
Quantitative Diffusion-Weighted MR Imaging: Is There a Prognostic Role in Noninvasively Predicting the Histopathologic Type of Uveal Melanomas?
 , , ,
, , ,  , , , , ,
, , , , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
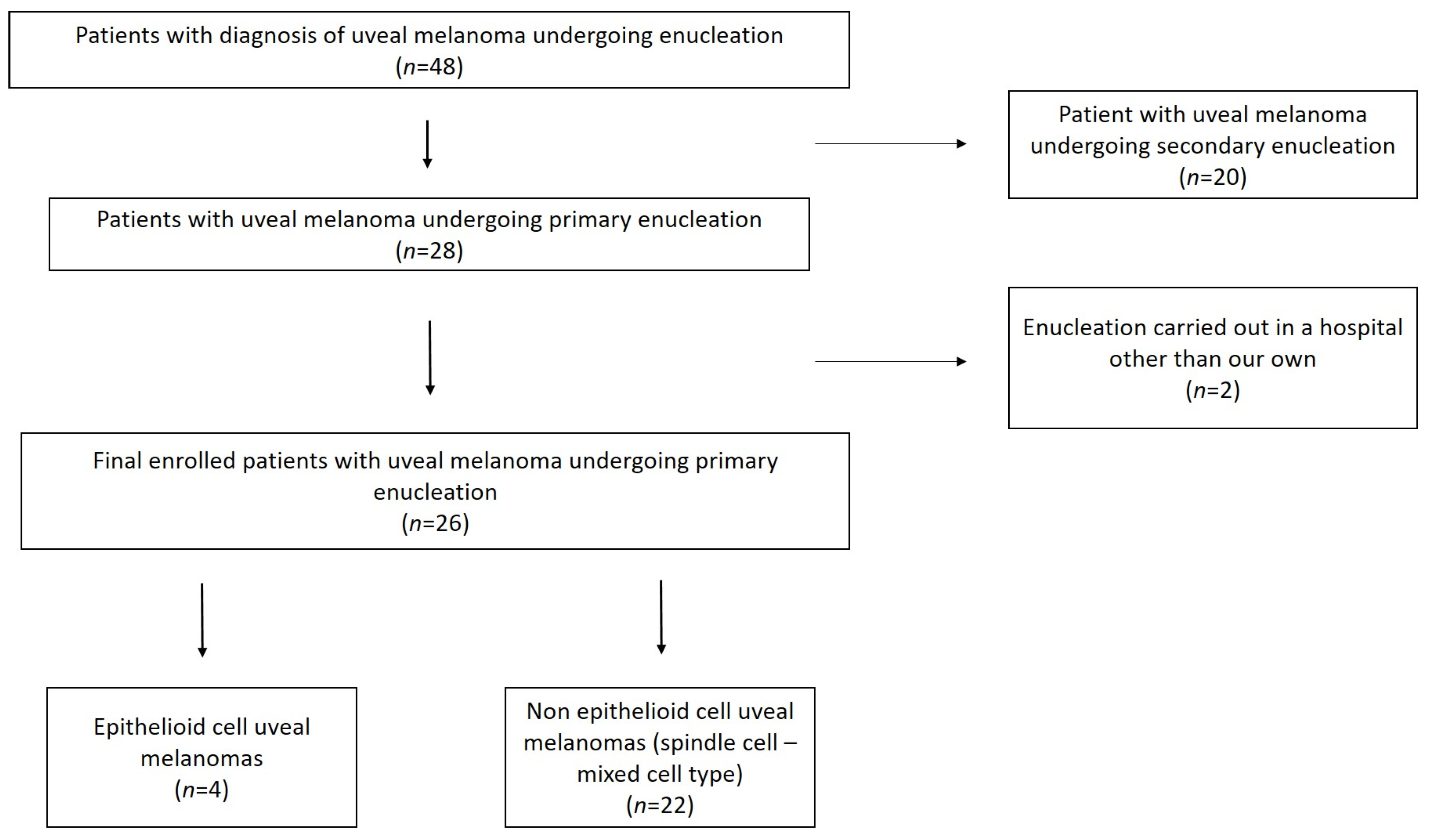
2.1. Patient Population and Selection Criteria
2.2. MRI Protocol
2.3. Histopathology
2.4. Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Study Population
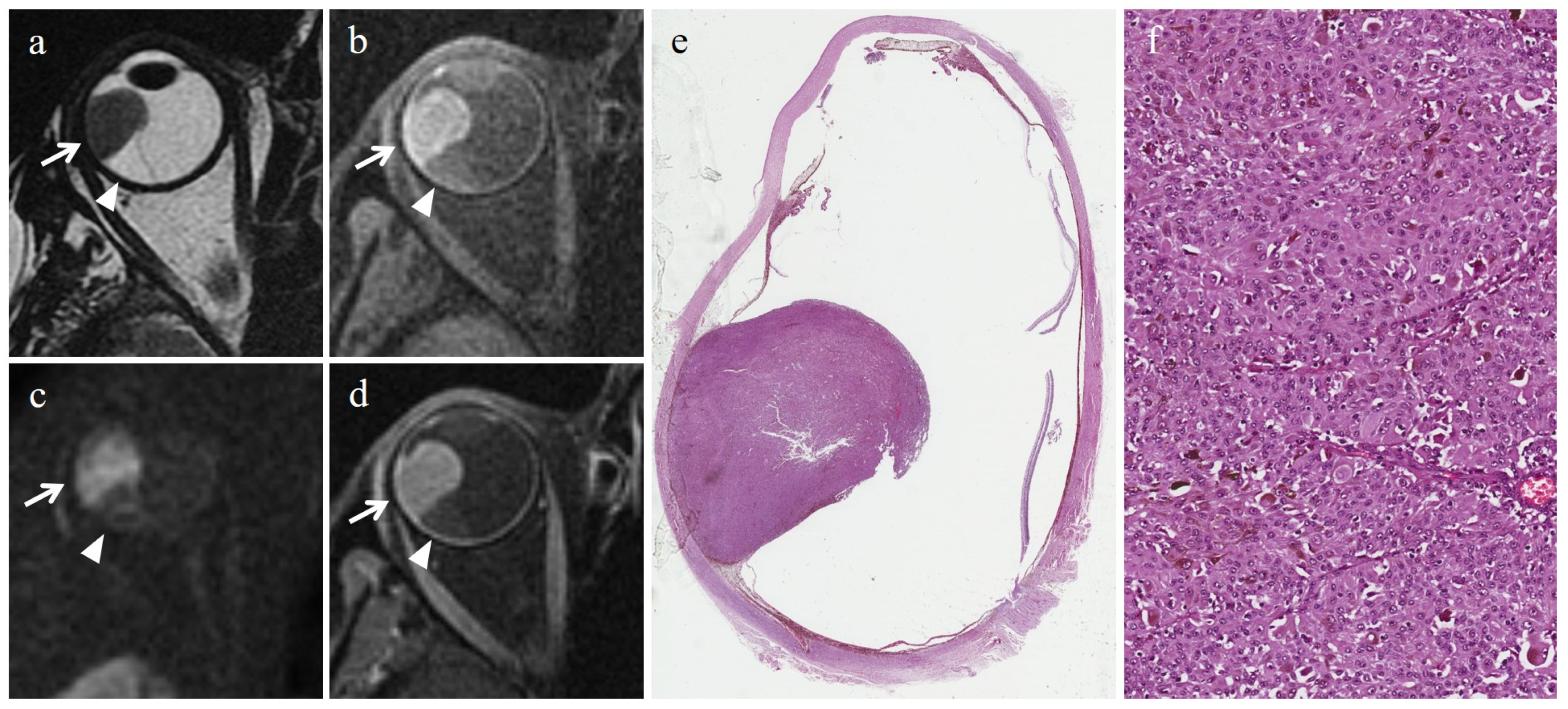
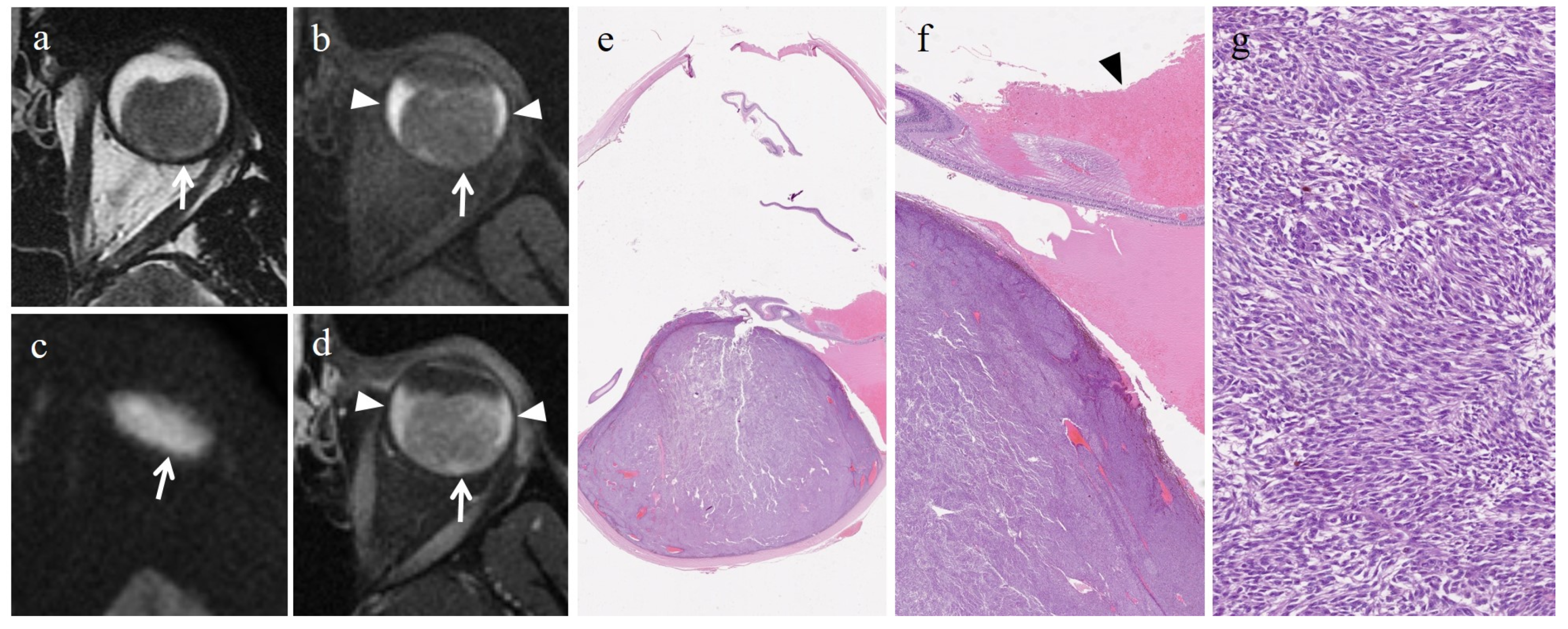
3.2. Histopathologic Findings
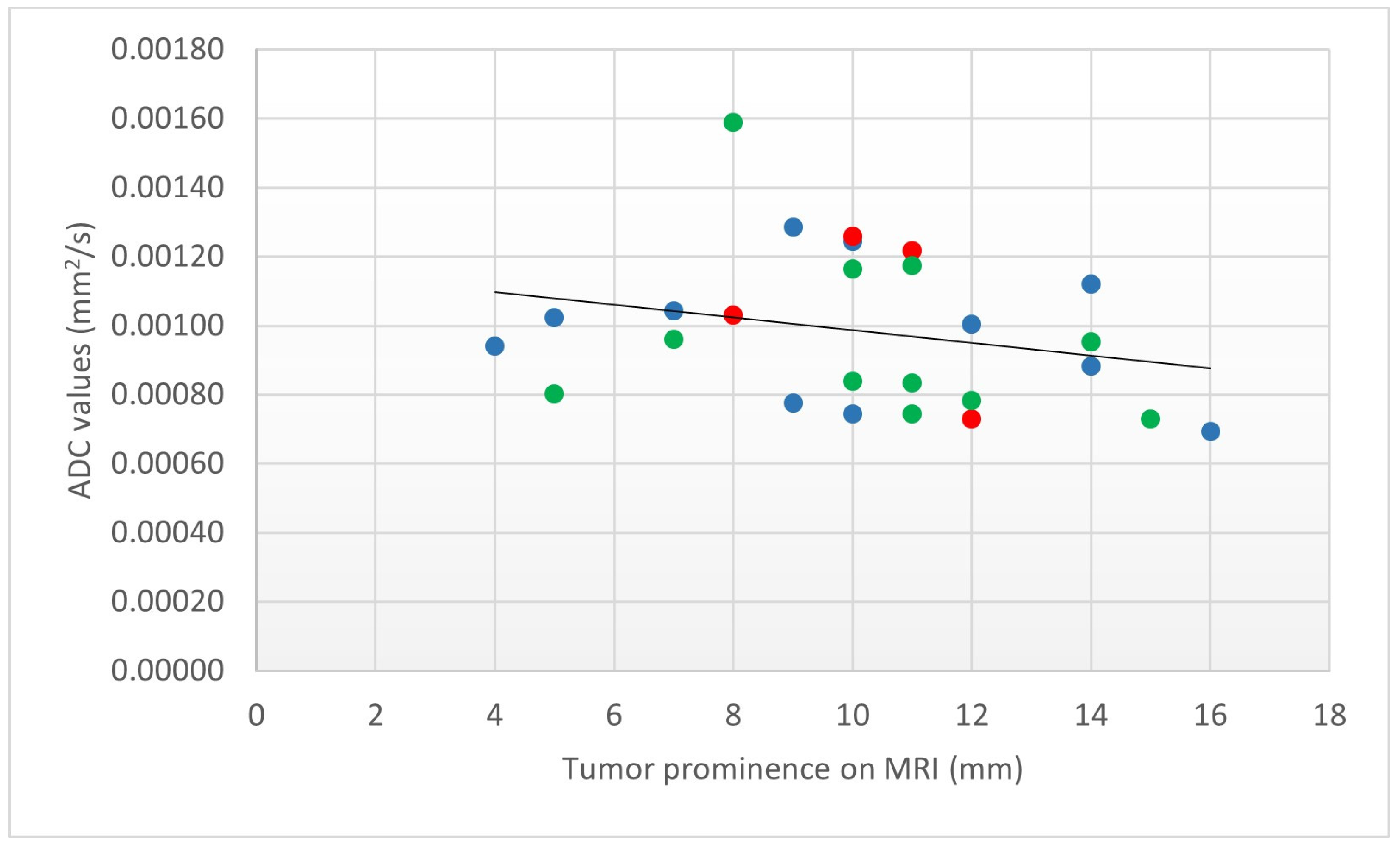
3.3. ADC Measurement and Relationship with Histologic Type
3.4. Tumor Dimensions and Relationship with Histopathologic Type
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gill, H.S.; Char, D.H. Uveal melanoma prognostication: From lesion size and cell type to molecular class. Can. J. Ophthalmol. 2012, 47, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Reinshagen, K.L.; Massoud, T.F.; Cunnane, M.B. Anatomy of the Orbit. Neuroimaging Clin. N. Am. 2022, 32, 699–711. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, N.W.; Budak, M.J.; White, R.D.; Zealley, I.A. MR-Eye: High-Resolution Microscopy Coil MRI for the Assessment of the Orbit and Periorbital Structures, Part 2: Clinical Applications. AJNR Am. J. Neuroradiol. 2021, 42, 1184–1189. [Google Scholar] [CrossRef] [PubMed]
- Souto, E.B.; Zielinska, A.; Luis, M.; Carbone, C.; Martins-Gomes, C.; Souto, S.B.; Silva, A.M. Uveal melanoma: Physiopathology and new in situ-specific therapies. Cancer Chemother. Pharmacol. 2019, 84, 15–32. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.A.; Jaarsma-Coes, M.G.; Marinkovic, M.; Verbist, B.; Verdijk, R.M.; Jager, M.J.; Luyten, G.P.M.; Beenakker, J.M. MR imaging characteristics of uveal melanoma with histopathological validation. Neuroradiology 2022, 64, 171–184. [Google Scholar] [CrossRef]
- Garg, G.; Kivelä, T.T.; Finger, P.T. Patients presenting with stage IV uveal melanoma: Lessons learned. Indian J. Ophthalmol. 2022, 70, 271–274. [Google Scholar] [CrossRef]
- Midena, E.; Segato, T.; Piermarocchi, S.; Boccato, P. Fine needle aspiration biopsy in ophthalmology. Surv. Ophthalmol. 1985, 29, 410–422. [Google Scholar] [CrossRef]
- Midena, E.; Parrozzani, R. Biopsies in uveal melanoma. Dev. Ophthalmol. 2012, 49, 81–95. [Google Scholar] [CrossRef]
- Frizziero, L.; Midena, E.; Trainiti, S.; Londei, D.; Bonaldi, L.; Bini, S.; Parrozzani, R. Uveal Melanoma Biopsy: A Review. Cancers 2019, 11, 1075. [Google Scholar] [CrossRef]
