The V-Raf Murine Sarcoma Viral Oncogene Homolog B (BRAF) oncogene, localized on chromosome 7q34, encodes for a serine–threonine protein kinase belonging to the rapidly accelerated fibrosarcoma (Raf) protein family (which also includes ARAF and CRAF proteins) [1]. Initially identified as a viral oncogene, the RAF gene was first described in 1983 [2]. Physiologically, Raf proteins and MAP kinase kinase kinases (MAPKKKs) play a key role in the mitogen-activated protein (MAP) kinase cascade [3]. In particular, they act as effectors of Rat sarcoma (Ras) proteins and as direct activators of the MAP kinase extracellular signal-regulated kinase (MEK)/extracellular signal-regulated kinase (ERK) pathway [4,5,6,7,8,9,10]. This pathway is associated with several cell functions, such as cell growth and proliferation, differentiation, migration, senescence, and apoptosis [11,12,13,14,15,16]. Generally, Raf proteins feature three conserved regions (CR), each having its own distinctive tasks. The CR1 domain is characterized by two subdomains: a Ras-binding domain (RBD), crucial for the interface with Ras proteins, and a cysteine-rich domain (CRD), necessary for the interaction with Ras proteins and Raf kinase domain auto-inhibition [17]. The CR2 domain works as an inhibitor against Ras protein binding and Raf activation [18]. Finally, CR3 features kinase activity [19].
The first evidence of an association between BRAF gene mutations and human cancers dates back to 2002 [20]. Generally, BRAF mutations are more frequently associated with human cancer than ARAF and CRAF alterations. As some studies suggest, this phenomenon may be due to the fact that whereas BRAF oncogenic activation is triggered by a substitution of a single amino acid, ARAF and CRAF oncogenic alterations require a double mutational event [21]. To date, BRAF mutations account for about 7% of all human solid tumors, with a high prevalence in papillary thyroid carcinomas (PTC), melanomas, colorectal cancers (CRC), and lung cancers [20,22,23,24,25,26,27]. The most common type of BRAF mutation is exon 15 p.V600E [20]. So far, about 200 BRAF mutant alleles have been described in human tumors [28]. Accordingly, BRAF mutations have been categorized into a three-class system according to their effect on the activity of BRAF protein (Table 1 and Figure 1 and Figure 2) [24,28,29,30,31].
Class I alterations are the most common ones. They include exon 15 p.V600 alterations. These mutations induce elevated levels of kinase activity, thereby promoting the activation of MEK/ERK pathways independently of Ras activation and protein dimerization [24,28,29,30,31]. Class II alterations are, instead, less common and involve several point mutations, in particular exon 11 p.G464E/V, exon 11 p. G469A/R/V, exon 15 p. L597Q/V, and exon 15 p.K601E/N/T, as well as gene fusions. Like class I, this class is Ras-independent. However, whereas Class I promotes only elevated levels of kinase activity, Class II triggers both intermediate and high kinase activity. Moreover, as opposed to Class I, Class II requires protein dimerization to activate the MEK/ERK pathway [24,28,29,30,31]. Finally, Class III alterations are associated with low or no kinase activity and require both Ras upstream activation and dimerization with CRAF to induce MER/ERK pathway activation; in addition, they commonly co-occur with upstream activating alterations such as Neuroblastoma RAS Viral Oncogene Homolog (NRAS) mutations, Neurofibromin 1 (NF1) loss, or receptor tyrosine kinase mutations [24,28,29,30,31].
Unlike Class II and Class III RAF-mutations, which may have less aggressive behavior, Class I mutations, namely, BRAF exon 15 p. V600, are associated with a higher degree of tumor aggressiveness and poor prognosis. Indeed, patients carrying this type of mutation have shorter disease-free survival (DFS) and bleaker overall survival (OS) rates than wild-type patients [34]. However, besides its prognostic role, accruing evidence has recently highlighted the role of BRAF exon p.V600 mutations, in particular BRAF exon 15 p. V600E, as predictive biomarkers of response to tyrosine kinase inhibitors (TKIs) [35,36,37].
In this review, we will examine the double facets of BRAF gene alterations in different tumor types to highlight the clinical relevance of this biomarker not only in improving the pathological assessment of human solid neoplasms but also in facilitating treatment decision-making and outcomes.
2. Prognostic Role of BRAF Mutations
2.1. Lung Cancer
The presence of BRAF mutations in non-small cell lung cancer (NSCLC) patients was first reported in 2011 [25]. Since then, subsequent studies have investigated the variable frequency of these alterations in NSCLC adenocarcinoma patients (from 1.5–3.5% to 7–8%) [31,38,39,40]. Regarding the subtypes of BRAF mutations, discordant results have been reported. For instance, whereas some authors highlight a higher prevalence of BRAF exon 15 p.V600E than BRAF non-p.V600E [25,41,42,43,44], others state opposite results [26,45,46]. Despite these contradictory findings, almost all NSCLC BRAF-mutated cases feature an adenocarcinoma morphology with a micropapillary growth pattern and strong expression of thyroid transcription factor 1 (TTF-1) [25]. Although BRAF mutations are strongly associated with glandular morphology, occasional reports have also described this alteration in small cell carcinoma and in different NSCLC subtypes, such as squamous cell carcinoma, large cell neuroendocrine carcinomas, and pulmonary sarcomatoid carcinomas [47,48,49,50]. Thus, it is conceivable that patients carrying BRAF mutations could be eligible to receive TKI treatments, even in the absence of an adenocarcinoma component.
From an epidemiological point of view, whereas some studies have indicated the higher frequency of BRAF mutations among females and current or former smokers [25,41], others have found no specific association between BRAF mutations and sex or tobacco smoking. Consequently, BRAF molecular testing by adopting next-generation sequencing (NGS) technologies in advanced-stage NSCLC patients is strongly recommended [51].
To date, the prognostic role of BRAF in NSCLC patients is still debated. Warth et al. showed a shorter disease-free survival (DFS) in BRAF exon 15 mutant patients than in wild-type patients [52]. Of note, they found no significant differences in the OS rates between the two groups [52]. A few years later, Zheng et al. reported contrasting results. Indeed, in their large-scale study aimed at identifying the prevalence of BRAF mutations among Chinese patients with lung adenocarcinoma, they found that the median relapse-free survival (RFS) of patients harboring either BRAF exon 11 or BRAF exon 15 was significantly longer than the RFS of NSCLC patients harboring other types of mutations, including Epidermal Growth Factor Receptor (EGFR), Kirsten Rat Sarcoma Viral Oncogene Homolog (KRAS), Anaplastic Lymphoma Kinase (ALK), Erb-B2 Receptor Tyrosine Kinase 2 (ERBB2), or wild-type (47.8 vs. 21.5 months) [53]. However, in a similar study, Paik et al. observed that the 2-year OS in patients harboring BRAF mutations was lower (57%) than that in patients harboring EGFR mutations (69%) and ALK rearrangements (91%). By contrast, it was higher in KRAS-mutated patients (40%) [43]. Similarly, Litvak et al. reported that the overall survival rate for patients with BRAF mutations was intermediate between those with KRAS (lower) and those with EGFR (higher) mutations [54].
On the other hand, several other studies have reported different OS rates. For instance, Kinno et al. described an insignificant difference between the OS rates of patients with BRAF exon 15 p.V600E and BRAF non-p.V600E mutations and wild-type patients [55]. Similarly, Villaruz et al. found no differences between the OS rates of BRAF-mutant patients and those harboring other genomic alterations [56]. Tissot et al., instead, highlighted a higher OS rate for BRAF-mutated NSCLC patients than for wild-type patients (22.1 vs. 14.5 months, respectively) [57]. Regarding the types of BRAF mutations influencing OS, the median OS was higher in BRAF exon 15 p.V600E mutants than in BRAF non-p.V600E mutants (25 vs. 13 months, respectively), even in stage IV patients (16 vs. 7 months, respectively) [57].
Clearly, the prognostic significance of BRAF mutations in lung cancer patients needs further elucidation. However, we are aware that planning prognostic perspective studies uninfluenced by BRAF-targeted therapies may be challenging, considering the burgeoning interest in BRAF as a predictive biomarker.
2.2. Melanoma
BRAF mutations occur in about 40–60% of melanomas [58]. A staggering 97% of these alterations are observed within exon 15 (codon 600) [59]. BRAF exon 15 is indeed the most common alteration, accounting for up to 90% of cases. It involves a T-to-A transversion in nucleotide 1799 (c.1799T>A), which, in turn, determines valine to glutamic acid substitution (p.V600E) [60]. Less frequently, a substitution from valine to lysine (p.V600K, 10–20%), arginine (p.V600R, 1%), methionine (p.V600M, 0.3%), or aspartic acid (p.V600D, 0.1%) may be observed within codon 600 [60]. Epidemiologically, BRAF-mutated melanomas occur in younger patients and very frequently display a superficial diffusion or nodular morphology. As opposed to wild-type cases, they are located in anatomical regions without chronic sun damage [61] and are more prone to metastasize to the brain than wild-type melanomas [23,62].
The prognostic role of BRAF in melanoma progression is not as controversial as in lung cancer patients. Broadly speaking, BRAF-mutated melanomas are characterized by more aggressive clinical features than wild-type ones [63]. Indeed, whereas a few studies report no significant differences in the survival rates of BRAF-mutated and wild-type metastatic melanoma patients [64,65], most highlight its negative prognostic factors [66]. For instance, Long et al. noted that although the time between disease presentation and metastatic progression is basically the same between BRAF-mutant and wild-type patients, a poorer median survival characterizes BRAF-mutant cases compared to wild-type patients (5.7 vs. 8.5 months, respectively) [61]. Still, Ekedahl et al. reported that BRAF-driven cases had a much worse prognosis than stage IV wild-types or NRAS-mutant melanoma patients [67]. As for OS, Moreau et al. reported that BRAF exon 15 p.V600 mutations correlated with poorer OS than wild-type cases (1.4 and 2.8 years, respectively) [68]. Likewise, Picard et al. and Barbour et al. demonstrated a negative prognostic role for BRAF mutations in stage III melanoma patients [69,70]. More recently, in a large systematic review and meta-analysis, Ny et al. confirmed the negative prognostic role of BRAF mutations in melanoma patients [71]. Moreover, BRAF seems to play a relevant prognostic role not only in the late stages but also in the earlier stages of the disease. For example, Cheng et al. found an association between BRAF mutations and poor prognosis in stage I and stage II melanoma patients [72]. Similarly, Nagore et al. reported poor prognosis in BRAF-driven localized melanomas [73].
2.3. Thyroid Cancer
The occurrence of BRAF mutation in thyroid cancer is even more complex to analyze. A large body of evidence indicates that the frequency of BRAF mutations (almost exclusively occurring as exon 15 p.V600E; from 18% to 87%) varies among thyroid cancers [74,75]. As a general rule, they occur more frequently in sporadic PTCs, in particular tall cell variant and aggressive microcarcinomas of adult patients [76,77], followed by PTC-derived anaplastic thyroid carcinomas (ATCs) and poorly differentiated carcinomas [74,78,79,80]. On the other hand, they are very rare or totally absent in other thyroid lesions, including medullary carcinomas, follicular carcinomas, and benign neoplasms [74,78,79,80]. In addition, our research group has demonstrated that BRAF exon 15 p.V600E point mutations play a diagnostic role in refining the risk of malignancy and treatment options in patients with cytological “indeterminate” nodules [81,82].
From a prognostic perspective, BRAF-mutated thyroid carcinomas feature more aggressive behavior and poorer outcomes than wild-types [77,83,84,85]. In addition, BRAF mutations have occasionally been associated with a higher risk of recurrence and persistence [83,86]. Consistently, Nikiforova et al. highlighted a significant association of BRAF mutations with extrathyroidal invasion and advanced stages at the time of diagnosis compared with wild-type cases [78]. Likewise, other clinical studies have reported a tight correlation between BRAF mutations and extrathyroidal diffusion [87,88,89]. In accordance with these findings, Elisei et al.’s 15-year follow-up study demonstrated the poorer prognostic outcome of BRAF exon 15 p.V600E-mutated patients compared to wild-types [77]. A few years later, Xing et al. carried out a retrospective multicenter study at 16 centers located in eight countries to investigate the role of the BRAF exon 15 p.V600E variant in PTC recurrence. Interestingly, their findings indicate that BRAF exon 15 p.V600E point mutation is a prognostic factor independent of the other conventional clinicopathological risk factors generally associated with PTC [90]. In addition, the authors emphasized that even in the early stages (stage I or II) of the disease and in micro-PTC, detection of BRAF exon 15 p.V600E is strongly associated with disease recurrence [90]. Similar results were also substantiated in another study by Elisei et al. [91]. Likewise, a significant negative correlation between BRAF exon 15 p.V600E point mutations and shorter OS rates was also emphasized in Liu et al.’s study [92].
