
Pulsed Electric Fields in Oncology: A Snapshot of Current Clinical Practices and Research Directions from the 4th World Congress of Electroporation

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Irreversible Electroporation
2.1. Principles of IRE
2.2. Prostate Cancer
2.3. Pancreatic Cancer
2.4. Liver Malignancies
2.4.1. Primary Liver Cancers
2.4.2. Liver Metastases
2.5. Localised Renal Cell Carcinoma
2.6. Research Directions—IRE
2.6.1. Gastrointestinal Tract
2.6.2. Immune Effect and Combined Strategies
2.6.3. High-Frequency Irreversible Electroporation
3. Gene Electrotherapy
3.1. Principles of GET
3.2. Melanoma
3.3. Merkel Cell Carcinoma
3.4. Breast Cancer
3.5. Urology
3.5.1. Prostate Cancer
3.5.2. Bladder and Renal Cancer
3.6. Research Directions—GET
3.6.1. Combination with PD-1 Blockade in Melanoma
3.6.2. Predictive Biomarkers
3.6.3. Cytokine/Chemokine Combinations
4. Electrochemotherapy
4.1. Principles of ECT
4.2. Skin Cancers
4.2.1. Melanoma
4.2.2. BCC
4.2.3. Cutaneous Squamous Cell Carcinoma
4.3. Skin metastases from Breast Cancer
4.4. Bone and Soft Tissue Tumours
4.4.1. Bone Metastases
4.4.2. Kaposi Sarcoma
4.4.3. Superficial Angiosarcoma
4.4.4. Deep-Seated Soft Tissue Sarcomas
4.4.5. Vascular Malformations
4.5. Intra-Abdominal Tumours
4.5.1. Pancreas
4.5.2. Liver
4.6. Gastrointestinal Cancers
4.6.1. Oesophageal Cancer
4.6.2. Colorectal Cancer
4.7. Research Directions—ECT
4.7.1. Aesthetic Outcome
4.7.2. Quality of Life
4.7.3. Exploiting Biological Factors
4.7.4. Combination with Immunotherapy
Melanoma
Hepatocellular Carcinoma
Head and Neck Squamous Cell Carcinoma
4.7.5. Evaluation of Local Response
4.7.6. Tumour Sensitivity to Histologic Subtype
4.7.7. Oldest-Old Patients
4.7.8. Neoadjuvant ECT
4.7.9. Adjuvant ECT
4.7.10. Bleomycin De-Escalation
4.7.11. Intra-Abdominal Malignancies
4.7.12. Endoscopic Application
Oral Cavity and Oropharynx
Gastrointestinal Tract
4.7.13. Research Methods
5. Calcium Electroporation
5.1. Principles of Ca-EP
5.2. Clinical Studies
5.3. Research Directions—Calcium EP
6. Tumour-Treating Fields
6.1. Principles of TTFs
6.2. Glioblastoma
6.3. Mesothelioma
6.4. Lung Cancer
6.5. Pancreatic Cancer
6.6. Ovarian Cancer
6.7. Research Directions—TTF
6.7.1. Preclinical Research
6.7.2. Clinical Research
7. Discussion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| APC | antigen-presenting cells | IRE | irreversible electroporation |
| BCC | basal cell carcinoma | LAPC | locally advanced pancreatic cancer |
| BCG | bacillus of Calmette-Guerin | MA-IRE | margin accentuation IRE |
| BEST | bleomycin electrosclerotherapy | MID | minimal important difference |
| BRPC | borderline resectable pancreatic cancer | mpMRI | multiparametric MRI |
| Ca-EP | calcium electroporation | MRI | magnetic resonance imaging |
| CEUS | contrast-enhanced ultrasound | MWA | microwave ablation |
| CR | complete response | NK | natural killer |
| CRLM | colorectal liver metastases | NSCLC | non-small cell lung cancer |
| CRR | complete response rate | ORR | overall response rate |
| cSCC | cutaneous squamous cell carcinoma | OS | overall survival |
| csPCa | clinically significant prostate cancer | PDAC | pancreatic ductal adenocarcinoma |
| CT | computed tomography | PEF | pulsed electric field |
| DAMPS | damage-associated molecular patterns | PET-CT | positron emission tomography-CT |
| DFS | disease-free survival | PFS | progression-free survival |
| ECT | electrochemotherapy | PMCA | plasma membrane calcium ATPase |
| EP | electroporation | PSA | prostatic specific antigen |
| ESOPE | European standard operating procedures of ECT | PSMA | prostate-specific membrane antigen |
| FG-ECT | fixed geometry ECT | QoL | quality of life |
| FIRE | focal IRE | RECIST | response evaluation criteria in solid tumours |
| GBM | glioblastoma | RESPECT | registry on percutaneous ECT |
| GET | gene electrotransfer | RFA | radiofrequency ablation |
| HCC | hepatocellular carcinoma | STING | stimulator of interferon gamma |
| H-FIRE | high-frequency IRE | TRAIL | tumour necrosis factor-related apoptosis-inducing ligand |
| HNSCC | head and neck squamous cell carcinoma | TTF | tumour-treating field |
| ICC | intrahepatic cholangiocarcinoma | US | ultrasound |
| ICD | immunogenic cell death | VG-ECT | variable geometry ECT |
| ILI | isolated limb infusion | V-SCC | vulvar squamous cell carcinoma |
| ILP | isolated limb perfusion | WCE | world congress of electroporation |
| InspECT | International network for sharing practices of ECT |
References
- Tsoucalas, G.; Karamanou, M.; Lymperi, M.; Gennimata, V.; Androutsos, G. The “Torpedo” Effect in Medicine. Int. Marit. Health 2014, 65, 65–67. [Google Scholar] [CrossRef] [Green Version]
- Okino, M.; Mohri, H. Effects of a high-voltage electrical impulse and an anticancer drug on in vivo growing tumors. Jpn. J. Cancer Res. 1987, 78, 1319–1321. [Google Scholar]
- Geboers, B.; Scheffer, H.J.; Graybill, P.M.; Ruarus, A.H.; Nieuwenhuizen, S.; Puijk, R.S.; van den Tol, P.M.; Davalos, R.V.; Rubinsky, B.; de Gruijl, T.D.; et al. High-Voltage Electrical Pulses in Oncology: Irreversible Electroporation, Electrochemotherapy, Gene Electrotransfer, Electrofusion, and Electroimmunotherapy. Radiology 2020, 295, 254–272. [Google Scholar] [CrossRef]
- Neumann, E.; Schaefer-Ridder, M.; Wang, Y.; Hofschneider, P.H. Gene Transfer into Mouse Lyoma Cells by Electroporation in High Electric Fields. EMBO J. 1982, 1, 841–845. [Google Scholar] [CrossRef]
- Mir, L.M.; Orlowski, S.; Belehradek, J.; Paoletti, C. Electrochemotherapy Potentiation of Antitumour Effect of Bleomycin by Local Electric Pulses. Eur. J. Cancer 1991, 27, 68–72. [Google Scholar] [CrossRef]
- Frandsen, S.K.; Gissel, H.; Hojman, P.; Tramm, T.; Eriksen, J.; Gehl, J. Direct Therapeutic Applications of Calcium Electroporation to Effectively Induce Tumor Necrosis. Cancer Res. 2012, 72, 1336–1341. [Google Scholar] [CrossRef] [Green Version]
- Frandsen, S.K.; Gehl, J. A Review on Differences in Effects on Normal and Malignant Cells and Tissues to Electroporation-Based Therapies: A Focus on Calcium Electroporation. Technol. Cancer Res. Treat. 2018, 17, 1533033818788077. [Google Scholar] [CrossRef]
- Hamilton, W.A.; Sale, A.J.H. Effects of high electric fields on microorganisms: II. Mechanism of action of the lethal effect. Biochim. Biophys. Acta 1967, 148, 789–800. [Google Scholar] [CrossRef]
- Davalos, R.V.; Mir, L.M.; Rubinsky, B. Tissue Ablation with Irreversible Electroporation. Ann. Biomed. Eng. 2005, 33, 223–231. [Google Scholar] [CrossRef]
- Moser, J.C.; Salvador, E.; Deniz, K.; Swanson, K.; Tuszynski, J.; Carlson, K.W.; Karanam, N.K.; Patel, C.B.; Story, M.; Lou, E.; et al. The Mechanisms of Action of Tumor Treating Fields. Cancer Res. 2022, 82, 3650–3658. [Google Scholar] [CrossRef]
- Rominiyi, O.; Vanderlinden, A.; Clenton, S.J.; Bridgewater, C.; Al-Tamimi, Y.; Collis, S.J. Tumour Treating Fields Therapy for Glioblastoma: Current Advances and Future Directions. Br. J. Cancer 2021, 124, 697–709. [Google Scholar] [CrossRef]
- Kundalia, K.; Hakeem, A.; Papoulas, M.; Mcphail, M.; Reddy, S.; Peddu, P.; Kibriya, N.; Atkinson, S.; Prachalias, A.; Srinivasan, P.; et al. Margin ACcentuation for Resectable Pancreatic Cancer Using Irreversible Electroporation—Results from the MACPIE-I Study. Eur. J. Surg. Oncol. 2021, 47, 2571–2578. [Google Scholar] [CrossRef]
- Algazi, A.; Bhatia, S.; Agarwala, S.; Molina, M.; Lewis, K.; Faries, M.; Fong, L.; Levine, L.P.; Franco, M.; Oglesby, A.; et al. Intratumoral Delivery of Tavokinogene Telseplasmid Yields Systemic Immune Responses in Metastatic Melanoma Patients. Ann. Oncol. 2020, 31, 532–540. [Google Scholar] [CrossRef] [Green Version]
- Campana, L.G.; Miklavčič, D.; Bertino, G.; Marconato, R.; Valpione, S.; Imarisio, I.; Dieci, M.V.; Granziera, E.; Cemazar, M.; Alaibac, M.; et al. Electrochemotherapy of Superficial Tumors—Current Status: Basic Principles, Operating Procedures, Shared Indications, and Emerging Applications. Semin. Oncol. 2019, 46, 173–191. [Google Scholar] [CrossRef] [Green Version]
- Ágoston, D.; Baltás, E.; Ócsai, H.; Rátkai, S.; Lázár, P.G.; Korom, I.; Varga, E.; Németh, I.B.; Viharosné, É.D.R.; Gehl, J.; et al. Evaluation of Calcium Electroporation for the Treatment of Cutaneous Metastases: A Double Blinded Randomised Controlled Phase II Trial. Cancers 2020, 12, 179. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.M.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields plus Maintenance Temozolomide vs. Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma a Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [Green Version]
- Davalos, R.V.; Otten, D.M.; Mir, L.M.; Rubinsky, B. Electrical Impedance Tomography for Imaging Tissue Electroporation. IEEE Trans. Biomed. Eng. 2004, 51, 761–767. [Google Scholar] [CrossRef]
- Giladi, M.; Schneiderman, R.S.; Voloshin, T.; Porat, Y.; Munster, M.; Blat, R.; Sherbo, S.; Bomzon, Z.; Urman, N.; Itzhaki, A.; et al. Mitotic Spindle Disruption by Alternating Electric Fields Leads to Improper Chromosome Segregation and Mitotic Catastrophe in Cancer Cells. Sci. Rep. 2015, 5, 18046. [Google Scholar] [CrossRef] [Green Version]
- Gera, N.; Yang, A.; Holtzman, T.S.; Lee, S.X.; Wong, E.T.; Swanson, K.D. Tumor Treating Fields Perturb the Localization of Septins and Cause Aberrant Mitotic Exit. PLoS ONE 2015, 10, e0125269. [Google Scholar] [CrossRef] [Green Version]
- Kirson, E.D.; Gurvich, Z.; Schneiderman, R.; Dekel, E.; Itzhaki, A.; Wasserman, Y.; Schatzberger, R.; Palti, Y. Disruption of Cancer Cell Replication by Alternating Electric Fields. Cancer Res. 2004, 64, 3288–3295. [Google Scholar] [CrossRef] [Green Version]
- Frandsen, S.K.; McNeil, A.K.; Novak, I.; McNeil, P.L.; Gehl, J. Difference in Membrane Repair Capacity between Cancer Cell Lines and a Normal Cell Line. J. Membr. Biol. 2016, 249, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Markelc, B.; Sersa, G.; Cemazar, M. Differential Mechanisms Associated with Vascular Disrupting Action of Electrochemotherapy: Intravital Microscopy on the Level of Single Normal and Tumor Blood Vessels. PLoS ONE 2013, 8, e59557. [Google Scholar] [CrossRef] [Green Version]
- Frandsen, S.K.; Krüger, M.B.; Mangalanathan, U.M.; Tramm, T.; Mahmood, F.; Novak, I.; Gehl, J. Normal and Malignant Cells Exhibit Differential Responses to Calcium Electroporation. Cancer Res. 2017, 77, 4389–4401. [Google Scholar] [CrossRef] [Green Version]
- Daud, A.I.; DeConti, R.C.; Andrews, S.; Urbas, P.; Riker, A.I.; Sondak, V.K.; Munster, P.N.; Sullivan, D.M.; Ugen, K.E.; Messina, J.L.; et al. Phase I Trial of Interleukin-12 Plasmid Electroporation in Patients with Metastatic Melanoma. J. Clin. Oncol. 2008, 26, 5896–5903. [Google Scholar] [CrossRef] [Green Version]
- Abidor, I.G.; Arakelyan, V.B.; Chernomordik, L.V.; Chizmadzhev, Y.A.; Pastushenko, V.F.; Tarasevich, M.R. Electric breakdown of bilayer lipid membranes: I. The main experimental facts and their qualitative discussion. J. Electroanal. Chem. 1979, 104, 37–52. [Google Scholar] [CrossRef]
- Tsong, T.Y. Electroporation of Cell Membranes. Biophys. J. 1991, 60, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Teissié, J.; Rols, M.P. An Experimental Evaluation of the Critical Potential Difference Inducing Cell Membrane Electropermeabilization. Biophys. J. 1993, 65, 409–413. [Google Scholar] [CrossRef] [Green Version]
- Edd, J.F.; Horowitz, L.; Davalos, R.V.; Mir, L.M.; Rubinsky, B. In Vivo Results of a New Focal Tissue Ablation Technique: Irreversible Electroporation. IEEE Trans. Biomed. Eng. 2006, 53, 1409–1415. [Google Scholar] [CrossRef]
- Li, W.; Fan, Q.; Ji, Z.; Qiu, X.; Li, Z. The Effects of Irreversible Electroporation (IRE) on Nerves. PLoS ONE 2011, 6, e18831. [Google Scholar] [CrossRef]
- Maor, E.; Ivorra, A.; Leor, J.; Rubinsky, B. The Effect of Irreversible Electroporation on Blood Vessels. Technol. Cancer Res. Treat. 2007, 6, 307–312. [Google Scholar] [CrossRef]
- Onik, G.; Mikus, P.; Rubinsky, B. Irreversible Electroporation: Implications for Prostate Ablation. Technol. Cancer Res. Treat. 2007, 6, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Bower, M.; Sherwood, L.; Li, Y.; Martin, R. Irreversible Electroporation of the Pancreas: Definitive Local Therapy without Systemic Effects. J. Surg. Oncol. 2011, 104, 22–28. [Google Scholar] [CrossRef]
- Rubinsky, B.; Onik, G.; Mikus, P. Irreversible Electroporation: A New Ablation Modality-Clinical Implications. Technol. Cancer Res. Treat. 2007, 6, 37–48. [Google Scholar] [CrossRef]
- Lee, E.W.; Loh, C.T.; Kee, S.T. Imaging Guided Percutaneous Irreversible Electroporation: Ultrasound and Immunohistological Correlation. Technol. Cancer Res. Treat. 2007, 6, 287–294. [Google Scholar] [CrossRef]
- Dupuy, D.E.; Aswad, B.; Ng, T. Irreversible Electroporation in a Swine Lung Model. Cardiovasc. Intervent. Radiol. 2011, 34, 391–395. [Google Scholar] [CrossRef]
- Tracy, C.R.; Kabbani, W.; Cadeddu, J.A. Irreversible Electroporation (IRE): A Novel Method for Renal Tissue Ablation. BJU Int. 2011, 107, 1982–1987. [Google Scholar] [CrossRef]
- Deodhar, A.; Monette, S.; Single, G.W.; Hamilton, W.C.; Thornton, R.; Maybody, M.; Coleman, J.A.; Solomon, S.B. Renal Tissue Ablation with Irreversible Electroporation: Preliminary Results in a Porcine Model. Urology 2011, 77, 754–760. [Google Scholar] [CrossRef]
- Neal, R.E.; Singh, R.; Hatcher, H.C.; Kock, N.D.; Torti, S.V.; Davalos, R.V. Treatment of Breast Cancer through the Application of Irreversible Electroporation Using a Novel Minimally Invasive Single Needle Electrode. Breast Cancer Res. Treat. 2010, 123, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Al-Sakere, B.; André, F.; Bernat, C.; Connault, E.; Opolon, P.; Davalos, R.V.; Rubinsky, B.; Mir, L.M. Tumor Ablation with Irreversible Electroporation. PLoS ONE 2007, 2, e1135. [Google Scholar] [CrossRef] [Green Version]
- Zager, Y.; Kain, D.; Landa, N.; Leor, J.; Maor, E. Optimization of Irreversible Electroporation Protocols for In-Vivo Myocardial Decellularization. PLoS ONE 2016, 11, e0165475. [Google Scholar] [CrossRef] [Green Version]
- Garcia, P.A.; Rossmeisl, J.H.; Neal, R.E.; Ellis, T.L.; Olson, J.D.; Henao-Guerrero, N.; Robertson, J.; Davalos, R.V. Intracranial Nonthermal Irreversible Electroporation: In Vivo Analysis. J. Membr. Biol. 2010, 236, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Aycock, K.N.; Davalos, R.V. Irreversible Electroporation: Background, Theory, and Review of Recent Developments in Clinical Oncology. Bioelectricity 2019, 1, 214–234. [Google Scholar] [CrossRef] [Green Version]
- Batista Napotnik, T.; Polajžer, T.; Miklavčič, D. Cell Death Due to Electroporation—A Review. Bioelectrochemistry 2021, 141, 107871. [Google Scholar] [CrossRef]
- ClinicalTrials.Gov. Available online: https://Clinicaltrials.Gov/Ct2/Results?Cond=Cancer&intr=Irreversible+Electroporation&Search=Apply&recrs=a&recrs=f&recrs=d&recrs=e&age_v=&gndr=&type=&rslt= (accessed on 16 January 2023).
