
Association between Cholecystectomy and the Incidence of Pancreaticobiliary Cancer after Endoscopic Choledocholithiasis Management

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
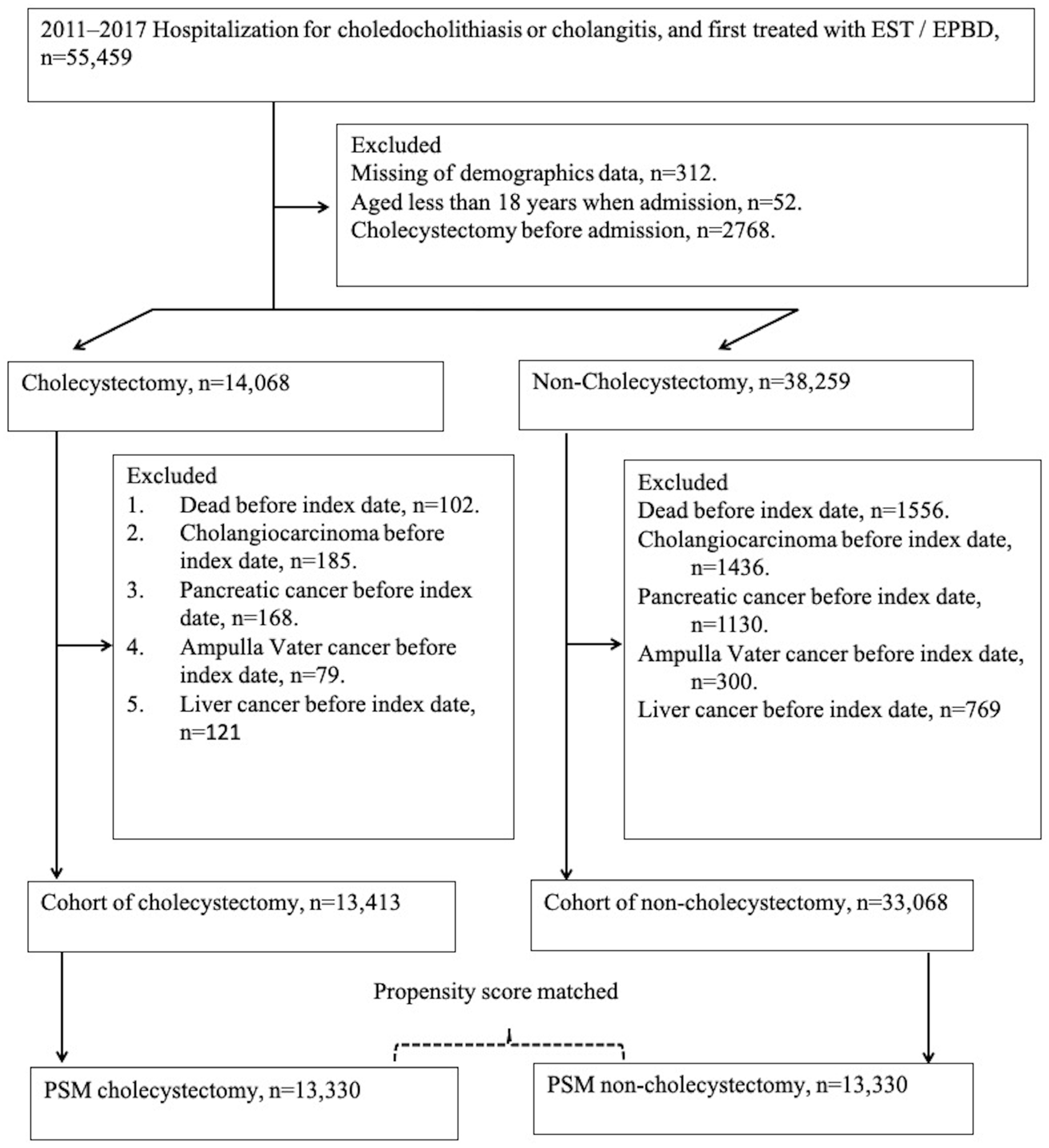
2.1. Definition of Study Population
2.2. Definition of Study Covariates
2.3. Identification of Study Events
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baiu, I.; Hawn, M.T. Choledocholithiasis. JAMA 2018, 320, 1506. [Google Scholar] [CrossRef]
- Pogorelic, Z.; Aralica, M.; Jukic, M.; Zitko, V.; Despot, R.; Juric, I. Gallbladder Disease in Children: A 20-year Single-center Experience. Indian Pediatr. 2019, 56, 384–386. [Google Scholar] [CrossRef]
- Huang, R.J.; Barakat, M.T.; Girotra, M.; Banerjee, S. Practice Patterns for Cholecystectomy After Endoscopic Retrograde Cholangiopancreatography for Patients With Choledocholithiasis. Gastroenterology 2017, 153, 762–771.e2. [Google Scholar] [CrossRef]
- Wang, C.-C.; Tsai, M.-C.; Wang, Y.-T.; Yang, T.-W.; Chen, H.-Y.; Sung, W.-W.; Huang, S.-M.; Tseng, M.-H.; Lin, C.-C. Role of Cholecystectomy in Choledocholithiasis Patients Underwent Endoscopic Retrograde Cholangiopancreatography. Sci. Rep. 2019, 9, 2168. [Google Scholar] [CrossRef]
- Khan, M.A.; Khan, Z.; Tombazzi, C.R.; Gadiparthi, C.; Lee, W.; Wilcox, C.M. Role of Cholecystectomy After Endoscopic Sphincterotomy in the Management of Choledocholithiasis in High-risk Patients: A Systematic Review and Meta-Analysis. J. Clin. Gastroenterol. 2018, 52, 579–589. [Google Scholar] [CrossRef]
- Lau, J.Y.; Leow, C.; Fung, T.M.; Suen, B.; Yu, L.; Lai, P.B.; Lam, Y.; Ng, E.K.; Lau, W.Y.; Chung, S.S.; et al. Cholecystectomy or Gallbladder In Situ After Endoscopic Sphincterotomy and Bile Duct Stone Removal in Chinese Patients. Gastroenterology 2006, 130, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, L.; Freedman, N.D.; Engels, E.A.; Warren, J.L.; Castro, F.; Koshiol, J. Gallstones, cholecystectomy, and risk of digestive system cancers. Am. J. Epidemiol. 