
Quality of Life (QoL) of Children and Adolescents Participating in a Precision Medicine Trial for High-Risk Childhood Cancer
 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
- What proportion of patients have difficulty in QoL domains at enrolment in a precision medicine trial for high-risk childhood cancer, and following receipt of trial results?
- Does patient QoL change from enrolment to following receipt of trial results?
- What are the predictors of patient QoL at trial enrolment and following receipt of trial results?
- What is the concordance between parent-proxy and patient self-report QoL?
2. Materials and Methods
2.1. Study Design
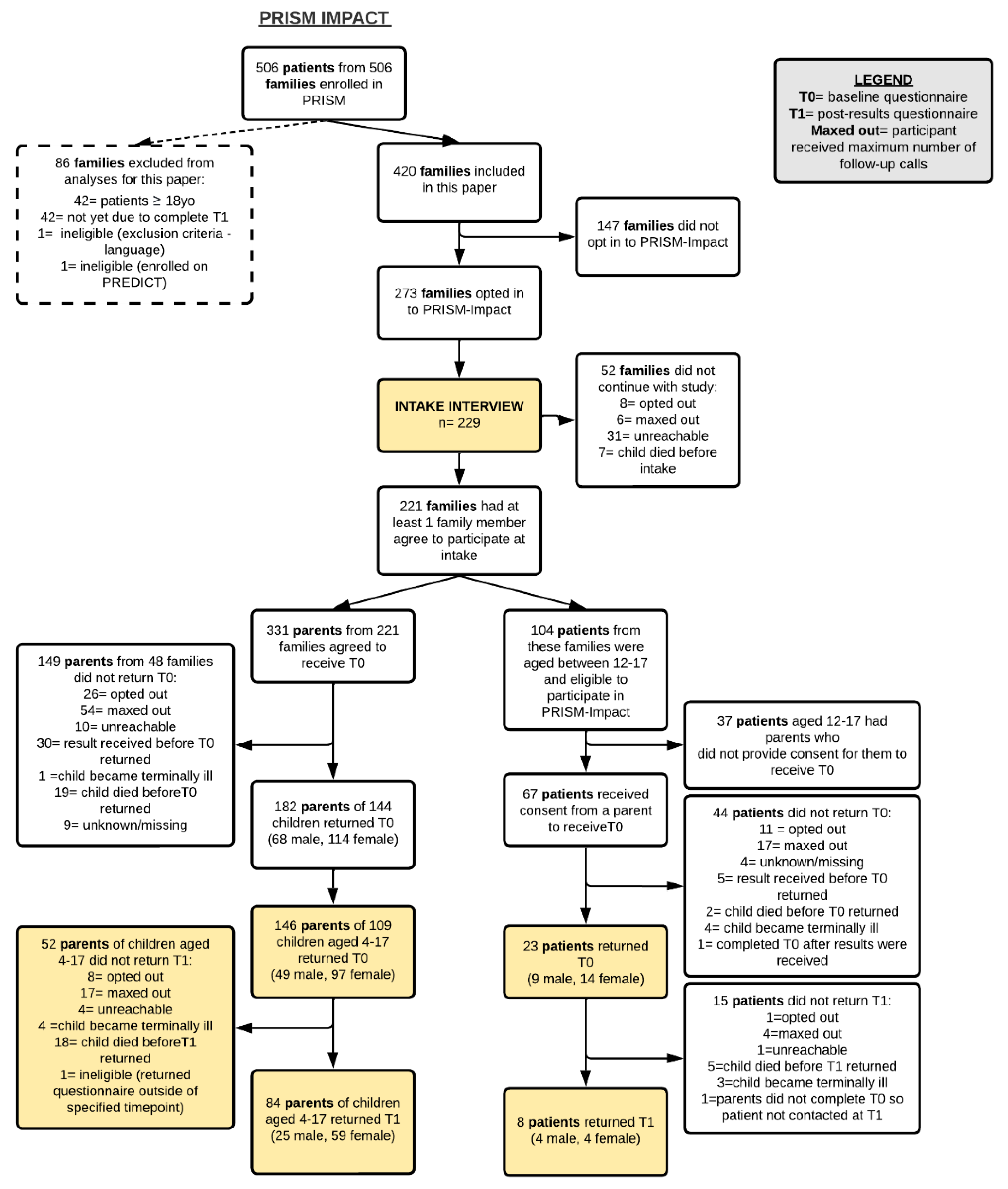
2.2. Participants
2.3. Procedures
2.4. Data Collection and Measures
2.4.1. Demographics
2.4.2. Clinical Information
2.4.3. MTB Outcomes
2.4.4. Patient QoL
2.5. Data Analysis
3. Results
3.1. Participant Demographics (Table 1 and Table 2)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parents With a Child Aged 4–17 at T0 (n = 136) | |
|---|---|
| Age, years | |
| Mean (SD) | 43.6 (6.3) |
| Median (IQR) | 43 (40, 47) |
| Range | 29–67 |
| (missing) | 1 |
| Gender, n (%) | |
| Female | 87 (64%) |
| Male | 49 (36%) |
| Highest level of education, n (%) | |
| High school only | 23 (17%) |
| Post High school (inc. vocational training) | 113 (83%) |
| Employment, n (%) | |
| Employed: Full-time | 66 (48.8%) |
| Employed: Part-time/casual | 38 (28.2%) |
| Not employed: Actively seeking work | 4 (3%) |
| Not employed: Not seeking work/retired/student | 9 (6.7%) |
| Not employed: Home duties | 18 (13.3%) |
| (missing) | 1 |
| Cultural or language diversity, n (%) | |
| First language English, Western/European | 102 (77.9%) |
| First language English, non-Western/European | 10 (7.6%) |
| First language other than English | 19 (14.5%) |
| (missing) | 5 |
| Rurality, n (%) | |
| Capital city | 88 (68.2%) |
| Other metropolitan centre | 10 (7.8%) |
| Rural/remote area | 31 (24%) |
| (missing) | 7 |
| Marital Status, n (%) | |
| Currently married or de facto | 119 (88%) |
| Separated/ divorced/ previous de facto | 16 (12%) |
| Widowed | 1 (1%) |
| Never married/ never de facto | 0 (0%) |
| Household income, n (%) | |
| Nil income | 7 (5.2%) |
| Less than $29,999 | 7 (5.2%) |
| $30,000–$59,000 | 14 (10.5%) |
| $60,000–$89,000 | 28 (20.9%) |
| $90,000–$120,000 | 14 (10.5%) |
| Greater than $120,000 | 50 (37.3%) |
| Prefer not to answer | 14 (10.5%) |
| (missing) | 2 |
| Number of other children, n (%) | |
| 0 | 20 (14.8%) |
| 1 | 47 (34.8%) |
| 2–3 | 59 (43.7%) |
| 4+ | 9 (6.7%) |
| (missing) | 1 |
| Patients Aged 4–17 Years Whose Parents Reported on QoL at T0 (n = 109) | Patients Aged 12–17 Years Who Self-Reported on QoL at T0 (n = 23) | |
|---|---|---|
| Age, years | ||
| Mean (SD) | 11.3 (4.2) | 14.8 (1.9) |
| Median (IQR) | 12 (8, 15) | 15 (13, 17) |
| Range | 4–17 | 12–17 |
| Gender, n (%) | ||
| Female | 49 (45%) | 14 (61%) |
| Male | 60 (55%) | 9 (39%) |
| Age of patient at time of diagnosis, years | ||
| Mean (SD) | 10.0 (4.5) | 13.0 (2.8) |
| Median (IQR) | 10 (6, 14) | 13.5 (11, 15.25) |
| Range | 0–17 | 7–17 |
| Diagnosis, n (%) | ||
| Central Nervous System | 42 (39%) | 5 (22%) |
| Sarcoma | 34 (31%) | 12 (52%) |
| Leukemia/Lymphoma | 14 (13%) | 4 (17%) |
| Neuroblastoma | 9 (8%) | 0 (0%) |
| Other | 10 (9%) | 2 (9%) |
| Number of relapses for patient prior to PRISM consent, n (%) | ||
| 0 | 46 (42%) | 11 (48%) |
| 1 | 47 (43%) | 10 (44%) |
| ≥2 | 16 (15%) | 2 (9%) |
| Received cancer treatment while awaiting testing results | ||
| Yes | 87 (79.8%) | 20 (87%) |
| No | 22 (20.2%) | 3 (13%) |
| Time (days) from initial cancer diagnosis * to PRISM enrolment | ||
| Median (IQR) | 418.5 (11.5, 818) | 359 (83, 699) |
| Range | 0–5586 | 1–4023 |
| Time (days) from cancer event ** resulting in patient being eligible for PRISM and enrolment | ||
