
Subtypes of Melanomas Associated with Different Degrees of Actinic Elastosis in Conventional Histology, Irrespective of Age and Body Site, Suggesting Chronic Ultraviolet Light Exposure as Driver for Lentigo Maligna Melanoma and Nodular Melanoma
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
- Intermittent sun exposure and the tendency to develop multiple melanocytic nevi;
- Multiple sunburns during childhood and general sun sensitivity with freckling (ephelides);
- Chronic sun exposure and the development of multiple lentigines.
2. Materials and Methods
2.1. Patient Characteristics and Inclusion Criteria
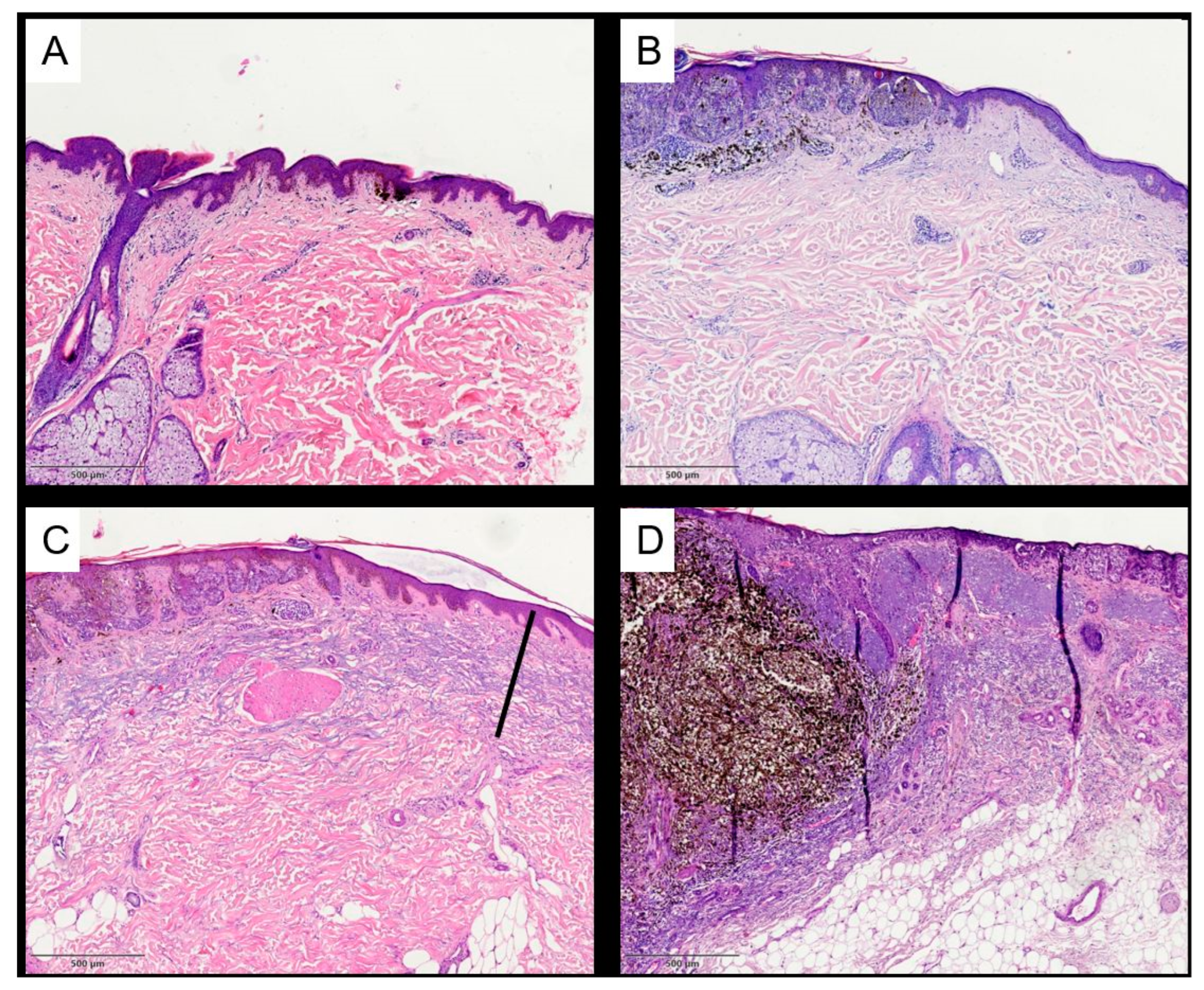
2.2. Histopathological Assessment
2.3. Statistical Analysis
2.4. Microscope and Digital Photography
3. Results
3.1. Clinical Characteristics and Histopathological Analysis: Nevi vs. Melanomas
3.2. Clinical Characteristics and Histopathological Analysis: Clinical Melanoma Subtypes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hendi, A.; Brodland, D.G.; Zitelli, J.A. Melanocytes in long-standing sun-exposed skin: Quantitative analysis using the MART-1 immunostain. Arch. Dermatol. 2006, 142, 871–876. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. WHO Classification of Skin Tumours, 4th ed.; Elder, D.E., Ed.; International Agency for Research on Cancer: Lyon, France, 2018; ISBN 9789283224402. [Google Scholar]
- Kurz, B.; Berneburg, M.; Singer, S. Sonnenschutz der menschlichen Haut: Grundlagen. Hautarzt 2022, 73, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Bastiaens, M.; Hoefnagel, J.; Westendorp, R.; Vermeer, B.-J.; Bouwes Bavinck, J.N. Solar lentigines are strongly related to sun exposure in contrast to ephelides. Pigment Cell Res. 2004, 17, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Praetorius, C.; Sturm, R.A.; Steingrimsson, E. Sun-induced freckling: Ephelides and solar lentigines. Pigment. Cell Melanoma Res. 2014, 27, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Krutmann, J.; Berneburg, M. Lichtalterung (Photoaging) der Haut: Was gibt es Neues? Hautarzt 2021, 72, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Dodd, A.T.; Morelli, J.; Mokrohisky, S.T.; Asdigian, N.; Byers, T.E.; Crane, L.A. Melanocytic nevi and sun exposure in a cohort of colorado children: Anatomic distribution and site-specific sunburn. Cancer Epidemiol. Biomark. Prev. 2007, 16, 2136–2143. [Google Scholar] [CrossRef]
- Gefeller, O.; Tarantino, J.; Lederer, P.; Uter, W.; Pfahlberg, A.B. The relation between patterns of vacation sun exposureand the development of acquired melanocytic nevi in German children 6–7 years of age. Am. J. Epidemiol. 2007, 165, 1162–1169. [Google Scholar] [CrossRef]
- Harth, Y.; Friedman-Birnbaum, R.; Linn, S. Influence of cumulative sun exposure on the prevalence of common acquired nevi. J. Am. Acad. Dermatol. 1992, 27, 21–24. [Google Scholar] [CrossRef]
- Schäfer, T.; Merkl, J.; Klemm, E.; Wichmann, H.-E.; Ring, J. The epidemiology of nevi and signs of skin aging in the adult general population: Results of the KORA-survey 2000. J. Investig. Dermatol. 2006, 126, 1490–1496. [Google Scholar] [CrossRef]
- Kennedy, C.; Bajdik, C.D.; Willemze, R.; de Gruijl, F.R.; Bouwes Bavinck, J.N. The influence of painful sunburns and lifetime sun exposure on the risk of actinic keratoses, seborrheic warts, melanocytic nevi, atypical nevi, and skin cancer. J. Investig. Dermatol. 2003, 120, 1087–1093. [Google Scholar] [CrossRef]
- Nikolaou, V.A.; Sypsa, V.; Stefanaki, I.; Gogas, H.; Papadopoulos, O.; Polydorou, D.; Plaka, M.; Tsoutsos, D.; Dimou, A.; Mourtzoukou, E.; et al. Risk associations of melanoma in a Southern European population: Results of a case/control study. Cancer Causes Control 2008, 19, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Hoersch, B.; Leiter, U.; Garbe, C. Is head and neck melanoma a distinct entity? A clinical registry-based comparative study in 5702 patients with melanoma. Br. J. Dermatol. 