The Oncogene AF1Q is Associated with WNT and STAT Signaling and Offers a Novel Independent Prognostic Marker in Patients with Resectable Esophageal Cancer

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Immunohistochemistry
2.3. Statistical Analysis
3. Results
3.1. AF1q Expression Analysis in Human Esophageal Cancer Samples
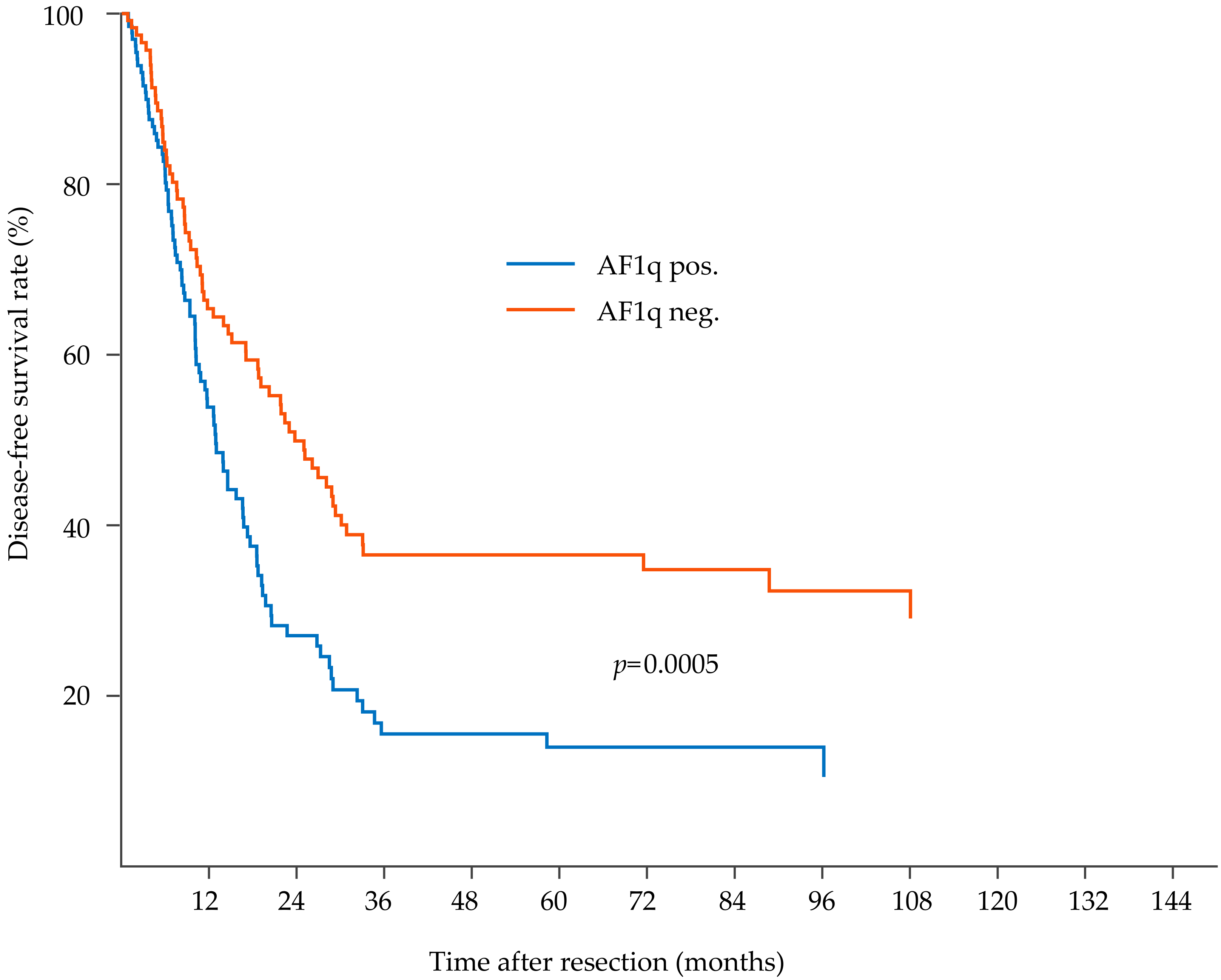
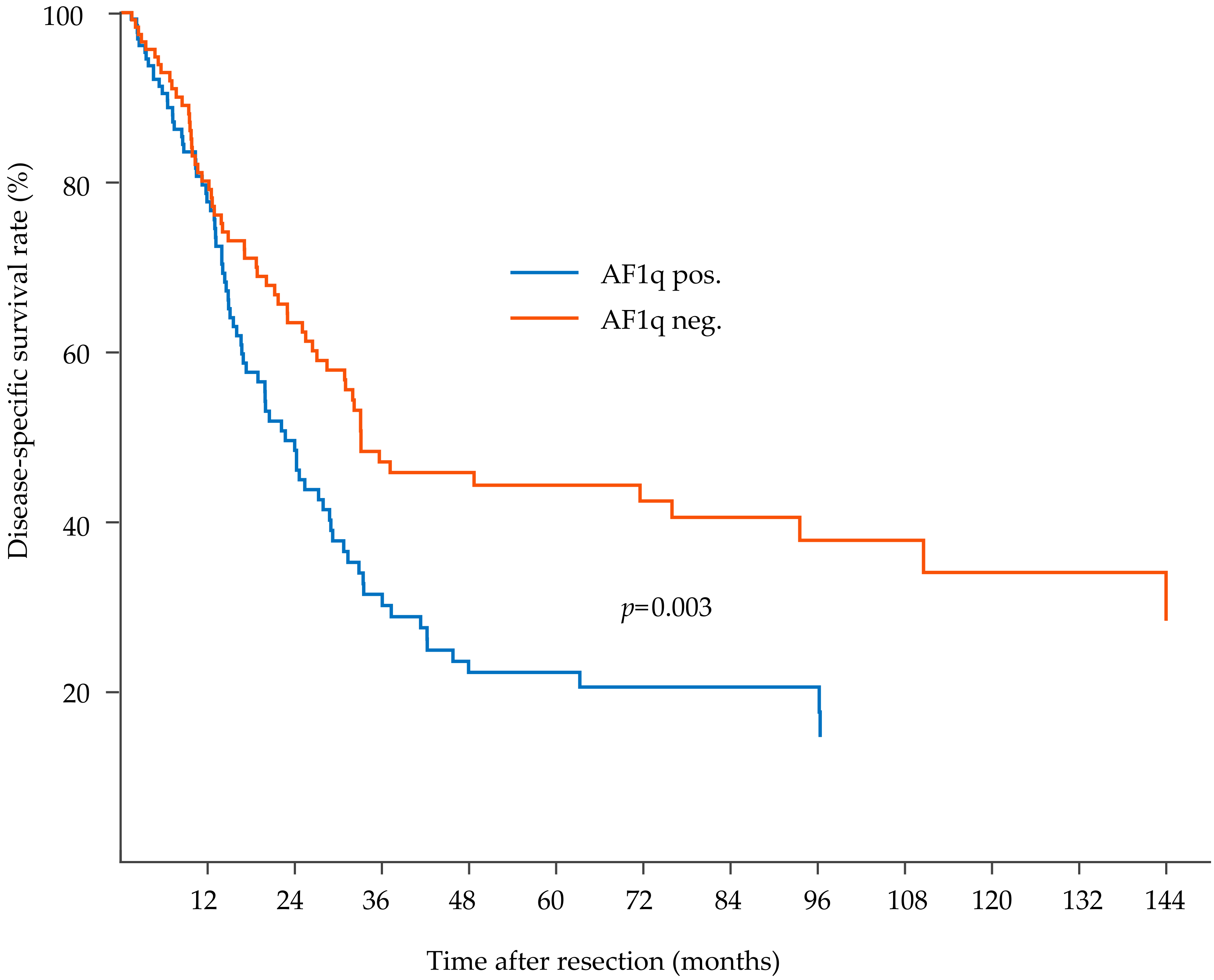
3.2. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tse, W.; Zhu, W.; Chen, H.S.; Cohen, A. A novel gene, AF1q, fused to MLL in t(1;11) (q21;q23), is specifically expressed in leukemic and immature hematopoietic cells. Blood 1995, 85, 650–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strunk, C.J.; Platzbecker, U.; Thiede, C.; Schaich, M.; Illmer, T.; Kang, Z.; Leahy, P.; Li, C.; Xie, X.; Laughlin, M.J.; et al. Elevated AF1q expression is a poor prognostic marker for adult acute myeloid leukemia patients with normal cytogenetics. Am. J. Hematol. 2009, 84, 308–309. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Schlederer, M.; Schreiber, M.; Ice, R.; Merkel, O.; Bilban, M.; Hofbauer, S.; Kim, S.; Addison, J.; Zou, J.; et al. AF1q is a novel TCF7 co-factor which activates CD44 and promotes breast cancer metastasis. Oncotarget 2015, 6, 20697–20710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tse, W.; Meshinchi, S.; Alonzo, T.A.; Stirewalt, D.L.; Gerbing, R.B.; Woods, W.G.; Appelbaum, F.R.; Radich, J.P. Elevated expression of the AF1q gene, an MLL fusion partner, is an independent adverse prognostic factor in pediatric acute myeloid leukemia. Blood 2004, 104, 3058–3063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, J.; Li, G.; Liu, L.; Wang, Y.; Li, X.; Gong, J. AF1q Mediates Tumor Progression in Colorectal Cancer by Regulating AKT Signaling. Int. J. Mol. Sci. 2017, 18, 987. [Google Scholar] [CrossRef]
- Liu, T.; Bohlken, A.; Kuljaca, S.; Lee, M.; Nguyen, T.; Smith, S.; Cheung, B.; Norris, M.D.; Haber, M.; Holloway, A.J.; et al. The retinoid anticancer signal: Mechanisms of target gene regulation. Br. J. Cancer 2005, 93, 310–318. [Google Scholar] [CrossRef]
- Co, N.; Tsang, W.; Wong, T.; Cheung, H.; Tsang, T.; Kong, S.; Kwok, T. Oncogene AF1q enhances doxorubicin-induced apoptosis through BAD-mediated mitochondrial apoptotic pathway. Mol. Cancer Ther. 2008, 7, 3160–3168. [Google Scholar] [CrossRef] [Green Version]