| Median (IQR) | 6 (1, 16.5) | 7 (1, 49) |
| Range | 0–834 | 0–155 |
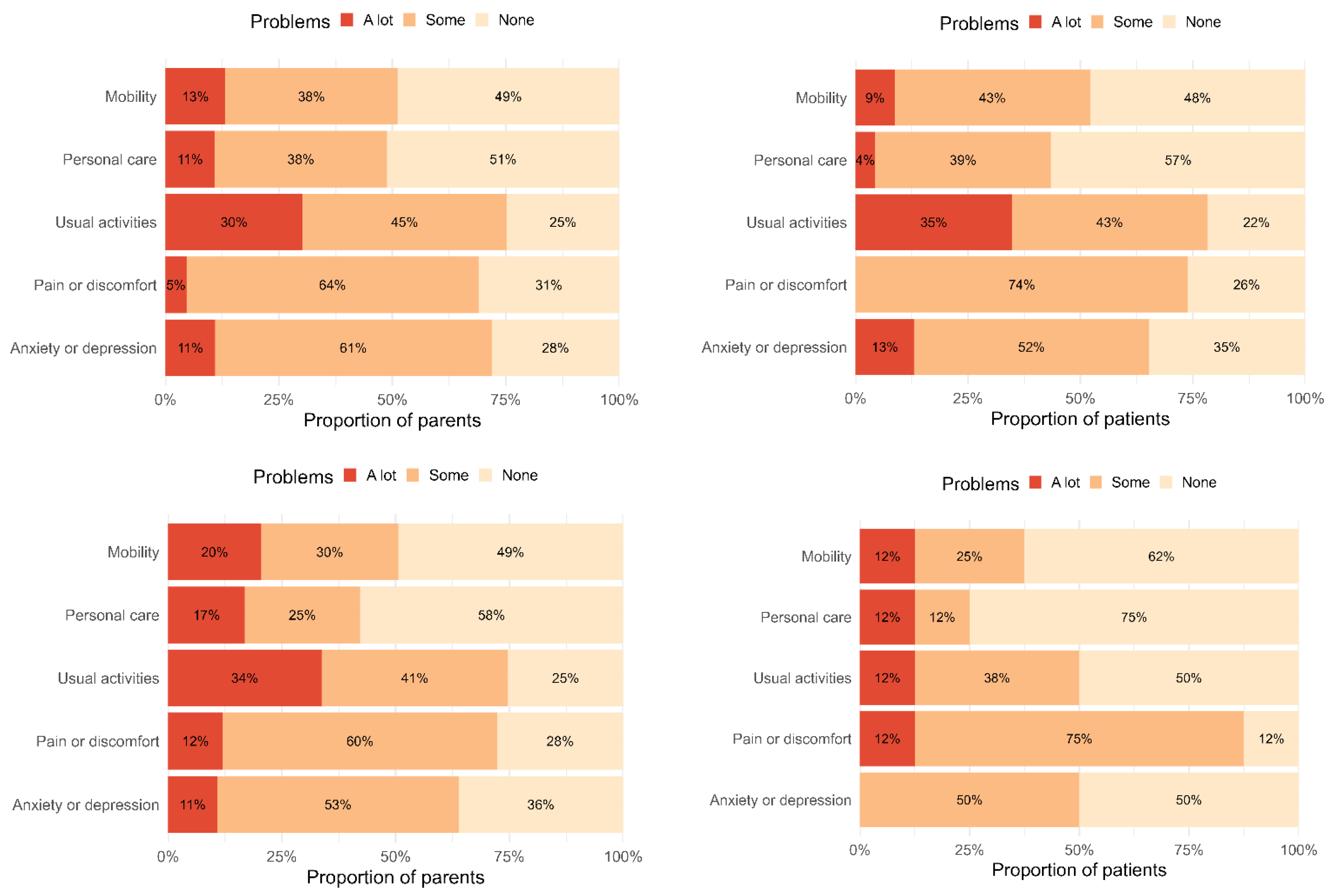
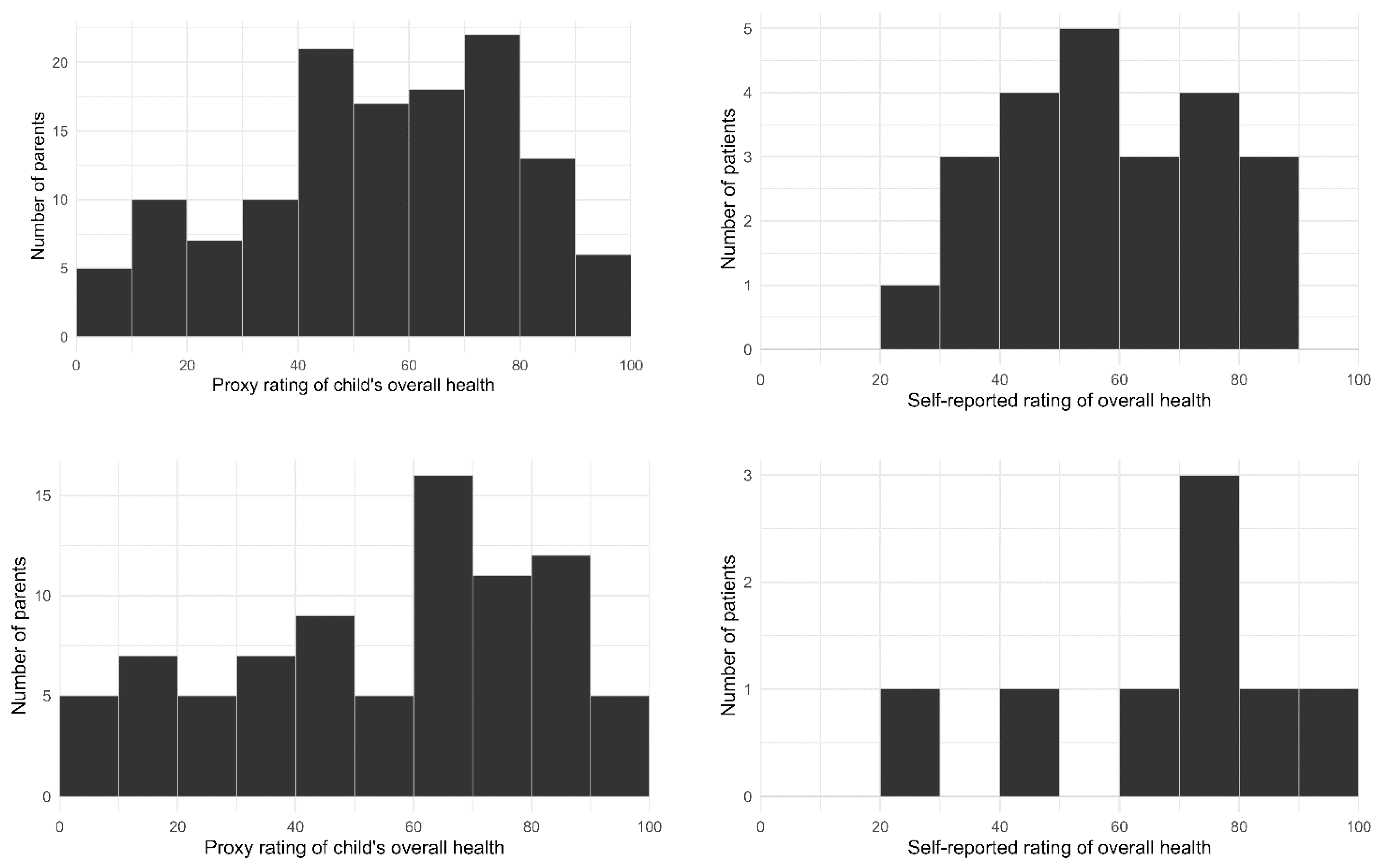
3.2. Patient QoL Shortly after Trial Enrolment (Table 3 and Table 4, Figure 2 and Figure 3)


| Parent-Proxy Reported QoL for Patients Aged 4–17 Years | Self-Reported QoL for Patients Aged 12–17 Years | |||
|---|---|---|---|---|
| T0 (n = 136) 1 | T1 (n = 84) 2 | T0 (n = 23) | T1 (n = 8) | |
| Domain | n, Valid % | n, Valid % | n, Valid % | n, Valid % |
| Problems with mobility (walking about) | ||||
| None | 63 (49%) | 4 (49%) | 11 (48%) | 5 (63%) |
| Some | 49 (38%) | 25 (30%) | 10 (44%) | 2 (25%) |
| A lot | 17 (13%) | 17 (21%) | 2 (9%) | 1 (13%) |
| Problems with self-care (looking after him/herself) | ||||
| None | 66 (51%) | 48 (58%) | 13 (57%) | 6 (75%) |
| Some | 49 (38%) | 21 (25%) | 9 (39%) | 1 (13%) |
| A lot | 14 (11%) | 14 (17%) | 1 (4%) | 1 (13%) |
| Problems doing usual activities | ||||
| None | 32 (25%) | 21 (25%) | 5 (22%) | 4 (50%) |
| Some | 58 (45%) | 34 (41%) | 10 (44%) | 3 (38%) |
| A lot | 39 (30%) | 28 (34%) | 8 (35%) | 1 (13%) |
| Having pain or discomfort | ||||
| None | 40 (31%) | 23 (28%) | 6 (26%) | 1 (13%) |
| Some | 83 (34%) | 50 (60%) | 17 (74%) | 6 (75%) |
| A lot | 6 (5%) | 10 (12%) | 0 (0%) | 1 (13%) |
| Feeling worried, sad or unhappy | ||||
| None | 36 (28%) | 30 (36%) | 8 (35%) | 4 (50%) |
| A bit | 78 (61%) | 44 (53%) | 12 (52%) | 4 (50%) |
| Very | 14 (11%) | 9 (11%) | 3 (13%) | 0 (0%) |
| Number of Domains | Parent-Proxy | Self-Report | ||
|---|---|---|---|---|
| T0 (N = 128) | T1 (N = 83) | T0 (N = 23) | T1 (N = 8) | |
| n (%) | n (%) | n (%) | n (%) | |
| 0 | 11 (9%) | 9 (11%) | 0 (0%) | 1 (12%) |
| 1 | 11 (9%) | 9 (11%) | 4 (17%) | 1 (12%) |
| 2 | 25 (20%) | 13 (16%) | 4 (17%) | 2 (25%) |
| 3 | 20 (16%) | 15 (18%) | 4 (17%) | 2 (25%) |
| 4 | 22 (17%) | 13 (16%) | 7 (30%) | 1 (12%) |
| 5 | 39 (30%) | 24 (29%) | 4 (17%) | 1 (12%) |
3.3. Patient QoL following Return of Results and Treatment Recommendations (Table 3 and Table 4, Figure 2 and Figure 3)
3.4. Change in QoL from Shortly after Enrolment to Following Receipt of Results (Table 5 and Table 6)
| Domain | Timepoint | Level of Problems, n (%) | OR | (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|---|
| None | Some | A lot | |||||
| Mobility | T0 | 35 (47%) | 26 (35%) | 13 (18%) | 1.50 | (0.74–3.01) | 0.260 |
| T1 | 34 (46%) | 23 (31%) | 17 (23%) | ||||
| Self-care | T0 | 39 (53%) | 27 (36%) | 8 (11%) | 0.93 | (0.45–1.90) | 0.840 |
| T1 | 43 (58%) | 19 (26%) | 12 (16%) | ||||
| Usual activities | T0 | 19 (26%) | 29 (39%) | 26 (35%) | 1.09 | (0.59–2.01) | 0.793 |
| T1 | 18 (24%) | 29 (39%) | 27 (36%) | ||||
| Pain/discomfort | T0 | 20 (27%) | 52 (70%) | 2 (3%) | 1.55 | (0.81–2.97) | 0.190 |
| T1 | 21 (28%) | 44 (59%) | 9 (12%) | ||||
| Anxiety/ depression | T0 | 21 (29%) | 44 (60%) | 8 (11%) | 0.72 | (0.37–1.41) | 0.343 |
| T1 | 25 (34%) | 41 (41%) | 7 (10%) | ||||
| Domain | Parent-Proxy | Self-Report | ||||||
|---|---|---|---|---|---|---|---|---|
| T1 | T1 | |||||||
| None | Some | A Lot | None | Some | A Lot | |||
| T0 | Mobility | None | 22 (30%) | 11 (15%) | 2 (3%) | 4 (50%) | 1 (12%) | 0 (0%) |
| Some | 11 (15%) | 9 (12%) | 6 (8%) | 1 (12%) | 1 (12%) | 0 (0%0 | ||
| A lot | 1 (1%) | 3 (4%) | 9 (12%) | 0 (0%) | 0 (0%) | 1 (12%) | ||
| Self-care | None | 29 (39%) | 7 (9%) | 3 (4%) | 6 (75%) | 0 (0%) | 0 (0%) | |
| Some | 14 (19%) | 9 (12%) | 4 (5%) | 0 (0%) | 1 (12%) | 1 (12%) | ||
| A lot | 0 (0%) | 3 (4%) | 5 (7%) | 0 (0%) | 0 (0%) | 0 (0%) | ||
| Usual activities | None | 10 (14%) | 6 (8%) | 3 (4%0 | 1 (12%) | 2 (25%) | 0 (0%) | |
| Some | 6 (8%) | 14 (19%) | 9 (12%) | 2 (25%) | 1 (12%) | 0 (0%) | ||
| A lot | 2 (3%) | 9 (12%) | 15 (20%) | 1 (12%) | 0 (0%) | 1 (12%) | ||
