
Expression Analysis of hsa-miR-181a-5p, hsa-miR-143-3p, hsa-miR-132-3p and hsa-miR-23a-3p as Biomarkers in Colorectal Cancer—Relationship to the Body Mass Index
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. RNA Extraction and microRNA (miRNA) Expression Analysis
2.3. Statistical Analysis
3. Results
3.1. Differences in miRNA Expression in Serum and Adipose Tissues between Subjects with and without CRC. Relationship to the BMI Values
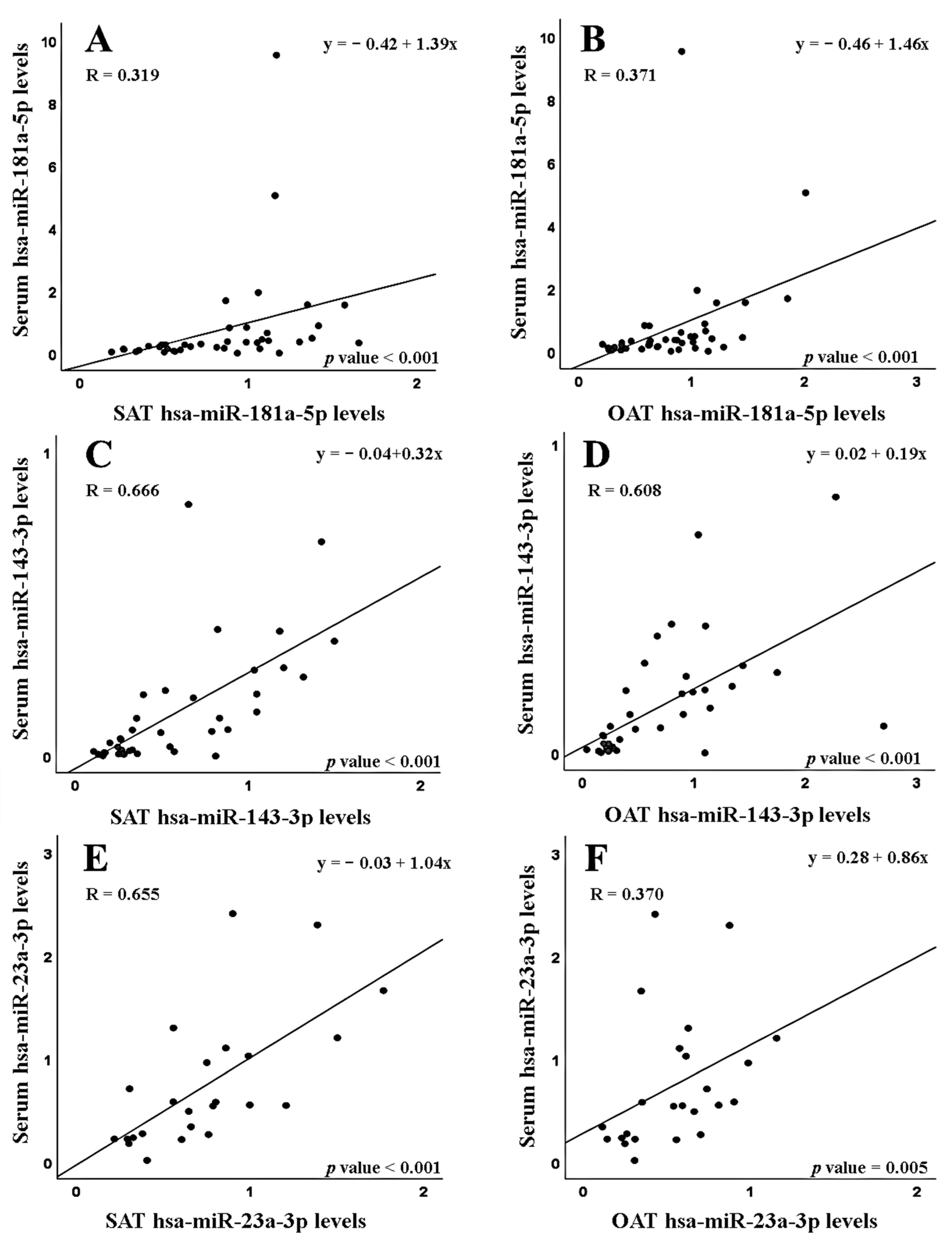
3.2. Correlations between Serum and Adipose Tissue miRNA Expression in Subjects with and without CRC
3.3. miRNA Expression Levels in Tumor and Non-Tumor Tissues from CRC Patients—Differences in Relation to Tumor Location
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Dekker, E.; Tanis, P.J.; Vleugels, J.L.A.; Kasi, P.M.; Wallace, M.B. Colorectal cancer. Lancet 2019, 394, 1467–1480. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, S.E.; Blackburn, O.A.; Marchildon, F.; Cohen, P. Insights into the Link Between Obesity and Cancer. Curr. Obes. Rep. 2017, 6, 195–203. [Google Scholar] [CrossRef]
- Gebert, L.F.R.; MacRae, I.J. Regulation of microRNA function in animals. Nat. Rev. Mol. Cell. Biol. 2019, 1, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Lizarbe, M.A.; Calle-Espinosa, J.; Fernández-Lizarbe, E.; Fernández-Lizarbe, S.; Robles, M.Á.; Olmo, N.; Turnay, J. Colorectal Cancer: From the Genetic Model to Posttranscriptional Regulation by Noncoding RNAs. Biomed. Res. Int. 2017, 2017, 7354260. [Google Scholar] [CrossRef] [Green Version]
- Mazziotta, C.; Cervellera, C.F.; Lanzillotti, C.; Touzé, A.; Gaboriaud, P.; Tognon, M.; Martini, F.; Rotondo, J.C. MicroRNA dysregulations in Merkel cell carcinoma: Molecular mechanisms and clinical applications. J. Med. Virol. 2023, 95, e28375. [Google Scholar] [CrossRef]
- Szczepanek, J. Role of microRNA dysregulation in childhood acute leukemias: Diagnostics, monitoring and therapeutics: A comprehensive review. World J. Clin. Oncol. 2020, 11, 348–369. [Google Scholar] [CrossRef]
- To, K.K.; Tong, C.W.; Wu, M.; Cho, W.C. MicroRNAs in the prognosis and therapy of colorectal cancer: From bench to bedside. World J. Gastroenterol. 2018, 24, 2949–2973. [Google Scholar] [CrossRef]
- Cirillo, F.; Catellani, C.; Sartori, C.; Lazzeroni, P.; Amarri, S.; Street, M.E. Obesity, Insulin Resistance, and Colorectal Cancer: Could miRNA Dysregulation Play A Role? Int. J. Mol. Sci. 2019, 20, 2922. [Google Scholar] [CrossRef] [Green Version]