2014, 179, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Siyin, S.T.; Yao, N.; Xu, G.; Chen, Y.T.; Duan, N.; Liu, S. Risk of primary liver cancer associated with gallstones and cholecystectomy: A competing risks analysis. Medicine 2020, 99, e22428. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Engels, E.A.; Landgren, O.; Chiao, E.; Henderson, L.; Amaratunge, H.C.; Giordano, T.P. Risk of hepatobiliary and pancreatic cancers after hepatitis C virus infection: A population-based study of U.S. veterans. Hepatology 2009, 49, 116–123. [Google Scholar] [CrossRef]
- Urbach, D.R.; Swanstrom, L.L.; Khajanchee, Y.S.; Hansen, P.D. Incidence of cancer of the pancreas, extrahepatic bile duct and ampulla of Vater in the United States, before and after the introduction of laparoscopic cholecystectomy. Am. J. Surg. 2001, 181, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Chow, W.H.; Johansen, C.; Gridley, G.; Mellemkjær, L.; Olsen, J.H. Gallstones, cholecystectomy and risk of cancers of the liver, biliary tract and pancreas. Br. J. Cancer 1999, 79, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Hu, J.; Feng, B.; Wang, W.; Yao, G.; Zhai, J.; Li, X. Increased Risk of Pancreatic Cancer Related to Gallstones and Cholecystectomy: A Systematic Review and Meta-Analysis. Pancreas 2016, 45, 503–509. [Google Scholar] [CrossRef]
- Labib, P.L.; Goodchild, G.; Pereira, S.P. Molecular Pathogenesis of Cholangiocarcinoma. BMC Cancer 2019, 19, 185. [Google Scholar] [CrossRef]
- Doherty, B.; Nambudiri, V.E.; Palmer, W.C. Update on the Diagnosis and Treatment of Cholangiocarcinoma. Curr. Gastroenterol. Rep. 2017, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Tseng, M.; Wu, S.; Yang, T.; Chen, H.; Sung, W.; Su, C.; Wang, Y.; Chen, W.; Lai, H.; et al. Symptomatic cholelithiasis patients have an increased risk of pancreatic cancer: A population-based study. J. Gastroenterol. Hepatol. 2021, 36, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Coats, M.; Shimi, S.M. Cholecystectomy and the risk of alimentary tract cancers: A systematic review. World J. Gastroenterol. 2015, 21, 3679–3693. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Lovrić, M.; Jukić, M.; Perko, Z. The Laparoscopic Cholecystectomy and Common Bile Duct Exploration: A Single-Step Treatment of Pediatric Cholelithiasis and Choledocholithiasis. Children 2022, 9, 1583. [Google Scholar] [CrossRef]