Different lines of research have also investigated the epigenetic mechanisms whereby BRAF mutation impairs iodine metabolism. Indeed, BRAF exon 15 p.V600E point mutation promotes the downregulation and silencing of sodium-iodide symporter (NIS), a gene involved in iodine metabolism, by inducing histone deacetylation [93,94]. This phenomenon explains why BRAF exon 15 p.V600E thyroid carcinomas are resistant to radioiodine treatment [83]. Building on this evidence, Oler et al. demonstrated that the downregulation and silencing of thyroid iodide-metabolizing genes may also be associated with poorly differentiated tumors featuring more aggressive behavior [95]. They also indicated that the expression of NIS and Thyroid Stimulating Hormone Receptor (TSHR) is more significantly reduced in BRAF-mutated patients than in BRAF wild-types [95]. Finally, the authors advanced the hypothesis that this phenomenon might be responsible for additional genetic alterations, eventually leading to tumor aggressiveness and dedifferentiation [95].
2.4. Colorectal Cancer
BRAF mutations are much less frequent in CRC, accounting for only 10% of reported cases [96,97]. As for the other cancer types, the vast majority of BRAF mutations occur in codon 600 (exon 15 p.V600E) [98]. Epidemiologically, BRAF-mutated CRCs are detected more frequently in women and older patients (>70 years) [99]. Morphologically, BRAF-mutated CRCs are primarily located in the proximal colon (right side) and show mucinous, serrated, and poorly differentiated histology [99,100]. Concerning the subtypes of BRAF mutations, non-p.V600E mutations seem to occur more frequently in men and younger patients, have low-grade histology, and are localized on the distal colon site, in contrast to BRAF exon 15 p.V600E mutations [101]. In addition, patients harboring BRAF non-p.V600E show a longer median OS than BRAF exon 15 p.V600E-mutated patients [101]. Epigenetically, BRAF-mutated CRCs feature a high CpG island methylator phenotype (CIMP-H) and high microsatellite instability (MSI-H) [102,103].
Regarding its impact on prognosis, CRC patients with BRAF exon 15 p.V600E mutations show lower OS, DFS, and cancer-specific survival (CSS) rates than wild-type patients, despite the stage of the disease (II or III) or the adoption of chemotherapeutic regimens after surgery [104]. Consistently, Roth et al. reported lower OS rates for BRAF-mutated patients than for wild-types [105]. Samowitz et al. highlighted that BRAF exon 15 p.V600E mutant CRC patients have a worse prognosis in terms of OS regardless of age, stage (II to IV), and tumor site compared to BRAF wild-type patients [98]. Notably, the authors also observed that BRAF exon 15 p.V600E mutant CRC patients featuring microsatellite-stable (MSS) tumor patterns had significantly lower OS rates than MSI tumors, regardless of the stage of the disease (II to IV) [98]. Conversely, BRAF mutations did not influence the better prognosis of MSI CRCs [98]. Similar results have been reported by Ogino et al. [106]. In their experience, the authors observed that BRAF-mutated CRC patients were characterized by worse outcomes than BRAF wild-type cases [106]. When considering both BRAF and MSI status, they observed the worst OS rate in BRAF-mutated and MSS CRC patients [106]. Interestingly, BRAF mutations only slightly affected the outcome of MSI-H tumors [106].
The negative prognostic role of BRAF mutations has long been established in the metastatic setting. Back in 2009, findings from FOCUS, a large, multicenter clinical trial, indicated that although BRAF mutation did not significantly affect progression-free survival (PFS), it did have a worse impact on the OS of patients, compared with wild-types [107]. Conversely, in a pooled analysis of four clinical trials (FOCUS, CAIRO, CAIRO2, and COIN), both median PFS and median OS rates were lower in BRAF-mutant patients than in wild-types [108]. In addition, the authors further observed that proficient mismatch repair (pMMR) of CRC tumors harboring BRAF mutations had a lower median PFS and OS than BRAF wild-types [108]. Another broad pooled analysis, assessing the independent negative prognostic role of BRAF mutations in OS, revealed that BRAF-mutant patients had a worse prognosis even after metastasectomy [109]. In accordance with these studies, several others have confirmed worse outcomes in BRAF-mutated patients after lung or liver metastasis surgical resections than in wild-types [110,111,112].
2.5. Other Lesions
Besides the high incidence of BRAF mutants in the neoplasms mentioned above, other less common entities may also feature BRAF mutations. Among these are pediatric low-grade gliomas (PLGGs). These lesions are highly frequent among pediatric patients harboring BRAF p.V600E point mutations and have poorer outcomes than wild-type patients [113,114]. Conversely, glioblastoma patients harboring BRAF exon 15 p.V600E have the same prognosis as wild-type patients, despite the prevalence of epithelioid morphology without isocitrate dehydrogenase (IDH) alterations [115].
In breast cancer patients, the prognostic scenario is very similar, albeit the frequency of these aberrant mutations is low. Generally, poorer prognosis is observed in triple-negative breast cancers [115]. In addition, BRAF gene alterations may be a rare cause of anti-human epidermal growth factor receptor 2 (HER2) therapy resistance [116].
Finally, BRAF mutations have also been detected in ovarian cancer. Indeed, Grisham et al. rather recently observed that BRAF mutations had better prognostic outcomes in early-stage low-grade serous ovarian cancer. The authors hypothesized that the better OS rates in these patients were due to the possibility that BRAF mutations in patients with serous borderline disease prevent progression to more aggressive stages [117].
3. Predictive Role of BRAF Mutations
3.1. Lung Cancer
Besides having a prognostic role, BRAF mutations have also emerged as positive predictive markers for identifying NSCLC patients who might benefit from the administration of targeted therapy [118,119,120,121]. Considerable evidence has demonstrated that BRAF inhibitors, namely, vemurafenib and dabrafenib, effectively work against BRAF exon 15 p. V600-positive tumor cells [122].
In a large study in which vemurafenib was administered to pretreated nonmelanoma BRAF exon 15 p.V600E-mutated patients, an objective response was observed in 42% of NSCLC patients, with a median PFS of 7.3 months and a 12-month PFS rate of 23% [123]. Consistently, the results of a vemurafenib basket (VE-BASKET) trial, involving n = 62 NSCLC patients, recently confirmed not only the efficacy of this BRAF inhibitor but also its safety profile in advanced-stage NSCLC BRAF exon 15 p.V600-positive patients [124]. Of note, vemurafenib also shows promising results in brain metastases [120].
The other BRAF inhibitor, dabrafenib, appears to be just as promising as vemurafenib. In a phase I dose-escalation trial, dabrafenib showed safety and efficacy in different solid tumors harboring BRAF exon 15 p.V600 point mutations, including NSCLC patients [125]. Noteworthy, in one study, dabrafenib was successfully adopted when a BRAF exon 15 p.V600E-mutated lung adenocarcinoma patient became resistant to vemurafenib [121]. In accordance with these studies, Gautschi et al. demonstrated the efficacy of different targeted therapies (vemurafenib, dabrafenib, sorafenib) in advanced-stage NSCLC patients harboring BRAF mutations [126]. They observed that the OS of patients receiving targeted therapies was longer in patients harboring a BRAF exon 15 p.V600E mutation than in those harboring non-p.V600E mutations (25.3 vs. 11.8 months) [126].
The efficacy of dabrafenib as monotherapy, or in combination with other drugs, has also been investigated in a phase-II clinical trial involving 84 BRAF (exon 15 p.V600E)-positive NSCLC patients. Patients were divided into two cohorts: Cohort A received dabrafenib alone [127], whereas Cohorts B and C received dabrafenib in combination with the MEK inhibitor trametinib [128,129]. On the whole, the objective response and disease control rates observed in Cohort A were 33% and 58%, respectively. In addition, the median PFS and median duration of response (DOR) were 5.5 and 9.6 months, respectively [127]. In Cohorts B and C, dabrafenib, together with trametinib, was administered to previously treated and untreated advanced-stage NSCLC patients harboring the BRAF exon 15 p.V600E point mutation [128,129]. In both cohorts, the combination showed clinically relevant antitumor activity in terms of overall responses (63.2% and 64.0%, respectively), PFS (8.6 and 14.6 months, respectively), DOR (9.0 and 15.2 months, respectively), and a manageable safety profile [128,129]. In addition, although the data were limited, the combination of these two inhibitors was able to act on brain metastasis [127,128,129]. After these promising results, the combination of dabrafenib and trametinib was approved by the Food and Drug Administration (FDA) and the European Medical Agency (EMA) for advanced-stage NSCLC patients harboring a BRAF exon 15 p.V600E point mutation, irrespective of previous treatments [130,131].
Regarding other types of BRAF inhibitors, anecdotal experiences have reported the efficacy of the multitarget kinase inhibitor sorafenib. Indeed, this inhibitor has a broad spectrum efficacy by acting on several types of kinases in BRAF non-p.V600-mutated patients (exon 11 p.G469R and exon 11 p.G469V). Among these are BRAF, CRAF, KIT Proto-Oncogene, Receptor Tyrosine Kinase (c-KIT), Fms Related Receptor Tyrosine Kinase 3 (FLT-3), Rearranged During Transfection (RET), Vascular Endothelial Growth Factor Receptor 2 (VEGFR-2), VEGFR-3 and Platelet-Derived Growth Factor Receptor Alpha (PDGFRA) in BRAF non-p.V600-mutated patients (exon 11 p.G469R and exon 11 p.G469V) [132,133]. Finally, two phase-I clinical trials demonstrated the efficacy and safety of ERK inhibitors (e.g., ulixertinib, an ERK1/2 kinase inhibitor) and pan-RAF inhibitors (e.g., LY3009120) in BRAF-mutant patients [134,135].
3.2. Melanoma
Like in lung cancer, BRAF mutations, in particular, exon 15 p. V600 point mutations, feature a positive predictive role in melanoma patients for the administration of TKIs [136]. In the BRIM-3 randomized, phase III clinical trial, the effect of vemurafenib on PFS and OS rates was compared with standard chemotherapy treatment (dacarbazine) in advanced-stage previously untreated melanoma patients harboring a BRAF exon 15 p.V600E point mutation [137]. Overall, patients treated with vemurafenib experienced a significant improvement in PFS, treatment response, and OS rates compared with chemotherapy-treated patients, with a tolerable profile of toxicity [137]. Likewise, in an extended follow-up analysis on the overall population of the BRIM-3 clinical trial, the authors confirmed the efficacy of vemurafenib on OS rates in advanced-stage previously untreated melanoma patients harboring BRAF exon 15 p.V600E or other less common exon 15 p.V600 point mutations compared with dacarbazine [138]. In another phase III, randomized, controlled clinical trial, in which the efficacy of dacarbazine was compared with the BRAF inhibitor dabrafenib, similar results were obtained in terms of PFS and OS in advanced-stage previously untreated melanoma patients harboring BRAF exon 15 p.V600 point mutations (p.V600E and p.V600K) [139,140].
As for lung cancer, several combination therapies have been investigated. One approach entails the combination of the BRAF inhibitor dabrafenib with the MEK inhibitor trametinib. In advanced-stage previously untreated melanoma patients harboring BRAF exon 15 p.V600 point mutations (p.V600E and p.V600K), such a combination significantly improved PFS (11.0 versus 8.8 months, respectively), OS (25.1 versus 18.7 months, respectively), and overall response rates (69.0% versus 53.0%, respectively) compared with dabrafenib alone [141,142,143,144]. Similar results have been reported for the association of BRAF inhibitor dabrafenib with the MEK inhibitor trametinib with respect to the BRAF inhibitor vemurafenib alone in terms of PFS (11.4 versus 7.3 months, respectively), objective response rate (ORR; 64.0% versus 51.0%, respectively) and 12-month OS (72.0% versus 65.0%) [145]. Another combination approach, adopted in the coBRIM clinical trial, involved the administration of the BRAF inhibitor vemurafenib and the MEK inhibitor cobimetinib [146]. Even in this case, the combination of the two drugs significantly improved OS and PFS rates in previously untreated advanced-stage BRAF exon 15 p.V600-mutated melanoma patients treated with the combination therapy compared with vemurafenib plus placebo (control group) [146]. Remarkably, no significant high-grade (3 or higher) adverse events were reported in the combination group [146]. Another valid combination approach is represented by the association of BRAF inhibitor encorafenib and MEK inhibitor binimetinib. In the COLUMBUS phase III clinical trial, previously treated or untreated advanced-stage melanoma patients harboring BRAF exon 15 p.V600E or p.V600K point mutations were randomly assigned to receive the combination regimen or single BRAF inhibitor therapies (vemurafenib or encorafenib). Overall, the combination strategy demonstrated, with respect to encorafenib or vemurafenib administration alone, a higher PFS (14.8 versus 9.2 versus 7.3 months, respectively), overall response rate (63.0% versus 51.0% versus 40.0%, respectively) and DOR (18.6 versus 15.2 versus 12.3 months, respectively) [147]. Interestingly, the association of BRAF and MEK inhibitors demonstrated a higher PFS (8 versus 3.7 months, respectively) and OS (17.3 versus 7.3 months, respectively) with respect to BRAF inhibitors alone in patients harboring rare BRAF non-p.V600 point mutations [148].
