

Detection and Classification of Hysteroscopic Images Using Deep Learning
 ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol and Selection Criteria
2.2. Study Outcomes
- accuracy of the DL model in the classification of intracavitary uterine lesions (overall and by category of lesion) with the aid of specific clinical factors to DL model performance;
- precision, sensitivity, specificity, and F1 score (i.e., the harmonic mean of precision and sensitivity) of the DL model in the classification of intracavitary uterine lesions (overall and by category of lesion), with and without the aid of specific clinical factors to DL model performance;
- precision, sensitivity, and F1 score of the DL model in the identification of intracavitary uterine lesions, with and without the aid of specific clinical factors to DL model performance;
- the best performance of the DL model during testing in the identification and classification of intracavitary uterine lesions (overall and by category of lesion).
2.3. Hysteroscopy and Image Processing
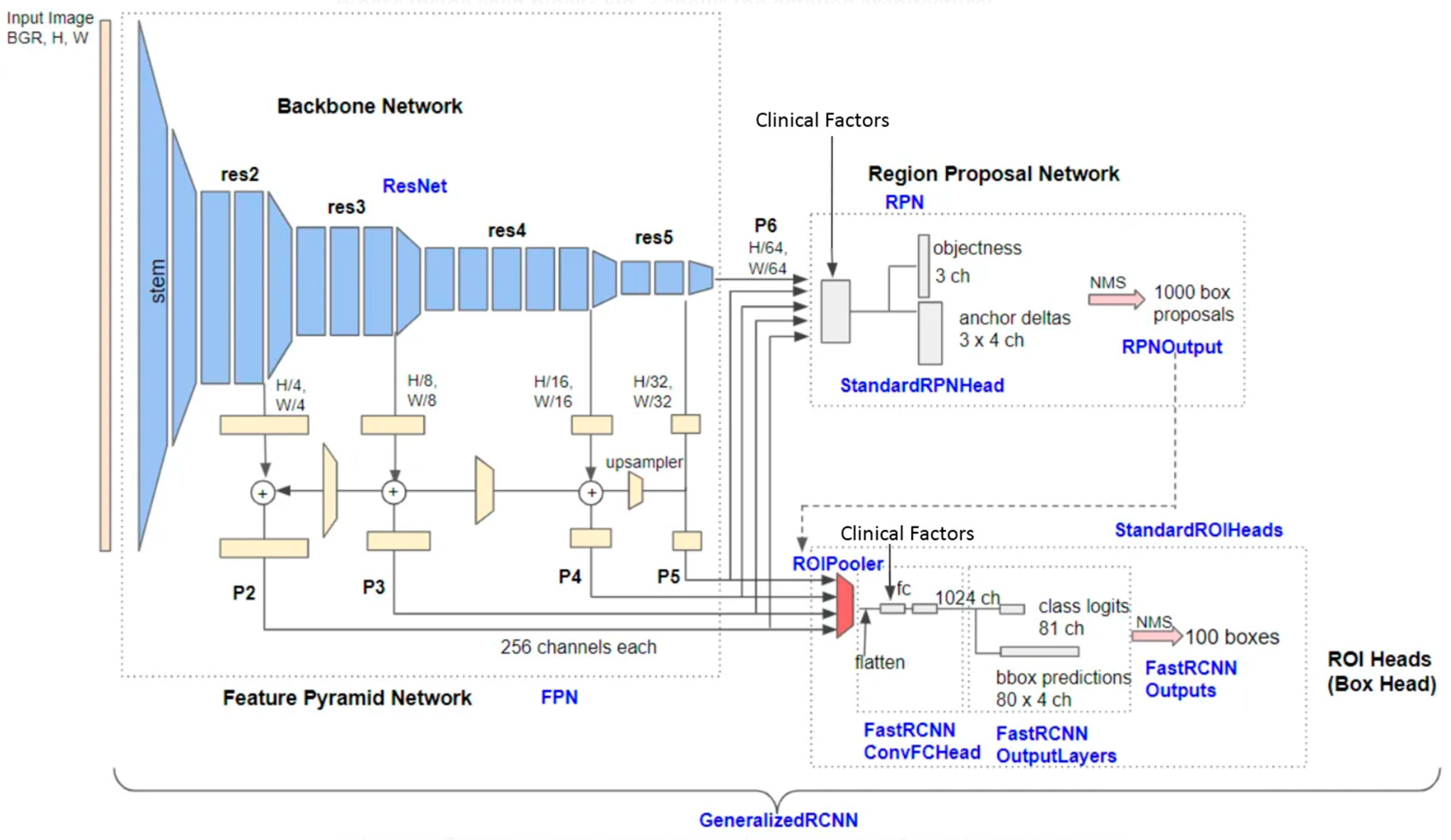
2.4. Deep Learning
- Random Vertical and Horizontal Flipping: each image in the training batch had a chance of being flipped either vertically or horizontally. This step introduces a variety of orientations, helping the model to learn features that are orientation-invariant.