- Bagger, M.; Tebering, J.F.; Kiilgaard, J.F. The ocular consequences and applicability of minimally invasive 25-gauge transvitreal retinochoroidal biopsy. Ophthalmology 2013, 120, 2565–2572. [Google Scholar] [CrossRef]
- Solnik, M.; Paduszyńska, N.; Czarnecka, A.M.; Synoradzki, K.J.; Yousef, Y.A.; Chorągiewicz, T.; Rejdak, R.; Toro, M.D.; Zweifel, S.; Dyndor, K.; et al. Imaging of Uveal Melanoma-Current Standard and Methods in Development. Cancers 2022, 14, 3147. [Google Scholar] [CrossRef]
- Thornton, S.; Coupland, S.E.; Heimann, H.; Hussain, R.; Groenewald, C.; Kacperek, A.; Damato, B.; Taktak, A.; Eleuteri, A.; Kalirai, H. Effects of plaque brachytherapy and proton beam radiotherapy on prognostic testing: A comparison of uveal melanoma genotyped by microsatellite analysis. Br. J. Ophthalmol. 2020, 104, 1462–1466. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Dalvin, L.A.; Vichitvejpaisal, P.; Mazloumi, M.; Ganguly, A.; Shields, J.A. Prognostication of uveal melanoma is simple and highly predictive using The Cancer Genome Atlas (TCGA) classification: A review. Indian J. Ophthalmol. 2019, 67, 1959–1963. [Google Scholar] [CrossRef]
- Hussain, R.N.; Coupland, S.E.; Kalirai, H.; Taktak, A.F.G.; Eleuteri, A.; Damato, B.E.; Groenewald, C.; Heimann, H. Small High-Risk Uveal Melanomas Have a Lower Mortality Rate. Cancers 2021, 13, 2267. [Google Scholar] [CrossRef] [PubMed]
- Markiewicz, A.; Donizy, P.; Nowak, M.; Krzyziński, M.; Elas, M.; Płonka, P.M.; Orłowska-Heitzmann, J.; Biecek, P.; Hoang, M.P.; Romanowska-Dixon, B. Amelanotic Uveal Melanomas Evaluated by Indirect Ophthalmoscopy Reveal Better Long-Term Prognosis Than Pigmented Primary Tumours-A Single Centre Experience. Cancers 2022, 14, 2753. [Google Scholar] [CrossRef] [PubMed]
- Angi, M.; Damato, B.; Kalirai, H.; Dodson, A.; Taktak, A.; Coupland, S.E. Immunohistochemical assessment of mitotic count in uveal melanoma. Acta Ophthalmol. 2011, 89, e155–e160. [Google Scholar] [CrossRef]
- Berus, T.; Halon, A.; Markiewicz, A.; Orlowska-Heitzman, J.; Romanowska-Dixon, B.; Donizy, P. Clinical, Histopathological and Cytogenetic Prognosticators in Uveal Melanoma—A Comprehensive Review. Anticancer Res. 2017, 37, 6541–6549. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Shields, C.L.; Shields, J.A. Prognostic factors in uveal melanoma. Melanoma Res. 2001, 11, 255–263. [Google Scholar] [CrossRef]
- Angi, M.; Kalirai, H.; Taktak, A.; Hussain, R.; Groenewald, C.; Damato, B.E.; Heimann, H.; Coupland, S.E. Prognostic biopsy of choroidal melanoma: An optimised surgical and laboratory approach. Br. J. Ophthalmol. 2017, 101, 1143–1146. [Google Scholar] [CrossRef]
