Analysis of Intensity-Modulated Radiation Therapy (IMRT), Proton and 3D Conformal Radiotherapy (3D-CRT) for Reducing Perioperative Cardiopulmonary Complications in Esophageal Cancer Patients

Abstract
:1. Introduction
2. Experimental
2.1. Patient Selection

{kind=link}
{kind=link}
| Patient | Histology | Tumor Location | TNM Stage | Stage Grouping | Treatment (Gy/fx) | PTV volume (cm3) |
|---|---|---|---|---|---|---|
| 1 | Adenocarcinoma | Distal 2/3 of esophagus | T3 N1 M0 | III | 50.4/28 | 1004.47 |
| 2 | Adenocarcinoma | AEG I | T3 N0 M0 | IIA | 50.4/28 | 1174.1 |
| 3 | Adenocarcinoma | AEG I | T3 N1 M0 | III | 50.4/28 | 876.76 |
| 4 | Adenocarcinoma | AEG II | T3 N1 M0 | III | 50.4/28 | 1416.68 |
| 5 | Adenocarcinoma | Distal 2/3 of esophagus | T2 N0 M0 | IIA | 50.4/28 | 666.47 |
| 6 | Adenocarcinoma | AEG II | T3 N1 M0 | III | 50.4/28 | 1866.24 |
| 7 | Adenocarcinoma | AEG I | T3 N1 M0 | III | 50.4/28 | 1509.503 |
| 8 | Adenocarcinoma | AEG II | T3 N1 M0 | III | 50.4/28 | 567.41 |
| 9 | Adenocarcinoma | Distal 2/3 of esophagus | T3 N1 M0 | III | 50.4/28 | 1084.7 |
| 10 | Adenocarcinoma | Distal 2/3 of esophagus | T3 N0 M0 | IIA | 50.4/28 | 813.12 |
2.2. Simulation and Treatment Planning
2.3. Plan Evaluation and Analysis
3. Results

3.1. Protons vs. IMRT
| Organ at Risk | Proton Plans | IMRT Plans | 3DCRT Plans | p-value | |||
|---|---|---|---|---|---|---|---|
| Proton vs. IMRT | Proton vs. 3DCRT | IMRT vs. 3DCRT | |||||
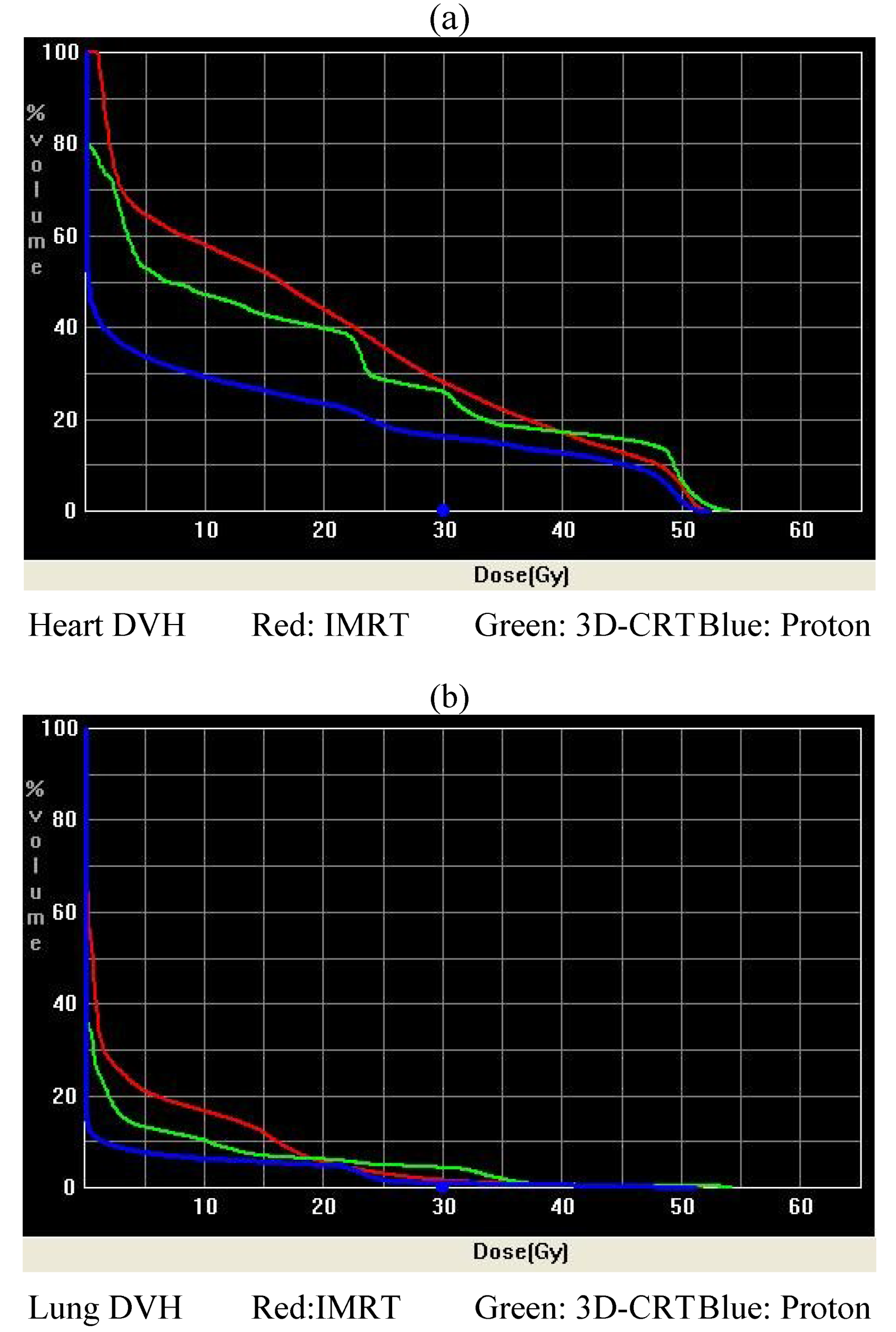
| Lung | V5 (%) | 21.4 ± 10.3 | 46.9 ± 17.6 | 34.1 ± 13.9 | 0.001 | 0.032 | 0.087 |
| V10 (%) | 19.4 ± 8.6 | 37.8 ± 14.7 | 29.1 ± 12.7 | 0.003 | 0.060 | 0.178 | |
| V15 (%) | 17.3 ± 7.5 | 27.9 ± 8.8 | 23.9 ± 11.3 | 0.009 | 0.141 | 0.390 | |
| V20 (%) | 15.3 ± 6.5 | 16.2 ± 5.8 | 22.1 ± 10.8 | 0.794 | 0.114 | 0.144 | |
| V30 (%) | 6.1 ± 2.9 | 6.6 ± 3.2 | 9.8 ± 5.1 | 0.720 | 0.067 | 0.113 | |
| V40 (%) | 4.3 ± 2.1 | 3.5 ± 2.0 | 4.7 ± 2.9 | 0.391 | 0.682 | 0.270 | |
| V50 (%) | 1.1 ± 1.0 | 1.6 ± 1.3 | 3.3 ± 2.1 | 0.251 | 0.008 | 0.043 | |
| Mean (Gy) | 6.0 ± 2.6 | 9.5 ± 3.2 | 9.4 ± 4.0 | 0.016 | 0.040 | 0.966 | |
| Stomach | V20 (%) | 66.8 ± 26.0 | 87.4 ± 22.9 | 85.1 ± 25.1 | 0.076 | 0.126 | 0.834 |
| V50 (%) | 29.8 ± 21.7 | 59.9 ± 28.0 | 40.0 ± 39.5 | 0.015 | 0.484 | 0.211 | |
| Liver | D 1/3 (Gy) | 0.2 ± 0.1 | 21.0 ± 4.7 | 28.9 ± 7.4 | 0.001 | 0.000 | 0.011 |
| D 2/3 (Gy) | 0.1 ± 0.1 | 12.4 ± 6.6 | 11.1 ± 11.8 | 0.001 | 0.016 | 0.754 | |
| Mean (Gy) | 3.6 ± 1.8 | 18.1 ± 4.6 | 20.3 ± 6.3 | 0.001 | 0.001 | 0.383 | |