- Random Brightness Adjustment: the brightness of each image was altered using a random factor ranging from 0.8 to 1.2. This variance in brightness ensures the model’s robustness against different lighting conditions.
- Random Contrast Adjustment: similarly, the contrast of each image was modified with a random factor within the same range (0.8 to 1.2). This step helps in training the model to identify features under various contrast levels.
3. Results
3.1. Study Population and Dataset
3.2. Model Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lasmar, R.B.; Barrozo, P.R.M.; de Oliveira, M.A.P.; Coutinho, E.S.F.; Dias, R. Validation of hysteroscopic view in cases of endometrial hyperplasia and cancer in patients with abnormal uterine bleeding. J. Minim. Invasive Gynecol. 2006, 13, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, R.; Tinelli, F.G.; Cicinelli, E.; Malvasi, A.; Tinelli, A. The role of hysteroscopy with eye-directed biopsy in postmenopausal women with uterine bleeding and endometrial atrophy. Menopause 2008, 15, 737–742. [Google Scholar] [CrossRef]
- Angioni, S.; Loddo, A.; Milano, F.; Piras, B.; Minerba, L.; Melis, G.B. Detection of benign intracavitary lesions in postmenopausal women with abnormal uterine bleeding: A prospective comparative study on outpatient hysteroscopy and blind biopsy. J. Minim. Invasive Gynecol. 2008, 15, 87–91. [Google Scholar] [CrossRef]
- Garuti, G.; Cellani, F.; Garzia, D.; Colonnelli, M.; Luerti, M. Accuracy of hysteroscopic diagnosis of endometrial hyperplasia: A retrospective study of 323 patients. J. Minim. Invasive Gynecol. 2005, 12, 247–253. [Google Scholar] [CrossRef]
- Bignardi, T.; Bosch, T.V.D.; Condous, G. Abnormal uterine and post-menopausal bleeding in the acute gynaecology unit. Best Pract. Res. Clin. Obstet. Gynaecol. 2009, 23, 595–607. [Google Scholar] [CrossRef] [PubMed]
- Dreisler, E.; Poulsen, L.G.; Antonsen, S.L.; Ceausu, I.; Depypere, H.; Erel, C.T.; Lambrinoudaki, I.; Pérez-López, F.R.; Simoncini, T.; Tremollieres, F.; et al. EMAS clinical guide: Assessment of the endometrium in peri and postmenopausal women. Maturitas 2013, 75, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Bosch, T.V.D.; Ameye, L.; Van Schoubroeck, D.; Bourne, T.; Timmerman, D. Intra-cavitary uterine pathology in women with abnormal uterine bleeding: A prospective study of 1220 women. Facts Views Vis. ObGyn 2015, 7, 17–24. [Google Scholar]
- Shang, M.; Zhang, W. Predictive factors of endometrial lesions in patients with abnormal uterine bleeding. Eur. J. Obstet. Gynecol. Reprod. Biol. 2023, 288, 67–72. [Google Scholar] [CrossRef]
