
Sonoelastography for Testicular Tumor Identification: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy

 ,
, 
 and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
- How well can sonoelastography distinguish a testicular neoplasm from a non-neoplasm (i.e., identify a tumor)?
- How well can sonoelastography classify benign and malignant tumors?
- What are the sonoelastographic determinants for the identification/classification? And how could they be obtained?
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Source
2.3. Search Strategy
2.4. Study Selection Process
2.5. Data Collection and Extraction
2.6. Methodological Quality Assessment
2.7. Meta-Analysis
3. Results
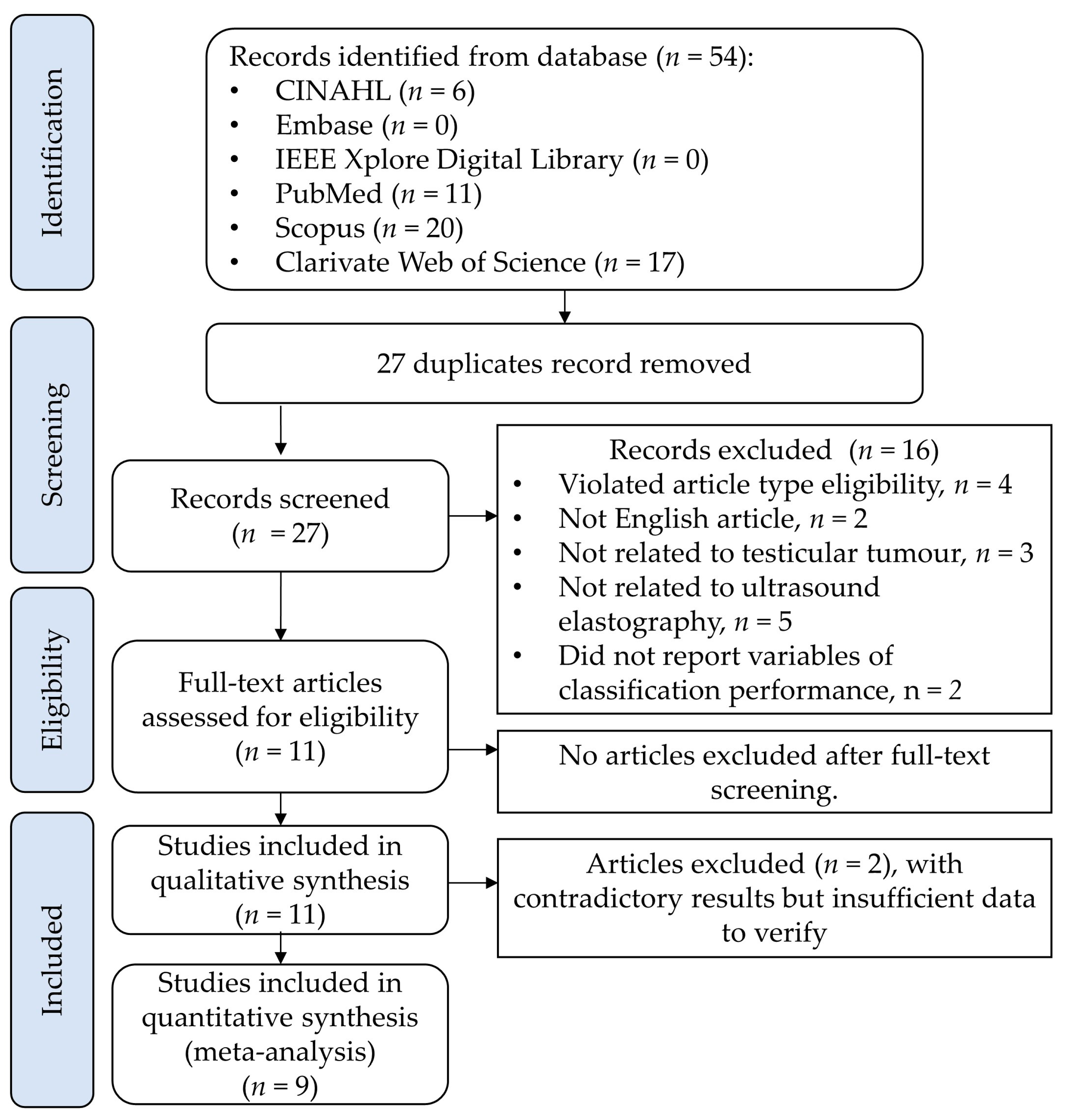
3.1. Search and Study Selection Results
3.2. Qualitative Synthesis
3.2.1. Population
3.2.2. Index Test
3.2.3. Reference Test
3.2.4. Outcome Measures and Classification
3.2.5. Study Quality (Risk of Bias and Applicability)
3.3. Quantitative Synthesis
Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peng, X.; Zeng, X.; Peng, S.; Deng, D.; Zhang, J. The association risk of male subfertility and testicular cancer: A systematic review. PLoS ONE 2009, 4, e5591. [Google Scholar] [CrossRef] [PubMed]
- Znaor, A.; Skakkebaek, N.E.; Rajpert-De Meyts, E.; Kuliš, T.; Laversanne, M.; Gurney, J.; Sarfati, D.; McGlynn, K.A.; Bray, F. Global patterns in testicular cancer incidence and mortality in 2020. Int. J. Cancer 2022, 151, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Gurney, J.K.; Florio, A.A.; Znaor, A.; Ferlay, J.; Laversanne, M.; Sarfati, D.; Bray, F.; McGlynn, K.A. International trends in the incidence of testicular cancer: Lessons from 35 years and 41 countries. Eur. Urol. 2019, 76, 615–623. [Google Scholar] [CrossRef]
- Znaor, A.; Lortet-Tieulent, J.; Jemal, A.; Bray, F. International variations and trends in testicular cancer incidence and mortality. Eur. Urol. 2014, 65, 1095–1106. [Google Scholar] [CrossRef]
- Garner, M.J.; Turner, M.C.; Ghadirian, P.; Krewski, D. Epidemiology of testicular cancer: An overview. Int. J. Cancer 2005, 116, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Le Cornet, C.; Lortet-Tieulent, J.; Forman, D.; Béranger, R.; Flechon, A.; Fervers, B.; Schüz, J.; Bray, F. Testicular cancer incidence to rise by 25% by 2025 in Europe? Model-based predictions in 40 countries using population-based registry data. Eur. J. Cancer 2014, 50, 831–839. [Google Scholar] [CrossRef]
- Winter, C.; Albers, P. Testicular germ cell tumors: Pathogenesis, diagnosis and treatment. Nat. Rev. Endocrinol. 2011, 7, 43–53. [Google Scholar] [CrossRef]
- Yin, X.; Xu, Y.; Man, X.; Liu, L.; Jiang, Y.; Zhao, L.; Cheng, W. Direct costs of both inpatient and outpatient care for all type cancers: The evidence from Beijing, China. Cancer Med. 2019, 8, 3250–3260. [Google Scholar] [CrossRef] [Green Version]
- Michaeli, T.; Michaeli, J.; Michaeli, D. Testicular cancer follow-up costs in Germany from 2000 to 2015. J. Cancer Res. Clin. Oncol. 2021, 147, 2249–2258. [Google Scholar] [CrossRef]
- Fung, C.; Dinh, P.C.; Fossa, S.D.; Travis, L.B. Testicular cancer survivorship. J. Natl. Compr. Cancer Netw. 2019, 17, 1557–1568. [Google Scholar] [CrossRef] [Green Version]
- Raphael, M.J.; Gupta, S.; Wei, X.; Peng, Y.; Soares, C.N.; Bedard, P.L.; Siemens, D.R.; Robinson, A.G.; Booth, C.M. Long-term mental health service utilization among survivors of testicular cancer: A population-based cohort study. J. Clin. Oncol. 2021, 39, 779–786. [Google Scholar] [CrossRef]
- Smith, A.B.; Rutherford, C.; Butow, P.; Olver, I.; Luckett, T.; Grimison, P.; Toner, G.; Stockler, M.; King, M. A systematic review of quantitative observational studies investigating psychological distress in testicular cancer survivors. Psycho-Oncology 2018, 27, 1129–1137. [Google Scholar] [CrossRef]
- Rincones, O.; Smith, A.B.; Naher, S.; Mercieca-Bebber, R.; Stockler, M. An updated systematic review of quantitative studies assessing anxiety, depression, fear of cancer recurrence or psychological distress in testicular cancer survivors. Cancer Manag. Res. 2021, 13, 3803–3816. [Google Scholar] [CrossRef] [PubMed]
- Schepisi, G.; De Padova, S.; De Lisi, D.; Casadei, C.; Meggiolaro, E.; Ruffilli, F.; Rosti, G.; Lolli, C.; Ravaglia, G.; Conteduca, V. Psychosocial issues in long-term survivors of testicular cancer. Front. Endocrinol. 2019, 10, 113. [Google Scholar] [CrossRef] [Green Version]