- Oliveira-Cunha, M.; Dennison, A.R.; Garcea, G. Late Complications After Endoscopic Sphincterotomy. Surg. Laparosc. Endosc. Percutaneous Tech. 2016, 26, 1–5. [Google Scholar] [CrossRef]
- Van Dyke, A.L.; Shiels, M.S.; Jones, G.S.; Pfeiffer, R.M.; Petrick, J.L.; Beebe-Dimmer, J.L.; Koshiol, J. Biliary tract cancer incidence and trends in the United States by demographic group, 1999-2013. Cancer 2019, 125, 1489–1498. [Google Scholar] [CrossRef]
- Wang, C.-C.; Tseng, M.-H.; Wu, S.-W.; Yang, T.-W.; Chen, H.-Y.; Sung, W.-W.; Su, C.-C.; Wang, Y.-T.; Lin, C.-C.; Tsai, M.-C. Cholecystectomy reduces subsequent cholangiocarcinoma risk in choledocholithiasis patients undergoing endoscopic intervention. World J. Gastrointest. Oncol. 2020, 12, 1381–1393. [Google Scholar] [CrossRef]
- Hsieh, C.-Y.; Su, C.-C.; Shao, S.-C.; Sung, S.-F.; Lin, S.-J.; Kao Yang, Y.-H.; Lai, E.C.-C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef]
- Singhal, T.; Balakrishnan, S.; Grandy-Smith, S.; Hunt, J.; Asante, M.; El-Hasani, S. Gallstones: Best served hot. JSLS 2006, 10, 332–335. [Google Scholar]
- Austin, P.C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2014, 33, 1242–1258. [Google Scholar] [CrossRef]
- Sekiya, S.; Suzuki, A. Intrahepatic cholangiocarcinoma can arise from Notch-mediated conversion of hepatocytes. J. Clin. Investig. 2012, 122, 3914–3918. [Google Scholar] [CrossRef]
- Murphy, G.; Michel, A.; Taylor, P.R.; Albanes, D.; Weinstein, S.J.; Virtamo, J.; Freedman, N.D. Association of seropositivity to Helicobacter species and biliary tract cancer in the ATBC study. Hepatology 2014, 60, 1963–1971. [Google Scholar] [CrossRef]
- Fukuda, K.; Kuroki, T.; Tajima, Y.; Tsuneoka, N.; Kitajima, T.; Matsuzaki, S.; Furui, J.; Kanematsu, T. Comparative analysis of Helicobacter DNAs and biliary pathology in patients with and without hepatobiliary cancer. Carcinogenesis 2002, 23, 1927–1931. [Google Scholar] [CrossRef]
