
Comparative Analysis of Atezolizumab Plus Bevacizumab and Hepatic Artery Infusion Chemotherapy in Unresectable Hepatocellular Carcinoma: A Multicenter, Propensity Score Study
 , , , , , , , , , , , and
, , , , , , , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Treatment Protocol
2.3. Endpoints and Response Evaluation
2.4. Statistical Analyses
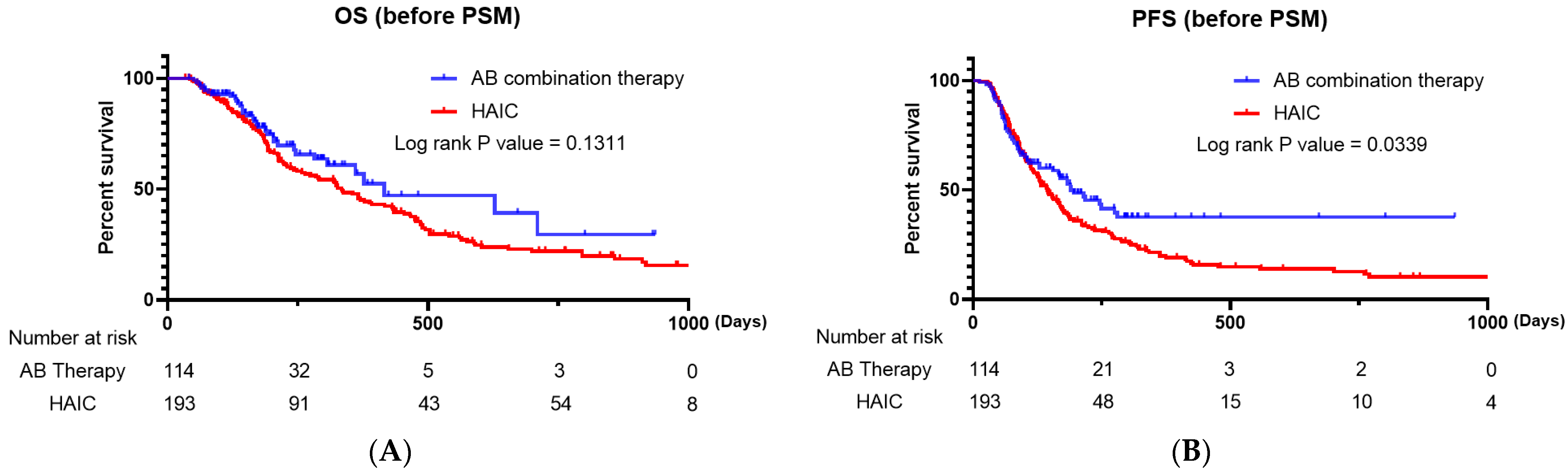
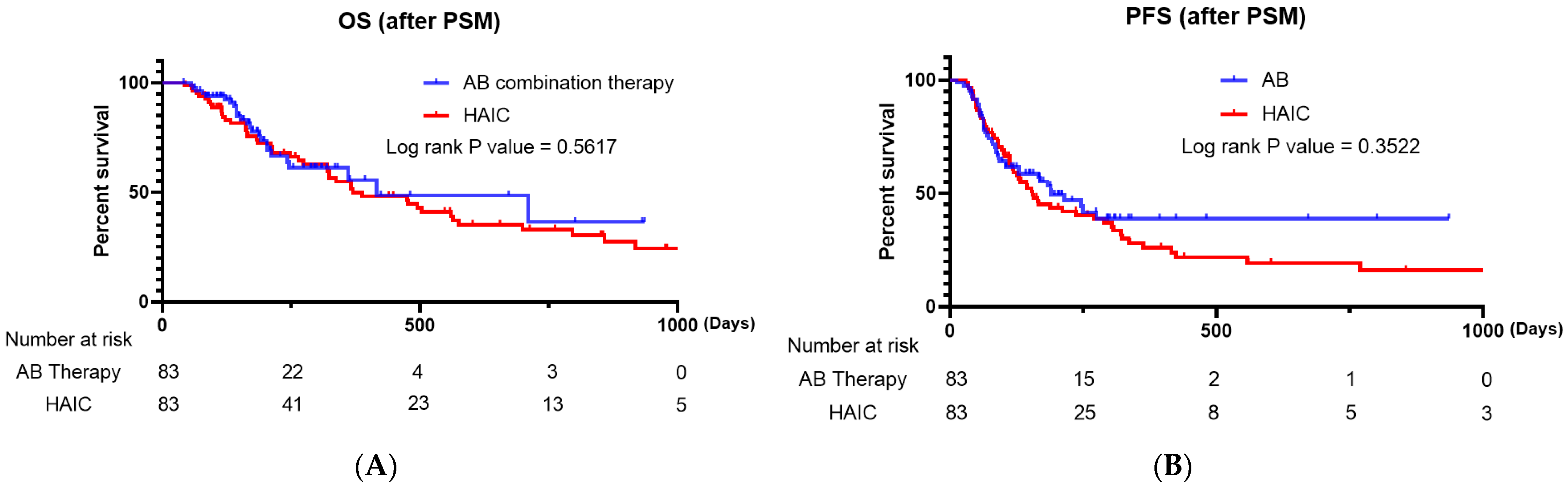
3. Results
3.1. Baseline Characteristics
3.2. Treatment Responses
3.3. Factors Associated with Survival Outcomes
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Jemal, A.; Ward, E.M.; Johnson, C.J.; Cronin, K.A.; Ma, J.; Ryerson, B.; Mariotto, A.; Lake, A.J.; Wilson, R.; Sherman, R.L.; et al. Annual report to the nation on the status of cancer, 1975–2014, featuring survival. J. Natl. Cancer Inst. 2017, 109, djx030. [Google Scholar] [CrossRef]
- Xu, J. Trends in liver cancer mortality among adults aged 25 and over in the United States, 2000–2016. NCHS Data Brief 2018, 314, 1–8. [Google Scholar]
- Daher, D.; Dahan, K.S.E.; Singal, A.G. Non-alcoholic fatty liver disease-related hepatocellular carcinoma. J. Liver Cancer 2023, 23, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Tsutsumi, T.; Nakano, D.; Eslam, M.; George, J.; Torimura, T. MAFLD enhances clinical practice for liver disease in the Asia-Pacific region. Clin. Mol. Hepatol. 2022, 28, 150–163. [Google Scholar] [CrossRef]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Kim, B.K.; Cheon, J.; Kim, H.; Kang, B.; Ha, Y.; Kim, D.Y.; Hwang, S.G.; Chon, Y.E.; Chon, H.J. Atezolizumab/bevacizumab vs. lenvatinib as first-line therapy for unresectable hepatocellular carcinoma: A real-world, multi-center study. Cancers 2022, 14, 1747. [Google Scholar] [CrossRef] [PubMed]
- Su, C.W.; Teng, W.; Lin, P.T.; Jeng, W.J.; Chen, K.A.; Hsieh, Y.C.; Chen, W.T.; Ho, M.M.; Hsieh, C.H.; Wang, C.T.; et al. Similar efficacy and safety between lenvatinib versus atezolizumab plus bevacizumab as the first-line treatment for unresectable hepatocellular carcinoma. Cancer Med. 2023, 12, 7077–7089. [Google Scholar] [CrossRef] [PubMed]
- Casadei-Gardini, A.; Rimini, M.; Rimassa, L.; Burgio, V.; Kudo, M.; Tada, T.; Shimose, S.; Suda, G.; Yoo, C.; Cheon, J.; et al. Atezolizumab plus bevacizumab versus lenvatinib or sorafenib in non-viral unresectable hepatocellular carcinoma: An international study. J. Clin. Oncol. 2022, 40, 4069. [Google Scholar] [CrossRef]