- Alexis, O.; Adeleye, A.O.; Worsley, A.J. Men’s experiences of surviving testicular cancer: An integrated literature review. J. Cancer Surviv. 2020, 14, 284–293. [Google Scholar] [CrossRef]
- Rajpert-De Meyts, E.; McGlynn, K.A.; Okamoto, K.; Jewett, M.A.; Bokemeyer, C. Testicular germ cell tumours. Lancet 2016, 387, 1762–1774. [Google Scholar] [CrossRef]
- Bray, F.; Richiardi, L.; Ekbom, A.; Forman, D.; Pukkala, E.; Cuninkova, M.; Møller, H. Do testicular seminoma and nonseminoma share the same etiology? Evidence from an age-period-cohort analysis of incidence trends in eight European countries. Cancer Epidemiol. Biomark. Prev. 2006, 15, 652–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Devesa, S.S.; McGlynn, K.A.; Møller, H. Interpreting the international trends in testicular seminoma and nonseminoma incidence. Nat. Clin. Pract. Urol. 2006, 3, 532–543. [Google Scholar] [CrossRef]
- Shaw, J. Diagnosis and treatment of testicular cancer. Am. Fam. Physician 2008, 77, 469–474. [Google Scholar] [PubMed]
- Cieślikowski, W.A.; Kasperczak, M.; Milecki, T.; Antczak, A. Reasons behind the Delayed Diagnosis of Testicular Cancer: A Retrospective Analysis. Int. J. Environ. Res. Public Health 2023, 20, 4752. [Google Scholar] [CrossRef] [PubMed]
- Aberger, M.; Wilson, B.; Holzbeierlein, J.M.; Griebling, T.L.; Nangia, A.K. Testicular self-examination and testicular cancer: A cost-utility analysis. Cancer Med. 2014, 3, 1629–1634. [Google Scholar] [CrossRef] [PubMed]
- Baird, D.C.; Meyers, G.J.; Hu, J.S. Testicular cancer: Diagnosis and treatment. Am. Fam. Physician 2018, 97, 261–268. [Google Scholar]
- Minhas, S.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropoulos, K.; Gül, M. European association of urology guidelines on male sexual and reproductive health: 2021 update on male infertility. Eur. Urol. 2021, 80, 603–620. [Google Scholar] [CrossRef] [PubMed]
- Rocher, L.; Ramchandani, P.; Belfield, J.; Bertolotto, M.; Derchi, L.E.; Correas, J.M.; Oyen, R.; Tsili, A.C.; Turgut, A.T.; Dogra, V. Incidentally detected non-palpable testicular tumours in adults at scrotal ultrasound: Impact of radiological findings on management Radiologic review and recommendations of the ESUR scrotal imaging subcommittee. Eur. Radiol. 2016, 26, 2268–2278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, C.; Huang, D.Y.; Sidhu, P.S. Elastography of focal testicular lesions: Current concepts and utility. Ultrasonography 2019, 38, 302. [Google Scholar] [CrossRef] [Green Version]
- Shilo, Y.; Zisman, A.; Lindner, A.; Raz, O.; Strauss, S.; Siegel, Y.I.; Segal, M.; Sandbank, J.; Leibovici, D. The predominance of benign histology in small testicular masses. Urol. Oncol. 2012, 30, 719–722. [Google Scholar] [CrossRef]
- Appelbaum, L.; Gaitini, D.; Dogra, V.S. Scrotal ultrasound in adults. Semin. Ultrasound CT MRI 2013, 34, 257–273. [Google Scholar] [CrossRef]
- Lung, P.F.; Jaffer, O.S.; Sellars, M.E.; Sriprasad, S.; Kooiman, G.G.; Sidhu, P.S. Contrast-enhanced ultrasound in the evaluation of focal testicular complications secondary to epididymitis. Am. J. Roentgenol. 2012, 199, W345–W354. [Google Scholar] [CrossRef]
- Garra, B.S. Elastography: History, principles, and technique comparison. Abdom. Imaging 2015, 40, 680–697. [Google Scholar] [CrossRef]
- Villani, R.; Lupo, P.; Sangineto, M.; Romano, A.D.; Serviddio, G. Liver Ultrasound Elastography in Non-Alcoholic Fatty Liver Disease: A State-of-the-Art Summary. Diagnostics 2023, 13, 1236. [Google Scholar] [CrossRef]
- Zheng, Y.-P.; Mak, T.-M.; Huang, Z.-M.; Cheung, C.-W.J.; Zhou, Y.-J.; He, J.-F. Liver fibrosis assessment using transient elastography guided with real-time b-mode ultrasound imaging. In 6th World Congress of Biomechanics (WCB 2010), 1–6 August 2010, Singapore: In Conjunction with 14th International Conference on Biomedical Engineering (ICBME) and 5th Asia Pacific Conference on Biomechanics (APBiomech); Springer Science & Business Media: Berlin, Germany, 2010; pp. 1036–1039. [Google Scholar]
- Liao, J.; Yang, H.; Yu, J.; Liang, X.; Chen, Z. Progress in the application of ultrasound elastography for brain diseases. J. Ultrasound Med. 2020, 39, 2093–2104. [Google Scholar] [CrossRef]
