
Relationship between Aldehyde Dehydrogenase, PD-L1 and Tumor-Infiltrating Lymphocytes with Pathologic Response and Survival in Breast Cancer
 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Objectives
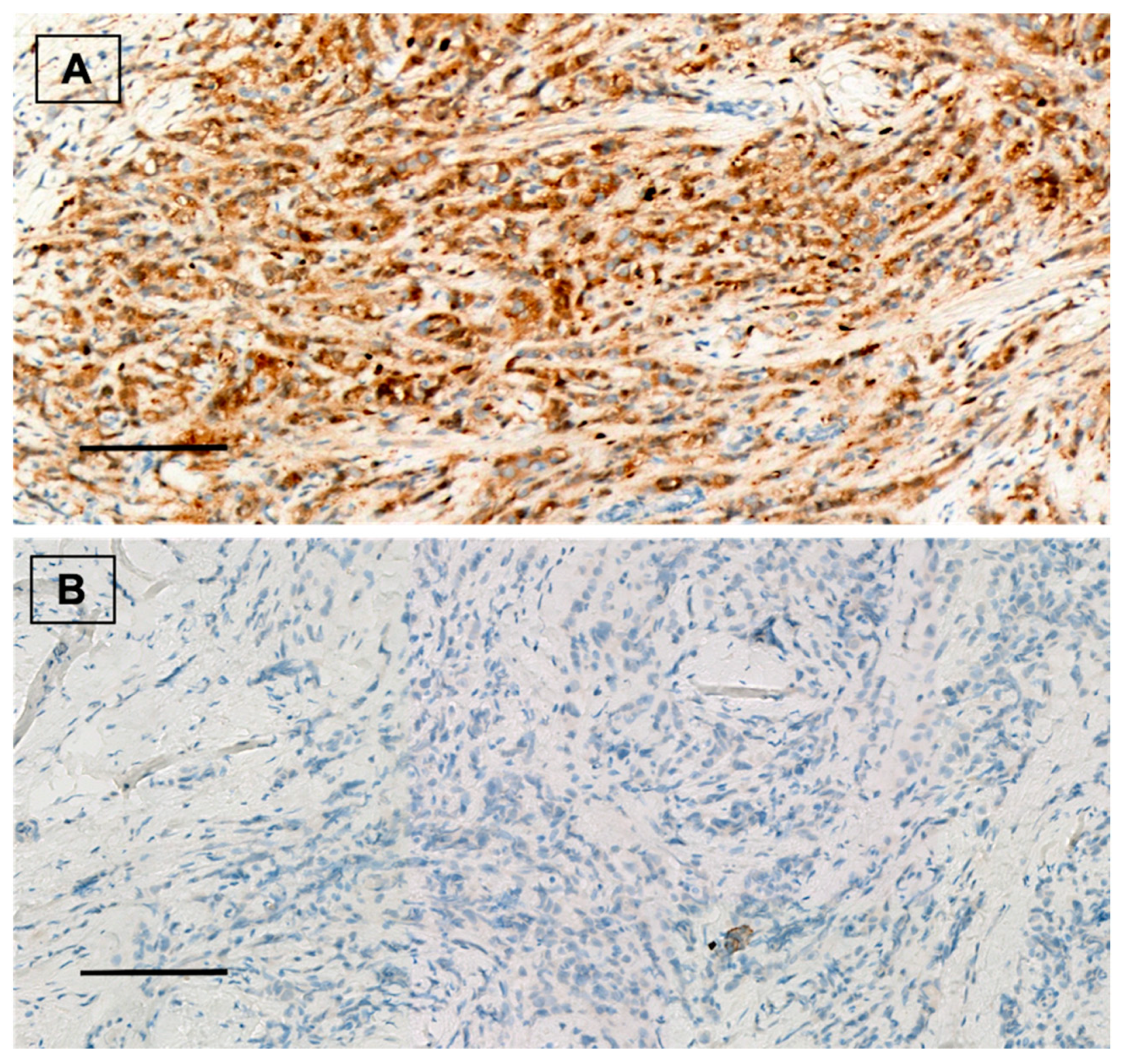
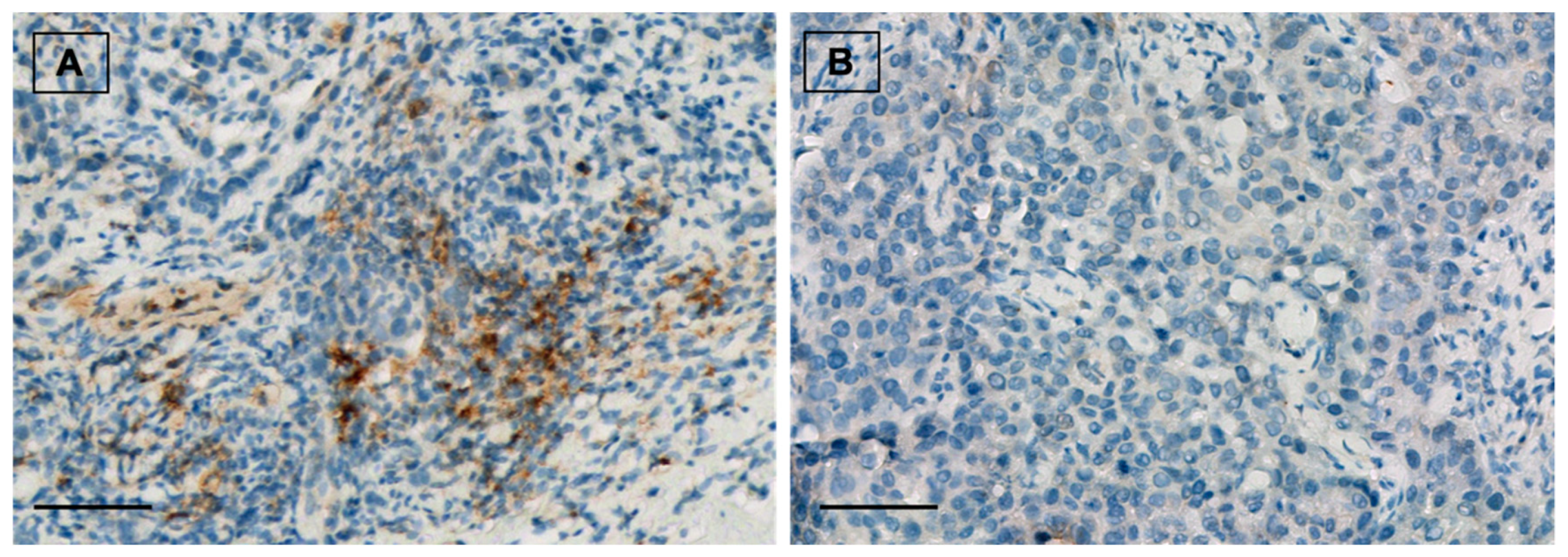
2.3. Immunohistochemistry Method
2.4. Statistical Analysis
3. Results
3.1. Study Population
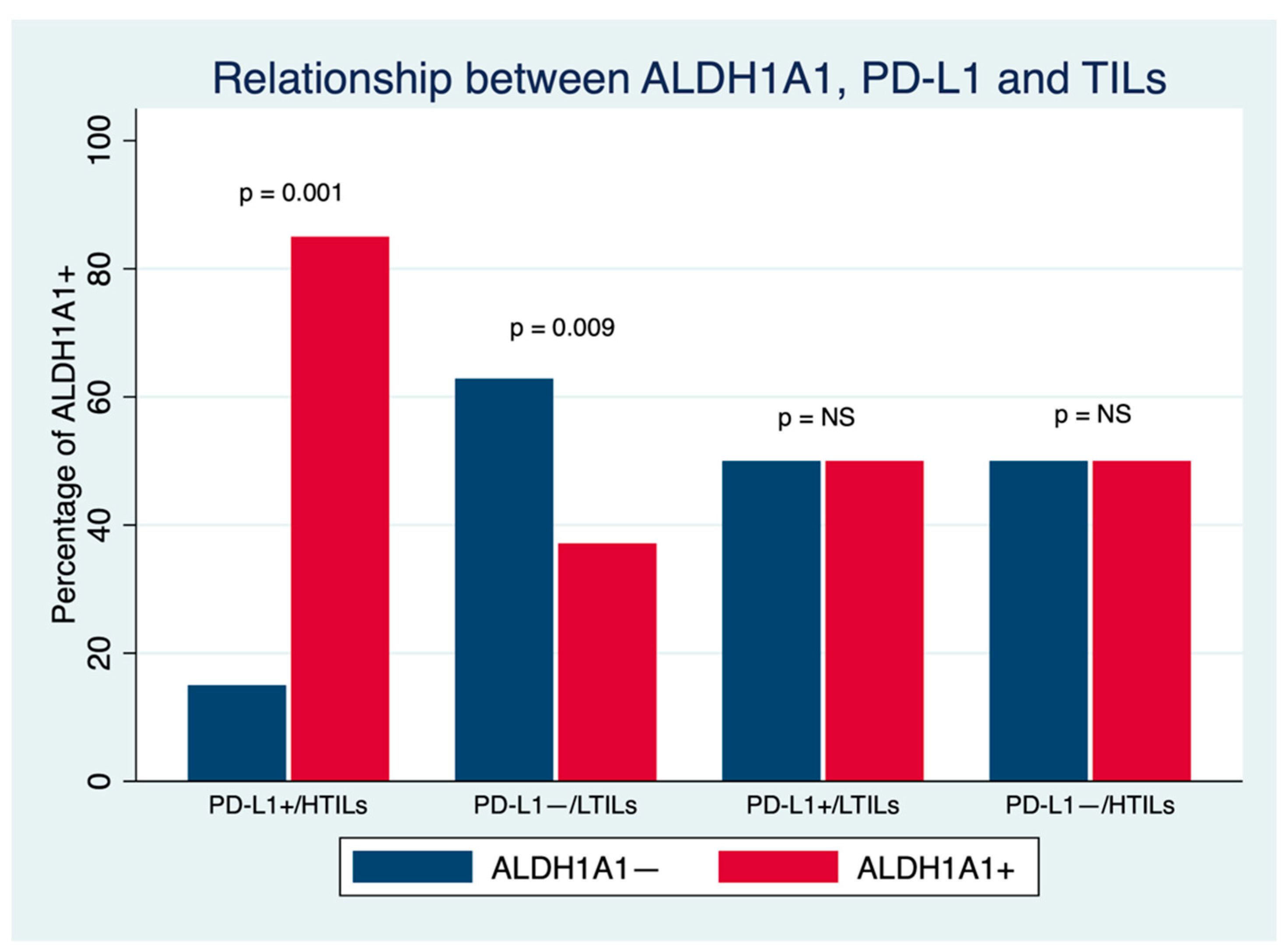
3.2. Relationship between ALDH1A1, PD-L1 and TILs
3.3. Relationship between ALDH1A1, PD-L1 and TILs with Clinicopathological Characteristics and Survival in Breast Cancer Patients
3.3.1. Relationship between ALDH1A1 and Clinicopathological Characteristics and Survival in Breast Cancer Patients
3.3.2. Relationship between PD-L1 and Clinicopathological Characteristics and Survival in Breast Cancer Patients
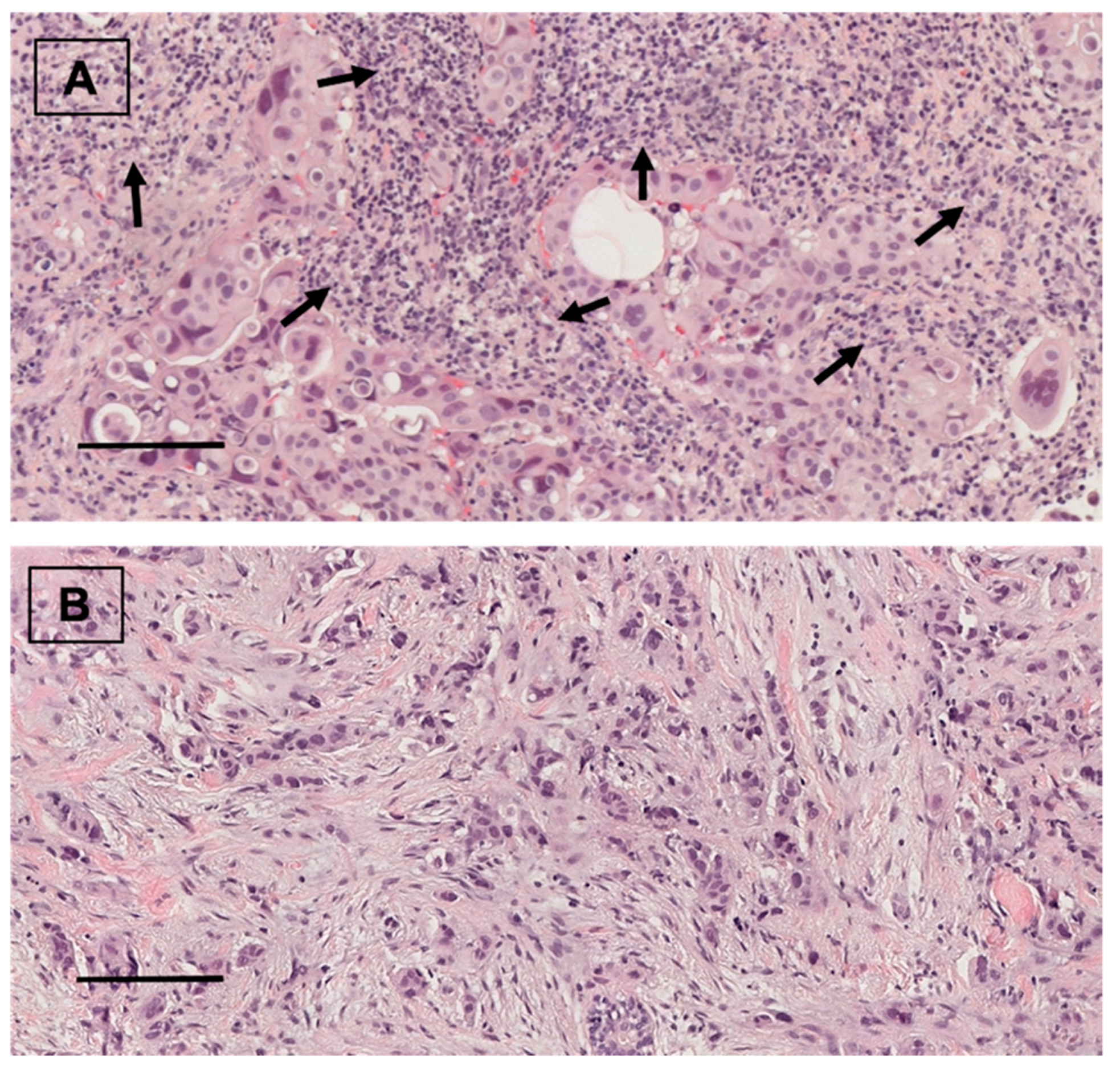
3.3.3. Relationship between TILs and Clinicopathological Characteristics and Survival in Breast Cancer Patients
3.3.4. Predictors of DFS and OS in the Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lüönd, F.; Tiede, S.; Christofori, G. Breast Cancer as an Example of Tumour Heterogeneity and Tumour Cell Plasticity during Malignant Progression. Br. J. Cancer 2021, 125, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Ginestier, C.; Hur, M.H.; Charafe-Jauffret, E.; Monville, F.; Dutcher, J.; Brown, M.; Jacquemier, J.; Viens, P.; Kleer, C.G.; Liu, S.; et al. ALDH1 Is a Marker of Normal and Malignant Human Mammary Stem Cells and a Predictor of Poor Clinical Outcome. Cell Stem Cell 2007, 1, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Tomita, H.; Tanaka, K.; Tanaka, T.; Hara, A. Aldehyde Dehydrogenase 1A1 in Stem Cells and Cancer. Oncotarget 2016, 7, 11018–11032. [Google Scholar] [CrossRef]
- Ginestier, C.; Wicinski, J.; Cervera, N.; Monville, F.; Finetti, P.; Bertucci, F.; Wicha, M.S.; Birnbaum, D.; Charafe-Jauffret, E. Retinoid Signaling Regulates Breast Cancer Stem Cell Differentiation. Cell Cycle 2009, 8, 3297–3302. [Google Scholar] [CrossRef]
- Li, J.; Zhang, B.; Yang, Y.; Jin, J.; Liu, Y. Aldehyde Dehydrogenase 1 as a Predictor of the Neoadjuvant Chemotherapy Response in Breast Cancer. Medicine 2018, 97, e12056. [Google Scholar] [CrossRef]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-Infiltrating Lymphocytes and Prognosis in Different Subtypes of Breast Cancer: A Pooled Analysis of 3771 Patients Treated with Neoadjuvant Therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef]