- Rantala, E.S.; Hernberg, M.M.; Piperno-Neumann, S.; Grossniklaus, H.E.; Kivelä, T.T. Metastatic uveal melanoma: The final frontier. Prog. Retin. Eye Res. 2022, 90, 101041. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L.; Shields, J.A. Uveal melanoma: Estimating prognosis. Indian J. Ophthalmol. 2015, 63, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Amaro, A.; Gangemi, R.; Piaggio, F.; Angelini, G.; Barisione, G.; Ferrini, S.; Pfeffer, U. The biology of uveal melanoma. Cancer Metastasis Rev. 2017, 36, 109–140. [Google Scholar] [CrossRef] [PubMed]
- Bagger, M.; Andersen, M.T.; Andersen, K.K.; Heegaard, S.; Andersen, M.K.; Kiilgaard, J.F. The prognostic effect of American Joint Committee on Cancer staging and genetic status in patients with choroidal and ciliary body melanoma. Investig. Ophthalmol. Vis. Sci. 2014, 56, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Foti, P.V.; Travali, M.; Farina, R.; Palmucci, S.; Spatola, C.; Raffaele, L.; Salamone, V.; Caltabiano, R.; Broggi, G.; Puzzo, L.; et al. Diagnostic methods and therapeutic options of uveal melanoma with emphasis on MR imaging—Part I: MR imaging with pathologic correlation and technical considerations. Insights Imaging 2021, 12, 66. [Google Scholar] [CrossRef] [PubMed]
- Robinson, H.; Eleuteri, A.; Sacco, J.J.; Hussain, R.; Heimann, H.; Taktak, A.F.G.; Damato, B.; Thompson, A.J.; Allen, T.; Kalirai, H.; et al. Sensitivity and Specificity of Different Prognostic Systems in Guiding Surveillance for Metastases in Uveal Melanoma. Cancers 2023, 15, 2610. [Google Scholar] [CrossRef] [PubMed]
- Dogrusöz, M.; Jager, M.J. Genetic prognostication in uveal melanoma. Acta Ophthalmol. 2018, 96, 331–347. [Google Scholar] [CrossRef]
- Kaštelan, S.; Mrazovac Zimak, D.; Ivanković, M.; Marković, I.; Gverović Antunica, A. Liver metastasis in uveal melanoma—Treatment options and clinical outcome. Front. Biosci. 2022, 27, 72. [Google Scholar] [CrossRef]
- McCannel, T.A. Fine-needle aspiration biopsy in the management of choroidal melanoma. Curr. Opin. Ophthalmol. 2013, 24, 262–266. [Google Scholar] [CrossRef]
- Singh, A.D.; Medina, C.A.; Singh, N.; Aronow, M.E.; Biscotti, C.V.; Triozzi, P.L. Fine-needle aspiration biopsy of uveal melanoma: Outcomes and complications. Br. J. Ophthalmol. 2016, 100, 456–462. [Google Scholar] [CrossRef]
- Le Guin, C.H.D.; Metz, K.A.; Lehmann, N.; Kreis, S.H.; Bornfeld, N.; Rudolf Lohmann, D.; Zeschnigk, M. Chromosome 3 is a valid marker for prognostic testing of biopsy material from uveal melanoma later treated by brachytherapy. Biomarkers 2019, 24, 134–140. [Google Scholar] [CrossRef]