- Ying, M.; Zheng, Y.-P.; Kot, B.C.-W.; Cheung, J.C.-W.; Cheng, S.C.-H.; Kwong, D.L.-W. Three-dimensional elastography for cervical lymph node volume measurements: A study to investigate feasibility, accuracy and reliability. Ultrasound Med. Biol. 2013, 39, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Z.; Smith, J.; Kim, K. Current Status and Advancement of Ultrasound Imaging Technologies in Musculoskeletal Studies. Curr. Phys. Med. Rehabil. Rep. 2022, 10, 45–51. [Google Scholar] [CrossRef]
- Chen, T.L.-W.; Agresta, C.E.; Lipps, D.B.; Provenzano, S.G.; Hafer, J.F.; Wong, D.W.-C.; Zhang, M.; Zernicke, R.F. Ultrasound elastographic assessment of plantar fascia in runners using rearfoot strike and forefoot strike. J. Biomech. 2019, 89, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.-J.; Lim, H.-J.; Ni, M.; Yan, W.-H.; Wong, D.W.-C.; Cheung, J.C.-W. Breast tumour classification using ultrasound elastography with machine learning: A systematic scoping review. Cancers 2022, 14, 367. [Google Scholar] [CrossRef]
- Mao, Y.-J.; Zha, L.-W.; Tam, A.Y.-C.; Lim, H.-J.; Cheung, A.K.-Y.; Zhang, Y.-Q.; Ni, M.; Cheung, J.C.-W.; Wong, D.W.-C. Endocrine Tumor Classification via Machine-Learning-Based Elastography: A Systematic Scoping Review. Cancers 2023, 15, 837. [Google Scholar] [CrossRef]
- Emara, D.M.; Naguib, N.N.; Yehia, M.; El Shafei, M.M. Ultrasound elastography in characterization of prostatic lesions: Correlation with histopathological findings. Br. J. Radiol. 2020, 93, 20200035. [Google Scholar] [CrossRef] [PubMed]
- Isidori, A.M.; Pozza, C.; Gianfrilli, D.; Giannetta, E.; Lemma, A.; Pofi, R.; Barbagallo, F.; Manganaro, L.; Martino, G.; Lombardo, F. Differential diagnosis of nonpalpable testicular lesions: Qualitative and quantitative contrast-enhanced US of benign and malignant testicular tumors. Radiology 2014, 273, 606–618. [Google Scholar] [CrossRef]
- Bertolotto, M.; Muça, M.; Currò, F.; Bucci, S.; Rocher, L.; Cova, M.A. Multiparametric US for scrotal diseases. Abdom. Radiol. 2018, 43, 899–917. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group*. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Trikalinos, T.A.; Balion, C.M.; Coleman, C.I.; Griffith, L.; Santaguida, P.L.; Vandermeer, B.; Fu, R. Chapter 8: Meta-analysis of test performance when there is a “gold standard”. J. Gen. Intern. Med. 2012, 27, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, T.A.; Alabousi, M.; Skidmore, B.; Korevaar, D.A.; Bossuyt, P.M.; Moher, D.; Thombs, B.; McInnes, M.D. Recommendations for reporting of systematic reviews and meta-analyses of diagnostic test accuracy: A systematic review. Syst. Rev. 2017, 6, 194. [Google Scholar] [CrossRef]
- Deeks, J.J.; Macaskill, P.; Irwig, L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 2005, 58, 882–893. [Google Scholar] [CrossRef]
- Freeman, S.C.; Kerby, C.R.; Patel, A.; Cooper, N.J.; Quinn, T.; Sutton, A.J. Development of an interactive web-based tool to conduct and interrogate meta-analysis of diagnostic test accuracy studies: MetaDTA. BMC Med. Res. Methodol. 2019, 19, 81. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Cooper, N.; Freeman, S.; Sutton, A. Graphical enhancements to summary receiver operating characteristic plots to facilitate the analysis and reporting of meta-analysis of diagnostic test accuracy data. Res. Synth. Methods 2021, 12, 34–44. [Google Scholar] [CrossRef]
- Aigner, F.; De Zordo, T.; Pallwein-Prettner, L.; Junker, D.; Schäfer, G.; Pichler, R.; Leonhartsberger, N.; Pinggera, G.; Dogra, V.S.; Frauscher, F.; et al. Real-time sonoelastography for the evaluation of testicular lesions. Radiology 2012, 263, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Auer, T.; De Zordo, T.; Dejaco, C.; Gruber, L.; Pichler, R.; Jaschke, W.; Dogra, V.S.; Aigner, F. Value of Multiparametric US in the Assessment of Intratesticular Lesions. Radiology 2017, 285, 640–649. [Google Scholar] [CrossRef] [Green Version]
- Corcioni, B.; Brandi, N.; Marasco, G.; Gaudiano, C.; De Cinque, A.; Ciccarese, F.; Ercolino, A.; Schiavina, R.; Brunocilla, E.; Renzulli, M.; et al. Multiparametric ultrasound for the diagnosis of Leydig cell tumours in non-palpable testicular lesions. Andrology 2022, 10, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- Goddi, A.; Sacchi, A.; Magistretti, G.; Almolla, J.; Salvadore, M.; Goddi, A.; Sacchi, A.; Magistretti, G.; Almolla, J.; Salvadore, M. Real-time tissue elastography for testicular lesion assessment. Eur. Radiol. 2012, 22, 721–730. [Google Scholar] [CrossRef] [Green Version]