- Jing, W.; Jin, G.; Zhou, X.; Zhou, Y.Q.; Zhang, Y.J.; Shao, C.H.; Hu, X.G. Diabetes mellitus and increased risk of cholangiocarcinoma: A meta-analysis. Eur. J. Cancer Prev. 2012, 21, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.F.; Zhao, X.H. Diabetes mellitus and increased risk of extrahepatic cholangiocarcinoma: A meta-analysis. Hepatogastroenterology 2013, 60, 684–687. [Google Scholar] [PubMed]
- Lipsett, P.A.; Pitt, H.A.; Colombani, P.M.; Boitnott, J.K.; Cameron, J.L. Choledochal Cyst Disease A Changing Pattern of Presentation. Ann. Surg. 1994, 220, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Wirth, T.C.; Kuebler, J.F.; Petersen, C.; Ure, B.M.; Madadi-Sanjani, O. Choledochal Cyst and Malignancy: A Plea for Lifelong Follow-Up. Eur. J. Pediatr. Surg. 2019, 29, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Palmer, W.C.; Patel, T. Are common factors involved in the pathogenesis of primary liver cancers? A meta-analysis of risk factors for intrahepatic cholangiocarcinoma. J. Hepatol. 2012, 57, 69–76. [Google Scholar] [CrossRef]
- Chapman, M.H.; Webster, G.J.; Bannoo, S.; Johnson, G.J.; Wittmann, J.; Pereira, S.P. Cholangiocarcinoma and dominant strictures in patients with primary sclerosing cholangitis: A 25-year single-centre experience. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1051–1058. [Google Scholar] [CrossRef]
- Watanapa, P.; Watanapa, W.B. Liver fluke-associated cholangiocarcinoma. Br. J. Surg. 2002, 89, 962–970. [Google Scholar] [CrossRef]
- Rassen, J.A.; Shelat, A.A.; Myers, J.; Glynn, R.J.; Rothman, K.J.; Schneeweiss, S. One-to-many propensity score matching in cohort studies. Pharmacoepidemiol. Drug Saf. 2012, 21, 69–80. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Li, Y.; Guo, L.; Mao, J.; Jiao, Z.; Guo, J.; Zhang, J.; Zhao, J. Cholelithiasis, cholecystectomy and risk of hepatocellular carcinoma: A meta-analysis. J. Cancer Res. Ther. 2014, 10, 834–838. [Google Scholar] [CrossRef]
