
Comparison of Short- and Long-Term Mortality in Patients with or without Cancer Admitted to the ICU for Septic Shock: A Retrospective Observational Study

 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
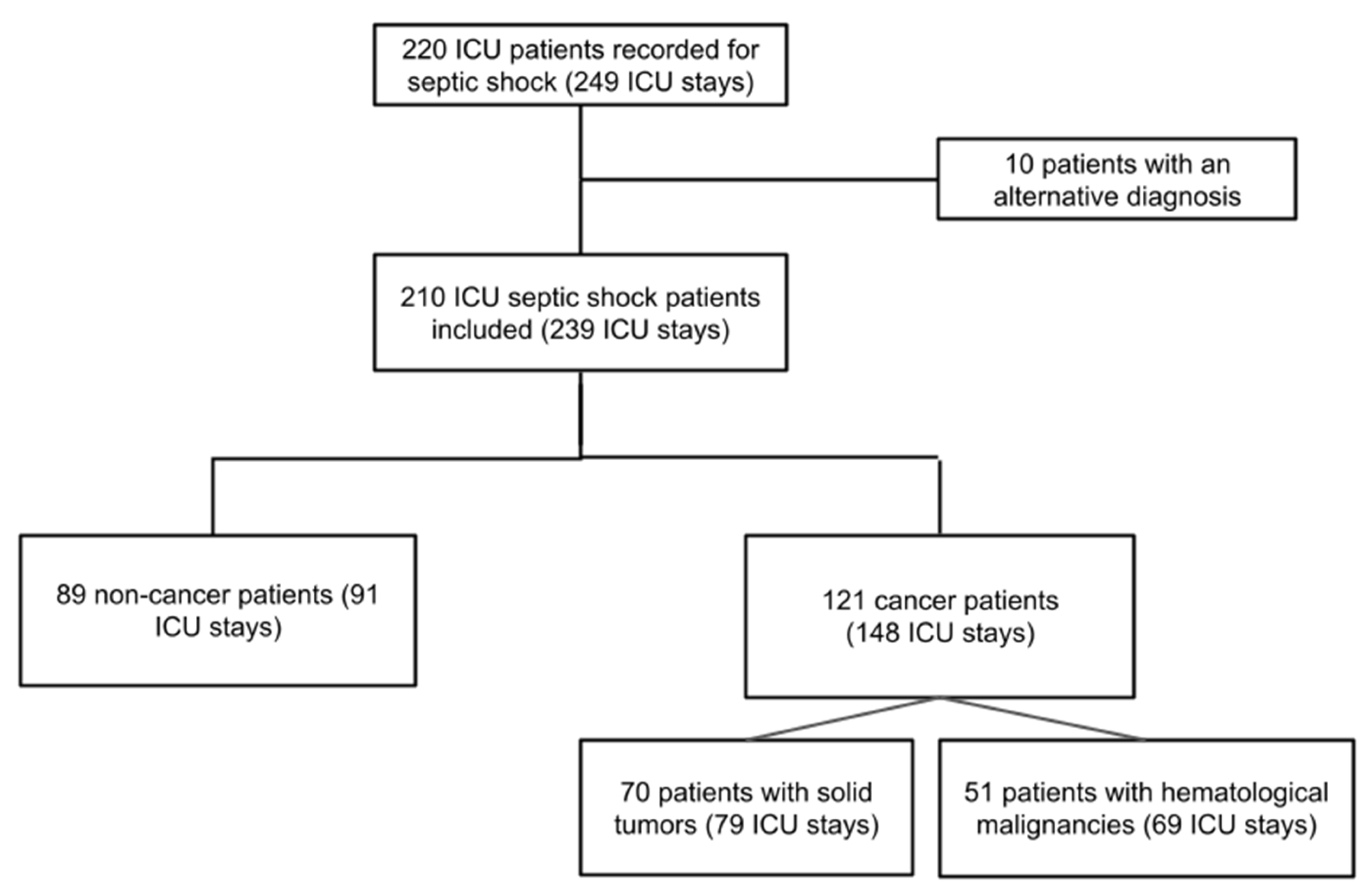
2.1. Study Population and Settings
2.2. Data Collection
2.3. Ethics
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Comparisons between Non-Cancer Patients versus Cancer Patients with SSh
3.3. Multivariate Analysis of Factors Associated with Mortality
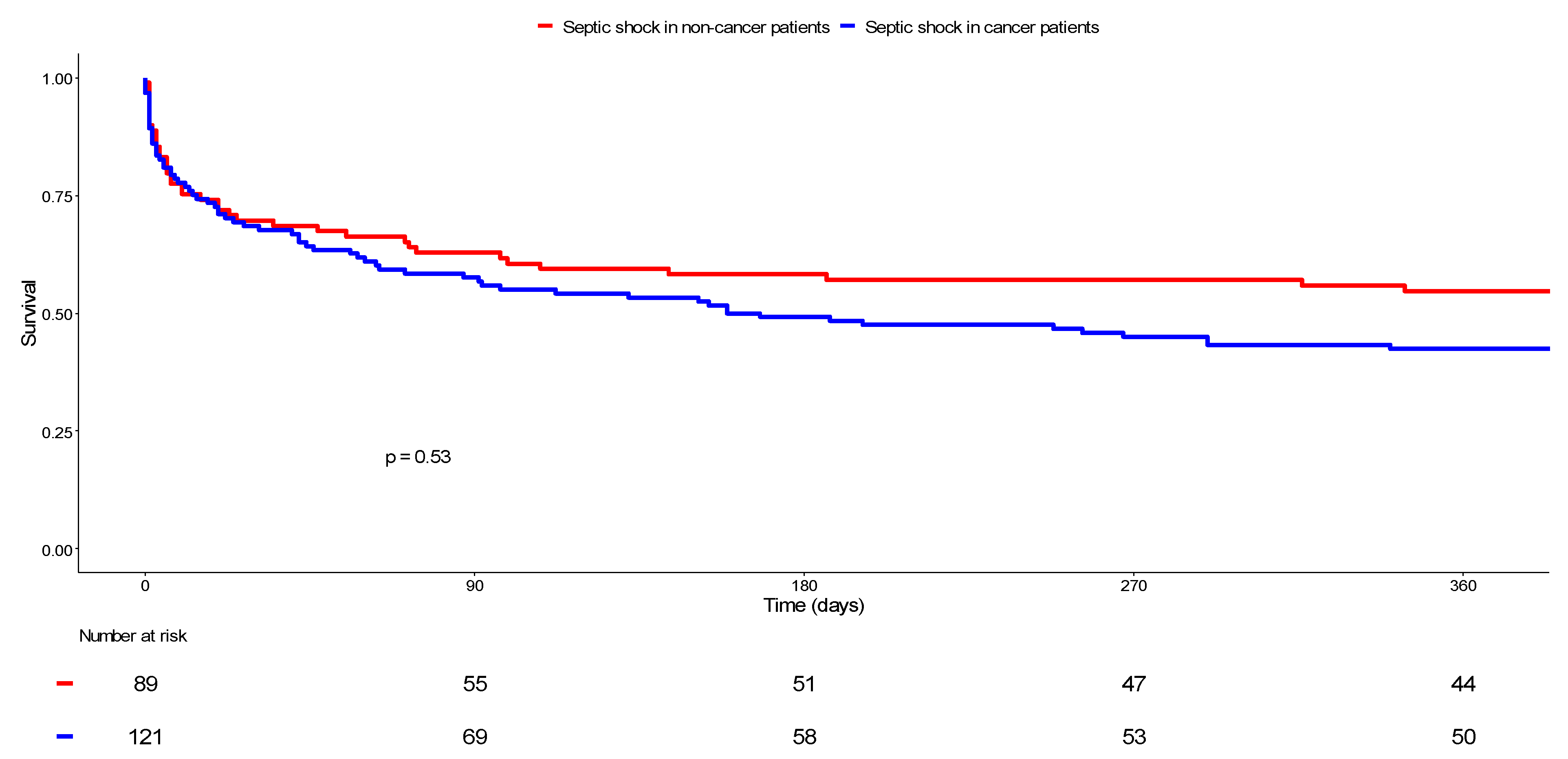
3.4. Long-Term Survival Outcome
3.5. Medical Economics Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Gustot, T. Multiple organ failure in sepsis: Prognosis and role of systemic inflammatory response. Curr. Opin. Crit. Care 2011, 17, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Leopold, S.J.; Cranendonk, D.R.; Van Der Poll, T. Host innate immune responses to sepsis. Virulence 2013, 5, 36–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, M.D.; Braun, L.A.; Cooper, L.M.; Johnston, J.; Weiss, R.V.; Qualy, R.L.; Linde-Zwirble, W. Hospitalized cancer patients with severe sepsis: Analysis of incidence, mortality, and associated costs of care. Crit. Care 2004, 8, R291–R298. [Google Scholar] [CrossRef] [Green Version]
- Kalathil, S.G.; Thanavala, Y. High immunosuppressive burden in cancer patients: A major hurdle for cancer immunotherapy. Cancer Immunol. Immunother. 2016, 65, 813–819. [Google Scholar] [CrossRef] [Green Version]
- Morrison, V.A. Immunosuppression Associated With Novel Chemotherapy Agents and Monoclonal Antibodies. Clin. Infect. Dis. 2014, 59, S360–S364. [Google Scholar] [CrossRef]
- Hensley, M.K.; Donnelly, J.; Carlton, E.; Prescott, H. Epidemiology and Outcomes of Cancer-Related Versus Non–Cancer-Related Sepsis Hospitalizations. Crit. Care Med. 2019, 47, 1310–1316. [Google Scholar] [CrossRef]
- Van de Louw, A.; Cohrs, A.; Leslie, D. Incidence of sepsis and associated mortality within the first year after cancer diagnosis in middle aged adults: A US population based study. PLoS ONE 2020, 15, e0243449. [Google Scholar] [CrossRef]