- Konstantatou, E.; Fang, C.; Romanos, O.; Derchi, L.E.; Bertolotto, M.; Valentino, M.; Kalogeropoulou, C.; Sidhu, P.S. Evaluation of Intratesticular Lesions with Strain Elastography Using Strain Ratio and Color Map Visual Grading: Differentiation of Neoplastic and Nonneoplastic Lesions. J. Ultrasound Med. 2019, 38, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Pozza, C.; Gianfrilli, D.; Fattorini, G.; Giannetta, E.; Barbagallo, F.; Nicolai, E.; Cristini, C.; Di Pierro, G.B.; Franco, G.; Lenzi, A.; et al. Diagnostic value of qualitative and strain ratio elastography in the differential diagnosis of non-palpable testicular lesions. Andrology 2016, 4, 1193–1203. [Google Scholar] [CrossRef]
- Reginelli, A.; D’Andrea, A.; Clemente, A.; Izzo, A.; Urraro, F.; Scala, F.; Nardone, V.; Guida, C.; Scialpi, M.; Cappabianca, S. Does multiparametric US improve diagnostic accuracy in the characterization of small testicular masses? Gland Surg. 2019, 8, S136–S141. [Google Scholar] [CrossRef] [PubMed]
- Rocher, L.; Criton, A.; Gennisson, J.-L.; Creze, M.; Albiges, L.; Ferlicot, S.; Bellin, M.-F.; Izard, V.; Correas, J.-M. Characterization of Testicular Masses in Adults: Performance of Combined Quantitative Shear Wave Elastography and Conventional Ultrasound. Ultrasound Med. Biol. 2019, 45, 720–731. [Google Scholar] [CrossRef]
- Roy, C.; de Marini, P.; Labani, A.; Leyendecker, P.; Ohana, M. Shear-wave elastography of the testicle: Potential role of the stiffness value in various common testicular diseases. Clin. Radiol. 2020, 75, 560.e9–560.e17. [Google Scholar] [CrossRef]
- Schröder, C.; Lock, G.; Schmidt, C.; Löning, T.; Dieckmann, K.-P. Real-Time Elastography and Contrast-Enhanced Ultrasonography in the Evaluation of Testicular Masses: A Comparative Prospective Study. Ultrasound Med. Biol. 2016, 42, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, M.S. Use of strain sonoelastography in differentiation of focal testicular lesions. Egypt. J. Radiol. Nucl. Med. 2017, 48, 485–491. [Google Scholar] [CrossRef]
- Sidhu, P.S.; Cantisani, V.; Dietrich, C.F.; Gilja, O.H.; Saftoiu, A.; Bartels, E.; Bertolotto, M.; Calliada, F.; Clevert, D.-A.; Cosgrove, D. The EFSUMB guidelines and recommendations for the clinical practice of contrast-enhanced ultrasound (CEUS) in non-hepatic applications: Update 2017 (long version). Ultraschall Der Med.-Eur. J. Ultrasound 2018, 39, e2–e44. [Google Scholar]
- Erkamp, R.Q.; Emelianov, S.Y.; Skovoroda, A.R.; O’Donnell, M. Nonlinear elasticity imaging: Theory and phantom study. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2004, 51, 532–539. [Google Scholar] [CrossRef]
- Schurich, M.; Aigner, F.; Frauscher, F.; Pallwein, L. The role of ultrasound in assessment of male fertility. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 144, S192–S198. [Google Scholar] [CrossRef]
- Konofagou, E.E.; Ophir, J.; Kallel, F.; Varghese, T. Elastographic dynamic range expansion using variable applied strains. Ultrason. Imaging 1997, 19, 145–166. [Google Scholar] [CrossRef]
- Varghese, T.; Zagzebski, J.; Frank, G.; Madsen, E. Elastographic imaging using a handheld compressor. Ultrason. Imaging 2002, 24, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Cantisani, V.; Di Leo, N.; Bertolotto, M.; Fresilli, D.; Granata, A.; Polti, G.; Polito, E.; Pacini, P.; Guiban, O.; Del Gaudio, G. Role of multiparametric ultrasound in testicular focal lesions and diffuse pathology evaluation, with particular regard to elastography: Review of literature. Andrology 2021, 9, 1356–1368. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, J.F.; Ewertsen, C.; Lönn, L.; Nielsen, M.B. Strain elastography ultrasound: An overview with emphasis on breast cancer diagnosis. Diagnostics 2013, 3, 117–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, A.; Ueno, E.; Tohno, E.; Kamma, H.; Takahashi, H.; Shiina, T.; Yamakawa, M.; Matsumura, T. Breast disease: Clinical application of US elastography for diagnosis. Radiology 2006, 239, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Sellars, M.E.; Clarke, J.L.; Sidhu, P.S. Features of testicular epidermoid cysts on contrast-enhanced sonography and real-time tissue elastography. J. Ultrasound Med. 2012, 31, 115–122. [Google Scholar] [CrossRef]
- Yusuf, G.; Konstantatou, E.; Sellars, M.E.; Huang, D.Y.; Sidhu, P.S. Multiparametric sonography of testicular hematomas: Features on grayscale, color Doppler, and contrast-enhanced sonography and strain elastography. J. Ultrasound Med. 2015, 34, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO classification of tumours of the urinary system and male genital organs—Part A: Renal, penile, and testicular tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef]