- Ji, D.; Chen, Z.; Li, M.; Zhan, T.; Yao, Y.; Zhang, Z.; Xi, J.; Yan, L.; Gu, J. MicroRNA-181a promotes tumor growth and liver metastasis in colorectal cancer by targeting the tumor suppressor WIF-1. Mol. Cancer. 2014, 13, 86. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Mi, Y.; Zheng, B.; Wei, P.; Gu, Y.; Zhang, Z.; Xu, Y.; Cai, S.; Li, X.; Li, D. Highly-metastatic colorectal cancer cell released miR-181a-5p-rich extracellular vesicles promote liver metastasis by activating hepatic stellate cells and remodelling the tumour microenvironment. J. Extracell. Vesicles. 2022, 11, e12186. [Google Scholar] [CrossRef]
- Sun, W.; Wang, X.; Li, J.; You, C.; Lu, P.; Feng, H.; Kong, Y.; Zhang, H.; Liu, Y.; Jiao, R.; et al. MicroRNA-181a promotes angiogenesis in colorectal cancer by targeting SRCIN1 to promote the SRC/VEGF signaling pathway. Cell. Death Dis. 2018, 9, 438. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Kim, S.J.; Choo, J.; Heo, G.; Yoo, J.W.; Jung, Y.; Rhee, S.H.; Im, E. miR-23a-3p is a Key Regulator of IL-17C-Induced Tumor Angiogenesis in Colorectal Cancer. Cells 2020, 9, 1363. [Google Scholar] [CrossRef]
- Lozano-Bartolomé, J.; Llauradó, G.; Portero-Otin, M.; Altuna-Coy, A.; Rojo-Martínez, G.; Vendrell, J.; Jorba, R.; Rodríguez-Gallego, E.; Chacón, M.R. Altered Expression of miR-181a-5p and miR-23a-3p Is Associated with Obesity and TNFα-Induced Insulin Resistance. J. Clin. Endocrinol. Metab. 2018, 103, 1447–1458. [Google Scholar] [CrossRef] [Green Version]
- Pidíkova, P.; Reis, R.; Herichova, I. miRNA Clusters with Down-Regulated Expression in Human Colorectal Cancer and Their Regulation. Int. J. Mol. Sci. 2020, 21, 4633. [Google Scholar] [CrossRef]
- Chen, X.; Guo, X.; Zhang, H.; Xiang, Y.; Chen, J.; Yin, Y.; Cai, X.; Wang, K.; Wang, G.; Ba, Y.; et al. Role of miR-143 targeting KRAS in colorectal tumorigenesis. Oncogene 2009, 28, 1385–1392. [Google Scholar] [CrossRef] [Green Version]
- Guo, L.; Fu, J.; Sun, S.; Zhu, M.; Zhang, L.; Niu, H.; Chen, Z.; Zhang, Y.; Guo, L.; Wang, S. MicroRNA-143-3p inhibits colorectal cancer metastases by targeting ITGA6 and ASAP3. Cancer Sci. 2019, 110, 805–816. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.B.; Luo, H.P.; Shi, Q.; Hao, Z.N.; Ding, Y.; Wang, Q.S.; Li, S.B.; Xiao, G.C.; Tong, S.L. miR-132 inhibits colorectal cancer invasion and metastasis via directly targeting ZEB2. World J. Gastroenterol. 2014, 20, 6515–6522. [Google Scholar] [CrossRef]
- Dahlman, I.; Belarbi, Y.; Laurencikiene, J.; Pettersson, A.M.; Arner, P.; Kulyté, A. Comprehensive functional screening of miRNAs involved in fat cell insulin sensitivity among women. Am. J. Physiol. Endocrinol. Metab. 2017, 312, E482–E494. [Google Scholar] [CrossRef] [Green Version]
