
Circulating Tumor DNA in Head and Neck Squamous Cell Carcinoma
by
 , , and
, , and
Anna Brandt
1,
Benjamin Thiele
2,
Christoph Schultheiß
3,
Eveline Daetwyler
4 and
Mascha Binder
3,4,* 1
Department of Internal Medicine 5, Hematology and Oncology, University Hospital of Erlangen, 91054 Erlangen, Germany
2
Department of Oncology, Hematology and Bone Marrow Transplantation with Section of Pneumology, University Medical Center Hamburg-Eppendorf, 20251 Hamburg, Germany
3
Internal Medicine IV, Oncology/Hematology, Martin-Luther-University Halle-Wittenberg, Ernst-Grube-Straße 40, 06120 Halle (Saale), Germany
4
Division of Medical Oncology, University Hospital Basel, 4031 Basel, Switzerland
*
Author to whom correspondence should be addressed.
Cancers 2023, 15(7), 2051; https://doi.org/10.3390/cancers15072051
Submission received: 1 March 2023
/
Revised: 21 March 2023
/
Accepted: 28 March 2023
/
Published: 30 March 2023
(This article belongs to the Special Issue The Biomarkers and Detection of Head and Neck Cancer)
Abstract
:Simple Summary
Head and Neck Squamous Cell Carcinomas (HNSCCs) are cancers that originate from cells of the head and neck region, including the mouth, nose, and throat. The diversity of these cell types is also mirrored by the high number of different mutations that promote cancer development and progression. For the clinical management of this disease, it is important to identify biomarkers that allow early detection or predict relapse and resistance to therapy. A non-invasive way to monitor these markers over time are so called liquid biopsies, which mostly refers to the detection and analysis of tumor cells or cell-free DNA (cfDNA) in the blood of patients. This review summarizes our current understanding of HNSCC genetics and discusses how the detection of genetic variation in the cfDNA of HNSCC patients can be used to monitor disease and guide therapy.
Abstract
Tumors shed cell-free DNA (cfDNA) into the plasma. “Liquid biopsies” are a diagnostic test to analyze cfDNA in order to detect minimal residual cancer, profile the genomic tumor landscape, and monitor cancers non-invasively over time. This technique may be useful in patients with head and neck squamous cell carcinoma (HNSCC) due to genetic tumor heterogeneity and limitations in imaging sensitivity. However, there are technical challenges that need to be overcome for the widespread use of liquid biopsy in the clinical management of these patients. In this review, we discuss our current understanding of HNSCC genetics and the role of cfDNA genomic analyses as an emerging precision diagnostic tool.
1. Introduction
Head and neck squamous cell carcinoma (HNSCC) is a type of cancer that affects the epithelial cells that line regions of the head and neck, including the mouth, nose, and throat (Figure 1) [1,2,3,4]. HNSCC is the seventh most common cancer worldwide, accounting for 3% of all new cancers and for 1.5% of all cancer deaths according to global cancer statistics (GLOBOCAN) [5]. Risk factors for HNSCC include tobacco and alcohol use, viral infections (human papillomavirus [HPV], Epstein-Barr virus [EBV]), poor oral hygiene, exposure to certain chemicals as well as some genetic syndromes, such as Fanconi anemia [1,2,3,4,6]. The majority of patients are diagnosed with locoregional disease, without evidence of metastatic spread, which is either amenable to surgery or chemoradiation (CRT) [1,4,7]. In patients with intermediate to high-risk resectable tumors, adjuvant treatment, consisting of radiotherapy or CRT, is used to reduce the risk of recurrence and to improve outcomes [1,8,9,10]. Despite advances in treatment, including adapting the chemotherapy and radiotherapy protocol, the recurrence rate remains high. Disease recurrence or development of metastases is reported in 50–60% of patients [4]. Whereby, many HNSCC relapses are locoregional and if detected early, can still be treated successfully [11,12,13]. Therefore, early relapse detection is a priority in the management of HNSCC, and efforts should be made to improve surveillance and monitoring strategies to detect recurrence as soon as possible. At present, these strategies involve regular imaging, clinical examinations, and biopsy.
The identification of non-invasive, blood or saliva-based biomarkers to detect HNSCC relapse would be a significant advance in the management of this disease. Cell-free deoxyribonucleic acid (cfDNA), is a promising candidate for such a biomarker, as it has been shown to reflect the presence of residual tumor cells and may be able to predict imminent relapse in different solid tumor settings [14,15]. The measurement of cfDNA through liquid biopsy is a minimally invasive and efficient approach that can be performed repeatedly, allowing for the frequent monitoring of disease progression [16,17]. The use of liquid biopsy for HNSCC may help to provide guidance for the intensity of clinical and radiological surveillance and allow for early detection and treatment of recurrent disease [18,19].
In this review, we discuss our current understanding of HNSCC genetics and the potential role of cfDNA genomic analyses as an emerging precision diagnostic tool in the management of these patients.
2. Genetics of HNSCC
2.1. Genetic Alterations in HNSCC
Despite originating from a variety of different tissues in the upper aerodigestive tract, HNSCC cells display recurrent patterns of structural genome aberrations and acquired somatic mutations [20,21,22,23,24,25,26,27,28,29,30,31,32]. Prominent copy number variations (CNVs) include loss of 3p, 8p 9p and 17p and amplification of 3q, 5p, 8q and 11q13 [20,22,33]. The substantial instability of HNSCC genomes is also illustrated by the mean size (6.7 megabases) and mean number of CNVs which ranges between 141 and 433 per sample [20,22]. While some CNVs are shared across HNSCC (e.g., focal amplification of 3q26/28 encompassing TP63, SOX2 and PIK3CA, or amplification of 11q13 regions encompassing FADD and PPFIA1), distinct CNV patterns reflect the HPV-associated dichotomization of HNSCC entities (Figure 1) [20,22,23]. For example, HPV+ tumors often display amplification of the genomic regions 20q11 (E2F1), 12p13 (LAG3, TNFRSF1) and 3q27/28 (ATR, BCL6, PSMD2, MAP3K13, ALG3, IGF2BP2), while HPV- HNSCC cells are enriched for amplifications of 7p11 (EGFR), 8p11 (FGFR1), 17q12 (ERBB2, CDK12), 5p15 (TERT), 9p24 (JAK2, CD274), 15q26 (ALDH1A3, IGF1R) and the coamplification of 11q13 (CCND1) and 11q22 (BIRC2, YAP1) [20,21,22,23,24]. In addition, HPV+ HNSCCs display deletion of regions at 11q23.3 (BIRC2, BIRC3, ATM), 14q32.32 (TRAF3), 13q14.2 (SMAD9, CCNA1) or 7q36.1 (CDK5, EZH2), while HPV- HNSCCs are commonly deleted at 9p21.3 (CDKN2A), 2q22.1 (LRP1B), 10q23.31 (PTEN), 9q34.3 (NOTCH1) and 18q21.2 (SMAD4) [20,21,22,23,24]. A notable HNSCC subtype beyond the HPV dichotomization is nasopharyngeal carcinoma (NPC). NPC is often associated with EBV infection and is endemic to Southeast Asia and North Africa [34,35]. NPCs show high frequencies of copy number gains at 1q, 3q, 8q 12p and 12q or deletions in 1p, 3p, 9p, 9q, 11q, 14q and 16q [34,36].
Across studies, the most commonly selected nonsynonymous single nucleotide alterations are located within the TP53, FAT1, CDKN2A, PIK3CA, NOTCH1, KMT2D, NSD1, CASP8 and AJUBA genes [20,21,24,25,27]. Notably, many of these somatic mutations are found in the amplified regions mentioned above [20]. While the general abundance of somatic single-nucleotide mutations in HNSCC is independent of HPV status [20,37], the spectra of mutations are different in HPV + tumors [20,21,25,37,38]. The most commonly mutated gene in HNSCC is TP53 with frequencies ranging up to 80% of HPV- cases [20,32,39,40]. Although HPV+ HNSCCs exhibit less frequent TP53 mutations (as also observed in EBV- NPCs [34]), they usually degrade TP53 via the HPV-encoded oncogenic ubiquitin ligase E6 [41]. The TP53 tumor suppressor safeguards the functionality of many critical cellular processes such as cell cycling, DNA damage response, senescence and metabolism which cancer cells collectively hijack to acquire their neoplastic growth capabilities [42,43,44,45,46]. In the absence of activating stress signals the proteasome ensures a high turnover of MDM2-ubiquitinated TP53 [42,47]. Following activation by genotoxic and non-genotoxic stress stimuli MDM2 is rapidly inactivated leading to TP53 accumulation and post-translational modifications [42,44,47]. Activated TP53 mainly but not exclusively acts as a transcription factor [48,49]. In HNSCC, defective TP53 signaling can increase proliferation [50], promote invasiveness [51] and genomic instability [52], result in radiation resistance [53] and affect the tumor immune microenvironment [54]. As a consequence, mutations in TP53 are associated with reduced survival [55].
After TP53, the second most mutated gene in HNSCC is FAT1, affecting around 20% of patients with HNSCC [20,56,57]. FAT1 encodes a multifunctional type 1 transmembrane cadherin-related protein that—after proteolytic activation—acts as a modulator of oncogenic Wnt/β-catenin signaling [58], the Hippo/YAP1 signalosome [59], Ena/VASP-mediated cytoskeletal dynamics [56] and the EGFR/MAPK pathway including EGR-Hippo crosstalk [60]. FAT1 mutations are associated with invasion and metastasis [57] and response to radiotherapy [61].
Mutations in CDKN2A, NOTCH1, and PIK3CA are found in about 10–30% of HNSCC cases dependent on cohort size and patient selection [20,21,25,26,38,62,63]. CDKN2A encodes the p16INK4A tumor suppressor which arrests cell cycle progression at the G1-S restriction point by inhibiting CDK4/6-mediated phosphorylation of retinoblastoma-associated protein (RB1), a prototypical cell cycle regulator and driver of carcinogenesis [64]. CDKN2A loss is associated with resistance to immunotherapy [65]. Interestingly, HNSCCs commonly share genetic events that cause simultaneous inactivation of TP53 and p16INK4A. In HPV- HNSCCs, TP53 loss-of-function mutations are associated with CDKN2A point mutations or the loss of 9p21.3, which encodes CDKN2A, while in HPV+ HNSCCs, TP53 and RB1 are degraded by the viral E6 and E7 oncoproteins [2,20,25,38]. The NOTCH1 tumor suppressor gene encodes a conserved transmembrane protein that exerts pivotal regulatory roles during development and substantially contributes to tissue homeostasis [66,67]. Although activating mutations have been described for, e.g., NOTCH [62,68] and TP53 [38,55], it is a distinctive attribute of HNSCCs that the most commonly detected genetic events result in the inactivation of tumor suppressors or genes acting in associated pathways. This most likely reflects the fact that HNSCCs originate from basal keratinocytes of the mucosal epithelia which are capable to self-renew and to give rise to terminally differentiated epithelial cells [2,69]. Epithelial self-renewal depends, among others, on downregulation of NOTCH, CDKN2A and the action of the TP53 family member TP63 [70,71,72]. In contrast, there is no clear evidence of oncogene-driven reversal of a non-proliferative terminal differentiated epithelial phenotype [69]. The detected mutation patterns thus indicate that HNSCCs exploit these mechanisms for neoplastic transformation, especially as initiating events [2,69]. Notably, one of the few oncogenes commonly activated in HNSCC is PIK3CA [20,21,25,26,73,74]. Activation of PIK3CA is usually detected in advanced-stage, HPV+ tumors and accompanied by further hits within the PTEN-PI3K-Akt pathway [73,74].
2.2. Therapeutic Implications of Driver Gene Aberrations in HNSCC
Patients with HNSCC, who have failed standard first-line therapies, have limited therapeutic options and may benefit from new targeted therapies. Marret et al. ranked recurrent molecular alterations in HNSCC on the basis of the European Society for Medical Oncology (ESMO) Scale for Clinical Actionability of Molecular Targets (ESCAT) and identified six of 33 actionable alterations as the most clinically relevant: HRAS activating mutations, high microsatellite instability (MSI-H), high tumor mutational burden (TMB-high), NTRK fusions, CDKN2A inactivating alterations, and EGFR amplifications [77].