2006, 155, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Shannon, C.M.; Mehta, N.K.; Li, H.; Nguyen, S.A.; Koochakzadeh, S.; Elston, D.M.; Kaczmar, J.M.; Day, T.A. Anatomic Region of Cutaneous Melanoma Impacts Survival and Clinical Outcomes: A Population-Based Analysis. Cancers 2023, 15, 1229. [Google Scholar] [CrossRef] [PubMed]
- Whiteman, D.C.; Watt, P.; Purdie, D.M.; Hughes, M.C.; Hayward, N.K.; Green, A.C. Melanocytic nevi, solar keratoses, and divergent pathways to cutaneous melanoma. J. Natl. Cancer Inst. 2003, 95, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Anna, B.; Blazej, Z.; Jacqueline, G.; Andrew, C.J.; Jeffrey, R.; Andrzej, S. Mechanism of UV-related carcinogenesis and its contribution to nevi/melanoma. Expert Rev. Dermatol. 2007, 2, 451–469. [Google Scholar] [CrossRef] [PubMed]
- Akbani, R.; Akdemir, K.C.; Aksoy, B.A.; Albert, M.; Ally, A.; Amin, S.B.; Arachchi, H.; Arora, A.; Auman, J.T.; Ayala, B.; et al. Genomic Classification of Cutaneous Melanoma. Cell 2015, 161, 1681–1696. [Google Scholar] [CrossRef]
- Naldi, L.; Altieri, A.; Imberti, G.L.; Gallus, S.; Bosetti, C.; La Vecchia, C. Sun exposure, phenotypic characteristics, and cutaneous malignant melanoma. An analysis according to different clinico-pathological variants and anatomic locations (Italy). Cancer Causes Control 2005, 16, 893–899. [Google Scholar] [CrossRef]
- Kvaskoff, M.; Siskind, V.; Green, A.C. Risk factors for lentigo maligna melanoma compared with superficial spreading melanoma: A case-control study in Australia. Arch. Dermatol. 2012, 148, 164–170. [Google Scholar] [CrossRef]
- Gaudy-Marqueste, C.; Madjlessi, N.; Guillot, B.; Avril, M.-F.; Grob, J.-J. Risk factors in elderly people for lentigo maligna compared with other melanomas: A double case-control study. Arch. Dermatol. 2009, 145, 418–423. [Google Scholar] [CrossRef]
- Schreiber, M.M.; Moon, T.E.; Bozzo, P.D. Chronic solar ultraviolet damage associated with malignant melanoma of the skin. J. Am. Acad. Dermatol. 1984, 10, 755–759. [Google Scholar] [CrossRef]