- Albers, P.; Albrecht, W.; Algaba, F.; Bokemeyer, C.; Cohn-Cedermark, G.; Fizazi, K.; Horwich, A.; Laguna, M.P.; Nicolai, N.; Oldenburg, J. Guidelines on testicular cancer: 2015 update. Eur. Urol. 2015, 68, 1054–1068. [Google Scholar] [CrossRef]
- Winstanley, A.; Mikuz, G.; Debruyne, F.; Schulman, C.; Parkinson, M.C. Handling and reporting of biopsy and surgical specimens of testicular cancer. Eur. Urol. 2004, 45, 564–573. [Google Scholar] [CrossRef]
- Manganaro, L.; Vinci, V.; Pozza, C.; Saldari, M.; Gianfrilli, D.; Pofi, R.; Bernardo, S.; Cantisani, V.; Lenzi, A.; Scialpi, M. A prospective study on contrast-enhanced magnetic resonance imaging of testicular lesions: Distinctive features of Leydig cell tumours. Eur. Radiol. 2015, 25, 3586–3595. [Google Scholar] [CrossRef]
- Zhelev, Z.; Garside, R.; Hyde, C. A qualitative study into the difficulties experienced by healthcare decision makers when reading a Cochrane diagnostic test accuracy review. Syst. Rev. 2013, 2, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, J.; Ioannidis, J.P.; Terrin, N.; Schmid, C.H.; Olkin, I. The case of the misleading funnel plot. BMJ 2006, 333, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Pinto, S.P.; Huang, D.Y.; Dinesh, A.A.; Sidhu, P.S.; Ahmed, K. A systematic review on the use of qualitative and quantitative contrast-enhanced ultrasound in diagnosing testicular abnormalities. Urology 2021, 154, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Min, L.; Jun, L.; Zhiqian, W.; Weiwei, Z. Research on acoustic radiation force impulse imaging in quantitative assessment of testicular stiffness in non-sterility varicocele patients. J. Diagn. Concepts Pract. 2019, 18, 543. [Google Scholar]
- Gilbertson, M.W.; Anthony, B.W. Force and position control system for freehand ultrasound. IEEE Trans. Robot. 2015, 31, 835–849. [Google Scholar] [CrossRef]
- Li, K.; Xu, Y.; Meng, M.Q.-H. An overview of systems and techniques for autonomous robotic ultrasound acquisitions. IEEE Trans. Med. Robot. Bionics 2021, 3, 510–524. [Google Scholar] [CrossRef]
- Marcon, J.; Trottmann, M.; Rübenthaler, J.; D’Anastasi, M.; Stief, C.; Reiser, M.; Clevert, D. Three-dimensional vs. two-dimensional shear-wave elastography of the testes–preliminary study on a healthy collective. Clin. Hemorheol. Microcirc. 2016, 64, 447–456. [Google Scholar] [CrossRef]
- Fan, C.; Sun, K.; Min, X.; Cai, W.; Lv, W.; Ma, X.; Li, Y.; Chen, C.; Zhao, P.; Qiao, J. Discriminating malignant from benign testicular masses using machine-learning based radiomics signature of appearance diffusion coefficient maps: Comparing with conventional mean and minimum ADC values. Eur. J. Radiol. 2022, 148, 110158. [Google Scholar] [CrossRef]
- Jiang, H.; Diao, Z.; Shi, T.; Zhou, Y.; Wang, F.; Hu, W.; Zhu, X.; Luo, S.; Tong, G.; Yao, Y.-D. A review of deep learning-based multiple-lesion recognition from medical images: Classification, detection and segmentation. Comput. Biol. Med. 2023, 157, 106726. [Google Scholar] [CrossRef]
- Wang, P.; Fan, E.; Wang, P. Comparative analysis of image classification algorithms based on traditional machine learning and deep learning. Pattern Recognit. Lett. 2021, 141, 61–67. [Google Scholar] [CrossRef]
- Nakata, N.; Siina, T. Ensemble Learning of Multiple Models Using Deep Learning for Multiclass Classification of Ultrasound Images of Hepatic Masses. Bioengineering 2023, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Moon, W.K.; Lee, Y.-W.; Ke, H.-H.; Lee, S.H.; Huang, C.-S.; Chang, R.-F. Computer-aided diagnosis of breast ultrasound images using ensemble learning from convolutional neural networks. Comput. Methods Programs Biomed. 2020, 190, 105361. [Google Scholar] [CrossRef] [PubMed]
- Trikalinos, T.A.; Balion, C.M. Chapter 9: Options for summarizing medical test performance in the absence of a “gold standard”. J. Gen. Intern. Med. 2012, 27, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Smeden, M.; Naaktgeboren, C.A.; Reitsma, J.B.; Moons, K.G.; de Groot, J.A. Latent class models in diagnostic studies when there is no reference standard—A systematic review. Am. J. Epidemiol. 2014, 179, 423–431. [Google Scholar] [CrossRef] [Green Version]