HRAS-activating mutations occur in approximately 4–8% of HNSCC patients [78]. HRAS oncogenic function is dependent on farnesylation and has been shown to be inhibited by tipifarnib, a selective inhibitor of farnesyltransferase, in HRAS mutant (mHRAS) HNSCC xenograft models [79]. In a single-arm, open-label phase II trial of tipifarnib for patients with recurrent and/or metastatic (R/M) HNSCC with mHRAS 20 patients were evaluable for response at the time of data cutoff [80]. The objective response rate for patients with the mHRAS variant allele frequency (VAF) of ≥20% was 55% (95% CI, 31.5 to 76.9), and median progression-free survival (PFS) on tipifarnib was 5.6 months (95% CI, 3.6 to 16.4) versus 3.6 months (95% CI, 1.3 to 5.2) on the last prior therapy, and the median overall survival (OS) was 15.4 months (95% CI, 7.0 to 29.7) [80]. Due to these encouraging results, the FDA has granted a “Breakthrough Therapy Designation” to tipifarnib for the treatment of patients with R/M mHRAS HNSCC with VAF ≥ 20% after disease progression on platinum-based chemotherapy in 2021.
In HNSCC the incidence of TMB-high, defined as ≥10 mutations per megabase (mut/Mb), is around 20% and the incidence of MSI-H is 1.2% [77]. TMB-high and MSI-H status has been correlated with the response to checkpoint blockade in basket trials which led to the tissue-agnostic FDA approval of pembrolizumab for advanced solid tumors meeting these criteria [81,82].
NTRK fusions are rare in HNSCC (<1%) [77]. There are currently two targeted therapeutic options for patients with NTRK gene fusions: the tropomyosin kinase (TRK) inhibitors entrectinib and larotrectinib [83,84]. In patients with advanced or metastatic NTRK fusion-positive solid tumors, the objective response rates ranged from 57% to 79% resulting in tissue-agnostic approvals by the EMA and FDA [77,83,84].
CDKN2A inactivating alterations that cause the hyperactivation of CDK4/6 are reported in 53.8% of HNSCC [77]. The selective CDK4/6 inhibitor palbociclib in combination with cetuximab showed promising activity in patients with platinum-resistant or cetuximab-resistant HPV-unrelated HNSCC in a non-randomized phase 2 trial [85]. However, in a double-blind randomized phase 2 trial (PALATINUS) there was no significant difference in median OS with palbociclib and cetuximab versus placebo and cetuximab [86]. Phase 2 and 3 trials are underway investigating palbociclib in biomarker selected patients with R/M HNSCC since the largest reduction in risk of death with palbociclib in the PALATINUS trial occurring in the subset with CDKN2A mutations [87].
EGFR amplifications are commonly found in patients with HNSCC [77]. Afatinib, an irreversible ERBB family blocker was evaluated as a second-line treatment in patients with R/M HNSCC in the LUX Head and Neck 1 trial [88]. Compared with methotrexate, afatinib was associated with significantly improved PFS (median 2.6 months for the afatinib group versus 1.7 months for the methotrexate group) [89]. A more pronounced benefit with afatinib was observed in patients with EGFR-amplified tumors [90].
In combination with chemotherapy in the first-line treatment of R/M HNSCC, EGFR copy number was not a predictive biomarker for the efficacy of cetuximab [91]. However, the presence of a single nucleotide polymorphism encoding EGFR-K521 represents an important mechanism of primary resistance to cetuximab in HNSCC [92]. This EGFR polymorphism is expressed in more than 40% of individuals and was shown to be associated with significantly shorter PFS upon palliative treatment with cetuximab plus chemotherapy or radiation [92]. TP53 is the most frequently altered gene in HNSCC with mutations detected in over two-thirds of patients [93] but evidence-based clinical data regarding TP53 actionability are scarce [77]. TP53 mutational status may, however, predict decreased sensitivity to cisplatin-based therapy [93]. Loss of function of p53 mutant proteins predicted a significantly lower pathologic complete response rate and suboptimal response to cisplatin-based neoadjuvant chemotherapy in patients with oral cavity squamous cell carcinoma [94].
2.3. Genetic Heterogeneity in HNSCC
The spatiotemporal genetic heterogeneity of solid tumors has been associated with a dismal prognosis due to decreased therapy response and higher rates of tumor recurrence [95,96]. This also applies to patients with HNSCCs, even in the setting of a favorable HPV+ tumor status [33,97,98,99].
Efforts to break the heterogeneous group of HNSCCs down into prognostically relevant subgroups utilized the bulk gene expression analysis of more than 279 tumor samples to define four distinct tumor expression subtypes [20,23,100]. Recent advances in single-cell RNA sequencing techniques have allowed for the further refinement of the HNSCC subtypes identified through bulk gene expression analysis. Specifically, these subtypes have been classified into three groups: malignant-basal, classical, and atypical tumors. Notably, the former mesenchymal subtype has been reclassified as malignant-basal tumors, which are characterized by an abundance of interspersed mesenchymal cells. While this subtyping approach has been successful in identifying distinct subgroups, there are still significant transcriptional differences observed both within and between patients. Interestingly, cells located at the leading edges of malignant-basal tumors have been found to partially express genes associated with epithelial-mesenchymal transition. This expression signature has been shown to be predictive for locoregional lymph node metastasis, highlighting the clinical significance of these subtypes [101]. However, further research is needed to fully understand the underlying mechanisms driving these transcriptional differences and how they may impact patient outcomes.
Another study has shed light on the genetic patterns of metastasis in HNSCCs, revealing two distinct subtypes with potential clinical implications. Patients with hematogenous metastasis exhibited upregulations of PD-L1 and PD-L2, suggesting that immune checkpoint inhibition may be a viable treatment option for this group. In contrast, patients with lymphatic metastasis showed a better response to chemotherapy in combination with locoregional radiotherapy [99].
In addition, prognostically relevant tumorigenic mutations were also found in tumor-adjacent tissue sometimes referred to as oral field cancerization [2,69,102]. In line with this observation, metachronous recurrent tumors were described to be concordant in only 60% of somatic nucleotide variants found in the primary tumor by whole exome sequencing [103]. The discovery of pre-malignantly transformed cell populations has important implications for understanding disease relapse and the development of secondary malignancies in HNSCC patients since these cell populations may be a source of relapse even in patients who are in full remission after first-line therapy. It could also explain the occurrence of frequently observed secondary malignancies. Future research will be needed to investigate the underlying mechanisms driving the transformation of these cells and to develop more effective treatment strategies to target them.
Taken together, liquid biopsy methods can indeed help to further elucidate the mutational landscapes of tumors, their surrounding tissue as well as their metastases. However, this complex spatiotemporal heterogeneity poses a great challenge and needs to be factored in for the future clinical application of liquid biopsy. Different techniques may need to be applied.
3. Genetic Analysis of Circulating cfDNA in Patients with HNSCC
3.1. cfDNA in Patients with Solid Tumors, Technical Challenges and Limitations
The analysis of cfDNA already generated multiple insights into tumor genetic composition [104], resistance mechanisms [105], tumor dissemination [106] and tumor evolution [107]. Due to its promising clinical applications, specifically for tumor detection, the identification of targetable driver mutations, the monitoring of disease during treatment and surveillance as well as its own prognostic relevance [108], cfDNA-based assays are increasingly being incorporated into clinical trials. This is also evident from the fact, that in February 2023 more than 1370 clinical trials were listed on clinicaltrials.gov and on euclinicaltrials.eu utilizing some form of cfDNA testing [109]. Moreover, several liquid biomarker tests received FDA approval [110]. There is a great variety of techniques ranging from fixed panels for the analysis of established tumor mutations to highly individualized approaches for the detection of patient-specific aberrations each of which has its own advantages and limitations [15,17].
The genetic heterogeneity of the primary tumor and metastatic lesions, tumor evolution on therapy or surveillance, shared genetic mutations of precursor lesions and coexisting germline mutations or clonal hematopoiesis are relevant biological challenges for all cfDNA analysis techniques [111]. Additionally, the amount of shedded tumor-derived cfDNA is very variable depending on the location, vascularization, cellular turnover and stage of the tumor among several other factors [112,113,114].
In addition to biological obstacles, the technical limitations of cfDNA analysis present significant challenges. During the pre-analytical phase, the use of specialized collection tubes with reagents for leukocyte stabilization can allow for the extension of storage and shipping times by up to 14 days at room temperature. In comparison, clinical practice often uses EDTA tubes which only offer a window of 2–4 h for further downstream processing [115,116]. Genomic deoxyribonucleic acid (gDNA) contamination is an acknowledged confounder which lowers the detection sensitivity due to interference. Controlling cfDNA input quantities is, therefore, essential to guarantee a certain sensitivity of the assay and reduce the false negative rates [117]. Commonly applied fluorometric methods for quantification are limited by the missing discrimination of cfDNA fragments and gDNA [118]. Although alternative methods such as capillary electrophoresis or quantitative polymerase chain reaction (qPCR) allow for a more precise estimation, they lack the detection of the presence of enzymatic inhibitors or again are biased by gDNA contamination. Alcaide et al. proposed a multiplex single-well droplet digital PCR assay to avoid these pitfalls [117].
Obtaining an accurate estimate of input cfDNA and minimizing gDNA contamination is crucial for precise estimations of potential tumor gene amplifications, such as HER2, which have important treatment implications. Typically, gene amplifications are deduced by calculating the relative ratio of the target gene to a copy number reference gene in close chromosomal proximity, which helps to exclude potential biases caused by genomic aneuploidy [119,120]. In summary, the optimization and assessment of analyte quality are crucial for ensuring the reliability of downstream analysis results, regardless of the technique used. It forms the foundation of the analysis process and is key to achieving accurate and consistent results.
Different techniques for cfDNA analysis have been developed, of which variants of next-generation sequencing, either amplicon- or capture-based (e.g., AmpliSeq HD [121], Safe-SeqS [122], CAPP-Seq with iDES [123] and digital droplet PCR (ddPCR) or BEAMING PCR [17]) are most often employed. These techniques are reported with limits of detections for VAFs between 0.0025% and 2% and have already been reviewed in detail elsewhere [124]. Figure 2 provides an overview of these techniques with their application in HNSCC and their sensitivity levels. All NGS-based techniques are prone to PCR errors and amplification biases depending on the library size, GC content and cfDNA fragment size. With the addition of unique molecular identifiers (UMI) cfDNA fragments can be tagged before amplification steps which enable in silico correction of these biases downstream. Computational algorithms such as iDES [123], PEC [125], TNER [126], ABEMUS [127] and SiNVICT [128] can correct for stereotypical PCR errors which become especially relevant at lower VAFs detection limits [123]. Although using different estimation models, most of these algorithms calculate and remove background mutation error counts based on healthy references.
Tumor-informed NGS-based approaches promise even further improvements in VAF detection limits; however, they are more laborious and complex due to their personalized nature and necessitate an initial tumor biopsy. Flach et al. recently described a detection limit down to 0.0006% VAF for 17 patients with HNSCC utilizing such a personalized cfDNA detection method. Thereby, the recurrence of disease could be detected 108 to 253 days before clinical progression [129]. Especially for the longitudinal tracking of patients with such sensitivities, great precautions must be taken to avoid the potential cross-contamination of samples.
ddPCR is a powerful alternative to NGS methods for the analysis of cfDNA in clinical routine due to its low cost, robustness and high sensitivity with VAFs detection of down to 0.01% [117,130]. However suitable shared mutated target genes need to be identified. Due to tumor heterogeneity and shared mutations in tumor-adjacent tissue in HNSCC described in Chapter 2.1, this might be a relevant limitation for the routine application of ddPCR.