- Zaorsky, N.G.; Churilla, T.M.; Egleston, B.; Fisher, S.G.; Ridge, J.A.; Horwitz, E.M.; Meyer, J.E. Causes of death among cancer patients. Ann. Oncol. 2016, 28, 400–407. [Google Scholar] [CrossRef]
- Te Marvelde, L.; Whitfield, A.; Shepheard, J.; Read, C.; Milne, R.L.; Whitfield, K. Epidemiology of sepsis in cancer patients in Victoria, Australia: A population-based study using linked data. Aust. N. Z. J. Public Health 2020, 44, 53–58. [Google Scholar] [CrossRef]
- Zembower, T.R. Epidemiology of infections in cancer patients. Cancer Treat. Res. 2014, 161, 43–89. [Google Scholar] [PubMed]
- Kochanek, M.; Schalk, E.; von Bergwelt-Baildon, M.; Beutel, G.; Buchheidt, D.; Hentrich, M.; Henze, L.; Kiehl, M.; Liebregts, T.; von Lilienfeld-Toal, M.; et al. Management of sepsis in neutropenic cancer patients: 2018 guidelines from the Infectious Diseases Working Party (AGIHO) and Intensive Care Working Party (iCHOP) of the German Society of Hematology and Medical Oncology (DGHO). Ann. Hematol. 2019, 98, 1051–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darmon, M.; Bourmaud, A.; Georges, Q.; Soares, M.; Jeon, K.; Oeyen, S.; Rhee, C.K.; Gruber, P.; Ostermann, M.; Hill, Q.A.; et al. Changes in critically ill cancer patients’ short-term outcome over the last decades: Results of systematic review with meta-analysis on individual data. Intensiv. Care Med. 2019, 45, 977–987. [Google Scholar] [CrossRef]
- López, R.; Pérez-Araos, R.; Baus, F.; Moscoso, C.; Salazar, Á.; Graf, J.; Montes, J.M.; Samtani, S. Outcomes of Sepsis and Septic Shock in Cancer Patients: Focus on Lactate. Front. Med. 2021, 8, 603275. [Google Scholar] [CrossRef] [PubMed]
- Chebl, R.B.; Safa, R.; Sabra, M.; Chami, A.; Berbari, I.; Jamali, S.; Makki, M.; Tamim, H.; Abou Dagher, G. Sepsis in patients with haematological versus solid cancer: A retrospective cohort study. BMJ Open 2021, 11, e038349. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Knaus, W.A.; Zimmerman, J.E.; Wagner, D.P.; Draper, E.A.; Lawrence, D.E. APACHE-acute physiology and chronic health evaluation: A physiologically based classification system. Crit. Care Med. 1981, 9, 591–597. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Legrand, M.; Max, A.; Peigne, V.; Mariotte, E.; Canet, E.; Debrumetz, A.; Lemiale, V.; Seguin, A.; Darmon, M.; Schlemmer, B.; et al. Survival in neutropenic patients with severe sepsis or septic shock. Crit. Care Med. 2012, 40, 43–49. [Google Scholar] [CrossRef]
- Zuber, B.; Tran, T.-C.; Aegerter, P.; Grimaldi, D.; Charpentier, J.; Guidet, B.; Mira, J.-P.; Pene, F. Impact of case volume on survival of septic shock in patients with malignancies. Crit. Care Med. 2012, 40, 55–62. [Google Scholar] [CrossRef]
- Rosolem, M.M.; Rabello, L.S.; Lisboa, T.; Caruso, P.; Costa, R.T.; Leal, J.V.; Salluh, J.I.; Soares, M. Critically ill patients with cancer and sepsis: Clinical course and prognostic factors. J. Crit. Care 2012, 27, 301–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, V.B.; Azevedo, L.C.; Silva, U.V.; Caruso, P.; Torelly, A.P.; Silva, E.; Carvalho, F.B.; Vianna, A.; Souza, P.C.; Godoy, M.M.; et al. Sepsis-Associated Outcomes in Critically Ill Patients with Malignancies. Ann. Am. Thorac. Soc. 2015, 12, 1185–1192. [Google Scholar] [CrossRef]
- Lemiale, V.; Pons, S.; Mirouse, A.; Tudesq, J.J.; Hourmant, Y.; Mokart, D.; Pène, F.; Kouatchet, A.; Mayaux, J.; Nyunga, M.; et al. Sepsis and Septic Shock in Patients with Malignancies: A Groupe de Recherche Respiratoire en Reanimation Onco-Hematologique Study. Crit. Care Med. 2020, 48, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Danai, P.A.; Moss, M.; Mannino, D.M.; Martin, G.S. The Epidemiology of Sepsis in Patients With Malignancy. Chest 2006, 129, 1432–1440. [Google Scholar] [CrossRef] [PubMed]
- Camou, F.; Didier, M.; Leguay, T.; Milpied, N.; Daste, A.; Ravaud, A.; Mourissoux, G.; Guisset, O.; Issa, N. Long-term prognosis of septic shock in cancer patients. Support. Care Cancer 2019, 28, 1325–1333. [Google Scholar] [CrossRef] [PubMed]
- Jamme, M.; Daviaud, F.; Charpentier, J.; Marin, N.; Thy, M.; Hourmant, Y.; Mira, J.P.; Pène, F. Time Course of Septic Shock in Immunocompromised and Nonimmunocompromised Patients. Crit. Care Med. 2017, 45, 2031–2039. [Google Scholar] [CrossRef]