- Drexler, K.; Drexler, H.; Karrer, S.; Landthaler, M.; Haferkamp, S.; Zeman, F.; Berneburg, M.; Niebel, D. Degree of Actinic Elastosis Is a Surrogate of Exposure to Chronic Ultraviolet Radiation and Correlates More Strongly with Cutaneous Squamous Cell Carcinoma than Basal Cell Carcinoma. Life 2023, 13, 811. [Google Scholar] [CrossRef] [PubMed]
- Mamalis, A.; Fiadorchanka, N.; Adams, L.; Serravallo, M.; Heilman, E.; Siegel, D.; Brody, N.; Jagdeo, J. An immunohistochemical panel to assess ultraviolet radiation-associated oxidative skin injury. J. Drugs Dermatol. 2014, 13, 574–578. [Google Scholar] [PubMed]
- Kvaskoff, M.; Pandeya, N.; Green, A.C.; Perry, S.; Baxter, C.; Davis, M.B.; Mortimore, R.; Westacott, L.; Wood, D.; Triscott, J.; et al. Solar elastosis and cutaneous melanoma: A site-specific analysis. Int. J. Cancer 2015, 136, 2900–2911. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Williamson, R.; Watt, P.; Hughes, M.C.; Green, A.C.; Whiteman, D.C. Sun exposure and host phenotype as predictors of cutaneous melanoma associated with neval remnants or dermal elastosis. Int. J. Cancer 2006, 119, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Pennie, M.L.; Soon, S.L.; Risser, J.B.; Veledar, E.; Culler, S.D.; Chen, S.C. Melanoma outcomes for Medicare patients: Association of stage and survival with detection by a dermatologist vs a nondermatologist. Arch. Dermatol. 2007, 143, 488–494. [Google Scholar] [CrossRef]
- Riegler, M.J.; Mannweiler, S.; Sturm, A.; Donnerer, A.; Darok, M.; Kopera, D. Thickness of actinic elastosis a surrogate marker of chronic UV-damage: A post mortem analysis of 41 cases. Dermatol. Ther. 2020, 33, e14037. [Google Scholar] [CrossRef]
- Moon, J.S.; Oh, C.H. Solar damage in skin tumors: Quantification of elastotic material. Dermatology 2001, 202, 289–292. [Google Scholar] [CrossRef]
- Vollmer, R.T. Solar elastosis in cutaneous melanoma. Am. J. Clin. Pathol. 2007, 128, 260–264. [Google Scholar] [CrossRef]