Still, another approach in BRAF-mutated advanced-stage melanoma patients is a combination of TKIs and immunotherapies. In murine models, in fact, TKIs favor immunotherapy activity by increasing tumor-infiltrating lymphocytes [149]. Nevertheless, severe toxicities have been reported for the association of ipilimumab (an anti-Cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) monoclonal antibody) and TKIs [150,151].
Promising results and manageable toxicities have been observed with concurrent administration of three agents: (1) durvalumab (anti-Programmed Death-Ligand 1 (PD-L1)) or pembrolizumab (anti-PD-1) plus dabrafenib plus trametinib [35]; (2) atezolizumab (anti-PD-L1) plus cobimetinib (MEK inhibitor) plus vemurafenib (BRAF inhibitor) [152]. Based on the results of the phase-III clinical trial IMspire 150, the FDA approved the use of the latter triple combination [153,154] for advanced-stage melanoma patients harboring BRAF exon 15 p.V600 point mutations. Conversely, the COMBI-I phase III clinical trial did not meet the primary end-point (PFS). In this study, the association of the anti-PD-1 spartalizumab plus dabrafenib plus trametinib did not significantly increase the PFS with respect to the association of dabrafenib plus trametinib [155].
3.3. Other Lesions
The efficacy of the combination strategy with debrafenib (BRAF inhibitor) and trametinib (MEK inhibitor) was strongly demonstrated in NCI-MATCH Trial Subprotocol H. Overall, in this study, which enrolled patients with different cancer types harboring BRAF exon 15 p.V600 mutations, an ORR of 38% was reached [156].
Regarding thyroid cancers, radioiodine treatment represents an adjuvant approach for early-stage patients undergoing thyroidectomy, and it is the most important therapeutic choice for advanced-stage patients [157]. However, as previously reported, BRAF exon 15 p.V600E-mutated thyroid carcinomas are resistant to the radioiodine treatment approach [83]. Nevertheless, these patients may benefit from targeted treatments. More recently, the efficacy of BRAF inhibitors vemurafenib for advanced-stage BRAF exon 15 p.V600E-mutated thyroid cancer patients refractory to radioiodine treatment [158] and dabrafenib for BRAF exon 15 p.V600E-mutated metastatic PTC patients has been demonstrated [159]. However, despite FDA approval, the European Medicines Agency (EMA) did not extend the use of vemurafenib and dabrafenib for the treatment of thyroid cancer patients due to the unfavorable toxicity profile [160]. Conversely, the combination of the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib showed promising results and tolerability in BRAF exon 15 p.V600E-mutated unresectable or metastatic anaplastic thyroid carcinoma patients and obtained FDA approval [161]. In fact, Subbiah et al. reported, in these patients without any other available treatment choice, an overall response rate of 69% demonstrates a meaningful therapeutic advance for this previously untreatable disease [162].
The combination strategy approach seemed to be more effective in CRC patients harboring a BRAF exon 15 p.V600E point mutation with respect to single-agent regimens. In the BEACON CRC phase III clinical trial, metastatic CRC patients harboring a BRAF exon 15 p.V600E point mutation, with disease progression after one or two previous treatment regimens, were randomized to receive encorafenib (BRAF inhibitor), binimetinib (MEK inhibitor), and cetuximab (anti-EGFR) or encorafenib and cetuximab, or other treatment approaches, including cetuximab and irinotecan or cetuximab and FOLFIRI (folinic acid, fluorouracil, and irinotecan). Overall, the median OS was 9.0, 8.4, and 5.4 months, respectively. Noteworthy, median PFS was higher in the triple-combination group (4.3 months) and in the association of encorafenib and cetuximab group (4.2 months) with respect to the other group (1.5 months). Similar promising results were reported for ORR (26.0%, 20.0%, and 2.0%, respectively). These data demonstrated the clinical efficacy of the combination strategy (encorafenib, binimetinib, and cetuximab) in previously treated metastatic CRC patients harboring a BRAF exon 15 p.V600E point mutation [163].
The combination strategy, with the BRAF inhibitor dabrafenib plus MEK inhibitor trametinib, demonstrated promising efficacy in patients with recurrent or refractory BRAF exon 15 p.V600E-mutated high-grade and low-grade gliomas. Overall, ORRs of 27.0% and 56.0% were reached [164].
4. Conclusions
BRAF mutations are reported in about 7% of solid tumors, with a high prevalence in PTC, melanoma, colorectal cancer, and lung cancer [20,22,23,24,25,26,27]. Located at codon 600 of exon 15, most of these mutations result in an amino acid substitution of valine to glutamic acid (p.V600E) [20]. Overall, about 200 BRAF mutant variants have been described in human tumors [28]. Like the two-faced mythological deity Janus, BRAF mutations are double-faceted, having both a prognostic and a predictive role. In fact, although BRAF mutations are typically associated with a negative prognostic role especially in, lung cancer, melanoma, thyroid, and CRC, their positive predictive role has recently emerged in melanoma, lung cancer, thyroid carcinoma, CRC, and other cancers, such as glioma patients. For this reason, implementing BRAF mutational analysis, alongside other clinically relevant gene alterations, is pivotal in selecting patients for targeted treatments. Noticeably, our research team at the Predictive Molecular Laboratory (Department of Public Health, University of Naples Federico II, Naples, Italy) has designed, developed, and validated a narrow NGS custom panel, named SiRe®, that is able to cover 568 mutations in six genes of clinical interest involved in four solid tumors: NSCLCs, CRCs, melanomas, and gastrointestinal stromal tumors. The six genes of interest include BRAF, EGFR, KRAS, NRAS, KIT, and PDGFRA. Moreover, we subsequently made this analysis even more efficient by optimizing the workflow so as to enable sequencing in both tissue and liquid biopsy specimens [26,165,166,167,168,169,170,171]. Alternatively, researchers in our lab and in other groups have also proposed more rapid diagnosis by adopting automated real-time polymerase chain reaction (RT-PCR) technologies [172,173,174,175]. Taking a further step, we have recently demonstrated the possibility of genotyping BRAF mutation directly from thyroid fine-needle aspiration (FNA) rinses to enable interventional cytopathologists to perform rapid molecular on-site evaluation (ROME) [172].
In conclusion, this literature review has highlighted the Janus-faced nature of BRAF mutations. Indeed, besides its well-documented prognostic role, BRAF mutations are emerging as crucial predictive markers in personalized cancer therapy. The relevance of BRAF as a new predictive marker lies in the fact that cancer patients harboring this mutation show poor response rates to conventional therapies. Therefore, correct identification of BRAF mutations, together with other types of aberrant molecular markers, is key to selecting patients for target treatments. Notably, as opposed to standard chemotherapy, a non-negligible percentage of BRAF-mutated cancer patients are benefitting from BRAF and/or MEK inhibitors and/or immunotherapy (anti-CTLA-4, -PD-1, -PD-L1) in terms of OS and tolerable toxicity. However, the efficacy, as well as safety profiles, of these treatments may vary among the different subsets of mutant BRAF tumors. For this reason, we adamantly support the application of molecular predictive laboratory devices that are able to cover at least BRAF exon 15 p.V600 clinically relevant mutations.
Author Contributions
Conceptualization, P.P., U.M., and G.T.; methodology, all authors; software, all authors; validation, all authors; formal analysis, all authors; investigation, all authors; resources, all authors; data curation, all authors; writing—original draft preparation, P.P., U.M., and G.T.; writing—review and editing, all authors; visualization, all authors; supervision, U.M. and G.T.; project administration, U.M. and G.T. All authors have read and agreed to the published version of the manuscript.
Funding
The authors have not received a specific grant for this review from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgments
We thank Paola Merolla for editing the manuscript.
Conflicts of Interest
Umberto Malapelle reports personal fees (as speaker bureau or advisor) from Boehringer Ingelheim, AstraZeneca, Roche, MSD, Amgen, and Merck, unrelated to the current work. Giancarlo Troncone reports personal fees (as speaker bureau or advisor) from Roche, MSD, Pfizer, and Bayer, unrelated to the current work. The other authors have nothing to disclose.
References
- Matallanas, D.; Birtwistle, M.; Romano, D.; Zebisch, A.; Rauch, J.; Von Kriegsheim, A.; Kolch, W. Raf Family Kinases: Old Dogs Have Learned New Tricks. Genes Cancer 2011, 2, 232–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapp, U.R.; Goldsborough, M.D.; Mark, G.E.; Bonner, T.I.; Groffen, J.; Reynolds, F.H.; Stephenson, J.R. Structure and biological activity of v-raf, a unique oncogene transduced by a retrovirus. Proc. Natl. Acad. Sci. USA 1983, 80, 4218–4222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Liu, H.T. MAPK signal pathways in the regulation of cell proliferation in mammalian cells. Cell Res. 2002, 12, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Kyriakis, J.M.; App, H.; Zhang, X.-F.; Banerjee, P.; Brautigan, D.L.; Rapp, U.R.; Avruch, J. Raf-1 activates MAP kinase-kinase. Nat. Cell Biol. 1992, 358, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Dent, P.; Haser, W.; Haystead, T.A.; Vincent, L.A.; Roberts, T.M.; Sturgill, T.W. Activation of mitogen-activated protein kinase kinase by v-Raf in NIH 3T3 cells and in vitro. Science 1992, 257, 1404–1407. [Google Scholar] [CrossRef]
- Zhang, X.-F.; Settleman, J.; Kyriakis, J.; Takeuchi-Suzuki, E.; Elledge, S.J.; Marshall, M.S.; Bruder, J.T.; Rapp, U.R.; Avruch, J. Normal and oncogenic p21ras proteins bind to the amino-terminal regulatory domain of c-Raf-1. Nat. Cell Biol. 1993, 364, 308–313. [Google Scholar] [CrossRef]
- Warne, P.H.; Vician, P.R.; Downward, J. Direct interaction of Ras and the amino-terminal region of Raf-1 in vitro. Nat. Cell Biol. 1993, 364, 352–355. [Google Scholar] [CrossRef]
- Vojtek, A.B.; Hollenberg, S.M.; Cooper, J.A. Mammalian Ras interacts directly with the serine/threonine kinase raf. Cell 1993, 74, 205–214. [Google Scholar] [CrossRef]
- Van Aelst, L.; Barr, M.; Marcus, S.; Polverino, A.; Wigler, M. Complex formation between RAS and RAF and other protein kinases. Proc. Natl. Acad. Sci. USA 1993, 90, 6213–6217. [Google Scholar] [CrossRef] [Green Version]