- Bagger, M.M. Intraocular biopsy of uveal melanoma Risk assessment and identification of genetic prognostic markers. Acta Ophthalmol. 2018, 96 (Suppl. A112), 1–28. [Google Scholar] [CrossRef] [PubMed]
- Bagger, M.; Smidt-Nielsen, I.; Andersen, M.K.; Jensen, P.K.; Heegaard, S.; Andersen, K.K.; Friis, S.; Kiilgaard, J.F. Long-Term Metastatic Risk after Biopsy of Posterior Uveal Melanoma. Ophthalmology 2018, 125, 1969–1976. [Google Scholar] [CrossRef] [PubMed]
- Jensen, O.A.; Prause, J.U.; Scherfig, E. Transvitreal retino-choroidal biopsy of suspected malignant lesions of the choroid. Follow-up of cases over 7 years. Acta Ophthalmol. Scand. 1997, 75, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Schoenfield, L.; Pettay, J.; Tubbs, R.R.; Singh, A.D. Variation of monosomy 3 status within uveal melanoma. Arch. Pathol. Lab. Med. 2009, 133, 1219–1222. [Google Scholar] [CrossRef] [PubMed]
- Dopierala, J.; Damato, B.E.; Lake, S.L.; Taktak, A.F.; Coupland, S.E. Genetic heterogeneity in uveal melanoma assessed by multiplex ligation-dependent probe amplification. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4898–4905. [Google Scholar] [CrossRef] [PubMed]
- Maat, W.; Jordanova, E.S.; Van Zelderen-Bhola, S.L.; Barthen, E.R.; Wessels, H.W.; Schalij-Delfos, N.E.; Jager, M.J. The heterogeneous distribution of monosomy 3 in uveal melanomas: Implications for prognostication based on fine-needle aspiration biopsies. Arch. Pathol. Lab. Med. 2007, 131, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Mensink, H.W.; Vaarwater, J.; Kiliç, E.; Naus, N.C.; Mooy, N.; Luyten, G.; Brüggenwirth, H.T.; Paridaens, D.; de Klein, A. Chromosome 3 intratumor heterogeneity in uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2009, 50, 500–504. [Google Scholar] [CrossRef]
- Chang, M.Y.; Rao, N.P.; Burgess, B.L.; Johnson, L.; McCannel, T.A. Heterogeneity of monosomy 3 in fine needle aspiration biopsy of choroidal melanoma. Mol. Vis. 2013, 19, 1892–1900. [Google Scholar]
- van den Bosch, T.; van Beek, J.G.; Vaarwater, J.; Verdijk, R.M.; Naus, N.C.; Paridaens, D.; de Klein, A.; Kiliç, E. Higher percentage of FISH-determined monosomy 3 and 8q amplification in uveal melanoma cells relate to poor patient prognosis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2668–2674. [Google Scholar] [CrossRef]
- Jaarsma-Coes, M.G.; Ferreira, T.A.; van Houdt, P.J.; van der Heide, U.A.; Luyten, G.P.M.; Beenakker, J.M. Eye-specific quantitative dynamic contrast-enhanced MRI analysis for patients with intraocular masses. Magn. Reson. Mater. Phys. Biol. Med. 2022, 35, 311–323. [Google Scholar] [CrossRef]
