
For Hepatocellular Carcinoma Treated with Yttrium-90 Microspheres, Dose Volumetrics on Post-Treatment Bremsstrahlung SPECT/CT Predict Clinical Outcomes
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Enrollment and Baseline Characteristics
2.2. Mapping Angiography and 99mTc-MAA Simulation
2.3. Post-Treatment 3D Advanced Dosimetry
2.4. Clinical Follow-Up, Treatment Response, and Toxicity Assessment
2.5. Statistics
3. Results
4. Discussion
- (1)
- Cold spots of volume >20 cc based on immediate post-TARE Y-90 dosimetric analysis trigger early imaging follow up. If there is anatomic concordance between regions of underdosing identified by dosimetry and areas of concern for residual disease in early imaging, informed by close attention to tumor marker dynamics, then these factors trigger multidisciplinary review and the discussion of early retreatment.
- (2)
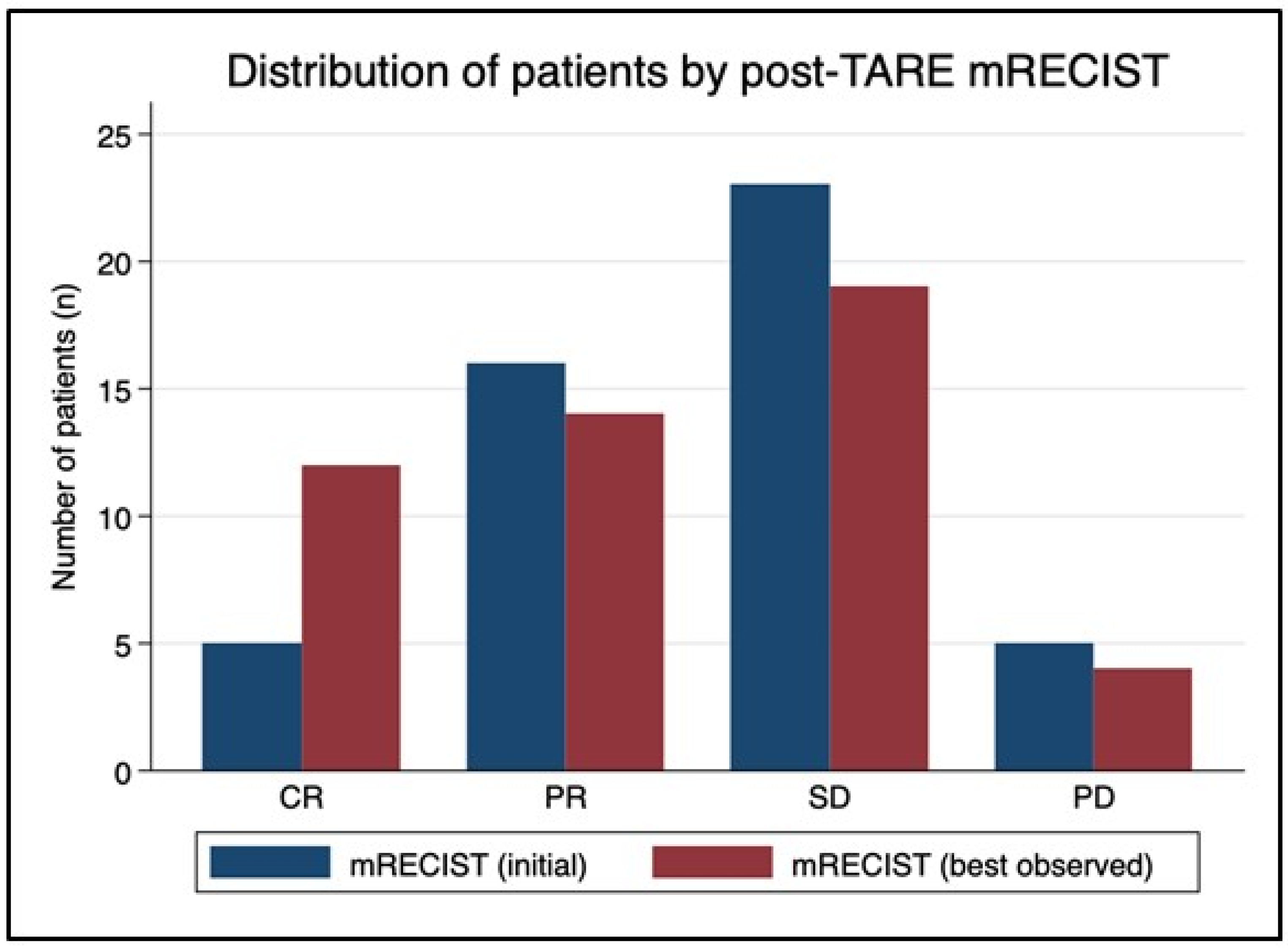
- If post-TARE dosimetry identifies excellent coverage of the tumor without cold volumes of significance, then early imaging follow-up is deferred to the norm of 3 months, and even then a finding on imaging of apparent residual disease or recurrence is met with caution, as median time to best mRECIST response in our cohort was 6 months, with a range beyond a year. Radiology assessments of post-TARE imaging are often the primary determinant for or against repeat intervention. Our findings provide evidence that conventional radiology at 3 months can miss a migration toward treatment response 30% of the time (12 out of 41 patients migrated toward OR after initial post-treatment imaging study). mRECIST guidelines remain the standard for the assessment of HCC response to local and systemic therapy [44], but volumetric dosimetry appears capable of supplementing and refining its utility in the post-TARE setting.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benson, A.B.; D’Angelica, M.I.; Abbott, D.E.; Abrams, T.A.; Alberts, S.R.; Anaya, D.A.; Anders, R.; Are, C.; Brown, D.; Chang, D.T.; et al. Guidelines Insights: Hepatobiliary Cancers, Version 2.2019. J. Natl. Compr. Cancer Netw. 2019, 17, 302–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, A.; Nag, S.; Salem, R.; Murthy, R.; McEwan, A.J.; Nutting, C.; Benson, A., 3rd; Espat, J.; Bilbao, I.J.; Sharma, R.A.; et al. Recommendations for Radioembolization of Hepatic Malignancies Using Yttrium-90 Microsphere Brachytherapy: A Consensus Panel Report from the Radioembolization Brachytherapy Oncology Consortium. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Biersack, H.-J.; Ezziddin, S. Radioembolization of Liver Tumors with Yttrium-90 Microspheres. Semin. Nucl. Med. 2010, 40, 105–121. [Google Scholar] [CrossRef] [Green Version]