- Co, N.; Tsang, W.; Tsang, T.; Yeung, H.; Yau, P.; Kong, S.K.; Kwok, T.T. AF1q enhancement of γ irradiation-induced apoptosis by up-regulation of BAD expression via NF-κB in human squamous carcinoma A431 cells. Oncol. Rep. 2010, 24, 547–554. [Google Scholar] [CrossRef]
- Tiberio, P.; Cavadini, E.; Callari, M.; Daidone, M.G.; Appierto, V. AF1q: A novel mediator of basal and 4-HPR-induced apoptosis in ovarian cancer cells. PLoS ONE 2012, 7, e39968. [Google Scholar] [CrossRef]
- Lin, H.; Shaffer, K.; Sun, Z.; Jay, G.; He, W.; Ma, W. AF1q, a differentially expressed gene during neuronal differentiation, transforms HEK cells into neuron-like cells. Mol. Brain Res. 2004, 131, 126–130. [Google Scholar] [CrossRef]
- Tse, W.; Deeg, H.; Stirewalt, D.; Appelbaum, F.; Radich, J.; Gooley, T. Increased AF1q gene expression in high-risk myelodysplastic syndrome. Br. J. Haematol. 2005, 128, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, S.; Joh, J.; Remick, S.C.; Miller, D.M.; Yan, J.; Kanaan, Z.; Chao, J.-H.; Krem, M.M.; Basu, S.K.; et al. MLLT11/AF1q boosts oncogenic STAT3 activity through Src-PDGFR tyrosine kinase signaling. Oncotarget 2016, 7, 43960–43973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anastas, J.N.; Moon, R.T. WNT signalling pathways as therapeutic targets in cancer. Nat. Rev. Cancer 2013, 13, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Lee, H.; Herrmann, A.; Buettner, R.; Jove, R. Revisiting STAT3 signalling in cancer: New and unexpected biological functions. Nat. Rev. Cancer 2014, 14, 736–746. [Google Scholar] [CrossRef] [PubMed]
- Vacante, M.; Borzì, A.M.; Basile, F.; Biondi, A. Biomarkers in colorectal cancer: Current clinical utility and future perspectives. World J. Clin. Cases 2018, 6, 869–881. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Li, Z.; Ji, M.; Tan, A.; Bemis, J.; Tse, J.; Huang, G.; Park, J.; Ji, C.; Chen, J.; et al. MIR29B regulates expression of MLLT11 (AF1Q), an MLL fusion partner, and low MIR29B expression associates with adverse cytogenetics and poor overall survival in AML. Br. J. Haematol. 2011, 153, 753–757. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Lordick, F.; Mariette, C.; Haustermans, K.; Obermannova, R.; Arnold, D.; Committee, E.G. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v50–v57. [Google Scholar] [CrossRef]