| Pain/ discomfort | None | 7 (9%) | 12 (16%) | 1 (1%) | 1 (12%) | 1 (12%) | 1 (12%) | |
| Some | 14 (19%) | 31 (42%) | 7 (9%) | 0 (0%) | 5 (62%) | 0 (0%) | ||
| A lot | 0 (0%) | 1 (1%) | 1 (1%) | 0 (0%) | 0 (0%) | 0 (0%) | ||
| Anxiety/ depression | None | 12 (16%) | 9 (12%) | 0 (0%) | 2 (25%) | 0 (0%) | 0 (0%) | |
| Some | 12 (16%) | 28 (38%) | 4 (5%) | 2 (25%) | 4 (50%) | 0 (0%) | ||
| A lot | 1 (1%) | 4 (5%) | 3 (4%) | 0 (0%) | 0 (0%) | 0 (0%) | ||
 Problem category unchanged at T1;
Problem category unchanged at T1;  Problem category indicates more difficulties at T1;
Problem category indicates more difficulties at T1;  Problem category indicates fewer difficulties at T1.
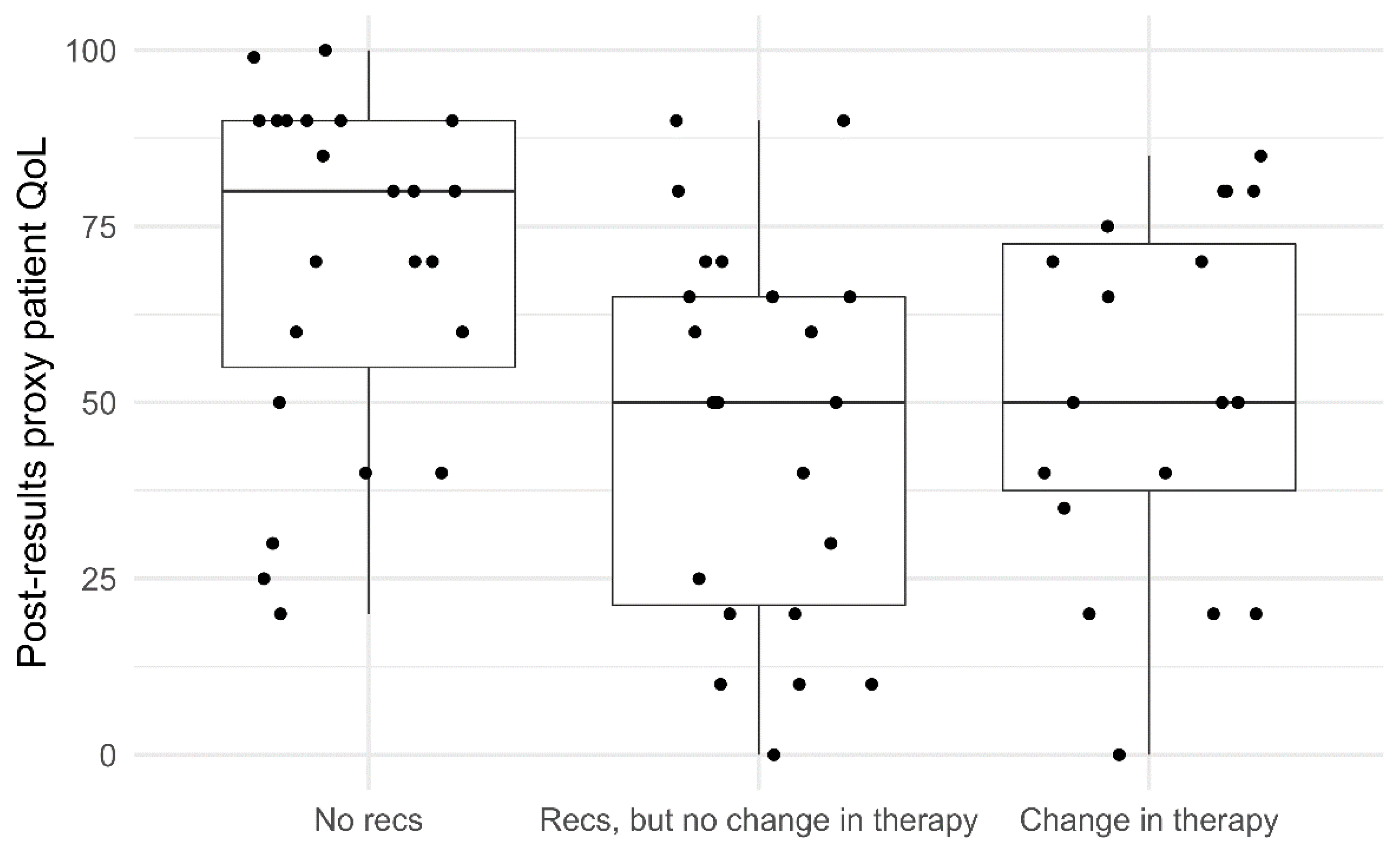
Problem category indicates fewer difficulties at T1.3.5. Factors Associated with Parent-Proxy Reported Patient QoL Shortly after Trial Enrolment and Following Receipt of Results (Table 7 and Figure 4)

| Associations between Characteristics and T0 Parent-Proxy EQ VAS (n = 129) * | ||||
|---|---|---|---|---|
| Predictor | Response Option | Difference | (95% CI) | p-value |
| Patient’s gender (vs. female) | Male | 2.7 | (−6.4, 11.9) | 0.562 |
| Patient’s diagnosis (vs. CNS) | Sarcoma | −4.3 | (−15.5, 6.9) | 0.457 |
| Leukaemia/Lymphoma | −8.0 | (−22.2, 6.2) | 0.275 | |
| Neuroblastoma | 13.2 | (−4.6, 31.0) | 0.151 | |
| Other | 4.2 | (−13.3, 21.5) | 0.641 | |
| Prior relapse (vs. no) | Yes | 6.5 | (−3.2, 16.3) | 0.194 |
| Age | Continuous variable | Smooth relationship | 0.509 | |
| Associations between MTB Treatment Recommendations and T1 Parent-Proxy EQ VAS (n = 64) * | ||||
| Predictor | Difference | (95% CI) | p-value | |
| Recommendation but no change (vs. no recommendation) | −22.5 | (−36.5, −8.5) | 0.006 | |
| Recommendation and change (vs. no recommendation) | −12.7 | (−27.3, 2.0) | 0.111 | |
3.6. Concordance between Parent-Proxy Reported Patient QoL and Patient Self-Reported QoL (Table 8)
| Pair Type | Domain | Weighted Kappa | 95% CI | Strength of Agreement |
|---|---|---|---|---|
| Mother-child | Mobility | 0.94 | 0.81–1.00 | Excellent |
| Personal care | 0.70 | 0.39–1.00 | Fair-Good | |
| Usual activities | 0.68 | 0.29–1.00 | Fair-Good | |
| Pain/discomfort | 0.00 | −0.56–0.56 | Poor | |
| Anxiety/depression | 0.13 | −0.45–0.70 | Poor | |
| Father-child | Mobility | 0.65 | 0.23–1.00 | Fair-Good |
| Personal care | 0.37 | −0.04–0.77 | Poor | |
| Usual activities | 0.25 | −0.28–0.79 | Poor | |
| Pain/discomfort | 0.42 | −0.17–1.00 | Fair-Good | |
| Anxiety/depression | 0.26 | −0.21–0.72 | Poor |
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forrest, S.J.; Geoerger, B.; Janeway, K.A. Precision medicine in pediatric oncology. Curr. Opin. Pediatr. 2018, 30, 17–24. [Google Scholar] [CrossRef]
- Langenberg, K.P.S.; Looze, E.J.; Molenaar, J.J. The Landscape of Pediatric Precision Oncology: Program Design, Actionable Alterations, and Clinical Trial Development. Cancers 2021, 13, 4324. [Google Scholar] [CrossRef]
- Momani, T.G.; Hathaway, D.K.; Mandrell, B.N. Factors Affecting Health-Related Quality of Life in Children Undergoing Curative Treatment for Cancer: A Review of the Literature. J. Pediatr. Oncol. Nurs. 2016, 33, 228–240. [Google Scholar] [CrossRef]
- Klassen, A.F.; Anthony, S.J.; Khan, A.; Sung, L.; Klaassen, R. Identifying determinants of quality of life of children with cancer and childhood cancer survivors: A systematic review. Support. Care Cancer 2011, 19, 1275–1287. [Google Scholar] [CrossRef]
- Bottomley, A.; Reijneveld, J.C.; Koller, M.; Flechtner, H.; Tomaszewski, K.A.; Greimel, E. 5th EORTC Quality of Life in Cancer Faculty. Current state of quality of life and patient-reported outcomes research. Eur. J. Cancer 2019, 121, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Anthony, S.J.; Selkirk, E.; Sung, L.; Klaassen, R.J.; Dix, D.; Scheinemann, K.; Klassen, A.F. Considering quality of life for children with cancer: A systematic review of patient-reported outcome measures and the development of a conceptual model. Qual. Life Res. 2014, 23, 771–789. [Google Scholar] [CrossRef]