- Tsang, J.; Au, W.; Lo, K.; Ni, Y.; Hlaing, T.; Hu, J.; Chan, S.; Chan, K.; Cheung, S.; Tse, G. PD-L1 Expression and Tumor Infiltrating PD-1+ Lymphocytes Associated with Outcome in HER2+ Breast Cancer Patients. Breast Cancer Res. Treat. 2017, 162, 19–30. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.; Schneeweiss, A.; Barrios, C.; Iwata, H.; Diéras, V. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Wu, Z.; Zhang, L.; Peng, J.; Xu, S.; Zhou, L.; Lin, Y.; Wang, Y.; Lu, J.; Yin, W.; Lu, J. Predictive and Prognostic Value of PDL1 Protein Expression in Breast Cancer Patients in Neoadjuvant Setting. Cancer Biol. Ther. 2019, 20, 941–947. [Google Scholar] [CrossRef] [Green Version]
- López, A.; Salas, C.; Provencio, M.; Córdoba, M.; Gamallo, C. Aldehyde Dehydrogenases in Early Stage Lung Cancer: Nuclear Expression. Clin. Transl. Oncol. 2014, 16, 931–934. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van Den Eynden, G.; Baehner, F.L.; Perez, E.A.; et al. The Evaluation of Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Arias-Pulido, H.; Cimino-Mathews, A.; Chaher, N.; Qualls, C.; Joste, N.; Colpaert, C.; Marotti, J.D.; Foisey, M.; Prossnitz, E.R.; Emens, L.A.; et al. The Combined Presence of CD20+ B Cells and PD-L1+ Tumor-Infiltrating Lymphocytes in Inflammatory Breast Cancer Is Prognostic of Improved Patient Outcome. Breast Cancer Res. Treat. 2018, 171, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Tomonori, T.; Koji, M.; Kenzo, S.; Seung Jin, K.; Yoshio, T.; Tetsuya, T.; Yasuhiro, T.; Shinzaburo, N. Association of Breast Cancer Stem Cells Identified by Aldehyde Dehydrogenase 1 Expression with Resistance to Sequential Paclitaxel and Epirubicin-Based Chemotherapy for Breast Cancers. Clin. Cancer Res. 2009, 15, 4234–4241. [Google Scholar] [CrossRef]
- Kida, K.; Ishikawa, T.; Yamada, A.; Shimada, K.; Narui, K.; Sugae, S.; Shimizu, D.; Tanabe, M.; Sasaki, T.; Ichikawa, Y.; et al. Effect of ALDH1 on Prognosis and Chemoresistance by Breast Cancer Subtype. Breast Cancer Res. Treat. 2016, 156, 261–269. [Google Scholar] [CrossRef]