- Garuti, G.; Angioni, S.; Mereu, L.; Calzolari, S.; Mannini, L.; Scrimin, F.; Casadio, P.; De Alberti, D.; Nappi, L.; Busato, E.; et al. Hysteroscopic view with targeted biopsy in the assessment of endometrial carcinoma. What is the rate of underestimatated diagnosis? The results of a multicenter Italian trial. Gynecol. Surg. 2020, 17, 10. [Google Scholar] [CrossRef]
- Jiang, Y.; Yang, M.; Wang, S.; Li, X.; Sun, Y. Emerging role of deep learning-based artificial intelligence in tumor pathology. Cancer Commun. 2020, 40, 154–166. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, S.; Zhang, S.; Wang, M.; Ding, Y.; Fang, J.; Qian, W.; Liu, Z.; Sun, K.; Jin, Y.; et al. Development of a Deep Learning Model to Identify Lymph Node Metastasis on Magnetic Resonance Imaging in Patients with Cervical Cancer. JAMA Netw. Open 2020, 3, e2011625. [Google Scholar] [CrossRef]
- Sone, K.; Toyohara, Y.; Taguchi, A.; Miyamoto, Y.; Tanikawa, M.; Uchino-Mori, M.; Iriyama, T.; Tsuruga, T.; Osuga, Y. Application of artificial intelligence in gynecologic malignancies: A review. J. Obstet. Gynaecol. Res. 2021, 47, 2577–2585. [Google Scholar] [CrossRef] [PubMed]
- Chlap, P.; Min, H.; Vandenberg, N.; Dowling, J.; Holloway, L.; Haworth, A. A review of medical image data augmentation techniques for deep learning applications. J. Med. Imaging Radiat. Oncol. 2021, 65, 545–563. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016; Available online: http://www.deeplearningbook.org (accessed on 20 March 2024).
- Lundervold, A.S.; Lundervold, A. An overview of deep learning in medical imaging focusing on MRI. Z. Für Med. Phys. 2018, 29, 102–127. [Google Scholar] [CrossRef]
- Takahashi, Y.; Sone, K.; Noda, K.; Yoshida, K.; Toyohara, Y.; Kato, K.; Inoue, F.; Kukita, A.; Taguchi, A.; Nishida, H.; et al. Automated system for diagnosing endometrial cancer by adopting deep-learning technology in hysteroscopy. PLoS ONE 2021, 16, e0248526. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Z.; Zhang, J.; Wang, C.; Wang, Y.; Chen, H.; Shan, L.; Huo, J.; Gu, J.; Ma, X. Deep learning model for classifying endometrial lesions. J. Transl. Med. 2021, 19, 10. [Google Scholar] [CrossRef]
- Sarno, L.; Neola, D.; Carbone, L.; Saccone, G.; Carlea, A.; Miceli, M.; Iorio, G.G.; Mappa, I.; Rizzo, G.; Di Girolamo, R.; et al. Use of artificial intelligence in obstetrics: Not quite ready for prime time. Am. J. Obstet. Gynecol. MFM 2023, 5, 100792. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; De Vet, H.C.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]
- Digging into Detectron 2—Part 1|by Hiroto Honda|Medium. Available online: https://medium.com/@hirotoschwert/digging-into-detectron-2-47b2e794fabd (accessed on 18 March 2024).