- Hilgard, P.; Hamami, M.; Fouly, A.E.; Scherag, A.; Müller, S.; Ertle, J.; Heusner, T.; Cicinnati, V.R.; Paul, A.; Bockisch, A.; et al. Radioembolization with yttrium-90 glass microspheres in hepatocellular carcinoma: European experience on safety and long-term survival. Hepatology 2010, 52, 1741–1749. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Gordon, A.C.; Mouli, S.; Hickey, R.; Kallini, J.; Gabr, A.; Mulcahy, M.F.; Baker, T.; Abecassis, M.; Miller, F.H.; et al. Y90 Radioembolization Significantly Prolongs Time to Progression Compared with Chemoembolization in Patients with Hepatocellular Carcinoma. Gastroenterology 2016, 151, 1155–1163.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangro, B.; Carpanese, L.; Cianni, R.; Golfieri, R.; Gasparini, D.; Ezziddin, S.; Paprottka, P.M.; Fiore, F.; Van Buskirk, M.; Bilbao, J.I.; et al. Survival after yttrium-90 resin microsphere radioembolization of hepatocellular carcinoma across Barcelona clinic liver cancer stages: A European evaluation. Hepatology 2011, 54, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Haste, P.; Tann, M.; Persohn, S.; LaRoche, T.; Aaron, V.; Mauxion, T.; Chauhan, N.; Dreher, M.R.; Johnson, M.S. Correlation of Technetium-99m Macroaggregated Albumin and Yttrium-90 Glass Microsphere Biodistribution in Hepatocellular Carcinoma: A Retrospective Review of Pretreatment Single Photon Emission CT and Posttreatment Positron Emission Tomography/CT. J. Vasc. Interv. Radiol. 2017, 28, 722–730.e1. [Google Scholar] [CrossRef]
- Kafrouni, M.; Allimant, C.; Fourcade, M.; Vauclin, S.; Guiu, B.; Mariano-Goulart, D.; Ben Bouallègue, F. Analysis of differences between 99mTc-MAA SPECT- and 90Y-microsphere PET-based dosimetry for hepatocellular carcinoma selective internal radiation therapy. EJNMMI Res. 2019, 9, 62. [Google Scholar] [CrossRef] [Green Version]
- Wondergem, M.; Smits, M.L.; Elschot, M.; de Jong, H.W.; Verkooijen, H.M.; van den Bosch, M.A.; Nijsen, J.F.; Lam, M.G. 99mTc-macroaggregated albumin poorly predicts the intrahepatic distribution of 90Y resin microspheres in hepatic radioembolization. J. Nucl. Med. 2013, 54, 1294–1301. [Google Scholar] [CrossRef] [Green Version]
- Vilgrain, V.; Pereira, H.; Assenat, E.; Guiu, B.; Ilonca, A.D.; Pageaux, G.-P.; Sibert, A.; Bouattour, M.; Lebtahi, R.; Allaham, W.; et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): An open-label randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1624–1636. [Google Scholar] [CrossRef]