- Moodie, S.A.; Willumsen, B.M.; Weber, M.J.; Wolfman, A. Complexes of Ras.GTP with Raf-1 and mitogen-activated protein kinase kinase. Science 1993, 260, 1658–1661. [Google Scholar] [CrossRef]
- Kim, E.K.; Choi, E.-J. Pathological roles of MAPK signaling pathways in human diseases. Biochim. Biophys. Acta Mol. Basis Dis. 2010, 1802, 396–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhillon, A.S.; Hagan, S.; Rath, O.; Kolch, W. MAP kinase signalling pathways in cancer. Oncogene 2007, 26, 3279–3290. [Google Scholar] [CrossRef] [Green Version]
- Wada, T.; Penninger, J.M. Mitogen-activated protein kinases in apoptosis regulation. Oncogene 2004, 23, 2838–2849. [Google Scholar] [CrossRef] [Green Version]
- Lu, N.; Malemud, C.J. Extracellular Signal-Regulated Kinase: A Regulator of Cell Growth, Inflammation, Chondrocyte and Bone Cell Receptor-Mediated Gene Expression. Int. J. Mol. Sci. 2019, 20, 3792. [Google Scholar] [CrossRef] [Green Version]
- Zou, J.; Lei, T.; Guo, P.; Yu, J.; Xu, Q.; Luo, Y.; Ke, R.; Huang, D. Mechanisms shaping the role of ERK1/2 in cellular senescence (Review). Mol. Med. Rep. 2019, 19, 759–770. [Google Scholar] [PubMed] [Green Version]
- Yaeger, R.; Corcoran, R.B. Targeting Alterations in the RAF–MEK Pathway. Cancer Discov. 2019, 9, 329–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, N.H.; Wu, X.; Frost, J.A. B-Raf and Raf-1 Are Regulated by Distinct Autoregulatory Mechanisms. J. Biol. Chem. 2005, 280, 16244–16253. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, A.S.; Meikle, S.; Yazici, Z.; Eulitz, M.; Kolch, W. Regulation of Raf-1 activation and signalling by dephosphorylation. EMBO J. 2002, 21, 64–71. [Google Scholar] [CrossRef]
- Chong, H.; Lee, J.; Guan, K. Positive and negative regulation of Raf kinase activity and function by phosphorylation. EMBO J. 2001, 20, 3716–3727. [Google Scholar] [CrossRef] [Green Version]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF gene in human cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef]
- Emuss, V.; Garnett, M.; Mason, C.; Marais, R.; Project, T.C.G. Mutations of C-RAF Are Rare in Human Cancer because C-RAF Has a Low Basal Kinase Activity Compared with B-RAF. Cancer Res. 2005, 65, 9719–9726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikiforov, Y.E.; Nikiforova, M.N. Molecular genetics and diagnosis of thyroid cancer. Nat. Rev. Endocrinol. 2011, 7, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Lopez-Beltran, A.; Massari, F.; MacLennan, G.T.; Montironi, R. Molecular testing for BRAF mutations to inform melanoma treatment decisions: A move toward precision medicine. Mod. Pathol. 2018, 31, 24–38. [Google Scholar] [CrossRef] [PubMed]
- Schirripa, M.; Biason, P.; Lonardi, S.; Pella, N.; Pino, M.S.; Urbano, F.; Antoniotti, C.; Cremolini, C.; Corallo, S.; Pietrantonio, F.; et al. Class 1, 2, and 3 BRAF-Mutated Metastatic Colorectal Cancer: A Detailed Clinical, Pathologic, and Molecular Characterization. Clin. Cancer Res. 2019, 25, 3954–3961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchetti, A.; Felicioni, L.; Malatesta, S.; Sciarrotta, M.G.; Guetti, L.; Chella, A.; Viola, P.; Pullara, C.; Mucilli, F.; Buttitta, F. Clinical Features and Outcome of Patients with Non–Small-Cell Lung Cancer Harboring BRAF Mutations. J. Clin. Oncol. 2011, 29, 3574–3579. [Google Scholar] [CrossRef]
- Pisapia, P.; Pepe, F.; Malapelle, U.; Troncone, G. BRAF Mutations in Lung Cancer. Acta Cytol. 2019, 63, 247–250. [Google Scholar] [CrossRef]
- Dhomen, N.; Marais, R. New insight into BRAF mutations in cancer. Curr. Opin. Genet. Dev. 2007, 17, 31–39. [Google Scholar] [CrossRef]
- Yao, Z.; Yaeger, R.; Rodrik-Outmezguine, V.S.; Tao, A.; Torres, N.M.; Chang, M.T.; Drosten, M.; Zhao, H.; Cecchi, F.; Hembrough, T.; et al. Tumours with class 3 BRAF mutants are sensitive to the inhibition of activated RAS. Nat. Cell Biol. 2017, 548, 234–238. [Google Scholar] [CrossRef]
- Bracht, J.W.P.; Karachaliou, N.; Bivona, T.G.; Lanman, R.B.; Faull, I.; Nagy, R.J.; Drozdowskyj, A.; Berenguer, J.; Fernandez-Bruno, M.; Molina-Vila, M.Á.; et al. BRAF Mutations Classes I, II, and III in NSCLC Patients Included in the SLLIP Trial: The Need for a New Pre-Clinical Treatment Rationale. Cancers 2019, 11, 1381. [Google Scholar] [CrossRef] [Green Version]
- Dankner, M.; Rose, A.A.N.; Rajkumar, S.; Siegel, P.M.; Watson, I.R. Classifying BRAF alterations in cancer: New rational therapeutic strategies for actionable mutations. Oncogene 2018, 37, 3183–3199. [Google Scholar] [CrossRef]
- Frisone, D.; Friedlaender, A.; Malapelle, U.; Banna, G.; Addeo, A. A BRAF new world. Crit. Rev. Oncol. Hematol. 2020, 152, 103008. [Google Scholar] [CrossRef] [PubMed]
- Mol*: Towards a Common Library and Tools for Web Moleculargraphics. Available online: https://diglib.eg.org/handle/10.2312/molva20181103 (accessed on 18 November 2020).
- Research Collaboratory for Structural Bioinformatics (RCSB) Protein Data Bank (PDB). Available online: https://www.rcsb.org/3d-view/4WO5/1 (accessed on 18 November 2020).
- Cohn, A.; Day, B.-M.; Abhyankar, S.; McKenna, E.; Riehl, T.; Puzanov, I. BRAFV600 mutations in solid tumors, other than metastatic melanoma and papillary thyroid cancer, or multiple myeloma: A screening study. OncoTargets Ther. 2017, 10, 965–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlick, A.C.; Fecher, L.; Ascierto, P.A.; Sullivan, R.J. Frontline Therapy for BRAF-Mutated Metastatic Melanoma: How Do You Choose, and Is There One Correct Answer? Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Anguera, G.; Majem, M. BRAF inhibitors in metastatic non-small cell lung cancer. J. Thorac. Dis. 2018, 10, 589–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, M.; Huang, L.-L.; Chen, J.-H.; Wu, J.; Xu, Q. The emerging treatment landscape of targeted therapy in non-small-cell lung cancer. Signal Transduct. Target. Ther. 2019, 4, 61. [Google Scholar] [CrossRef] [Green Version]
- Leonetti, A.; Facchinetti, F.; Rossi, G.; Minari, R.; Conti, A.; Friboulet, L.; Tiseo, M.; Planchard, D. BRAF in non-small cell lung cancer (NSCLC): Pickaxing another brick in the wall. Cancer Treat. Rev. 2018, 66, 82–94. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature 2014, 511, 543–550. [Google Scholar] [CrossRef]
- Imielinski, M.; Berger, A.H.; Hammerman, P.S.; Hernandez, B.; Pugh, T.J.; Hodis, E.; Cho, J.; Suh, J.; Capelletti, M.; Sivachenko, A.; et al. Mapping the Hallmarks of Lung Adenocarcinoma with Massively Parallel Sequencing. Cell 2012, 150, 1107–1120. [Google Scholar] [CrossRef] [Green Version]
- Cardarella, S.; Ogino, A.; Nishino, M.; Butaney, M.; Shen, J.; Lydon, C.; Yeap, B.Y.; Sholl, L.M.; Johnson, B.E.; Jänne, P.A. Clinical, Pathologic, and Biologic Features Associated with BRAF Mutations in Non-Small Cell Lung Cancer. Clin. Cancer Res. 2013, 19, 4532–4540. [Google Scholar] [CrossRef] [Green Version]
- Ding, X.; Zhang, Z.; Jiang, T.; Li, X.; Zhao, C.; Su, B.; Zhou, C. Clinicopathologic characteristics and outcomes of Chinese patients with non-small-cell lung cancer and BRAF mutation. Cancer Med. 2017, 6, 555–562. [Google Scholar] [CrossRef]
- Paik, P.K.; Arcila, M.E.; Fara, M.; Sima, C.S.; Miller, V.A.; Kris, M.G.; Ladanyi, M.; Riely, G.J. Clinical Characteristics of Patients with Lung Adenocarcinomas Harboring BRAF Mutations. J. Clin. Oncol. 2011, 29, 2046–2051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, C.; Andelkovic, V.; Ladwa, R.; Pavlakis, N.; Zhou, C.; Hirsch, F.; Richard, D.; O’Byrne, K. Targeting BRAF mutations in non-small cell lung cancer. Transl. Lung Cancer Res. 2019, 8, 1119–1124. [Google Scholar] [CrossRef] [PubMed]
- Salimian, K.J.; Fazeli, R.; Zheng, G.; Ettinger, D.; Maleki, Z. V600E BRAF versus Non-V600E BRAF Mutated Lung Adenocarcinomas: Cytomorphology, Histology, Coexistence of Other Driver Mutations and Patient Characteristics. Acta Cytol. 2018, 62, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Noeparast, A.; Teugels, E.; Giron, P.; Verschelden, G.; De Brakeleer, S.; DeCoster, L.; De Grève, J. Non-V600 BRAF mutations recurrently found in lung cancer predict sensitivity to the combination of Trametinib and Dabrafenib. Oncotarget 2017, 8, 60094–60108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Cancer Genome Atlas Research Network. Comprehensive genomic characterization of squamous cell lung cancers. Nature 2012, 489, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Brustugun, O.T.; Khattak, A.M.; Trømborg, A.K.; Beigi, M.; Beiske, K.; Lund-Iversen, M.; Helland, Å. BRAF-mutations in non-small cell lung cancer. Lung Cancer 2014, 84, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Schrock, A.B.; Li, S.D.; Frampton, G.M.; Suh, J.; Braun, E.; Mehra, R.; Buck, S.C.; Bufill, J.A.; Peled, N.; Karim, N.A.; et al. Pulmonary Sarcomatoid Carcinomas Commonly Harbor Either Potentially Targetable Genomic Alterations or High Tumor Mutational Burden as Observed by Comprehensive Genomic Profiling. J. Thorac. Oncol. 2017, 12, 932–942. [Google Scholar] [CrossRef] [Green Version]
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretić, L.; Kong, G.; Leenders, F.; Lu, X.; Fernández-Cuesta, L.; Bosco, G.; et al. Comprehensive genomic profiles of small cell lung cancer. Nat. Cell Biol. 2015, 524, 47–53. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.; Barlesi, F.; Lolkema, M.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: A report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Warth, A.; Penzel, R.; Lindenmaier, H.; Brandt, R.; Stenzinger, A.; Herpel, E.; Goeppert, B.; Thomas, M.; Herth, F.J.; Dienemann, H.; et al. EGFR, KRAS, BRAF and ALK gene alterations in lung adenocarcinomas: Patient outcome, interplay with morphology and immunophenotype. Eur. Respir. J. 2014, 43, 872–883. [Google Scholar] [CrossRef] [Green Version]
- Zheng, D.; Wang, R.; Pan, Y.; Zheng, S.; Zhang, Y.; Li, H.; Cheng, C.; Gong, R.; Li, Y.; Shen, X.; et al. Prevalence and Clinicopathological Characteristics of BRAF Mutations in Chinese Patients with Lung Adenocarcinoma. Ann. Surg. Oncol. 2015, 22, S1284–S1291. [Google Scholar] [CrossRef] [PubMed]
- Litvak, A.M.; Paik, P.K.; Woo, K.M.; Sima, C.S.; Hellmann, M.D.; Arcila, M.E.; Ladanyi, M.; Rudin, C.M.; Kris, M.G.; Riely, G.J. Clinical Characteristics and Course of 63 Patients with BRAF Mutant Lung Cancers. J. Thorac. Oncol. 2014, 9, 1669–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinno, T.; Tsuta, K.; Shiraishi, K.; Mizukami, T.; Suzuki, M.; Yoshida, A.; Suzuki, K.; Asamura, H.; Furuta, K.; Kohno, T.; et al. Clinicopathological features of nonsmall cell lung carcinomas with BRAF mutations. Ann. Oncol. 2014, 25, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Villaruz, L.C.; Socinski, M.A.; Abberbock, S.; Berry, L.D.; Johnson, B.E.; Kwiatkowski, D.J.; Iafrate, A.J.; Varella-Garcia, M.; Franklin, W.A.; Camidge, D.R.; et al. Clinicopathologic features and outcomes of patients with lung adenocarcinomas harboring BRAF mutations in the Lung Cancer Mutation Consortium. Cancer 2015, 121, 448–456. [Google Scholar] [CrossRef] [Green Version]