- Jordan, S.D.; Krüger, M.; Willmes, D.M.; Redemann, N.; Wunderlich, F.T.; Brönneke, H.S.; Merkwirth, C.; Kashkar, H.; Olkkonen, V.M.; Böttger, T.; et al. Obesity-induced overexpression of miRNA-143 inhibits insulin-stimulated AKT activation and impairs glucose metabolism. Nat. Cell. Biol. 2011, 13, 434–446. [Google Scholar] [CrossRef]
- Ardila, H.J.; Sanabria-Salas, M.C.; Meneses, X.; Rios, R.; Huertas-Salgado, A.; Serrano, M.L. Circulating miR-141-3p, miR-143-3p and miR-200c-3p are differentially expressed in colorectal cancer and advanced adenomas. Mol. Clin. Oncol. 2019, 11, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pliakou, E.; Lampropoulou, D.I.; Dovrolis, N.; Chrysikos, D.; Filippou, D.; Papadimitriou, C.; Vezakis, A.; Aravantinos, G.; Gazouli, M. Circulating miRNA Expression Profiles and Machine Learning Models in Association with Response to Irinotecan-Based Treatment in Metastatic Colorectal Cancer. Int. J. Mol. Sci. 2022, 24, 46. [Google Scholar] [CrossRef] [PubMed]
- Qin, D.; Wei, R.; Liu, S.; Zhu, S.; Zhang, S.; Min, L. A Circulating miRNA-Based Scoring System Established by WGCNA to Predict Colon Cancer. Anal. Cell. Pathol. 2019, 2019, 1571045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Høye, E.; Fromm, B.; Böttger, P.H.M.; Domanska, D.; Torgunrud, A.; Lund-Andersen, C.; Abrahamsen, T.W.; Fretland, A.A.; Dagenborg, V.J.; Lorenz, S.; et al. A comprehensive framework for analysis of microRNA sequencing data in metastatic colorectal cancer. NAR Cancer. 2022, 4, zcab051. [Google Scholar] [CrossRef] [PubMed]
- Elias, K.M.; Fendler, W.; Stawiski, K.; Fiascone, S.J.; Vitonis, A.F.; Berkowitz, R.S.; Frendl, G.; Konstantinopoulos, P.; Crum, C.P.; Kedzierska, M.; et al. Diagnostic potential for a serum miRNA neural network for detection of ovarian cancer. Elife 2017, 6, e28932. [Google Scholar] [CrossRef] [PubMed]
- Neville, M.J.; Collins, J.M.; Gloyn, A.L.; McCarthy, M.I.; Karpe, F. Comprehensive human adipose tissue mRNA and microRNA endogenous control selection for quantitative real-time-PCR normalization. Obesity (Silver Spring) 2011, 19, 888–892. [Google Scholar] [CrossRef]
- Klöting, N.; Berthold, S.; Kovacs, P.; Schön, M.R.; Fasshauer, M.; Ruschke, K.; Stumvoll, M.; Blüher, M. MicroRNA expression in human omental and subcutaneous adipose tissue. PLoS ONE 2009, 4, e4699. [Google Scholar] [CrossRef] [Green Version]
- Heneghan, H.M.; Miller, N.; McAnena, O.J.; O’Brien, T.; Kerin, M.J. Differential miRNA expression in omental adipose tissue and in the circulation of obese patients identifies novel metabolic biomarkers. J. Clin. Endocrinol. Metab. 2011, 96, E846–E850. [Google Scholar] [CrossRef] [Green Version]
