
Racial/Ethnic Disparities in Mortality Related to Access to Care for Major Cancers in the United States

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
Statistical Analysis
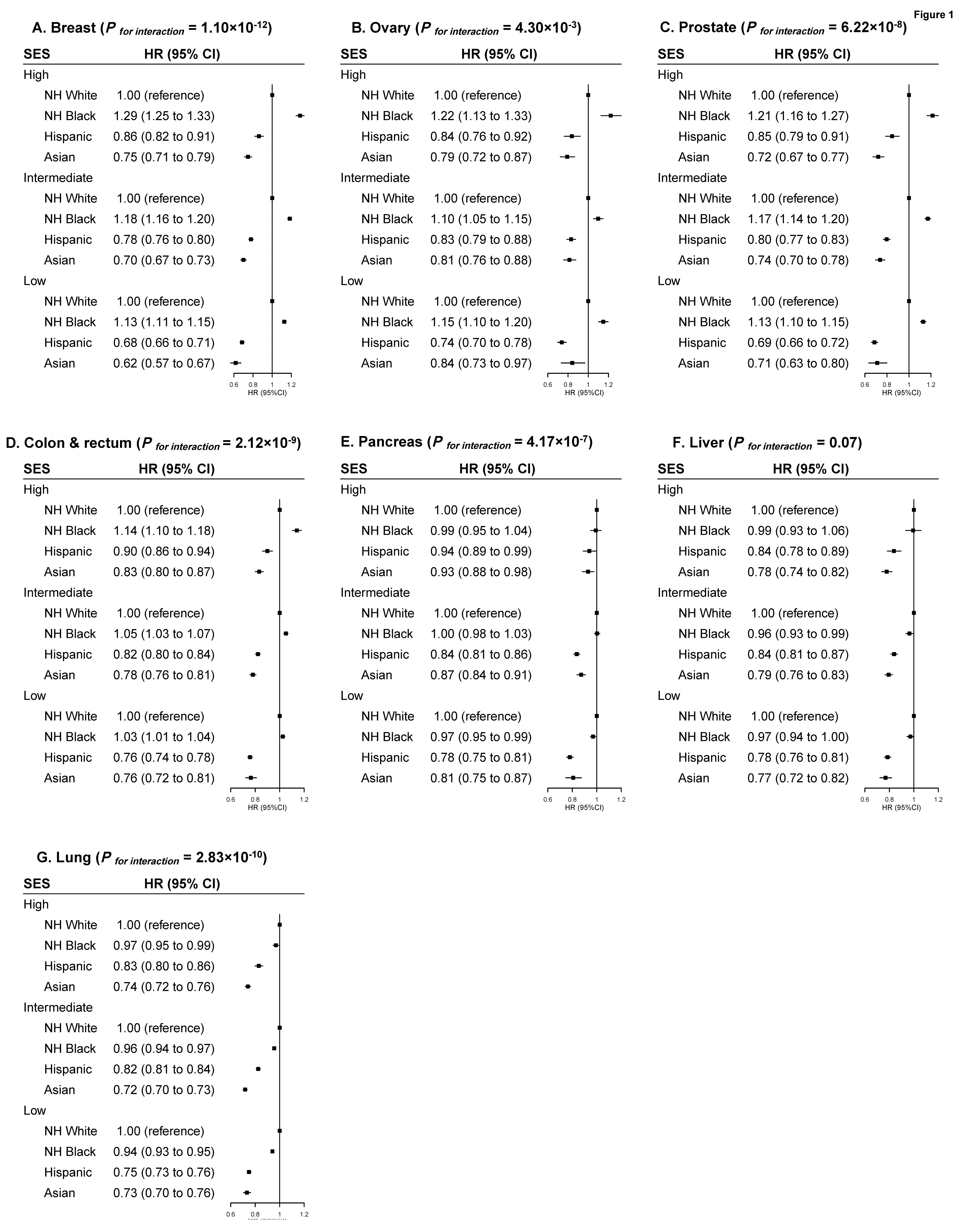
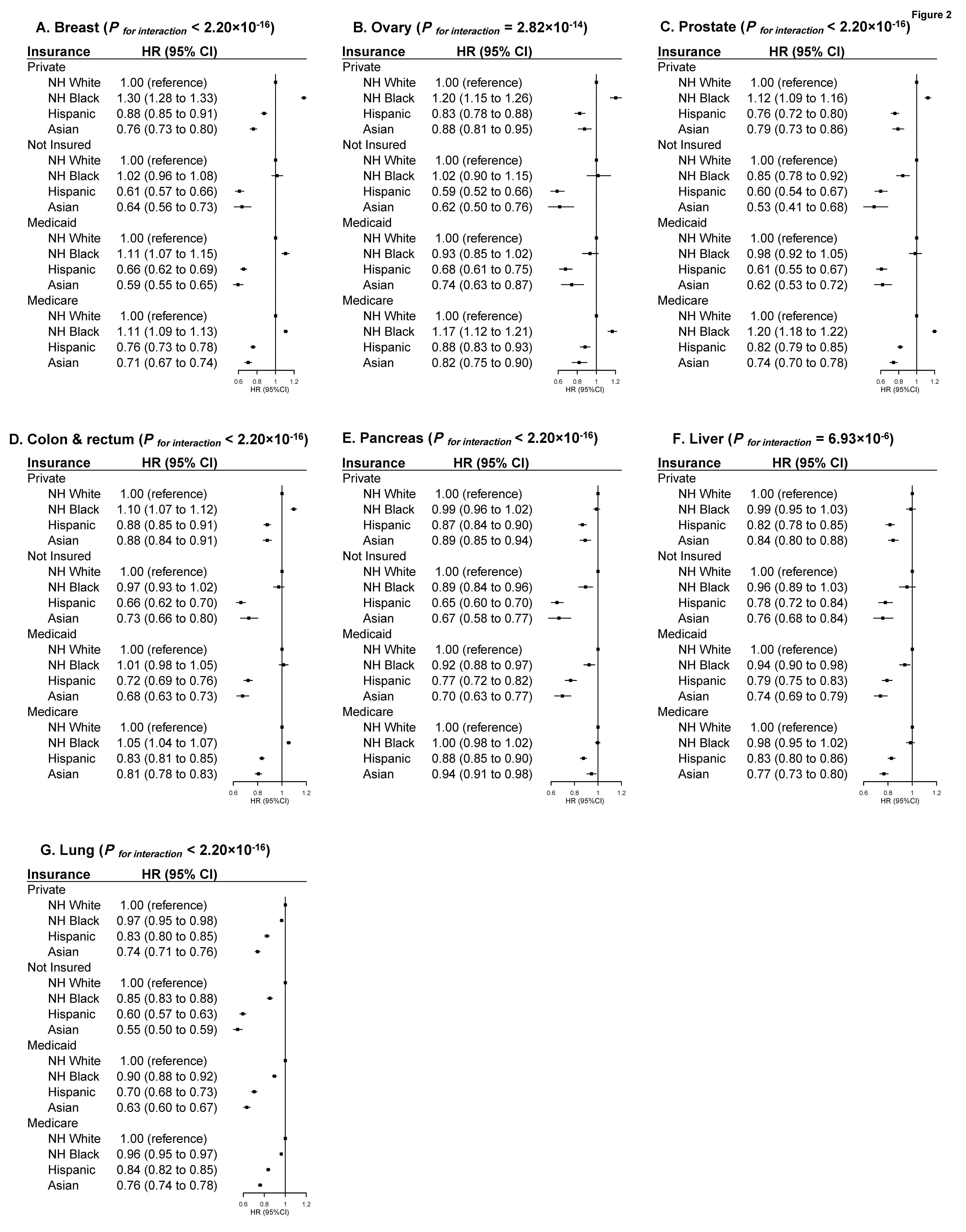
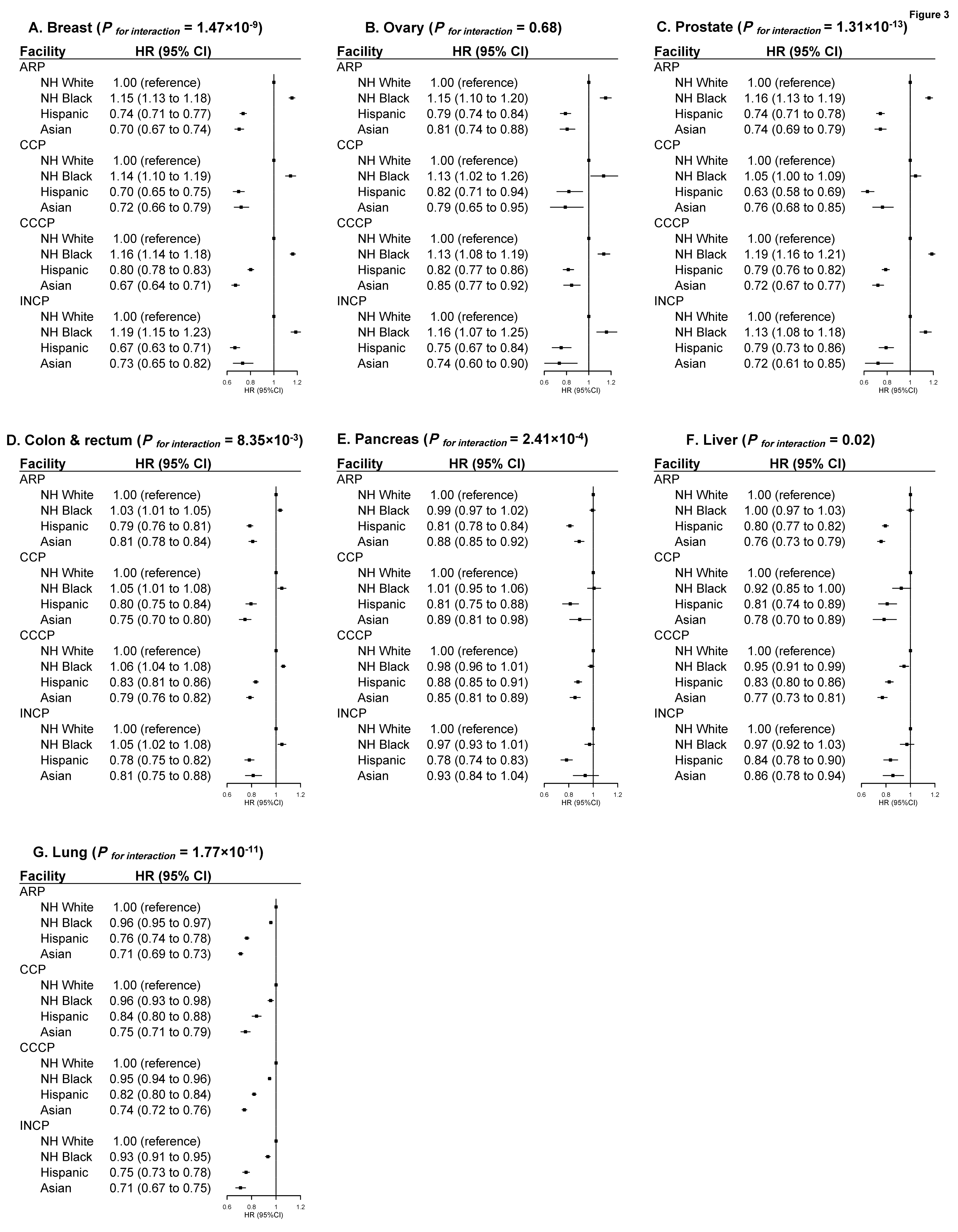
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- American Cancer Society. Cancer Facts & Figures 2019; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Ward, E.; Jemal, A.; Cokkinides, V.; Singh, G.K.; Cardinez, C.; Ghafoor, A.; Thun, M. Cancer Disparities by Race/Ethnicity and Socioeconomic Status. CA A Cancer J. Clin. 2004, 54, 78–93. [Google Scholar] [CrossRef]
- DeSantis, C.E.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Cancer Statistics for African Americans, 2019. CA Cancer J. Clin. 2019, 69, 211–233. [Google Scholar] [CrossRef] [Green Version]
- Aizer, A.A.; Wilhite, T.J.; Chen, M.-H.; Graham, P.L.; Choueiri, T.K.; Hoffman, K.E.; Martin, N.E.; Trinh, Q.-D.; Hu, J.C.; Nguyen, P.L. Lack of Reduction in Racial Disparities in Cancer-Specific Mortality over a 20-Year Period. Cancer 2014, 120, 1532–1539. [Google Scholar] [CrossRef]
- Miller, K.D.; Sauer, A.G.; Ortiz, A.P.; Fedewa, S.A.; Pinheiro, P.S.; Tortolero-Luna, G.; Martinez-Tyson, D.; Jemal, A.; Siegel, R.L. Cancer Statistics for Hispanics/Latinos, 2018. CA A Cancer J. Clin. 2018, 68, 425–445. [Google Scholar] [CrossRef] [Green Version]
- Torre, L.A.; Sauer, A.M.G.; Chen, M.S.; Kagawa-Singer, M.; Jemal, A.; Siegel, R.L. Cancer Statistics for Asian Americans, Native Hawaiians, and Pacific Islanders, 2016: Converging Incidence in Males and Females. CA Cancer J. Clin. 2016, 66, 182–202. [Google Scholar] [CrossRef]
- Pal, S.K.; Miller, M.J.; Agarwal, N.; Chang, S.M.; Chavez-MacGregor, M.; Cohen, E.; Cole, S.; Dale, W.; Magid Diefenbach, C.S.; Disis, M.L.; et al. Clinical Cancer Advances 2016: Annual Report on Progress against Cancer from the American Society of Clinical Oncology. J. Clin. Oncol. 2019, 37, 834–849. [Google Scholar] [CrossRef] [Green Version]