- Resnick, M.J.; Koyama, T.; Fan, K.-H.; Albertsen, P.C.; Goodman, M.; Hamilton, A.S.; Hoffman, R.M.; Potosky, A.L.; Stanford, J.L.; Stroup, A.M.; et al. Long-Term Functional Outcomes after Treatment for Localized Prostate Cancer. N. Engl. J. Med. 2013, 368, 436–445. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Teoh, J.; Laguna, P.; Dominguez-Escrig, J.; Barret, E.; Ramon-Borja, J.C.; Muir, G.; Bohr, J.; Pelechano Gómez, P.; Ng, C.-F.; et al. Effect of Focal vs. Extended Irreversible Electroporation for the Ablation of Localized Low- or Intermediate-Risk Prostate Cancer on Early Oncological Control. JAMA Surg. 2023, 158, 343–349. [Google Scholar] [CrossRef]
- Scheltema, M.J.; Geboers, B.; Blazevski, A.; Doan, P.; Katelaris, A.; Agrawal, S.; Barreto, D.; Shnier, R.; Delprado, W.; Thompson, J.E.; et al. Median 5-Year Outcomes of Primary Focal Irreversible Electroporation for Localised Prostate Cancer. BJU Int. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Gielchinsky, I.; Lev-Cohain, N. Focal Irreversible Electroporation for Localized Prostate Cancer—Oncological and Safety Outcomes Using MpMRI and Transperineal Biopsy Follow-Up. Res. Rep. Urol. 2023, 15, 27–35. [Google Scholar] [CrossRef]
- Blazevski, A.; Scheltema, M.J.; Yuen, B.; Masand, N.; Nguyen, T.V.; Delprado, W.; Shnier, R.; Haynes, A.M.; Cusick, T.; Thompson, J.; et al. Oncological and Quality-of-Life Outcomes following Focal Irreversible Electroporation as Primary Treatment for Localised Prostate Cancer: A Biopsy-Monitored Prospective Cohort. Eur. Urol. Oncol. 2020, 3, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Blazevski, A.; Amin, A.; Scheltema, M.J.; Balakrishnan, A.; Haynes, A.M.; Barreto, D.; Cusick, T.; Thompson, J.; Stricker, P.D. Focal Ablation of Apical Prostate Cancer Lesions with Irreversible Electroporation (IRE). World J. Urol. 2021, 39, 1107–1114. [Google Scholar] [CrossRef]
- Yaxley, W.J.; Gianduzzo, T.; Kua, B.; Oxford, R.; Yaxley, J.W. Focal Therapy for Prostate Cancer with Irreversible Electroporation: Oncological and Functional Results of a Single Institution Study. Investig. Clin. Urol. 2022, 63, 285–293. [Google Scholar] [CrossRef]
- Cribbs, K.A.; Manning, E.F.; Zhou, J.; Lahue, B.J.; Polascik, T.J. Real-World Comparative Safety and Effectiveness of Irreversible Electroporation and High-Intensity Focused Ultrasound for Prostate Cancer Ablation. Urology 2023, 174, 7–17. [Google Scholar] [CrossRef]
- Guenther, E.; Klein, N.; Zapf, S.; Weil, S.; Schlosser, C.; Rubinsky, B.; Stehling, M.K. Prostate Cancer Treatment with Irreversible Electroporation (IRE): Safety, Efficacy and Clinical Experience in 471 Treatments. PLoS ONE 2019, 14, e0215093. [Google Scholar] [CrossRef] [Green Version]
- Geboers, B.; Scheltema, M.J.; Blazevski, A.; Katelaris, A.; Doan, P.; Ali, I.; Agrawal, S.; Barreto, D.; Matthews, J.; Haynes, A.M.; et al. Median 4-Year Outcomes of Salvage Irreversible Electroporation for Localized Radio-Recurrent Prostate Cancer. BJU Int. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Blazevski, A.; Geboers, B.; Scheltema, M.J.; Gondoputro, W.; Doan, P.; Katelaris, A.; Agrawal, S.; Baretto, D.; Matthews, J.; Haynes, A.M.; et al. Salvage Irreversible Electroporation for Radio-Recurrent Prostate Cancer—The Prospective FIRE Trial. BJU Int. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Giganti, F.; Stabile, A.; Giona, S.; Marenco, J.; Orczyk, C.; Moore, C.M.; Allen, C.; Kirkham, A.; Emberton, M.; Punwani, S. Prostate Cancer Treated with Irreversible Electroporation: MRI-Based Volumetric Analysis and Oncological Outcome. Magn. Reson. Imaging 2019, 58, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Jung, E.M.; Engel, M.; Wiggermann, P.; Schicho, A.; Lerchbaumer, M.; Stroszczynski, C.; Fischer, T.; Wiesinger, I. Contrast Enhanced Ultrasound (CEUS) with Parametric Imaging after Irreversible Electroporation (IRE) of the Prostate to Assess the Success of Prostate Cancer Treatment. Clin. Hemorheol. Microcirc. 2021, 77, 303–310. [Google Scholar] [CrossRef]
- Shin, D.; Yoon, C.E.; Kwon, H.J.; Moon, H.W.; Park, Y.H.; Cho, H.J.; Ha, U.; Hong, S.H.; Park, S.Y.; Ha, S.; et al. Irreversible Electroporation for Prostate Cancer Using PSMA PET-CT. Prostate Int. 2022, 11, 40–45. [Google Scholar] [CrossRef]
- Collettini, F.; Enders, J.; Stephan, C.; Fischer, T.; Baur, A.D.J.; Penzkofer, T.; Busch, J.; Hamm, B.; Gebauer, B. Image-Guided Irreversible Electroporation of Localized Prostate Cancer: Functional and Oncologic Outcomes. Radiology 2019, 292, 250–257. [Google Scholar] [CrossRef]
- Frey, G.T.; Padula, C.A.; Toskich, B.B.; Stauffer, J.A. Intraoperative Irreversible Electroporation in Locally Advanced Pancreatic Cancer: A Guide for the Interventional Radiologist. Semin. Intervent. Radiol. 2019, 36, 386–391. [Google Scholar] [CrossRef]
- Martin, R.C.G.; Kwon, D.; Chalikonda, S.; Sellers, M.; Kotz, E.; Scoggins, C.; McMasters, K.M.; Watkins, K. Treatment of 200 Locally Advanced (Stage III) Pancreatic Adenocarcinoma Patients with Irreversible Electroporation Safety and Efficacy. Ann. Surg. 2015, 262, 486–492. [Google Scholar] [CrossRef]
- Kwon, D.; McFarland, K.; Velanovich, V.; Martin, R.C.G. Borderline and Locally Advanced Pancreatic Adenocarcinoma Margin Accentuation with Intraoperative Irreversible Electroporation. Surgery 2014, 156, 910–920. [Google Scholar] [CrossRef]
- Belfiore, M.P.; Ronza, F.M.; Romano, F.; Ianniello, G.P.; De Lucia, G.; Gallo, C.; Marsicano, C.; Di Gennaro, T.L.; Belfiore, G. Percutaneous CT-Guided Irreversible Electroporation Followed by Chemotherapy as a Novel Neoadjuvant Protocol in Locally Advanced Pancreatic Cancer: Our Preliminary Experience. Int. J. Surg. 2015, 21, S34–S39. [Google Scholar] [CrossRef]
- Dunki-Jacobs, E.M.; Philips, P.; Martin, R.C.G. Evaluation of Resistance as a Measure of Successful Tumor Ablation during Irreversible Electroporation of the Pancreas. J. Am. Coll. Surg. 2014, 218, 179–187. [Google Scholar] [CrossRef]
- He, C.; Wang, J.; Sun, S.; Zhang, Y.; Lin, X.; Lao, X.; Cui, B.; Li, S. Irreversible Electroporation versus Radiotherapy after Induction Chemotherapy on Survival in Patients with Locally Advanced Pancreatic Cancer: A Propensity Score Analysis. BMC Cancer 2019, 19, 394. [Google Scholar] [CrossRef]
- Flak, R.V.; Stender, M.T.; Jensen, T.M.; Andersen, K.L.; Henriksen, S.D.; Mortensen, P.B.; Sall, M.; Thorlacius-Ussing, O. Treatment of Locally Advanced Pancreatic Cancer with Irreversible Electroporation—A Danish Single Center Study of Safety and Feasibility. Scand. J. Gastroenterol. 2019, 54, 252–258. [Google Scholar] [CrossRef]
- Yan, L.; Chen, Y.L.; Su, M.; Liu, T.; Xu, K.; Liang, F.; Gu, W.Q.; Lu, S.C. A Single-Institution Experience with Open Irreversible Electroporation for Locally Advanced Pancreatic Carcinoma. Chin. Med. J. 2016, 129, 2920–2925. [Google Scholar] [CrossRef]
- Yang, P.C.; Huang, K.W.; Pua, U.; Kim, M.D.; Li, S.P.; Li, X.Y.; Liang, P.C. Prognostic Factor Analysis of Irreversible Electroporation for Locally Advanced Pancreatic Cancer—A Multi-Institutional Clinical Study in Asia. Eur. J. Surg. Oncol. 2020, 46, 811–817. [Google Scholar] [CrossRef]
- He, C.; Huang, X.; Zhang, Y.; Cai, Z.; Lin, X.; Li, S. Comparison of Survival between Irreversible Electroporation Followed by Chemotherapy and Chemotherapy Alone for Locally Advanced Pancreatic Cancer. Front. Oncol. 2020, 10, 6. [Google Scholar] [CrossRef]
- Ruarus, A.H.; Vroomen, L.G.P.H.; Geboers, B.; van Veldhuisen, E.; Puijk, R.S.; Nieuwenhuizen, S.; Besselink, M.G.; Zonderhuis, B.M.; Kazemier, G.; de Gruijl, T.D.; et al. Percutaneous Irreversible Electroporation in Locally Advanced and Recurrent Pancreatic Cancer (PANFIRE-2): A Multicenter, Prospective, Single-Arm, Phase II Study. Radiology 2020, 294, 212–220. [Google Scholar] [CrossRef]
- Davis, J.M.K.; Salibi, P.N.; Motz, B.M.; Vrochides, D.; McKillop, I.H.; Iannitti, D.A. Irreversible Electroporation-Assisted Resection for Locally Advanced Pancreas Cancer. Surg. Innov. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Ansari, D.; Kristoffersson, S.; Andersson, R.; Bergenfeldt, M. The Role of Irreversible Electroporation (IRE) for Locally Advanced Pancreatic Cancer: A Systematic Review of Safety and Efficacy. Scand. J. Gastroenterol. 2017, 52, 1165–1171. [Google Scholar] [CrossRef]
- Martin, R.C.G.; Schoen, E.C.; Philips, P.; Egger, M.E.; McMasters, K.M.; Scoggins, C.R. Impact of Margin Accentuation with Intraoperative Irreversible Electroporation on Local Recurrence in Resected Pancreatic Cancer. Surgery 2023, 173, 581–589. [Google Scholar] [CrossRef]
- Simmerman, E.; Chung, J.; Lawson, A.; Kruse, E. Application of Irreversible Electroporation Ablation as Adjunctive Treatment for Margin Enhancement: Safety and Efficacy. J. Surg. Res. 2020, 246, 260–268. [Google Scholar] [CrossRef]
- Woeste, M.R.; Wilson, K.D.; Kruse, E.J.; Weiss, M.J.; Christein, J.D.; White, R.R.; Martin, R.C.G. Optimizing Patient Selection for Irreversible Electroporation of Locally Advanced Pancreatic Cancer: Analyses of Survival. Front. Oncol. 2022, 11, 5701. [Google Scholar] [CrossRef]
- Orcutt, S.T.; Anaya, D.A. Liver Resection and Surgical Strategies for Management of Primary Liver Cancer. Cancer Control. 2018, 25, 1073274817744621. [Google Scholar] [CrossRef] [Green Version]
- Cohen, E.I.; Field, D.; Lynskey, G.E.; Kim, A.Y. Technology of Irreversible Electroporation and Review of Its Clinical Data on Liver Cancers. Expert. Rev. Med. Devices 2018, 15, 99–106. [Google Scholar] [CrossRef]
- Gupta, P.; Maralakunte, M.; Sagar, S.; Kumar, M.P.; Bhujade, H.; Chaluvashetty, S.B.; Kalra, N. Efficacy and Safety of Irreversible Electroporation for Malignant Liver Tumors: A Systematic Review and Meta-Analysis. Eur. Radiol. 2021, 31, 6511–6521. [Google Scholar] [CrossRef]
- Freeman, E.; Cheung, W.; Kavnoudias, H.; Majeed, A.; Kemp, W.; Roberts, S.K. Irreversible Electroporation for Hepatocellular Carcinoma: Longer-Term Outcomes at a Single Centre. Cardiovasc. Intervent. Radiol. 2021, 44, 247–253. [Google Scholar] [CrossRef]