- Landrier, J.F.; Derghal, A.; Mounien, L. MicroRNAs in Obesity and Related Metabolic Disorders. Cells 2019, 8, 859. [Google Scholar] [CrossRef] [Green Version]
- Wei, Z.; Cui, L.; Mei, Z.; Liu, M.; Zhang, D. miR-181a mediates metabolic shift in colon cancer cells via the PTEN/AKT pathway. FEBS Lett. 2014, 588, 1773–1779. [Google Scholar] [CrossRef]
- Ayers, D.; Boughanem, H.; Macías-González, M. Epigenetic Influences in the Obesity/Colorectal Cancer Axis: A Novel Theragnostic Avenue. J. Oncol. 2019, 2019, 7406078. [Google Scholar] [CrossRef] [Green Version]
- Thomou, T.; Mori, M.A.; Dreyfuss, J.M.; Konishi, M.; Sakaguchi, M.; Wolfrum, C.; Rao, T.N.; Winnay, J.N.; Garcia-Martin, R.; Grinspoon, S.K.; et al. Adipose-derived circulating miRNAs regulate gene expression in other tissues. Nature 2017, 542, 450–455. [Google Scholar] [CrossRef] [Green Version]
- Hwang, I.; Kim, J.B. Two Faces of White Adipose Tissue with Heterogeneous Adipogenic Progenitors. Diabetes Metab. J. 2019, 43, 752–762. [Google Scholar] [CrossRef]
- Haffa, M.; Holowatyj, A.N.; Kratz, M.; Toth, R.; Benner, A.; Gigic, B.; Habermann, N.; Schrotz-King, P.; Böhm, J.; Brenner, H.; et al. Transcriptome Profiling of Adipose Tissue Reveals Depot-Specific Metabolic Alterations Among Patients with Colorectal Cancer. J. Clin. Endocrinol. Metab. 2019, 104, 5225–5237. [Google Scholar] [CrossRef]
- Klimcáková, E.; Roussel, B.; Márquez-Quiñones, A.; Kovácová, Z.; Kováciková, M.; Combes, M.; Siklová-Vítková, M.; Hejnová, J.; Srámková, P.; Bouloumié, A.; et al. Worsening of obesity and metabolic status yields similar molecular adaptations in human subcutaneous and visceral adipose tissue: Decreased metabolism and increased immune response. J. Clin. Endocrinol. Metab. 2011, 96, E73–E82. [Google Scholar] [CrossRef] [Green Version]
- Ji, C.; Guo, X. The clinical potential of circulating microRNAs in obesity. Nat. Rev. Endocrinol. 2019, 12, 731–743. [Google Scholar] [CrossRef]
- Hata, A.; Kashima, R. Dysregulation of microRNA biogenesis machinery in cancer. Crit. Rev. Biochem. Mol. Biol. 2016, 51, 121–134. [Google Scholar] [CrossRef]
- Ak, S.; Tunca, B.; Tezcan, G.; Cecener, G.; Egeli, U.; Yilmazlar, T.; Ozturk, E.; Yerci, O. MicroRNA expression patterns of tumors in early-onset colorectal cancer patients. J. Surg. Res. 2014, 191, 113–122. [Google Scholar] [CrossRef]