- Brawley, O.W.; Freeman, H.P. Race and Outcomes: Is This the End of the Beginning for Minority Health Research? J. Natl. Cancer Inst. 1999, 91, 1908–1909. [Google Scholar] [CrossRef] [Green Version]
- Albain, K.S.; Unger, J.M.; Crowley, J.J.; Coltman, C.A.; Hershman, D.L. Racial Disparities in Cancer Survival among Randomized Clinical Trials Patients of the Southwest Oncology Group. J. Natl. Cancer Inst. 2009, 101, 984–992. [Google Scholar] [CrossRef] [Green Version]
- Winchester, D.P.; Stewart, A.K.; Phillips, J.L.; Ward, E.E. The National Cancer Data Base: Past, Present, and Future. Ann. Surg. Oncol. 2010, 17, 4–7. [Google Scholar] [CrossRef] [Green Version]
- U.S. Census Bureau. 2010 Census Summary File 1; U.S. Census Bureau: Suitland, MD, USA, 2012.
- National Cancer Data Base Participant Use Data File (PUF) Data Dictionary. Version: PUF 2014. Containing Cases Diagnosed in 2004–2014; American College of Surgeons: Chicago, IL, USA, 2014. [Google Scholar]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2017, 2819372. [Google Scholar] [CrossRef]
- Fontenot, K.; Semega, J.; Kollar, M.; U.S. Census Bureau. Current Population Reports, P60–263, Income and Poverty in the United States: 2017; U.S. Government Printing Office: Washington, DC, USA, 2018.
- Manuel, J.I. Racial/Ethnic and Gender Disparities in Health Care Use and Access. Health Serv. Res. 2018, 53, 1407–1429. [Google Scholar] [CrossRef]
- Hargraves, J.L.; Cunningham, P.J.; Hughes, R.G. Racial and Ethnic Differences in Access to Medical Care in Managed Care Plans. Health Serv. Res. 2001, 36, 853–868. [Google Scholar]
- Kish, J.K.; Yu, M.; Percy-Laurry, A.; Altekruse, S.F. Racial and Ethnic Disparities in Cancer Survival by Neighborhood Socioeconomic Status in Surveillance, Epidemiology, and End Results (SEER) Registries. J. Natl. Cancer Inst. Monogr. 2014, 2014, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Albano, J.D.; Ward, E.; Jemal, A.; Anderson, R.; Cokkinides, V.E.; Murray, T.; Henley, J.; Liff, J.; Thun, M.J. Cancer Mortality in the United States by Education Level and Race. J. Natl. Cancer Inst. 2007, 99, 1384–1394. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.; Lee, S.; Matejkowski, J. The Effects of State Medicaid Expansion on Low-Income Individuals’ Access to Health Care: Multilevel Modeling. Popul. Health Manag. 2018, 21, 235–244. [Google Scholar] [CrossRef]
- Adamson, B.J.S.; Cohen, A.B.; Estevez, M.; Magee, K.; Williams, E.; Gross, C.P.; Meropol, N.J.; Davidoff, A.J. Affordable Care Act (ACA) Medicaid Expansion Impact on Racial Disparities in Time to Cancer Treatment. J. Clin. Oncol. 2019, 37, LBA1. [Google Scholar] [CrossRef]
- Braveman, P.A.; Cubbin, C.; Egerter, S.; Williams, D.R.; Pamuk, E. Socioeconomic Disparities in Health in the United States: What the Patterns Tell Us. Am. J. Public Health 2010, 100, S186–S196. [Google Scholar] [CrossRef]
- Singh, G.K.; Siahpush, M. Increasing Inequalities in All-Cause and Cardiovascular Mortality among US Adults Aged 25–64 Years by Area Socioeconomic Status, 1969–1998. Int. J. Epidemiol. 2002, 31, 600–613. [Google Scholar] [CrossRef]
- Kagawa-Singer, M.; Dadia, A.V.; Yu, M.C.; Surbone, A. Cancer, Culture, and Health Disparities: Time to Chart a New Course? CA A Cancer J. Clin. 2010, 60, 12–39. [Google Scholar] [CrossRef]
- White-Means, S.I.; Osmani, A.R. Racial and Ethnic Disparities in Patient-Provider Communication with Breast Cancer Patients: Evidence from 2011 MEPS and Experiences with Cancer Supplement. Inquiry 2017, 54, 46958017727104. [Google Scholar] [CrossRef] [Green Version]
- Chou, W.-Y.S.; Hamel, L.M.; Thai, C.L.; Debono, D.; Chapman, R.A.; Albrecht, T.L.; Penner, L.A.; Eggly, S. Discussing Prognosis and Treatment Goals with Patients with Advanced Cancer: A Qualitative Analysis of Oncologists’ Language. Health Expect 2017, 20, 1073–1080. [Google Scholar] [CrossRef]
- Penner, L.A.; Dovidio, J.F.; Gonzalez, R.; Albrecht, T.L.; Chapman, R.; Foster, T.; Harper, F.W.K.; Hagiwara, N.; Hamel, L.M.; Shields, A.F.; et al. The Effects of Oncologist Implicit Racial Bias in Racially Discordant Oncology Interactions. J. Clin. Oncol. 2016, 34, 2874–2880. [Google Scholar] [CrossRef] [Green Version]