| Spinal Cord | Dmax (Gy) | 11.6 ± 10.0 | 36.9 ± 3.5 | 31.2 ± 9.7 | 0.001 | 0.001 | 0.097 |
| Heart | V25 (%) | 23.7 ± 7.8 | 54.1 ± 15.2 | 56.3 ± 22.3 | 0.001 | 0.001 | 0.802 |
| V30 (%) | 20.9 ± 7.1 | 42.3 ± 15.3 | 32.7 ± 9.4 | 0.001 | 0.005 | 0.109 | |
| V40 (%) | 16.2 ± 6.4 | 25.5 ± 11.0 | 25.8 ± 8.8 | 0.036 | 0.012 | 0.942 | |
| V50 (%) | 2.8 ± 2.3 | 12.0 ± 8.6 | 20.0 ± 12.6 | 0.008 | 0.002 | 0.118 | |
| Mean (Gy) | 12.6 ± 3.9 | 28.5 ± 5.5 | 27.5 ± 5.2 | 0.001 | 0.001 | 0.692 | |
| LAD | Mean (Gy) | 0.4 ± 0.6 | 17.6 ± 5.8 | 15.1 ± 8.2 | 0.001 | 0.001 | 0.441 |
| Max (Gy) | 5.4 ± 8.7 | 31.4 ± 3.6 | 26.9 ± 4.8 | 0.001 | 0.001 | 0.028 | |
| Left Ventricle | Mean (Gy) | 13.9 ± 6.6 | 30.3 ± 5.6 | 27.3 ± 5.6 | 0.001 | 0.001 | 0.250 |
| Max (Gy) | 51.4 ± 0.9 | 52.3 ± 0.8 | 50.6 ± 10.6 | 0.029 | 0.808 | 0.613 | |
| Pericardium | Mean (Gy) | 13.5 ± 1.8 | 26.0 ± 5.1 | 24.8 ± 4.2 | 0.001 | 0.001 | 0.552 |
| Max (Gy) | 52.6 ± 1.3 | 53.4 ± 0.5 | 55.3 ± 2.0 | 0.118 | 0.003 | 0.015 | |
3.2. Protons vs. 3D-CRT
3.3. IMRT vs. 3D-CRT
4. Discussion

5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar]
- Gebski, V.; Burmeister, B.; Smithers, B.M.; Foo, K.; Zalcberg, J.; Simes, J. Australasian Gastro-Intestinal Trials Group. Survival benefits from neoadjuvant chemoradiotherapy or chemotherapy in oesophageal carcinoma: A meta-analysis. Lancet Oncol. 2007, 8, 226–234. [Google Scholar]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar]
- Ling, F.C.F.; Durkin, A.E.; Ferguson, M.K. Induction therapy does not increase surgical morbidity after esophagectomy for cancer. Ann. Thoracic Surg. 2004, 78, 1783–1789. [Google Scholar]
- Wang, S.L.; Liao, Z.X.; Vaporciyan, A.A.; Tucker, S.L.; Liu, H.; Wei, X.; Swisher, S.; Ajani, J.A.; Cox, J.D.; Komaki, R. Investigation of clinical and dosimetric factors associated with postoperative pulmonary complications in esophageal cancer patients treated with concurrent chemoradiotherapy followed by surgery. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 692–699. [Google Scholar]
- Girinsky, T.; Pichenot, C.; Beaudre, A.; Ghalibafian, M.; Lefkopoulos, D. Is intensity-modulated radiotherapy better than conventional radiation treatment and three-dimensional conformal radiotherapy for mediastinal masses in patients with Hodgkin’s disease, and is there a role for beam orientation optimization and dose constraints assigned to virtual volumes? Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 218–226. [Google Scholar]