- Huang, R.; Xiang, G.; Duan, X.; Wang, H.; He, K.; Xiao, J. MiR-132-3p inhibits proliferation, invasion and migration of colorectal cancer cells via down-regulating FOXP2 expression. Acta Biochim. Pol. 2022, 69, 371–377. [Google Scholar] [CrossRef]
- Yong, C.; Xiao-lu, H.; Xiao-xiang, Y.; Yun, Z.; Tao, W. Decreased expression of miR-132 in CRC tissues and its inhibitory function on tumor progression. Open. Life Sci. 2016, 11, 130–135. [Google Scholar] [CrossRef]
- Moreno, E.C.; Pascual, A.; Prieto-Cuadra, D.; Laza, V.F.; Molina-Cerrillo, J.; Ramos-Muñoz, M.E.; Rodríguez-Serrano, E.M.; Soto, J.L.; Carrato, A.; García-Bermejo, M.L.; et al. Novel Molecular Characterization of Colorectal Primary Tumors Based on miRNAs. Cancers 2019, 11, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Li, L.; Ma, J.; Yang, S.; Zou, C.; Yu, X. miRNA and mRNA Integration Network Construction Reveals Novel Key Regulators in Left-Sided and Right-Sided Colon Adenocarcinoma. Biomed. Res. Int. 2019, 2019, 7149296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mjelle, R.; Sjursen, W.; Thommesen, L.; Sætrom, P.; Hofsli, E. Small RNA expression from viruses, bacteria and human miRNAs in colon cancer tissue and its association with microsatellite instability and tumor location. BMC Cancer 2019, 19, 161. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.L.; Herrick, J.S.; Pellatt, D.F.; Mullany, L.E.; Stevens, J.R.; Wolff, E.; Hoffman, M.D.; Wolff, R.K.; Samowitz, W. Site-specific associations between miRNA expression and survival in colorectal cancer cases. Oncotarget 2016, 7, 60193–60205. [Google Scholar] [CrossRef] [Green Version]
- Dumas, J.F.; Brisson, L. Interaction between adipose tissue and cancer cells: Role for cancer progression. Cancer Metastasis Rev. 2021, 40, 31–46. [Google Scholar] [CrossRef]
- Di Franco, S.; Bianca, P.; Sardina, D.S.; Turdo, A.; Gaggianesi, M.; Veschi, V.; Nicotra, A.; Mangiapane, L.R.; Lo Iacono, M.; Pillitteri, I.; et al. Adipose stem cell niche reprograms the colorectal cancer stem cell metastatic machinery. Nat. Commun. 2021, 12, 5006. [Google Scholar] [CrossRef]
- Liu, Y.; Tan, J.; Ou, S.; Chen, J.; Chen, L. Adipose-derived exosomes deliver miR-23a/b to regulate tumor growth in hepatocellular cancer by targeting the VHL/HIF axis. J. Physiol. Biochem. 2019, 75, 391–401. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | CRC * Group (N = 43 Patients) | Control Group (N = 22 Patients) | p Value |
|---|---|---|---|
| Mean age (years) ± standard error | 71.65 ± 1.91 | 55.50 ± 2.87 | <0.001 1 |
| Gender, N (%) | 0.017 2 | ||
| Male | 29 (67.44) | 8 (36.36) | |
| Female | 14 (32.56) | 14 (63.64) | |
| BMI ≠ group, N (value, mean ± standard error) | 0.613 2 | ||