- Xu, F.; Li, S.; Zhang, J.; Wang, L.; Wu, X.; Wang, J.; Huang, Q.; Lai, M. Cancer Stemness, Immune Cells, and Epithelial–Mesenchymal Transition Cooperatively Predict Prognosis in Colorectal Carcinoma. Clin. Colorectal Cancer 2018, 17, 579–592. [Google Scholar] [CrossRef]
- Lotfinejad, P.; Kazemi, T.; Mokhtarzadeh, A.; Shanehbandi, D.; Jadidi Niaragh, F.; Safaei, S.; Asadi, M.; Baradaran, B. PD-1/PD-L1 Axis Importance and Tumor Microenvironment Immune Cells. Life Sci. 2020, 259, 118297. [Google Scholar] [CrossRef]
- Bazewicz, C.; Dinavahi, S.; Schell, T.; Robertson, G. Aldehyde Dehydrogenase in Regulatory T-Cell Development, Immunity and Cancer. Immunology 2019, 156, 47–55. [Google Scholar] [CrossRef]
- Terzuoli, E.; Bellan, C.; Aversa, S.; Ciccone, V.; Morbidelli, L.; Giachetti, A.; Donnini, S.; Ziche, M. ALDH3A1 Overexpression in Melanoma and Lung Tumors Drives Cancer Stem Cell Expansion, Impairing Immune Surveillance through Enhanced PD-L1 Output. Cancers 2019, 11, 1963. [Google Scholar] [CrossRef]
- Masciale, V.; Grisendi, G.; Banchelli, F.; D’Amico, R.; Maiorana, A.; Sighinolfi, P.; Pinelli, M.; Lovati, E.; Stefani, A.; Morandi, U.; et al. Correlating Tumor-Infiltrating Lymphocytes and Lung Cancer Stem Cells: A Cross-Sectional Study. Ann. Transl. Med. 2019, 7, 619. [Google Scholar] [CrossRef]
- Almozyan, S.; Colak, D.; Mansour, F.; Alaiya, A.; Al-Harazi, O.; Qattan, A.; Al-Mohanna, F.; Al-Alwan, M.; Ghebeh, H. PD-L1 Promotes OCT4 and Nanog Expression in Breast Cancer Stem Cells by Sustaining PI3K/AKT Pathway Activation. Int. J. Cancer 2017, 141, 1402–1412. [Google Scholar] [CrossRef] [PubMed]
- Polónia, A.; Pinto, R.; Cameselle-Teijeiro, J.; Schmitt, F.; Paredes, J. Prognostic Value of Stromal Tumour Infiltrating Lymphocytes and Programmed Cell Death-Ligand 1 Expression in Breast Cancer. J. Clin. Pathol. 2017, 70, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Všianská, P.; Bezděková, R.; Kryukov, F.; Almáši, M.; Pour, L.; Penka, M.; Hájek, R.; Říhová, L. Activity of Aldehyde Dehydrogenase in B-Cell and Plasma Cell Subsets of Monoclonal Gammopathy Patients and Healthy Donors. Eur. J. Haematol. 2017, 98, 19–25. [Google Scholar] [CrossRef]