- Jaarsma-Coes, M.G.; Ferreira, T.A.; Marinkovic, M.; Vu, T.H.K.; van Vught, L.; van Haren, G.R.; Rodrigues, M.F.; Klaver, Y.L.B.; Verbist, B.M.; Luyten, G.P.M.; et al. Comparison of Magnetic Resonance Imaging-Based and Conventional Measurements for Proton Beam Therapy of Uveal Melanoma. Ophthalmol. Retina 2023, 7, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.A.; Pinheiro, C.F.; Saraiva, P.; Jaarsma-Coes, M.G.; Van Duinen, S.G.; Genders, S.W.; Marinkovic, M.; Beenakker, J.M. MR and CT Imaging of the Normal Eyelid and its Application in Eyelid Tumors. Cancers 2020, 12, 658. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.A.; Grech Fonk, L.; Jaarsma-Coes, M.G.; van Haren, G.G.R.; Marinkovic, M.; Beenakker, J.M. MRI of Uveal Melanoma. Cancers 2019, 11, 377. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, J.M.; Camacho, J.C.; Kokabi, N.; Xing, M.; Kim, H.S. The Role of Diffusion-Weighted Imaging (DWI) in Locoregional Therapy Outcome Prediction and Response Assessment for Hepatocellular Carcinoma (HCC): The New Era of Functional Imaging Biomarkers. Diagnostics 2015, 5, 546–563. [Google Scholar] [CrossRef] [PubMed]
- McLean, I.W.; Foster, W.D.; Zimmerman, L.E.; Gamel, J.W. Modifications of Callender’s classification of uveal melanoma at the Armed Forces Institute of Pathology. Am. J. Ophthalmol. 1983, 96, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Foti, P.V.; Farina, R.; Coronella, M.; Palmucci, S.; Montana, A.; Sigona, A.; Reibaldi, M.; Longo, A.; Russo, A.; Avitabile, T.; et al. Diffusion-weighted magnetic resonance imaging for predicting and detecting the response of ocular melanoma to proton beam therapy: Initial results. Radiol. Med. 2015, 120, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Foti, P.V.; Inì, C.; Broggi, G.; Farina, R.; Palmucci, S.; Spatola, C.; Liardo, R.L.E.; Milazzotto, R.; Raffaele, L.; Salamone, V.; et al. Histopathologic and MR Imaging Appearance of Spontaneous and Radiation-Induced Necrosis in Uveal Melanomas: Initial Results. Cancers 2022, 14, 215. [Google Scholar] [CrossRef]
- Tang, M.C.Y.; Ferreira, T.A.; Marinkovic, M.; Jaarsma-Coes, M.G.; Klaassen, L.; Vu, T.H.K.; Creutzberg, C.L.; Rodrigues, M.F.; Horeweg, N.; Klaver, Y.L.B.; et al. MR-based follow-up after brachytherapy and proton beam therapy in uveal melanoma. Neuroradiology 2023, 65, 1271–1285. [Google Scholar] [CrossRef]
- Social Science Statistics. Available online: https://www.socscistatistics.com/ (accessed on 12 July 2023).