- Wang, J.; Wei, C.; Tucker, S.L.; Myles, B.; Palmer, M.; Hofstetter, W.L.; Swisher, S.G.; Ajani, J.A.; Cox, J.D.; Komaki, R.; et al. Predictors of postoperative complications after trimodality therapy for esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 885–891. [Google Scholar]
- Gayed, I.W.; Liu, H.H.; Yusuf, S.W.; Komaki, R.; Wei, X.; Wang, X.; Chang, J.Y.; Swafford, J.; Broemeling, L.; Liao, Z. The prevalence of myocardial ischemia after concurrent chemoradiation therapy as detected by gated myocardial perfusion imaging in patients with esophageal cancer. J. Nucl. Med. 2006, 47, 1756–1762. [Google Scholar]
- Zhang, X.; Zhao, K.L.; Guerrero, T.M.; McGuire, S.E.; Yaremko, B.; Komaki, R.; Cox, J.D.; Hui, Z.; Li, Y.; Newhauser, W.D.; et al. Four-dimensional computed tomography-based treatment planning for intensity-modulated radiation therapy and proton therapy for distal esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 278–287. [Google Scholar]
- Krueger, E.A.; Schipper, M.J.; Koelling, T.; Marsh, R.B.; Butler, J.B.; Pierce, L.J. Cardiac chamber and coronary artery doses associated with postmastectomy radiotherapy techniques to the chest wall and regional nodes. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1195–1203. [Google Scholar]
- Feng, M.; Moran, J.M.; Koelling, T.; Chughtai, A.; Chan, J.L.; Freedman, L.; Hayman, J.A.; Jagsi, R.; Jolly, S.; Larouere, J.; et al. Development and validation of a heart atlas to study cardiac exposure to radiation following treatment for breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 10–18. [Google Scholar]
- Wei, X.; Liu, H.H.; Tucker, S.L.; Wang, S.; Mohan, R.; Cox, J.D.; Komaki, R.; Liao, Z. Risk factors for pericardial effusion in inoperable esophageal cancer patients treated with definitive chemoradiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 707–714. [Google Scholar]
- Iori, M.; Cattaneo, G.M.; Cagni, E.; Fiorino, C.; Borasi, G.; Riccardo, C.; Iotti, C.; Fazio, F.; Nahum, A.E. Dose-volume and biological-model based comparison between helical tomotherapy and (inverse-planned) IMAT for prostate tumours. Radiother. Oncol. 2008, 88, 34–45. [Google Scholar]
- Whitelaw, G.L.; Blasiak-Wal, I.; Cooke, K.; Usher, C.; Macdougall, N.D.; Plowman, P.N. A dosimetric comparison between two intensity-modulated radiotherapy techniques: Tomotherapy vs. dynamic linear accelerator. Br. J. Radiol. 2008, 81, 333–340. [Google Scholar]