- Scheffer, H.J.; Nielsen, K.; De Jong, M.C.; Van Tilborg, A.A.J.M.; Vieveen, J.M.; Bouwman, A.; Meijer, S.; Van Kuijk, C.; Van Den Tol, P.; Meijerink, M.R. Irreversible Electroporation for Nonthermal Tumor Ablation in the Clinical Setting: A Systematic Review of Safety and Efficacy. J. Vasc. Interv. Radiol. 2014, 25, 997–1011. [Google Scholar] [CrossRef]
- Meijerink, M.R.; Ruarus, A.H.; Vroomen, L.G.P.H.; Puijk, R.S.; Geboers, B.; Nieuwenhuizen, S.; Van Den Bemd, B.A.T.; Nielsen, K.; De Vries, J.J.J.; Van Lienden, K.P.; et al. Irreversible Electroporation to Treat Unresectable Colorectal Liver Metastases (COLDFIRE-2): A Phase II, Two-Center, Single-Arm Clinical Trial. Radiology 2021, 299, 470–480. [Google Scholar] [CrossRef]
- Nieuwenhuizen, S.; Puijk, R.S.; van den Bemd, B.; Aldrighetti, L.; Arntz, M.; van den Boezem, P.B.; Bruynzeel, A.M.E.; Burgmans, M.C.; de Cobelli, F.; Coolsen, M.M.E.; et al. Resectability and Ablatability Criteria for the Treatment of Liver only Colorectal Metastases: Multidisciplinary Consensus Document from the COLLISION Trial Group. Cancers 2020, 12, 1779. [Google Scholar] [CrossRef]
- Koethe, Y.; Wilson, N.; Narayanan, G. Irreversible Electroporation for Colorectal Cancer Liver Metastasis: A Review. Int. J. Hyperth. 2022, 39, 682–687. [Google Scholar] [CrossRef]
- Cannon, R.; Ellis, S.; Hayes, D.; Narayanan, G.; Martin, R.C.G. Safety and Early Efficacy of Irreversible Electroporation for Hepatic Tumors in Proximity to Vital Structures. J. Surg. Oncol. 2013, 107, 544–549. [Google Scholar] [CrossRef]
- Hosein, P.J.; Echenique, A.; Loaiza-Bonilla, A.; Froud, T.; Barbery, K.; Rocha Lima, C.M.; Yrizarry, J.M.; Narayanan, G. Percutaneous Irreversible Electroporation for the Treatment of Colorectal Cancer Liver Metastases with a Proposal for a New Response Evaluation System. J. Vasc. Interv. Radiol. 2014, 25, 1233–1239.e2. [Google Scholar] [CrossRef]
- Lencioni, R.; Crocetti, L.; Narayanan, G. Irreversible Electroporation in the Treatment of Hepatocellular Carcinoma. Tech. Vasc. Interv. Radiol. 2015, 18, 135–139. [Google Scholar] [CrossRef]
- Dollinger, M.; Zeman, F.; Niessen, C.; Lang, S.A.; Beyer, L.P.; Müller, M.; Stroszczynski, C.; Wiggermann, P. Bile Duct Injury after Irreversible Electroporation of Hepatic Malignancies: Evaluation of MR Imaging Findings and Laboratory Values. J. Vasc. Interv. Radiol. 2016, 27, 96–103. [Google Scholar] [CrossRef]
- Verloh, N.; Jensch, I.; Lürken, L.; Haimerl, M.; Dollinger, M.; Renner, P.; Wiggermann, P.; Werner, J.M.; Zeman, F.; Stroszczynski, C.; et al. Similar Complication Rates for Irreversible Electroporation and Thermal Ablation in Patients with Hepatocellular Tumors. Radiol. Oncol. 2019, 53, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Dollinger, M.; Beyer, L.P.; Haimerl, M.; Niessen, C.; Jung, E.M.; Zeman, F.; Stroszczynski, C.; Wiggermann, P. Adverse Effects of Irreversible Electroporation of Malignant Liver Tumors under CT Fluoroscopic Guidance: A Single-Center Experience. Diagn. Interv. Radiol. 2015, 21, 471–475. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Huang, W.; Wu, Z.; Wang, Y.; Wang, Q.; Wang, Z.; Liu, Q.; Liu, J.; Wang, S.; Ding, X.; et al. Percutaneous Ablation of Hepatic Tumors at the Hepatocaval Confluence Using Irreversible Electroporation: A Preliminary Study. Curr. Oncol. 2022, 29, 3950–3961. [Google Scholar] [CrossRef]
- Stillström, D.; Beermann, M.; Engstrand, J.; Freedman, J.; Nilsson, H. Initial Experience with Irreversible Electroporation of Liver Tumours. Eur. J. Radiol. Open 2019, 6, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Kriegmair, M.C.; Wagener, N.; Diehl, S.J.; Rathmann, N. Ablative Therapien Kleiner Nierentumoren. Urol. A 2018, 57, 285–294. [Google Scholar] [CrossRef]
- Chan, V.W.S.; Lenton, J.; Smith, J.; Jagdev, S.; Ralph, C.; Vasudev, N.; Bhattarai, S.; Lewington, A.; Kimuli, M.; Cartledge, J.; et al. Multimodal Image-Guided Ablation on Management of Renal Cancer in Von-Hippel-Lindau Syndrome Patients from 2004 to 2021 at a Specialist Centre: A Longitudinal Observational Study. Eur. J. Surg. Oncol. 2022, 48, 672–679. [Google Scholar] [CrossRef]
- Buijs, M.; Zondervan, P.J.; de Bruin, D.M.; van Lienden, K.P.; Bex, A.; van Delden, O.M. Feasibility and Safety of Irreversible Electroporation (IRE) in Patients with Small Renal Masses: Results of a Prospective Study. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 183.e1–183.e8. [Google Scholar] [CrossRef]
- Wendler, J.J.; Pech, M.; Fischbach, F.; Jürgens, J.; Friebe, B.; Baumunk, D.; Porsch, M.; Blaschke, S.; Schindele, D.; Siedentopf, S.; et al. Initial Assessment of the Efficacy of Irreversible Electroporation in the Focal Treatment of Localized Renal Cell Carcinoma with Delayed-Interval Kidney Tumor Resection (Irreversible Electroporation of Kidney Tumors Before Partial Nephrectomy [IRENE] Trial—An Ablate-and-Resect Pilot Study). Urology 2018, 114, 224–232. [Google Scholar] [CrossRef]
- Canvasser, N.E.; Sorokin, I.; Lay, A.H.; Morgan, M.S.C.; Ozayar, A.; Trimmer, C.; Cadeddu, J.A. Irreversible Electroporation of Small Renal Masses: Suboptimal Oncologic Efficacy in an Early Series. World J. Urol. 2017, 35, 1549–1555. [Google Scholar] [CrossRef]
- Dai, J.C.; Morgan, T.N.; Steinberg, R.L.; Johnson, B.A.; Garbens, A.; Cadeddu, J.A. Irreversible Electroporation for the Treatment of Small Renal Masses: 5-Year Outcomes. J. Endourol. 2021, 35, 1586–1592. [Google Scholar] [CrossRef]
- Min Wah, T.; Lenton, J.; Smith, J.; Bassett, P.; Jagdev, S.; Ralph, C.; Vasudev, N.; Bhattarai, S.; Kimuli, M.; Cartledge, J. Irreversible electroporation (IRE) in renal cell carcinoma (RCC): A mid-term clinical experience. Eur. Radiol. 2021, 31, 7491–7499. [Google Scholar] [CrossRef]
- Ren, F.; Li, Q.; Gao, X.; Zhu, K.; Zhang, J.; Chen, X.; Yan, X.; Chu, D.; Hu, L.; Gao, Z.; et al. Electrical and Thermal Analyses of Catheter-Based Irreversible Electroporation of Digestive Tract. Int. J. Hyperth. 2019, 36, 854–867. [Google Scholar] [CrossRef] [Green Version]
- Jeon, H.J.; Choi, H.S.; Keum, B.; Bang, E.J.; Lee, K.W.; Kim, S.H.; Yim, S.Y.; Lee, J.M.; Kim, E.S.; Seo, Y.S.; et al. Feasibility and Effectiveness of Endoscopic Irreversible Electroporation for the Upper Gastrointestinal Tract: An Experimental Animal Study. Sci. Rep. 2021, 11, 15353. [Google Scholar] [CrossRef]
- ClinicalTrials.Gov: Irreversible Electroporation (IRE) For Unresectable Esophageal Neoplasms. Available online: Https://Clinicaltrials.Gov/Ct2/Show/Study/NCT02430701 (accessed on 14 February 2023).
- Gong, X.; Chen, Z.; Hu, J.J.; Liu, C. Advances of Electroporation-Related Therapies and the Synergy with Immunotherapy in Cancer Treatment. Vaccines 2022, 10, 1942. [Google Scholar] [CrossRef]
- Shi, X.; O’Neill, C.; Wang, X.; Chen, Y.; Yu, Y.; Tan, M.; Lv, G.; Li, Y.; Martin, R.C.; Martin, R.C. Irreversible Electroporation Enhances Immunotherapeutic Effect in the Off-Target Tumor in a Murine Model of Orthotopic HCC. Am. J. Cancer Res. 2021, 11, 3304–3319. [Google Scholar]
- Sersa, G.; Teissie, J.; Cemazar, M.; Signori, E.; Kamensek, U.; Marshall, G.; Miklavcic, D. Electrochemotherapy of Tumors as in Situ Vaccination Boosted by Immunogene Electrotransfer. Cancer Immunol. Immunother. 2015, 64, 1315–1327. [Google Scholar] [CrossRef] [Green Version]
- Shankara Narayanan, J.S.; Ray, P.; Hayashi, T.; Whisenant, T.C.; Vicente, D.; Carson, D.A.; Miller, A.M.; Schoenberger, S.P.; White, R.R. Irreversible Electroporation Combined with Checkpoint Blockade and TLR7 Stimulation Induces Antitumor Immunity in a Murine Pancreatic Cancer Model. Cancer Immunol. Res. 2019, 7, 1714–1726. [Google Scholar] [CrossRef]
- Burbach, B.J.; O’Flanagan, S.D.; Shao, Q.; Young, K.M.; Slaughter, J.R.; Rollins, M.R.; Street, T.J.L.; Granger, V.E.; Beura, L.K.; Azarin, S.M.; et al. Irreversible Electroporation Augments Checkpoint Immunotherapy in Prostate Cancer and Promotes Tumor Antigen-Specific Tissue-Resident Memory CD8+ T Cells. Nat. Commun. 2021, 12, 3862. [Google Scholar] [CrossRef]
- Scheffer, H.J.; Stam, A.G.M.; Geboers, B.; Vroomen, L.G.P.H.; Ruarus, A.; de Bruijn, B.; van den Tol, M.P.; Kazemier, G.; Meijerink, M.R.; de Gruijl, T.D. Irreversible Electroporation of Locally Advanced Pancreatic Cancer Transiently Alleviates Immune Suppression and Creates a Window for Antitumor T Cell Activation. Oncoimmunology 2019, 8, 1652532. [Google Scholar] [CrossRef] [Green Version]
- Pandit, H.; Hong, Y.K.; Li, Y.; Rostas, J.; Pulliam, Z.; Li, S.P.; Martin, R.C.G. Evaluating the Regulatory Immunomodulation Effect of Irreversible Electroporation (IRE) in Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2019, 26, 800–806. [Google Scholar] [CrossRef]
- O’Neill, C.; Hayat, T.; Hamm, J.; Healey, M.; Zheng, Q.; Li, Y.; Martin, R.C.G. A Phase 1b Trial of Concurrent Immunotherapy and Irreversible Electroporation in the Treatment of Locally Advanced Pancreatic Adenocarcinoma. Surgery 2020, 168, 610–616. [Google Scholar] [CrossRef]
- He, C.; Sun, S.; Zhang, Y.; Li, S. Irreversible Electroporation plus Anti-Pd-1 Antibody versus Irreversible Electroporation Alone for Patients with Locally Advanced Pancreatic Cancer. J. Inflamm. Res. 2021, 14, 4795–4807. [Google Scholar] [CrossRef]
- Lin, M.; Zhang, X.; Liang, S.; Luo, H.; Alnaggar, M.; Liu, A.; Yin, Z.; Chen, J.; Niu, L.; Jiang, Y. Irreversible Electroporation plus Allogenic Vγ9Vδ2 T Cells Enhances Antitumor Effect for Locally Advanced Pancreatic Cancer Patients. Signal Transduct. Target. Ther. 2020, 5, 215. [Google Scholar] [CrossRef]
- Yang, Y.; Qin, Z.; Du, D.; Wu, Y.; Qiu, S.; Mu, F.; Xu, K.; Chen, J. Safety and Short-Term Efficacy of Irreversible Electroporation and Allogenic Natural Killer Cell Immunotherapy Combination in the Treatment of Patients with Unresectable Primary Liver Cancer. Cardiovasc. Intervent. Radiol. 2019, 42, 48–59. [Google Scholar] [CrossRef]