An emerging field of cfDNA analysis is fragmentomics [131,132,133,134,135]. This term refers to applications that characterize cfDNA fragmentation and topology patterns that mirror chromatin compaction, gene regulation and the epigenome [132,135,136]. These patterns show high specificity with respect to tissue origin and disease and are thus discussed as promising cancer biomarkers [137,138]. While the general feasibility of this approach has been shown for HNSCC [133], fragmentomics is still in its infancy and many technical and conceptual issues need to be resolved.
Great improvements in cfDNA analysis have brought a variety of techniques into reach for future clinical application. Depending on the summarized limitations certain techniques might be better suited for certain clinical applications (e.g., tumor detection, profiling, surveillance). To ensure the robustness and standardization of these assays quality standards and controls are proposed which will help with the translation into clinical practice [139].
3.2. Specific Considerations on cfDNA in HNSCC
In HNSCC, studies examining cfDNA have not only focused on blood but also on saliva samples [16,140]. DNA that is released from the basal side of the tumor cells into the lymphatic and venous system should be detectable in the plasma, whereas DNA that is released from the apical side of the cells should be found in the saliva [141].
To explore the utility of tumor-derived DNA from different body sites for the diagnosis and surveillance of HNSCC, Wang et al. collected saliva and plasma before definite treatment for primary HNSCC (n = 71) and before salvage treatment for recurrent HNSCC (n = 22) [141]. Each tumor tissue sample was evaluated for a genetic alteration (either the presence of HPV or a somatic mutation), then this alteration was used to query the corresponding saliva and plasma samples [141]. In saliva, tumor DNA was found in 100% of patients with tumors of the oral cavity and in 47–70% of patients with cancers of other sites [141]. In plasma, tumor DNA was found in 80% of patients with oral cavity tumors, and in 86–100% of patients with cancers of other sites [141]. Thus, the sensitivity for detection of tumor DNA in the saliva was site-dependent and higher for tumors of the oral cavity [141]. Overall, increased sensitivity was demonstrated when assays of two compartments were combined [141]. Furthermore, tumor DNA in the saliva was found after surgery in three patients before the clinical diagnosis of recurrence, but in none of the five patients without recurrence [141].
Tumor-specific alterations such as gene methylation represent a strategy to differentiate between tumor-free circulating DNA and tumor-derived cfDNA in HNSCC patients [142]. Fung et al. evaluated the use of ddPCR for tumor suppressor gene methylation in the oral rinses of 50 patients with HNSCC and 58 controls for early disease detection and monitoring [143]. The degree of methylation of the markers PAX5, Endothelin Receptor β (EDNRB), and Deleted in Colorectal Cancer (DCC) was studied in HNSCC biopsies and corresponding pretreatment oral rinses [143]. The best results were obtained for the marker PAX5 with a sensitivity in oral rinses of 84.0% (95% CI, 70.9 to 92.8) and a specificity of 87.9% (95% CI, 76.7 to 95.0) [143]; 76.9% of the relapse cases had a rebound of methylation above presurgery levels in at least one of the tested markers before confirmed recurrence [143].
Interestingly, PAX5 methylation analyzed by ddPCR technology was also used to assess histologically cancer-negative deep surgical margin samples obtained from 82 HNSCC surgeries by an imprinting procedure and primary tissue collection [144]. PAX5 methylated imprint margins were an excellent predictor of poor locoregional recurrence-free survival (HR = 3.89, 95% CI, 1.19 to 17.52, p = 0.023) by multivariate analysis [144].
Notably, the association of HNSCC with HPV or EBV infection offers the potential to use virus-derived cfDNA as a marker. For example, it has been reported that circulating HPV DNA correlates with tumor burden [145] or staging [146]. For a detailed overview of this topic, we refer to the review of Aulakh et al. [140].
3.3. Liquid Biopsy in Early Stage HNSCC
A few studies have investigated minimal residual disease (MRD) detection by mutant cfDNA analysis in patients with HNSCC who underwent resection with curative intent [129,130,147,148,149]. Table 1 provides an overview of these studies.
Van Ginkel et al. show that ddPCR-based detection of TP53 mutations in blood samples from HNSCC patients with the locoregional disease is generally feasible, opening up avenues for post-treatment surveillance [130]. Jonas et al. confirm the feasibility of ddPCR-based liquid biopsy monitoring in this setting [147]. Moreover, this group—by analysis of post-surgery blood samples—shows that mutant cfDNA identifies patients at risk for early relapse and that increasing VAF precedes clinical progression. Flach et al. show that a high-sensitivity NGS-based approach may also achieve the sensitivity necessary to detect tumor-derived mutations in cfDNA in post-surgery samples [129]. With this approach, mutant cfDNA could be detected at levels as low as a VAF of 0.0006%. In all cases of clinical recurrence, mutant cfDNA was detected prior to progression, with lead times ranging from 108 to 253 days. In a study by Egyud et al., the baseline cfDNA detection rate among seven patients with verified tumor mutations was 86% (six out of seven patients) with 68% (15/22) of the mutations detected [148]. Two of four patients with recurrent disease had detectable cfDNA prior to recurrence [148]. Longitudinal cfDNA monitoring in HNSCC patients was also performed by Kogo et al. [149]. In seven of 18 HNSCC patients who had undergone curative treatment (surgery, radiotherapy or chemoradiotherapy) cfDNA tested positive again or did not test negative, and all seven patients relapsed [149]. Patients who remained negative for cfDNA during follow-up (n = 11) had a significantly better prognosis than those who became cfDNA positive [149].
Despite the low patient numbers included in these trials, these studies collectively indicate that patients with post-surgical detection of mutant cfDNA eventually relapse. Liquid biopsy positivity typically precedes clinical relapse by several months.
3.4. Liquid Biopsy in Advanced HNSCC
Liquid biopsies have the potential to enhance precision medicine for patients with advanced HNSCC. However, only a limited number of studies have shown the effectiveness of this method for detecting druggable lesions and monitoring disease and resistance in patients with R/M HNSCC.
Galot et al. determined the utility of liquid biopsy to detect potentially actionable mutations in cfDNA [151]. They found mutant cfDNA in around 70% of patients with metastatic disease and in 30% of patients with locoregional recurrent disease by targeted NGS including some patients with potentially actionable PIK3CA mutations as well as variants not found in the matched tumor tissue. The randomized phase 2 BERIL-1 trial includes an experimental combination of buparlisib and paclitaxel applied in the second line setting in R/M HNSCC. The biomarker translational study accompanying the trial analyzed cfDNA and found that the presence of TP53 alterations and HPV-negative status was associated with increased benefit from the combination, indicating that phosphatidylinositol 3-kinase (PI3K) inhibition may improve outcomes in this subset of patients historically characterized by poorer clinical outcome [153]. Interestingly, patients with low TMB had an improved response to buparlisib and paclitaxel as opposed to studies with checkpoint inhibitors where patients with high TMB had a better response to treatment [81,153]. Another study evaluated Bimiralisib, an inhibitor of the Phosphatidylinositol-3 Kinase pathway, in patients with R/M HNSCC after chemo- and immunotherapy [154]. Only patients with a detectable NOTCH1 mutation in the tissue sample were included in this trial based on preclinical data supporting the susceptibility to this drug in this subset of patients. The cfDNA-based detection of NOTCH1 mutations showed satisfactory concordance with tissue analysis, suggesting that this biomarker can be conveniently detected in the blood for future trials. However, to our knowledge, there are no data from HNSCC trials available with biomarker-guided patient selection based on cfDNA analysis. In this trial, changes in the cfDNA quantity during treatment were consistent with the clinical course and cfDNA collected at the time of disease progression showed new molecular alterations such as PIK3CA, BRAF, and TP53 mutations [154].
In addition to pre-therapeutic screening in patients with R/M HNSCC, serial analysis of cfDNA may provide insights into tumor control and the development of resistance traits over time. Our own study investigated tumor evolution in patients with R/M HNSCC treated with cetuximab/platinum/5-fluorouracil [155]. The study used targeted NGS to detect mutations in EGFR, KRAS, NRAS, and HRAS. In patients with on-treatment progression, 46% showed acquired RAS mutations in cfDNA before clinical resistance emerged, indicating a significant correlation between the emergence of RAS mutant clones and clinical resistance. The study also showed the potential of liquid biopsies to detect imminent resistance before clinical progression occurs.
The ongoing FOCUS study (NCT05075122) investigates the combination of a cancer vaccine with pembrolizumab in patients with R/M HNSCC. The biomarker part of this study includes serial liquid biopsy monitoring in R/M HNSCC as a predictor of disease progression. To search for potentially emerging resistant tumor subclones, the liquid biopsy panel contains genes previously reported to be involved in resistance to checkpoint inhibitors.
Table 1 summarizes the presented selection of studies exploring liquid biopsy for disease monitoring in R/M HNSCC.
4. Conclusions
For HNSCC, there is a great need for the identification of new biomarkers due to the high risk of relapse in locoregional disease after initial treatment and the limited therapeutic options in the metastatic setting. These biomarkers should identify minimal residual disease, assess treatment response, monitor disease activity, profile genomic tumor landscape, and detect targetable alterations and resistance mechanisms. All this can be offered by the analysis of cfDNA as a new type of specific and non-invasive biomarker, detected through liquid biopsy. In HNSCC, the analysis can be performed in both the blood and saliva with increased sensitivity when both analyses are combined. However, the limitations of this method should be taken into consideration. One crucial factor in analyzing cfDNA is the technical procedure as well as the standardization of the assays. The currently available data for HNSCC show that the potential usefulness of a distinct platform and/or marker depends on the respective cancer entity, stage and also diagnostic aim. More clinical studies will be necessary to investigate whether a change in therapy, based on this cfDNA analysis, will improve patient outcomes as the primary endpoint, compared to the current standard procedure consisting of clinical and radiological measures. These studies also need to define appropriate genetic markers for specific clinical endpoints, since liquid biopsy approaches remain purely experimental at this stage. Only when these data are available, will liquid biopsy fulfill its promise as a cost-effective, minimally invasive approach for cancer diagnostics.
To conclude, cfDNA analysis is becoming increasingly important in the management of HNSCC patients in the context of personalized and precision cancer medicine. Nevertheless, despite encouraging data, further research is mandatory in order to shed more light on this analysis before it is widely integrated into daily clinical practice.
Author Contributions
A.B., B.T., C.S., E.D. and M.B. contributed to the conceptualization and writing of the review. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
M.B. Consulting and Honoraria: BMS, Amgen, Gilead, Sanofi Aventis. Contracted Research: Novartis, Servier, Hexal Biosimilars, BMS, Merck, Janssen. All other authors declare no conflicts of interest.