- Thomas, N.E.; Kricker, A.; From, L.; Busam, K.; Millikan, R.C.; Ritchey, M.E.; Armstrong, B.K.; Lee-Taylor, J.; Marrett, L.D.; Anton-Culver, H.; et al. Associations of cumulative sun exposure and phenotypic characteristics with histologic solar elastosis. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2932–2941. [Google Scholar] [CrossRef]
- Kaskel, P.; Lange, U.; Sander, S.; Huber, M.A.; Utikal, J.; Leiter, U.; Krähn, G.; Meurer, M.; Kron, M. Ultraviolet exposure and risk of melanoma and basal cell carcinoma in Ulm and Dresden, Germany. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 134–142. [Google Scholar] [CrossRef]
- Titus, L.; Barnhill, R.L.; Lott, J.P.; Piepkorn, M.W.; Elder, D.E.; Frederick, P.D.; Nelson, H.D.; Carney, P.A.; Knezevich, S.R.; Weinstock, M.A.; et al. The influence of tumor regression, solar elastosis, and patient age on pathologists’ interpretation of melanocytic skin lesions. Lab. Investig. 2017, 97, 187–193. [Google Scholar] [CrossRef]
- Konopinski, J.C.; Danialan, R.; Torres-Cabala, C.A.; Tetzlaff, M.T.; Nagarajan, P.; Curry, J.L.; Ivan, D.; Prieto, V.G.; Aung, P.P. Melanoma coexisting with solar elastosis: A potential pitfall in the differential diagnosis between nevus and melanoma. Hum. Pathol. 2019, 84, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Millán-Esteban, D.; Peña-Chilet, M.; García-Casado, Z.; Manrique-Silva, E.; Requena, C.; Bañuls, J.; López-Guerrero, J.A.; Rodríguez-Hernández, A.; Traves, V.; Dopazo, J.; et al. Mutational Characterization of Cutaneous Melanoma Supports Divergent Pathways Model for Melanoma Development. Cancers 2021, 13, 5219. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, E.F.; Chen, Y.Q.; Kopp, J.B.; Fisher, L.; Brown, D.B.; Hahn, P.J.; Robey, F.A.; Lakkakorpi, J.; Uitto, J. Long-term sun exposure alters the collagen of the papillary dermis. Comparison of sun-protected and photoaged skin by northern analysis, immunohistochemical staining, and confocal laser scanning microscopy. J. Am. Acad. Dermatol. 