- Yao, S.; Johnson, C.; Hu, Q.; Yan, L.; Liu, B.; Ambrosone, C.B.; Wang, J.; Liu, S. Differences in Somatic Mutation Landscape of Hepatocellular Carcinoma in Asian American and European American Populations. Oncotarget 2016, 7, 40491–40499. [Google Scholar] [CrossRef] [Green Version]
- Lo, F.-Y.; Chang, J.-W.; Chang, I.-S.; Chen, Y.-J.; Hsu, H.-S.; Huang, S.-F.K.; Tsai, F.-Y.; Jiang, S.S.; Kanteti, R.; Nandi, S.; et al. The Database of Chromosome Imbalance Regions and Genes Resided in Lung Cancer from Asian and Caucasian Identified by Array-Comparative Genomic Hybridization. BMC Cancer 2012, 12, 235. [Google Scholar] [CrossRef] [Green Version]
- Deng, J.; Chen, H.; Zhou, D.; Zhang, J.; Chen, Y.; Liu, Q.; Ai, D.; Zhu, H.; Chu, L.; Ren, W.; et al. Comparative Genomic Analysis of Esophageal Squamous Cell Carcinoma between Asian and Caucasian Patient Populations. Nat. Commun. 2017, 8, 1533. [Google Scholar] [CrossRef] [Green Version]
- Trinh, Q.-D.; Nguyen, P.L.; Leow, J.J.; Dalela, D.; Chao, G.F.; Mahal, B.A.; Nayak, M.; Schmid, M.; Choueiri, T.K.; Aizer, A.A. Cancer-Specific Mortality of Asian Americans Diagnosed with Cancer: A Nationwide Population-Based Assessment. J. Natl. Cancer Inst. 2015, 107, djv054. [Google Scholar] [CrossRef] [Green Version]
- Ellis, L.; Canchola, A.J.; Spiegel, D.; Ladabaum, U.; Haile, R.; Gomez, S.L. Racial and Ethnic Disparities in Cancer Survival: The Contribution of Tumor, Sociodemographic, Institutional, and Neighborhood Characteristics. J. Clin. Oncol. 2018, 36, 25–33. [Google Scholar] [CrossRef]
- Newman, L.A.; Griffith, K.A.; Jatoi, I.; Simon, M.S.; Crowe, J.P.; Colditz, G.A. Meta-Analysis of Survival in African American and White American Patients with Breast Cancer: Ethnicity Compared with Socioeconomic Status. J. Clin. Oncol. 2006, 24, 1342–1349. [Google Scholar] [CrossRef]