Abbreviations
| CNV | copy number variations |
| cfDNA | cell-free DNA |
| CRT | chemoradiation |
| ddPCR | digital droplet polymerase chain reaction |
| DNA | deoxyribonucleic acid |
| EBV | Epstein-Barr virus |
| ESCAT | ESMO Scale for Clinical Actionability of molecular Targets |
| ESMO | European Society for Medical Oncology |
| gDNA | genomic deoxyribonucleic acid |
| GC | guanine-cytosine |
| HNSCC | Head and neck squamous cell carcinoma |
| HPV | human papillomavirus |
| HPV + HNSCC | Human papillomavirus associated head and neck squamous cell carcinoma |
| HPV- HNSCC | HPV negative HNSCC |
| mHRAS | mutant HRAS |
| MSI | microsatellite instability |
| MSI-H | high microsatellite instability |
| Mut/Mb | mutations per megabase |
| MRD | minimal residual disease |
| NPC | nasopharyngeal carcinoma |
| NGS | next-generation sequencing |
| OS | overall survival |
| PCR | polymerase chain reaction |
| PFS | progression-free survival |
| qPCR | quantitative polymerase chain reaction |
| R/M HNSCC | recurrent and/or metastatic head and neck squamous cell carcinoma |
| TMB | tumor mutational burden |
| VAF | variant allele frequency |
References
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Leemans, C.R.; Braakhuis, B.J.; Brakenhoff, R.H. The molecular biology of head and neck cancer. Nat. Rev. Cancer 2011, 11, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and neck cancer. Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV-associated head and neck cancer: A virus-related cancer epidemic. Lancet Oncol. 2010, 11, 781–789. [Google Scholar] [CrossRef] [Green Version]
- Ruffin, A.T.; Li, H.; Vujanovic, L.; Zandberg, D.P.; Ferris, R.L.; Bruno, T.C. Improving head and neck cancer therapies by immunomodulation of the tumour microenvironment. Nat. Rev. Cancer 2022, 23, 173–188. [Google Scholar] [CrossRef]
- Alsahafi, E.; Begg, K.; Amelio, I.; Raulf, N.; Lucarelli, P.; Sauter, T.; Tavassoli, M. Clinical update on head and neck cancer: Molecular biology and ongoing challenges. Cell Death Dis. 2019, 10, 540. [Google Scholar] [CrossRef] [Green Version]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefebvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Rettig, E.M.; D’Souza, G. Epidemiology of head and neck cancer. Surg. Oncol. Clin. N. Am. 2015, 24, 379–396. [Google Scholar] [CrossRef]
- Leeman, J.E.; Li, J.G.; Pei, X.; Venigalla, P.; Zumsteg, Z.S.; Katsoulakis, E.; Lupovitch, E.; McBride, S.M.; Tsai, C.J.; Boyle, J.O.; et al. Patterns of Treatment Failure and Postrecurrence Outcomes Among Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma After Chemoradiotherapy Using Modern Radiation Techniques. JAMA Oncol. 2017, 3, 1487–1494. [Google Scholar] [CrossRef] [Green Version]
- Mehanna, H.; Kong, A.; Ahmed, S.K. Recurrent head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S181–S190. [Google Scholar] [CrossRef]
- Mehanna, H.; Wong, W.L.; McConkey, C.C.; Rahman, J.K.; Robinson, M.; Hartley, A.G.; Nutting, C.; Powell, N.; Al-Booz, H.; Robinson, M.; et al. PET-CT Surveillance versus Neck Dissection in Advanced Head and Neck Cancer. N. Engl. J. Med. 2016, 374, 1444–1454. [Google Scholar] [CrossRef]
- Alix-Panabieres, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Pantel, K.; Alix-Panabieres, C. Liquid biopsy and minimal residual disease—Latest advances and implications for cure. Nat. Rev. Clin. Oncol. 2019, 16, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Tivey, A.; Church, M.; Rothwell, D.; Dive, C.; Cook, N. Circulating tumour DNA—Looking beyond the blood. Nat. Rev. Clin. Oncol. 2022, 19, 600–612. [Google Scholar] [CrossRef]
- Lone, S.N.; Nisar, S.; Masoodi, T.; Singh, M.; Rizwan, A.; Hashem, S.; El-Rifai, W.; Bedognetti, D.; Batra, S.K.; Haris, M.; et al. Liquid biopsy: A step closer to transform diagnosis, prognosis and future of cancer treatments. Mol. Cancer 2022, 21, 79. [Google Scholar] [CrossRef]
- Schmidt, H.; Kulasinghe, A.; Kenny, L.; Punyadeera, C. The development of a liquid biopsy for head and neck cancers. Oral Oncol. 2016, 61, 8–11. [Google Scholar] [CrossRef]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Genome Atlas, N. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature 2015, 517, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Stransky, N.; Egloff, A.M.; Tward, A.D.; Kostic, A.D.; Cibulskis, K.; Sivachenko, A.; Kryukov, G.V.; Lawrence, M.S.; Sougnez, C.; McKenna, A.; et al. The mutational landscape of head and neck squamous cell carcinoma. Science 2011, 333, 1157–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Chen, Y.; Luo, H.; Cai, H. The Landscape of Somatic Copy Number Alterations in Head and Neck Squamous Cell Carcinoma. Front. Oncol. 2020, 10, 321. [Google Scholar] [CrossRef] [Green Version]
- Walter, V.; Yin, X.; Wilkerson, M.D.; Cabanski, C.R.; Zhao, N.; Du, Y.; Ang, M.K.; Hayward, M.C.; Salazar, A.H.; Hoadley, K.A.; et al. Molecular subtypes in head and neck cancer exhibit distinct patterns of chromosomal gain and loss of canonical cancer genes. PLoS ONE 2013, 8, e56823. [Google Scholar] [CrossRef]
- Pickering, C.R.; Zhang, J.; Yoo, S.Y.; Bengtsson, L.; Moorthy, S.; Neskey, D.M.; Zhao, M.; Ortega Alves, M.V.; Chang, K.; Drummond, J.; et al. Integrative genomic characterization of oral squamous cell carcinoma identifies frequent somatic drivers. Cancer Discov. 2013, 3, 770–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lechner, M.; Frampton, G.M.; Fenton, T.; Feber, A.; Palmer, G.; Jay, A.; Pillay, N.; Forster, M.; Cronin, M.T.; Lipson, D.; et al. Targeted next-generation sequencing of head and neck squamous cell carcinoma identifies novel genetic alterations in HPV+ and HPV- tumors. Genome Med. 2013, 5, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, N.; Frederick, M.J.; Pickering, C.R.; Bettegowda, C.; Chang, K.; Li, R.J.; Fakhry, C.; Xie, T.X.; Zhang, J.; Wang, J.; et al. Exome sequencing of head and neck squamous cell carcinoma reveals inactivating mutations in NOTCH1. Science 2011, 333, 1154–1157. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.R.; Chen, Z.; Faden, D.L.; Agrawal, N.; Li, R.J.; Hanna, G.J.; Iyer, N.G.; Boot, A.; Rozen, S.G.; Vettore, A.L.; et al. The mutational landscape of early- and typical-onset oral tongue squamous cell carcinoma. Cancer 2021, 127, 544–553. [Google Scholar] [CrossRef]
- Vettore, A.L.; Ramnarayanan, K.; Poore, G.; Lim, K.; Ong, C.K.; Huang, K.K.; Leong, H.S.; Chong, F.T.; Lim, T.K.; Lim, W.K.; et al. Mutational landscapes of tongue carcinoma reveal recurrent mutations in genes of therapeutic and prognostic relevance. Genome Med. 2015, 7, 98. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.F.; Chiang, S.L.; Lin, C.Y.; Chang, J.G.; Chung, C.M.; Ko, A.M.; Lin, Y.Z.; Lee, C.H.; Lee, K.W.; Chen, M.K.; et al. Somatic Mutations and Genetic Variants of NOTCH1 in Head and Neck Squamous Cell Carcinoma Occurrence and Development. Sci. Rep. 2016, 6, 24014. [Google Scholar] [CrossRef] [Green Version]
- Farah, C.S. Molecular landscape of head and neck cancer and implications for therapy. Ann. Transl. Med. 2021, 9, 915. [Google Scholar] [CrossRef]
- Campbell, J.D.; Yau, C.; Bowlby, R.; Liu, Y.; Brennan, K.; Fan, H.; Taylor, A.M.; Wang, C.; Walter, V.; Akbani, R.; et al. Genomic, Pathway Network, and Immunologic Features Distinguishing Squamous Carcinomas. Cell Rep. 2018, 23, 194–212.e196. [Google Scholar] [CrossRef] [Green Version]
- Ju, Y.; Wu, X.; Wang, H.; Li, B.; Long, Q.; Zhang, D.; Chen, H.; Xiao, N.; Li, F.; Zhang, S.; et al. Genomic Landscape of Head and Neck Squamous Cell Carcinoma Across Different Anatomic Sites in Chinese Population. Front. Genet. 2021, 12, 680699. [Google Scholar] [CrossRef] [PubMed]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat. Rev. Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.C.W.; Hui, E.P.; Lo, K.W.; Lam, W.K.J.; Johnson, D.; Li, L.; Tao, Q.; Chan, K.C.A.; To, K.F.; King, A.D.; et al. Nasopharyngeal carcinoma: An evolving paradigm. Nat. Rev. Clin. Oncol. 2021, 18, 679–695. [Google Scholar] [CrossRef]
- Luo, W. Nasopharyngeal carcinoma ecology theory: Cancer as multidimensional spatiotemporal “unity of ecology and evolution” pathological ecosystem. Theranostics 2023, 13, 1607–1631. [Google Scholar] [CrossRef]
- Lo, K.W.; Chung, G.T.; To, K.F. Deciphering the molecular genetic basis of NPC through molecular, cytogenetic, and epigenetic approaches. Semin. Cancer Biol. 2012, 22, 79–86. [Google Scholar] [CrossRef]
- Seiwert, T.Y.; Zuo, Z.; Keck, M.K.; Khattri, A.; Pedamallu, C.S.; Stricker, T.; Brown, C.; Pugh, T.J.; Stojanov, P.; Cho, J.; et al. Integrative and comparative genomic analysis of HPV-positive and HPV-negative head and neck squamous cell carcinomas. Clin. Cancer Res. 2015, 21, 632–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deneka, A.Y.; Baca, Y.; Serebriiskii, I.G.; Nicolas, E.; Parker, M.I.; Nguyen, T.T.; Xiu, J.; Korn, W.M.; Demeure, M.J.; Wise-Draper, T.; et al. Association of TP53 and CDKN2A Mutation Profile with Tumor Mutation Burden in Head and Neck Cancer. Clin. Cancer Res. 2022, 28, 1925–1937. [Google Scholar] [CrossRef]
- Zhou, G.; Liu, Z.; Myers, J.N. TP53 Mutations in Head and Neck Squamous Cell Carcinoma and Their Impact on Disease Progression and Treatment Response. J. Cell. Biochem. 2016, 117, 2682–2692. [Google Scholar] [CrossRef] [Green Version]
- Nathan, C.A.; Khandelwal, A.R.; Wolf, G.T.; Rodrigo, J.P.; Makitie, A.A.; Saba, N.F.; Forastiere, A.A.; Bradford, C.R.; Ferlito, A. TP53 mutations in head and neck cancer. Mol. Carcinog. 2022, 61, 385–391. [Google Scholar] [CrossRef]
- Dong, H.; Shu, X.; Xu, Q.; Zhu, C.; Kaufmann, A.M.; Zheng, Z.M.; Albers, A.E.; Qian, X. Current Status of Human Papillomavirus-Related Head and Neck Cancer: From Viral Genome to Patient Care. Virol. Sin. 2021, 36, 1284–1302. [Google Scholar] [CrossRef]
- Aubrey, B.J.; Strasser, A.; Kelly, G.L. Tumor-Suppressor Functions of the TP53 Pathway. Cold Spring Harb. Perspect. Med. 2016, 6, a026062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Strasser, A.; Kelly, G.L. Should mutant TP53 be targeted for cancer therapy? Cell Death Differ. 2022, 29, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.F.; Kelly, G.L.; Strasser, A. Of the many cellular responses activated by TP53, which ones are critical for tumour suppression? Cell Death Differ. 2022, 29, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Boutelle, A.M.; Attardi, L.D. p53 and Tumor Suppression: It Takes a Network. Trends Cell Biol. 2021, 31, 298–310. [Google Scholar] [CrossRef]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef]