- Wang, Y.; Xie, L.F.; Lin, J. Gallstones and cholecystectomy in relation to risk of liver cancer. Eur. J. Cancer Prev. 2019, 28, 61–67. [Google Scholar] [CrossRef]
- Chen, Y.K.; Yeh, J.-H.; Lin, C.-L.; Peng, C.-L.; Sung, F.-C.; Hwang, I.-M.; Kao, C.-H. Cancer risk in patients with cholelithiasis and after cholecystectomy: A nationwide cohort study. J. Gastroenterol. 2014, 49, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Nordenstedt, H.; Mattsson, F.; El-Serag, H.; Lagergren, J. Gallstones and cholecystectomy in relation to risk of intra- and extrahepatic cholangiocarcinoma. Br. J. Cancer 2012, 106, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Wang, Y.; Huang, H.; Bian, J.; Wang, A.; Long, J.; Zheng, Y.; Sang, X.; Xu, Y.; Lu, X.; et al. Systematic review and meta-analysis: Cholecystectomy and the risk of cholangiocarcinoma. Oncotarget 2017, 8, 59648–59657. [Google Scholar] [CrossRef]
- Ahn, H.S.; Kim, H.J.; Kang, T.U.; Park, S.M. Cholecystectomy reduces the risk of cholangiocarcinoma in patients with complicated gallstones, but has negligible effect on hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2022, 37, 669–677. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Non-Cholecystectomy | Cholecystectomy | ASD | |
|---|---|---|---|
| n | 13,330 | 13,330 | |
| Index year | 0.000 | ||
| 2011, 2012 | 2932 (22.00%) | 2911 (21.84%) | |
| 2013, 2014 | 3615 (27.12%) | 3585 (26.89%) | |
| 2015, 2016 | 4144 (31.09%) | 4189 (31.43%) | |
| 2017, 2018 | 2639 (19.80%) | 2645 (19.84%) | |
| Sex | 0.004 | ||
| Male | 7111 (53.35%) | 7047 (52.87%) | |
| Female | 6219 (46.65%) | 6283 (47.13%) | |
| Age | 0.000 | ||
| <50 | 3662 (27.47%) | 3636 (27.28%) | |
| 50–60 | 2516 (18.87%) | 2510 (18.83%) | |
| 60–70 | 2934 (22.01%) | 2988 (22.42%) | |
| ≥70 | 4218 (31.64%) | 4196 (31.48%) | |
| Urbanization | 0.000 | ||
| High urbanization | 3928 (29.47%) | 3872 (29.05%) | |
| Moderate urbanization | 4147 (31.11%) | 4160 (31.21%) | |
| Developing town | 2128 (15.96%) | 2094 (15.71%) | |
| General town | 1833 (13.75%) | 1848 (13.86%) | |
| Aged town | 368 (2.76%) | 367 (2.75%) | |