- Chu, H.; Chen, S.; Louis, T.A. Random effects models in a meta-analysis of the accuracy of two diagnostic tests without a gold standard. J. Am. Stat. Assoc. 2009, 104, 512–523. [Google Scholar] [CrossRef] [Green Version]
- Trikalinos, T.A.; Kulasingam, S.; Lawrence, W.F. Chapter 10: Deciding whether to complement a systematic review of medical tests with decision modeling. J. Gen. Intern. Med. 2012, 27, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Sainfort, F.; Kuntz, K.M.; Gregory, S.; Butler, M.; Taylor, B.C.; Kulasingam, S.; Kane, R.L. Adding decision models to systematic reviews: Informing a framework for deciding when and how to do so. Value Health 2013, 16, 133–139. [Google Scholar] [CrossRef]
- Grasso, M.; Blanco, S.; Raber, M.; Nespoli, L. Elasto-sonography of the testis: Preliminary experience. Arch. Ital. Urol. Androl. 2010, 82, 160–163. [Google Scholar]
- Lock, G.; Schröder, C.; Schmidt, C.; Anheuser, P.; Loening, T.; Dieckmann, K. Contrast-enhanced ultrasound and real-time elastography for the diagnosis of benign Leydig cell tumors of the testis–a single center report on 13 cases. Ultraschall Der Med.-Eur. J. Ultrasound 2014, 35, 534–539. [Google Scholar] [CrossRef]
- Patel, K.V.; Huang, D.Y.; Sidhu, P.S. Metachronous bilateral segmental testicular infarction: Multi-parametric ultrasound imaging with grey-scale ultrasound, Doppler ultrasound, contrast-enhanced ultrasound (CEUS) and real-time tissue elastography (RTE). J. Ultrasound 2014, 17, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, M.R.; Møller, H.; Osther, P.J.S.; Vedsted, P.; Holst, R.; Rafaelsen, S.R. Comparison of tissue stiffness using shear wave elastography in men with normal testicular tissue, testicular microlithiasis and testicular cancer. Ultrasound Int. Open 2017, 3, E150–E155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dikici, A.S.; Er, M.E.; Alis, D.; Samanci, C.; Ustabasioglu, F.E.; Demirdag, C.; Durak, H.; Kantarci, F.; Mihmanli, I. Is there any difference between seminomas and nonseminomatous germ cell tumors on shear wave elastography? A preliminary study. J. Ultrasound Med. 2016, 35, 2575–2580. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.K.; Harky, A. The importance of risk of bias assessment in meta-analyses: Does controlling heterogeneity suffice? Eur. J. Cardio-Thorac. Surg. 2020, 58, 1102. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Sterne, J.A.; Higgins, J.P.; Egger, M. Investigating and dealing with publication bias and other reporting biases in meta-analyses of health research: A review. Res. Synth. Methods 2021, 12, 248–259. [Google Scholar] [CrossRef]
- Sharifabadi, A.D.; Korevaar, D.; McGrath, T.; van Es, N.; Frank, R.; Cherpak, L.; Dang, W.; Salameh, J.; Nguyen, F.; Stanley, C. Reporting bias in imaging: Higher accuracy is linked to faster publication. Eur. Radiol. 2018, 28, 3632–3639. [Google Scholar] [CrossRef]
- Nyaga, V.N.; Aerts, M.; Arbyn, M. ANOVA model for network meta-analysis of diagnostic test accuracy data. Stat. Methods Med. Res. 2018, 27, 1766–1784. [Google Scholar] [CrossRef] [Green Version]
- Belfield, J.; Findlay-Line, C. Testicular Germ Cell Tumours—The Role of Conventional Ultrasound. Cancers 2022, 14, 3882. [Google Scholar] [CrossRef]
- Maxwell, F.; Savignac, A.; Bekdache, O.; Calvez, S.; Lebacle, C.; Arama, E.; Garrouche, N.; Rocher, L. Leydig Cell Tumors of the Testis: An Update of the Imaging Characteristics of a Not So Rare Lesion. Cancers 2022, 14, 3652. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Sample Size | Mean Age | Sampling | Patient Source | Referral Indications |
|---|---|---|---|---|---|
| Aigner et al. [47] (2012) | 50 PP/PT | 42 (18–81) | Retrospective, consecutive | - | Patients with clinical suspicion of testicular tumor |
| Auer et al. [48] (2017) | 55 PP/PT | 39.5 (SD: 14.9) | Retrospective, consecutive | Radiology department | Evaluations of scrotal pain, scrotal abnormality, varicoceles, infertility, sexual development disorder, and F/U indetermined scrotal ultrasound findings. |
| Corcioni et al. [49] (2022) | * 78 PP/81 PT | 34.3 (SD:12.2)+ 35.8 (SD:12.2)− | Prospective, consecutive | University hospital | Infertility, andrological screening, testicular pain |
| Goddi et al. [50] (2012) | 88 PT | # 34 (2 months–89 years) | Consecutive | Medical Center | Scrotal abnormalities |
| Konstantatou et al. [51] (2019) | 86 PP/PT | Median: 36 (16–81) | Retrospective, consecutive | Hospital | Acute and nonacute scrotal conditions, indetermined focal intratesticular abnormality |