- Buchert, M.; Burns, C.J.; Ernst, M. Targeting JAK kinase in solid tumors: Emerging opportunities and challenges. Oncogene 2016, 35, 939–951. [Google Scholar] [CrossRef]
- Hubbard, J.M.; Grothey, A. Napabucasin: An Update on the First-in-Class Cancer Stemness Inhibitor. Drugs 2017, 77, 1091–1103. [Google Scholar] [CrossRef]
- Dembowsky, K. A Safety and Pharmacokinetic Phase I/Ib Study of AMC303 in Patients With Solid Tumours. 2016. Available online: https://clinicaltrials.gov/ct2/show/NCT03009214 (accessed on 1 August 2016).
- Menke-van der Houven, C.W.; van Oordt, C.G.R.; van Herpen, C.; Coveler, A.L.; Mahalingam, D.; Verheul, H.M.; van der Graaf, W.T.; Christen, R.; Rüttinger, D.; Weigand, S.; et al. First-in-human phase I clinical trial of RG7356, an anti-CD44 humanized antibody, in patients with advanced, CD44-expressing solid tumors. Oncotarget 2016, 7, 80046–80058. [Google Scholar] [Green Version]
- Rice, T.W.; Patil, D.T.; Blackstone, E.H. 8th edition AJCC/UICC staging of cancers of the esophagus and esophagogastric junction: Application to clinical practice. Ann. Cardiothorac. Surg. 2017, 6, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Odze, R.; Flejou, J.; Boffetta, P.; Hofler, H.; Montgomery, E.; Spechler, S. Adenocarcinoma of the oesophgogastric junction. In WHO Classification of Tumours of the Digestive System, World Health Organization Classification of Tumours; Bosman, F., Carneiro, F., Hruban, R., Theise, N., Eds.; IARC Press: Lyon, Paris, 2010; pp. 39–44. [Google Scholar]
- Mandard, A.M.; Dalibard, F.; Mandard, J.C.; Marnay, J.; Henry-Amar, M.; Petiot, J.F.; Roussel, A.; Jacob, J.H.; Segol, P.; Samama, G.; et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Schoppmann, S.F.; Jesch, B.; Friedrich, J.; Jomrich, G.; Maroske, F.; Birner, P. Phosphorylation of signal transducer and activator of transcription 3 (STAT3) correlates with Her-2 status, carbonic anhydrase 9 expression and prognosis in esophageal cancer. Clin. Exp. Metastasis 2012, 29, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Addison, J.B.; Koontz, C.; Fugett, J.H.; Creighton, C.J.; Chen, D.; Farrugia, M.K.; Padon, R.R.; Voronkova, M.A.; McLaughlin, S.L.; Livengood, R.H.; et al. KAP1 Promotes Proliferation and Metastatic Progression of Breast Cancer Cells. Cancer Res. 2015, 75, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Chu, T.