- Dess, R.T.; Hartman, H.E.; Mahal, B.A.; Soni, P.D.; Jackson, W.C.; Cooperberg, M.R.; Amling, C.L.; Aronson, W.J.; Kane, C.J.; Terris, M.K.; et al. Association of Black Race with Prostate Cancer–Specific and Other-Cause Mortality. JAMA Oncol. 2019, 5, 975–983. [Google Scholar] [CrossRef] [Green Version]
- Clegg, L.X.; Li, F.P.; Hankey, B.F.; Chu, K.; Edwards, B.K. Cancer Survival among US Whites and Minorities: A SEER (Surveillance, Epidemiology, and End Results) Program Population-Based Study. Arch. Intern. Med. 2002, 162, 1985–1993. [Google Scholar] [CrossRef] [Green Version]
- Jemal, A.; Ward, E.M.; Johnson, C.J.; Cronin, K.A.; Ma, J.; Ryerson, B.; Mariotto, A.; Lake, A.J.; Wilson, R.; Sherman, R.L.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2014, Featuring Survival. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef]
- Cronin, K.A.; Lake, A.J.; Scott, S.; Sherman, R.L.; Noone, A.-M.; Howlader, N.; Henley, S.J.; Anderson, R.N.; Firth, A.U.; Ma, J.; et al. Annual Report to the Nation on the Status of Cancer, Part I: National Cancer Statistics. Cancer 2018, 124, 2785–2800. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, P.S.; Morris, C.R.; Liu, L.; Bungum, T.J.; Altekruse, S.F. The Impact of Follow-up Type and Missed Deaths on Population-Based Cancer Survival Studies for Hispanics and Asians. J. Natl. Cancer Inst. Monogr. 2014, 2014, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Turra, C.M.; Elo, I.T. The Impact of Salmon Bias on the Hispanic Mortality Advantage. Popul. Res. Policy Rev. 2008, 27, 515–530. [Google Scholar] [CrossRef] [Green Version]
- Abraído-Lanza, A.F.; Dohrenwend, B.P.; Ng-Mak, D.S.; Turner, J.B. The Latino Mortality Paradox: A Test of the “Salmon Bias” and Healthy Migrant Hypotheses. Am. J. Public Health 1999, 89, 1543–1548. [Google Scholar] [CrossRef] [Green Version]
- Martinez Tyson, D.; Medina-Ramirez, P.; Flores, A.M.; Siegel, R.; Aguado Loi, C. Unpacking Hispanic Ethnicity-Cancer Mortality Differentials among Hispanic Subgroups in the United States, 2004–2014. Front. Public Health 2018, 6, 219. [Google Scholar] [CrossRef] [Green Version]