- Tissot, C.; Couraud, S.; Tanguy, R.; Bringuier, P.-P.; Girard, N.; Souquet, P.-J. Clinical characteristics and outcome of patients with lung cancer harboring BRAF mutations. Lung Cancer 2016, 91, 23–28. [Google Scholar] [CrossRef]
- Hayward, N.K.; Wilmott, J.S.; Waddell, N.; Johansson, P.A.; Field, M.A.; Nones, K.; Patch, A.-M.; Kakavand, H.; Alexandrov, L.B.; Burke, H.; et al. Whole-genome landscapes of major melanoma subtypes. Nat. Cell Biol. 2017, 545, 175–180. [Google Scholar] [CrossRef]
- Ihle, M.A.; Fassunke, J.; König, K.; Grünewald, I.; Schlaak, P.D.M.; Kreuzberg, N.; Tietze, L.; Schildhaus, H.-U.; Büttner, R.; Merkelbach-Bruse, S. Comparison of high resolution melting analysis, pyrosequencing, next generation sequencing and immunohistochemistry to conventional Sanger sequencing for the detection of p.V600E and non-p.V600E BRAFmutations. BMC Cancer 2014, 14, 13. [Google Scholar] [CrossRef] [Green Version]
- Bradish, J.R.; Cheng, L. Molecular pathology of malignant melanoma: Changing the clinical practice paradigm toward a personalized approach. Hum. Pathol. 2014, 45, 1315–1326. [Google Scholar] [CrossRef]
- Long, G.V.; Menzies, A.M.; Nagrial, A.M.; Haydu, L.E.; Hamilton, A.L.; Mann, G.J.; Hughes, T.M.; Thompson, J.F.; Scolyer, R.A.; Kefford, R.F. Prognostic and Clinicopathologic Associations of Oncogenic BRAF in Metastatic Melanoma. J. Clin. Oncol. 2011, 29, 1239–1246. [Google Scholar] [CrossRef]
- Ribas, A.; Flaherty, K.T. BRAF targeted therapy changes the treatment paradigm in melanoma. Nat. Rev. Clin. Oncol. 2011, 8, 426–433. [Google Scholar] [CrossRef]
- Hugdahl, E.; Kalvenes, M.B.; Puntervoll, H.E.; Ladstein, R.G.; Akslen, L.A. BRAF-V600E expression in primary nodular melanoma is associated with aggressive tumour features and reduced survival. Br. J. Cancer 2016, 114, 801–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frauchiger, A.L.; Mangana, J.; Rechsteiner, M.; Moch, H.; Seifert, B.; Braun, R.P.; Dummer, R.; Goldinger, S.M. Prognostic relevance of lactate dehydrogenase and serum S100 levels in stage IV melanoma with known BRAF mutation status. Br. J. Dermatol. 2016, 174, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Carlino, M.S.; Haydu, L.E.; Kakavand, H.; Menzies, A.M.; Hamilton, A.L.; Yu, B.; Ng, C.C.; Cooper, W.A.; Thompson, J.F.; Kefford, R.F.; et al. Correlation of BRAF and NRAS mutation status with outcome, site of distant metastasis and response to chemotherapy in metastatic melanoma. Br. J. Cancer 2014, 111, 292–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heppt, M.V.; Siepmann, T.; Engel, J.; Schubert-Fritschle, G.; Eckel, R.; Mirlach, L.; Kirchner, T.; Jung, A.; Gesierich, A.; Ruzicka, T.; et al. Prognostic significance of BRAF and NRAS mutations in melanoma: A German study from routine care. BMC Cancer 2017, 17, 536. [Google Scholar] [CrossRef] [PubMed]
- Ekedahl, H.; Cirenajwis, H.; Harbst, K.; Carneiro, A.; Nielsen, K.; Olsson, H.; Lundgren, L.; Ingvar, C.; Jönsson, G. The clinical significance of BRAF and NRAS mutations in a clinic-based metastatic melanoma cohort. Br. J. Dermatol. 2013, 169, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Moreau, S.; Saiag, P.; Aegerter, P.; Bosset, D.; Longvert, C.; Hélias-Rodzewicz, Z.; Marin, C.; Peschaud, F.; Chagnon, S.; Zimmermann, U.; et al. Prognostic Value of BRAF V600 Mutations in Melanoma Patients after Resection of Metastatic Lymph Nodes. Ann. Surg. Oncol. 2012, 19, 4314–4321. [Google Scholar] [CrossRef] [PubMed]
- Picard, M.; Pham, D.N.; D’Incan, M.; Mansard, S.; Dechelotte, P.; Pereira, B.; Mondie, J.M.; Barthelemy, I. Is BRAF a prognostic factor in stage III skin melanoma? A retrospective study of 72 patients after positive sentinel lymph node dissection. Br. J. Dermatol. 2014, 171, 108–114. [Google Scholar] [CrossRef]
- Barbour, A.P.; Tang, Y.H.; Armour, N.; Dutton-Register, K.; Krause, L.; Loffler, K.A.; Lambie, D.; Burmeister, B.; Thomas, J.; Smithers, B.M.; et al. BRAF mutation status is an independent prognostic factor for resected stage IIIB and IIIC melanoma: Implications for melanoma staging and adjuvant therapy. Eur. J. Cancer 2014, 50, 2668–2676. [Google Scholar] [CrossRef]
- Ny, L.; Hernberg, M.; Nyakas, M.; Koivunen, J.; Oddershede, L.; Yoon, M.; Wang, X.; Guyot, P.; Geisler, J. BRAF mutational status as a prognostic marker for survival in malignant melanoma: A systematic review and meta-analysis. Acta Oncol. 2020, 59, 833–844. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Lu, J.; Chen, G.; Ardekani, G.S.; Rotte, A.; Martinka, M.; Xu, X.; McElwee, K.J.; Zhang, G.; Zhou, Y. Stage-specific prognostic biomarkers in melanoma. Oncotarget 2015, 6, 4180–4189. [Google Scholar] [CrossRef] [Green Version]
- Nagore, E.; Requena, C.; Traves, V.; Guillén, C.; Hayward, N.K.; Whiteman, D.; Hacker, E. Prognostic value of BRAF mutations in localized cutaneous melanoma. J. Am. Acad. Dermatol. 2014, 70, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Xing, M. BRAF mutation in thyroid cancer. Endocr. Relat. Cancer 2005, 12, 245–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trovisco, V.; Soares, P.; Sobrinho-Simões, M. B-RAF mutations in the etiopathogenesis, diagnosis, and prognosis of thyroid carcinomas. Hum. Pathol. 2006, 37, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Adeniran, A.J.; Zhu, Z.; Gandhi, M.; Steward, D.L.; Fidler, J.P.; Giordano, T.J.; Biddinger, P.W.; Nikiforov, Y.E. Correlation between Genetic Alterations and Microscopic Features, Clinical Manifestations, and Prognostic Characteristics of Thyroid Papillary Carcinomas. Am. J. Surg. Pathol. 2006, 30, 216–222. [Google Scholar] [CrossRef]
- Elisei, R.; Ugolini, C.; Viola, D.; Lupi, C.; Biagini, A.; Giannini, R.; Romei, C.; Miccoli, P.; Pinchera, A.; Basolo, F. BRAF(V600E) mutation and outcome of patients with papillary thyroid carcinoma: A 15-year median follow-up study. J. Clin. Endocrinol. Metab. 2008, 93, 3943–3949. [Google Scholar] [CrossRef] [Green Version]
- Nikiforova, M.N.; Kimura, E.T.; Gandhi, M.; Biddinger, P.W.; Knauf, J.A.; Basolo, F.; Zhu, Z.; Giannini, R.; Salvatore, G.; Fusco, A.; et al. BRAF Mutations in Thyroid Tumors Are Restricted to Papillary Carcinomas and Anaplastic or Poorly Differentiated Carcinomas Arising from Papillary Carcinomas. J. Clin. Endocrinol. Metab. 2003, 88, 5399–5404. [Google Scholar] [CrossRef]
- Xing, M.; Vasko, V.; Tallini, G.; Larin, A.; Wu, G.; Udelsman, R.; Ringel, M.D.; Ladenson, P.W.; Sidransky, D. BRAF T1796A Transversion Mutation in Various Thyroid Neoplasms. J. Clin. Endocrinol. Metab. 2004, 89, 1365–1368. [Google Scholar] [CrossRef]
- Cohen, Y.; Rosenbaum, E.; Clark, U.P.; Zeiger, M.A.; Umbricht, C.; Tufano, R.P.; Sidransky, D.; Westra, W.H. Mutational analysis of BRAF in fine needle aspiration biopsies of the thyroid: A potential application for the preoperative assessment of thyroid nodules. Clin. Cancer Res. 2004, 10, 2761–2765. [Google Scholar] [CrossRef] [Green Version]
- Bellevicine, C.; Migliatico, I.; Sgariglia, R.; Bs, M.N.; Vigliar, E.; Pisapia, P.; Iaccarino, A.; Bruzzese, D.; Fonderico, F.; Salvatore, D.; et al. Evaluation of BRAF, RAS, RET/PTC, and PAX8/PPARg alterations in different Bethesda diagnostic categories: A multicentric prospective study on the validity of the 7-gene panel test in 1172 thyroid FNAs deriving from different hospitals in South Italy. Cancer Cytopathol. 2020, 128, 107–118. [Google Scholar] [CrossRef]
- Bellevicine, C.; Sgariglia, R.; Malapelle, U.; Vigliar, E.; Nacchio, M.; Ciancia, G.; Eszlinger, M.; Paschke, R.; Troncone, G. Young investigator challenge: Can the Ion AmpliSeq Cancer Hotspot Panel v2 be used for next-generation sequencing of thyroid FNA samples? Cancer Cytopathol. 2016, 124, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Xing, M.; Westra, W.H.; Tufano, R.P.; Cohen, Y.; Rosenbaum, E.; Rhoden, K.J.; Carson, K.A.; Vasko, V.; Larin, A.; Tallini, G.; et al. BRAF Mutation Predicts a Poorer Clinical Prognosis for Papillary Thyroid Cancer. J. Clin. Endocrinol. Metab. 2005, 90, 6373–6379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Lee, E.S.; Kim, Y.S. Clinicopathologic significance of BRAF V600E mutation in papillary carcinomas of the thyroid: A meta-analysis. Cancer 2007, 110, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Park, Y.J.; Lim, J.A.; Ahn, H.Y.; Lee, E.K.; Lee, Y.J.; Kim, K.W.; Hahn, S.K.; Youn, Y.K.; Kim, K.H.; et al. The association of the BRAF(V600E) mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer: A meta-analysis. Cancer 2012, 118, 1764–1773. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Weng, J.; Bauer, J.; Ranvier, G.; Clark, O.H.; Duh, Q.-Y.; Shibru, D.; Bastian, B.; Griffin, A. The Prevalence and Prognostic Value of BRAF Mutation in Thyroid Cancer. Ann. Surg. 2007, 246, 466–471. [Google Scholar] [CrossRef]
- Namba, H.; Nakashima, M.; Hayashi, T.; Hayashida, N.; Maeda, S.; Rogounovitch, T.I.; Ohtsuru, A.; Saenko, V.A.; Kanematsu, T.; Yamashita, S. Clinical implication of hot spot BRAF mutation, V599E, in papillary thyroid cancers. J. Clin. Endocrinol. Metab. 2003, 88, 4393–4397. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.H.; Kang, D.W.; Kim, S.H.; Seong, I.O.; Kang, D.Y. Mutations of the BRAF Gene in Papillary Thyroid Carcinoma in a Korean Population. Yonsei Med. J. 2004, 45, 818–821. [Google Scholar] [CrossRef] [Green Version]
- Rivera, M.; Ricarte-Filho, J.; Tuttle, R.M.; Ganly, I.; Shaha, A.; Knauf, J.; Fagin, J.; Ghossein, R. Molecular, Morphologic, and Outcome Analysis of Thyroid Carcinomas According to Degree of Extrathyroid Extension. Thyroid 2010, 20, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Shong, Y.K.; Kim, T.Y.; Viola, D.; Elisei, R.; Bendlová, B.; Yip, L.; Mian, C.; et al. Association between BRAF V600E mutation and recurrence of papillary thyroid cancer. J. Clin. Oncol. 2015, 33, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Elisei, R.; Viola, D.; Torregrossa, L.; Giannini, R.; Romei, C.; Ugolini, C.; Molinaro, E.; Agate, L.; Biagini, A.; Lupi, C.; et al. TheBRAFV600E Mutation Is an Independent, Poor Prognostic Factor for the Outcome of Patients with Low-Risk Intrathyroid Papillary Thyroid Carcinoma: Single-Institution Results from a Large Cohort Study. J. Clin. Endocrinol. Metab. 2012, 97, 4390–4398. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Chen, T.; Liu, Z. Associations between BRAFV600E and prognostic factors and poor outcomes in papillary thyroid carcinoma: A meta-analysis. World J. Surg. Oncol. 2016, 14, 241. [Google Scholar] [CrossRef] [Green Version]