- Damato, B.; Eleuteri, A.; Taktak, A.F.; Coupland, S.E. Estimating prognosis for survival after treatment of choroidal melanoma. Prog. Retin. Eye Res. 2011, 30, 285–295. [Google Scholar] [CrossRef]
- Bagger, M.; Andersen, M.T.; Heegaard, S.; Andersen, M.K.; Kiilgaard, J.F. Transvitreal Retinochoroidal Biopsy Provides a Representative Sample from Choroidal Melanoma for Detection of Chromosome 3 Aberrations. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5917–5924. [Google Scholar] [CrossRef]
- Young, T.A.; Rao, N.P.; Glasgow, B.J.; Moral, J.N.; Straatsma, B.R. Fluorescent in situ hybridization for monosomy 3 via 30-gauge fine-needle aspiration biopsy of choroidal melanoma in vivo. Ophthalmology 2007, 114, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Damato, B.; Duke, C.; Coupland, S.E.; Hiscott, P.; Smith, P.A.; Campbell, I.; Douglas, A.; Howard, P. Cytogenetics of uveal melanoma: A 7-year clinical experience. Ophthalmology 2007, 114, 1925–1931. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Materin, M.A.; Teixeira, L.; Mashayekhi, A.; Ganguly, A.; Shields, J.A. Small choroidal melanoma with chromosome 3 monosomy on fine-needle aspiration biopsy. Ophthalmology 2007, 114, 1919–1924. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Ganguly, A.; Bianciotto, C.G.; Turaka, K.; Tavallali, A.; Shields, J.A. Prognosis of uveal melanoma in 500 cases using genetic testing of fine-needle aspiration biopsy specimens. Ophthalmology 2011, 118, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Angi, M.; Gibran, S.K.; Damato, B.E. Subfoveal choroidal neovascularization complicating 25-gauge trans-retinal choroidal tumor biopsy. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 1643–1645. [Google Scholar] [CrossRef] [PubMed]
- Han, L.M.; Khanafshar, E.; Afshar, A.R.; Calkins, S.M. The diagnostic utility of next-generation sequencing on FNA biopsies of melanocytic uveal lesions. Cancer Cytopathol. 2020, 128, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Mascalchi, M.; Filippi, M.; Floris, R.; Fonda, C.; Gasparotti, R.; Villari, N. Diffusion-weighted MR of the brain: Methodology and clinical application. Radiol. Med. 2005, 109, 155–197. [Google Scholar]
- Koh, D.M.; Collins, D.J. Diffusion-weighted MRI in the body: Applications and challenges in oncology. AJR Am. J. Roentgenol. 2007, 188, 1622–1635. [Google Scholar] [CrossRef]
- Padhani, A.R. Diffusion magnetic resonance imaging in cancer patient management. Semin. Radiat. Oncol. 2011, 21, 119–140. [Google Scholar] [CrossRef]
- Lenz, C.; Klarhöfer, M.; Scheffler, K.; Winter, L.; Sommer, G. Assessing extracranial tumors using diffusion-weighted whole-body MRI. Z. Med. Phys. 2011, 21, 79–90. [Google Scholar] [CrossRef]
- Schmid-Tannwald, C.; Oto, A.; Reiser, M.F.; Zech, C.J. Diffusion-weighted MRI of the abdomen: Current value in clinical routine. J. Magn. Reson. Imaging 2013, 37, 35–47. [Google Scholar] [CrossRef] [PubMed]
- De Perrot, T.; Sadjo Zoua, C.; Glessgen, C.G.; Botsikas, D.; Berchtold, L.; Salomir, R.; De Seigneux, S.; Thoeny, H.C.; Vallée, J.P. Diffusion-Weighted MRI in the Genitourinary System. J. Clin. Med. 2022, 11, 1921. [Google Scholar] [CrossRef] [PubMed]
- Jaarsma-Coes, M.G.; Klaassen, L.; Marinkovic, M.; Luyten, G.P.M.; Vu, T.H.K.; Ferreira, T.A.; Beenakker, J.M. Magnetic Resonance Imaging in the Clinical Care for Uveal Melanoma Patients-A Systematic Review from an Ophthalmic Perspective. Cancers 2023, 15, 2995. [Google Scholar] [CrossRef] [PubMed]
- Beenakker, J.M.; Brouwer, N.J.; Chau, C.; Coupland, S.E.; Fiorentzis, M.; Heimann, H.; Heufelder, J.; Joussen, A.M.; Kiilgaard, J.F.; Kivelä, T.T.; et al. Outcome Measures of New Technologies in Uveal Melanoma: Review from the European Vision Institute Special Interest Focus Group Meeting. Ophthalmic Res. 2023, 66, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Sepahdari, A.R.; Aakalu, V.K.; Setabutr, P.; Shiehmorteza, M.; Naheedy, J.H.; Mafee, M.F. Indeterminate orbital masses: Restricted diffusion at MR imaging with echo-planar diffusion-weighted imaging predicts malignancy. Radiology 2010, 256, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Sepahdari, A.R.; Kapur, R.; Aakalu, V.K.; Villablanca, J.P.; Mafee, M.F. Diffusion-weighted imaging of malignant ocular masses: Initial results and directions for further study. AJNR Am. J. Neuroradiol. 2012, 33, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Sepahdari, A.R.; Politi, L.S.; Aakalu, V.K.; Kim, H.J.; Razek, A.A. Diffusion-weighted imaging of orbital masses: Multi-institutional data support a 2-ADC threshold model to categorize lesions as benign, malignant, or indeterminate. AJNR Am. J. Neuroradiol. 2014, 35, 170–175. [Google Scholar] [CrossRef]
- Erb-Eigner, K.; Willerding, G.; Taupitz, M.; Hamm, B.; Asbach, P. Diffusion-weighted imaging of ocular melanoma. Investig. Radiol. 2013, 48, 702–707. [Google Scholar] [CrossRef]
- Foti, P.V.; Longo, A.; Reibaldi, M.; Russo, A.; Privitera, G.; Spatola, C.; Raffaele, L.; Salamone, V.; Farina, R.; Palmucci, S.; et al. Uveal melanoma: Quantitative evaluation of diffusion-weighted MR imaging in the response assessment after proton-beam therapy, long-term follow-up. Radiol. Med. 2017, 122, 131–139. [Google Scholar] [CrossRef]