- Hermann, A.-L.; Dieudonné, A.; Ronot, M.; Sanchez, M.; Pereira, H.; Chatellier, G.; Garin, E.; Castera, L.; Lebtahi, R.; Vilgrain, V. Relationship of Tumor Radiation–absorbed Dose to Survival and Response in Hepatocellular Carcinoma Treated with Transarterial Radioembolization with 90Y in the SARAH Study. Radiology 2020, 296, 673–684. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.; Garin, E.; Maccauro, M.; Kappadath, S.C.; Sze, D.Y.; Turkmen, C.; Cantasdemir, M.; Haste, P.; Herrmann, K.; Alsuhaibani, H.S.; et al. A global evaluation of advanced dosimetry in transarterial radioembolization of hepatocellular carcinoma with Yttrium-90: The TARGET study. Eur. J. Nucl. Med. 2022, 49, 3340–3352. [Google Scholar] [CrossRef]
- Bentzen, S.M.; Constine, L.S.; Deasy, J.O.; Eisbruch, A.; Jackson, A.; Marks, L.B.; Haken, R.K.T.; Yorke, E.D. Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC): An Introduction to the Scientific Issues. Int. J. Radiat. Oncol. 2010, 76, S3–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grégoire, V.; Mackie, T. State of the art on dose prescription, reporting and recording in Intensity-Modulated Radiation Therapy (ICRU report No. 83). Cancer Radiother. 2011, 15, 555–559. [Google Scholar] [CrossRef]
- Dean, M.J.R.; Mellon, E.; Fields, E.; Yechieli, R.; Mak, R. CB-CHOP: A simple acronym for evaluating a radiation treatment plan. Appl. Rad. Oncol. 2017, 6, 28–30. [Google Scholar]
- Moran, V.; Prieto, E.; Sancho, L.; Rodriguez-Fraile, M.; Soria, L.; Zubiria, A.; Marti-Climent, J.M. Impact of the dosimetry approach on the resulting (90)Y radioembolization planned absorbed doses based on (99m)Tc-MAA SPECT-CT: Is there agreement between dosimetry methods? EJNMMI Phys. 2020, 7, 72. [Google Scholar] [CrossRef]
- Braat, A.J.; Smits, M.L.; Braat, M.N.; Hoven, A.F.V.D.; Prince, J.F.; de Jong, H.W.; Bosch, M.A.V.D.; Lam, M.G. 90Y Hepatic Radioembolization: An Update on Current Practice and Recent Developments. J. Nucl. Med. 2015, 56, 1079–1087. [Google Scholar] [CrossRef] [Green Version]
- Siman, W.; Mikell, J.K.; Kappadath, S.C. Practical reconstruction protocol for quantitative 90 Y bremsstrahlung SPECT/CT. Med. Phys. 2016, 43, 5093–5103. [Google Scholar] [CrossRef] [Green Version]
- Dewaraja, Y.K.; Chun, S.Y.; Srinivasa, R.N.; Kaza, R.K.; Cuneo, K.C.; Majdalany, B.S.; Novelli, P.M.; Ljungberg, M.; Fessler, J.A. Improved quantitative90Y bremsstrahlung SPECT/CT reconstruction with Monte Carlo scatter modeling. Med. Phys. 2017, 44, 6364–6376. [Google Scholar] [CrossRef] [Green Version]
- Kataria, T.; Sharma, K.; Subramani, V.; Karrthick, K.P.; Bisht, S.S. Homogeneity Index: An objective tool for assessment of conformal radiation treatments. J. Med. Phys. 2012, 37, 207–213. [Google Scholar] [CrossRef]