- Liebl, M.C.; Hofmann, T.G. The Role of p53 Signaling in Colorectal Cancer. Cancers 2021, 13, 2195. [Google Scholar] [CrossRef]
- Sullivan, K.D.; Galbraith, M.D.; Andrysik, Z.; Espinosa, J.M. Mechanisms of transcriptional regulation by p53. Cell Death Differ. 2018, 25, 133–143. [Google Scholar] [CrossRef] [Green Version]
- Ho, T.; Tan, B.X.; Lane, D. How the Other Half Lives: What p53 Does When It Is Not Being a Transcription Factor. Int. J. Mol. Sci. 2019, 21, 13. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, N.; Zhao, M.; Tang, L.; Patel, A.A.; Xi, Q.; Van, H.T.; Takahashi, H.; Osman, A.A.; Zhang, J.; Wang, J.; et al. Gain-of-function mutant p53 promotes the oncogenic potential of head and neck squamous cell carcinoma cells by targeting the transcription factors FOXO3a and FOXM1. Oncogene 2018, 37, 1279–1292. [Google Scholar] [CrossRef] [Green Version]
- Neskey, D.M.; Osman, A.A.; Ow, T.J.; Katsonis, P.; McDonald, T.; Hicks, S.C.; Hsu, T.K.; Pickering, C.R.; Ward, A.; Patel, A.; et al. Evolutionary Action Score of TP53 Identifies High-Risk Mutations Associated with Decreased Survival and Increased Distant Metastases in Head and Neck Cancer. Cancer Res. 2015, 75, 1527–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klinakis, A.; Rampias, T. TP53 mutational landscape of metastatic head and neck cancer reveals patterns of mutation selection. EBioMedicine 2020, 58, 102905. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, M.N.D.; Mierzwa, M.; D’Silva, N.J. Radiation resistance in head and neck squamous cell carcinoma: Dire need for an appropriate sensitizer. Oncogene 2020, 39, 3638–3649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Xie, T.; Wang, B.; Wang, R.; Cai, Y.; Yuan, B.; Gleber-Netto, F.O.; Tian, X.; Rodriguez-Rosario, A.E.; Osman, A.A.; et al. Mutant p53 drives an immune cold tumor immune microenvironment in oral squamous cell carcinoma. Commun. Biol. 2022, 5, 757. [Google Scholar] [CrossRef] [PubMed]
- Poeta, M.L.; Manola, J.; Goldwasser, M.A.; Forastiere, A.; Benoit, N.; Califano, J.A.; Ridge, J.A.; Goodwin, J.; Kenady, D.; Saunders, J.; et al. TP53 mutations and survival in squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2007, 357, 2552–2561. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.G.; Saba, N.F.; Teng, Y. The diverse functions of FAT1 in cancer progression: Good, bad, or ugly? J. Exp. Clin. Cancer Res. 2022, 41, 248. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.C.; Lin, L.H.; Yu, S.Y.; Kao, S.Y.; Chang, K.W.; Cheng, H.W.; Liu, C.J. FAT1 somatic mutations in head and neck carcinoma are associated with tumor progression and survival. Carcinogenesis 2018, 39, 1320–1330. [Google Scholar] [CrossRef]
- Morris, L.G.; Kaufman, A.M.; Gong, Y.; Ramaswami, D.; Walsh, L.A.; Turcan, S.; Eng, S.; Kannan, K.; Zou, Y.; Peng, L.; et al. Recurrent somatic mutation of FAT1 in multiple human cancers leads to aberrant Wnt activation. Nat. Genet. 2013, 45, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Martin, D.; Degese, M.S.; Vitale-Cross, L.; Iglesias-Bartolome, R.; Valera, J.L.C.; Wang, Z.; Feng, X.; Yeerna, H.; Vadmal, V.; Moroishi, T.; et al. Assembly and activation of the Hippo signalome by FAT1 tumor suppressor. Nat. Commun. 2018, 9, 2372. [Google Scholar] [CrossRef] [Green Version]
- Ando, T.; Arang, N.; Wang, Z.; Costea, D.E.; Feng, X.; Goto, Y.; Izumi, H.; Gilardi, M.; Ando, K.; Gutkind, J.S. EGFR Regulates the Hippo pathway by promoting the tyrosine phosphorylation of MOB1. Commun. Biol. 2021, 4, 1237. [Google Scholar] [CrossRef]
- Kim, S.I.; Woo, S.R.; Noh, J.K.; Lee, M.K.; Lee, Y.C.; Lee, J.W.; Ko, S.G.; Eun, Y.G. Clinical significance of FAT1 gene mutation and mRNA expression in patients with head and neck squamous cell carcinoma. Mol. Oncol. 2022, 16, 1661–1679. [Google Scholar] [CrossRef]
- Sun, W.; Gaykalova, D.A.; Ochs, M.F.; Mambo, E.; Arnaoutakis, D.; Liu, Y.; Loyo, M.; Agrawal, N.; Howard, J.; Li, R.; et al. Activation of the NOTCH pathway in head and neck cancer. Cancer Res. 2014, 74, 1091–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, C.T.; Yang, L.Y.; Lee, L.Y.; Lin, C.Y.; Wang, H.M.; Ng, S.H.; Yen, T.C.; Fan, W.L.; Hsieh, J.C. Whole-exome sequencing identifies biosignatures that predict adverse survival outcomes in surgically treated patients with oral cavity squamous cell carcinoma. Oral Oncol. 2021, 122, 105547. [Google Scholar] [CrossRef]
- Sherr, C.J. Cancer cell cycles. Science 1996, 274, 1672–1677. [Google Scholar] [CrossRef] [Green Version]
- Gutiontov, S.I.; Turchan, W.T.; Spurr, L.F.; Rouhani, S.J.; Chervin, C.S.; Steinhardt, G.; Lager, A.M.; Wanjari, P.; Malik, R.; Connell, P.P.; et al. CDKN2A loss-of-function predicts immunotherapy resistance in non-small cell lung cancer. Sci. Rep. 2021, 11, 20059. [Google Scholar] [CrossRef]
- Zhou, B.; Lin, W.; Long, Y.; Yang, Y.; Zhang, H.; Wu, K.; Chu, Q. Notch signaling pathway: Architecture, disease, and therapeutics. Signal Transduct. Target. Ther. 2022, 7, 95. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.A.; Huang, C.; Li, Q.; Kazi, S.A.; Byers, L.A.; Wang, J.; Johnson, F.M.; Frederick, M.J. NOTCH1 Signaling in Head and Neck Squamous Cell Carcinoma. Cells 2020, 9, 2677. [Google Scholar] [CrossRef]
- Feeney, L.; Hapuarachi, B.; Adderley, H.; Rack, S.; Morgan, D.; Walker, R.; Rauch, R.; Herz, E.; Kaye, J.; Harrington, K.; et al. Clinical disease course and survival outcomes following disease recurrence in adenoid cystic carcinoma with and without NOTCH signaling pathway activation. Oral Oncol. 2022, 133, 106028. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Danes, A.; Blanpain, C. Deciphering the cells of origin of squamous cell carcinomas. Nat. Rev. Cancer 2018, 18, 549–561. [Google Scholar] [CrossRef] [PubMed]
- D’Arcangelo, D.; Tinaburri, L.; Dellambra, E. The Role of p16(INK4a) Pathway in Human Epidermal Stem Cell Self-Renewal, Aging and Cancer. Int. J. Mol. Sci. 2017, 18, 1591. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, B.C.; Lefort, K.; Mandinova, A.; Antonini, D.; Devgan, V.; Della Gatta, G.; Koster, M.I.; Zhang, Z.; Wang, J.; Tommasi di Vignano, A.; et al. Cross-regulation between Notch and p63 in keratinocyte commitment to differentiation. Genes Dev. 2006, 20, 1028–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yugawa, T.; Nishino, K.; Ohno, S.; Nakahara, T.; Fujita, M.; Goshima, N.; Umezawa, A.; Kiyono, T. Noncanonical NOTCH signaling limits self-renewal of human epithelial and induced pluripotent stem cells through ROCK activation. Mol. Cell. Biol. 2013, 33, 4434–4447. [Google Scholar] [CrossRef] [Green Version]
- Lui, V.W.; Hedberg, M.L.; Li, H.; Vangara, B.S.; Pendleton, K.; Zeng, Y.; Lu, Y.; Zhang, Q.; Du, Y.; Gilbert, B.R.; et al. Frequent mutation of the PI3K pathway in head and neck cancer defines predictive biomarkers. Cancer Discov. 2013, 3, 761–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichols, A.C.; Palma, D.A.; Chow, W.; Tan, S.; Rajakumar, C.; Rizzo, G.; Fung, K.; Kwan, K.; Wehrli, B.; Winquist, E.; et al. High frequency of activating PIK3CA mutations in human papillomavirus-positive oropharyngeal cancer. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 617–622. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; He, Y.; Xu, J.; Wang, R.; Chen, R.; Xia, X. The incidence of NTRK fusion in Chinese head and neck cancer and response to crizotinib treatment. J. Clin. Oncol. 2020, 38, e18532. [Google Scholar] [CrossRef]
- Stransky, N.; Cerami, E.; Schalm, S.; Kim, J.L.; Lengauer, C. The landscape of kinase fusions in cancer. Nat. Commun. 2014, 5, 4846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marret, G.; Bièche, I.; Dupain, C.; Borcoman, E.; du Rusquec, P.; Ricci, F.; Hescot, S.; Sablin, M.P.; Tresca, P.; Bello, D.; et al. Genomic Alterations in Head and Neck Squamous Cell Carcinoma: Level of Evidence According to ESMO Scale for Clinical Actionability of Molecular Targets (ESCAT). JCO Precis. Oncol. 2021, 5, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Mountzios, G.; Rampias, T.; Psyrri, A. The mutational spectrum of squamous-cell carcinoma of the head and neck: Targetable genetic events and clinical impact. Ann. Oncol. 2014, 25, 1889–1900. [Google Scholar] [CrossRef] [PubMed]
- Gilardi, M.; Wang, Z.; Proietto, M.; Chillà, A.; Calleja-Valera, J.L.; Goto, Y.; Vanoni, M.; Janes, M.R.; Mikulski, Z.; Gualberto, A.; et al. Tipifarnib as a Precision Therapy for. Mol. Cancer Ther. 2020, 19, 1784–1796. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.L.; Brana, I.; Haddad, R.; Bauman, J.; Bible, K.; Oosting, S.; Wong, D.J.; Ahn, M.J.; Boni, V.; Even, C.; et al. Tipifarnib in Head and Neck Squamous Cell Carcinoma With. J. Clin. Oncol. 2021, 39, 1856–1864. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients with Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results from the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: Integrated analysis of three phase 1-2 trials. Lancet Oncol. 2020, 21, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.S.; DuBois, S.G.; Kummar, S.; Farago, A.F.; Albert, C.M.; Rohrberg, K.S.; van Tilburg, C.M.; Nagasubramanian, R.; Berlin, J.D.; Federman, N.; et al. Larotrectinib in patients with TRK fusion-positive solid tumours: A pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 2020, 21, 531–540. [Google Scholar] [CrossRef]
- Adkins, D.; Ley, J.; Neupane, P.; Worden, F.; Sacco, A.G.; Palka, K.; Grilley-Olson, J.E.; Maggiore, R.; Salama, N.N.; Trinkaus, K.; et al. Palbociclib and cetuximab in platinum-resistant and in cetuximab-resistant human papillomavirus-unrelated head and neck cancer: A multicentre, multigroup, phase 2 trial. Lancet Oncol. 2019, 20, 1295–1305. [Google Scholar] [CrossRef]