- Mercieca-Bebber, R.; King, M.T.; Calvert, M.J.; Stockler, M.R.; Friedlander, M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat. Outcome Meas. 2018, 9, 353–367. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, T.L.; Rocque, G.B. Pathway to Precision Patient-Reported Outcomes. J. Clin. Oncol. 2021, 39, 3770–3772. [Google Scholar] [CrossRef]
- Trama, A.; Dieci, M. Quality of life in clinical trials for children. Eur. J. Clin. Pharmacol. 2011, 67 (Suppl. S1), 41–47. [Google Scholar] [CrossRef] [Green Version]
- Leahy, A.B.; Steineck, A. Patient-Reported Outcomes in Pediatric Oncology: The Patient Voice as a Gold Standard. JAMA Pediatr. 2020, 174, e202868. [Google Scholar] [CrossRef]
- Meeske, K.; Katz, E.R.; Palmer, S.N.; Burwinkle, T.; Varni, J.W. Parent proxy-reported health-related quality of life and fatigue in pediatric patients diagnosed with brain tumors and acute lymphoblastic leukemia. Cancer 2004, 101, 2116–2125. [Google Scholar] [CrossRef]
- Sung, L.; Klaassen, R.J.; Dix, D.; Pritchard, S.; Yanofsky, R.; Dzolganovski, B.; Almeida, R.; Klassen, A. Identification of paediatric cancer patients with poor quality of life. Br. J. Cancer 2009, 100, 82–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward-Smith, P.; Hamlin, J.; Bartholomew, J.; Stegenga, K. Quality of Life Among Adolescents with Cancer. J. Pediatr. Oncol. Nurs. 2007, 24, 166–171. [Google Scholar] [CrossRef]
- Barakat, L.P.; Li, Y.; Hobbie, W.L.; Ogle, S.K.; Hardie, T.; Volpe, E.M.; Szabo, M.M.; Reilly, M.; Deatrick, J.A. Health-related quality of life of adolescent and young adult survivors of childhood brain tumors. Psycho-Oncology 2015, 24, 804–811. [Google Scholar] [CrossRef] [Green Version]
- Landolt, M.A.; Vollrath, M.; Niggli, F.K.; Gnehm, H.E.; Sennhauser, F.H. Health-related quality of life in children with newly diagnosed cancer: A one year follow-up study. Health Qual. Life Outcomes 2006, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- Fardell, J.E.; Vetsch, J.; Trahair, T.; Mateos, M.K.; Grootenhuis, M.A.; Touyz, L.M.; Marshall, G.M.; Wakefield, C.E. Health-related quality of life of children on treatment for acute lymphoblastic leukemia: A systematic review. Pediatr. Blood Cancer 2017, 64, e26489. [Google Scholar] [CrossRef]
- Alcoser, P.W.; Rodgers, C. Treatment strategies in childhood cancer. J. Pediatr. Nurs. 2003, 18, 103–112. [Google Scholar] [CrossRef]
- Eiser, C.; Eiser, J.R.; Stride, C.B. Quality of life in children newly diagnosed with cancer and their mothers. Health Qual. Life Outcomes 2005, 3, 29. [Google Scholar] [CrossRef] [Green Version]
- Bult, M.K.; van Bindsbergen, K.L.A.; Schepers, S.A.; de Ridder-Sluiter, H.G.; Verhaak, C.M.; van Litsenburg, R.R.L.; Merks, J.H.M.; van Noesel, M.M.; Grootenhuis, M.A. Health-Related Quality of Life of Adolescents with Cancer During the First Year of Treatment. J. Adolesc. Young Adult Oncol. 2019, 8, 616–622. [Google Scholar] [CrossRef]
- Engelen, V.; Koopman, H.M.; Detmar, S.B.; Raat, H.; van de Wetering, M.D.; Brons, P.; Anninga, J.K.; Abbink, F.; Grootenhuis, M.A. Health-related quality of life after completion of successful treatment for childhood cancer. Pediatr. Blood Cancer 2011, 56, 646–653. [Google Scholar] [CrossRef]
- Waters, E.B.; Wake, M.A.; Hesketh, K.D.; Ashley, D.M.; Smibert, E. Health-related quality of life of children with acute lymphoblastic leukaemia: Comparisons and correlations between parent and clinician reports. Int. J. Cancer 2003, 103, 514–518. [Google Scholar] [CrossRef]
- Crane, S.; Backus, L.; Stockman, B.; Carpenter, J.S.; Lin, L.; Haase, J. Understanding Treatment Burden and Quality of Life Impact of Participating in an Early-Phase Pediatric Oncology Clinical Trial: A Pilot Study. J. Pediatr. Oncol. Nurs. 2018, 35, 25–35. [Google Scholar] [CrossRef] [Green Version]