| Agriculture town | 605 (4.54%) | 636 (4.77%) | |
| Village | 321 (2.41%) | 353 (2.65%) | |
| Insured category | 0.083 | ||
| Government | 701 (5.26%) | 721 (5.41%) | |
| Privately held company | 7235 (54.28%) | 7124 (53.44%) | |
| Agricultural organizations | 2379 (17.85%) | 2387 (17.91%) | |
| Low-income | 90 (0.68%) | 103 (0.77%) | |
| Non-labor force | 2737 (20.53%) | 2776 (20.83%) | |
| Others | 188 (1.41%) | 219 (1.64%) | |
| Co-morbidity | |||
| Chronic hepatitis B | 1029 (7.72%) | 1134 (8.51%) | 0.029 |
| Chronic hepatitis C | 406 (3.05%) | 465 (3.49%) | 0.025 |
| Helicobacter infection | 397 (2.98%) | 466 (3.50%) | 0.029 |
| Diabetes mellitus | 4222 (31.67%) | 4210 (31.58%) | 0.002 |
| CKD | 1276 (9.57%) | 1270 (9.53%) | 0.002 |
| Congenital cystic disease of liver | 93 (0.70%) | 90 (0.68%) | 0.003 |
| Inflammatory bowel diseases | 375 (2.81%) | 427 (3.20%) | 0.023 |
| Liver cirrhosis | 516 (3.87%) | 510 (3.83%) | 0.002 |
| Non-Cholecystectomy | Cholecystectomy | p Value | |
|---|---|---|---|
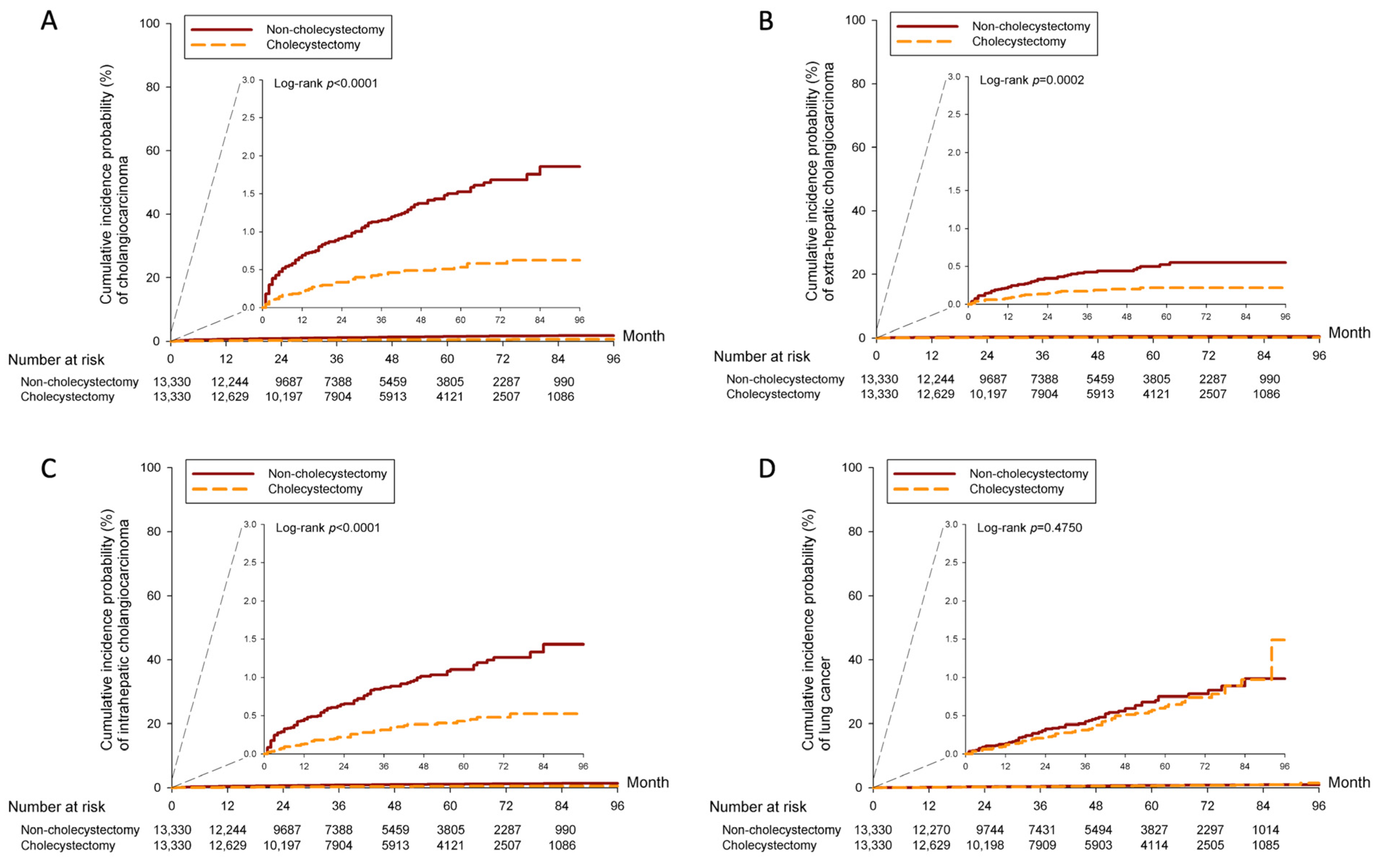
| Cholangiocarcinoma | |||
| Observed person-years | 47,718.8 | 50,262.1 | |
| Incident cases | 168 | 60 | |
| Incidence rate † | 3.52 (3.03–4.1) | 1.19 (0.93–1.54) | |
| Crude HR (95% CI) | Reference | 0.34 (0.26–0.46) | <0.0001 |
| Adjusted HR (95% CI) | Reference | 0.34 (0.25–0.46) | <0.0001 |
| ICC | |||
| Observed person-years | 47,768.3 | 50,276.6 | |
| Incident cases | 117 | 46 | |
| Incidence rate † | 2.45 (2.04–2.94) | 0.91 (0.69–1.22) | |
| Crude HR (95% CI) | Reference | 0.38 (0.27–0.53) | <0.0001 |
| Adjusted HR (95% CI) | Reference | 0.37 (0.26–0.52) | <0.0001 |
| ECC | |||
| Observed person-years | 47,825.8 | 50,286.9 | |
| Incident cases | 52 | 24 | |
| Incidence rate † | 1.09 (0.83–1.43) | 0.48 (0.32–0.71) | |
| Crude HR (95% CI) | Reference | 0.45 (0.28–0.73) | 0.0011 |
| Adjusted HR (95% CI) | Reference | 0.44 (0.27–0.72) | 0.0010 |
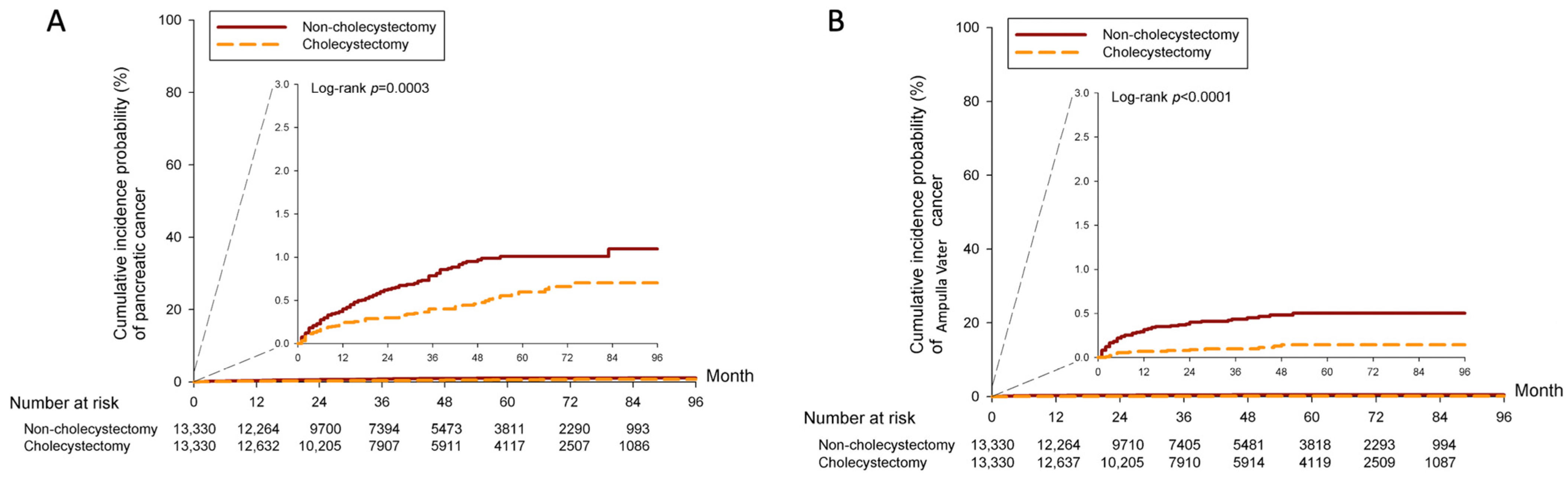
| Pancreatic cancer | |||
| Observed person-years | 47,785.9 | 50,273.8 | |
| Incident cases | 101 | 61 | |
| Incidence rate † | 2.11 (1.74–2.57) | 1.21 (0.94–1.56) | |