- Feuvret, L.; Noel, G.; Mazeron, J.J.; Bey, P. Conformity index: A review. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, P.; Sebestyen, Z.; Farkas, R.; Bellyei, S.; Szigeti, A.; Gulyban, A.; Horvath, Z.; Doczi, T.; Mangel, L. Conformal stereotactic radiosurgery therapy: Plan evaluation methods and results. Magy. Onkol. 2011, 55, 85–90. [Google Scholar] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, L.; Xu, Y.; Chen, X.; Xie, X.; Liang, B.; Dai, J. A new homogeneity index definition for evaluation of radiotherapy plans. J. Appl. Clin. Med. Phys. 2019, 20, 50–56. [Google Scholar] [CrossRef]
- Ballangrud, A.; Kuo, L.; Happersett, L.; Lim, S.; Li, X.; Beal, K.; Yamada, Y.; LoSasso, T.; Mechalakos, J. SU-F-T-613: Multi-Lesion Cranial SRS VMAT Plan Quality. Med. Phys. 2016, 43, 3604–3605. [Google Scholar] [CrossRef]
- Tas, B.; Durmus, I.F.; Okumus, A.; Uzel, O.E. Correlation between Heterogeneity index (HI) and Gradient Index (GI) for high dose stereotactic radiotherapy/radiosurgery (SRT/SRS). AIP Conf. Proc. 2017, 1815, 90004. [Google Scholar] [CrossRef]
- Paliwal, B.R.; Bayouth, J.E.; Saenz, D.L. A dose homogeneity and conformity evaluation between ViewRay and pinnacle-based linear accelerator IMRT treatment plans. J. Med. Phys. 2014, 39, 64–70. [Google Scholar] [CrossRef]
- Chan, K.T.; Alessio, A.M.; Johnson, G.E.; Vaidya, S.; Kwan, S.W.; Monsky, W.; Wilson, A.E.; Lewis, D.H.; Padia, S.A. Prospective Trial Using Internal Pair-Production Positron Emission Tomography to Establish the Yttrium-90 Radioembolization Dose Required for Response of Hepatocellular Carcinoma. Int. J. Radiat. Oncol. 2018, 101, 358–365. [Google Scholar] [CrossRef]
- Srinivas, S.M.; Natarajan, N.; Kuroiwa, J.; Gallagher, S.; Nasr, E.; Shah, S.N.; DiFilippo, F.P.; Obuchowski, A.N.; Bazerbashi, B.; Yu, N.; et al. Determination of Radiation Absorbed Dose to Primary Liver Tumors and Normal Liver Tissue Using Post-Radioembolization 90Y PET. Front. Oncol. 2014, 4, 255. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.S.; Paeng, J.C.; Kim, H.C.; Chung, J.W.; Cheon, G.J.; Chung, J.K.; Lee, D.S.; Kang, K.W. PET/CT-Based Dosimetry in 90Y-Microsphere Selective Internal Radiation Therapy: Single Cohort Comparison With Pretreatment Planning on (99m)Tc-MAA Imaging and Correlation with Treatment Efficacy. Medicine 2015, 94, e945. [Google Scholar] [CrossRef]
- Strigari, L.; Sciuto, R.; Rea, S.; Carpanese, L.; Pizzi, G.; Soriani, A.; Iaccarino, G.; Benassi, M.; Ettorre, G.M.; Maini, C.L. Efficacy and Toxicity Related to Treatment of Hepatocellular Carcinoma with 90Y-SIR Spheres: Radiobiologic Considerations. J. Nucl. Med. 2010, 51, 1377–1385. [Google Scholar] [CrossRef] [PubMed]