- Laetsch, T.W.; Myers, G.D.; Baruchel, A.; Dietz, A.C.; Pulsipher, M.A.; Bittencourt, H.; Buechner, J.; De Moerloose, B.; Davis, K.L.; Nemecek, E.; et al. Patient-reported quality of life after tisagenlecleucel infusion in children and young adults with relapsed or refractory B-cell acute lymphoblastic leukaemia: A global, single-arm, phase 2 trial. Lancet Oncol. 2019, 20, 1710–1718. [Google Scholar] [CrossRef]
- Lee, J.; Gillam, L.; Visvanathan, K.; Hansford, J.R.; McCarthy, M.C. Clinical Utility of Precision Medicine in Pediatric Oncology: A Systematic Review. JCO Precis. Oncol. 2021, 5, 1088–1102. [Google Scholar] [CrossRef]
- Mody, R.J.; Prensner, J.R.; Everett, J.; Parsons, D.W.; Chinnaiyan, A.M. Precision medicine in pediatric oncology: Lessons learned and next steps. Pediatr. Blood Cancer 2017, 64, e26288. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.; Mayoh, C.; Lau, L.M.S.; Khuong-Quang, D.A.; Pinese, M.; Kumar, A.; Barahona, P.; Wilkie, E.E.; Sullivan, P.; Bowen-James, R.; et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat. Med. 2020, 26, 1742–1753. [Google Scholar] [CrossRef]
- Vetsch, J.; Wakefield, C.E.; Duve, E.; McGill, B.C.; Warby, M.; Tucker, K.M.; Malkin, D.; Lau, L.; Ziegler, D.S. Parents’, Health Care Professionals’, and Scientists’ Experiences of a Precision Medicine Pilot Trial for Patients with High-Risk Childhood Cancer: A Qualitative Study. JCO Precis. Oncol. 2019, 3, 1–11. [Google Scholar] [CrossRef]
- Pincez, T.; Clément, N.; Lapouble, E.; Pierron, G.; Kamal, M.; Bieche, I.; Bernard, V.; Fréneaux, P.; Michon, J.; Orbach, D.; et al. Feasibility and clinical integration of molecular profiling for target identification in pediatric solid tumors. Pediatr. Blood Cancer 2017, 64, e26365. [Google Scholar] [CrossRef]
- Hansford, J.R. Personalised medicine in paediatric oncology: Ethical practice outside the clinical trial framework? J. Paediatr. Child Health 2019, 55, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Maurer, S.H.; Hinds, P.S.; Spunt, S.L.; Furman, W.L.; Kane, J.R.; Baker, J.N. Decision making by parents of children with incurable cancer who opt for enrollment on a phase I trial compared with choosing a do not resuscitate/terminal care option. J. Clin. Oncol. 2010, 28, 3292–3298. [Google Scholar] [CrossRef]
- Sammarco, A. Perceived social support, uncertainty, and quality of life of younger breast cancer survivors. Cancer Nurs. 2001, 24, 212–219. [Google Scholar] [CrossRef]
- McGill, B.C.; Wakefield, C.E.; Hetherington, K.; Munro, L.J.; Warby, M.; Lau, L.; Tyrrell, V.; Ziegler, D.S.; O’Brien, T.A.; Marshall, G.M.; et al. “Balancing Expectations with Actual Realities”: Conversations with Clinicians and Scientists in the First Year of a High-Risk Childhood Cancer Precision Medicine Trial. J. Pers. Med. 2020, 10, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senapati, A.; Mateos, M.K.; Hetherington, K.; Ziegler, D.S.; Lau, L.M.; Wakefield, C.E.; Marshall, G. PRISM Engagement with CLINicians Study (PRE-CLIN): Therapeutic Decision Making in a Study of One. In Proceedings of the ANZCHOG Virtual Annual Scientific Meeting, Virtual Conference, 23–25 June 2021. [Google Scholar]
- Lillie, E.O.; Patay, B.; Diamant, J.; Issell, B.; Topol, E.J.; Schork, N.J. The n-of-1 clinical trial: The ultimate strategy for individualizing medicine? Pers. Med. 2011, 8, 161–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldman, L.; Hancock, K.; Gallinger, B.; Johnstone, B.; Brunga, L.; Malkin, D.; Barrera, M.; Villani, A. Perspectives and Experiences of Parents and Adolescents Who Participate in a Pediatric Precision Oncology Program: “When You Feel Helpless, This Kind of Thing Is Very Helpful”. JCO Precis. Oncol. 2022, 6, e2100444. [Google Scholar] [CrossRef] [PubMed]