- Tolsma, V.; Schwebel, C.; Azoulay, E.; Darmon, M.; Souweine, B.; Vesin, A.; Goldgran-Toledano, D.; Lugosi, M.; Jamali, S.; Cheval, C.; et al. Sepsis severe or septic shock: Outcome according to immune status and immunodeficiency profile. Chest 2014, 146, 1205–1213. [Google Scholar] [CrossRef]
- Pène, F.; Percheron, S.; Lemiale, V.; Viallon, V.; Claessens, Y.-E.; Marqué, S.; Charpentier, J.; Angus, D.C.; Cariou, A.; Chiche, J.-D.; et al. Temporal changes in management and outcome of septic shock in patients with malignancies in the intensive care unit. Crit. Care Med. 2008, 36, 690–696. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Jones, G.; David, S.; Olariu, E.; Cadwell, K.K. Frequency and mortality of septic shock in Europe and North America: A systematic review and meta-analysis. Crit. Care 2019, 23, 196–206. [Google Scholar] [CrossRef] [Green Version]
- Larché, J.; Azoulay, É.; Fieux, F.; Mesnard, L.; Moreau, D.; Thiery, G.; Darmon, M.; Le Gall, J.-R.; Schlemmer, B. Improved survival of critically ill cancer patients with septic shock. Intensiv. Care Med. 2003, 29, 1688–1695. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Ji, X.; Song, Y.; Wang, X.; Zheng, W.; Lin, N.; Tu, M.; Xie, Y.; Ping, L.; Ying, Z.; et al. Improving survival of 3760 patients with lymphoma: Experience of an academic center over two decades. Cancer Med. 2020, 9, 3765–3774. [Google Scholar] [CrossRef]
- Azoulay, E.; Soares, M.; Darmon, M.; Benoit, D.; Pastores, S.; Afessa, B. Intensive care of the cancer patient: Recent achievements and remaining challenges. Ann. Intensiv. Care 2011, 1, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Meziani, F.; Levi, M. What’s new in the diagnostic criteria of disseminated intravascular coagulation? Intensive Care Med. 2016, 42, 1062–1064. [Google Scholar] [CrossRef] [PubMed]