- Go, E.J.; Yang, H.; Chon, H.J.; Yang, D.; Ryu, W.; Kim, D.H.; Han, D.K.; Kim, C.; Park, W. Combination of Irreversible Electroporation and Sting Agonist for Effective Cancer Immunotherapy. Cancers 2020, 12, 3123. [Google Scholar] [CrossRef]
- Lasarte-Cia, A.; Lozano, T.; Cano, D.; Martín-Otal, C.; Navarro, F.; Gorraiz, M.; Casares, N.; Vivas, I.; Lasarte, J.J. Intratumoral STING Agonist Injection Combined with Irreversible Electroporation Delays Tumor Growth in a Model of Hepatocarcinoma. Biomed. Res. Int. 2021, 2021, 8852233. [Google Scholar] [CrossRef]
- Peng, H.; Shen, J.; Long, X.; Zhou, X.; Zhang, J.; Xu, X.; Huang, T.; Xu, H.; Sun, S.; Li, C.; et al. Local Release of TGF-β Inhibitor Modulates Tumor-Associated Neutrophils and Enhances Pancreatic Cancer Response to Combined Irreversible Electroporation and Immunotherapy. Adv. Sci. 2022, 9, 2105240. [Google Scholar] [CrossRef]
- Arena, C.B.; Sano, M.B.; Rylander, M.N.; Davalos, R.V. Theoretical Considerations of Tissue Electroporation with High-Frequency Bipolar Pulses. IEEE Trans. Biomed. Eng. 2011, 58, 1474–1482. [Google Scholar] [CrossRef]
- Ivey, J.W.; Latouche, E.L.; Sano, M.B.; Rossmeisl, J.H.; Davalos, R.V.; Verbridge, S.S. Targeted Cellular Ablation Based on the Morphology of Malignant Cells. Sci. Rep. 2015, 5, 17157. [Google Scholar] [CrossRef] [Green Version]
- Arena, C.B.; Sano, M.B.; Rossmeisl, J.H.; Caldwell, J.L.; Garcia, P.A.; Rylander, M.N.; Davalos, R.V. High-Frequency Irreversible Electroporation (H-FIRE) for Non-Thermal Ablation without Muscle Contraction. Biomed. Eng. Online 2011, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- Ringel-Scaia, V.M.; Beitel-White, N.; Lorenzo, M.F.; Brock, R.M.; Huie, K.E.; Coutermarsh-Ott, S.; Eden, K.; McDaniel, D.K.; Verbridge, S.S.; Rossmeisl, J.H.; et al. High-Frequency Irreversible Electroporation Is an Effective Tumor Ablation Strategy That Induces Immunologic Cell Death and Promotes Systemic Anti-Tumor Immunity. EBioMedicine 2019, 44, 112–125. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, I.A.; Latouche, E.L.; DeWitt, M.R.; Swet, J.H.; Kirks, R.C.; Baker, E.H.; Iannitti, D.A.; Vrochides, D.; Davalos, R.V.; McKillop, I.H. Induction of Rapid, Reproducible Hepatic Ablations Using next-Generation, High Frequency Irreversible Electroporation (H-FIRE) in Vivo. HPB 2016, 18, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Partridge, B.R.; O’Brien, T.J.; Lorenzo, M.F.; Coutermarsh-Ott, S.L.; Barry, S.L.; Stadler, K.; Muro, N.; Meyerhoeffer, M.; Allen, I.C.; Davalos, R.V.; et al. High-Frequency Irreversible Electroporation for Treatment of Primary Liver Cancer: A Proof-of-Principle Study in Canine Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2020, 31, 482–491.e4. [Google Scholar] [CrossRef]
- Campelo, S.N.; Lorenzo, M.F.; Partridge, B.; Alinezhadbalalami, N.; Kani, Y.; Garcia, J.; Saunier, S.; Thomas, S.C.; Hinckley, J.; Verbridge, S.S.; et al. High-Frequency Irreversible Electroporation Improves Survival and Immune Cell Infiltration in Rodents with Malignant Gliomas. Front. Oncol. 2023, 13, 1171278. [Google Scholar] [CrossRef]
- Lorenzo, M.F.; Campelo, S.N.; Arroyo, J.P.; Aycock, K.N.; Hinckley, J.; Arena, C.B.; Rossmeisl, J.H.; Davalos, R.V. An Investigation for Large Volume, Focal Blood-Brain Barrier Disruption with High-Frequency Pulsed Electric Fields. Pharmaceuticals 2021, 14, 1333. [Google Scholar] [CrossRef]
- Lorenzo, M.F.; Thomas, S.C.; Kani, Y.; Hinckley, J.; Lee, M.; Adler, J.; Verbridge, S.S.; Hsu, F.C.; Robertson, J.L.; Davalos, R.V.; et al. Temporal Characterization of Blood–Brain Barrier Disruption with High-Frequency Electroporation. Cancers 2019, 11, 1850. [Google Scholar] [CrossRef] [Green Version]
- Moshkovits, Y.; Grynberg, D.; Heller, E.; Maizels, L.; Maor, E. Differential Effect of High-Frequency Electroporation on Myocardium vs. Non-Myocardial Tissues. Europace 2023, 25, 748–755. [Google Scholar] [CrossRef]
- Heller, E.; Garcia-Sanchez, T.; Moshkovits, Y.; Rabinovici, R.; Grynberg, D.; Segev, A.; Asirvatham, S.J.; Ivorra, A.; Maor, E. Comparing High-Frequency with Monophasic Electroporation Protocols in an In Vivo Beating Heart Model. JACC Clin. Electrophysiol. 2021, 7, 959–964. [Google Scholar] [CrossRef]
- Dong, S.; Wang, H.; Zhao, Y.; Sun, Y.; Yao, C. First Human Trial of High-Frequency Irreversible Electroporation Therapy for Prostate Cancer. Technol. Cancer Res. Treat. 2018, 17, 1533033818789692. [Google Scholar] [CrossRef]
- Wang, H.; Xue, W.; Yan, W.; Yin, L.; Dong, B.; He, B.; Yu, Y.; Shi, W.; Zhou, Z.; Lin, H.; et al. Extended Focal Ablation of Localized Prostate Cancer with High-Frequency Irreversible Electroporation: A Nonrandomized Controlled Trial. JAMA Surg. 2022, 157, 693–700. [Google Scholar] [CrossRef]
- Heller, L.; Pottinger, C.; Jaroszeski, M.J.; Gilbert, R.; Heller, R. In Vivo Electroporation of Plasmids Encoding GM-CSF or Interleukin-2 into Existing B16 Melanomas Combined with Electrochemotherapy Induces Long-Term Antitumour Immunity. Melanoma Res. 2000, 10, 577–583. [Google Scholar] [CrossRef]
- Heller, L.; Merkler, K.; Westover, J.; Cruz, Y.; Coppola, D.; Benson, K.; Daud, A.; Heller, R. Evaluation of Toxicity following Electrically Mediated Interleukin-12 Gene Delivery in a B16 Mouse Melanoma Model. Clin. Cancer Res. 2006, 12, 3177–3183. [Google Scholar] [CrossRef] [Green Version]
- Cha, E.; Daud, A. Plasmid IL-2 Electroporation in Melanoma. Hum. Vaccin. Immunother. 2012, 8, 1734–1738. [Google Scholar] [CrossRef] [Green Version]
- Algazi, A.P.; Twitty, C.G.; Tsai, K.K.; Le, M.; Pierce, R.; Browning, E.; Hermiz, R.; Canton, D.A.; Bannavong, D.; Oglesby, A.; et al. Phase II Trial of IL-12 Plasmid Transfection and PD-1 Blockade in Immunologically Quiescent Melanoma. Clin. Cancer Res. 2020, 26, 2827–2837. [Google Scholar] [CrossRef]
- Bhatia, S.; Longino, N.V.; Miller, N.J.; Kulikauskas, R.; Iyer, J.G.; Ibrani, D.; Blom, A.; Byrd, D.R.; Parvathaneni, U.; Twitty, C.G.; et al. Intratumoral Delivery of Plasmid IL12 via Electroporation Leads to Regression of Injected and Noninjected Tumors in Merkel Cell Carcinoma. Clin. Cancer Res. 2020, 26, 598–607. [Google Scholar] [CrossRef] [Green Version]
- Telli, M.L.; Nagata, H.; Wapnir, I.; Acharya, C.R.; Zablotsky, K.; Fox, B.A.; Bifulco, C.B.; Jensen, S.M.; Ballesteros-Merino, C.; Le, M.H.; et al. Intratumoral Plasmid IL12 Expands CD8þ T Cells and Induces a CXCR3 Gene Signature in Triple-Negative Breast Tumors That Sensitizes Patients to Anti–PD-1 Therapy. Clin. Cancer Res. 2021, 27, 2481–2493. [Google Scholar] [CrossRef]
- Kiełbik, A.; Szlasa, W.; Saczko, J.; Kulbacka, J. Electroporation-Based Treatments in Urology. Cancers 2020, 12, 2208. [Google Scholar] [CrossRef]
- Low, L.; Mander, A.; Mccann, K.; Dearnaley, D.; Tjelle, T.; Mathiesen, I.; Stevenson, F.; Ottensmeier, C.H. DNA Vaccination with Electroporation Induces Increased Antibody Responses in Patients with Prostate Cancer. Hum. Gene Ther. 2009, 20, 1269–1278. [Google Scholar] [CrossRef]
- Eriksson, F.; Tötterman, T.; Maltais, A.K.; Pisa, P.; Yachnin, J. DNA Vaccine Coding for the Rhesus Prostate Specific Antigen Delivered by Intradermal Electroporation in Patients with Relapsed Prostate Cancer. Vaccine 2013, 31, 3843–3848. [Google Scholar] [CrossRef]
- Daud, A.I.; Loo, K.; Pauli, M.L.; Sanchez-Rodriguez, R.; Sandoval, P.M.; Taravati, K.; Tsai, K.; Nosrati, A.; Nardo, L.; Alvarado, M.D.; et al. Tumor Immune Profiling Predicts Response to Anti-PD-1 Therapy in Human Melanoma. J. Clin. Investig. 2016, 126, 3447–3452. [Google Scholar] [CrossRef]
- Fernandez-Penas, P.; Carlino, M.; Tsai, K.; Atkinson, V.; Shaheen, M.; Thomas, S.; Mihalcioiu, C.; Van Hagen, T.; Roberts-Thomson, R.; Haydon, A.; et al. 799 Durable Responses and Immune Activation with Intratumoral Electroporation of PIL-12 plus Pembrolizumab in Actively Progressing Anti-PD-1 Refractory Advanced Melanoma: KEYNOTE 695 Interim Data. J. Immunother. Cancer 2020, 8, A477. [Google Scholar] [CrossRef]
- Han, M.; Nguyen, B.; Lee, J.Y.; Browning, E.; Zhang, J.; Mukhopadhyay, A.; Gujar, R.; Salazar, J.; Hermiz, R.; Svenson, L.; et al. Intratumoral Electroporation of Plasmid Encoded IL12 and Membrane-Anchored Anti-CD3 Increases Systemic Tumor Immunity. Mol. Cancer Res. 2022, 20, 983–995. [Google Scholar] [CrossRef]
- Mir, L.M. Bases and Rationale of the Electrochemotherapy. Eur. J. Cancer Suppl. 2006, 4, 38–44. [Google Scholar] [CrossRef]
- Tounekti, O.; Belehradek, J.; Mir, L.M. Bleomycin, an Apoptosis-Mimetic Drug That Induces Two Types of Cell Death Depending on the Number of Molecules Internalized. Cancer Res. 1993, 53, 5462–5469. [Google Scholar]
- Poddevin, B.; Orlowski, S.; Belehradek, J., Jr.; Mirt, L.M. Very high cytotoxicity of bleomycin introduced into the cytosol of cells in culture. Biochem. Pharmacol. 1991, 42, S67–S75. [Google Scholar] [CrossRef]
- Sersa, G.; Stabuc, B.; Cemazar, M.; Jancar, B.; Miklavcic, D.; Rudolf, Z. Electrochemotherapy with Cisplatin: Potentiation of Local Cisplatin Antitumour EVectiveness by Application of Electric Pulses in Cancer Patients. Eur. J. Cancer 1998, 34, 1213–1218. [Google Scholar] [CrossRef]
- Sersa, G.; Jarm, T.; Kotnik, T.; Coer, A.; Podkrajsek, M.; Sentjurc, M.; Miklavcic, D.; Kadivec, M.; Kranjc, S.; Secerov, A.; et al. Vascular Disrupting Action of Electroporation and Electrochemotherapy with Bleomycin in Murine Sarcoma. Br. J. Cancer 2008, 98, 388–398. [Google Scholar] [CrossRef] [Green Version]
- Jarm, T.; Cemazar, M.; Miklavcic, D.; Sersa, G. Antivascular Effects of Electrochemotherapy: Implications in Treatment of Bleeding Metastases. Expert. Rev. Anticancer Ther. 2010, 10, 729–746. [Google Scholar] [CrossRef]
- Gerlini, G.; Di Gennaro, P.; Borgognoni, L. Enhancing Anti-Melanoma Immunity by Electrochemotherapy and in Vivo Dendritic-Cell Activation. Oncoimmunology 2012, 1, 1655–1657. [Google Scholar] [CrossRef] [Green Version]