- Xing, M. Molecular pathogenesis and mechanisms of thyroid cancer. Nat. Rev. Cancer 2013, 13, 184–199. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Liu, D.; Murugan, A.K.; Liu, Z.; Xing, M. Histone deacetylation of NIS promoter underlies BRAF V600E-promoted NIS silencing in thyroid cancer. Endocr. Relat. Cancer 2013, 21, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Oler, G.; Cerutti, J.M. High prevalence of BRAF mutation in a Brazilian cohort of patients with sporadic papillary thyroid carcinomas: Correlation with more aggressive phenotype and decreased expression of iodide-metabolizing genes. Cancer 2009, 115, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Garcia, E.; Argiles, G.; Elez, E.; Tabernero, J. BRAF mutant colorectal cancer: Prognosis, treatment, and new perspectives. Ann. Oncol. 2017, 28, 2648–2657. [Google Scholar] [CrossRef] [PubMed]
- Malapelle, U.; Pisapia, P.; Sgariglia, R.; Vigliar, E.; Biglietto, M.; Carlomagno, C.; Giuffrè, G.; Bellevicine, C.; Troncone, G. Less frequently mutated genes in colorectal cancer: Evidences from next-generation sequencing of 653 routine cases. J. Clin. Pathol. 2016, 69, 767–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samowitz, W.S.; Sweeney, C.; Herrick, J.; Albertsen, H.; Levin, T.R.; Murtaugh, M.A.; Wolff, R.K.; Slattery, M.L. Poor survival associated with the BRAF V600E mutation in microsatellite-stable colon cancers. Cancer Res. 2005, 65, 6063–6069. [Google Scholar] [CrossRef] [Green Version]
- Gonsalves, W.I.; Mahoney, M.R.; Sargent, D.J.; Nelson, G.D.; Alberts, S.R.; Sinicrope, F.A.; Goldberg, R.M.; Limburg, P.J.; Thibodeau, S.N.; Grothey, A.; et al. Patient and Tumor Characteristics and BRAF and KRAS Mutations in Colon Cancer, NCCTG/Alliance N0147. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef]
- Clarke, C.N.; Kopetz, S. BRAF mutant colorectal cancer as a distinct subset of colorectal cancer: Clinical characteristics, clinical behavior, and response to targeted therapies. J. Gastrointest. Oncol. 2015, 6, 660–667. [Google Scholar]
- Jones, J.C.; Renfro, L.A.; Al-Shamsi, H.O.; Schrock, A.B.; Rankin, A.; Zhang, B.Y.; Kasi, P.M.; Voss, J.S.; Leal, A.D.; Sun, J.; et al. Non-V600BRAF Mutations Define a Clinically Distinct Molecular Subtype of Metastatic Colorectal Cancer. J. Clin. Oncol. 2017, 35, 2624–2630. [Google Scholar] [CrossRef]
- Guinney, J.; Dienstmann, R.; Wang, X.; De Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef]
- Missiaglia, E.; Jacobs, B.; D’Ario, G.; Di Narzo, A.; Soneson, C.; Budinska, E.; Popovici, V.; Vecchione, L.; Gerster, S.; Yan, P.; et al. Distal and proximal colon cancers differ in terms of molecular, pathological, and clinical features. Ann. Oncol. 2014, 25, 1995–2001. [Google Scholar] [CrossRef] [PubMed]
- Fariña-Sarasqueta, A.; Van Lijnschoten, G.; Moerland, E.; Creemers, G.-J.; Lemmens, V.E.P.P.; Rutten, H.J.T.; Brule, A.J.C.V.D. The BRAF V600E mutation is an independent prognostic factor for survival in stage II and stage III colon cancer patients. Ann. Oncol. 2010, 21, 2396–2402. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.D.; Tejpar, S.; Delorenzi, M.; Yan, P.; Fiocca, R.; Klingbiel, D.; Dietrich, D.; Biesmans, B.; Bodoky, G.; Barone, C.; et al. Prognostic Role of KRAS and BRAF in Stage II and III Resected Colon Cancer: Results of the Translational Study on the PETACC-3, EORTC 40993, SAKK 60-00 Trial. J. Clin. Oncol. 2010, 28, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Shima, K.; Meyerhardt, J.A.; McCleary, N.J.; Ng, K.; Hollis, D.; Saltz, L.B.; Mayer, R.J.; Schaefer, P.; Whittom, R.; et al. Predictive and prognostic roles of BRAF mutation in stage III colon cancer: Results from intergroup trial CALGB 89803. Clin. Cancer Res. 2012, 18, 890–900. [Google Scholar] [CrossRef] [Green Version]
- Richman, S.D.; Seymour, M.T.; Chambers, P.; Elliott, F.; Daly, C.L.; Meade, A.M.; Taylor, G.; Barrett, J.H.; Quirke, P. KRAS and BRAF mutations in advanced colorectal cancer are associated with poor prognosis but do not preclude benefit from oxaliplatin or irinotecan: Results from the MRC FOCUS trial. J. Clin. Oncol. 2009, 27, 5931–5937. [Google Scholar] [CrossRef]
- Venderbosch, S.; Nagtegaal, I.D.; Maughan, T.S.; Smith, C.G.; Cheadle, J.P.; Fisher, D.; Kaplan, R.; Quirke, P.; Seymour, M.T.; Richman, S.D.; et al. Mismatch Repair Status and BRAF Mutation Status in Metastatic Colorectal Cancer Patients: A Pooled Analysis of the CAIRO, CAIRO2, COIN, and FOCUS Studies. Clin. Cancer Res. 2014, 20, 5322–5330. [Google Scholar] [CrossRef] [Green Version]
- Seligmann, J.F.; Fisher, D.; Smith, C.G.; Richman, S.D.; Elliott, F.; Brown, S.; Adams, R.; Maughan, T.; Quirke, P.; Cheadle, J.; et al. Investigating the poor outcomes of BRAF-mutant advanced colorectal cancer: Analysis from 2530 patients in randomised clinical trials. Ann. Oncol. 2017, 28, 562–568. [Google Scholar] [CrossRef]
- Renaud, S.; Romain, B.; Falcoz, P.-E.; Olland, A.; Santelmo, N.; Brigand, C.; Rohr, S.; Guenot, D.; Massard, G. KRAS and BRAF mutations are prognostic biomarkers in patients undergoing lung metastasectomy of colorectal cancer. Br. J. Cancer 2015, 112, 720–728. [Google Scholar] [CrossRef] [Green Version]
- Schirripa, M.; Bergamo, F.; Cremolini, C.; Casagrande, M.; Lonardi, S.; Aprile, G.; Yang, D.; Marmorino, F.; Pasquini, G.; Sensi, E.; et al. BRAF and RAS mutations as prognostic factors in metastatic colorectal cancer patients undergoing liver resection. Br. J. Cancer 2015, 112, 1921–1928. [Google Scholar] [CrossRef] [Green Version]
- Yaeger, R.; Cercek, A.; Chou, J.F.; Sylvester, B.E.; Kemeny, N.E.; Hechtman, J.F.; Ladanyi, M.; Rosen, N.; Weiser, M.R.; Capanu, M.; et al. BRAF mutation predicts for poor outcomes after metastasectomy in patients with metastatic colorectal cancer. Cancer 2014, 120, 2316–2324. [Google Scholar] [CrossRef]
- Lassaletta, A.; Zapotocky, M.; Mistry, M.; Ramaswamy, V.; Honnorat, M.; Krishnatry, R.; Stucklin, A.G.; Zhukova, N.; Arnoldo, A.; Ryall, S.; et al. Therapeutic and Prognostic Implications of BRAF V600E in Pediatric Low-Grade Gliomas. J. Clin. Oncol. 2017, 35, 2934–2941. [Google Scholar] [CrossRef] [PubMed]
- Horbinski, C.; Nikiforova, M.N.; Hagenkord, J.M.; Hamilton, R.L.; Pollack, I.F. Interplay among BRAF, p16, p53, and MIB1 in pediatric low-grade gliomas. Neuro Oncol. 2012, 14, 777–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behling, F.; Schittenhelm, J. Oncogenic BRAF Alterations and Their Role in Brain Tumors. Cancers 2019, 11, 794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albanell, J.; Elvin, J.A.; Ali, S.M.; Schrock, A.B.; Chung, J.; Vergilio, J.-A.; Suh, J.; Ramkissoon, S.; Severson, E.A.; Daniel, S.; et al. BRAF: An emerging target for triple-negative breast cancer. J. Clin. Oncol. 2017, 35, 1099. [Google Scholar] [CrossRef]
- Grisham, R.N.; Iyer, G.; Garg, K.; Delair, D.; Hyman, D.M.; Zhou, Q.; Iasonos, A.; Berger, M.F.; Dao, F.; Spriggs, D.R.; et al. BRAF mutation is associated with early stage disease and improved outcome in patients with low-grade serous ovarian cancer. Cancer 2012, 119, 548–554. [Google Scholar] [CrossRef]
- Gautschi, O.; Pauli, C.; Strobel, K.; Hirschmann, A.; Printzen, G.; Aebi, S.; Diebold, J. A Patient with BRAF V600E Lung Adenocarcinoma Responding to Vemurafenib. J. Thorac. Oncol. 2012, 7, e23–e24. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.; Michielin, O.; Zimmermann, S. Dramatic Response Induced by Vemurafenib in a BRAF V600E-Mutated Lung Adenocarcinoma. J. Clin. Oncol. 2013, 31, e341–e344. [Google Scholar] [CrossRef]
- Robinson, S.D.; O’Shaughnessy, J.A.; Cowey, C.L.; Konduri, K. BRAF V600E-mutated lung adenocarcinoma with metastases to the brain responding to treatment with vemurafenib. Lung Cancer 2014, 85, 326–330. [Google Scholar] [CrossRef]
- Schmid, S.; Siano, M.; Joerger, M.; Rodriguez, R.; Müller, J.; Früh, M. Response to dabrafenib after progression on vemurafenib in a patient with advanced BRAF V600E-mutant bronchial adenocarcinoma. Lung Cancer 2015, 87, 85–87. [Google Scholar] [CrossRef]
- Mazieres, J.; Cropet, C.; Montané, L.; Barlesi, F.; Souquet, P.; Quantin, X.; Dubos-Arvis, C.; Otto, J.; Favier, L.; Avrillon, V.; et al. Vemurafenib in non-small-cell lung cancer patients with BRAFV600 and BRAFnonV600 mutations. Ann. Oncol. 2020, 31, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Hyman, D.M.; Puzanov, I.; Subbiah, V.; Faris, J.E.; Chau, I.; Blay, J.Y.; Wolf, J.; Raje, N.S.; Diamond, E.L.; Hollebecque, A.; et al. Vemurafenib in Multiple Nonmelanoma Cancers with BRAF V600 Mutations. N. Engl. J. Med. 2015, 373, 726–736. [Google Scholar] [CrossRef]
- Subbiah, V.; Gervais, R.; Riely, G.; Hollebecque, A.; Blay, J.Y.; Felip, E.; Schuler, M.; Gonçalves, A.; Italiano, A.; Keedy, V.; et al. Efficacy of Vemurafenib in Patients with Non-Small-Cell Lung Cancer with BRAF V600 Mutation: An Open-Label, Single-Arm Cohort of the Histology-Independent VE-BASKET Study. JCO Precis. Oncol. 2019, 3. [Google Scholar] [CrossRef]
- Falchook, G.S.; Long, G.V.; Kurzrock, R.; Kim, K.B.; Arkenau, T.H.; Brown, M.P.; Hamid, O.; Infante, J.R.; Millward, M.; Pavlick, A.C.; et al. Dabrafenib in patients with melanoma, untreated brain metastases, and other solid tumours: A phase 1 dose-escalation trial. Lancet 2012, 379, 1893–1901. [Google Scholar] [CrossRef] [Green Version]
- Gautschi, O.; Milia, J.; Cabarrou, B.; Bluthgen, M.V.; Besse, B.; Smit, E.F.; Wolf, J.; Peters, S.; Früh, M.; Koeberle, D.; et al. Targeted Therapy for Patients with BRAF-Mutant Lung Cancer: Results from the European EURAF Cohort. J. Thorac. Oncol. 2015, 10, 1451–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planchard, D.; Kim, T.M.; Mazieres, J.; Quoix, E.; Riely, G.; Barlesi, F.; Souquet, P.J.; Smit, E.F.; Groen, H.J.; Kelly, R.J.; et al. Dabrafenib in patients with BRAF(V600E)-positive advanced non-small-cell lung cancer: A single-arm, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 642–650. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Besse, B.; Groen, H.J.M.; Souquet, P.J.; Quoix, E.; Baik, C.S.; Barlesi, F.; Kim, T.M.; Mazieres, J.; Novello, S.; et al. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: An open-label, multicentre phase 2 trial. Lancet Oncol. 2016, 17, 984–993. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M., Jr.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: An open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Approved Drugs—FDA Grants Regular Approval to Dabrafenib and Trametinib Combination for Metastatic NSCLC with BRAF V600E Mutation. 2017. Available online: https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm564331.htm (accessed on 18 November 2020).
- Trametinib in Combination with Dabrafenib Is Indicated for the Treatment of Adult Patients with Advanced Non-Small Cell Lung Cancer with a BRAF V600 Mutation. 2017. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Summary_of_opinion/human/002643/WC500222159.pdf (accessed on 18 November 2020).