- Gray, B.N.; Burton, M.A.; Kelleher, D.K.; Anderson, J.; Klemp, P. Selective internal radiation (SIR) therapy for treatment of liver metastases: Measurement of response rate. J. Surg. Oncol. 1989, 42, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.Y.; Leung, W.T.; Ho, S.; Leung, N.W.; Chan, M.; Lin, J.; Metreweli, C.; Johnson, P.; Li, A.K. Treatment of inoperable hepatocellular carcinoma with intrahepatic arterial yttrium-90 microspheres: A phase I and II study. Br. J. Cancer 1994, 70, 994–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, M.A.; Gray, B.N.; Klemp, P.F.; Kelleher, D.K.; Hardy, N. Selective internal radiation therapy: Distribution of radiation in the liver. Eur. J. Cancer Clin. Oncol. 1989, 25, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- Wollner, I.; Knutsen, C.; Smith, P.; Prieskorn, D.; Chrisp, C.; Andrews, J.; Juni, J.; Warber, S.; Kleveringm, J.; Crudup, J.; et al. Effects of hepatic arterial yttrium 90 glass microspheres in dogs. Cancer 1988, 61, 1336–1344. [Google Scholar] [CrossRef]
- Sun, J.; Zhang, T.; Wang, J.; Li, W.; Zhang, A.; He, W.; Zhang, D.; Li, D.; Ding, J.; Duan, X. Biologically effective dose (BED) of stereotactic body radiation therapy (SBRT) was an important factor of therapeutic efficacy in patients with hepatocellular carcinoma (</=5 cm). BMC Cancer 2019, 19, 846. [Google Scholar]
- Spieler, B.; Portelance, L.; Mellon, E. Stereotactic ablative radiation therapy in the treatment of liver tumors. Appl. Radiat. Oncol. 2018, 7, 17–23. [Google Scholar]
- Spieler, B.M.E.; Jones, P.D.; Giap, H.; Feun, L.; Venkat, S.; Portelance, L. Stereotactic ablative radiotherapy for hepatocellular carcinoma. Hepatoma Res. 2019, 5, 4. [Google Scholar] [CrossRef]
- Sapir, E.; Tao, Y.; Schipper, M.J.; Bazzi, L.; Novelli, P.M.; Devlin, P.; Owen, D.; Cuneo, K.C.; Lawrence, T.S.; Parikh, N.D.; et al. Stereotactic Body Radiation Therapy as an Alternative to Transarterial Chemoembolization for Hepatocellular Carcinoma. Int. J. Radiat. Oncol. 2017, 100, 122–130. [Google Scholar] [CrossRef]
- Mahadevan, A.; Blanck, O.; Lanciano, R.; Peddada, A.; Sundararaman, S.; D’Ambrosio, D.; Sharma, S.; Perry, D.; Kolker, J.; Davis, J. Stereotactic Body Radiotherapy (SBRT) for liver metastasis—Clinical outcomes from the international multi-institutional RSSearch(R) Patient Registry. Radiat. Oncol. 2018, 13, 26. [Google Scholar] [CrossRef] [Green Version]
- Kok, E.N.D.; Jansen, E.P.M.; Heeres, B.C.; Kok, N.F.M.; Janssen, T.; van Werkhoven, E.; Sanders, F.R.K.; Ruers, T.J.M.; Nowee, M.E.; Kuhlmann, K.F.D. High versus low dose Stereotactic Body Radiation Therapy for hepatic metastases. Clin. Transl. Radiat. Oncol. 2020, 20, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seldon, C.; Thornton, L.; Ezuddin, N.; Yang, B.; Zikria, J.; Venkat, S.; Mohan, P.; Studenski, M.; Portelance, L.; Spieler, B. Can Post-Treatment Dosimetry Predict Clinical Outcomes in Segmental Transarterial Radioembolization of Hepatocellular Carcinoma? Int. J. Radiat. Oncol. 2022, 114, e179–e180. [Google Scholar] [CrossRef]