- Rimini, M.; Rimassa, L.; Ueshima, K.; Burgio, V.; Shigeo, S.; Tada, T.; Suda, G.; Yoo, C.; Cheon, J.; Pinato, D.J.; et al. Atezolizumab plus bevacizumab versus lenvatinib or sorafenib in non-viral unresectable hepatocellular carcinoma: An international propensity score matching analysis. ESMO Open 2022, 7, 100591. [Google Scholar] [CrossRef]
- Chen, C.T.; Liu, T.H.; Shao, Y.Y.; Liu, K.L.; Liang, P.C.; Lin, Z.Z. Revisiting hepatic artery infusion chemotherapy in the treatment of advanced hepatocellular carcinoma. Int. J. Mol. Sci. 2021, 22, 12880. [Google Scholar] [CrossRef]
- Yoon, J.S.; Lee, H.A.; Kim, H.Y.; Sinn, D.H.; Lee, D.H.; Hong, S.K.; Cho, J.Y.; Choi, J.; Chang, Y.; Kong, H.J.; et al. Hepatocellular carcinoma in Korea: An analysis of the 2015 Korean Nationwide Cancer Registry. J. Liver Cancer 2021, 21, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Obi, S.; Sato, S.; Kawai, T. Current status of hepatic arterial infusion chemotherapy. Liver Cancer 2015, 4, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Sung, P.S.; Yang, K.; Bae, S.H.; Oh, J.S.; Chun, H.J.; Nam, H.C.; Jang, J.W.; Choi, J.Y.; Yoon, S.K. Reduction of intrahepatic tumour by hepatic arterial infusion chemotherapy prolongs survival in hepatocellular carcinoma. Anticancer Res. 2019, 39, 3909–3916. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Han, J.W.; Sung, P.S.; Lee, S.K.; Yang, H.; Nam, H.C.; Yoo, S.H.; Lee, H.L.; Kim, H.Y.; Lee, S.W.; et al. Comparative analysis of lenvatinib and hepatic arterial infusion chemotherapy in unresectable hepatocellular carcinoma: A multi-center, propensity score study. J. Clin. Med. 2021, 10, 4045. [Google Scholar] [CrossRef]
- Ueshima, K.; Ogasawara, S.; Ikeda, M.; Yasui, Y.; Terashima, T.; Yamashita, T.; Obi, S.; Sato, S.; Aikata, H.; Ohmura, T.; et al. Hepatic arterial infusion chemotherapy versus sorafenib in patients with advanced hepatocellular carcinoma. Liver Cancer 2020, 9, 583–595. [Google Scholar] [CrossRef]
- Hatooka, M.; Kawaoka, T.; Aikata, H.; Inagaki, Y.; Morio, K.; Nakahara, T.; Murakami, E.; Tsuge, M.; Hiramatsu, A.; Imamura, M.; et al. Hepatic arterial infusion chemotherapy followed by sorafenib in patients with advanced hepatocellular carcinoma (HICS 55): An open label, non-comparative, phase II trial. BMC Cancer 2018, 18, 633. [Google Scholar] [CrossRef]
- Choi, J.H.; Chung, W.J.; Bae, S.H.; Song, D.S.; Song, M.J.; Kim, Y.S.; Yim, H.J.; Jung, Y.K.; Suh, S.J.; Park, J.Y.; et al. Randomized, prospective, comparative study on the effects and safety of sorafenib vs. hepatic arterial infusion chemotherapy in patients with advanced hepatocellular carcinoma with portal vein tumor thrombosis. Cancer Chemother. Pharmacol. 2018, 82, 469–478. [Google Scholar] [CrossRef]