- Cremeens, J.; Eiser, C.; Blades, M. Characteristics of health-related self-report measures for children aged three to eight years: A review of the literature. Qual. Life Res. 2006, 15, 739–754. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, P.R.; Rajan, S.; Sudeepthi, B.L.; Abdul Nazir, C.P. Patient-reported outcomes: A new era in clinical research. Perspect. Clin. Res. 2011, 2, 137–144. [Google Scholar] [CrossRef]
- Sav, A.; King, M.A.; Whitty, J.A.; Kendall, E.; McMillan, S.S.; Kelly, F.; Hunter, B.; Wheeler, A.J. Burden of treatment for chronic illness: A concept analysis and review of the literature. Health Expect. 2015, 18, 312–324. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, M.C.; De Abreu Lourenco, R.; McMillan, L.J.; Meshcheriakova, E.; Cao, A.; Gillam, L. Finding Out What Matters in Decision-Making Related to Genomics and Personalized Medicine in Pediatric Oncology: Developing Attributes to Include in a Discrete Choice Experiment. Patient-Patient-Cent. Outcomes Res. 2020, 13, 347–361. [Google Scholar] [CrossRef]
- De Abreu Lourenco, R.; McCarthy, M.C.; McMillan, L.J.; Sullivan, M.; Gillam, L. Understanding decisions to participate in genomic medicine in children’s cancer care: A comparison of what influences parents, health care providers, and the general community. Pediatr. Blood Cancer 2021, 68, e29101. [Google Scholar] [CrossRef]
- Weaver, M.S.; Heinze, K.E.; Kelly, K.P.; Wiener, L.; Casey, R.L.; Bell, C.J.; Wolfe, J.; Garee, A.M.; Watson, A.; Hinds, P.S. Palliative Care as a Standard of Care in Pediatric Oncology. Pediatr Blood Cancer 2015, 62 (Suppl. S5), S829–S833. [Google Scholar] [CrossRef]
- Ranallo, L. Improving the Quality of End-of-Life Care in Pediatric Oncology Patients Through the Early Implementation of Palliative Care. J. Pediatr. Oncol. Nurs. 2017, 34, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Snaman, J.; McCarthy, S.; Wiener, L.; Wolfe, J. Pediatric Palliative Care in Oncology. J. Clin. Oncol. 2020, 38, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Burwinkle, T.M.; Lane, M.M. Health-related quality of life measurement in pediatric clinical practice: An appraisal and precept for future research and application. Health Qual. Life Outcomes 2005, 3, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjadj, D.; Deshmukh, S.; Jabado, N. Entering the era of precision medicine in pediatric oncology. Nat. Med. 2020, 26, 1684–1685. [Google Scholar] [CrossRef]
- Clarke, S.A.; Eiser, C. The measurement of health-related quality of life (QOL) in paediatric clinical trials: A systematic review. Health Qual. Life Outcomes 2004, 2, 66. [Google Scholar] [CrossRef] [Green Version]
- Calvert, M.J.; O’Connor, D.J.; Basch, E.M. Harnessing the patient voice in real-world evidence: The essential role of patient-reported outcomes. Nat. Rev. Drug Discov. 2019, 18, 731–732. [Google Scholar] [CrossRef]
- Cheng, J.D.; Hitt, J.; Koczwara, B.; Schulman, K.A.; Burnett, C.B.; Gaskin, D.J.; Rowland, J.H.; Meropol, N.J. Impact of quality of life on patient expectations regarding phase I clinical trials. J. Clin. Oncol. 2000, 18, 421–428. [Google Scholar] [CrossRef]
- Basch, E. Patient-Reported Outcomes—Harnessing Patients’ Voices to Improve Clinical Care. N. Engl. J. Med. 2017, 376, 105–108. [Google Scholar] [CrossRef]
- Rubin, R.R.; Peyrot, M. Quality of life and diabetes. Diabetes Metab. Res. Reviews 1999, 15, 205–218. [Google Scholar] [CrossRef]
- Lollar, D.J.; Simeonsson, R.J.; Nanda, U. Measures of outcomes for children and youth. Arch. Phys. Med. Rehabil. 2000, 81, S46–S52. [Google Scholar] [CrossRef]
- EuroQol Foundation. EQ-5D-Y User Guide; EuroQol Research Foundation: Rotterdam, The Netherlands, 2020. [Google Scholar]