- Adkins, D.R.; Lin, J.C.; Sacco, A.; Ley, J.; Oppelt, P.; Vanchenko, V.; Komashko, N.; Yen, C.J.; Wise-Draper, T.; Lopez-Picazo Gonzalez, J.; et al. Palbociclib and cetuximab compared with placebo and cetuximab in platinum-resistant, cetuximab-naïve, human papillomavirus-unrelated recurrent or metastatic head and neck squamous cell carcinoma: A double-blind, randomized, phase 2 trial. Oral. Oncol. 2021, 115, 105192. [Google Scholar] [CrossRef]
- Adkins, D.; Ley, J.; Cohen, J.; Oppelt, P. The Potential for Selective Cyclin-Dependent Kinase 4/6 Inhibition in the Therapy for Head and Neck Squamous Cell Carcinoma. Cancer J. 2022, 28, 377–380. [Google Scholar] [CrossRef]
- Machiels, J.P.; Haddad, R.I.; Fayette, J.; Licitra, L.F.; Tahara, M.; Vermorken, J.B.; Clement, P.M.; Gauler, T.; Cupissol, D.; Grau, J.J.; et al. Afatinib versus methotrexate as second-line treatment in patients with recurrent or metastatic squamous-cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): An open-label, randomised phase 3 trial. Lancet Oncol. 2015, 16, 583–594. [Google Scholar] [CrossRef]
- Beyaert, S.; Machiels, J.P.; Schmitz, S. Vaccine-Based Immunotherapy for Head and Neck Cancers. Cancers 2021, 13, 6041. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Licitra, L.F.; Burtness, B.; Fayette, J.; Gauler, T.; Clement, P.M.; Grau, J.J.; Del Campo, J.M.; Mailliez, A.; Haddad, R.I.; et al. Biomarkers predict enhanced clinical outcomes with afatinib versus methotrexate in patients with second-line recurrent and/or metastatic head and neck cancer. Ann. Oncol. 2017, 28, 2526–2532. [Google Scholar] [CrossRef]
- Licitra, L.; Mesia, R.; Rivera, F.; Remenár, É.; Hitt, R.; Erfán, J.; Rottey, S.; Kawecki, A.; Zabolotnyy, D.; Benasso, M.; et al. Evaluation of EGFR gene copy number as a predictive biomarker for the efficacy of cetuximab in combination with chemotherapy in the first-line treatment of recurrent and/or metastatic squamous cell carcinoma of the head and neck: EXTREME study. Ann. Oncol. 2011, 22, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Braig, F.; Kriegs, M.; Voigtlaender, M.; Habel, B.; Grob, T.; Biskup, K.; Blanchard, V.; Sack, M.; Thalhammer, A.; Ben Batalla, I.; et al. Cetuximab Resistance in Head and Neck Cancer Is Mediated by EGFR-K. Cancer Res. 2017, 77, 1188–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osman, A.A.; Neskey, D.M.; Katsonis, P.; Patel, A.A.; Ward, A.M.; Hsu, T.K.; Hicks, S.C.; McDonald, T.O.; Ow, T.J.; Alves, M.O.; et al. Evolutionary Action Score of TP53 Coding Variants Is Predictive of Platinum Response in Head and Neck Cancer Patients. Cancer Res. 2015, 75, 1205–1215. [Google Scholar] [CrossRef] [Green Version]
- Perrone, F.; Bossi, P.; Cortelazzi, B.; Locati, L.; Quattrone, P.; Pierotti, M.A.; Pilotti, S.; Licitra, L. TP53 mutations and pathologic complete response to neoadjuvant cisplatin and fluorouracil chemotherapy in resected oral cavity squamous cell carcinoma. J. Clin. Oncol. 2010, 28, 761–766. [Google Scholar] [CrossRef]
- Andor, N.; Graham, T.A.; Jansen, M.; Xia, L.C.; Aktipis, C.A.; Petritsch, C.; Ji, H.P.; Maley, C.C. Pan-cancer analysis of the extent and consequences of intratumor heterogeneity. Nat. Med. 2016, 22, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Marusyk, A.; Janiszewska, M.; Polyak, K. Intratumor Heterogeneity: The Rosetta Stone of Therapy Resistance. Cancer Cell 2020, 37, 471–484. [Google Scholar] [CrossRef]
- Mroz, E.A.; Tward, A.D.; Hammon, R.J.; Ren, Y.; Rocco, J.W. Intra-tumor genetic heterogeneity and mortality in head and neck cancer: Analysis of data from the Cancer Genome Atlas. PLoS Med. 2015, 12, e1001786. [Google Scholar] [CrossRef] [Green Version]
- Schrank, T.P.; Lenze, N.; Landess, L.P.; Hoyle, A.; Parker, J.; Lal, A.; Sheth, S.; Chera, B.S.; Patel, S.N.; Hackman, T.G.; et al. Genomic heterogeneity and copy number variant burden are associated with poor recurrence-free survival and 11q loss in human papillomavirus-positive squamous cell carcinoma of the oropharynx. Cancer 2021, 127, 2788–2800. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Zhang, X.L.; You, R.; Liu, Y.P.; Cai, H.M.; Liu, L.Z.; Liu, X.F.; Zou, X.; Xie, Y.L.; Zou, R.H.; et al. Evolutionary route of nasopharyngeal carcinoma metastasis and its clinical significance. Nat. Commun. 2023, 14, 610. [Google Scholar] [CrossRef]
- Chung, C.H.; Parker, J.S.; Karaca, G.; Wu, J.; Funkhouser, W.K.; Moore, D.; Butterfoss, D.; Xiang, D.; Zanation, A.; Yin, X.; et al. Molecular classification of head and neck squamous cell carcinomas using patterns of gene expression. Cancer Cell 2004, 5, 489–500. [Google Scholar] [CrossRef] [Green Version]
- Puram, S.V.; Tirosh, I.; Parikh, A.S.; Patel, A.P.; Yizhak, K.; Gillespie, S.; Rodman, C.; Luo, C.L.; Mroz, E.A.; Emerick, K.S.; et al. Single-Cell Transcriptomic Analysis of Primary and Metastatic Tumor Ecosystems in Head and Neck Cancer. Cell 2017, 171, 1611–1624.e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.; Xie, C.; Yang, L.; Liu, Y.; Zeng, J.; Li, X.; Fang, X.; Fan, Y.; Zhao, S.; Kuang, N.; et al. The genomic architectures of tumour-adjacent tissues, plasma and saliva reveal evolutionary underpinnings of relapse in head and neck squamous cell carcinoma. Br. J. Cancer 2021, 125, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, M.L.; Goh, G.; Chiosea, S.I.; Bauman, J.E.; Freilino, M.L.; Zeng, Y.; Wang, L.; Diergaarde, B.B.; Gooding, W.E.; Lui, V.W.; et al. Genetic landscape of metastatic and recurrent head and neck squamous cell carcinoma. J. Clin. Investig. 2016, 126, 169–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, B.; Chen, C.T.; Goyal, L.; Walmsley, C.; Pinto, C.J.; Baiev, I.; Allen, R.; Henderson, L.; Saha, S.; Reyes, S.; et al. Cell-free DNA captures tumor heterogeneity and driver alterations in rapid autopsies with pre-treated metastatic cancer. Nat. Commun. 2021, 12, 3199. [Google Scholar] [CrossRef]
- Gunderson, C.C.; Radhakrishnan, R.; Gomathinayagam, R.; Husain, S.; Aravindan, S.; Moore, K.M.; Dhanasekaran, D.N.; Jayaraman, M. Circulating Tumor Cell-Free DNA Genes as Prognostic Gene Signature for Platinum Resistant Ovarian Cancer Diagnosis. Biomark. Insights 2022, 17, 11772719221088404. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Petricca, J.; Ye, W.; Guan, J.; Zeng, Y.; Cheng, N.; Gong, L.; Shen, S.Y.; Hua, J.T.; Crumbaker, M.; et al. The cell-free DNA methylome captures distinctions between localized and metastatic prostate tumors. Nat. Commun. 2022, 13, 6467. [Google Scholar] [CrossRef]
- Kujala, J.; Hartikainen, J.M.; Tengstrom, M.; Sironen, R.; Auvinen, P.; Kosma, V.M.; Mannermaa, A. Circulating Cell-Free DNA Reflects the Clonal Evolution of Breast Cancer Tumors. Cancers 2022, 14, 1332. [Google Scholar] [CrossRef]
- Mondelo-Macia, P.; Garcia-Gonzalez, J.; Abalo, A.; Mosquera-Presedo, M.; Aguin, S.; Mateos, M.; Lopez-Lopez, R.; Leon-Mateos, L.; Muinelo-Romay, L.; Diaz-Pena, R. Plasma cell-free DNA and circulating tumor cells as prognostic biomarkers in small cell lung cancer patients. Transl. Lung Cancer Res. 2022, 11, 1995–2009. [Google Scholar] [CrossRef]
- Cisneros-Villanueva, M.; Hidalgo-Perez, L.; Rios-Romero, M.; Cedro-Tanda, A.; Ruiz-Villavicencio, C.A.; Page, K.; Hastings, R.; Fernandez-Garcia, D.; Allsopp, R.; Fonseca-Montano, M.A.; et al. Cell-free DNA analysis in current cancer clinical trials: A review. Br. J. Cancer 2022, 126, 391–400. [Google Scholar] [CrossRef]
- Vasseur, D.; Sassi, H.; Bayle, A.; Tagliamento, M.; Besse, B.; Marzac, C.; Arbab, A.; Auger, N.; Cotteret, S.; Aldea, M.; et al. Next-Generation Sequencing on Circulating Tumor DNA in Advanced Solid Cancer: Swiss Army Knife for the Molecular Tumor Board? A Review of the Literature Focused on FDA Approved Test. Cells 2022, 11, 1901. [Google Scholar] [CrossRef]
- Song, P.; Wu, L.R.; Yan, Y.H.; Zhang, J.X.; Chu, T.; Kwong, L.N.; Patel, A.A.; Zhang, D.Y. Limitations and opportunities of technologies for the analysis of cell-free DNA in cancer diagnostics. Nat. Biomed. Eng. 2022, 6, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.S.; Park, C.H.; Lee, S.; Park, H.S. Clinicopathological parameters for circulating tumor DNA shedding in surgically resected non-small cell lung cancer with EGFR or KRAS mutation. PLoS ONE 2020, 15, e0230622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbosh, C.; Birkbak, N.J.; Wilson, G.A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D.A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature 2017, 545, 446–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, L.; Belloum, Y.; Wikman, H.; Pantel, K. Clinical relevance of blood-based ctDNA analysis: Mutation detection and beyond. Br. J. Cancer 2021, 124, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Salvianti, F.; Gelmini, S.; Costanza, F.; Mancini, I.; Sonnati, G.; Simi, L.; Pazzagli, M.; Pinzani, P. The pre-analytical phase of the liquid biopsy. N. Biotechnol. 2020, 55, 19–29. [Google Scholar] [CrossRef]
- Greytak, S.R.; Engel, K.B.; Parpart-Li, S.; Murtaza, M.; Bronkhorst, A.J.; Pertile, M.D.; Moore, H.M. Harmonizing Cell-Free DNA Collection and Processing Practices through Evidence-Based Guidance. Clin. Cancer Res. 2020, 26, 3104–3109. [Google Scholar] [CrossRef] [Green Version]
- Alcaide, M.; Cheung, M.; Hillman, J.; Rassekh, S.R.; Deyell, R.J.; Batist, G.; Karsan, A.; Wyatt, A.W.; Johnson, N.; Scott, D.W.; et al. Evaluating the quantity, quality and size distribution of cell-free DNA by multiplex droplet digital PCR. Sci. Rep. 2020, 10, 12564. [Google Scholar] [CrossRef]
- Henikoff, S.; Church, G.M. Simultaneous Discovery of Cell-Free DNA and the Nucleosome Ladder. Genetics 2018, 209, 27–29. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, Y.; Okamoto, W.; Kato, T.; Esaki, T.; Kato, K.; Komatsu, Y.; Yuki, S.; Masuishi, T.; Nishina, T.; Ebi, H.; et al. Circulating tumor DNA-guided treatment with pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer: A phase 2 trial. Nat. Med. 2021, 27, 1899–1903. [Google Scholar] [CrossRef]
- Garcia-Murillas, I.; Turner, N.C. Assessing HER2 Amplification in Plasma cfDNA. Methods Mol. Biol. 2018, 1768, 161–172. [Google Scholar] [CrossRef]