| Normal weight (BMI ≠ ≤ 24.9 Kg/m2) | 8 (23.02 ± 0.62) | 3 (23.55 ± 0.53) | |
| Overweight/Obesity (BMI ≠ ≥ 25 kg/m2) | 35 (27.72 ± 0.52) | 19 (37.89 ± 1.78) | |
| Tumor location, N (%) | |||
| Right colon | 23 (53.49) | - | |
| Left colon | 13 (30.23) | - | |
| Rectum | 7 (16.28) | - | |
| TNM stage, N (%) | |||
| I | 6 (13.95) | - | |
| II | 16 (37.21) | - | |
| III | 18 (41.86) | - | |
| IV | 3 (6.98) | - |
| Mean Relative miRNA Expression (2−∆∆Ct) ± Standard Error | |||
|---|---|---|---|
| miRNA Samples | CRC 3 | Controls | p Value 4 |
| hsa-miR-181a-5p | |||
| Serum | 0.23 ± 0.059 | 0.25 ± 0.037 | 0.128 |
| SAT 1 | 0.66 ± 0.073 | 0.84 ± 0.164 | 0.365 |
| OAT 2 | 0.63 ± 0.067 | 1.25 ± 0.232 | <0.001 |
| hsa-miR-143-3p | |||
| Serum | 0.04 ± 0.009 | 0.02 ± 0.003 | 0.380 |
| SAT 1 | 0.29 ± 0.025 | 0.39 ± 0.110 | 0.840 |
| OAT 2 | 0.24 ± 0.019 | 0.46 ± 0.105 | 0.031 |
| hsa-miR-132-3p | |||
| Serum | 0.18 ± 0.031 | 0.18 ± 0.078 | 0.482 |
| SAT 1 | 0.18 ± 0.018 | 0.44 ± 0.139 | 0.005 |
| OAT 2 | 0.22 ± 0.023 | 0.49 ± 0.165 | 0.119 |
| hsa-miR-23a-3p | |||
| Serum | 0.74 ± 0.126 | 1.21 ± 0.453 | 0.242 |
| SAT 1 | 0.75 ± 0.083 | 1.99 ± 0.824 | 0.044 |
| OAT 2 | 0.54 ± 0.057 | 1.42 ± 0.353 | <0.001 |
| Mean Relative miRNA Expression (2−∆∆Ct) ± Standard Error | ||||||
|---|---|---|---|---|---|---|
| Normal Weight | p Value 4,5 | Overweight/Obese | p Value 4,5 | |||
| miRNA Samples | CRC 3 | Control | CRC 3 | Control | ||
| hsa-miR-181a-5p | ||||||
| Serum | 0.08 ± 0.028 | 0.29 ± 0.041 | 0.008 4 | 0.26 ± 0.068 | 0.24 ± 0.046 | 0.677 5 |
| SAT 1 | 0.63 ± 0.078 | 0.70 ± 0.097 | 0.602 4 | 0.67 ± 0.087 | 0.87 ± 0.197 | 0.403 5 |
| OAT 2 | 0.73 ± 0.161 | 0.86 ± 0.157 | 0.640 4 | 0.61 ± 0.075 | 1.33 ± 0.272 | <0.001 5 |
| hsa-miR-143-3p | ||||||
| Serum | 0.01 ± 0.004 | 0.03 ± 0.010 | 0.117 4 | 0.04 ± 0.011 | 0.01 ± 0.002 | 0.071 5 |
| SAT 1 | 0.25 ± 0.056 | 0.36 ± 0.102 | 0.340 4 | 0.29 ± 0.028 | 0.40 ± 0.132 | 0.538 5 |
| OAT 2 | 0.23 ± 0.029 | 0.30 ± 0.088 | 0.371 4 | 0.25 ± 0.022 | 0.49 ± 0.122 | 0.032 5 |
| hsa-miR-132-3p | ||||||
| Serum | 0.08 ± 0.025 | 0.46 ± 0.361 | 0.289 5 | 0.20 ± 0.036 | 0.10 ± 0.013 | 0.137 5 |
| SAT 1 | 0.15 ± 0.031 | 0.22 ± 0.072 | 0.315 4 | 0.18 ± 0.021 | 0.48 ± 0.164 | 0.008 5 |
| OAT 2 | 0.21 ± 0.013 | 0.15 ± 0.025 | 0.054 4 | 0.22 ± 0.028 | 0.55 ± 0.190 | 0.043 5 |
| hsa-miR-23a-3p | ||||||
| Serum | 0.26 ± 0.111 | 3.10 ± 1.921 | 0.034 5 | 0.83 ± 0.141 | 0.70 ± 0.119 | 0.921 5 |
| SAT 1 | 0.50 ± 0.171 | 1.09 ± 0.024 | 0.086 4 | 0.80 ± 0.091 | 2.17 ± 0.987 | 0.187 5 |
| OAT 2 | 0.42 ± 0.130 | 0.79 ± 0.075 | 0.141 4 | 0.57 ± 0.063 | 1.54 ± 0.410 | 0.002 5 |