- Granito, A.; Forgione, A.; Marinelli, S.; Renzulli, M.; Ielasi, L.; Sansone, V.; Benevento, F.; Piscaglia, F.; Tovoli, F. Experience with regorafenib in the treatment of hepatocellular carcinoma. Ther. Adv. Gastroenterol. 2021, 14, 17562848211016959. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Lencioni, R. mRECIST for HCC: Performance and novel refinements. J. Hepatol. 2020, 72, 288–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velec, M.; Haddad, C.R.; Craig, T.; Wang, L.; Lindsay, P.; Brierley, J.; Brade, A.; Ringash, J.; Wong, R.K.; Kim, J.; et al. Predictors of Liver Toxicity Following Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 939–946. [Google Scholar] [CrossRef]
- Lam, M.G.E.H.; Louie, J.D.; Iagaru, A.H.; Goris, M.L.; Sze, D.Y. Safety of Repeated Yttrium-90 Radioembolization. Cardiovasc. Interv. Radiol. 2013, 36, 1320–1328. [Google Scholar] [CrossRef]
- Badar, W.; Van Ha, T.; Zangan, S.; Navuluri, R.; Pillai, A.; Baker, T.; Dalag, L.; Han, R.; Ahmed, O. Safety and efficacy of repeat Y90 radioembolization to the same hepatic arterial territory. Br. J. Radiol. 2021, 94, 20200752. [Google Scholar] [CrossRef]
- Masthoff, M.; Schindler, P.; Harders, F.; Heindel, W.; Wilms, C.; Schmidt, H.H.; Pascher, A.; Stegger, L.; Rahbar, K.; Wildgruber, M.; et al. Repeated radioembolization in advanced liver cancer. Ann. Transl. Med. 2020, 8, 1055. [Google Scholar] [CrossRef]
- Hardy-Abeloos, C.; Lazarev, S.; Ru, M.; Kim, E.; Fischman, A.; Moshier, E.; Rosenzweig, K.; Buckstein, M. Safety and Efficacy of Liver Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma After Segmental Transarterial Radioembolization. Int. J. Radiat. Oncol. 2019, 105, 968–976. [Google Scholar] [CrossRef] [Green Version]
- Padia, S.A.; Alessio, A.; Kwan, S.W.; Lewis, D.H.; Vaidya, S.; Minoshima, S. Comparison of Positron Emission Tomography and Bremsstrahlung Imaging to Detect Particle Distribution in Patients Undergoing Yttrium-90 Radioembolization for Large Hepatocellular Carcinomas or Associated Portal Vein Thrombosis. J. Vasc. Interv. Radiol. 2013, 24, 1147–1153. [Google Scholar] [CrossRef]
- Trotta, N.; Collette, B.; Mathey, C.; Vierasu, I.; Bucalau, A.; Verset, G.; Moreno-Reyes, R.; Goldman, S. Comparison of PMT-based TF64 and SiPM-based Vereos PET/CT systems for 90Y imaging and dosimetry optimization: A quantitative study. Med. Phys. 2022, 49, 7567–7582. [Google Scholar] [CrossRef] [PubMed]
- Studenski, M.; Witte, M.; Spieler, B.; Georgiou, M.F.; Portelance, L. Comparison of Two Commercial Software Packages for Y-90 SIRT Dosimetry; AAPM ePoster Library: Alexandria, VA, USA, 2020. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Variable | N | % | Clinical Variable | N | % | |
|---|---|---|---|---|---|---|
| Patients | 43 | 100 | All | 43 | 100 | |