- Hirotsu, Y.; Otake, S.; Ohyama, H.; Amemiya, K.; Higuchi, R.; Oyama, T.; Mochizuki, H.; Goto, T.; Omata, M. Dual-molecular barcode sequencing detects rare variants in tumor and cell free DNA in plasma. Sci. Rep. 2020, 10, 3391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinde, I.; Wu, J.; Papadopoulos, N.; Kinzler, K.W.; Vogelstein, B. Detection and quantification of rare mutations with massively parallel sequencing. Proc. Natl. Acad. Sci. USA 2011, 108, 9530–9535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, A.M.; Lovejoy, A.F.; Klass, D.M.; Kurtz, D.M.; Chabon, J.J.; Scherer, F.; Stehr, H.; Liu, C.L.; Bratman, S.V.; Say, C.; et al. Integrated digital error suppression for improved detection of circulating tumor DNA. Nat. Biotechnol. 2016, 34, 547–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito Abate, R.; Frezzetti, D.; Maiello, M.R.; Gallo, M.; Camerlingo, R.; De Luca, A.; De Cecio, R.; Morabito, A.; Normanno, N. Next Generation Sequencing-Based Profiling of Cell Free DNA in Patients with Advanced Non-Small Cell Lung Cancer: Advantages and Pitfalls. Cancers 2020, 12, 3804. [Google Scholar] [CrossRef]
- Kim, C.S.; Mohan, S.; Ayub, M.; Rothwell, D.G.; Dive, C.; Brady, G.; Miller, C. In silico error correction improves cfDNA mutation calling. Bioinformatics 2019, 35, 2380–2385. [Google Scholar] [CrossRef] [Green Version]
- Deng, S.; Lira, M.; Huang, D.; Wang, K.; Valdez, C.; Kinong, J.; Rejto, P.A.; Bienkowska, J.; Hardwick, J.; Xie, T. TNER: A novel background error suppression method for mutation detection in circulating tumor DNA. BMC Bioinform. 2018, 19, 387. [Google Scholar] [CrossRef] [Green Version]
- Casiraghi, N.; Orlando, F.; Ciani, Y.; Xiang, J.; Sboner, A.; Elemento, O.; Attard, G.; Beltran, H.; Demichelis, F.; Romanel, A. ABEMUS: Platform-specific and data-informed detection of somatic SNVs in cfDNA. Bioinformatics 2020, 36, 2665–2674. [Google Scholar] [CrossRef]
- Kockan, C.; Hach, F.; Sarrafi, I.; Bell, R.H.; McConeghy, B.; Beja, K.; Haegert, A.; Wyatt, A.W.; Volik, S.V.; Chi, K.N.; et al. SiNVICT: Ultra-sensitive detection of single nucleotide variants and indels in circulating tumour DNA. Bioinformatics 2017, 33, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Flach, S.; Howarth, K.; Hackinger, S.; Pipinikas, C.; Ellis, P.; McLay, K.; Marsico, G.; Forshew, T.; Walz, C.; Reichel, C.A.; et al. Liquid BIOpsy for MiNimal RESidual DiSease Detection in Head and Neck Squamous Cell Carcinoma (LIONESS)-a personalised circulating tumour DNA analysis in head and neck squamous cell carcinoma. Br. J. Cancer 2022, 126, 1186–1195. [Google Scholar] [CrossRef]
- van Ginkel, J.H.; Huibers, M.M.H.; van Es, R.J.J.; de Bree, R.; Willems, S.M. Droplet digital PCR for detection and quantification of circulating tumor DNA in plasma of head and neck cancer patients. BMC Cancer 2017, 17, 428. [Google Scholar] [CrossRef]
- Thierry, A.R. Circulating DNA fragmentomics and cancer screening. Cell Genom. 2023, 3, 100242. [Google Scholar] [CrossRef] [PubMed]
- Chiu, R.W.K.; Heitzer, E.; Lo, Y.M.D.; Mouliere, F.; Tsui, D.W.Y. Cell-Free DNA Fragmentomics: The New “Omics” on the Block. Clin. Chem. 2020, 66, 1480–1484. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Sun, K.; Peng, W.; Cheng, S.H.; Ni, M.; Yeung, P.C.; Heung, M.M.S.; Xie, T.; Shang, H.; Zhou, Z.; et al. Plasma DNA End-Motif Profiling as a Fragmentomic Marker in Cancer, Pregnancy, and Transplantation. Cancer Discov. 2020, 10, 664–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, S.C.; Lo, Y.M.D. Cell-Free DNA Fragmentomics in Liquid Biopsy. Diagnostics 2022, 12, 978. [Google Scholar] [CrossRef]
- Lo, Y.M.D.; Han, D.S.C.; Jiang, P.; Chiu, R.W.K. Epigenetics, fragmentomics, and topology of cell-free DNA in liquid biopsies. Science 2021, 372, eaaw3616. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y. At the dawn: Cell-free DNA fragmentomics and gene regulation. Br. J. Cancer 2022, 126, 379–390. [Google Scholar] [CrossRef]
- Gianni, C.; Palleschi, M.; Merloni, F.; Di Menna, G.; Sirico, M.; Sarti, S.; Virga, A.; Ulivi, P.; Cecconetto, L.; Mariotti, M.; et al. Cell-Free DNA Fragmentomics: A Promising Biomarker for Diagnosis, Prognosis and Prediction of Response in Breast Cancer. Int. J. Mol. Sci. 2022, 23, 14197. [Google Scholar] [CrossRef]
- Gunning, A.; Kumar, S.; Williams, C.K.; Berger, B.M.; Naber, S.P.; Gupta, P.B.; Del Vecchio Fitz, C.; Kuperwasser, C. Analytical Validation of NavDx, a cfDNA-Based Fragmentomic Profiling Assay for HPV-Driven Cancers. Diagnostics 2023, 13, 725. [Google Scholar] [CrossRef] [PubMed]
- Godsey, J.H.; Silvestro, A.; Barrett, J.C.; Bramlett, K.; Chudova, D.; Deras, I.; Dickey, J.; Hicks, J.; Johann, D.J.; Leary, R.; et al. Generic Protocols for the Analytical Validation of Next-Generation Sequencing-Based ctDNA Assays: A Joint Consensus Recommendation of the BloodPAC’s Analytical Variables Working Group. Clin. Chem. 2020, 66, 1156–1166. [Google Scholar] [CrossRef] [PubMed]
- Aulakh, S.S.; Silverman, D.A.; Young, K.; Dennis, S.K.; Birkeland, A.C. The Promise of Circulating Tumor DNA in Head and Neck Cancer. Cancers 2022, 14, 2968. [Google Scholar] [CrossRef]
- Wang, Y.; Springer, S.; Mulvey, C.L.; Silliman, N.; Schaefer, J.; Sausen, M.; James, N.; Rettig, E.M.; Guo, T.; Pickering, C.R.; et al. Detection of somatic mutations and HPV in the saliva and plasma of patients with head and neck squamous cell carcinomas. Sci. Transl. Med. 2015, 7, 293ra104. [Google Scholar] [CrossRef] [Green Version]
- Pall, A.H.; Jakobsen, K.K.; Grønhøj, C.; von Buchwald, C. Circulating tumour DNA alterations as biomarkers for head and neck cancer: A systematic review. Acta Oncol. 2020, 59, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Fung, S.Y.H.; Chan, K.C.A.; Wong, E.W.Y.; Ng, C.W.K.; Cho, R.; Yeung, Z.W.C.; Lam, J.W.K.; Chan, J.Y.K. Droplet digital PCR of tumor suppressor gene methylation in serial oral rinses of patients with head and neck squamous cell carcinoma. Head Neck 2021, 43, 1812–1822. [Google Scholar] [CrossRef]
- Hayashi, M.; Guerrero-Preston, R.; Sidransky, D.; Koch, W.M. Paired box 5 methylation detection by droplet digital PCR for ultra-sensitive deep surgical margins analysis of head and neck squamous cell carcinoma. Cancer Prev. Res. 2015, 8, 1017–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, G.J.; Supplee, J.G.; Kuang, Y.; Mahmood, U.; Lau, C.J.; Haddad, R.I.; Janne, P.A.; Paweletz, C.P. Plasma HPV cell-free DNA monitoring in advanced HPV-associated oropharyngeal cancer. Ann. Oncol. 2018, 29, 1980–1986. [Google Scholar] [CrossRef] [PubMed]
- Veyer, D.; Wack, M.; Mandavit, M.; Garrigou, S.; Hans, S.; Bonfils, P.; Tartour, E.; Belec, L.; Wang-Renault, S.F.; Laurent-Puig, P.; et al. HPV circulating tumoral DNA quantification by droplet-based digital PCR: A promising predictive and prognostic biomarker for HPV-associated oropharyngeal cancers. Int. J. Cancer 2020, 147, 1222–1227. [Google Scholar] [CrossRef]
- Jonas, H.; Simnica, D.; Bussmann, L.; Zech, H.; Doescher, J.; Laban, S.; Busch, C.J.; Binder, M. Early relapse detection by monitoring of circulating cell-free DNA in patients with localized head and neck squamous cell carcinoma: A subgroup analysis of the multicenter randomized clinical trial IMSTAR-HN. Oral Oncol. 2022, 126, 105733. [Google Scholar] [CrossRef]
- Egyud, M.; Sridhar, P.; Devaiah, A.; Yamada, E.; Saunders, S.; Ståhlberg, A.; Filges, S.; Krzyzanowski, P.M.; Kalatskaya, I.; Jiao, W.; et al. Plasma circulating tumor DNA as a potential tool for disease monitoring in head and neck cancer. Head Neck 2019, 41, 1351–1358. [Google Scholar] [CrossRef]
- Kogo, R.; Manako, T.; Iwaya, T.; Nishizuka, S.; Hiraki, H.; Sasaki, Y.; Idogawa, M.; Tokino, T.; Koide, A.; Komune, N.; et al. Individualized circulating tumor DNA monitoring in head and neck squamous cell carcinoma. Cancer Med. 2022, 11, 3960–3968. [Google Scholar] [CrossRef]
- Zech, H.B.; Moeckelmann, N.; Boettcher, A.; Muenscher, A.; Binder, M.; Vettorazzi, E.; Bokemeyer, C.; Schafhausen, P.; Betz, C.S.; Busch, C.J. Phase III study of nivolumab alone or combined with ipilimumab as immunotherapy versus standard of care in resectable head and neck squamous cell carcinoma. Future Oncol. 2020, 16, 3035–3043. [Google Scholar] [CrossRef]
- Galot, R.; van Marcke, C.; Helaers, R.; Mendola, A.; Goebbels, R.M.; Caignet, X.; Ambroise, J.; Wittouck, K.; Vikkula, M.; Limaye, N.; et al. Liquid biopsy for mutational profiling of locoregional recurrent and/or metastatic head and neck squamous cell carcinoma. Oral Oncol. 2020, 104, 104631. [Google Scholar] [CrossRef] [PubMed]
- Soulières, D.; Faivre, S.; Mesía, R.; Remenár, É.; Li, S.H.; Karpenko, A.; Dechaphunkul, A.; Ochsenreither, S.; Kiss, L.A.; Lin, J.C.; et al. Buparlisib and paclitaxel in patients with platinum-pretreated recurrent or metastatic squamous cell carcinoma of the head and neck (BERIL-1): A randomised, double-blind, placebo-controlled phase 2 trial. Lancet Oncol. 2017, 18, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Soulieres, D.; Licitra, L.; Mesia, R.; Remenar, E.; Li, S.H.; Karpenko, A.; Chol, M.; Wang, Y.A.; Solovieff, N.; Bourdeau, L.; et al. Molecular Alterations and Buparlisib Efficacy in Patients with Squamous Cell Carcinoma of the Head and Neck: Biomarker Analysis from BERIL-1. Clin. Cancer Res. 2018, 24, 2505–2516. [Google Scholar] [CrossRef] [Green Version]
- Johnson, F.M.; Janku, F.; Gouda, M.A.; Tran, H.T.; Kawedia, J.D.; Schmitz, D.; Streefkerk, H.; Lee, J.J.; Andersen, C.R.; Deng, D.; et al. Inhibition of the Phosphatidylinositol-3 Kinase Pathway Using Bimiralisib in Loss-of-Function NOTCH1-Mutant Head and Neck Cancer. Oncologist 2022, 27, 1004-e926. [Google Scholar] [CrossRef]
- Braig, F.; Voigtlaender, M.; Schieferdecker, A.; Busch, C.J.; Laban, S.; Grob, T.; Kriegs, M.; Knecht, R.; Bokemeyer, C.; Binder, M. Liquid biopsy monitoring uncovers acquired RAS-mediated resistance to cetuximab in a substantial proportion of patients with head and neck squamous cell carcinoma. Oncotarget 2016, 7, 42988–42995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Risk factors, anatomical sites and recurrent mutations in HNSCC. HNSCC is generally subgrouped in HPV+ and HPV- subsets. Common (but not entirely exclusive) genomic alterations per subtype are indicated.
Figure 1.