- Sereno, M.; Moreno, V.; Moreno, R.J.; Gómez-Raposo, C.; García, S.S.; Hernández, J.R.; Falagan, S.; Zambrana, T.F.; Casado, S.E. A significant response to sorafenib in a woman with advanced lung adenocarcinoma and a BRAF non-V600 mutation. Anticancer Drugs 2015, 26, 1004–1007. [Google Scholar] [CrossRef]
- Gardini, A.C.; Chiadini, E.; Faloppi, L.; Marisi, G.; Delmonte, A.; Scartozzi, M.; Loretelli, C.; Lucchesi, A.; Oboldi, D.; Dubini, A.; et al. Efficacy of sorafenib in BRAF-mutated non-small-cell lung cancer (NSCLC) and no response in synchronous BRAF wild type-hepatocellular carcinoma: A case report. BMC Cancer 2016, 16, 429. [Google Scholar] [CrossRef]
- Sullivan, R.J.; Infante, J.R.; Janku, F.; Wong, D.J.L.; Sosman, J.A.; Keedy, V.; Patel, M.R.; Shapiro, G.I.; Mier, J.W.; Tolcher, A.W.; et al. First-in-Class ERK1/2 Inhibitor Ulixertinib (BVD-523) in Patients with MAPK Mutant Advanced Solid Tumors: Results of a Phase I Dose-Escalation and Expansion Study. Cancer Discov. 2018, 8, 184–195. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, R.J.; Hollebecque, A.; Flaherty, K.T.; Shapiro, G.I.; Rodon Ahnert, J.; Millward, M.J.; Zhang, W.; Gao, L.; Sykes, A.; Willard, M.D.; et al. A Phase I Study of LY3009120, a Pan-RAF Inhibitor, in Patients with Advanced or Metastatic Cancer. Mol. Cancer Ther. 2020, 19, 460–467. [Google Scholar] [CrossRef] [Green Version]
- Luther, C.; Swami, U.; Zhang, J.; Milhem, M.; Zakharia, Y. Advanced stage melanoma therapies: Detailing the present and exploring the future. Crit. Rev. Oncol. 2019, 133, 99–111. [Google Scholar] [CrossRef]
- Chapman, P.B.; Hauschild, A.; Robert, C.; Haanen, J.B.; Ascierto, P.; Larkin, J.; Dummer, R.; Garbe, C.; Testori, A.; Maio, M.; et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N. Engl. J. Med. 2011, 364, 2507–2516. [Google Scholar] [CrossRef] [Green Version]
- McArthur, G.A.; Chapman, P.B.; Robert, C.; Larkin, J.; Haanen, J.B.; Dummer, R.; Ribas, A.; Hogg, D.; Hamid, O.; Ascierto, P.A.; et al. Safety and efficacy of vemurafenib in BRAF(V600E) and BRAF(V600K) mutation-positive melanoma (BRIM-3): Extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol. 2014, 15, 323–332. [Google Scholar] [CrossRef] [Green Version]
- Hauschild, A.; Grob, J.-J.; Demidov, L.V.; Jouary, T.; Gutzmer, R.; Millward, M.; Rutkowski, P.; Blank, C.U.; Miller, W.H.; Kaempgen, E.; et al. Dabrafenib in BRAF-mutated metastatic melanoma: A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2012, 380, 358–365. [Google Scholar] [CrossRef]
- Hauschild, A.; Ascierto, P.A.; Schadendorf, D.; Grob, J.-J.; Ribas, A.; Kiecker, F.; Dutriaux, C.; Demidov, L.V.; Lebbé, C.; Rutkowski, P.; et al. Long-term outcomes in patients with BRAF V600-mutant metastatic melanoma receiving dabrafenib monotherapy: Analysis from phase 2 and 3 clinical trials. Eur. J. Cancer 2020, 125, 114–120. [Google Scholar] [CrossRef]
- Long, G.V.; Weber, J.S.; Infante, J.R.; Kim, K.B.; Daud, A.; Gonzalez, R.; Sosman, J.A.; Hamid, O.; Schuchter, L.; Cebon, J.; et al. Overall Survival and Durable Responses in Patients with BRAF V600-Mutant Metastatic Melanoma Receiving Dabrafenib Combined With Trametinib. J. Clin. Oncol. 2016, 34, 871–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, G.V.; Flaherty, K.T.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; De Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; et al. Dabrafenib plus trametinib versus dabrafenib monotherapy in patients with metastatic BRAF V600E/K-mutant melanoma: Long-term survival and safety analysis of a phase 3 study. Ann. Oncol. 2017, 28, 1631–1639. [Google Scholar] [CrossRef]
- Long, G.V.; Eroglu, Z.; Infante, J.; Patel, S.; Daud, A.; Johnson, D.B.; Gonzalez, R.; Kefford, R.; Hamid, O.; Schuchter, L.; et al. Long-Term Outcomes in Patients with BRAF V600–Mutant Metastatic Melanoma Who Received Dabrafenib Combined with Trametinib. J. Clin. Oncol. 2018, 36, 667–673. [Google Scholar] [CrossRef]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; De Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.J.; et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N. Engl. J. Med. 2014, 371, 1877–1888. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved Overall Survival in Melanoma with Combined Dabrafenib and Trametinib. N. Engl. J. Med. 2015, 372, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Larkin, J.; Ascierto, P.A.; Dréno, B.; Atkinson, V.; Liszkay, G.; Maio, M.; Mandalà, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Combined Vemurafenib and Cobimetinib in BRAF-Mutated Melanoma. N. Engl. J. Med. 2014, 371, 1867–1876. [Google Scholar] [CrossRef] [Green Version]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2018, 19, 603–615. [Google Scholar] [CrossRef] [Green Version]
- Menzer, C.; Menzies, A.M.; Carlino, M.S.; Reijers, I.; Groen, E.J.; Eigentler, T.; De Groot, J.W.B.; Van Der Veldt, A.A.; Johnson, D.B.; Meiss, F.; et al. Targeted Therapy in Advanced Melanoma with Rare BRAF Mutations. J. Clin. Oncol. 2019, 37, 3142–3151. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Peng, W.; Xu, C.; Lou, Y.; Zhang, M.; Wargo, J.A.; Chen, J.Q.; Li, H.S.; Watowich, S.S.; Yang, Y.; et al. BRAF Inhibition Increases Tumor Infiltration by T cells and Enhances the Antitumor Activity of Adoptive Immunotherapy in Mice. Clin. Cancer Res. 2013, 19, 393–403. [Google Scholar] [CrossRef] [Green Version]
- Ribas, A.; Hodi, F.S.; Callahan, M.; Konto, C.; Wolchok, J. Hepatotoxicity with Combination of Vemurafenib and Ipilimumab. N. Engl. J. Med. 2013, 368, 1365–1366. [Google Scholar] [CrossRef] [PubMed]
- Minor, D.R.; Puzanov, I.; Callahan, M.K.; Hug, B.A.; Hoos, A. Severe gastrointestinal toxicity with administration of trametinib in combination with dabrafenib and ipilimumab. Pigment. Cell Melanoma Res. 2015, 28, 611–612. [Google Scholar] [CrossRef]
- Sullivan, R.J.; Hamid, O.; Gonzalez, R.; Infante, J.R.; Patel, M.R.; Hodi, F.S.; Lewis, K.D.; Tawbi, H.A.; Hernandez, G.; Wongchenko, M.J.; et al. Atezolizumab plus cobimetinib and vemurafenib in BRAF-mutated melanoma patients. Nat. Med. 2019, 25, 929–935. [Google Scholar] [CrossRef]
- Gutzmer, R.; Stroyakovskiy, D.; Gogas, H.; Robert, C.; Lewis, K.; Protsenko, S.; Pereira, R.P.; Eigentler, T.; Rutkowski, P.; Demidov, L.; et al. Atezolizumab, vemurafenib, and cobimetinib as first-line treatment for unresectable advanced BRAFV600 mutation-positive melanoma (IMspire150): Primary analysis of the randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2020, 395, 1835–1844. [Google Scholar] [CrossRef]
- FDA Approves Genentech’s Tecentriq Plus Cotellic Zelboraf for People with Advanced Melanoma. Available online: Gene.com/media/press-releases/14868/2020-07-30/fda-approves-genentechs-tecentriq-plus-c (accessed on 18 November 2020).
- Nathan, P.; Dummer, R.; Long, G.V.; Ascierto, P.A.; Tawbi, H.A.; Robert, C.; Rutkowski, P.; Leonov, O.; Dutriaux, C.; Mandala, M.; et al. LBA43—Spartalizumab plus dabrafenib and trametinib (Sparta-DabTram) in patients (pts) with previously untreated BRAF V600–mutant unresectable or metastatic melanoma: Results from the randomized part 3 of the phase III COMBI-i trial. Ann. Oncol. 2020, 31, S1142–S1215. [Google Scholar] [CrossRef]
- Salama, A.K.S.; Li, S.; Macrae, E.R.; Park, J.-I.; Mitchell, E.P.; Zwiebel, J.A.; Chen, H.X.; Gray, R.J.; McShane, L.M.; Rubinstein, L.V.; et al. Dabrafenib and Trametinib in Patients with Tumors with BRAFV600E Mutations: Results of the NCI-MATCH Trial Subprotocol H. J. Clin. Oncol. 2020, 38, 3895–3904. [Google Scholar] [CrossRef]
- Cabanillas, M.E.; Patel, A.; Danysh, B.P.; Dadu, R.; Kopetz, S.; Falchook, G. BRAF Inhibitors: Experience in Thyroid Cancer and General Review of Toxicity. Horm. Cancer 2015, 6, 21–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brose, M.S.; Cabanillas, M.E.; Cohen, E.E.; Wirth, L.J.; Riehl, T.; Yue, H.; Sherman, S.I.; Sherman, E.J. Vemurafenib in patients with BRAF(V600E)-positive metastatic or unresectable papillary thyroid cancer refractory to radioactive iodine: A non-randomised, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Falchook, G.S.; Millward, M.; Hong, D.; Naing, A.; Piha-Paul, S.; Waguespack, S.G.; Cabanillas, M.E.; Sherman, S.I.; Martin, C.; Curtis, M.; et al. BRAF Inhibitor Dabrafenib in Patients with Metastatic BRAF-Mutant Thyroid Cancer. Thyroid 2015, 25, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crispo, F.; Notarangelo, T.; Pietrafesa, M.; Lettini, G.; Storto, G.; Sgambato, A.; Maddalena, F.; Landriscina, M. BRAF Inhibitors in Thyroid Cancer: Clinical Impact, Mechanisms of Resistance and Future Perspectives. Cancers 2019, 11, 1388. [Google Scholar] [CrossRef] [Green Version]
- FDA Approves Dabrafenib Plus Trametinib for Anaplastic Thyroid Cancer with BRAF V600E Mutation. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-dabrafenib-plus-trametinib-anaplastic-thyroid-cancer-braf-v600e-mutation (accessed on 18 November 2020).