- Kwong, S.L.; Chen, M.S.; Snipes, K.P.; Bal, D.G.; Wright, W.E. Asian Subgroups and Cancer Incidence and Mortality Rates in California. Cancer 2005, 104, 2975–2981. [Google Scholar] [CrossRef] [Green Version]
- Gomez, S.L.; Glaser, S.L. Misclassification of Race/Ethnicity in a Population-Based Cancer Registry (United States). Cancer Causes Control 2006, 17, 771–781. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cancer Site | Unadjusted 5-Year Survival Rates (%) | Adjusted 5-Year Survival Rates (%) * | ||||||
|---|---|---|---|---|---|---|---|---|
| NH-White | NH-Black | Hispanic | Asian | NH-White | NH-Black | Hispanic | Asian | |
| Breast | 86.9 | 80.8 | 89.0 | 92.6 | 91.4 | 87.4 | 92.0 | 93.7 |
| Ovary | 46.7 | 40.4 | 56.3 | 62.4 | 49.7 | 44.4 | 56.1 | 56.8 |
| Prostate | 88.8 | 85.8 | 89.1 | 90.6 | 92.4 | 89.3 | 93.1 | 94.6 |
| Colon and Rectum | 58.1 | 55.1 | 63.4 | 66.3 | 61.3 | 56.9 | 64.5 | 67.0 |
| Pancreas | 9.6 | 10.0 | 14.1 | 14.0 | 3.7 | 4.8 | 8.0 | 7.0 |
| Liver | 20.9 | 18.0 | 23.6 | 31.1 | 13.4 | 13.7 | 18.7 | 21.7 |
| Lung | 19.7 | 17.9 | 23.0 | 26.0 | 11.5 | 12.5 | 19.5 | 22.2 |
| Race/Ethnicity | HR (95% CI) * | ||||||
|---|---|---|---|---|---|---|---|
| Breast Cancer | Ovarian Cancer | Prostate Cancer | Colorectal Cancer | Pancreatic Cancer | Liver Cancer | Lung Cancer | |
| NH-white | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NH-black | 1.27 (1.26 to 1.29) | 1.20 (1.17 to 1.23) | 1.31 (1.30 to 1.33) | 1.11 (1.10 to 1.12) | 1.03 (1.02 to 1.05) | 1.00 (0.98 to 1.02) | 0.98 (0.97 to 0.98) |
| Hispanic | 0.84 (0.83 to 0.86) | 0.84 (0.81 to 0.87) | 0.84 (0.82 to 0.86) | 0.87 (0.85 to 0.88) | 0.86 (0.84 to 0.88) | 0.82 (0.81 to 0.84) | 0.81 (0.80 to 0.82) |
| Asian | 0.69 (0.67 to 0.71) | 0.80 (0.76 to 0.85) | 0.70 (0.67 to 0.73) | 0.79 (0.78 to 0.81) | 0.87 (0.85 to 0.90) | 0.78 (0.76 to 0.80) | 0.72 (0.71 to 0.73) |
| HR (95% CI) | |||||||
|---|---|---|---|---|---|---|---|
| Breast Cancer | Ovarian Cancer | Prostate Cancer | Colorectal Cancer | Pancreatic Cancer | Liver Cancer | Lung Cancer | |
| Neighborhood-level SES | |||||||