- Imaizumi, A.; Obata, T.; Kershaw, J.; Tachibana, Y.; Abe, Y.; Shibata, S.; Nitta, N.; Aoki, I.; Yasui, M.; Higashi, T. Quantitative measurement of diffusion-weighted imaging signal using expression-controlled aquaporin-4 cells: Comparative study of 2-compartment and diffusion kurtosis imaging models. PLoS ONE 2022, 17, e0266465. [Google Scholar] [CrossRef]
- Qayyum, A. Diffusion-weighted imaging in the abdomen and pelvis: Concepts and applications. Radiographics 2009, 29, 1797–1810. [Google Scholar] [CrossRef]
- Baliyan, V.; Das, C.J.; Sharma, R.; Gupta, A.K. Diffusion weighted imaging: Technique and applications. World J. Radiol. 2016, 8, 785–798. [Google Scholar] [CrossRef] [PubMed]
- Drake-Pérez, M.; Boto, J.; Fitsiori, A.; Lovblad, K.; Vargas, M.I. Clinical applications of diffusion weighted imaging in neuroradiology. Insights Imaging 2018, 9, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Russo, A.; Reibaldi, M.; Russo, D.; Varricchio, S.; Bonfiglio, V.; Spatola, C.; Barbagallo, C.; Foti, P.V.; Avitabile, T.; et al. Histopathology and Genetic Biomarkers of Choroidal Melanoma. Appl. Sci. 2020, 10, 8081. [Google Scholar] [CrossRef]
- Bai, Y.; Liu, T.; Chen, L.; Gao, H.; Wei, W.; Zhang, G.; Wang, L.; Kong, L.; Liu, S.; Liu, H.; et al. Study of Diffusion Weighted Imaging Derived Diffusion Parameters as Biomarkers for the Microenvironment in Gliomas. Front. Oncol. 2021, 11, 672265. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zheng, J.; Yang, C.; Peng, J.; Liu, N.; Yang, L.; Zhang, X.M. Application of intravoxel incoherent motion diffusion-weighted imaging in hepatocellular carcinoma. World J. Gastroenterol. 2022, 28, 3334–3345. [Google Scholar] [CrossRef]
- Liu, N.; Yang, X.; Lei, L.; Pan, K.; Liu, Q.; Huang, X. Intravoxel Incoherent Motion Model in Differentiating the Pathological Grades of Esophageal Carcinoma: Comparison of Mono-Exponential and Bi-Exponential Fit Model. Front. Oncol. 2021, 11, 625891. [Google Scholar] [CrossRef]
- Lu, Y.; Jansen, J.F.; Mazaheri, Y.; Stambuk, H.E.; Koutcher, J.A.; Shukla-Dave, A. Extension of the intravoxel incoherent motion model to non-gaussian diffusion in head and neck cancer. J. Magn. Reson. Imaging 2012, 36, 1088–1096. [Google Scholar] [CrossRef]
- Mikayama, R.; Yabuuchi, H.; Sonoda, S.; Kobayashi, K.; Nagatomo, K.; Kimura, M.; Kawanami, S.; Kamitani, T.; Kumazawa, S.; Honda, H. Comparison of intravoxel incoherent motion diffusion-weighted imaging between turbo spin-echo and echo-planar imaging of the head and neck. Eur. Radiol. 2018, 28, 316–324. [Google Scholar] [CrossRef]
- Norris, C.D.; Quick, S.E.; Parker, J.G.; Koontz, N.A. Diffusion MR Imaging in the Head and Neck: Principles and Applications. Neuroimaging Clin. N. Am. 2020, 30, 261–282. [Google Scholar] [CrossRef]
- An, H.; Ma, X.; Pan, Z.; Guo, H.; Lee, E.Y.P. Qualitative and quantitative comparison of image quality between single-shot echo-planar and interleaved multi-shot echo-planar diffusion-weighted imaging in female pelvis. Eur. Radiol. 2020, 30, 1876–1884. [Google Scholar] [CrossRef] [PubMed]
- Bilmin, K.; Synoradzki, K.J.; Czarnecka, A.M.; Spałek, M.J.; Kujawska, T.; Solnik, M.; Merks, P.; Toro, M.D.; Rejdak, R.; Fiedorowicz, M. New Perspectives for Eye-Sparing Treatment Strategies in Primary Uveal Melanoma. Cancers 2021, 14, 134. [Google Scholar] [CrossRef] [PubMed]
- Foti, P.V.; Travali, M.; Farina, R.; Palmucci, S.; Spatola, C.; Liardo, R.L.E.; Milazzotto, R.; Raffaele, L.; Salamone, V.; Caltabiano, R.; et al. Diagnostic methods and therapeutic options of uveal melanoma with emphasis on MR imaging—Part II: Treatment indications and complications. Insights Imaging 2021, 12, 67. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MRI Protocol | T2W FSE | T2W FSE STIR | T1W FSE | T1W FSE Fat Sat | DWI SE EPI |
|---|---|---|---|---|---|
| Acquisition plane | axial, coronal | axial, coronal | axial, coronal | axial, coronal | axial |
| Repetition time/Echo time (ms) | 3220/120 | 3700/50 | 550/14.9 | 450/15.1 | 4800/89.9 |
| Flip angle | 90° | 90° | 90° | 90° | 90° |
| Echo train length | 19 | 12 | 2 | 2 | - |
| N. of averages | 4 | 3 | 3 | 2 | 8 |
| Slice thickness (mm) | 3 | 3 | 3 | 3 | 4 |
| Interslice gap (mm) | 0.3 | 0.3 | 0.3 | 0.3 | 0.4 |
| Field of view (mm) | 160 × 160 | 160 × 160 | 160 × 160 | 160 × 160 | 200 × 200 |
| Matrix | 352 × 256 | 256 × 256 | 256 × 224 | 256 × 256 | 192 × 192 |
| Frequency direction | Superior to inferior | Anterior to posterior | Right to left | Right to left | Right to left |
| b-value (s/mm2) | - | - | - | - | 0–1000 |
| Scan time | 3 min 20 s | 4 min 12 s | 3 min 30 s | 3 min 30 s | 3 min 40 s |
| Patient | Gender | Age | Eye | Tumor Location | Histologic Type |
|---|---|---|---|---|---|
| 1 | Male | 55 | Left | Choroid | Epithelioid cell type |
| 2 | Female | 55 | Right | Choroid | Spindle cell type |
| 3 | Female | 80 | Right | Choroid | Epithelioid cell type |
| 4 | Female | 81 | Left | Choroid | Spindle cell type |
| 5 | Male | 77 | Right | Choroid and ciliary body | Spindle cell type |
| 6 | Male | 70 | Right | Choroid and ciliary body | Mixed cell type |
| 7 | Male | 40 | Left | Choroid | Spindle cell type |
| 8 | Male | 54 | Right | Choroid and ciliary body | Mixed cell type |
| 9 | Female | 69 | Left | Choroid | Spindle cell type |