- Zhang, W.; Ouyang, D.; Huang, Z.; Che, X. Hepatic arterial infusion chemotherapy versus sorafenib for advanced hepatocellular carcinoma with portal vein tumor thrombus: An updated meta-analysis and systematic review. Front. Oncol. 2023, 13, 1085166. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef]
- Korean Liver Cancer Association (KLCA); National Cancer Center (NCC) Korea. 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma. J. Liver Cancer 2023, 23, 1126–1240. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, H.; Niizeki, T.; Nagamatsu, H.; Ueshima, K.; Nomura, T.; Kuzuya, T.; Kasai, K.; Kooka, Y.; Hiraoka, A.; Sugimoto, R.; et al. Survival benefit of hepatic arterial infusion chemotherapy over sorafenib in the treatment of locally progressed hepatocellular carcinoma. Cancers 2021, 13, 646. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Cheon, J.; Yoo, C.; Hong, J.Y.; Kim, H.S.; Lee, D.W.; Lee, M.A.; Kim, J.W.; Kim, I.; Oh, S.B.; Hwang, J.E.; et al. Efficacy and safety of atezolizumab plus bevacizumab in Korean patients with advanced hepatocellular carcinoma. Liver Int. 2022, 42, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Fulgenzi, C.A.M.; Cheon, J.; D’Alessio, A.; Nishida, N.; Ang, C.; Marron, T.U.; Wu, L.; Saeed, A.; Wietharn, B.; Cammarota, A.; et al. Reproducible safety and efficacy of atezolizumab plus bevacizumab for HCC in clinical practice: Results of the AB-real study. Eur. J. Cancer 2022, 175, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Casadei-Gardini, A.; Rimini, M.; Tada, T.; Suda, G.; Shimose, S.; Kudo, M.; Cheon, J.; Finkelmeier, F.; Lim, H.Y.; Rimassa, L.; et al. Atezolizumab plus bevacizumab versus lenvatinib for unresectable hepatocellular carcinoma: A large real-life worldwide population. Eur. J. Cancer 2023, 180, 9–20. [Google Scholar] [CrossRef]
- Persano, M.; Rimini, M.; Tada, T.; Suda, G.; Shimose, S.; Kudo, M.; Cheon, J.; Finkelmeier, F.; Lim, H.Y.; Rimassa, L.; et al. Clinical outcomes with atezolizumab plus bevacizumab or lenvatinib in patients with hepatocellular carcinoma: A multicenter real-world study. J. Cancer Res. Clin. Oncol. 2023, 149, 5591–5602. [Google Scholar] [CrossRef]
- D’Alessio, A.; Weinmann, A.; Galle, P.R.; Fulgenzi, C.A.M.; Bettinger, D.; Bengsch, B.; Vogel, A.; Balcar, L.; Scheiner, B.; Navaid, M.; et al. Real-world use of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and Child-Pugh A and B cirrhosis. J. Clin. Oncol. 2022, 40, 393. [Google Scholar] [CrossRef]
- Facciorusso, A.; Serviddio, G.; Muscatiello, N. Transarterial radioembolization vs chemoembolization for hepatocarcinoma patients: A systematic review and meta-analysis. World J. Hepatol. 2016, 8, 770–778. [Google Scholar] [CrossRef]