- Revel, A.; Shushan, A. Investigation of the infertile couple: Hysteroscopy with endometrial biopsy is the gold standard investigation for abnormal uterine bleeding. Hum. Reprod. 2002, 17, 1947–1949. [Google Scholar] [CrossRef]
- Yang, L.C.; Chaudhari, A. The Use of Hysteroscopy for the Diagnosis and Treatment of Intrauterine Pathology: ACOG Committee Opinion, Number 800. Obstetrics and gynecology. Obstet. Gynecol. 2020, 135, e138–e148. [Google Scholar] [CrossRef]
- Garuti, G.; Sagrada, P.F.; Frigoli, A.; Fornaciari, O.; Finco, A.; Mirra, M.; Soligo, M. Hysteroscopic biopsy compared with endometrial curettage to assess the preoperative rate of atypical hyperplasia underestimating endometrial carcinoma. Arch. Gynecol. Obstet. 2023, 308, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Zhao, A.; Du, X.; Yuan, S.; Shen, W.; Zhu, X.; Wang, W. Automated Detection of Endometrial Polyps from Hysteroscopic Videos Using Deep Learning. Diagnostics 2023, 13, 1409. [Google Scholar] [CrossRef] [PubMed]
- Reznak, L.; Kudela, M. Comparison of ultrasound with hysteroscopic and histological findings for intrauterine assessment. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czechoslov. 2018, 162, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Casadio, P.; Raffone, A.; Travaglino, A.; Raimondo, D.; Zizolfi, B.; Armano, G.; Buonaiuto, R.; Insabato, L.; Mollo, A.; Seracchioli, R.; et al. Oncologic outcomes of conservative treatment of atypical polypoid adenomyoma of the uterus: A two-center experience. Int. J. Gynecol. Obstet. 2022, 159, 79–85. [Google Scholar] [CrossRef]
- Smorgick, N.; Barel, O.; Fuchs, N.; Ben-Ami, I.; Pansky, M.; Vaknin, Z. Hysteroscopic management of retained products of conception: Meta-analysis and literature review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 173, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Croce, S.; Devouassoux-Shisheboran, M.; Pautier, P.; Ray-Coquard, I.; Treilleux, I.; Neuville, A.; Arnould, L.; Just, P.-A.; Belda, M.A.L.F.; Averous, G.; et al. Uterine sarcomas and rare uterine mesenchymal tumors with malignant potential. Diagnostic guidelines of the French Sarcoma Group and the Rare Gynecological Tumors Group. Gynecol. Oncol. 2022, 167, 373–389. [Google Scholar] [CrossRef]
- Casadio, P.; Magnarelli, G.; La Rosa, M.; Alletto, A.; Arena, A.; Fontana, E.; Morra, C.; Talamo, M.R.; Fabbri, M.; Giovannico, K.; et al. Uterine Fundus Remodeling after Hysteroscopic Metroplasty: A Prospective Pilot Study. J. Clin. Med. 2021, 10, 260. [Google Scholar] [CrossRef]


{kind=link}
| Hyperparameter | Sampling Method | Range/Options |
|---|---|---|
| Learning Rate (lr) | Log Uniform Distribution | 1 × 10−5 to 1 × 10−2 |
| RPN Loss Weight | Uniform Distribution | 0 to 1 |
| ROI Heads Loss Weight | Uniform Distribution | 0 to 1 |
| ROIs Per Image | Categorical | 32, 64, 128, 256, 512 |
| Random Brightness * | Uniform Distribution | 0 to 1 |
| Random Contrast * | Uniform Distribution | 0 to 1 |
| Repeat Factor Th ** | Uniform Distribution | 0.1 to 1 |
| Hyperparameter | Value |
|---|---|
| Learning Rate (lr) | 0.0015884830145038431 |
| ROIs Per Image | 256 |
| RPN Loss Weight | 0.8635956597511065 |
| ROI Heads Loss Weight | 0.5995106068965408 |
| Repeat Factor Th ** | 0.45776224748623207 |
| Random Contrast * | 0.2 |
| Random Brightness * | 0.2 |
| Patients (n = 266) | Benign Focal Lesions (n = 186) | Benign Diffuse Lesions (n = 25) | Preneoplastic and Neoplastic Lesions (n = 55) | |