- McIntosh, A.; Read, P.W.; Khandelwal, S.R.; Arthur, D.W.; Turner, A.B.; Ruchala, K.J.; Olivera, G.H.; Jeswani, S.; Sheng, K. Evaluation of coplanar partial left breast irradiation using tomotherapy-based topotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 603–610. [Google Scholar]
- Sheng, K.; Molloy, J.A.; Larner, J.M.; Read, P.W. A dosimetric comparison of non-coplanar IMRT versus Helical Tomotherapy for nasal cavity and paranasal sinus cancer. Radiother. Oncol. 2007, 82, 174–178. [Google Scholar]
- Joseph, K.J.; Syme, A.; Small, C.; Warkentin, H.; Quon, H.; Ghosh, S.; Field, C.; Pervez, N.; Tankel, K.; Patel, S.; et al. A treatment planning study comparing helical tomotherapy with intensity-modulated radiotherapy for the treatment of anal cancer. Radiother. Oncol. 2010, 94, 60–66. [Google Scholar]
- Yang, G.Y.; McCloskey, S.A.; Khushalani, N.I. Principles of modern radiation techniques for esophageal and gastroeseophageal junction cancers. Gastrointest Cancer Res. 2009, 3, S6–S10. [Google Scholar]
- Hazard, L.; Yang, G.; McAleer, M.F.; Hayman, J.; Willett, C. Principles and techniques of radiation therapy for esophageal and gastroesophageal junction cancers. J. Natl. Compr. Canc. Netw. 2008, 6, 870–878. [Google Scholar]
- Kim, T.H.; Cho, K.H.; Pyo, H.R.; Lee, J.S.; Zo, J.I.; Lee, D.H.; Lee, J.M.; Kim, H.Y.; Hwangbo, B.; Park, S.Y.; et al. Dose-volumetric parameters for predicting severe radiation pneumonitis after three-dimensional conformal radiation therapy for lung cancer. Radiology 2005, 235, 208–215. [Google Scholar]
- Tsujino, K.; Hirota, S.; Endo, M.; Obayashi, K.; Kotani, Y.; Satouchi, M.; Kado, T.; Takada, Y. Predictive value of dose-volume histogram parameters for predicting radiation pneumonitis after concurrent chemoradiation for lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 110–115. [Google Scholar]
- Liu, H.; Zhang, X.; Vinogradskiy, Y.Y.; Swisher, S.G.; Komaki, R.; Chang, J.Y. Predicting radiation pneumonitis after stereotactic ablative radiation therapy in patients previously treated with conventional thoracic radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 1017–1023. [Google Scholar]
- Wang, S.; Liao, Z.; Wei, X.; Liu, H.H.; Tucker, S.L.; Hu, C.S.; Mohan, R.; Cox, J.D.; Komaki, R. Analysis of clinical and dosimetric factors associated with treatment-related pneumonitis (TRP) in patients with non-small-cell lung cancer (NSCLC) treated with concurrent chemotherapy and three-dimensional conformal radiotherapy (3D-CRT). Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 1399–1407. [Google Scholar]