| Serum Mean Relative miRNA Expression (2−∆∆Ct) ± Standard Error | |||
|---|---|---|---|
| miRNA | Normal Weight CRC 1 Patients | Overweight/obese CRC 1 Patients | p Value 2 |
| hsa-miR-181a-5p | 0.08 ± 0.028 | 0.26 ± 0.068 | 0.045 |
| hsa-miR-143-3p | 0.01 ± 0.004 | 0.04 ± 0.011 | 0.054 |
| hsa-miR-132-3p | 0.08 ± 0.025 | 0.20 ± 0.036 | 0.088 |
| hsa-miR-23a-3p | 0.26 ± 0.111 | 0.83 ± 0.141 | 0.054 |
| Serum Mean (and Median) Relative miRNA Expression (2−∆∆Ct) ± Standard Error | |||
|---|---|---|---|
| miRNA | Normal Weight Controls | Overweight/Obese Controls | p Value 1 |
| hsa-miR-181a-5p | 0.29 ± 0.041 (0.252) | 0.24 ± 0.046 (0.175) | 0.073 |
| hsa-miR-143-3p | 0.03 ± 0.010 (0.017) | 0.01 ± 0.002 (0.013) | 0.052 |
| hsa-miR-132-3p | 0.46 ± 0.361 (0.117) | 0.10 ± 0.013 (0.089) | 0.243 |
| hsa-miR-23a-3p | 3.10 ± 1.921 (1.820) | 0.70 ± 0.119 (0.571) | 0.073 |
| Serum–Adipose Tissue Correlations in miRNA Levels Correlation Coefficients (p Values) | ||||||||
|---|---|---|---|---|---|---|---|---|
| hsa-miR-181a-5p | hsa-miR-143-3p | hsa-miR-132-3p | hsa-miR-23a-3p | |||||
| BMI 1 Group | S 2—SAT 3 | S 2—OAT 4 | S 2—SAT 3 | S 2—OAT 4 | S 2—SAT 3 | S 2—OAT 4 | S 2—SAT 3 | S 2—OAT 4 |
| Normal weight | 0.619 5 (0.102 5) | 0.190 5 (0.651 5) | 0.881 5 (0.004 5) | 0.762 5 (0.028 5) | 0.714 5 (0.047 5) | 0.717 6 (0.045 6) | 0.782 6 (0.218 6) | 0.400 5 (0.600 5) |
| Overweight/ Obese | 0.646 5 (<0.001 5) | 0.665 5 (<0.001 5) | 0.708 5 (<0.001 5) | 0.740 5 (<0.001 5) | −0.097 5 (0.599 5) | −0.192 5 (0.277 5) | 0.657 5 (0.002 5) | 0.430 5 (0.058 5) |
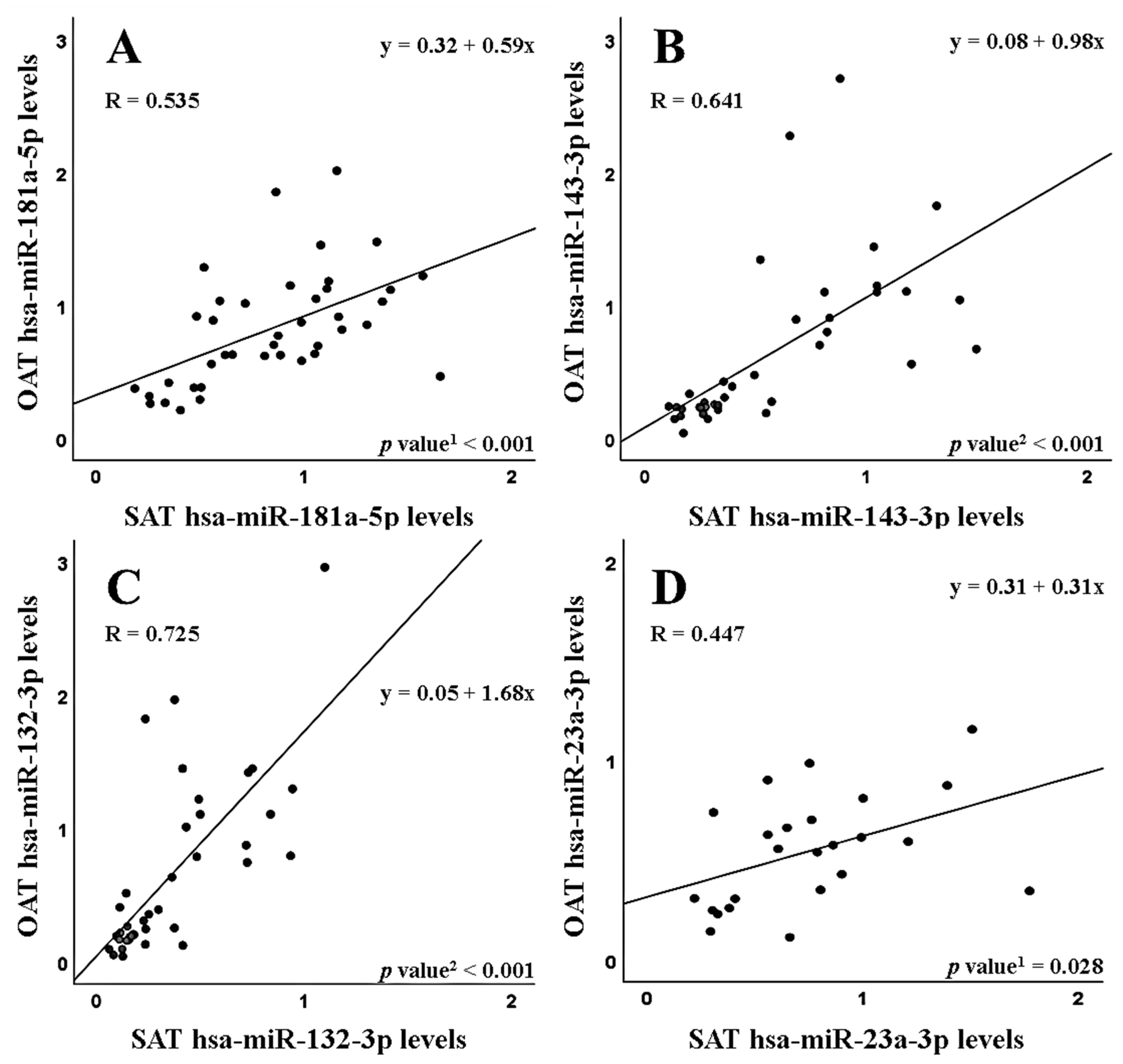
| SAT 1–OAT 2 Correlations in miRNA Expression Correlation Coefficients (p Values) | ||||
|---|---|---|---|---|
| BMI 3 Group | hsa-miR-181a-5p | hsa-miR-143-3p | hsa-miR-132-3p | hsa-miR-23a-3p |
| Normal weight | 0.636 4 (0.090 4) | 0.881 5 (0.004 5) | 0.833 5 (0.010 5) | 0.400 5 (0.600 5) |
| Overweight/Obese | 0.560 4 (<0.001 4) | 0.792 5 (<0.001 5) | 0.755 5 (<0.001 5) | 0.350 4 (0.131 4) |
| Mean Relative miRNA Expression (2−∆∆Ct) ± Standard Error | |||
|---|---|---|---|
| miRNA | Tumor Tissue | Non-Tumor Tissue | p Value 1 |
| hsa-miR-181a-5p | 1.02 ± 0.092 | 1.26 ± 0.137 | 0.278 |
| hsa-miR-143-3p | 0.59 ± 0.152 | 2.30 ± 0.456 | <0.001 |
| hsa-miR-132-3p | 0.97 ± 0.124 | 1.38 ± 0.164 | 0.031 |
| hsa-miR-23a-3p | 1.17 ± 0.221 | 1.46 ± 0.176 | 0.021 |
| Mean Relative miRNA Expression (2−∆∆Ct) ± Standard Error | |||
|---|---|---|---|
| miRNA Samples | Tumors from the Right Colon | Tumors from the Left Colon | p Value 4,5 |
| hsa-miR-181a-5p | |||