- Di Gennaro, P.; Gerlini, G.; Urso, C.; Sestini, S.; Brandani, P.; Pimpinelli, N.; Borgognoni, L. CD4+FOXP3+ T Regulatory Cells Decrease and CD3+CD8+ T Cells Recruitment in TILs from Melanoma Metastases after Electrochemotherapy. Clin. Exp. Metastasis 2016, 33, 787–798. [Google Scholar] [CrossRef]
- Campana, L.G.; Edhemovic, I.; Soden, D.; Perrone, A.M.; Scarpa, M.; Campanacci, L.; Cemazar, M.; Valpione, S.; Miklavčič, D.; Mocellin, S.; et al. Electrochemotherapy—Emerging Applications Technical Advances, New Indications, Combined Approaches, and Multi-Institutional Collaboration. Eur. J. Surg. Oncol. 2019, 45, 92–102. [Google Scholar] [CrossRef]
- Gehl, J.; Sersa, G.; Matthiessen, L.W.; Muir, T.; Soden, D.; Occhini, A.; Quaglino, P.; Curatolo, P.; Campana, L.G.; Kunte, C.; et al. Updated Standard Operating Procedures for Electrochemotherapy of Cutaneous Tumours and Skin Metastases. Acta Oncol. 2018, 57, 874–882. [Google Scholar] [CrossRef]
- Gasbarrini, A.; Boriani, S.; Capanna, R.; Casadei, R.; Di Martino, A.; Spinelli, M.S.; Papapietro, N.; Piccioli, A.; Italian Orthopaedic Society Bone Metastasis Study Group. Management of Patients with Metastasis to the Vertebrae: Recommendations from the Italian Orthopaedic Society (SIOT) Bone Metastasis Study Group. Expert. Rev. Anticancer Ther. 2014, 14, 143–150. [Google Scholar] [CrossRef]
- Petrelli, F.; Ghidini, A.; Simioni, A.; Campana, L.G. Impact of Electrochemotherapy in Metastatic Cutaneous Melanoma: A Contemporary Systematic Review and Meta-Analysis. Acta Oncol. 2022, 61, 533–544. [Google Scholar] [CrossRef]
- Campana, L.G.; Peric, B.; Mascherini, M.; Spina, R.; Kunte, C.; Kis, E.; Rozsa, P.; Quaglino, P.; Jones, R.P.; Clover, A.J.P.; et al. Combination of Pembrolizumab with Electrochemotherapy in Cutaneous Metastases from Melanoma: A Comparative Retrospective Study from the Inspect and Slovenian Cancer Registry. Cancers 2021, 13, 4289. [Google Scholar] [CrossRef]
- Campana, L.G.; Quaglino, P.; de Terlizzi, F.; Mascherini, M.; Brizio, M.; Spina, R.; Bertino, G.; Kunte, C.; Odili, J.; Matteucci, P.; et al. Health-Related Quality of Life Trajectories in Melanoma Patients after Electrochemotherapy: Real-World Insights from the InspECT Register. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 2352–2363. [Google Scholar] [CrossRef]
- Campana, L.G.; Testori, A.; Mozzillo, N.; Rossi, C.R. Treatment of Metastatic Melanoma with Electrochemotherapy. J. Surg. Oncol. 2014, 109, 301–307. [Google Scholar] [CrossRef]
- Snoj, M.; Rudolf, Z.; Cemazar, M.; Jancar, B.; Sersa, G. Successful Sphincter-Saving Treatment of Anorectal Malignant Melanoma with Electrochemotherapy, Local Excision and Adjuvant Brachytherapy. Anticancer Drugs 2005, 16, 345–348. [Google Scholar] [CrossRef]
- Farricha, V.; Quaglino, P.; Brizio, M.; de Terlizzi, F.; Bartolo, J.; Carvalhal, S.; Caracò, C.; di Monta, G. Safety and Efficacy of Electrochemotherapy in a Series of Patients with Nonmetastasized Primary or Recurrent Anorectal Malignant Melanoma. Melanoma Res. 2021, 31, 76–80. [Google Scholar] [CrossRef]
- Bertino, G.; Muir, T.; Odili, J.; Groselj, A.; Marconato, R.; Curatolo, P.; Kis, E.; Lonkvist, C.K.; Clover, J.; Quaglino, P.; et al. Treatment of Basal Cell Carcinoma with Electrochemotherapy: Insights from the InspECT Registry (2008–2019). Curr. Oncol. 2022, 29, 5324–5337. [Google Scholar] [CrossRef]
- Bertino, G.; Groselj, A.; Campana, L.G.; Kunte, C.; Schepler, H.; Gehl, J.; Muir, T.; Clover, J.A.P.; Quaglino, P.; Kis, E.; et al. Electrochemotherapy for the Treatment of Cutaneous Squamous Cell Carcinoma: The INSPECT Experience (2008–2020). Front. Oncol. 2022, 12, 951662. [Google Scholar] [CrossRef]
- Cohen, P.R. Pleomorphic Appearance of Breast Cancer Cutaneous Metastases. Cureus 2021, 13, e20301. [Google Scholar] [CrossRef]
- Huang, S.; Parekh, V.; Waisman, J.; Jones, V.; Yuan, Y.; Vora, N.; Li, R.; Jung, J.; Kruper, L.; Abdulla, F.; et al. Cutaneous Metastasectomy: Is There a Role in Breast Cancer? A Systematic Review and Overview of Current Treatment Modalities. J. Surg. Oncol. 2022, 126, 217–238. [Google Scholar] [CrossRef]
- Ferioli, M.; Perrone, A.M.; Buwenge, M.; Arcelli, A.; Zamagni, A.; Macchia, G.; Deodato, F.; Cilla, S.; Tagliaferri, L.; de Terlizzi, F.; et al. Electrochemotherapy of Skin Metastases from Breast Cancer: A Systematic Review. Clin. Exp. Metastasis 2021, 38, 1–10. [Google Scholar] [CrossRef]
- Campana, L.G.; Valpione, S.; Falci, C.; Mocellin, S.; Basso, M.; Corti, L.; Balestrieri, N.; Marchet, A.; Rossi, C.R. The Activity and Safety of Electrochemotherapy in Persistent Chest Wall Recurrence from Breast Cancer after Mastectomy: A Phase-II Study. Breast Cancer Res. Treat. 2012, 134, 1169–1178. [Google Scholar] [CrossRef]
- Campanacci, L.; Cevolani, L.; de Terlizzi, F.; Saenz, L.; Alì, N.; Bianchi, G.; Donati, D.M. Electrochemotherapy Is Effective in the Treatment of Bone Metastases. Curr. Oncol. 2022, 29, 1672–1682. [Google Scholar] [CrossRef]
- Curatolo, P.; Quaglino, P.; Marenco, F.; Mancini, M.; Nardò, T.; Mortera, C.; Rotunno, R.; Calvieri, S.; Bernengo, M.G. Electrochemotherapy in the Treatment of Kaposi Sarcoma Cutaneous Lesions: A Two-Center Prospective Phase II Trial. Ann. Surg. Oncol. 2012, 19, 192–198. [Google Scholar] [CrossRef]
- Latini, A.; Bonadies, A.; Trento, E.; Bultrini, S.; Cota, C.; Solivetti, F.M.; Ferraro, C.; Ardigò, M.; Amorosi, B.; Palamara, G.; et al. Effective Treatment of Kaposi’s Sarcoma by Electrochemotherapy and Intravenous Bleomycin Administration. Dermatol. Ther. 2012, 25, 214–218. [Google Scholar] [CrossRef]
- Starita, N.; di Monta, G.; Cerasuolo, A.; Marone, U.; Anniciello, A.M.; Botti, G.; Buonaguro, L.; Buonaguro, F.M.; Tornesello, M.L. Effect of Electrochemotherapy on Human Herpesvirus 8 Kinetics in Classic Kaposi Sarcoma. Infect. Agent Cancer 2017, 12, 35. [Google Scholar] [CrossRef] [Green Version]
- Campana, L.G.; Kis, E.; Bottyán, K.; Orlando, A.; de Terlizzi, F.; Mitsala, G.; Careri, R.; Curatolo, P.; Snoj, M.; Sersa, G.; et al. Electrochemotherapy for Advanced Cutaneous Angiosarcoma: A European Register-Based Cohort Study from the International Network for Sharing Practices of Electrochemotherapy (InspECT). Int. J. Surg. 2019, 72, 34–42. [Google Scholar] [CrossRef]
- Guida, M.; Campana, L.G.; Curatolo, P.; Strippoli, S.; Bonadies, A.; Grilz, G.; Cabula, C.; Rotunno, R.; Bucher, S.; Solari, N.; et al. Local Treatment with Electrochemotherapy of Superficial Angiosarcomas: Efficacy and Safety Results from a Multi-Institutional Retrospective Study. J. Surg. Oncol. 2016, 114, 246–253. [Google Scholar] [CrossRef]
- Campana, L.G.; Valpione, S.; Tosi, A.; Rastrelli, M.; Rossi, C.R.; Aliberti, C. Angiosarcoma on Lymphedema (Stewart-Treves Syndrome): A 12-Year Follow-up after Isolated Limb Perfusion, Limb Infusion, and Electrochemotherapy. J. Vasc. Interv. Radiol. 2016, 27, 444–446. [Google Scholar] [CrossRef]
- Cencelj-Arnez, R.; Novak, J.; Klevisar Ivancic, A.; Bosnjak, M.; Cemazar, M.; Snoj, M. Radiotherapy-Associated Angiosarcoma in the Breast Reconstructed by Autologous Free-Flap and Treated with Electrochemotherapy. Radiol. Oncol. 2020, 55, 77–81. [Google Scholar] [CrossRef]
- Simioni, A.; Valpione, S.; Granziera, E.; Rossi, C.R.; Cavallin, F.; Spina, R.; Sieni, E.; Aliberti, C.; Stramare, R.; Campana, L.G. Ablation of Soft Tissue Tumours by Long Needle Variable Electrode-Geometry Electrochemotherapy: Final Report from a Single-Arm, Single-Centre Phase-2 Study. Sci. Rep. 2020, 10, 2291. [Google Scholar] [CrossRef] [Green Version]
- Ottlakan, A.; Lazar, G.; Hideghety, K.; Koszo, R.L.; Deak, B.; Nagy, A.; Besenyi, Z.; Bottyan, K.; Vass, G.Z.; Olah, J.; et al. Clinical Considerations of Bleomycin Based Electrochemotherapy with Variable Electrode Geometry Electrodes for Inoperable, Deep-Seated Soft Tissue Sarcomas. Bioelectrochemistry 2022, 148, 108220. [Google Scholar] [CrossRef]
- Kostusiak, M.; Murugan, S.; Muir, T. Bleomycin Electrosclerotherapy Treatment in the Management of Vascular Malformations. Dermatol. Surg. 2022, 48, 67–71. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Piccirillo, M.; Palaia, R.; Petrillo, A.; Lastoria, S.; Izzo, F. Electrochemotherapy in Locally Advanced Pancreatic Cancer: Preliminary Results. Int. J. Surg. 2015, 18, 230–236. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Petrillo, A.; Grassi, R.; Belli, A.; Palaia, R.; Izzo, F.; Carrafiello, G.; Miele, V. Local Ablation of Pancreatic Tumors: State of the Art and Future Perspectives. World J. Gastroenterol. 2021, 27, 3413–3428. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; D’Alessio, V.; Simonetti, I.; Grassi, F.; Silvestro, L.; Palaia, R.; Belli, A.; Patrone, R.; Piccirillo, M.; et al. Percutanous Electrochemotherapy (ECT) in Primary and Secondary Liver Malignancies: A Systematic Review. Diagnostics 2023, 13, 209. [Google Scholar] [CrossRef]
- Egeland, C.; Baeksgaard, L.; Johannesen, H.; Löfgren, J.; Plaschke, C.; Svendsen, L.; Gehl, J.; Achiam, M. Endoscopic Electrochemotherapy for Esophageal Cancer: A Phase I Clinical Study. Endosc. Int. Open 2018, 06, E727–E734. [Google Scholar] [CrossRef] [Green Version]
- Falk Hansen, H.; Bourke, M.; Stigaard, T.; Clover, J.; Buckley, M.; O’Riordain, M.; Winter, D.C.; Hjorth Johannesen, H.; Hansen, R.H.; Heebøll, H.; et al. Electrochemotherapy for Colorectal Cancer Using Endoscopic Electroporation: A Phase 1 Clinical Study. Endosc. Int. Open 2020, 08, E124–E132. [Google Scholar] [CrossRef] [Green Version]
- Rega, D.; Granata, V.; Petrillo, A.; Pace, U.; di Marzo, M.; Fusco, R.; D’alessio, V.; Nasti, G.; Romano, C.; Avallone, A.; et al. Electrochemotherapy of Primary Colon Rectum Cancer and Local Recurrence: Case Report and Prospective Analysis. J. Clin. Med. 2022, 11, 2745. [Google Scholar] [CrossRef]