- Clere-Jehl, R.; Merdji, H.; Kassem, M.; Macquin, C.; De Cauwer, A.; Sibony, A.; Kurihara, K.; Minniti, L.; Abou Fayçal, C.; Bahram, S.; et al. A Translational Investigation of IFN-alpha and STAT1 Signaling in Endothelial Cells during Septic Shock Provides Therapeutic Perspectives. Am. J. Respir. Cell. Mol. Biol. 2021, 65, 167–175. [Google Scholar] [CrossRef]
- Chambers, P.; Jani, Y.; Wei, L.; Kipps, E.; Forster, M.D.; Wong, I.C.K. Patient factors and their impact on neutropenic events: A systematic review and meta-analysis. Support Care Cancer 2019, 27, 2413–2424. [Google Scholar] [CrossRef] [Green Version]
- Lustberg, M.B. Management of neutropenia in cancer patients. Clin. Adv. Hematol. Oncol. 2012, 10, 825–826. [Google Scholar]
- Bouteloup, M.; Perinel, S.; Bourmaud, A.; Azoulay, E.; Mokart, D.; Darmon, M. Outcomes in adult critically ill cancer patients with and without neutropenia: A systematic review and meta-analysis of the Groupe de Recherche en Reanimation Respiratoire du patient d’Onco-Hematologie (GRRR-OH). Oncotarget 2017, 8, 1860–1870. [Google Scholar] [CrossRef] [Green Version]
- Azoulay, E.; Schellongowski, P.; Darmon, M.; Bauer, P.R.; Benoit, D.; Depuydt, P.; Divatia, J.V.; Lemiale, V.; van Vliet, M.; Meert, A.P.; et al. The Intensive Care Medicine research agenda on critically ill oncology and hematology patients. Intensiv. Care Med. 2017, 43, 1366–1382. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Patients N = 210 | Non-Cancer Patients n = 89 | Cancer Patients n = 121 | p Value | |
|---|---|---|---|---|
| Age (years) | 66.5 [56.3–77.0] | 69.0 [57.0–82.0] | 64.0 [56.0–75.0] | 0.02 * |
| Male | 125 (59.5) | 52 (63.4) | 73 (57.0) | 0.36 |
| Comorbidities | ||||
| Hypertension | 111 (53.1) | 54 (60.7) | 57 (47.5) | 0.06 |
| Body mass index | 25.1 [21.9–29.1] | 26.1 [23.3–30.1] | 24.2 [21.3–27.7] | <0.01 * |
| Cardiovascular diseases | 88 (41.9) | 44 (49.4) | 44 (36.4) | 0.06 |
| Diabetes mellitus | 62 (29.7) | 34 (38.2) | 28 (23.3) | 0.02 * |
| Pre-existing renal failure | 28 (13.3) | 16 (18.0) | 12 (9.9) | 0.09 |
| Respiratory diseases | 68 (32.4) | 35 (39.3) | 33 (27.3) | 0.07 |
| Knaus score | 6.0 [5.0–6.0] | 6.0 [5.0–6.0] | 6.0 [6.0–6.0] | <0.01 * |
| Charlson Comorbidity Index | 6.0 [3.0–9.0] | 5.0 [2.0–7.0] | 7.0 [4.0–10.0] | <0.01 * |