| Tumor tissue | 0.88 ± 0.136 | 1.30 ± 0.242 | 0.119 4 |
| Non-tumor tissue | 1.61 ± 0.192 | 0.96 ± 0.210 | 0.044 4 |
| T/N 1 | 0.58 ± 0.076 | 1.64 ± 0.331 | 0.002 5 |
| Serum | 0.19 ± 0.034 | 0.16 ± 0.032 | 0.536 4 |
| SAT 2 | 0.78 ± 0.124 | 0.53 ± 0.063 | 0.133 4 |
| OAT 3 | 0.66 ± 0.097 | 0.58 ± 0.093 | 0.591 4 |
| hsa-miR-143-3p | |||
| Tumor tissue | 0.48 ± 0.244 | 0.67 ± 0.320 | 0.673 5 |
| Non-tumor tissue | 2.51 ± 0.948 | 2.46 ± 1.118 | 0.800 5 |
| T/N 1 | 2.36 ± 2.233 | 2.46 ± 2.045 | 0.735 5 |
| Serum | 0.05 ± 0.017 | 0.01 ± 0.002 | 0.105 5 |
| SAT 2 | 0.33 ± 0.042 | 0.23 ± 0.029 | 0.100 4 |
| OAT 3 | 0.27 ± 0.026 | 0.21 ± 0.026 | 0.161 4 |
| hsa-miR-132-3p | |||
| Tumor tissue | 0.98 ± 0.285 | 0.94 ± 0.277 | 0.800 5 |
| Non-tumor tissue | 1.81 ± 0.350 | 0.79 ± 0.139 | 0.028 5 |
| T/N 1 | 1.20 ± 0.749 | 1.57 ± 0.731 | 0.272 5 |
| Serum | 0.21 ± 0.043 | 0.16 ± 0.071 | 0.247 5 |
| SAT 2 | 0.22 ± 0.034 | 0.13 ± 0.008 | 0.083 5 |
| OAT 3 | 0.26 ± 0.037 | 0.18 ± 0.038 | 0.133 4 |
| hsa-miR-23a-3p | |||
| Tumor tissue | 1.38 ± 0.387 | 0.83 ± 0.160 | 0.398 5 |
| Non-tumor tissue | 1.85 ± 0.249 | 0.89 ± 0.189 | 0.016 4 |
| T/N 1 | 0.87 ± 0.316 | 1.36 ± 0.578 | 0.205 5 |
| Serum | 0.92 ± 0.175 | 0.47 ± 0.134 | 0.054 5 |
| SAT 2 | 1.01 ± 0.127 | 0.44 ± 0.071 | 0.003 4 |
| OAT 3 | 0.71 ± 0.079 | 0.38 ± 0.079 | 0.011 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tesolato, S.E.; González-Gamo, D.; Barabash, A.; Claver, P.; de la Serna, S.C.; Domínguez-Serrano, I.; Dziakova, J.; de Juan, C.; Torres, A.J.; Iniesta, P. Expression Analysis of hsa-miR-181a-5p, hsa-miR-143-3p, hsa-miR-132-3p and hsa-miR-23a-3p as Biomarkers in Colorectal Cancer—Relationship to the Body Mass Index. Cancers 2023, 15, 3324. https://doi.org/10.3390/cancers15133324
Tesolato SE, González-Gamo D, Barabash A, Claver P, de la Serna SC, Domínguez-Serrano I, Dziakova J, de Juan C, Torres AJ, Iniesta P. Expression Analysis of hsa-miR-181a-5p, hsa-miR-143-3p, hsa-miR-132-3p and hsa-miR-23a-3p as Biomarkers in Colorectal Cancer—Relationship to the Body Mass Index. Cancers. 2023; 15(13):3324. https://doi.org/10.3390/cancers15133324
Chicago/Turabian StyleTesolato, Sofía Elena, Daniel González-Gamo, Ana Barabash, Paula Claver, Sofía Cristina de la Serna, Inmaculada Domínguez-Serrano, Jana Dziakova, Carmen de Juan, Antonio José Torres, and Pilar Iniesta. 2023. "Expression Analysis of hsa-miR-181a-5p, hsa-miR-143-3p, hsa-miR-132-3p and hsa-miR-23a-3p as Biomarkers in Colorectal Cancer—Relationship to the Body Mass Index" Cancers 15, no. 13: 3324. https://doi.org/10.3390/cancers15133324