| Gender | Child Pugh score | |||||
| Female | 10 | 23.3 | A | 40 | 93.0 | |
| Male | 33 | 76.7 | B | 3 | 7.0 | |
| Ethnicity | BCLC Stage | |||||
| Asian | 1 | 2.3 | A | 12 | 27.9 | |
| Black | 5 | 11.6 | B | 18 | 41.9 | |
| Hispanic | 10 | 23.3 | C | 13 | 30.2 | |
| Multiracial | 1 | 2.3 | Prior RFA | |||
| White | 26 | 60.5 | No | 40 | 93.0 | |
| Alcohol | Yes | 3 | 7.0 | |||
| No | 29 | 67.4 | Prior SABR | |||
| Yes | 14 | 32.6 | No | 41 | 95.3 | |
| HCV | Yes | 2 | 4.7 | |||
| No | 23 | 53.5 | Prior TACE | |||
| Yes | 20 | 46.5 | No | 35 | 81.4 | |
| NASH | Yes | 8 | 18.6 | |||
| No | 31 | 72.1 | Prior resection | |||
| Yes | 12 | 27.9 | No | 41 | 95.3 | |
| Hemochromatosis | Yes | 2 | 4.7 | |||
| No | 41 | 95.3 | Prior MWA | |||
| Yes | 2 | 4.7 | No | 39 | 90.7 | |
| Tumor distribution | Yes | 4 | 9.3 | |||
| Diffuse | 2 | 4.7 | ECOG score | |||
| Multifocal | 26 | 60.5 | 0 | 22 | 51.2 | |
| Unifocal | 15 | 34.9 | 1 | 20 | 46.5 | |
| Portal HTN on imaging | 2 | 1 | 2.3 | |||
| Unknown | 1 | 2.3 | ||||
| Absent | 26 | 60.5 | TARE treatments | 51 | 100 | |
| Present | 16 | 37.2 | Theraspheres | 30 | 58.8 | |
| Portal vein tumor thrombus | SIRSpheres | 21 | 41.2 | |||
| No | 29 | 67.4 | ||||
| Yes | 14 | 32.6 | ||||
| Clinical Variable | Median | Minimum | Maximum | Std Dev | ||
| age | 67 | 48 | 86 | 7.95 | ||
| AFP | 58.2 | 1.6 | 60,500 | 13,020 | ||
| albumin | 3.9 | 1.3 | 4.7 | 0.56 | ||
| bilirubin | 0.9 | 0.20 | 2.6 | 0.54 | ||
| INR | 1.13 | 0.93 | 2.1 | 0.19 | ||
| creatinine | 0.90 | 0.39 | 5.6 | 0.83 | ||
| MELD score | 6.5 | 0.64 | 16.8 | 4.11 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taswell, C.S.; Studenski, M.; Pennix, T.; Stover, B.; Georgiou, M.; Venkat, S.; Jones, P.; Zikria, J.; Thornton, L.; Yechieli, R.; et al. For Hepatocellular Carcinoma Treated with Yttrium-90 Microspheres, Dose Volumetrics on Post-Treatment Bremsstrahlung SPECT/CT Predict Clinical Outcomes. Cancers 2023, 15, 645. https://doi.org/10.3390/cancers15030645
Taswell CS, Studenski M, Pennix T, Stover B, Georgiou M, Venkat S, Jones P, Zikria J, Thornton L, Yechieli R, et al. For Hepatocellular Carcinoma Treated with Yttrium-90 Microspheres, Dose Volumetrics on Post-Treatment Bremsstrahlung SPECT/CT Predict Clinical Outcomes. Cancers. 2023; 15(3):645. https://doi.org/10.3390/cancers15030645
Chicago/Turabian StyleTaswell, Crystal Seldon, Matthew Studenski, Thomas Pennix, Bryan Stover, Mike Georgiou, Shree Venkat, Patricia Jones, Joseph Zikria, Lindsay Thornton, Raphael Yechieli, and et al. 2023. "For Hepatocellular Carcinoma Treated with Yttrium-90 Microspheres, Dose Volumetrics on Post-Treatment Bremsstrahlung SPECT/CT Predict Clinical Outcomes" Cancers 15, no. 3: 645. https://doi.org/10.3390/cancers15030645