| Crude HR (95% CI) | Reference | 0.58 (0.43–0.80) | 0.0009 |
| Adjusted HR (95% CI) | Reference | 0.58 (0.42–0.79) | 0.0007 |
| Ampulla Vater cancer | |||
| Observed person-years | 47,829.0 | 50,289.0 | |
| Incident cases | 49 | 15 | |
| Incidence rate † | 1.02 (0.77–1.36) | 0.3 (0.18–0.49) | |
| Crude HR (95% CI) | Reference | 0.30 (0.17–0.53) | <0.0001 |
| Adjusted HR (95% CI) | Reference | 0.30 (0.17–0.53) | <0.0001 |
| Lung cancer | |||
| Observed person-years | 47,765.7 | 50,171.8 | |
| Incident cases | 135 | 96 | |
| Incidence rate † | 2.83 (2.39–3.35) | 1.91 (1.57–2.34) | |
| Crude HR (95% CI) | Reference | 0.88 (0.63–1.24) | 0.4753 |
| Adjusted HR (95% CI) | Reference | 0.86 (0.61–1.21) | 0.3737 |
| Cholecystectomy aHR (95% CI) | |
|---|---|
| Excluded Patients Followed <24 months | |
| Incidence rate | |
| Cholangiocarcinoma | 0.30 (0.17–0.51) |
| ICC | 0.44 (0.25–0.75) |
| ECC | 0.46 (0.18–1.14) |
| Pancreatic cancer | 0.84 (0.47–1.48) |
| Ampulla Vater cancer | 0.48 (0.16–1.40) |
| Lung cancer | 1.05 (0.65–1.68) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-C.; Huang, J.-Y.; Weng, L.-H.; Hsu, Y.-C.; Sung, W.-W.; Huang, C.-Y.; Lin, C.-C.; Wei, J.C.-C.; Tsai, M.-C. Association between Cholecystectomy and the Incidence of Pancreaticobiliary Cancer after Endoscopic Choledocholithiasis Management. Cancers 2024, 16, 977. https://doi.org/10.3390/cancers16050977
Wang C-C, Huang J-Y, Weng L-H, Hsu Y-C, Sung W-W, Huang C-Y, Lin C-C, Wei JC-C, Tsai M-C. Association between Cholecystectomy and the Incidence of Pancreaticobiliary Cancer after Endoscopic Choledocholithiasis Management. Cancers. 2024; 16(5):977. https://doi.org/10.3390/cancers16050977
Chicago/Turabian StyleWang, Chi-Chih, Jing-Yang Huang, Li-Han Weng, Yao-Chun Hsu, Wen-Wei Sung, Chao-Yen Huang, Chun-Che Lin, James Cheng-Chung Wei, and Ming-Chang Tsai. 2024. "Association between Cholecystectomy and the Incidence of Pancreaticobiliary Cancer after Endoscopic Choledocholithiasis Management" Cancers 16, no. 5: 977. https://doi.org/10.3390/cancers16050977