| Pozza et al. [52] (2016) | 106 PP | 34.5 (28–41.2) | Prospective, consecutive | Inpatients and outpatients referred to University | Infertility, andrological screening, F/U contralateral or ipsilateral tumor, testicular pain, varicocele, Klinefelter’s syndrome, F/U microlithiasis, elevated level of alpha-fetoprotein |
| Reginelli et al. [53] (2019) | 54 PP/PT | Median: 42.2 (10–64) | Retrospective, consecutive | - | Clinical suspicion of testicular mass |
| Rocher et al. [54] (2019) | 86 PP 89 PT | 37.9 (SD: 13.2) | Prospective, consecutive | - | Infertility, pain, abnormal self-palpation, and others |
| Roy et al. [55] (2020) | ! 338 PP 606 PT | 43.2 (SD: 17.2, 17–78) | Prospective, consecutive | Ultrasound department | - |
| Schröder et al. [56] (2016) | 67 PP 68 PT | Median: 39.8 (18–83) | Prospective, Consecutive | - | Suspicious testicular mass |
| Shaaban [57] (2017) | 21 PP 23 PT | 30 (18–54) | - | - | - |
| Non-Neoplastic (Non-Tumor) | Neoplastic (Tumor) | |
|---|---|---|
| Benignity | Malignancy | |
|
|
|
| Article | Index Test (Instrument) | Measurements and Features | ||
|---|---|---|---|---|
| Elastography | Other B-Mode US/Doppler | Comparison | ||
| Aigner et al. [47] | SE: HI Vision EUB 8500 | Sequoia 512 | B vs. Doppler vs. SE |
|
| Auer et al. [48] | SE: HI Vision Ascendus | Logic E9 | Doppler vs. CEUS vs. SE vs. (Doppler + SE) vs. (CEUS + SE) |
|
| Corcioni et al. [49] | SE: Aplio 500 | Esaote MyLab 70 Gold XVG | SE vs. CEUS |
|
| Goddi et al. [50] | SE: HI Vision EUB 8500 | Preirus | B + SE + Doppler |
|
| Konstantatou et al. [51] | SE: Hitachi HV900 | Siemens S2000 | B vs. Doppler vs. SE |
|
| Pozza et al. [52] | SE: Philips IU22 | - | B vs. SE |
|
| Reginelli et al. [53] | SE: Hi-Vision Preirus | - | SE vs. (B + Doppler) vs. (B + Doppler + SE) |
|
| Rocher et al. [54] | SWE: Aixplorer | Aplio 500 | SWE vs. (B + Doppler) vs. (B + Doppler + SWE) |
|
| Roy et al. [55] | SWE: Aplio 500 | - | SWE |
|
| Schröder et al. [56] | SE: - | Philips iU-22 | SE vs. (B + Doppler) |
|
| Shaaban [57] | SE: Hitachi Hi Vision Avius | - | B + Doppler + SE |
|
| Article | Reference Test | No. of Radiologist (yr. exp) | Blind | |
|---|---|---|---|---|
| Test for (+) | Test for (−) | |||
| Aigner et al. [47] | HPA | Benign: F/U in 6 weeks & 3 months. Inflammation: F/U after 2–3 days & then weekly Infarction: F/U within 24 h. | 1 (>5) | YES |
| Auer et al. [48] | HPA | Sonographic F/U within the 1st 2–3 days, then weekly up to 6 week, & after 3 months | 2 (>10 in SE) | YES |
| Corcioni et al. [49] | HPA, patients declined HPA underwent F/U at least 2 years. | 1 (>10) | - | |
| Goddi et al. [50] | HPA | F/U every 3 or 6 months | 3 (>20 in US) | - |
| Konstantatou et al. [51] | HPA | F/U until resolution or non-progression was documented | 2 (6 & 7 in SE) | YES |
| Pozza et al. [52] | Biomarkers (human chorionic gonadotropin, placental alkaline phosphatase, alpha-fetoprotein, carcinoembryonic antigen, ferritin, lactate dehydrogenase) | 2 (>5) | YES | |
| HPA, patients declined HPA underwent F/U every 3 months for a min of 18 months | Repeated F/U (6 consecutive scans) | |||
| Reginelli et al. [53] | Biomarkers (alpha-fetoprotein, beta-human chorionic gonadotropin) | 1 (15) | - | |
| Nodules > = 2 cm: HPA. Nodules < 2 cm with malignant pattern: Inguinoscrotal exploration | F/U over time | |||
| Rocher et al. [54] | HPA | Clinical tests (17-hydroxyprogesterone, C-reactive protein, leukocytes) | 1 (>20 in US) | - |
| Roy et al. [55] | History, clinical tests, B-mode and Doppler ultrasound, recovery after antibiotic treatment, abscesses confirmed surgically, no modification of ultrasound on F/U > 1 year | 2 (6 & 20) | - | |
| Schröder et al. [56] | HPA | 1 (-) | - | |
| Shaaban [57] | HPA | F/U up to one month | 1 (8 in SE) | - |
| Article | Classification | Modality | Evaluation Metrics and Outcomes | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Acc | Sn/Rc | Sp | PPV/Pc | NPV | AUC | Others | |||
| Aigner et al. [47] | Tumor vs. non-tumor | SE | 94% | 100% | 81% | 92% | 100% | - | - |
| B | 92% | 100% | 75% | 89% | 100% | - | - | ||
| Auer et al. [48] | Malignant vs. benign | SE | 78.2% | 100% | 72.1% | - | - | - | - |
| Doppler | 83.6% | 66.7% | 88.4% | - | - | - | - | ||
| CEUS | 81.8% | 100% | 76.7% | - | - | - | - | ||
| SE + Doppler | 89.1% | 66.7% | 95.3% | - | - | - | - | ||