Risk factors, anatomical sites and recurrent mutations in HNSCC. HNSCC is generally subgrouped in HPV+ and HPV- subsets. Common (but not entirely exclusive) genomic alterations per subtype are indicated.

Figure 2.
Liquid biopsy monitoring of cfDNA in HNSCC. In HNSCC, cfDNA is sampled from saliva or blood to diagnose, monitor and guide treatment decisions. Examples of technical approaches to quantify cfDNA in patient samples are indicated including thresholds of sensitivity.
Figure 2.
Liquid biopsy monitoring of cfDNA in HNSCC. In HNSCC, cfDNA is sampled from saliva or blood to diagnose, monitor and guide treatment decisions. Examples of technical approaches to quantify cfDNA in patient samples are indicated including thresholds of sensitivity.


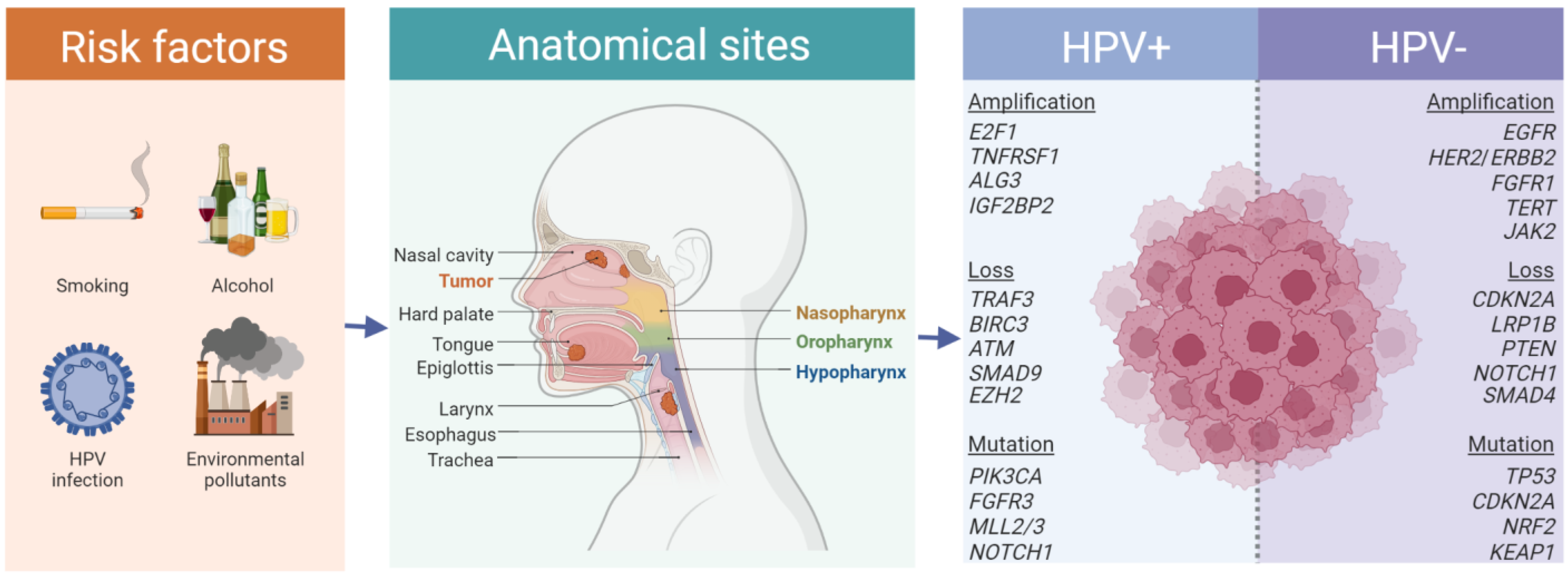{kind=link}
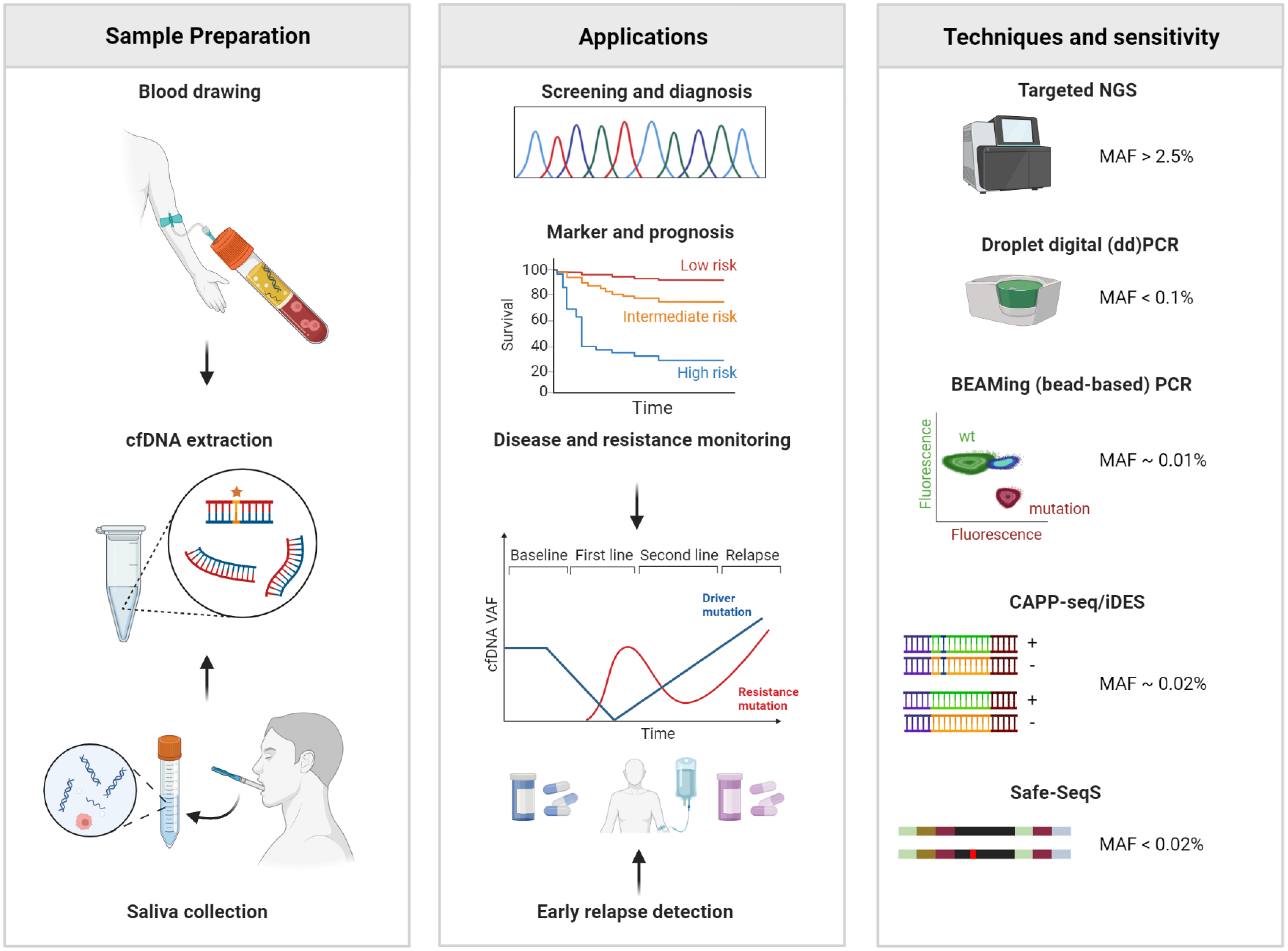{kind=link}
Table 1.
Key studies on liquid biopsy applications in HNSCC.
| Tumor Stage and Treatment | No. of Patients (n) | DNA Source | Technique | Study Results | Reference |
|---|---|---|---|---|---|
| Stage II-IVA surgically treated | n = 6 | Tumor tissue and pretreatment plasma samples | ddPCR | TP53 mutations were determined in primary tumor samples from 6 pts and in all cases pretreatment plasma samples were found positive for targeted TP53 mutations. | van Ginkel et al. [130] |
| Pts treated with curative intent in the IMSTAR-HN trial [150] | n = 19 | Tumor tissue and serial plasma samples | NGS and ddPCR | 11 pts were liquid biopsy positive before treatment initiation. Upon treatment, 8 of 11 pts fully cleared their ctDNA after surgery, none of these pts showed disease recurrence. 4 pts showed newly emerging or persistent ctDNA positivity in the treatment course. With a median follow-up of 93 weeks, 2 of these 4 pts had disease progression. | Jonas et al. [147] |
| Stage III-IVB surgically treated | n = 17 | Tumor tissue and serial plasma samples | Whole-exome sequencing, targeted NGS | ctDNA was detected in baseline samples taken prior to surgery in 17 of 17 pts. In all cases with clinical recurrence, ctDNA was detected prior to progression with lead times ranging from 108 to 253 days. | Flach et al. [129] |
| Stage I-IV | n = 8 | Tumor tissue and serial plasma samples | Whole-exome sequencing, targeted NGS | Tumor mutations were verified in 7 of 8 pts. Baseline ctDNA was positive in 6 pts. Recurrence occurred in 4 pts, 2 of whom had detectable ctDNA prior to recurrence. | Egyud et al. [148] |
| Treatment with curative intent | n = 26 | Tumor tissue and serial plasma samples | dPCR | Patients who remained negative for ctDNA during follow-up after initial curative treatment (n = 11) had significantly better prognosis than those who reverted to ctDNA positivity (n = 7; p < 0.0001; log-rank test). | Kogo et al. [149] |
| R/M disease | n = 39 | Tumor tissue and plasma samples | Targeted NGS | ctDNA was detected in 51% of pts with a higher probability of detection in metastatic than locoregional recurrent disease (70% vs. 30%, p = 0.025). Liquid biopsies did not reflect the complete mutational profile of the tumor but were shown to have the potential to identify actionable mutations as well as variants not found in the matched tumor tissue. | Galot et al. [151] |
| Pts with R/M disease treated in the BERIL-1 trial [152] | n = 112 | Tumor tissue and plasma samples | NGS | Pts with TP53 alterations, HPV-negative status, and low mutational load derived survival benefit with the combination of buparlisib and paclitaxel. | Soulieres et al. [153] |
| R/M NOTCH1-mutant disease after platinum chemotherapy and PD-1-inhibitors | n = 6 | Tumor tissue and serial plasma samples | Targeted NGS | NOTCH1 mutations in ctDNA collected at baseline were detected in 83% of pts. Changes in the ctDNA quantity during treatment were consistent with the clinical course. In addition, ctDNA samples collected at progression showed new emerging molecular alterations such as PIK3CA, BRAF, TP53, and others. | Johnson et al. [154] |
| Pts treated with cetuximab in curative and palliative intent | n = 46 | Tumor tissue and peripheral blood obtained after initiation of cetuximab treatment | Targeted NGS | 46% of pts with on-treatment disease progression showed acquired RAS mutations, while no RAS mutations were found in the non-progressive pts, indicating that acquisition of RAS mutant clones correlated significantly with clinical resistance. | Braig et al. [155] |
R/M = recurrent or metastatic; ddPCR = Droplet Digital PCR; NGS = next generation sequencing; dPCR = digital PCR Figure 1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Brandt, A.; Thiele, B.; Schultheiß, C.; Daetwyler, E.; Binder, M. Circulating Tumor DNA in Head and Neck Squamous Cell Carcinoma. Cancers 2023, 15, 2051. https://doi.org/10.3390/cancers15072051
AMA Style
Brandt A, Thiele B, Schultheiß C, Daetwyler E, Binder M. Circulating Tumor DNA in Head and Neck Squamous Cell Carcinoma. Cancers. 2023; 15(7):2051. https://doi.org/10.3390/cancers15072051
Chicago/Turabian StyleBrandt, Anna, Benjamin Thiele, Christoph Schultheiß, Eveline Daetwyler, and Mascha Binder. 2023. "Circulating Tumor DNA in Head and Neck Squamous Cell Carcinoma" Cancers 15, no. 7: 2051. https://doi.org/10.3390/cancers15072051
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.