- Subbiah, V.; Kreitman, R.J.; Wainberg, Z.A.; Cho, J.Y.; Schellens, J.H.; Soria, J.C.; Wen, P.Y.; Zielinski, C.; Cabanillas, M.E.; Urbanowitz, G.; et al. Dabrafenib and Trametinib Treatment in Patients with Locally Advanced or Metastatic BRAF V600–Mutant Anaplastic Thyroid Cancer. J. Clin. Oncol. 2018, 36, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Roviello, G.; D’Angelo, A.; Petrioli, R.; Roviello, F.; Cianchi, F.; Nobili, S.; Mini, E.; Lavacchi, D. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. Transl. Oncol. 2020, 13, 100795. [Google Scholar] [CrossRef]
- Wen, P.; Stein, A.; Bent, M.V.D.; De Greve, J.; Dietrich, S.; De Vos, F.; Von Bubnoff, N.; Van Linde, M.; Lai, A.; Prager, G.; et al. Actr-30. Updated efficacy and safety of dabrafenib plus trametinib in patients with recurrent/refractory BRAF V600e–mutated high-grade glioma (hgg) and low-grade glioma (lgg). Neuro Oncol. 2019, 21, vi19–vi20. [Google Scholar] [CrossRef]
- Pepe, F.; De Luca, C.; Smeraglio, R.; Pisapia, P.; Sgariglia, R.; Nacchio, M.; Russo, M.; Serra, N.; Rocco, D.; Battiloro, C.; et al. Performance analysis of SiRe next-generation sequencing panel in diagnostic setting: Focus on NSCLC routine samples. J. Clin. Pathol. 2019, 72, 38–45. [Google Scholar] [CrossRef]
- Pisapia, P.; Pepe, F.; Smeraglio, R.; Russo, M.; Rocco, D.; Sgariglia, R.; Nacchio, M.; De Luca, C.; Vigliar, E.; Bellevicine, C.; et al. Cell free DNA analysis by SiRe® next generation sequencing panel in non small cell lung cancer patients: Focus on basal setting. J. Thorac. Dis. 2017, 9, S1383–S1390. [Google Scholar] [CrossRef] [Green Version]
- Nacchio, M.; Sgariglia, R.; Gristina, V.; Pisapia, P.; Pepe, F.; De Luca, C.; Migliatico, I.; Clery, E.; Greco, L.; Vigliar, E.; et al. KRAS mutations testing in non-small cell lung cancer: The role of Liquid biopsy in the basal setting. J. Thorac. Dis. 2020, 12, 3836–3843. [Google Scholar] [CrossRef]
- Malapelle, U.; Mayo, D.L.C.C.; Rocco, D.; Garzon, M.; Pisapia, P.; Jordana-Ariza, N.; Russo, M.; Sgariglia, R.; De Luca, C.; Pepe, F.; et al. Development of a gene panel for next-generation sequencing of clinically relevant mutations in cell-free DNA from cancer patients. Br. J. Cancer 2017, 116, 802–810. [Google Scholar] [CrossRef] [Green Version]
- Pisapia, P.; Malapelle, U.; Roma, G.; Saddar, S.; Zheng, Q.; Pepe, F.; Bruzzese, D.; Vigliar, E.; Bellevicine, C.; Luthra, R.; et al. Consistency and reproducibility of next-generation sequencing in cytopathology: A second worldwide ring trial study on improved cytological molecular reference specimens. Cancer Cytopathol. 2019, 127, 285–296. [Google Scholar] [CrossRef]
- Malapelle, U.; Mayo, D.L.C.C.; Molina-Vila, M.A.; Rosell, R.; Savic, S.; Bihl, M.; Bubendorf, L.; Salto-Tellez, M.; De Biase, D.; Tallini, G.; et al. Consistency and reproducibility of next-generation sequencing and other multigene mutational assays: A worldwide ring trial study on quantitative cytological molecular reference specimens. Cancer Cytopathol. 2017, 125, 615–626. [Google Scholar] [CrossRef]
- Pisapia, P.; Rocco, D.; Pepe, F.; De Luca, C.; Battiloro, C.; Smeraglio, R.; Cieri, M.; Bellevicine, C.; Troncone, G.; Malapelle, U. EGFR exon 19 deletion switch and development of p.L792Q mutation as a new resistance mechanism to osimertinib: A case report and literature review. Transl. Cancer Res. 2018, 8, S64–S69. [Google Scholar] [CrossRef]
- De Luca, C.; Sgariglia, R.; Nacchio, M.; Pisapia, P.; Migliatico, I.; Clery, E.; Gragnano, G.; Campione, S.; Vigliar, E.; Malapelle, U.; et al. Rapid on-site Molecular Evaluation in thyroid cytopathology: A same-day cytological and molecular diagnosis. Diagn. Cytopathol. 2020, 48, 300–307. [Google Scholar] [CrossRef]
- Prieto-Potin, I.; Montagut, C.; Bellosillo, B.; Evans, M.; Smith, M.; Melchior, L.; Reiltin, W.; Bennett, M.; Pennati, V.; Castiglione, F.; et al. Multicenter Evaluation of the Idylla NRAS-BRAF Mutation Test in Metastatic Colorectal Cancer. J. Mol. Diagn. 2018, 20, 664–676. [Google Scholar] [CrossRef]
- Van Haele, M.; Borght, S.V.; Ceulemans, A.; Wieërs, M.; Metsu, S.; Sagaert, X.; Weynand, B. Rapid clinical mutational testing of KRAS, BRAF and EGFR: A prospective comparative analysis of the Idylla technique with high-throughput next-generation sequencing. J. Clin. Pathol. 2019, 73, 35–41. [Google Scholar] [CrossRef]
- Petty, D.R.; Hassan, O.A.; Barker, C.S.; O’Neill, S.S. Rapid BRAF Mutation Testing in Pigmented Melanomas. Am. J. Dermatopathol. 2020, 42, 343–348. [Google Scholar] [CrossRef]
Figure 1.
3D representation of the BRAF protein. The red arrows highlight the codons in which the main BRAF mutations arise. This figure was created using Mol* PDB ID Mol* and Research Collaboratory for Structural Bioinformatics (RCSB) Protein Data Bank (PDB) [32,33].

Figure 2.
3D representation of BRAF mutations within the three-class system of classification. In particular from left to right: Class I p.V600; Class II p.G464, p. G469, p. L597, p.K601; Class III p.V459, p.G466, p.S467, p.G469, p.N581, p.D594, p.F595, p.G596. This figure was created by using Mol* PDB ID Mol* and Research Collaboratory for Structural Bioinformatics (RCSB) Protein Data Bank (PDB) [32,33].
Figure 2.
3D representation of BRAF mutations within the three-class system of classification. In particular from left to right: Class I p.V600; Class II p.G464, p. G469, p. L597, p.K601; Class III p.V459, p.G466, p.S467, p.G469, p.N581, p.D594, p.F595, p.G596. This figure was created by using Mol* PDB ID Mol* and Research Collaboratory for Structural Bioinformatics (RCSB) Protein Data Bank (PDB) [32,33].


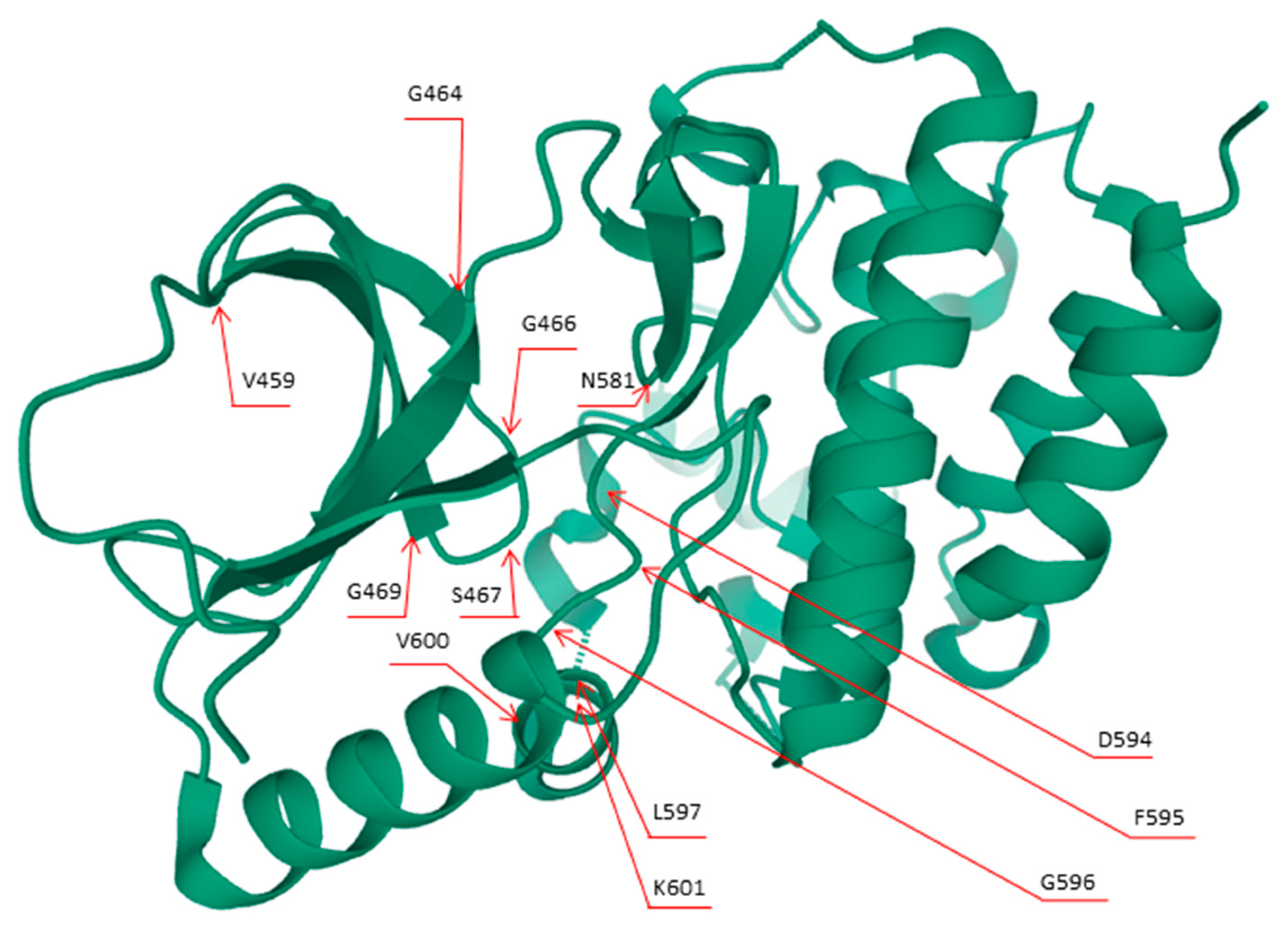{kind=link}
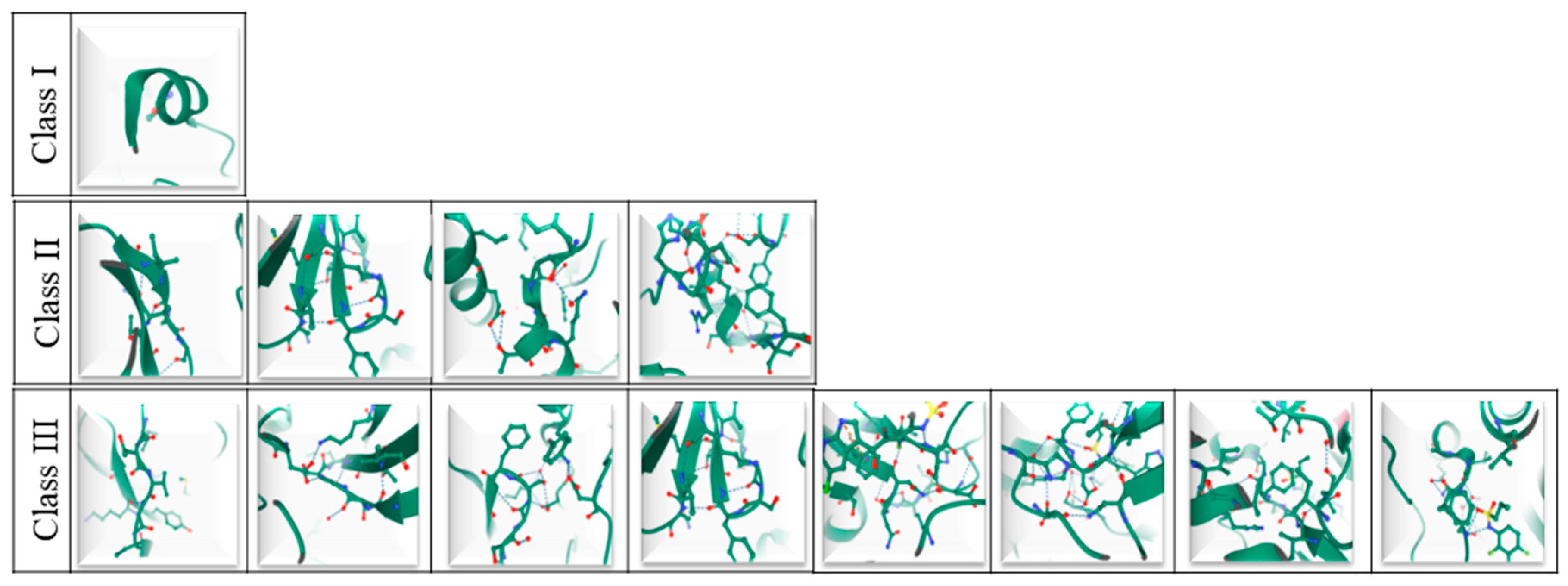{kind=link}
Table 1.
BRAF mutations classification system.
| Class I | Class II | Class III |
|---|---|---|
| p.V600D/E/K/M/R | p.G464E/V; p. G469A/R/V; p. L597Q/V; p.K601E/N/T; gene fusions | p.D287H; p.V459L; p.G466A/E/V; p.S467L; p.G469E; p.N581I/S; p.D594A/G/H/N; p.F595L; p.G596D/R |
Abbreviation: BRAF, V-Raf Murine Sarcoma Viral Oncogene Homolog B.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Pisapia, P.; Pepe, F.; Iaccarino, A.; Sgariglia, R.; Nacchio, M.; Russo, G.; Gragnano, G.; Malapelle, U.; Troncone, G. BRAF: A Two-Faced Janus. Cells 2020, 9, 2549. https://doi.org/10.3390/cells9122549
AMA Style
Pisapia P, Pepe F, Iaccarino A, Sgariglia R, Nacchio M, Russo G, Gragnano G, Malapelle U, Troncone G. BRAF: A Two-Faced Janus. Cells. 2020; 9(12):2549. https://doi.org/10.3390/cells9122549
Chicago/Turabian StylePisapia, Pasquale, Francesco Pepe, Antonino Iaccarino, Roberta Sgariglia, Mariantonia Nacchio, Gianluca Russo, Gianluca Gragnano, Umberto Malapelle, and Giancarlo Troncone. 2020. "BRAF: A Two-Faced Janus" Cells 9, no. 12: 2549. https://doi.org/10.3390/cells9122549
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.