- Lee, H.K.; Vaporciyan, A.A.; Cox, J.D.; Tucker, S.L.; Putnam, J.B., Jr.; Ajani, J.A.; Liao, Z.; Swisher, S.G.; Roth, J.A.; Smythe, W.R.; et al. Postoperative pulmonary complications after preoperative chemoradiation for esophageal carcinoma: Correlation with pulmonary dose-volume histogram parameters. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 1317–1322. [Google Scholar]
- Taylor, C.W.; Povall, J.M.; McGale, P.; Nisbet, A.; Dodwell, D.; Smith, J.T.; Darby, S.C. Cardiac dose from tangential breast cancer radiotherapy in the year 2006. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 501–507. [Google Scholar]
- Taylor, C.W.; Broǿnnum, D.; Darby, S.C.; Gagliardi, G.; Hall, P.; Jensen, M.B.; McGale, P.; Nisbet, A.; Ewertz, M. Cardiac dose estimates from Danish and Swedish breast cancer radiotherapy during 1977–2001. Radiother. Oncol. 2001, 100, 176–183. [Google Scholar]
- Ishikura, S.; Nihei, K.; Ohtsu, A.; Boku, N.; Hironaka, S.; Mera, K.; Muto, M.; Ogino, T.; Yoshida, S. Long-term toxicity after definitive chemoradiotherapy for squamous cell carcinoma of the thoracic esophagus. J. Clin. Oncol. 2003, 21, 2697–2702. [Google Scholar]
- Cosset, J.M.; Henry-Amar, M.; Pellae-Cosset, B.; Carde, P.; Girinski, T.; Tubiana, M.; Hayat, M. Pericarditis and myocardial infarctions after Hodgkin’s disease therapy. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 447–449. [Google Scholar]
- Hancock, S.L.; Tucker, M.A.; Hoppe, R.T. Factors affecting late mortality from heart disease after treatment of Hodgkin’s disease. JAMA 1993, 270, 1949–1955. [Google Scholar]
- Hatakenaka, M.; Yonezawa, M.; Nonoshita, T.; Nakamura, K.; Yabuuchi, H.; Shioyama, Y.; Nagao, M.; Matsuo, Y.; Kamitani, T.; Higo, T.; et al. Acute cardiac impairment associated with concurrent chemoradiotherapy for esophageal cancer: Magnetic resonance evaluation. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e67–e73. [Google Scholar]
- Fukada, J.; Shigematsu, N.; Takeuchi, H.; Ohashi, T.; Saikawa, Y.; Takaishi, H.; Hanada, T.; Shiraishi, Y.; Kitagawa, Y.; Fukuda, K. Symptomatic pericardial effusion after chemoradiation therapy in esophageal cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 487–493. [Google Scholar]
- Darby, S.C.; Cutter, D.J.; Boerma, M.; Constine, L.S.; Fajardo, L.F.; Kodama, K.; Mabuchi, K.; Marks, L.B.; Mettler, F.A.; Pierce, L.J.; et al. Radiation-related heart disease: Current knowledge and future prospects. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 656–665. [Google Scholar]