- Schipilliti, F.M.; Onorato, M.; Arrivi, G.; Panebianco, M.; Lerinò, D.; Milano, A.; Roberto, M.; Capalbo, C.; Mazzuca, F. Electrochemotherapy for Solid Tumors: Literature Review and Presentation of a Novel Endoscopic Approach. Radiol. Oncol. 2022, 56, 285–291. [Google Scholar] [CrossRef]
- Ferioli, M.; Guido, A.; Buwenge, M.; Coe, M.; Galuppi, A.; de Terlizzi, F.; Poggioli, G.; Morganti, A.G. Anorectal Adenocarcinoma Recurrence Successfully Treated with Electrochemotherapy: A Case Report. Anticancer Drugs 2020, 31, 73–75. [Google Scholar] [CrossRef]
- Bonadies, A.; Bertozzi, E.; Cristiani, R.; Govoni, F.A.; Migliano, E. Electrochemotherapy in Skin Malignancies of Head and Neck Cancer Patients: Clinical Efficacy and Aesthetic Benefits. Acta Derm. Venereol. 2019, 99, 1246–1252. [Google Scholar] [CrossRef]
- Lyons, P.; Kennedy, A.; Clover, A.J.P. Electrochemotherapy and Basal Cell Carcinomas: First-Time Appraisal of the Efficacy of Electrochemotherapy on Survivorship Using FACE-Q. JPRAS Open 2021, 27, 119–128. [Google Scholar] [CrossRef]
- Campana, L.G.; Testori, A.; Curatolo, P.; Quaglino, P.; Mocellin, S.; Framarini, M.; Borgognoni, L.; Ascierto, P.A.; Mozzillo, N.; Guida, M.; et al. Treatment Efficacy with Electrochemotherapy: A Multi-Institutional Prospective Observational Study on 376 Patients with Superficial Tumors. Eur. J. Surg. Oncol. 2016, 42, 1914–1923. [Google Scholar] [CrossRef] [Green Version]
- Campana, L.G.; Mocellin, S.; Basso, M.; Puccetti, O.; De Salvo, G.L.; Chiarion-Sileni, V.; Vecchiato, A.; Corti, L.; Rossi, C.R.; Nitti, D. Bleomycin-Based Electrochemotherapy: Clinical Outcome from a Single Institution’s Experience with 52 Patients. Ann. Surg. Oncol. 2009, 16, 191–199. [Google Scholar] [CrossRef]
- Bertino, G.; Sersa, G.; De Terlizzi, F.; Occhini, A.; Plaschke, C.C.; Groselj, A.; Langdon, C.; Grau, J.J.; McCaul, J.A.; Heuveling, D.; et al. European Research on Electrochemotherapy in Head and Neck Cancer (EURECA) Project: Results of the Treatment of Skin Cancer. Eur. J. Cancer 2016, 63, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Bastrup, F.A.; Vissing, M.; Gehl, J. Electrochemotherapy with Intravenous Bleomycin for Patients with Cutaneous Malignancies, across Tumour Histology: A Systematic Review. Acta Oncol. 2022, 61, 1093–1104. [Google Scholar] [CrossRef]
- Sersa, G.; Ursic, K.; Cemazar, M.; Heller, R.; Bosnjak, M.; Campana, L.G. Biological Factors of the Tumour Response to Electrochemotherapy: Review of the Evidence and a Research Roadmap. Eur. J. Surg. Oncol. 2021, 47, 1836–1846. [Google Scholar] [CrossRef]
- Justesen, T.F.; Orhan, A.; Raskov, H.; Nolsoe, C.; Gögenur, I. Electroporation and Immunotherapy—Unleashing the Abscopal Effect. Cancers 2022, 14, 2876. [Google Scholar] [CrossRef]
- Heppt, M.V.; Eigentler, T.K.; Kähler, K.C.; Herbst, R.A.; Göppner, D.; Gambichler, T.; Ulrich, J.; Dippel, E.; Loquai, C.; Schell, B.; et al. Immune Checkpoint Blockade with Concurrent Electrochemotherapy in Advanced Melanoma: A Retrospective Multicenter Analysis. Cancer Immunol. Immunother. 2016, 65, 951–959. [Google Scholar] [CrossRef]
- Theurich, S.; Rothschild, S.I.; Hoffmann, M.; Fabri, M.; Sommer, A.; Garcia-Marquez, M.; Thelen, M.; Schill, C.; Merki, R.; Schmid, T.; et al. Local Tumor Treatment in Combination with Systemic Ipilimumab Immunotherapy Prolongs Overall Survival in Patients with Advanced Malignant Melanoma. Cancer Immunol. Res. 2016, 4, 744–754. [Google Scholar] [CrossRef] [Green Version]
- Trotovšek, B.; Djokić, M.; Čemažar, M.; Serša, G. New era of electrochemotherapy in treatment of liver tumors in conjunction with immunotherapies. World J. Gastroenterol. 2021, 27, 8216–8226. [Google Scholar] [CrossRef]
- Machiels, J.P.; René Leemans, C.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous Cell Carcinoma of the Oral Cavity, Larynx, Oropharynx and Hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef]
- Plaschke, C.C.; Bertino, G.; McCaul, J.A.; Grau, J.J.; de Bree, R.; Sersa, G.; Occhini, A.; Groselj, A.; Langdon, C.; Heuveling, D.A.; et al. European Research on Electrochemotherapy in Head and Neck Cancer (EURECA) Project: Results from the Treatment of Mucosal Cancers. Eur. J. Cancer 2017, 87, 172–181. [Google Scholar] [CrossRef]
- Pisani, S.; Bertino, G.; Prina-Mello, A.; Locati, L.D.; Mauramati, S.; Genta, I.; Dorati, R.; Conti, B.; Benazzo, M. Electroporation in Head-and-Neck Cancer: An Innovative Approach with Immunotherapy and Nanotechnology Combination. Cancers 2022, 14, 5363. [Google Scholar] [CrossRef]
- Campana, L.G.; Clover, A.J.P.; Valpione, S.; Quaglino, P.; Gehl, J.; Kunte, C.; Snoj, M.; Cemazar, M.; Rossi, C.R.; Miklavcic, D.; et al. Recommendations for Improving the Quality of Reporting Clinical Electrochemotherapy Studies Based on Qualitative Systematic Review. Radiol. Oncol. 2016, 50, 1–13. [Google Scholar] [CrossRef]
- Campana, L.G.; Valpione, S.; Mocellin, S.; Sundararajan, R.; Granziera, E.; Sartore, L.; Chiarion-Sileni, V.; Rossi, C.R. Electrochemotherapy for Disseminated Superficial Metastases from Malignant Melanoma. Br. J. Surg. 2012, 99, 821–830. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Salati, S.; Petrillo, A.; di Bernardo, E.; Grassi, R.; Palaia, R.; Danti, G.; la Porta, M.; Cadossi, M.; et al. A Systematic Review about Imaging and Histopathological Findings for Detecting and Evaluating Electroporation Based Treatments Response. Int. J. Environ. Res. Public Health 2021, 18, 5592. [Google Scholar] [CrossRef]
- Clover, A.J.P.; de Terlizzi, F.; Bertino, G.; Curatolo, P.; Odili, J.; Campana, L.G.; Kunte, C.; Muir, T.; Brizio, M.; Sersa, G.; et al. Electrochemotherapy in the Treatment of Cutaneous Malignancy: Outcomes and Subgroup Analysis from the Cumulative Results from the Pan-European International Network for Sharing Practice in Electrochemotherapy Database for 2482 Lesions in 987 Patients. Eur. J. Cancer 2020, 138, 30–40. [Google Scholar] [CrossRef]
- Cabula, C.; Campana, L.G.; Grilz, G.; Galuppo, S.; Bussone, R.; de Meo, L.; Bonadies, A.; Curatolo, P.; de Laurentiis, M.; Renne, M.; et al. Electrochemotherapy in the Treatment of Cutaneous Metastases from Breast Cancer: A Multicenter Cohort Analysis. Ann. Surg. Oncol. 2015, 22, 442–450. [Google Scholar] [CrossRef]
- Campana, L.G.; Marconato, R.; Valpione, S.; Galuppo, S.; Alaibac, M.; Rossi, C.R.; Mocellin, S. Basal Cell Carcinoma: 10-Year Experience with Electrochemotherapy. J. Transl. Med. 2017, 15, 122. [Google Scholar] [CrossRef] [Green Version]
- Sersa, G.; Mascherini, M.; di Prata, C.; Odili, J.; de Terlizzi, F.; McKenzie, G.A.G.; Clover, A.J.P.; Bertino, G.; Spina, R.; Groselj, A.; et al. Outcomes of Older Adults Aged 90 and over with Cutaneous Malignancies after Electrochemotherapy with Bleomycin: A Matched Cohort Analysis from the InspECT Registry. Eur. J. Surg. Oncol. 2021, 47, 902–912. [Google Scholar] [CrossRef]
- Perrone, A.M.; Galuppi, A.; Borghese, G.; Corti, B.; Ferioli, M.; della Gatta, A.N.; Bovicelli, A.; Morganti, A.G.; de Iaco, P. Electrochemotherapy Pre-Treatment in Primary Squamous Vulvar Cancer. Our Preliminary Experience. J. Surg. Oncol. 2018, 117, 1813–1817. [Google Scholar] [CrossRef]
- Fabrizio, T.; Cagiano, L.; de Terlizzi, F.; Grieco, M.P. Neoadjuvant Treatment by ECT in Cutaneous Malignant Neoplastic Lesions. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 904–912. [Google Scholar] [CrossRef]
- Rega, D.; Granata, V.; Petrillo, A.; Pace, U.; Sassaroli, C.; Di Marzo, M.; Cervone, C.; Fusco, R.; D’alessio, V.; Nasti, G.; et al. Organ Sparing for Locally Advanced Rectal Cancer after Neoadjuvant Treatment Followed by Electrochemotherapy. Cancers 2021, 13, 3199. [Google Scholar] [CrossRef]
- Campana, L.G.; Balestrieri, N.; Menin, N. Adjuvant Skin-Sparing Electrochemotherapy in a Breast Cancer Patient with a Prosthetic Implant: 5-Year Follow-up Outcomes. J. Surg. Case Rep. 2022, 2022, rjac199. [Google Scholar] [CrossRef]
- Izzo, F.; Granata, V.; Fusco, R.; D’alessio, V.; Petrillo, A.; Lastoria, S.; Piccirillo, M.; Albino, V.; Belli, A.; Tafuto, S.; et al. Clinical Phase I/II Study: Local Disease Control and Survival in Locally Advanced Pancreatic Cancer Treated with Electrochemotherapy. J. Clin. Med. 2021, 10, 1305. [Google Scholar] [CrossRef] [PubMed]
- Perri, F.; Longo, F.; Fusco, R.; D’alessio, V.; Aversa, C.; Pavone, E.; Pontone, M.; Marciano, M.L.; Villano, S.; Franco, P.; et al. Electrochemotherapy as a First Line Treatment in Recurrent Squamous Cell Carcinoma of the Oral Cavity and Oropharynx Pdl-1 Negative and/or with Evident Contraindication to Immunotherapy: A Randomized Multicenter Controlled Trial. Cancers 2021, 13, 2210. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.; Grocott, P.; Purssell, E.; Murrells, T. Electrochemotherapy for the Palliative Management of Cutaneous Metastases: A Systematic Review and Meta-Analysis. Eur. J. Surg. Oncol. 2019, 45, 2257–2267. [Google Scholar] [CrossRef]
- Curatolo, P.; Careri, R.; Simioni, A.; Campana, L.G. Cryotherapy, Imiquimod, and Electrochemotherapy Are Effective Options for Kaposi Sarcoma: A Call for Standardization to Allow for Comparisons and Informed Decisions. J. Cutan Med. Surg. 2020, 24, 218–219. [Google Scholar] [CrossRef]
- Campana, L.G.; Gehl, J. Cutaneous Metastases from Breast Cancer: Considerations for Implementing Rigorous Evaluation of Local Therapies. J. Surg. Oncol. 2022, 126, 1145–1147. [Google Scholar] [CrossRef]
- Gibot, L.; Montigny, A.; Baaziz, H.; Fourquaux, I.; Audebert, M.; Rols, M.P. Calcium Delivery by Electroporation Induces in Vitro Cell Death through Mitochondrial Dysfunction without DNA Damages. Cancers 2020, 12, 425. [Google Scholar] [CrossRef] [Green Version]
- Frandsen, S.K.; Vissing, M.; Gehl, J. A Comprehensive Review of Calcium Electroporation—A Novel Cancer Treatment Modality. Cancers 2020, 12, 290. [Google Scholar] [CrossRef] [Green Version]
- Frandsen, S.K.; Gibot, L.; Madi, M.; Gehl, J.; Rols, M.P. Calcium Electroporation: Evidence for Differential Effects in Normal and Malignant Cell Lines, Evaluated in a 3D Spheroid Model. PLoS ONE 2015, 10, e0144028. [Google Scholar] [CrossRef] [Green Version]