- Song, M.J. Hepatic artery infusion chemotherapy for advanced hepatocellular carcinoma. World J. Gastroenterol. 2015, 21, 3843–3849. [Google Scholar] [CrossRef]
- Ahn, Y.E.; Suh, S.J.; Yim, H.J.; Seo, Y.S.; Yoon, E.L.; Kim, T.H.; Lee, Y.S.; Yim, S.Y.; Kim, H.R.; Kang, S.H.; et al. Comparison of sorafenib versus hepatic arterial infusion chemotherapy-based treatment for advanced hepatocellular carcinoma with portal vein tumor thrombosis. Gut Liver 2021, 15, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Osaki, Y.; Kita, R.; Kimura, T. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma in Japan. Cancers 2012, 4, 165–183. [Google Scholar] [CrossRef] [PubMed]
- Song, D.S.; Song, M.J.; Bae, S.H.; Chung, W.J.; Jang, J.Y.; Kim, Y.S.; Lee, S.H.; Park, J.Y.; Yim, H.J.; Cho, S.B.; et al. A comparative study between sorafenib and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. J. Gastroenterol. 2015, 50, 445–454. [Google Scholar] [CrossRef]
- D’Alessio, A.; Fulgenzi, C.A.M.; Nishida, N.; Schönlein, M.; von Felden, J.; Schulze, K.; Wege, H.; Gaillard, V.E.; Saeed, A.; Wietharn, B.; et al. Preliminary evidence of safety and tolerability of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and Child-Pugh A and B cirrhosis: A real-world study. Hepatology 2022, 76, 1000–1012. [Google Scholar] [CrossRef]
- Kumari, S.; Mukherjee, S.; Sinha, D.; Abdisalaam, S.; Krishnan, S.; Asaithamby, A. Immunomodulatory effects of radiotherapy. Int. J. Mol. Sci. 2020, 21, 8151. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Toom, S.; Avula, A.; Kumar, V.; Rahma, O.E. The immune modulation effect of locoregional therapies and its potential synergy with immunotherapy in hepatocellular carcinoma. J. Hepatocell. Carcinoma 2020, 7, 11–17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| AB Combination Therapy (n = 114) | HAIC (n = 193) | p-Value | |
|---|---|---|---|
| Age, y | 63.28 (11.86) | 61.99 (11.75) | 0.658 |
| Sex | 0750 | ||
| Male | 99 (86.84%) | 170 (88.08%) | |
| Female | 15 (13.16%) | 23 (11.92%) | |
| BCLC stage | 0.002 | ||
| 0/A (very early, early) | 0 | 2 (1.1%) | |
| B (intermediate) | 9 (9.7%) | 44 (23.5%) | |
| C (advanced) | 105 (90.3%) | 147 (75.4%) | |
| D (end stage) | 0 | 0 | |
| Etiology | 0.893 | ||
| HBV | 73 (64.04%) | 127 (65.80%) | |
| HCV | 4 (3.51%) | 6 (3.11%) | |
| Alcohol use | 20 (17.54%) | 28 (14.51%) | |
| Others | 17 (14.91%) | 32 (16.58%) | |
| Child–Pugh class | <0.001 | ||
| A | 106 (92.98%) | 135 (69.95%) | |