-H.; Chan, H.-H.; Hu, T.-H.; Wang, E.M.; Ma, Y.-L.; Huang, S.-C.; Wu, J.-C.; Chang, Y.-C.; Weng, W.-T.; Wen, Z.-H.; et al. Celecoxib enhances the therapeutic efficacy of epirubicin for Novikoff hepatoma in rats. Cancer Med. 2018, 7, 2567–2580. [Google Scholar] [CrossRef]
- Jin, H.; Sun, W.; Zhang, Y.; Yan, H.; Liufu, H.; Wang, S.; Chen, C.; Gu, J.; Hua, X.; Zhou, L.; et al. MicroRNA-411 Downregulation Enhances Tumor Growth by Upregulating MLLT11 Expression in Human Bladder Cancer. Mol. Ther. Nucleic Acids 2018, 11, 312–322. [Google Scholar] [CrossRef] [Green Version]
- Schemper, M.; Smith, T.L. A Note on Quantifying Follow-up in Studies of Failure Time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Rice, T.; Kelsen, D.; Blackstone, E.; Ishwaran, H.; Patil, D.; Bass, A.; Erasmus, J.; Gerdes, H.; Hofstetter, W. Esophagus and Esophagogastric Junction. In AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Yu, H.; Kortylewski, M.; Pardoll, D. Crosstalk between cancer and immune cells: Role of STAT3 in the tumour microenvironment. Nat. Rev. Immunol. 2007, 7, 41–51. [Google Scholar] [CrossRef]
- Phesse, T.J.; Buchert, M.; Stuart, E.; Flanagan, D.J.; Faux, M.; Afshar-Sterle, S.; Walker, F.; Zhang, H.H.; Nowell, C.J.; Jorissen, R. Partial inhibition of gp130-Jak-Stat3 signaling prevents Wnt–b-catenin–mediated intestinal tumor growth and regeneration. Cancer Biol. 2014, 7, 1–11. [Google Scholar] [CrossRef]
- Naor, D.; Wallach-Dayan, S.B.; Zahalka, M.A.; Sionov, R.V. Involvement of CD44, a molecule with a thousand faces, in cancer dissemination. Semin. Cancer Biol. 2008, 18, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Zoller, M. CD44: Can a cancer-initiating cell profit from an abundantly expressed molecule? Nat. Rev. Cancer 2011, 11, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.Z.; Li, D.Q.; Hou, Y.F.; Wu, J.; Lu, J.S.; Di, G.H.; Jin, W.; Ou, Z.L.; Shen, Z.Z.; Shao, Z.M. Identification of the functional role of AF1Q in the progression of breast cancer. Breast Cancer Res. Treat. 