- Ravens-Sieberer, U.; Wille, N.; Badia, X.; Bonsel, G.; Burstrom, K.; Cavrini, G.; Devlin, N.; Egmar, A.C.; Gusi, N.; Herdman, M.; et al. Feasibility, reliability, and validity of the EQ-5D-Y: Results from a multinational study. Qual. Life Res. 2010, 19, 887–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gusi, N.; Perez-Sousa, M.A.; Gozalo-Delgado, M.; Olivares, P.R. Validity and reliability of the Spanish EQ-5D-Y proxy version. Pediatrics 2014, 81, 212–219. [Google Scholar] [CrossRef]
- Shiroiwa, T.; Fukuda, T.; Shimozuma, K. Psychometric properties of the Japanese version of the EQ-5D-Y by self-report and proxy-report: Reliability and construct validity. Qual. Life Res. 2019, 28, 3093–3105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.; Ferguson, G.D.; Jelsma, J. The use of the EQ-5D-Y health related quality of life outcome measure in children in the Western Cape, South Africa: Psychometric properties, feasibility and usefulness—A longitudinal, analytical study. Health Qual. Life Outcomes 2017, 15, 12. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.; Scott, C.; Jelsma, J.; Abraham, D.; Verstraete, J. Validity and feasibility of the self-report EQ-5D-Y as a generic Health-Related Quality of Life outcome measure in children and adolescents with Juvenile Idiopathic Arthritis in Western Cape, South Africa. South Afr. J. Physiother. 2019, 75, 1335. [Google Scholar] [CrossRef] [Green Version]
- Kreimeier, S.; Greiner, W. EQ-5D-Y as a Health-Related Quality of Life Instrument for Children and Adolescents: The Instrument’s Characteristics, Development, Current Use, and Challenges of Developing Its Value Set. Value Health 2019, 22, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Flynn, T.; Stevens, K.; Brazier, J.; Huynh, E.; Sawyer, M.; Roberts, R.; Ratcliffe, J. Assessing the Health-Related Quality of Life of Australian Adolescents: An Empirical Comparison of the Child Health Utility 9D and EQ-5D-Y Instruments. Value Health 2015, 18, 432–438. [Google Scholar] [CrossRef] [Green Version]
- Mayoral, K.; Rajmil, L.; Murillo, M.; Garin, O.; Pont, A.; Alonso, J.; Bel, J.; Perez, J.; Corripio, R.; Carreras, G.; et al. Measurement Properties of the Online EuroQol-5D-Youth Instrument in Children and Adolescents with Type 1 Diabetes Mellitus: Questionnaire Study. J. Med. Internet Res. 2019, 21, e14947. [Google Scholar] [CrossRef]
- Sousa, M.Á.P.; Sánchez-Toledo, P.O.; Fuertea, N.G. Parent-child discrepancy in the assessment of health-related quality of life using the EQ-5D-Y questionnaire. Arch. Argent. Pediatr. 2017, 115, 541–546. [Google Scholar]
- Sinlapamongkolkul, P.; Surapolchai, P. Health-Related Quality of Life in Thai Children with Thalassemia as Evaluated by PedsQL and EQ-5D-Y: A Single-Center Experience. Mediterr. J. Hematol. Infect. Dis. 2020, 12, e2020036. [Google Scholar] [CrossRef]
- Scalone, L.; Tommasetto, C.; Matteucci, M.C.; Selleri, P.; Broccoli, S.; Pacelli, B.; Cavrini, G. Assessing Quality of Life in Children and Adolescents: Development and Validation of the Italian Version of EQ-5D-Y. Ital. J. Public Health 2011, 8, 331–341. [Google Scholar] [CrossRef]
- Otto, C.; Barthel, D.; Klasen, F.; Nolte, S.; Rose, M.; Meyrose, A.-K.; Klein, M.; Thyen, U.; Ravens-Sieberer, U. Predictors of self-reported health-related quality of life according to the EQ-5D-Y in chronically ill children and adolescents with asthma, diabetes, and juvenile arthritis: Longitudinal results. Qual. Life Res. 2018, 27, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Eidt-Koch, D.; Mittendorf, T.; Greiner, W. Cross-sectional validity of the EQ-5D-Y as a generic health outcome instrument in children and adolescents with cystic fibrosis in Germany. BMC Pediatr. 2009, 9, 55. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Weighed kappa: Nominal scale agreement with provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.I.-K. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- McBride, G.B. A Proposal for Strength-of-Agreement Criteria for Lin’s Concordance Correlation Coefficient; National Institute of Water & Atmospheric Research Ltd.: Hamilton, New Zealand, 2005. [Google Scholar]