| B | 8 (7.02%) | 55 (28.50%) | |
| C | 0 | 3 (1.55%) | |
| ECOG performance status score | 0.060 | ||
| 0 | 83 (72.81%) | 150 (77.72%) | |
| 1 | 28 (24.56%) | 30 (15.54%) | |
| 2 | 3 (2.63%) | 13 (6.74%) | |
| 3 | 0 | 0 | |
| 4 | 0 | 0 | |
| Serum AFP level (ng/mL) | 9621.65 (19,063.01) | 15,280.12 (34,030.43) | 0.004 |
| Tumor size | 6.51 (5.66) | 8.43 (4.81) | 0.027 |
| Portal vein invasion | 0.039 | ||
| No | 55 (48.25%) | 59 (30.57%) | |
| Yes | 59 (51.75%) | 123 (63.73%) | |
| Distant metastasis | <0.001 | ||
| No | 46 (40.35%) | 145 (75.13%) | |
| Yes | 68 (59.65%) | 48 (24.87%) | |
| Previous treatment | <0.001 | ||
| No | 69 (60.53%) | 76 (39.38%) | |
| Yes | 45 (39.47%) | 117 (60.62%) |
| AB Combination Therapy (n = 83) | HAIC (n = 83) | p-Value | |
|---|---|---|---|
| Age, y | 62.64 (12.55) | 61.92 (13.00) | 0.978 |
| Sex | 0.633 | ||
| Male | 72 (86.75%) | 74 (89.16%) | |
| Female | 11 (13.25) | 9 (10.84) | |
| BCLC stage | |||
| 0/A (very early, early) | 0 | 0 | 0.417 |
| B (intermediate) | 9 (10.84%) | 6 (7.23%) | |
| C (advanced) | 74 (89.16%) | 77 (92.77%) | |
| D (end stage) | 0 | 0 | |
| Etiology | 0.533 | ||
| HBV | 50 (60.24%) | 55 (66.27%) | |
| HCV | 3 (3.61%) | 3 (3.61%) | |
| Alcohol use | 17 (20.48%) | 10 (12.08%) | |
| Others | 13 (15.66%) | 15 (18.07%) | |
| Child–Pugh class | 1.000 | ||
| A | 75 (90.36%) | 75 (90.36%) | |
| B | 8 (9.64%) | 8 (9.64%) | |
| C | 0 | 0 | |
| ECOG performance status score | 0.984 | ||
| 0 | 60 (72.29%) | 61 (73.49%) | |
| 1 | 21 (25.30%) | 20 (24.10%) | |
| 2 | 2 (2.41%) | 2 (2.41%) | |
| 3 | 0 | 0 | |
| 4 | 0 | 0 | |
| Serum AFP level (ng/mL) | 10,746.41 (19,713.23) | 16,524.46 (36,228.35) | 0.204 |
| Tumor size | 8.21 (5.49) | 8.18 (5.24) | 0.969 |
| Portal vein invasion | 0.098 | ||
| No | 32 (38.55%) | 22 (26.51%) | |
| Yes | 51 (61.45%) | 61 (73.49%) | |
| Distant metastasis | 0.347 | ||
| No | 44 (53.01%) | 50 (60.24%) | |
| Yes | 39 (46.99%) | 33 (39.76%) | |
| Previous treatment | 0.349 | ||
| No | 40 (48.19%) | 34 (40.96%) | |
| Yes | 43 (51.81%) | 49 (59.04%) |
| Treatment Responses | AB Combination Therapy (n = 114) | HAIC (n = 193) | p-Value |
|---|---|---|---|
| <0.001 | |||
| CR | 6 (5.26%) | 11 (5.70%) | |
| PR | 36 (31.58%) | 31 (16.06%) | |
| SD | 43 (37.72%) | 135 (69.95%) | |
| PD | 29 (25.44%) | 15 (7.77%) | |
| ORR | 42/114 (36.84%) | 42/193 (21.76%) | 0.003 |
| DCR | 85/114 (74.56%) | 177/193 | <0.001 |
| Treatment Responses | AB Combination Therapy (n = 83) | HAIC (n = 83) | p-Value |
|---|---|---|---|
| 0.001 | |||
| CR | 1 (1.20%) | 9 (10.84%) | |
| PR | 29 (34.94%) | 15 (18.07%) | |