| Cognitive impairment | 24 (11.4) | 20 (22.5) | 4 (3.3) | <0.01 * |
| History of prior ICU stay | 125 (59.5) | 42 (47.2) | 83 (68.6) | <0.01 * |
| Long-term mortality # | ||||
| At d90 | 84 (40.4) | 33(37.5) | 51 (42.5) | 0.47 |
| At d180 | 98 (47.3) | 37 (42.0) | 61(51.3) | 0.19 |
| At d365 (1 year) | 109 (53.7) | 40 (47.6) | 69 (58.0) | 0.14 |
| All Stays N = 239 | Stays of Non-Cancer Patients n = 91 | Stays of Cancer Patients n = 148 | p Value | |
|---|---|---|---|---|
| Treatments before ICU admission | ||||
| Fluid therapy | 178 (76.1) | 67 (74.4) | 111 (77.1) | 0.65 |
| Norepinephrine | 80 (33.9) | 32 (35.2) | 48 (33.1) | 0.74 |
| Site of infection | ||||
| Respiratory tract | 104 (43.5) | 42 (46.2) | 62 (41.9) | 0.52 |
| Urinary tract | 58 (24.3) | 25 (27.5) | 33 (22.3) | 0.36 |
| Gastrointestinal tract | 75 (31.4) | 28 (30.8) | 47 (31.8) | 0.87 |
| Skin and soft tissue | 27 (11.3) | 18 (19.8) | 9 (6.1) | <0.01 * |
| CRBSI | 19 (8.0) | 3 (3.3) | 16 (10.8) | 0.04 * |
| Central nervous system | 1 (0.4) | 1 (1.1) | 0 (0.0) | 0.76 |
| Osteoarticular system | 7 (2.9) | 6 (6.6) | 1 (0.7) | 0.03 * |
| Other sites | 10 (4.2) | 7 (7.7) | 3 (2.0) | 0.08 |
| Unknown site | 23 (9.6) | 3 (3.3) | 20 (13.5) | <0.01 * |
| Laboratory findings # | ||||
| Creatinine (μmol/L) | 130.0 [87.1–192.7] | 134.0 [92.0–236.0] | 118.0 [83.4–172.3] | 0.03 * |
| CRP (mg/L) | 166.5 [92.7–249.5] | 172.5 [99.1–249.1] | 163.0 [84.0–249.3] | 0.42 |
| Lactate (mmol/L) | 2.6 [1.7–4.1] | 2.7 [1.8–4.1] | 2.4 [1.6–4.2] | 0.98 |
| Hemoglobin (g/dL) | 9.6 [8.2–11.0] | 10.5 [8.9–12.3] | 9.1 [7.8–10.2] | <0.01 * |
| WBC count (109/L) | 14.1 [9.1–22.3] | 16.4 [11.5–23.1] | 12.3 [5.3–21.6] | <0.01 * |
| Neutrophil count (109/L) | 11.7 [6.6–19.0] | 14.0 [10.1–20.2] | 9.5 [3.8–18.4] | <0.01 * |
| Platelet count (109/L) | 133.0 [63.0–235.0] | 177.0 [110.5–270.5] | 105.0 [34.0–211.5] | <0.01 * |
| ICU stay | ||||
| SAPS II | 51.0 [42.0–68.0] | 50.0 [43.5–65.5] | 55.5 [41.8–68.0] | 0.44 |
| Duration of ATB therapy (days) | 5.0 [3.0–10.5] | 6.0 [3.0–11.0] | 5.0 [2.0–10.3] | 0.25 |