| 10 | Female | 79 | Left | Choroid | Mixed cell type |
| 11 | Male | 64 | Left | Choroid | Spindle cell type |
| 12 | Male | 49 | Left | Choroid | Mixed cell type |
| 13 | Female | 72 | Left | Choroid | Mixed cell type |
| 14 | Female | 47 | Left | Choroid | Mixed cell type |
| 15 | Male | 70 | Left | Choroid | Spindle cell type |
| 16 | Female | 36 | Right | Choroid and ciliary body | Spindle cell type |
| 17 | Male | 35 | Left | Choroid | Epithelioid cell type |
| 18 | Female | 69 | Right | Choroid | Mixed cell type |
| 19 | Female | 65 | Right | Choroid | Epithelioid cell type |
| 20 | Male | 39 | Left | Choroid | Spindle cell type |
| 21 | Male | 61 | Right | Choroid | Mixed cell type |
| 22 | Male | 40 | Right | Choroid | Spindle cell type |
| 23 | Male | 61 | Right | Choroid | Mixed cell type |
| 24 | Female | 86 | Left | Choroid | Mixed cell type |
| 25 | Male | 72 | Left | Choroid | Spindle cell type |
| 26 | Male | 66 | Left | Choroid | Mixed cell type |
| Patient | Histologic Type | Mean ADC Values (×10−3 mm2/s) | Tumor Prominence (mm) * at MRI | Tumor Largest Basal Diameter (mm) at MRI |
|---|---|---|---|---|
| 1 | Epithelioid cell type | 0.00103 | 8 | 20 |
| 2 | Spindle cell type | 0.00102 | 5 | 10 |
| 3 | Epithelioid cell type | 0.00122 | 11 | 12 |
| 4 | Spindle cell type | 0.00100 | 12 | 16 |
| 5 | Spindle cell type | 0.00069 | 16 | 21 |
| 6 | Mixed cell type | 0.00074 | 11 | 23 |
| 7 | Spindle cell type | 0.00124 | 10 | 14 |
| 8 | Mixed cell type | 0.00116 | 10 | 14 |
| 9 | Spindle cell type | 0.00094 | 4 | 14 |
| 10 | Mixed cell type | 0.00083 | 11 | 12 |
| 11 | Spindle cell type | 0.00104 | 7 | 18 |
| 12 | Mixed cell type | 0.00117 | 11 | 16 |
| 13 | Mixed cell type | 0.00095 | 14 | 14 |
| 14 | Mixed cell type | 0.00159 | 8 | 15 |
| 15 | Spindle cell type | 0.00112 | 14 | 15 |
| 16 | Spindle cell type | 0.00129 | 9 | 12 |
| 17 | Epithelioid cell type | 0.00126 | 10 | 19 |
| 18 | Mixed cell type | 0.00096 | 7 | 16.5 |
| 19 | Epithelioid cell type | 0.00073 | 12 | 10 |
| 20 | Spindle cell type | 0.00088 | 14 | 19 |
| 21 | Mixed cell type | 0.00078 | 12 | 19 |
| 22 | Spindle cell type | 0.00074 | 10 | 12.5 |
| 23 | Mixed cell type | 0.00080 | 5 | 12 |
| 24 | Mixed cell type | 0.00073 | 15 | 18 |
| 25 | Spindle cell type | 0.00078 | 9 | 12.5 |
| 26 | Mixed cell type | 0.00084 | 10 | 15 |
| Enrolled Population | Mean ADC Values ± (SD) (×10−3 mm2/s) |
|---|---|
| Patients with UM (tot.) (n = 26) | 0.98 ± 0.22 |
| Epithelioid cell type UM (n = 4) | 1.06 ± 0.24 |
| Spindle cell type UM (n = 11) | 0.98 ± 0.19 |
| Mixed cell type UM (n = 11) | 0.96 ± 0.26 |
| Non-epithelioid cell type UM (n = 22) | 0.97 ± 0.22 |
| One-way ANOVA | F2, 23 = 0.27; p = 0.76 |
| Unpaired t-test | t(24) = 0.22, p = 0.82 |
| Patient | Histologic Type | Tumor Prominence (mm) * at MRI | Tumor Prominence (mm) at Histology | Tumor Largest Basal Diameter (mm) at MRI | Tumor Largest Basal Diameter (mm) at Histology |
|---|---|---|---|---|---|
| 1 | Epithelioid cell type | 8 | 13 | 20 | 20 |
| 2 | Spindle cell type | 5 | 5 | 10 | 7 |
| 3 | Epithelioid cell type | 11 | 8 | 12 | 13 |
| 4 | Spindle cell type | 12 | 10 | 16 | 14 |
| 5 | Spindle cell type | 16 | 15 | 21 | 20 |
| 6 | Mixed cell type | 11 | 12 | 23 | 13 |
| 7 | Spindle cell type | 10 | 11 | 14 | 12 |
| 8 | Mixed cell type | 10 | 10 | 14 | 12 |
| 9 | Spindle cell type | 4 | 3 | 14 | 16 |
| 10 | Mixed cell type | 11 | 10 | 12 | 10.5 |
| 11 | Spindle cell type | 7 | 10 | 18 | 15 |
| 12 | Mixed cell type | 11 | 10 | 16 | 12 |
| 13 | Mixed cell type | 14 | 7 | 14 | 12 |
| 14 | Mixed cell type | 8 | 10 | 15 | 20 |
| 15 | Spindle cell type | 14 | 7 | 15 | 17 |
| 16 | Spindle cell type | 9 | 7 | 12 | 9 |
| 17 | Epithelioid cell type | 10 | 10 | 19 | 15 |
| 18 | Mixed cell type | 7 | 5 | 16.5 | 15 |
| 19 | Epithelioid cell type | 12 | 11 | 10 | 12 |
| 20 | Spindle cell type | 14 | 13 | 19 | 16 |
| 21 | Mixed cell type | 12 | 11 | 19 | 17 |
| 22 | Spindle cell type | 10 | 10 | 12.5 | 11 |
| 23 | Mixed cell type | 5 | 4 | 12 | 15 |
| 24 | Mixed cell type | 15 | 10 | 18 | 18 |
| 25 | Spindle cell type | 9 | 6 | 12.5 | 10 |
| 26 | Mixed cell type | 10 | 12 | 15 | 15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foti, P.V.; Inì, C.; Broggi, G.; Farina, R.; Palmucci, S.; Spatola, C.; Lo Greco, M.C.; David, E.; Caltabiano, R.; Puzzo, L.; et al. Quantitative Diffusion-Weighted MR Imaging: Is There a Prognostic Role in Noninvasively Predicting the Histopathologic Type of Uveal Melanomas? Cancers 2023, 15, 5627. https://doi.org/10.3390/cancers15235627
Foti PV, Inì C, Broggi G, Farina R, Palmucci S, Spatola C, Lo Greco MC, David E, Caltabiano R, Puzzo L, et al. Quantitative Diffusion-Weighted MR Imaging: Is There a Prognostic Role in Noninvasively Predicting the Histopathologic Type of Uveal Melanomas? Cancers. 2023; 15(23):5627. https://doi.org/10.3390/cancers15235627
Chicago/Turabian StyleFoti, Pietro Valerio, Corrado Inì, Giuseppe Broggi, Renato Farina, Stefano Palmucci, Corrado Spatola, Maria Chiara Lo Greco, Emanuele David, Rosario Caltabiano, Lidia Puzzo, and et al. 2023. "Quantitative Diffusion-Weighted MR Imaging: Is There a Prognostic Role in Noninvasively Predicting the Histopathologic Type of Uveal Melanomas?" Cancers 15, no. 23: 5627. https://doi.org/10.3390/cancers15235627