2008, 111, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Dong, Q.; Yao, M.; Shi, M.; Ye, J.; Zhao, L.; Su, J.; Gu, W.; Xie, W.; Wang, K.; et al. Establishment of an experimental human lung adenocarcinoma cell line SPC-A-1BM with high bone metastases potency by (99m)Tc-MDP bone scintigraphy. Nucl. Med. Biol. 2009, 36, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Bartley, A.N.; Washington, M.K.; Ventura, C.B.; Ismaila, N.; Colasacco, C.; Benson, A.B., III; Carrato, A.; Gulley, M.L.; Jain, D.; Kakar, S.; et al. HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline From the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology. Am. J. Clin. Pathol. 2016, 146, 647–669. [Google Scholar] [CrossRef]
- Schoppmann, S.F.; Jesch, B.; Friedrich, J.; Wrba, F.; Schultheis, A.; Pluschnig, U.; Maresch, J.; Zacherl, J.; Hejna, M.; Birner, P. Expression of Her-2 in carcinomas of the esophagus. Am. J. Surg. Pathol. 2010, 34, 1868–1873. [Google Scholar] [CrossRef]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef]
- Kerr, K.; Bubendorf, L.; Edelman, M.; Marchetti, A.; Mok, T.; Novello, S.; O’Byrne, K.; Stahel, R.; Peters, S.; Felip, E. ESMO Consensus Guidelines: Pathology and molecular biomarkers for non-small-cell lung cancer. Ann. Oncol. 2014, 25, 1681–1690. [Google Scholar] [CrossRef]
- Qing, Y.; Stark, G.R. Alternative activation of STAT1 and STAT3 in response to interferon-gamma. J. Biol. Chem. 2004, 279, 41679–41685. [Google Scholar] [CrossRef]
- Peterson, L.W.; Artis, D. Intestinal epithelial cells: Regulators of barrier function and immune homeostasis. Nat. Rev. Immunol. 2014, 14, 141–153. [Google Scholar] [CrossRef]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D.; Committee, E.G. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Factor | Patients with EC, n = 278 (100.0) | Patients with AF1q-positive EC, n = 138 (49.6) | Patients with AF1q-negative EC, n = 140 (50.4) | p-value |
| Female sex | 65 (23.4) | 28 (43.1) | 37 (56.9) | 0.23 * |
| Male sex | 213 (76.6) | 110 (51.6) | 103 (48.4) | |
| Age | 63.3 (34–90) | 63.8 (38–90) | 63.9 (34–90) | rs = 0.03 ** (0.65) |
| Adiposity | 16 (5.8) | 10 (62.5) | 6 (37.5) | 0.11 * |
| Reflux | 5 (1.8) | 2 (40.0) | 3 (60) | 0.22 * |
| Neoadjuvant therapy | 68 (24.5) | 47 (69.1) | 21 (30.9) | 0.0002 * |