- Iglesia, M.; Vincent, B.; Parker, J.; Hoadley, K.; Carey, L.; Perou, C.; Serody, J. Prognostic B-Cell Signatures Using MRNA-Seq in Patients with Subtype-Specific Breast and Ovarian Cancer. Clin. Cancer Res. 2014, 20, 3818–3829. [Google Scholar] [CrossRef]
- Resetkova, E.; Reis-Filho, J.S.; Jain, R.K.; Mehta, R.; Thorat, M.A.; Nakshatri, H.; Badve, S. Prognostic Impact of ALDH1 in Breast Cancer: A Story of Stem Cells and Tumor Microenvironment. Breast Cancer Res. Treat. 2010, 123, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Korkaya, H.; Paulson, A.; Iovino, F.; Wicha, M.S. HER2 Regulates the Mammary Stem/Progenitor Cell Population Driving Tumorigenesis and Invasion. Oncogene 2008, 27, 6120–6130. [Google Scholar] [CrossRef]
- Koppaka, V.; Chen, Y.; Mehta, G.; Orlicky, D.J.; Thompson, D.C.; Jester, J.V.; Vasiliou, V. ALDH3A1 Plays a Functional Role in Maintenance of Corneal Epithelial Homeostasis. PLoS ONE 2016, 11, e0146433. [Google Scholar] [CrossRef]
- Wang, L.; Lin, D.; Fu, Y.; Lai, M. Nuclear Aldehyde Dehydrogenase 1A1 (ALDH1A1) Expression Is a Favorable Prognostic Indicator in Colorectal Carcinoma. Pathol. Res. Pract. 2016, 212, 791–799. [Google Scholar] [CrossRef]
- Shenasa, E.; Stovgaard, E.S.; Jensen, M.; Asleh, K.; Riaz, N.; Gao, D.; Leung, S.; Ejlertsen, B.; Laenkholm, A.; Nielsen, T.O. Neither Tumor-Infiltrating Lymphocytes nor Cytotoxic T Cells Predict Enhanced Benefit from Chemotherapy in the DBCG77B Phase III Clinical Trial. Cancers 2022, 14, 3808. [Google Scholar] [CrossRef]
- Matsumoto, H.; Aye, A.; Huihua, T.; Joe, L. Increased CD4 and CD8-Positive T Cell Infiltrate Signifies Good Prognosis in a Subset of Triple-Negative Breast Cancer. Breast Cancer Res. Treat. 2016, 2, 237–242. [Google Scholar] [CrossRef]
- Rathore, A.S.; Kumar, S.; Konwar, R.; Srivastava, A.N.; Makker, A.; Goel, M.M. Presence of CD3+ Tumor Infiltrating Lymphocytes Is Significantly Associated with Good Prognosis in Infiltrating Ductal Carcinoma of Breast. Indian J. Cancer 2013, 50, 239–244. [Google Scholar] [CrossRef]
- Garaud, S.; Buisseret, L.; Solinas, C.; Gu-Trantien, C.; De Wind, A.; Van Den Eynden, G.; Naveaux, C.; Lodewyckx, J.N.; Boisson, A.; Duvillier, H.; et al. Tumor-Infiltrating B Cells Signal Functional Humoral Immune Responses in Breast Cancer. JCI Insight 2019, 4, e129641. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, D.; Mazzotta, M.; Pizzuti, L.; Krasniqi, E.; Gamucci, T.; Natoli, C.; Grassadonia, A.; Tinari, N.; Tomao, S.; Sperduti, I.; et al. Neoadjuvant Immune-Checkpoint Blockade in Triple-Negative Breast Cancer: Current Evidence and Literature-Based Meta-Analysis of Randomized Trials. Cancers 2020, 12, 2497. [Google Scholar] [CrossRef]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant Atezolizumab in Combination with Sequential Nab-Paclitaxel and Anthracycline-Based Chemotherapy versus Placebo and Chemotherapy in Patients with Early-Stage Triple-Negative Breast Cancer (IMpassion031): A Randomised, Double-Blind, Phase 3 Trial. Lancet 2020, 396, 1090–1100. [Google Scholar] [CrossRef]
- McArthur, H.L.; Leal, J.H.S.; Page, D.B.; Abaya, C.D.; Basho, R.K.; Phillips, M.; Chan, D.; Hool, H.; Park, D.J.; El-Masry, M.; et al. Neoadjuvant HER2-Targeted Therapy +/− Immunotherapy with Pembrolizumab (NeoHIP): An Open-Label Randomized Phase II Trial. J. Clin. Oncol. 2022, 40, TPS624. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 75 |
|---|---|
| Age | 53.6 ±11.7 years |
| Obesity | 21 (28%) |
| Menopausal status | |
| - Premenopausal | 34 (45.3%) |
| - Postmenopausal | 41 (54.7%) |
| Histology type | |
| - Ductal | 67 (89.3%) |
| - Lobular | 6 (8%) |
| - Metaplastic | 2 (2.7%) |
| Histopathological grade | |
| - Well differentiated | 3 (4%) |
| - Moderately differentiated | 23 (30.7%) |
| - Poorly differentiated | 49 (65.3%) |
| Ki67 | 50% (35–80%) |
| Positive androgen receptor | 43 (57.33%) |
| Tumor size | |
| - >5 cm | 32 (42.67%) |
| - ≤5 cm | 43 (57.33%) |
| Positive lymph nodes | 52 (69.33%) |
| Tumor subtype | |
| - HER2+ (a) | 43 (57.3%) |
| - TN (b) | 32 (42.7%) |
| Neoadjuvant therapy | |
| - Anthracycline | 74 (98.6%) |
| - Taxanes | 74 (98.6%) |
| - Carboplatin | 2 (6.25%) |
| - Anti-HER2 therapy | 39 (52%) |
| Pathologic complete response | 37 (49.33%) |
| ALDH1A1 (c) expression | |
| - Positive | 40 (53%) |
| - Negative | 35 (47%) |
| PD-L1 (d) expression | |
| - Positive | 28 (37.3%) |
| - Negative | 47 (62.7%) |
| TILs (e) | |
| - HTILs (f) | 32 (42.7%) |
| - LTILs (g) | 43 (57.3%) |
| Variables | ALDH1+ (n = 40) (a) | ALDH1− (n = 35) (b) | p Value |
|---|---|---|---|
| Age | 53.8 (±12) | 53.1 (±11) | 0.805 |
| Obesity | 13 (32.5%) | 8 (22.9%) | 0.353 |
| Menopausal status | |||