- Falk, H.; Matthiessen, L.W.; Wooler, G.; Gehl, J. Calcium Electroporation for Treatment of Cutaneous Metastases: A Randomized Double-Blinded Phase II Study, Comparing the Effect of Calcium Electroporation with Electrochemotherapy. Acta Oncol. 2018, 57, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Falk, H.; Lambaa, S.; Johannesen, H.H.; Wooler, G.; Venzo, A.; Gehl, J. Electrochemotherapy and Calcium Electroporation Inducing a Systemic Immune Response with Local and Distant Remission of Tumors in a Patient with Malignant Melanoma—A Case Report. Acta Oncol. 2017, 56, 1126–1131. [Google Scholar] [CrossRef] [Green Version]
- Falk, H.; Forde, P.F.; Bay, M.L.; Mangalanathan, U.M.; Hojman, P.; Soden, D.M.; Gehl, J. Calcium Electroporation Induces Tumor Eradication, Long-Lasting Immunity and Cytokine Responses in the CT26 Colon Cancer Mouse Model. Oncoimmunology 2017, 6, e1301332. [Google Scholar] [CrossRef] [Green Version]
- Jensen, K.B.; Lonkvist, C.K.; Gehl, J.; Vissing, M. Calcium Electroporation for Management of Cutaneous Metastases in HER2-Positive Breast Cancer: A Case Report. Case Rep. Dermatol. 2022, 14, 330–338. [Google Scholar] [CrossRef]
- Vissing, M.; Ploen, J.; Pervan, M.; Vestergaard, K.; Schnefeldt, M.; Frandsen, S.K.; Rafaelsen, S.R.; Lindhardt, C.L.; Jensen, L.H.; Rody, A.; et al. Study Protocol Designed to Investigate Tumour Response to Calcium Electroporation in Cancers Affecting the Skin: A Non-Randomised Phase II Clinical Trial. BMJ Open 2021, 11, e046779. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, K.; Vissing, M.; Gehl, J.; Lindhardt, C.L. Qualitative Investigation of Experience and Quality of Life in Patients Treated with Calcium Electroporation for Cutaneous Metastases. Cancers 2023, 15, 599. [Google Scholar] [CrossRef]
- Stranzenbach, R.; Doerler, M.; Scholl, L.; Bechara, F.G. Calcium Electroporation in Primary Cutaneous Marginal Zone Lymphoma. J. Dtsch. Dermatol. Ges. 2021, 19, 1510–1512. [Google Scholar] [CrossRef]
- Plaschke, C.C.; Gehl, J.; Johannesen, H.H.; Fischer, B.M.; Kjaer, A.; Lomholt, A.F.; Wessel, I. Calcium Electroporation for Recurrent Head and Neck Cancer: A Clinical Phase I Study. Laryngoscope Investig. Otolaryngol. 2019, 4, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egeland, C.; Baeksgaard, L.; Gehl, J.; Gögenur, I.; Achiam, M.P. Palliative Treatment of Esophageal Cancer Using Calcium Electroporation. Cancers 2022, 14, 5283. [Google Scholar] [CrossRef]
- Broholm, M.; Vogelsang, R.; Bulut, M.; Stigaard, T.; Falk, H.; Frandsen, S.; Pedersen, D.L.; Perner, T.; Fiehn, A.-M.K.; Mølholm, I.; et al. Endoscopic Calcium Electroporation for Colorectal Cancer: A Phase I Study. Endosc. Int. Open 2023, 11, E451–E459. [Google Scholar] [CrossRef]
- Ahmed-Salim, Y.; Saso, S.; Meehan, H.E.; Galazis, N.; Phelps, D.L.; Jones, B.P.; Chan, M.; Chawla, M.; Lathouras, K.; Gabra, H.; et al. A Novel Application of Calcium Electroporation to Cutaneous Manifestations of Gynaecological Cancer. Eur. J. Gynaecol. Oncol. 2021, 42, 662–672. [Google Scholar] [CrossRef]
- Falk, H.; Vissing, M.; Wooler, G.; Gehl, J. Calcium Electroporation for Keloids: A First-in-Man Phase i Study. Dermatology 2021, 237, 961–969. [Google Scholar] [CrossRef]
- Davies, A.M.; Weinberg, U.; Palti, Y. Tumor Treating Fields: A New Frontier in Cancer Therapy. Ann. N. Y. Acad. Sci. 2013, 1291, 86–95. [Google Scholar] [CrossRef]
- Chen, D.; Le, S.B.; Hutchinson, T.E.; Calinescu, A.A.; Sebastian, M.; Jin, D.; Liu, T.; Ghiaseddin, A.; Rahman, M.; Tran, D.D. Tumor Treating Fields Dually Activate STING and AIM2 Inflammasomes to Induce Adjuvant Immunity in Glioblastoma. J. Clin. Investig. 2022, 132, e149258. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Wong, E.T.; Kanner, A.A.; Steinberg, D.; Engelhard, H.; Heidecke, V.; Kirson, E.D.; Taillibert, S.; Liebermann, F.; Dbalý, V.; et al. NovoTTF-100A versus Physician’s Choice Chemotherapy in Recurrent Glioblastoma: A Randomised Phase III Trial of a Novel Treatment Modality. Eur. J. Cancer 2012, 48, 2192–2202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceresoli, G.L.; Aerts, J.G.; Dziadziuszko, R.; Ramlau, R.; Cedres, S.; van Meerbeeck, J.P.; Mencoboni, M.; Planchard, D.; Chella, A.; Crinò, L.; et al. Tumour Treating Fields in Combination with Pemetrexed and Cisplatin or Carboplatin as First-Line Treatment for Unresectable Malignant Pleural Mesothelioma (STELLAR): A Multicentre, Single-Arm Phase 2 Trial. Lancet Oncol. 2019, 20, 1702–1709. [Google Scholar] [CrossRef]
- Jones, T.H.; Song, J.W.; Abushahin, L. Tumor Treating Fields: An Emerging Treatment Modality for Thoracic and Abdominal Cavity Cancers. Transl. Oncol. 2022, 15, 101296. [Google Scholar] [CrossRef] [PubMed]
- Mrugala, M.M.; Engelhard, H.H.; Dinh Tran, D.; Kew, Y.; Cavaliere, R.; Villano, J.L.; Annenelie Bota, D.; Rudnick, J.; Love Sumrall, A.; Zhu, J.J.; et al. Clinical Practice Experience with NovoTTF-100ATM System for Glioblastoma: The Patient Registry Dataset (PRiDe). Semin. Oncol. 2014, 41, S4–S13. [Google Scholar] [CrossRef] [Green Version]
- Rivera, F.; Benavides, M.; Gallego, J.; Guillen-Ponce, C.; Lopez-Martin, J.; Küng, M. Tumor Treating Fields in Combination with Gemcitabine or Gemcitabine plus Nab-Paclitaxel in Pancreatic Cancer: Results of the PANOVA Phase 2 Study. Pancreatology 2019, 19, 64–72. [Google Scholar] [CrossRef]
- Gkika, E.; Grosu, A.L.; Mercade, T.M.; Gracián, A.C.; Brunner, T.B.; Schultheiß, M.; Pazgan-Simon, M.; Seufferlein, T.; Touchefeu, Y. Tumor-Treating Fields Concomitant with Sorafenib in Advanced Hepatocellular Cancer: Results of the HEPANOVA Phase II Study. Cancers 2022, 14, 1568. [Google Scholar] [CrossRef]
- Pohling, C.; Nguyen, H.; Chang, E.; Schubert, K.E.; Nie, Y.; Bashkirov, V.; Yamamoto, V.; Zeng, Y.; Stupp, R.; Schulte, R.W.; et al. Current Status of the Preclinical Evaluation of Alternating Electric Fields as a Form of Cancer Therapy. Bioelectrochemistry 2023, 149, 108287. [Google Scholar] [CrossRef]
- Pless, M.; Droege, C.; von Moos, R.; Salzberg, M.; Betticher, D. A Phase I/II Trial of Tumor Treating Fields (TTFields) Therapy in Combination with Pemetrexed for Advanced Non-Small Cell Lung Cancer. Lung Cancer 2013, 81, 445–450. [Google Scholar] [CrossRef]
- Anadkat, M.J.; Lacouture, M.; Friedman, A.; Horne, Z.D.; Jung, J.; Kaffenberger, B.; Kalmadi, S.; Ovington, L.; Kotecha, R.; Abdullah, H.I.; et al. Expert Guidance on Prophylaxis and Treatment of Dermatologic Adverse Events with Tumor Treating Fields (TTFields) Therapy in the Thoracic Region. Front. Oncol. 2023, 12, 975473. [Google Scholar] [CrossRef] [PubMed]
- Benson, L. Tumor Treating Fields Technology: Alternating Electric Field Therapy for the Treatment of Solid Tumors. Semin. Oncol. Nurs. 2018, 34, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Onafowokan, O.O.; de Liguori Carino, N. Needle Tract Seeding following Percutaneous Irreversible Electroporation for Hepatocellular Carcinoma. BMJ Case Rep. 2022, 15, e251880. [Google Scholar] [CrossRef] [PubMed]
- Miranda, P.C.; Mekonnen, A.; Salvador, R.; Basser, P.J. Predicting the Electric Field Distribution in the Brain for the Treatment of Glioblastoma. Phys. Med. Biol. 2014, 59, 4137–4147. [Google Scholar] [CrossRef]
- Ballo, M.T.; Urman, N.; Lavy-Shahaf, G.; Grewal, J.; Bomzon, Z.; Toms, S. Correlation of Tumor Treating Fields Dosimetry to Survival Outcomes in Newly Diagnosed Glioblastoma: A Large-Scale Numerical Simulation-Based Analysis of Data from the Phase 3 EF-14 Randomized Trial. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1106–1113. [Google Scholar] [CrossRef] [Green Version]
- Naveh, A.; Hershkovich, H.S.; Kirson, E.D.; Weinberg, U.; Bomzon, Z. Transducer Array Layout Optimization for the Treatment of Pancreatic Cancer Using Tumor Treating Fields (TTFields) in the Phase 3 PANOVA-3 Trial. J. Clin. Oncol. 2019, 37, e15766. [Google Scholar] [CrossRef]
- Blatt, R.; Davidi, S.; Munster, M.; Shteingauz, A.; Cahal, S.; Zeidan, A.; Marciano, T.; Bomzon, Z.; Haber, A.; Giladi, M.; et al. In vivo safety of Tumor Treating Fields (TTFields) applied to the torso. Front. Oncol. 2021, 11, 744951. [Google Scholar] [CrossRef]
- Ghiaseddin, A.P.; Shin, D.; Melnick, K.; Tran, D.D. Tumor Treating Fields in the Management of Patients with Malignant Gliomas. Curr. Treat. Options Oncol. 2020, 21, 76. [Google Scholar] [CrossRef]
- Mannarino, L.; Mirimao, F.; Panini, N.; Paracchini, L.; Marchini, S.; Beltrame, L.; Amodeo, R.; Grosso, F.; Libener, R.; De Simone, I.; et al. Tumor Treating Fields Affect Mesothelioma Cell Proliferation by Exerting Histotype-Dependent Cell Cycle Checkpoint Activations and Transcriptional Modulations. Cell Death Dis. 2022, 13, 612. [Google Scholar] [CrossRef]
- Vergote, I.; von Moos, R.; Manso, L.; Van Nieuwenhuysen, E.; Concin, N.; Sessa, C. Tumor Treating Fields in Combination with Paclitaxel in Recurrent Ovarian Carcinoma: Results of the INNOVATE Pilot Study. Gynecol. Oncol. 2018, 150, 471–477. [Google Scholar] [CrossRef] [Green Version]
- Voloshin, T.; Kaynan, N.; Davidi, S.; Porat, Y.; Shteingauz, A.; Schneiderman, R.S.; Zeevi, E.; Munster, M.; Blat, R.; Tempel Brami, C.; et al. Tumor-Treating Fields (TTFields) Induce Immunogenic Cell Death Resulting in Enhanced Antitumor Efficacy When Combined with Anti-PD-1 Therapy. Cancer Immunol. Immunother. 2020, 69, 1191–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voloshin, T.; Schneiderman, R.S.; Volodin, A.; Shamir, R.R.; Kaynan, N.; Zeevi, E.; Koren, L.; Klein-Goldberg, A.; Paz, R.; Giladi, M.; et al. Tumor Treating Fields (Ttfields) Hinder Cancer Cell Motility through Regulation of Microtubule and Acting Dynamics. Cancers 2020, 12, 3016. [Google Scholar] [CrossRef]