| SD | 33 (39.76%) | 49 (59.04%) | |
| PD | 20 (24.10%) | 10 (12.05%) | |
| ORR | 30/83 (36.14%) | 24/83 (28.92%) | 0.320 |
| DCR | 63/83 (75.90%) | 73/83 (87.95%) | 0.044 |
| Variables | Overall Survival | Progression-Free Survival | ||||
|---|---|---|---|---|---|---|
| Univariate (p-Value) | Multivariate (p-Value) | HR (95% CI) | Univariate (p-Value) | Multivariate (p-Value) | HR (95% CI) | |
| AB therapy vs. HAIC | 0.132 | 0.034 | ||||
| Age | 0.306 | 0.226 | ||||
| Sex | 0.735 | 0.743 | ||||
| Etiology | 0.052 | 0.446 | ||||
| Tumor size | 0.150 | 0.100 | ||||
| Serum AFP < 1000 ng/mL | 0.111 | 0.046 | 0.131 | 0.810 (0.616–1.065) | ||
| ECOG performance status 0 and 1 | 0.002 | 0.078 | 0.929 (0.738–2.435) | 0.151 | ||
| Distant metastasis | 0.071 | 0.005 | 0.002 | 1.572 (1.182–2.092) | ||
| Portal vein invasion | 0.964 | 0.517 | ||||
| Child–Pugh class A | <0.001 | <0.001 | 0.397 (0.277–0.568) | <0.001 | <0.001 | 0.435 (0.314–0.603) |
| Previous treatment | 0.132 | 0.061 | ||||
| Adverse Events | AB Combination Therapy (n = 114) | HAIC (n = 193) | p-Value |
|---|---|---|---|
| Total | 22 | 69 | 0.001 |
| AST/ALT (>×5 ULN) | 8 | 32 | 0.016 |
| Colitis | 3 | 3 | 0.510 |
| Fatigue | 3 | 8 | 0.013 |
| Pneumonitis | 1 | 0 | 0.192 |
| Hyperbilirubinemia | 2 | 26 | 0.001 |
| Skin rash | 1 | 0 | 0.192 |
| Anaphylactic shock | 1 | 0 | 0.192 |
| Myositis | 1 | 0 | 0.192 |
| Asthma | 1 | 0 | 0.192 |
| Thyroiditis | 1 | 0 | 0.192 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.H.; Nam, H.-C.; Kim, C.-W.; Cho, H.S.; Yoo, J.-S.; Han, J.W.; Jang, J.W.; Choi, J.Y.; Yoon, S.K.; Yang, H.; et al. Comparative Analysis of Atezolizumab Plus Bevacizumab and Hepatic Artery Infusion Chemotherapy in Unresectable Hepatocellular Carcinoma: A Multicenter, Propensity Score Study. Cancers 2023, 15, 4233. https://doi.org/10.3390/cancers15174233
Kim JH, Nam H-C, Kim C-W, Cho HS, Yoo J-S, Han JW, Jang JW, Choi JY, Yoon SK, Yang H, et al. Comparative Analysis of Atezolizumab Plus Bevacizumab and Hepatic Artery Infusion Chemotherapy in Unresectable Hepatocellular Carcinoma: A Multicenter, Propensity Score Study. Cancers. 2023; 15(17):4233. https://doi.org/10.3390/cancers15174233
Chicago/Turabian StyleKim, Ji Hoon, Hee-Chul Nam, Chang-Wook Kim, Hee Sun Cho, Jae-Sung Yoo, Ji Won Han, Jeong Won Jang, Jong Young Choi, Seung Kew Yoon, Hyun Yang, and et al. 2023. "Comparative Analysis of Atezolizumab Plus Bevacizumab and Hepatic Artery Infusion Chemotherapy in Unresectable Hepatocellular Carcinoma: A Multicenter, Propensity Score Study" Cancers 15, no. 17: 4233. https://doi.org/10.3390/cancers15174233