| - Premenopausal | 14 (35.0%) | 20 (57.1%) | 0.055 |
| - Postmenopausal | 26 (65.0%) | 15 (42.9%) | |
| Histology type | |||
| - Ductal | 35 (87.5%) | 32 (91.4%) | 0.087 |
| - Lobular | 5 (12.5%) | 1 (2.9%) | |
| - Metaplastic | 0 (0%) | 2 (5.7%) | |
| Histopathological grade | |||
| - Well differentiated | 1 (2.5%) | 2 (5.7%) | 0.587 |
| - Moderately differentiated | 14 (35.0%) | 9 (25.7%) | |
| - Poorly differentiated | 25 (62.5%) | 24 68.6%) | |
| Ki67 | 50% (32.5–80%) | 50% (30–70%) | 0.390 |
| Positive androgen receptor | 22 (55.0%) | 21 (60.0%) | 0.662 |
| Tumor size | |||
| - >5 cm | 12 (30.0%) | 20 (57.1%) | 0.018 |
| - ≤5 cm | 28 (70.0%) | 15 (42.9%) | |
| Positive lymph nodes | 26 (65%) | 26 (74.3) | 0.384 |
| - Tumor subtype | |||
| - HER2+ (c) | 23 (57.5%) | 20 (57.1%) | 0.975 |
| - TN (d) | 17 (42.5%) | 15 (42.9%) | |
| Neoadjuvant therapy | |||
| - Anthracycline | 39 (97.5%) | 35 (100%) | 1.000 |
| - Taxanes | 40 (100%) | 34 (97.1%) | 0.467 |
| - Carboplatin | 2 (5%) | 0 (0%) | 0.495 |
| - Anti-HER2 therapy | 22 (55.0%) | 17 (48.6%) | 0.578 |
| Pathologic complete response | |||
| - Yes | 24 (60%) | 13 (37.14%) | 0.048 |
| - No | 16 (40%) | 22 (62.86%) |
| Variables | PDL1+ (n = 28) (a) | PDL1− (n = 47) (b) | p Value |
|---|---|---|---|
| Age | 52.4 (±10.4) | 54,1 (±12.4) | 0.547 |
| Obesity | 7 (25%) | 14 (29.8%) | 0.655 |
| Menopausal status | |||
| - Premenopausal | 13 (46.4%) | 21 (44.8%) | 0.883 |
| - Postmenopausal | 15 (53.4%) | 26 (55.3%) | |
| Histology type | |||
| - Ductal | 26 (92.9%) | 41 (87.2%) | 0.481 |
| - Lobular | 1 (3.6%) | 5 (10.6%) | |
| - Metaplastic | 1 (3.6%) | 1 (2.13%) | |
| Histopathological grade | |||
| - Well differentiated | 2 (7.1%) | 1 (2.1%) | 0.380 |
| - Moderately differentiated | 10 (35.7%) | 13 (27.7%) | |
| - Poorly differentiated | 16 (57.1%) | 33 (70.2%) | |
| Ki67 | 50% (40–80%) | 50% (30–80%) | 0.154 |
| Positive androgen receptor | 16 (37.2%) | 27 (62.7%) | 0.979 |
| Tumor size | |||
| - >5 cm | 6 (21.4%) | 26 (55.3%) | 0.004 |
| - ≤5 cm | 22 (78.6%) | 21 (44.7%) | |
| Positive lymph nodes | 21 (75%) | 31 (66%) | 0.411 |
| Tumor subtype | |||
| - HER2+ (c) | 15 (53.6%) | 28 (59.6%) | 0.611 |
| - TN (d) | 13 (46.4%) | 19 (40.4%) | |
| Neoadjuvant therapy | |||
| - Anthracycline | 28 (100%) | 46 (97.9%) | 1.000 |