|---|---|---|---|---|
| Age, mean (range) | 53.5 (27–87) | 52 (27–83) | 45 (29–76) | 62.2 (39–87) |
| Menopausal status, n (%) | 132 (49.62) | 83 (44.62) | 5 (20) | 44 (80) |
| Abnormal uterine bleeding, n (%) | 118 (44.36) | 69 (37.09) | 7 (28) | 42 (76.3) |
| Hormonal therapy, n(%) | 24 (9.02) | 13 (6.98) | 0 (0) | 11 (20) |
| Tamoxifen users, n (%) | 6 (2.25) | 5 (2.68) | 1 (4) | 0 (0) |
| Patients (n) | Images (n) | Patients in Training Set (n) | Images in Training Set (n) | Patients in Validation Set (n) | Images in Validation Set (n) | Patients in Testing Set (n) | Images in Testing Set (n) | |
|---|---|---|---|---|---|---|---|---|
| Benign focal lesion | 186 | 1110 | 111 | 667 | 37 | 273 | 38 | 170 |
| Benign diffuse lesion | 25 | 140 | 14 | 82 | 7 | 38 | 7 | 20 |
| Preneoplastic and neoplastic lesion | 55 | 250 | 32 | 159 | 10 | 35 | 10 | 56 |
| Total | 266 | 1500 | 157 | 908 | 54 | 355 | 55 | 237 |
| Precision | Recall | Specificity | F1 | Accuracy | |
|---|---|---|---|---|---|
| Benign focal lesion | 82.96 ± 0.54 | 92.64 ± 2.14 | 36.85 ± 7.18 | 87.29 ± 0.92 | 79.55 ± 1.29 |
| Benign diffuse lesion | 29.93 ± 8.58 | 21.17 ± 5.83 | 97.13 ± 1.45 | 28.27 ± 4.02 | 90.1 ± 0.91 |
| Pre-neoplastic/neoplastic lesion | 51.7 ± 6.64 | 35.16 ± 7.67 | 94.32 ± 1.81 | 42.19 ± 5.32 | 85.63 ± 1.16 |
| Overall | 63.03 ± 6.14 | 49.66 ± 5.5 | 76.1 ± 3.67 | 52.58 ± 3.43 | 85.09 ± 1.18 |
| Precision | Recall | Specificity | F1 | Accuracy | |
|---|---|---|---|---|---|
| Benign focal lesion | 84.25 ± 1.18 | 94.31 ± 2.24 | 39.59 ± 6.79 | 88.8 ± 0.97 | 81.97 ± 1.15 |
| Benign diffuse lesion | 48.78 ± 6.22 | 29.92 ± 5.99 | 96.2 ± 1.45 | 34.45 ± 4.65 | 90.61 ± 1.14 |
| Pre-neoplastic/neoplastic lesion | 67.97 ± 5.51 | 32.19 ± 7.06 | 96.52 ± 1.35 | 43.01 ± 5.43 | 87.07 ± 1 |
| Overall | 67 ± 4.4 | 52.14 ± 5.37 | 77.44 ± 3.37 | 55.42 ± 3.76 | 86.55 ± 1.15 |
| Clinical Factors | Detection | Precision | Recall | F1 |
|---|---|---|---|---|
| No | 66.41 ± 3.39 | 88.27 ± 2.54 | 72.87 ± 3.5 | 79.43 ± 2.55 |
| Yes | 66.58 ± 4.64 | 86.82 ± 3.34 | 73.49 ± 4.56 | 79.18 ± 3.62 |
| Lesion | Precision | Recall | Specificity | F1 | Accuracy |
|---|---|---|---|---|---|
| Benign focal lesion | 85.23 | 94.07 | 46.34 | 89.44 | 82.95 |
| Benign diffuse lesion | 37.5 | 50 | 93.9 | 42.86 | 90.91 |
| Pre-neoplastic/neoplastic lesion | 72.73 | 27.59 | 97.96 | 40 | 86.36 |
| Overall | 80.11 | 80.11 | 90.06 | 80.11 | 86.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raimondo, D.; Raffone, A.; Salucci, P.; Raimondo, I.; Capobianco, G.; Galatolo, F.A.; Cimino, M.G.C.A.; Travaglino, A.; Maletta, M.; Ferla, S.; et al. Detection and Classification of Hysteroscopic Images Using Deep Learning. Cancers 2024, 16, 1315. https://doi.org/10.3390/cancers16071315
Raimondo D, Raffone A, Salucci P, Raimondo I, Capobianco G, Galatolo FA, Cimino MGCA, Travaglino A, Maletta M, Ferla S, et al. Detection and Classification of Hysteroscopic Images Using Deep Learning. Cancers. 2024; 16(7):1315. https://doi.org/10.3390/cancers16071315
Chicago/Turabian StyleRaimondo, Diego, Antonio Raffone, Paolo Salucci, Ivano Raimondo, Giampiero Capobianco, Federico Andrea Galatolo, Mario Giovanni Cosimo Antonio Cimino, Antonio Travaglino, Manuela Maletta, Stefano Ferla, and et al. 2024. "Detection and Classification of Hysteroscopic Images Using Deep Learning" Cancers 16, no. 7: 1315. https://doi.org/10.3390/cancers16071315