| Factor | Patients with EC, n = 278 (100.0) | Patients with AF1q-positive EC, n = 138 (49.6) | Patients with AF1q-negative EC, n = 140 (50.4) | p-value |
| Histological tumor subtype | ||||
| ESCC | 118 (42.4) | 54 (45.8) | 64 (54.2) | rs = 0.02 ** (0.88) |
| AC | 160 (57.6) | 84 (52.5) | 76 (47.5) | |
| EAC | 67 (24.1) | 42 (62.7) | 25 (37.3) | n.a. |
| AEG | 93 (33.5) | 42 (45.2) | 51 (54.8) | |
| AJCC/UICC tumor staging ESCC n = 118 (42.4) | ||||
| IB | 3 (2.5) | 0 (0.0) | 3 (100.0) | rs = 0.06 ** (0.55) |
| IIA | 32 (27.1) | 15 (46.9) | 17 (53.1) | |
| IIIA | 13 (11.0) | 6 (46.2) | 7 (53.8) | |
| IIIB | 45 (38.1) | 20 (44.4) | 25 (55.6) | |
| IVA | 19 (15.3) | 10 (55.6) | 8 (44.4) | |
| IVB | 7 (5.9) | 3 (42.9) | 4 (57.1) | |
| AJCC/UICC tumor staging EAC n = 67 (24.1)/AEG n = 93 (33.5) | ||||
| IC | 8 (5.0) | 4 (50.0) | 4 (50.0) | rs = 0.12 ** (0.14) |
| IIA | 3 (1.9) | 0 (0.0) | 3 (100.0) | |
| IIB | 21 (13.1.) | 10 (47.6) | 11 (32.4) | |
| IIIA | 8 (5.0) | 2 (25.0) | 6 (75.0) | |
| IIIB | 59 (36.9) | 33 (55.9) | 26 (44.1) | |
| IVA | 61 (38.1) | 35 (57.4) | 26 (42.6) | |
| Regional lymph nodes pN | ||||
| N1 | 119 (44.1) | 65 (54.6) | 54 (45.4) | 0.18 * |
| Tumor grading G | ||||
| G1 | 11 (4.0) | 4 (36.4) | 7 (63.6) | rs = 0.02 ** (0.69) |
| G2 | 132 (47.5) | 66 (50.0) | 66 (50.0) | |
| G3 | 135 (48.6) | 68 (50.4) | 67 (49.6) | |
| Resection margin R | ||||
| R0 | 228 (82.0) | 104 (45.6) | 124 (54.5) | 0.004 * |
| R1 | 50 (18.0) | 34 (68.0) | 16 (32.0) | |
| Histological response to neoadjuvant therapy | ||||
| none | 7 (10.3) | 7 (10.3) | 0 (0.0) | rs = 0.22 ** (0.09) |
| poor | 30 (44.1) | 21 (70.0) | 9 (30.0) | |
| moderate | 17 (25.0) | 11 (64.7) | 6 (35.3) | |
| good | 4 (5.9) | 2 (50.0) | 2 (50.0) | |
| Factor | Patients with AF1q-positive EC, n = 133 (49.6) | Patients with AF1q-negative EC, n = 135 (50.4) | p-value |
| CD44, n = 268 (100) | |||
| positive, n = 94 (35.1) | 58 (21.6) | 36 (13.5) | 0.004 |
| negative, n = 174 (74.9) | 75 (28.0) | 99 (36.9) | |
| Factor | Patients with AF1q-positive EC, n = 117 (51.5) | Patients with AF1q-negative EC, n = 110 (48.5) | p-value |
| pYSTAT3, n = 227 (100) | |||
| positive, n = 101 (44.5) | 66 (29.1) | 35 (15.4) | 0.0002 |
| negative, n = 126 (55.5) | 51 (22.4) | 75 (33.1) | |