- Fakhry, H.; Goldenberg, M.; Sayer, G.; Aye, S.S.; Bagot, K.; Pi, S.; Ghazzaoui, R.; Vo, N.; Gowrinathan, S.; Bolton, M.; et al. Health-related quality of life in childhood cancer. J. Dev. Behav. Pediatr. JDBP 2013, 34, 419–440. [Google Scholar] [CrossRef] [PubMed]
- Peeters, J.; Meitert, J.; Paulides, M.; Wiener, A.; Beck, J.D.; Calaminus, G.; Langer, T. Health-related Quality of Life (HRQL) in ALL-patients Treated with Chemotherapy only—A Report from the Late Effects Surveillance System in Germany. Klin. Pädiatrie 2009, 221, 156–161. [Google Scholar] [CrossRef]
- Kazak, A.E.; Abrams, A.N.; Banks, J.; Christofferson, J.; DiDonato, S.; Grootenhuis, M.A.; Kabour, M.; Madan-Swain, A.; Patel, S.K.; Zadeh, S.; et al. Psychosocial Assessment as a Standard of Care in Pediatric Cancer. Pediatr. Blood Cancer 2015, 62, S426–S459. [Google Scholar] [CrossRef] [Green Version]
- Hinds, P.S.; Oakes, L.L.; Hicks, J.; Powell, B.; Srivastava, D.K.; Spunt, S.L.; Harper, J.; Baker, J.N.; West, N.K.; Furman, W.L. “Trying to be a good parent” as defined by interviews with parents who made phase I, terminal care, and resuscitation decisions for their children. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 5979–5985. [Google Scholar] [CrossRef] [Green Version]
- Vander Haegen, M.; Etienne, A.M. Intolerance of uncertainty as the vulnerability factor among parents of childhood cancer survivors: A 3-month follow-up study. J. Psychosoc. Oncol. 2018, 36, 437–453. [Google Scholar] [CrossRef]
- Gunter, M.D.; Duke, G. Reducing Uncertainty in Families Dealing with Childhood Cancers: An Integrative Literature Review. Pediatr. Nurs. 2018, 44, 21–37. [Google Scholar]
- Brown, K.A.; Barbarin, O.A. Gender differences in parenting a child with cancer. Soc. Work. Health Care 1996, 22, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Agnihotri, K.; Awasthi, S.; Singh, U.; Chandra, H.; Thakur, S. A study of concordance between adolescent self-report and parent-proxy report of health-related quality of life in school-going adolescents. J. Psychosom. Res. 2010, 69, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Fischer, A.R.; Frewer, L.J. Socio-psychological determinants of public acceptance of technologies: A review. Public Underst. Sci. 2012, 21, 782–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derrett, S.; Herdman, M.; Ngwira, L.G.; Moore, E.Y.; Jelsma, J. A New Approach to Assessing Children’s Interpretation of Severity Qualifiers in a Multi-Attribute Utility Instrument-The EQ-5D-Y-5L: Development and Testing. Patient 2021, 14, 591–600. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hetherington, K.; Wakefield, C.E.; Kunalan, K.P.K.; Donoghoe, M.W.; McGill, B.C.; Fardell, J.E.; Daly, R.; Deyell, R.J.; Ziegler, D.S. Quality of Life (QoL) of Children and Adolescents Participating in a Precision Medicine Trial for High-Risk Childhood Cancer. Cancers 2022, 14, 5310. https://doi.org/10.3390/cancers14215310
Hetherington K, Wakefield CE, Kunalan KPK, Donoghoe MW, McGill BC, Fardell JE, Daly R, Deyell RJ, Ziegler DS. Quality of Life (QoL) of Children and Adolescents Participating in a Precision Medicine Trial for High-Risk Childhood Cancer. Cancers. 2022; 14(21):5310. https://doi.org/10.3390/cancers14215310
Chicago/Turabian StyleHetherington, Kate, Claire E. Wakefield, Kavitha P. K. Kunalan, Mark W. Donoghoe, Brittany C. McGill, Joanna E. Fardell, Rebecca Daly, Rebecca J. Deyell, and David S. Ziegler. 2022. "Quality of Life (QoL) of Children and Adolescents Participating in a Precision Medicine Trial for High-Risk Childhood Cancer" Cancers 14, no. 21: 5310. https://doi.org/10.3390/cancers14215310