- Kirson, E.D.; Giladi, M.; Gurvich, Z.; Itzhaki, A.; Mordechovich, D.; Schneiderman, R.S.; Wasserman, Y.; Ryffel, B.; Goldsher, D.; Palti, Y. Alternating Electric Fields (TTFields) Inhibit Metastatic Spread of Solid Tumors to the Lungs. Clin. Exp. Metastasis 2009, 26, 633–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, E.; Patel, C.B.; Pohling, C.; Young, C.; Song, J.; Flores, T.A.; Zeng, Y.; Joubert, L.M.; Arami, H.; Natarajan, A.; et al. Tumor Treating Fields Increases Membrane Permeability in Glioblastoma Cells. Cell Death Discov. 2018, 4, 113. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Shi, W.; Zhao, Q.; Zheng, Z.; Liu, Z.; Meng, L.; Dong, L.; Jiang, X. Progress and Prospect in Tumor Treating Fields Treatment of Glioblastoma. Biomed. Pharmacother. 2021, 141, 111810. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.; Lee, W.S.; Sai, S.; Kim, J.Y.; Kim, J.K.; Kim, E.H. Tumor-Treating Fields in Combination with Sorafenib Restrain the Proliferation of Liver Cancer in Vitro. Oncol. Lett. 2022, 24, 338. [Google Scholar] [CrossRef]
- Bomzon, Z.; Wenger, C.; Proescholdt, M.; Mohan, S. Tumor-Treating Fields at EMBC 2019: A Roadmap to Developing a Framework for TTFields Dosimetry and Treatment Planning. In Brain and Human Body Modeling 2020: Computational Human Models Presented at EMBC 2019 and the BRAIN Initiative; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 3–17. ISBN 9783030456238. [Google Scholar]
- Spratt, D.E.; Spratt, E.A.G.; Wu, S.; de Rosa, A.; Lee, N.Y.; Lacouture, M.E.; Barker, C.A. Efficacy of Skin-Directed Therapy for Cutaneous Metastases from Advanced Cancer: A Meta-Analysis. J. Clin. Oncol. 2014, 32, 3144–3155. [Google Scholar] [CrossRef] [Green Version]
- Colombo, G.L.; Matteo, S.; Mir, L.M. Cost-Effectiveness Analysis of Electrochemotherapy with the CliniporatorTM vs. Other Methods for the Control and Treatment of Cutaneous and Subcutaneous Tumors. Ther. Clin. Risk Manag. 2008, 4, 541–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirc, E.; Federici, C.; Bošnjak, M.; Perić, B.; Reberšek, M.; Pecchia, L.; Glumac, N.; Čemažar, M.; Snoj, M.; Serša, G.; et al. Early Cost-Effectiveness Analysis of Electrochemotherapy as a Prospect Treatment Modality for Skin Melanoma. Clin. Ther. 2020, 42, 1535–1548.e2. [Google Scholar] [CrossRef]
- Connock, M.; Auguste, P.; Dussart, C.; Guyotat, J.; Armoiry, X. Cost-Effectiveness of Tumor-Treating Fields Added to Maintenance Temozolomide in Patients with Glioblastoma: An Updated Evaluation Using a Partitioned Survival Model. J. Neurooncol. 2019, 143, 605–611. [Google Scholar] [CrossRef]
- Guzauskas, G.F.; Pollom, E.L.; Stieber, V.W.; Wang, B.C.M.; Garrison, L.P. Tumor Treating Fields and Maintenance Temozolomide for Newly-Diagnosed Glioblastoma: A Cost-Effectiveness Study. J. Med. Econ. 2019, 22, 1006–1013. [Google Scholar] [CrossRef] [Green Version]
- de la Rosette, J.; Dominguez-Escrig, J.; Zhang, K.; Teoh, J.; Barret, E.; Ramon-Borja, J.C.; Muir, G.; Bohr, J.; de Reijke, T.; Ng, C.F.; et al. Multicenter, Randomized, Single-Blind, 2-Arm Intervention Study Evaluating the Adverse Events and Quality of Life after Irreversible Electroporation for the Ablation of Localized Low-Intermediate Risk Prostate Cancer. J. Urol. 2023, 209, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Boc, N.; Edhemovic, I.; Kos, B.; Music, M.M.; Brecelj, E.; Trotovsek, B.; Bosnjak, M.; Djokic, M.; Miklavcic, D.; Cemazar, M.; et al. Ultrasonographic Changes in the Liver Tumors as Indicators of Adequate Tumor Coverage with Electric Field for Effective Electrochemotherapy. Radiol. Oncol. 2018, 52, 383–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rennert, J.; Wiesinger, I.; Schicho, A.; Wiggermann, P.; Stroszczynski, C.; Beyer, L.P.; Jung, E.M. Color Coded Perfusion Imaging with Contrast Enhanced Ultrasound (Ceus) for Post-Interventional Success Control Following Irreversible Electroporation (Ire) of Primary and Secondary Malignant Liver Lesions. J. Gastrointest. Liver Dis. 2019, 28, 311–318. [Google Scholar] [CrossRef]
- Ruarus, A.H.; Vroomen, L.G.P.H.; Puijk, R.S.; Scheffer, H.J.; Zonderhuis, B.M.; Kazemier, G.; van den Tol, M.P.; Berger, F.H.; Meijerink, M.R. Irreversible Electroporation in Hepatopancreaticobiliary Tumours. Can. Assoc. Radiol. J. 2018, 69, 38–50. [Google Scholar] [CrossRef]
- Heller, R.; Heller, L.C. Gene Electrotransfer Clinical Trials. Adv. Genet. 2015, 89, 235–262. [Google Scholar] [CrossRef]
- Rosazza, C.; Meglic, S.H.; Zumbusch, A.; Rols, M.-P.; Miklavcic, D. Gene Electrotransfer: A Mechanistic Perspective. Curr. Gene Ther. 2016, 16, 98–129. [Google Scholar] [CrossRef] [Green Version]
- Da Luz, J.C.D.S.; Antunes, F.; Clavijo-Salomon, M.A.; Signori, E.; Tessarollo, N.G.; Strauss, B.E. Clinical Applications and Immunological Aspects of Electroporation-Based Therapies. Vaccines 2021, 9, 727. [Google Scholar] [CrossRef]
- Martin, R.C.G.; Durham, A.N.; Besselink, M.G.; Iannitti, D.; Weiss, M.J.; Wolfgang, C.L.; Huang, K.W. Irreversible Electroporation in Locally Advanced Pancreatic Cancer: A Call for Standardization of Energy Delivery. J. Surg. Oncol. 2016, 114, 865–871. [Google Scholar] [CrossRef]
- Campana, L.G.; Farronato, S.; Hodgetts, J.; Odili, J.; Vecchiato, A.; Bracken, A.; Baier, S.; Bechara, F.G.; Borgognoni, L.; Caracò, C.; et al. European E-Delphi Process to Define Expert Consensus on Electrochemotherapy Treatment Indications, Procedural Aspects, and Quality Indicators in Melanoma. Br. J. Surg. 2023, 110, 818–830. [Google Scholar] [CrossRef] [PubMed]
- Neal, R.E.; Rossmeisl, J.H.; Robertson, J.L.; Arena, C.B.; Davis, E.M.; Singh, R.N.; Stallings, J.; Davalos, R.V. Improved Local and Systemic Anti-Tumor Efficacy for Irreversible Electroporation in Immunocompetent versus Immunodeficient Mice. PLoS ONE 2013, 8, e64559. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Li, Z.; Han, X.; Zhu, Z.; Li, Z.; Zhao, Y.; Liu, Z.; Lv, Y. Irreversible Electroporation: An Emerging Immunomodulatory Therapy on Solid Tumors. Front. Immunol. 2022, 12, 811726. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Sun, S.; Zhang, Y.; Xie, F.; Li, S. The Role of Irreversible Electroporation in Promoting M1 Macrophage Polarization via Regulating the HMGB1-RAGE-MAPK Axis in Pancreatic Cancer. Oncoimmunology 2021, 10, 1897295. [Google Scholar] [CrossRef] [PubMed]
- Bigi, L.; Galdo, G.; Cesinaro, A.M.; Vaschieri, C.; Marconi, A.; Pincelli, C.; Fantini, F. Electrochemotherapy Induces Apoptotic Death in Melanoma Metastases: A Histologic and Immunohistochemical Investigation. Clin. Cosmet. Investig. Dermatol. 2016, 9, 451–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zane, K.E.; Cloyd, J.M.; Mumtaz, K.S.; Wadhwa, V.; Makary, M.S. Metastatic Disease to the Liver: Locoregional Therapy Strategies and Outcomes. World J. Clin. Oncol. 2021, 12, 725–745. [Google Scholar] [CrossRef] [PubMed]






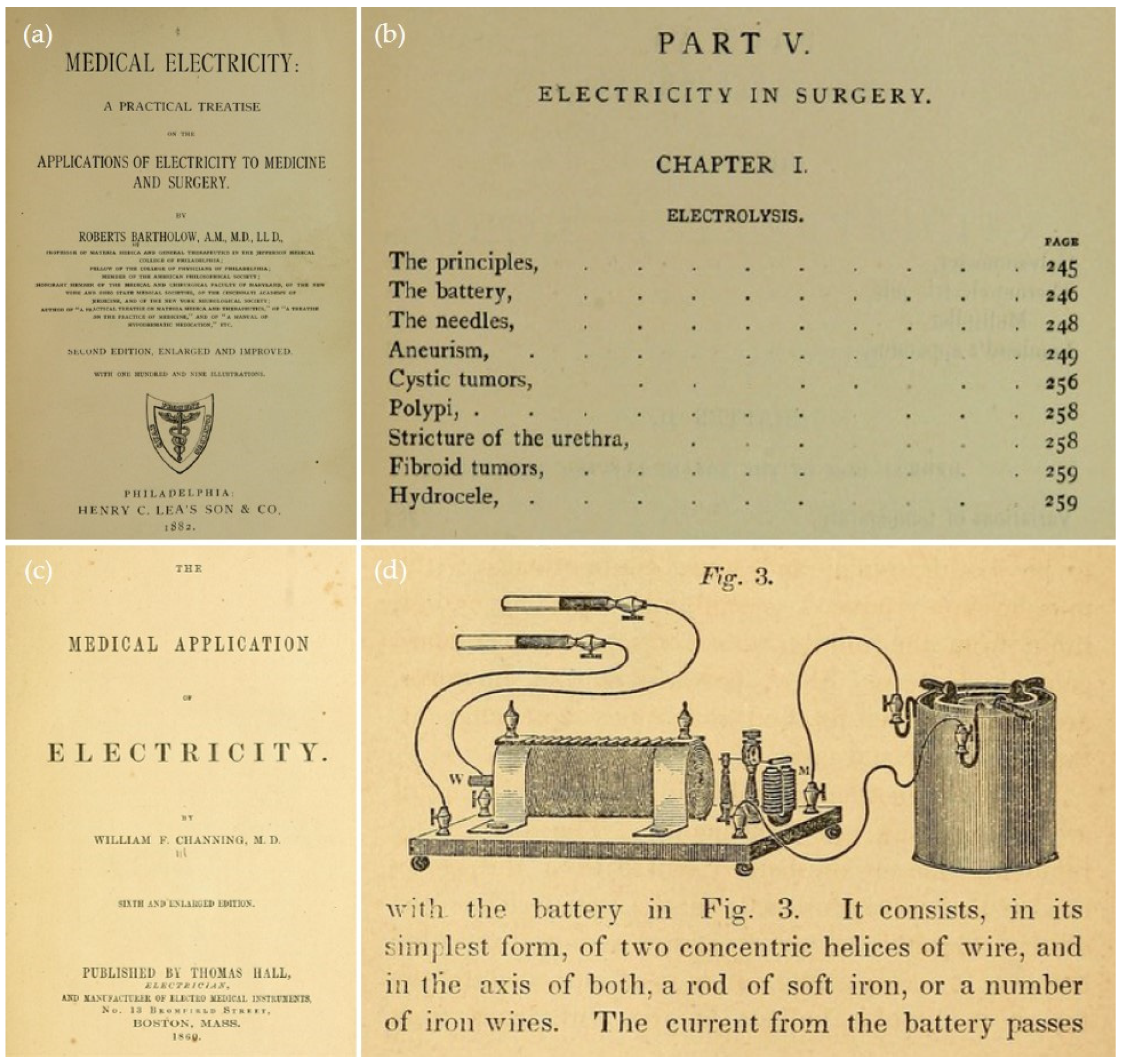{kind=link}
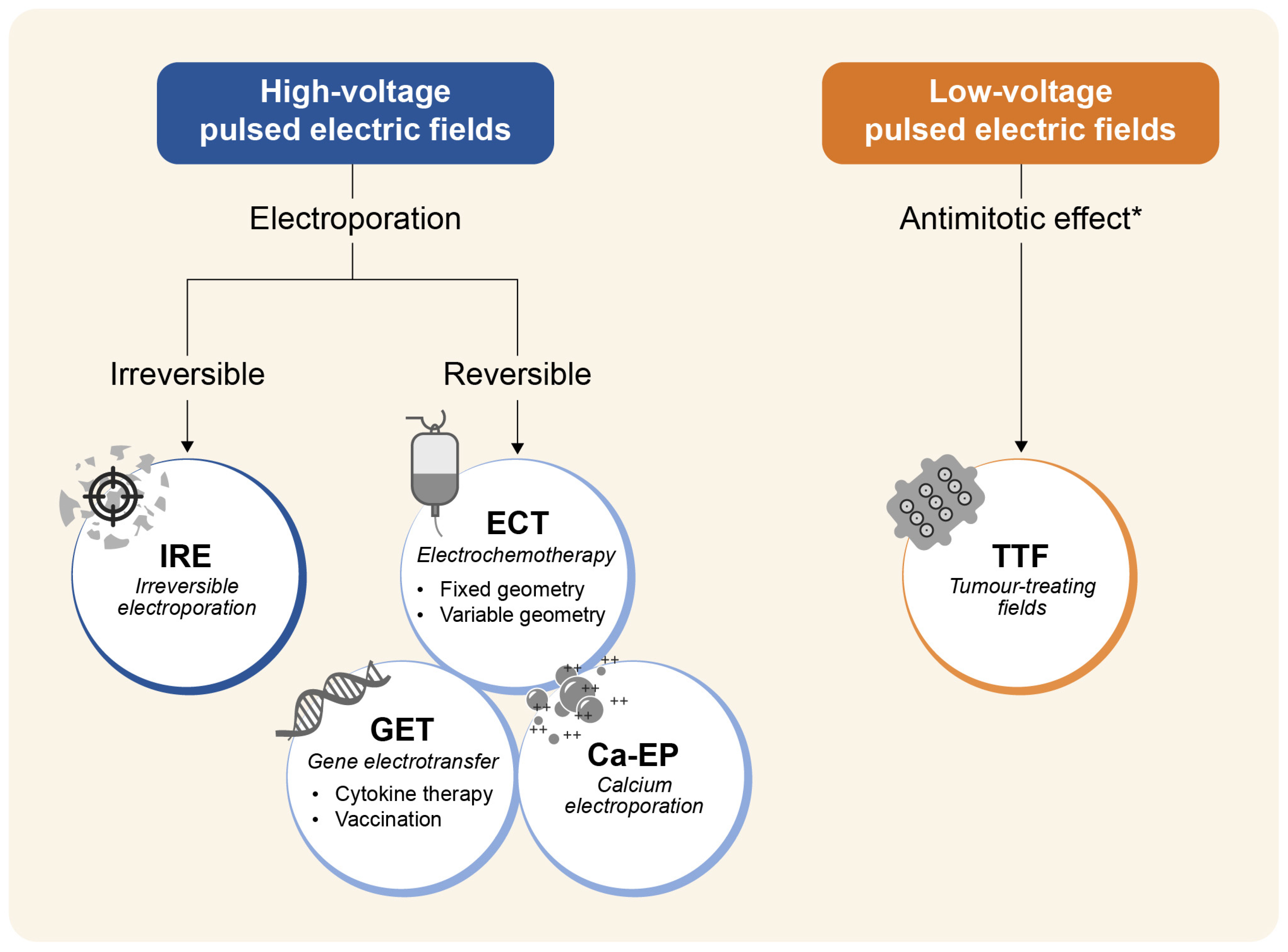{kind=link}
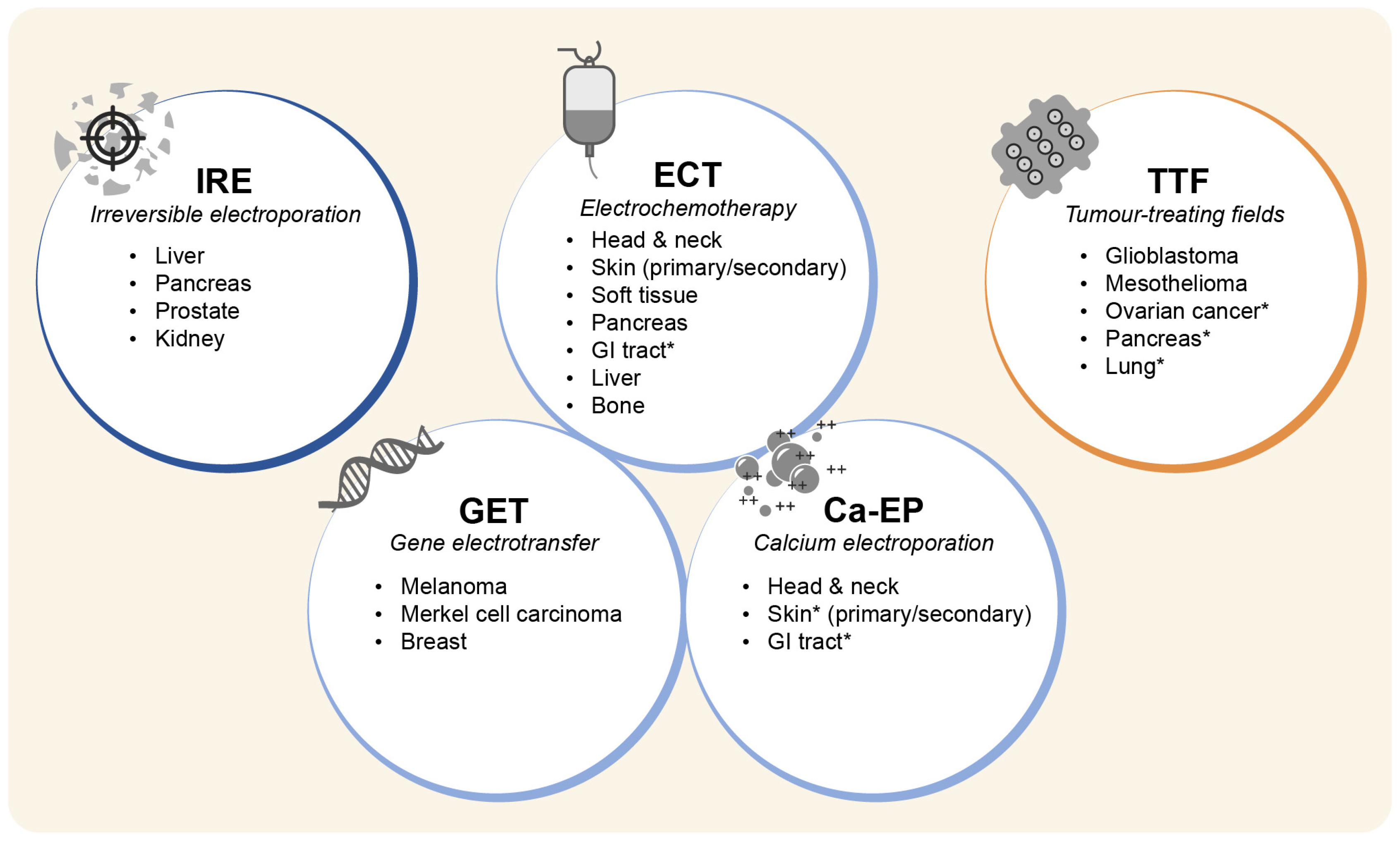{kind=link}
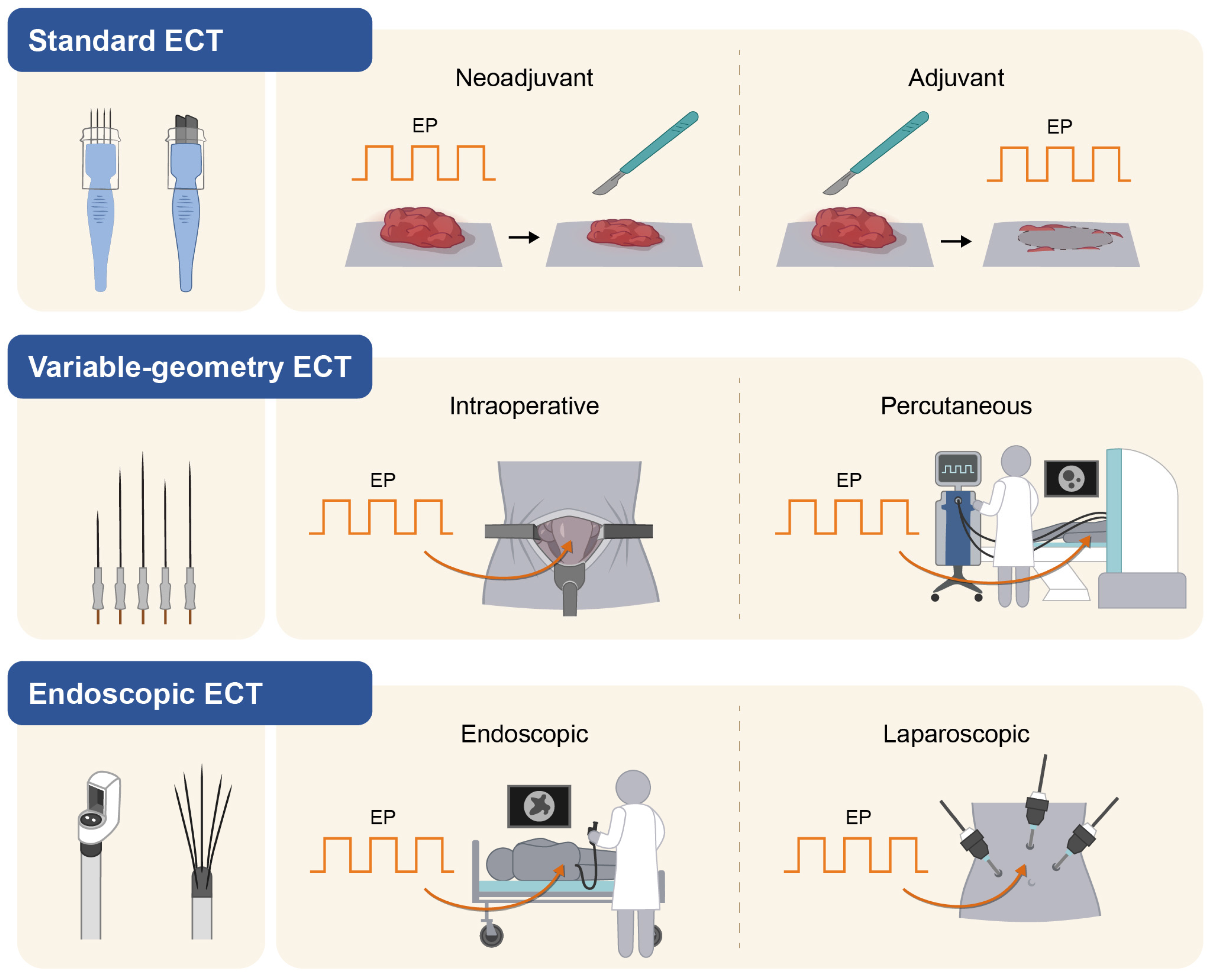{kind=link}
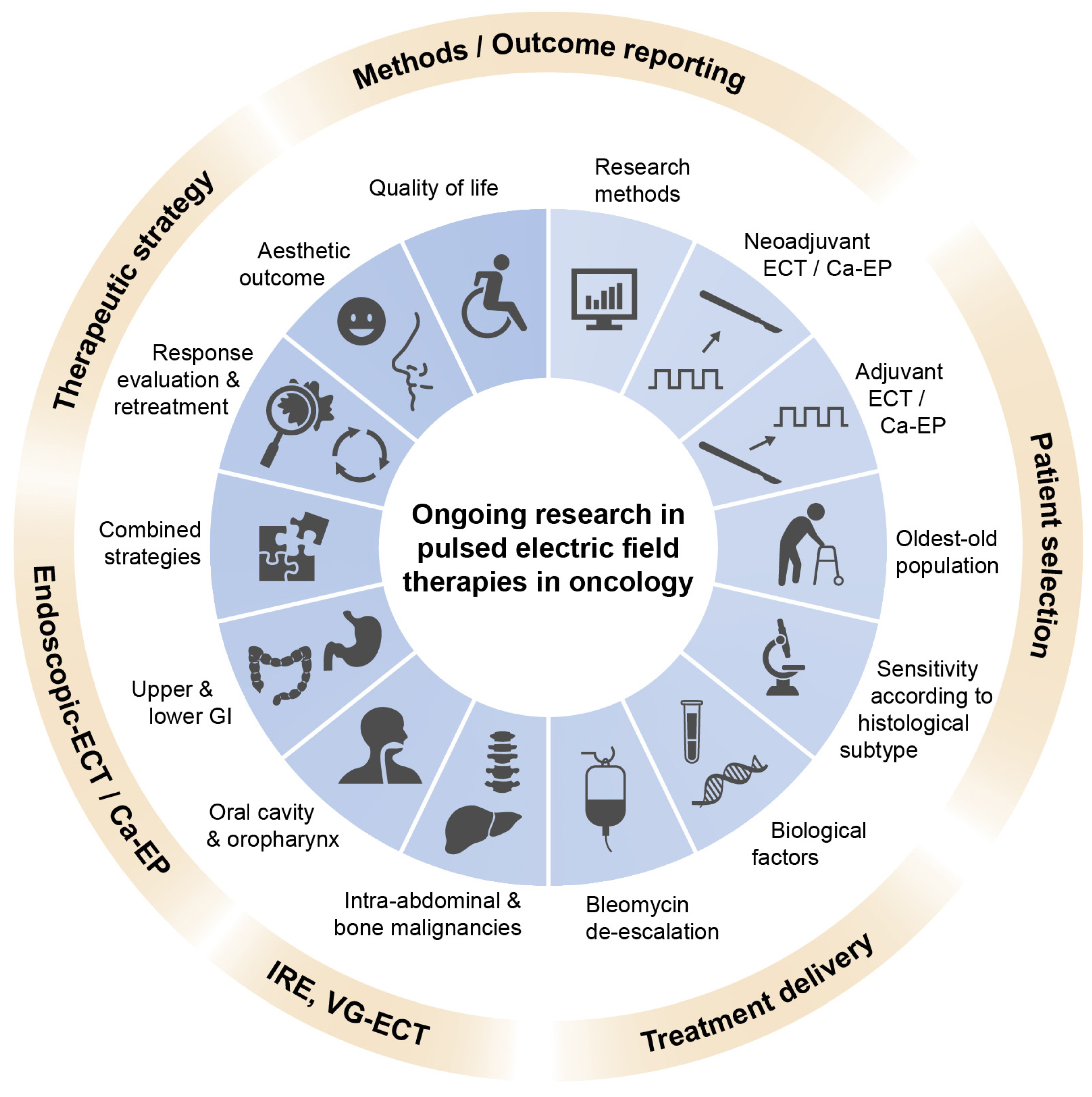{kind=link}
| Tumour | Setting | Study Type | Treatment | Reference |
|---|---|---|---|---|
| HNCSCC 1 | recurrent disease | Phase-2, randomised | ECT vs. cetuximab, CDDP/CBDCA, 5-FU | [209] |
| Rectal cancer | Primary, locally advanced | Phase-2, randomised | Neo-adjuvant Tx 2 → surgery vs. Neo-adjuvant Tx 2 → ECT 3 → surgery | [206] |
| Rectal cancer | Primary, locally advanced | Phase-2, randomised | Neo-adjuvant Tx n.s. → surgery vs. Neo-adjuvant Tx n.s. → ECT 4 → surgery | NCT03040180 |
| Rectal/ sigmoid cancer | Primary, resectable | Phase-2, randomised | ECT → surgery vs. EP alone → surgery | NCT04816045 |
| Gastric cancer | Inoperable | Phase-1 | Bleomycin-ECT | NCT04139070 |
| IRE/H-FIRE | GET | ECT | Ca-EP | TTF | |
|---|---|---|---|---|---|
| Target tumours | Deep-seated | Superficial | Superficial Deep-seated | Superficial Deep-seated | Deep-seated |
| Approved indications | Liver mts | Melanoma | Skin | - | Glioblastoma |
| Liver cancers | Head & neck | - | Mesothelioma | ||
| Pancreas | Bone mts | - | |||
| Prostate | |||||
| Investigational indications | GI cancers | Merkel cell | GI cancers | Skin | Lung |
| Breast | Liver mts | GI cancers | Pancreas | ||
| Liver cancers | Barrett’s | Ovary | |||
| Pancreas | Head neck | ||||
| Keloids | |||||
| Pulse application | Needle electrodes | Needle electrode | Needle/plate electrodes | Needle/plate electrodes | Contact transducer |
| Anaesthesia | Gen | Loc/Sed | Loc/Sed/Gen | Loc/Sed | No |
| Procedure complexity | +++ 1 | +++ 2 | + 3/+++ 4 | + 5 | + 6 |
| Use of CT | no | no | yes | no | no/yes |
| Approval | USA, EU, AUS, Asia | USA | EU, AUS | No | USA, Canada, EU |
| Systemic effect | no | yes | no | Yes/? | yes |
| Specific requirements | Image guidance | Gene therapy licensed facility | Image guidance (only VG-ECT) | No | Patient compliance 6 Image guidance/radiotherapy expertise |
| Costs | ++ | ++/+++ | +/++ | + | +++ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campana, L.G.; Daud, A.; Lancellotti, F.; Arroyo, J.P.; Davalos, R.V.; Di Prata, C.; Gehl, J. Pulsed Electric Fields in Oncology: A Snapshot of Current Clinical Practices and Research Directions from the 4th World Congress of Electroporation. Cancers 2023, 15, 3340. https://doi.org/10.3390/cancers15133340
Campana LG, Daud A, Lancellotti F, Arroyo JP, Davalos RV, Di Prata C, Gehl J. Pulsed Electric Fields in Oncology: A Snapshot of Current Clinical Practices and Research Directions from the 4th World Congress of Electroporation. Cancers. 2023; 15(13):3340. https://doi.org/10.3390/cancers15133340
Chicago/Turabian StyleCampana, Luca G., Adil Daud, Francesco Lancellotti, Julio P. Arroyo, Rafael V. Davalos, Claudia Di Prata, and Julie Gehl. 2023. "Pulsed Electric Fields in Oncology: A Snapshot of Current Clinical Practices and Research Directions from the 4th World Congress of Electroporation" Cancers 15, no. 13: 3340. https://doi.org/10.3390/cancers15133340