| Factor | AF1q-positive local EC, n = 18 (56.3) | AF1q-negative local EC, n = 14 (43.7) | p-value |
| Lymph node metastases, n = 32 (100) | |||
| AF1q positive, n = 19 (59.4) | 14 (43.8) | 5 (15.6) | 0.016 |
| AF1q negative, n = 13 (40.6) | 4 (12.5) | 9 (28.1) | |
| Factor | Univariate p-Value | Multivariable p-Value | HR | 95% CI Low | 95% CI High |
| Disease-free survival | |||||
| AF1q | 0.0005 | 0.01 | 1.5 | 1.1 | 2.2 |
| Neoadjuvant therapy | 0.0002 | 0.005 | 1.7 | 1.2 | 2.6 |
| Histological tumor subtype * | 0.16 | 0.0004 | 1.9 | 1.3 | 2.7 |
| Local tumor stage pT | 0.001 | 0.07 | n.a. | ||
| Regional lymph nodes pN | <0.0001 | <0.0001 | 2.3 | 1.6 | 3.2 |
| Tumor grading G | 0.13 | 0.30 | n.a. | ||
| Resection margin R | 0.02 | 0.50 | n.a. | ||
| Disease-specific survival | |||||
| AF1q | 0.003 | 0.03 | 1.5 | 1.0 | 2.1 |
| Neoadjuvant therapy | 0.10 | 0.83 | n.a. | ||
| Histological tumor subtype * | 0.30 | 0.003 | 1.8 | 1.2 | 2.7 |
| Local tumor stage pT | 0.0004 | 0.007 | 1.9 | 1.2 | 3.0 |
| Regional lymph nodes pN | <0.0001 | <0.0001 | 2.2 | 1.5 | 3.2 |
| Tumor grading G | 0.22 | 0.48 | n.a. | ||
| Resection margin R | 0.01 | 0.31 | n.a. | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruber, E.S.; Oberhuber, G.; Birner, P.; Schlederer, M.; Kenn, M.; Schreiner, W.; Jomrich, G.; Schoppmann, S.F.; Gnant, M.; Tse, W.; et al. The Oncogene AF1Q is Associated with WNT and STAT Signaling and Offers a Novel Independent Prognostic Marker in Patients with Resectable Esophageal Cancer. Cells 2019, 8, 1357. https://doi.org/10.3390/cells8111357
Gruber ES, Oberhuber G, Birner P, Schlederer M, Kenn M, Schreiner W, Jomrich G, Schoppmann SF, Gnant M, Tse W, et al. The Oncogene AF1Q is Associated with WNT and STAT Signaling and Offers a Novel Independent Prognostic Marker in Patients with Resectable Esophageal Cancer. Cells. 2019; 8(11):1357. https://doi.org/10.3390/cells8111357
Chicago/Turabian StyleGruber, Elisabeth S., Georg Oberhuber, Peter Birner, Michaela Schlederer, Michael Kenn, Wolfgang Schreiner, Gerd Jomrich, Sebastian F. Schoppmann, Michael Gnant, William Tse, and et al. 2019. "The Oncogene AF1Q is Associated with WNT and STAT Signaling and Offers a Novel Independent Prognostic Marker in Patients with Resectable Esophageal Cancer" Cells 8, no. 11: 1357. https://doi.org/10.3390/cells8111357