1996, 34, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Vierkötter, A.; Ranft, U.; Krämer, U.; Sugiri, D.; Reimann, V.; Krutmann, J. The SCINEXA: A novel, validated score to simultaneously assess and differentiate between intrinsic and extrinsic skin ageing. J. Dermatol. Sci. 2009, 53, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Perrot, J.L.; Labeille, B.; Biron, A.C.; Vierkötter, A.; Heusèle, C.; Nizard, C.; Schnebert, S.; Barthelemy, J.C.; Cambazard, F. Skin tumours and skin aging in 209 French elderly people: The PROOF study. Eur. J. Dermatol. 2016, 26, 470–476. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nevi (n = 92) | Melanomas (n = 503) | p | |
|---|---|---|---|
| Subtype of melanoma | - | SSM = 167 (33.2%) NMM = 199 (39.6%) LMM = 91 (18.1%) ALM = 27 (5.4%) Other/unspecified = 19 (3.8%) | - |
| Sex | Male = 30 (32.6%) Female = 62 (67.4%) | Male = 296 (58.8%) Female = 207 (41.2%) | - |
| Age at diagnosis (y) | 46.0 (±15.7) | 68.9 (±14.5) | ≤0.001 |
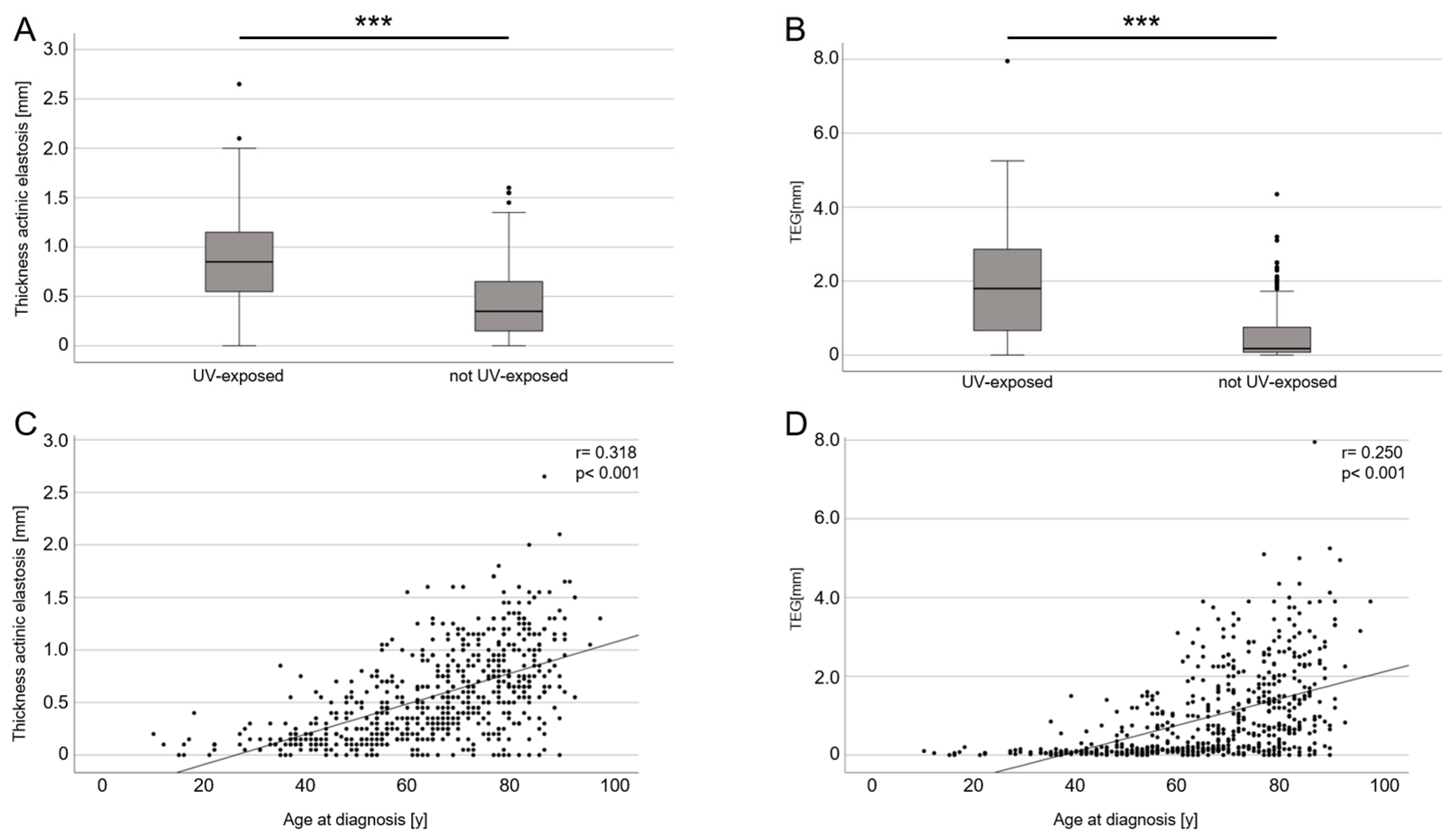
| UV-exposed body site | 16 (17.4%) | 159 (31.6%) | ≤0.001 |
| Mean depth of AE (mm) | 0.27 (±0.28) | 0.62 (±0.43) | ≤0.001 |
| TEG (mm) | 0.31 (±0.56) | 1.05 (±1.16) | ≤0.001 |
| Category | Lentigo Maligna Melanoma (n = 91) | Other Subtypes of Melanomas (n = 412) | p |
|---|---|---|---|
| Sex | male = 47 (51.6%) female = 44 (48.4%) | male = 249 (60.4%) female = 163 (39.6%) | |
| Age at diagnosis (y) | 76.1 (±9.8) | 67.2 (±14.8) | ≤0.001 |
| UV-exposed body site | 77 (84.6%) | 82 (19.9%) | ≤0.001 |
| Head and neck | 73 (80.2%) | 62 (15%) | ≤0.001 |
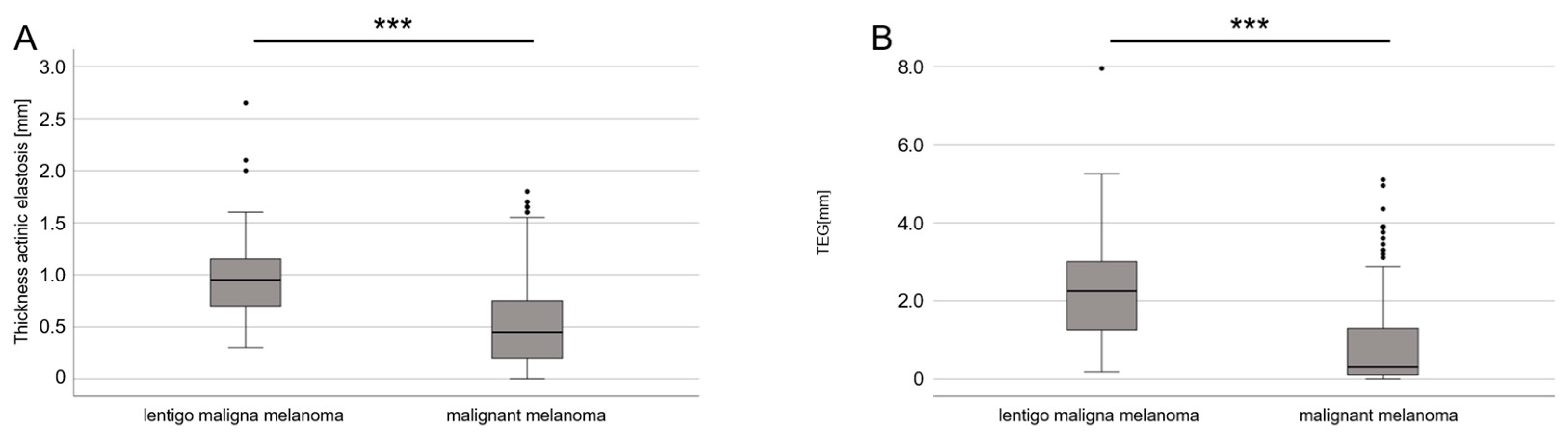
| Mean depth of AE (mm) | 0.96 (±0.38) | 0.54 (±0.40) | ≤0.001 |
| TEG (mm) | 2.22 (±1.26) | 0.80 (±0.96) | ≤0.001 |
| Depth of AE | TEG | |||||
|---|---|---|---|---|---|---|
| Category | Unstandardized Coefficients | Statistics | Unstandardized Coefficients | Statistics | ||
| B | Std. Error | p | B | Std. Error | p | |