- Sandaro, A.; Petruzzelli, M.F.; D’Errico, M.P.; Grimaldi, L.; Pili, G.; Portaluri, M. Radiation-induced cardiac damage in early left breast cancer patients: Risk factors, biological mechanisms, radiobiology, and dosimetric constraints. Radiother. Oncol. 2012, 103, 133–142. [Google Scholar]
- Host, H.; Brennhovd, I.O.; Loeb, M. Postoperative radiotherapy in breast cancer—Long-term results from the Oso study. Int. J. Radiat. Oncol. Biol. Phys. 1986, 12, 727–732. [Google Scholar]
- Nilsson, G.; Holmberg, L.; Garmo, H.; Duvernoy, O.; Sjögren, I.; Lagerqvist, B.; Blomqvist, C. Distribution of coronary artery stenosis after radiation for breast cancer. J. Clin. Oncol. 2012, 30, 380–386. [Google Scholar]
- Gagliardi, G.; Constine, L.S.; Moiseekno, V.; Correa, C.; Pierce, L.J.; Allen, A.M.; Marks, L.B. Radiation dose-volume effects in the heart. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S77–S85. [Google Scholar]
- Isacsson, U.; Lennernas, B.; Grusell, E.; Jung, B.; Montelius, A.; Glimelius, B. Comparative treatment planning between proton and x-ray therapy in esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 441–450. [Google Scholar]
- Martin, S.; Chen, J.Z.; Rashid Dar, A.; Yartsev, S. Dosimetric comparison of helical tomotherapy, RapidArc, and a novel IMRT & Arc technique for esophageal carcinoma. Radiother. Oncol. 2011, 101, 431–437. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ling, T.C.; Slater, J.M.; Nookala, P.; Mifflin, R.; Grove, R.; Ly, A.M.; Patyal, B.; Slater, J.D.; Yang, G.Y. Analysis of Intensity-Modulated Radiation Therapy (IMRT), Proton and 3D Conformal Radiotherapy (3D-CRT) for Reducing Perioperative Cardiopulmonary Complications in Esophageal Cancer Patients. Cancers 2014, 6, 2356-2368. https://doi.org/10.3390/cancers6042356
Ling TC, Slater JM, Nookala P, Mifflin R, Grove R, Ly AM, Patyal B, Slater JD, Yang GY. Analysis of Intensity-Modulated Radiation Therapy (IMRT), Proton and 3D Conformal Radiotherapy (3D-CRT) for Reducing Perioperative Cardiopulmonary Complications in Esophageal Cancer Patients. Cancers. 2014; 6(4):2356-2368. https://doi.org/10.3390/cancers6042356
Chicago/Turabian StyleLing, Ted C., Jerry M. Slater, Prashanth Nookala, Rachel Mifflin, Roger Grove, Anh M. Ly, Baldev Patyal, Jerry D. Slater, and Gary Y. Yang. 2014. "Analysis of Intensity-Modulated Radiation Therapy (IMRT), Proton and 3D Conformal Radiotherapy (3D-CRT) for Reducing Perioperative Cardiopulmonary Complications in Esophageal Cancer Patients" Cancers 6, no. 4: 2356-2368. https://doi.org/10.3390/cancers6042356