| SE + CEUS | 94.5% | 100% | 93.0% | - | - | - | - | ||
| Corcioni et al. [49] | Malignant vs. benign | SE | - | 66.7% | - | - | - | - | - |
| LCT vs. non-LCT | - | 36.0% | - | - | - | - | - | ||
| LCT vs. non-LCT | CEUS | - | 96.9% | 94.0% | - | - | 0.954 | DOR: 480.5 | |
| Goddi et al. [50] | Malignant vs. benign | SE: VES | 95.8% | 87.5% | 98.2% | 93.3% | 96.4% | - | - |
| Konstantatou et al. [51] | Malignant vs. benign | Doppler | - | 77.4% | 81.8% | - | - | - | - |
| SE: SR | - | 74.2% | 70.9% | - | - | 0.722 | - | ||
| SE: VES | 58.1% | 80.7% | 45.5% | 45.5% | 80.7% | 0.620 | - | ||
| Neoplastic vs. non-neoplastic | Doppler | - | 68.8% | 97.4% | - | - | - | - | |
| SE: SR | - | 68.8% | 81.6% | - | - | 0.730 | - | ||
| SE: VES | 70.9% | 81.3% | 57.9% | 70.9% | 71.0% | 0.715 | - | ||
| Pozza et al. [52] | Malignant vs. benign | B | - | 89.2% | 85.5% | 76.7% | 93.7% | 0.878 | - |
| SE: SR | - | 59.4% | 66.6% | 48.9% | 75.4% | 0.631 | - | ||
| SE: VES | - | 81.1% | 79.7% | 68.2% | 88.7% | 0.804 | - | ||
| Neoplastic vs. non-neoplastic | B | - | 94.6% | 87.1% | 94.7% | 87.1% | 0.910 | - | |
| SE: SR | - | 69.3% | 61.3% | 81.2% | 45.2% | 0.653 | - | ||
| SE: VES | - | 58.7% | 100% | 100% | 50% | 0.793 | - | ||
| Reginelli et al. [53] | ! Malignant vs. benign | B + Doppler | 81.0% | 86.0% | 64.0% | 84.0% | 48.0% | - | - |
| SE | 87.0% | 85.0% | 78.0% | 93.0% | 71.0% | - | - | ||
| B + Doppler + SE | 90.0% | 100% | 83.0% | 91.0% | 100% | - | - | ||
| Rocher et al. [54] | (Malignant + Burnout tumor) vs. benign LCT | B + Doppler: size | 77.9% | 67.3% | 96.4% | 97.1% | 62.8% | 0.88 | - |
| SWE: SD | 79.8% | 93.9% | 62.5% | 75.4% | 89.3% | 0.77 | - | ||
| B + Doppler + SWE: # | 86.5% | 95.9% | 75.0% | 82.5% | 93.8% | 0.93 | - | ||
| * (Malignant + Burnout tumor) vs. (Benign LCT + other benign tumors) | B + Doppler: Calcification score | 74.2% | 55.1% | 97.5% | 96.4% | 63.9% | 0.85 | - | |
| SWE: SD | 79.8% | 93.9% | 62.5% | 75.4% | 89.3% | 0.77 | - | ||
| B + Doppler + SWE: # | 86.5% | 95.9% | 75.0% | 82.5% | 93.8% | 0.91 | - | ||
| Roy et al. [55] | ! Tumor vs. non-tumor | SWE: ROI filling | - | 82% | 81% | 85% | 98% | 0.881 | - |
| Schröder et al. [56] | Neoplastic vs. non-neoplastic | B | 88.2% | 100% | 42.9% | 87.1% | 100% | - | - |
| Doppler | 82.1% | 81.1% | 85.7% | 95.6% | 54.5% | - | - | ||
| SE: VES | 84.6% | 98.1% | 25.0% | 85.2% | 75.0% | - | - | ||
| SE: ΔVES | 89.1% | 97.8% | 50.0% | 89.8% | 83.3% | - | - | ||
| SE: SR | 81.1% | 90.5% | 45.5% | 86.4% | 55.6% | - | - | ||
| B + SE: Q-size | 61.1% | 56.7% | 83.3% | 94.4% | 27.8% | - | - | ||
| CEUS | 91.0% | 92.6% | 84.6% | 96.2% | 73.3% | - | - | ||
| Shaaban [57] | ! Neoplastic vs. non-neoplastic | B + Doppler + SE | - | 100% | 40% | 37.5% | 100% | - | - |
| Comparison | Subgroup Analysis | Pooled Sensitivity (95% CI) | Pooled Specificity (95% CI) | Pooled DOR (95% CI) |
|---|---|---|---|---|
| Non-neoplasm vs. Neoplasm | Summary | 92.1% (62.8% to 98.7%) | 79.2% (26.2% to 97.6%) | 44.21 (5.48 to 356.79) |
| SE color code | - | - | - | |
| SE scoring system | 84.4% (58.5% to 95.4%) | 72.1% (13.9% to 97.6%) | 14.01 (2.10 to 93.46) | |
| SWE | - | - | - | |
| Benignity vs. Malignancy | Summary | 86.0% (79.7% to 90.6%) | 82.4% (60.4% to 93.5%) | 28.71 (9.60 to 85.88) |
| SE color code | 86.% (65.9% to 95.3%) | 82.2% (57.0% to 94.1%) | 26.77 (7.14 to 115.84) | |
| SE scoring system | 83.2% (73.5% to 89.8%) | 84.6% (43.3% to 97.5%) | 27.22 (2.81 to 263.27) | |
| SWE | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, D.K.-H.; Cheng, E.S.-W.; Mao, Y.-J.; Zheng, Y.; Yao, K.-Y.; Ni, M.; Zhang, Y.-Q.; Wong, D.W.-C.; Cheung, J.C.-W. Sonoelastography for Testicular Tumor Identification: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. Cancers 2023, 15, 3770. https://doi.org/10.3390/cancers15153770
Lai DK-H, Cheng ES-W, Mao Y-J, Zheng Y, Yao K-Y, Ni M, Zhang Y-Q, Wong DW-C, Cheung JC-W. Sonoelastography for Testicular Tumor Identification: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. Cancers. 2023; 15(15):3770. https://doi.org/10.3390/cancers15153770
Chicago/Turabian StyleLai, Derek Ka-Hei, Ethan Shiu-Wang Cheng, Ye-Jiao Mao, Yi Zheng, Ke-Yu Yao, Ming Ni, Ying-Qi Zhang, Duo Wai-Chi Wong, and James Chung-Wai Cheung. 2023. "Sonoelastography for Testicular Tumor Identification: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy" Cancers 15, no. 15: 3770. https://doi.org/10.3390/cancers15153770