| Low | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Intermediate | 0.95 (0.94 to 0.96) | 0.93 (0.91 to 0.95) | 0.86 (0.85 to 0.88) | 0.95 (0.94 to 0.96) | 0.96 (0.94 to 0.97) | 0.98 (0.96 to 0.99) | 0.97 (0.96 to 0.97) |
| High | 0.82 (0.81 to 0.83) | 0.84 (0.82 to 0.86) | 0.71 (0.70 to 0.72) | 0.86 (0.85 to 0.87) | 0.89 (0.88 to 0.90) | 0.91 (0.89 to 0.93) | 0.91 (0.90 to 0.92) |
| Insurance | |||||||
| Private | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Not insured | 1.63 (1.59 to 1.67) | 1.21 (1.17 to 1.27) | 1.68 (1.62 to 1.74) | 1.44 (1.42 to 1.47) | 1.15 (1.12 to 1.18) | 1.24 (1.20 to 1.28) | 1.24 (1.23 to 1.26) |
| Medicaid | 1.77 (1.74 to 1.79) | 1.32 (1.27 to 1.37) | 1.83 (1.78 to 1.89) | 1.50 (1.48 to 1.53) | 1.20 (1.18 to 1.23) | 1.19 (1.16 to 1.21) | 1.22 (1.21 to 1.23) |
| Medicare | 1.23 (1.22 to 1.25) | 1.06 (1.04 to 1.08) | 1.18 (1.16 to 1.19) | 1.14 (1.13 to 1.15) | 1.07 (1.05 to 1.08) | 1.12 (1.10 to 1.14) | 1.10 (1.10 to 1.11) |
| Other government | 1.17 (1.11 to 1.22) | 1.14 (1.05 to 1.25) | 1.38 (1.33 to 1.44) | 1.11 (1.07 to 1.15) | 1.06 (1.01 to 1.10) | 1.09 (1.03 to 1.15) | 1.05 (1.03 to 1.07) |
| Unknown | 1.05 (1.02 to 1.08) | 0.95 (0.90 to 1.01) | 1.00 (0.97 to 1.04) | 1.10 (1.07 to 1.13) | 0.97 (0.94 to 1.00) | 1.09 (1.04 to 1.14) | 1.07 (1.05 to 1.08) |
| Urban/rural Residence | |||||||
| Metro | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Urban | 1.03 (1.01 to 1.04) | 0.99 (0.96 to 1.01) | 1.01 (0.99 to 1.03) | 1.02 (1.01 to 1.03) | 1.03 (1.02 to 1.05) | 1.10 (1.07 to 1.12) | 1.01 (1.01 to 1.02) |
| Rural | 1.02 (0.99 to 1.05) | 1.02 (0.96 to 1.08) | 0.97 (0.94 to 1.01) | 0.99 (0.96 to 1.01) | 1.02 (0.99 to 1.06) | 1.07 (1.01 to 1.14) | 1.01 (1.00 to 1.03) |
| Unknown | 1.32 (1.29 to 1.35) | 1.26 (1.21 to 1.31) | 1.32 (1.28 to 1.36) | 1.27 (1.24 to 1.29) | 1.12 (1.09 to 1.14) | 1.20 (1.16 to 1.24) | 1.13 (1.12 to 1.15) |
| Facility type | |||||||
| Community | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Comprehensive Community | 0.95 (0.94 to 0.96) | 1.00 (0.97 to 1.03) | 0.90 (0.89 to 0.92) | 0.98 (0.97 to 0.99) | 0.96 (0.94 to 0.97) | 0.95 (0.92 to 0.98) | 0.97 (0.96 to 0.98) |