| - Taxanes | 28 (100%) | 46 (97.9%) | 1.000 |
| - Carboplatin | 0 (0%) | 2 (4.3%) | 0.526 |
| - Anti-HER2 therapy | 14 (50%) | 25 (53.2%) | 0.789 |
| Pathologic complete response | |||
| - Yes | 15 (53.6%) | 22 (46.8%) | 0.571 |
| - No | 13 (46.4%) | 25 (53.2%) |
| Variables | HTILs (n = 32) (a) | LTILs (n = 43) (b) | p Value |
|---|---|---|---|
| Age | 54.1 (±9.7) | 52.9 (±13) | 0.663 |
| Obesity | 12 (37.5%) | 9 (20.9%) | 0.114 |
| Menopausal status | |||
| - Premenopausal | 10 (31.2%) | 24 (55.8%) | 0.035 |
| - Postmenopausal | 22 (68.8%) | 19 (44.2%) | |
| Histology type | |||
| - Ductal | 30 (93.8%) | 37 (86.1%) | 0.597 |
| - Lobular | 2 (6.3%) | 4 (9.3%) | |
| - Metaplastic | 0 (0%) | 2 (4.7%) | |
| Histopathological grade | |||
| - Well differentiated | 1 (3.1%) | 2 (4.7%) | 0.584 |
| - Moderately differentiated | 12 (37.5%) | 11 (25.6%) | |
| - Poorly differentiated | 19 (59.4%) | 30 (69.7%) | |
| Ki 67 | 50% (32.5–80%) | 50% (30–80%) | 0.667 |
| Positive androgen receptor | 18 (56.3) | 25 (58.1) | 0.870 |
| Tumor size | |||
| - >5 cm | 6 (18.8%) | 26 (60.5%) | <0.001 |
| - ≤5 cm | 26 (81.2%) | 17 (39.5%) | |
| Positive lymph nodes | 19 (59.4%) | 33 (76.7%) | 0.107 |
| Tumor subtype | |||
| - HER2+ (c) | 19 (59.4%) | 24 (55.8%) | 0.758 |
| - TN (d) | 13 (40.6%) | 19 (44.2%) | |
| Neoadjuvant therapy | |||
| - Anthracycline | 32 (100%) | 42 (97.7%) | 1.000 |
| - Taxanes | 32 (100%) | 42 (97.7%) | 1.000 |
| - Carboplatin | 1 (3.1%) | 1 (2.3%) | 1.000 |
| - Anti-HER2 therapy | 17 (53.1%) | 22 (51.2%) | 0.866 |
| - Pathologic complete response | |||
| - Yes | 18 (56.3%) | 19 (44.2%) | 0.301 |
| - No | 14 (43.7%) | 24 (55.8%) |
| Variables | DFS (a) | OS (b) | ||
|---|---|---|---|---|
| Univariante Analysis | Multivariante Analysis | Univariante Analysis | Multivariante Analysis | |
| HR (95% CI); p Value | HR (95% CI); p Value | HR (95% CI); p Value | HR (95% CI); p Value | |
| Age | 1.0 (0.97–1.03); | 1.01 (0.97–1.05); | ||
| p = 0.939 | p = 0.662 | |||
| Obesity | 0.69 (0.28–1.70); | 0.98 (0.89–1.09); | ||
| p = 0.416 | p = 0.748 | |||
| Hormonal status | 0.99 (0.47–2.10); | 1.54 (0.62–3.87); | ||
| p = 0.995 | p = 0.355 | |||
| Histology type (against ductal type) − Lobular − Metaplastic | 1.40 (0.42–4.66) | 1.38 (0.32–5.99) | ||