| LMM vs. MM | 0.123 | 0.047 | 0.008 | 0.521 | 0.117 | <0.001 |
| Age at diagnosis | 0.012 | 0.001 | <0.001 | 0.027 | 0.003 | <0.001 |
| UV-exposed body site | 0.285 | 0.038 | <0.001 | 1.031 | 0.096 | <0.001 |
| Depth of AE | TEG | |||||
|---|---|---|---|---|---|---|
| Category | Unstandardized Coefficients | Statistics | Unstandardized Coefficients | Statistics | ||
| B | Std. Error | p | B | Std. Error | p | |
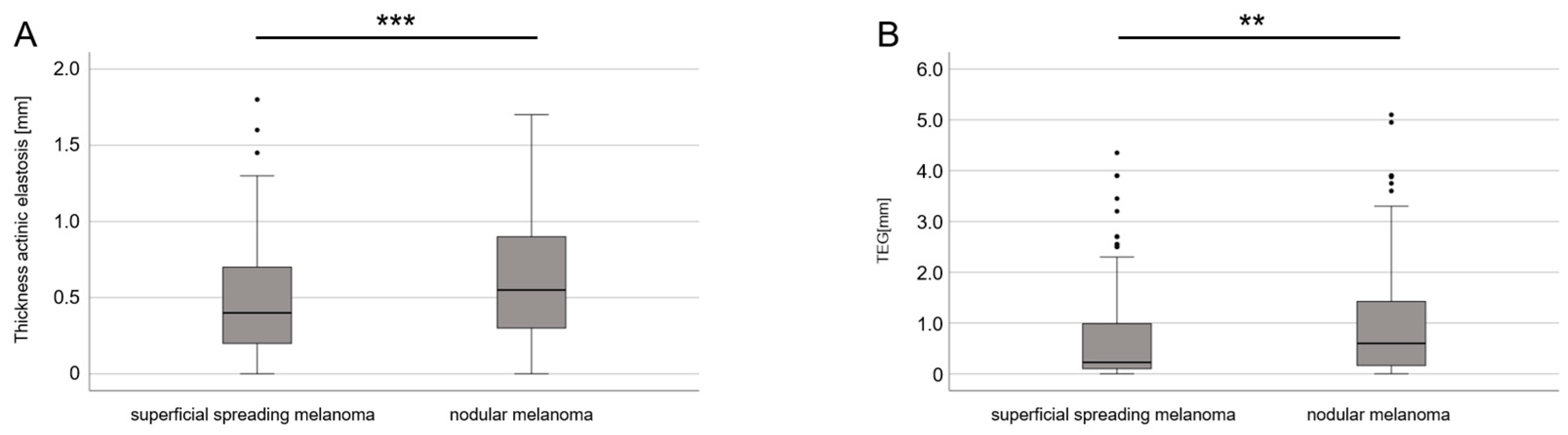
| SSM vs. NMM | 0.089 | 0.033 | 0.007 | 0.093 | 0.080 | 0.246 |
| Age at diagnosis | 0.012 | 0.001 | <0.001 | 0.026 | 0.003 | <0.001 |
| UV-exposed body site | 0.278 | 0.042 | <0.001 | 1.088 | 0.102 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drexler, K.; Zenderowski, V.; Schreieder, L.; Koschitzki, K.; Karrer, S.; Berneburg, M.; Haferkamp, S.; Niebel, D. Subtypes of Melanomas Associated with Different Degrees of Actinic Elastosis in Conventional Histology, Irrespective of Age and Body Site, Suggesting Chronic Ultraviolet Light Exposure as Driver for Lentigo Maligna Melanoma and Nodular Melanoma. Cancers 2024, 16, 1. https://doi.org/10.3390/cancers16010001
Drexler K, Zenderowski V, Schreieder L, Koschitzki K, Karrer S, Berneburg M, Haferkamp S, Niebel D. Subtypes of Melanomas Associated with Different Degrees of Actinic Elastosis in Conventional Histology, Irrespective of Age and Body Site, Suggesting Chronic Ultraviolet Light Exposure as Driver for Lentigo Maligna Melanoma and Nodular Melanoma. Cancers. 2024; 16(1):1. https://doi.org/10.3390/cancers16010001
Chicago/Turabian StyleDrexler, Konstantin, Veronika Zenderowski, Laura Schreieder, Kevin Koschitzki, Sigrid Karrer, Mark Berneburg, Sebastian Haferkamp, and Dennis Niebel. 2024. "Subtypes of Melanomas Associated with Different Degrees of Actinic Elastosis in Conventional Histology, Irrespective of Age and Body Site, Suggesting Chronic Ultraviolet Light Exposure as Driver for Lentigo Maligna Melanoma and Nodular Melanoma" Cancers 16, no. 1: 1. https://doi.org/10.3390/cancers16010001