| Academic/Research | 0.85 (0.83 to 0.86) | 0.95 (0.92 to 0.98) | 0.76 (0.75 to 0.77) | 0.90 (0.89 to 0.91) | 0.81 (0.80 to 0.83) | 0.77 (0.74 to 0.79) | 0.89 (0.89 to 0.90) |
| Integrated Network | 0.91 (0.89 to 0.92) | 1.00 (0.97 to 1.04) | 0.86 (0.84 to 0.88) | 0.96 (0.95 to 0.98) | 0.92 (0.90 to 0.94) | 0.91 (0.88 to 0.95) | 0.95 (0.94 to 0.95) |
| Unknown | 2.34 (2.28 to 2.41) | 1.06 (0.99 to 1.12) | 5.01 (3.92 to 6.41) | 2.02 (1.96 to 2.07) | 0.81 (0.77 to 0.85) | 0.86 (0.80 to 0.92) | 0.92 (0.89 to 0.95) |
| Region | |||||||
| Northeast | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Midwest | 1.06 (1.05 to 1.08) | 1.07 (1.05 to 1.10) | 1.04 (1.03 to 1.06) | 1.06 (1.05 to 1.07) | 1.12 (1.10 to 1.13) | 1.12 (1.09 to 1.14) | 1.08 (1.08 to 1.09) |
| South | 1.01 (0.99 to 1.02) | 0.98 (0.96 to 1.00) | 1.04 (1.02 to 1.05) | 1.06 (1.05 to 1.07) | 1.10 (1.09 to 1.11) | 1.07 (1.05 to 1.09) | 1.04 (1.03 to 1.05) |
| West | 0.94 (0.93 to 0.96) | 1.00 (0.97 to 1.03) | 0.95 (0.93 to 0.96) | 1.03 (1.02 to 1.05) | 1.07 (1.05 to 1.08) | 1.07 (1.05 to 1.10) | 1.06 (1.05 to 1.06) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, F.; Shu, X.; Pal, T.; Berlin, J.; Nguyen, S.M.; Zheng, W.; Bailey, C.E.; Shu, X.-O. Racial/Ethnic Disparities in Mortality Related to Access to Care for Major Cancers in the United States. Cancers 2022, 14, 3390. https://doi.org/10.3390/cancers14143390
Wang F, Shu X, Pal T, Berlin J, Nguyen SM, Zheng W, Bailey CE, Shu X-O. Racial/Ethnic Disparities in Mortality Related to Access to Care for Major Cancers in the United States. Cancers. 2022; 14(14):3390. https://doi.org/10.3390/cancers14143390
Chicago/Turabian StyleWang, Fei, Xiang Shu, Tuya Pal, Jordan Berlin, Sang M. Nguyen, Wei Zheng, Christina E. Bailey, and Xiao-Ou Shu. 2022. "Racial/Ethnic Disparities in Mortality Related to Access to Care for Major Cancers in the United States" Cancers 14, no. 14: 3390. https://doi.org/10.3390/cancers14143390