| 7.51 (1.66–34.04); | 7.42 (1.67–32.90); | |||
| p = 0.105 | p = 0.110 | |||
| TN (c) (against HER2+) (d) | 1.37 (0.65–2.89); | 2.02 (0.83–4.88); | ||
| p = 0.403 | p = 0.120 | |||
| Ki67 | 1.00 (0.99–1.02); | 1.02 (0.99–1.03); | ||
| p = 0.796 | p = 0.214 | |||
| Positive androgen receptor | 0.62 (0.29–1.30); | 0.37 (0.15–1.92); | 0.32 (0.13–0.80); | |
| p = 0.201 | p = 0.031 | p = 0.014 | ||
| Tumor size > 5 cm | 3.95 (1.78–8.75); | 3.37 (1.30–8.76); | 6.53 (2.18–19.56); | 8.12 (2.24–29.45); |
| p = 0.01 | p = 0.012 | p = 0.001 | p = 0.001 | |
| Positive lymph nodes | 2.74 (0.95–7.91); | 1.75 (0.59–5.24); | ||
| p = 0.062 | p = 0.316 | |||
| ALDH1A1+ (e) | 0.060 (0.28–1.27); | 0.073 (0.30–1.77); | ||
| p = 0.181 | p = 0.489 | |||
| PD-L1+ (f) | 0.81 (0.36–1.79); | 0.83 (0.32–2.17); | ||
| p = 0.598 | p = 0.707 | |||
| HTILs (g) | 0.39 (0.17–0.93); | 0.68 (0.26–1.75); | 0.44 (0.16–0.22); | |
| p = 0.033 | p = 0.424 | p = 0.115 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López Flores, M.; Honrado Franco, E.; Sánchez Cousido, L.F.; Minguito-Carazo, C.; Sanz Guadarrama, O.; López González, L.; Vallejo Pascual, M.E.; Molina de la Torre, A.J.; García Palomo, A.; López González, A. Relationship between Aldehyde Dehydrogenase, PD-L1 and Tumor-Infiltrating Lymphocytes with Pathologic Response and Survival in Breast Cancer. Cancers 2022, 14, 4418. https://doi.org/10.3390/cancers14184418
López Flores M, Honrado Franco E, Sánchez Cousido LF, Minguito-Carazo C, Sanz Guadarrama O, López González L, Vallejo Pascual ME, Molina de la Torre AJ, García Palomo A, López González A. Relationship between Aldehyde Dehydrogenase, PD-L1 and Tumor-Infiltrating Lymphocytes with Pathologic Response and Survival in Breast Cancer. Cancers. 2022; 14(18):4418. https://doi.org/10.3390/cancers14184418
Chicago/Turabian StyleLópez Flores, Mariana, Emiliano Honrado Franco, Luis Felipe Sánchez Cousido, Carlos Minguito-Carazo, Oscar Sanz Guadarrama, Laura López González, María Eva Vallejo Pascual, Antonio José Molina de la Torre, Andrés García Palomo, and Ana López González. 2022. "Relationship between Aldehyde Dehydrogenase, PD-L1 and Tumor-Infiltrating Lymphocytes with Pathologic Response and Survival in Breast Cancer" Cancers 14, no. 18: 4418. https://doi.org/10.3390/cancers14184418