| Antifungal therapy | 121 (50.6) | 33 (36.3) | 88 (59.5) | <0.01 * |
| Catecholamines | 226 (94.6) | 87 (95.6) | 139 (93.9) | 0.81 |
| Renal replacement therapy | 70 (29.3) | 33 (36.3) | 37 (25.0) | 0.06 |
| NIV | 55 (23.0) | 26 (28.6) | 29 (19.6) | 0.11 |
| Mechanical ventilation | 143 (59.8) | 60 (65.9) | 83 (56.1) | 0.13 |
| Duration of MV (days) | 5.0 [2.0–11.0] | 6.0 [2.8–15.5] | 5.0 [2.0–10.5] | 0.38 |
| DIC | 44 (18.6) | 18 (20.0) | 26 (17.8) | 0.67 |
| MODS | 79 (33.1) | 36 (39.6) | 43 (29.1) | 0.09 |
| ARDS | 26 (10.9) | 9 (9.9) | 17 (11.5) | 0.70 |
| Transfusions | 152 (63.6) | 45 (49.5) | 107 (72.3) | <0.01 * |
| Red blood cells | 143 (59.8) | 43 (47.3) | 100 (67.6) | <0.01 * |
| Fresh frozen plasma | 51 (21.3) | 18 (19.8) | 33 (22.3) | 0.64 |
| Platelet concentrates | 87 (36.4) | 18 (19.8) | 69 (46.6) | <0.01 * |
| Advance directives | 13 (5.4) | 6 (6.6) | 7 (4.7) | 0.73 |
| LTE in the ICU | 47 (19.7) | 18 (19.8) | 29 (19.6) | 0.97 |
| Outcome | ||||
| ICU LOS (days) | 5.0 [3.0–13.0] | 6.0 [3.0–15.0] | 5.0 [2.0–11.3] | 0.27 |
| Total LOS (days) | 24.0 [12.0–42.0] | 19.5 [10.8–41.0] | 25.5 [13.8–42.0] | 0.33 |
| Mortality | ||||
| At d28 | 65 (27.3) | 27 (29.7) | 38 (25.9) | 0.52 |
| In the ICU | 72 (30.3) | 27 (30.0) | 45 (30.4) | 0.95 |
| In hospital | 91 (39.2) | 32 (35.6) | 59 (41.6) | 0.36 |
| (a) ICU Mortality | Odds Ratio | 95%CI | p Value |
| Age (years) | 1.00 | [0.98–1.02] | 0.91 |
| Cancer patients with SSh | 1.41 | [0.65–3.04] | 0.38 |
| Solid tumors | 1.48 | [0.62–3.51] | 0.37 |
| Hematological malignancies | 1.33 | [0.53–3.32] | 0.54 |
| ARDS | 1.03 | [0.39–2.75] | 0.95 |
| Renal replacement therapy | 2.29 | [1.06–4.93] | 0.03 * |
| DIC | 5.89 | [2.49–13.92] | <0.01 * |
| Mechanical ventilation | 7.85 | [2.90–21.20] | <0.01 * |
| Nosocomial infection | 1.82 | [0.89–3.69] | 0.10 |
| Bacteremia | 1.39 | [0.67–2.88] | 0.37 |
| (b) In-hospital mortality | |||
| Age (years) | 1.01 | [0.99–1.04] | 0.19 |
| Cancer patients with SSh | 1.99 | [0.98–4.03] | 0.06 |
| Solid tumors | 2.52 | [1.12–5.67] | 0.03 * |
| Hematological malignancies | 1.62 | [0.67–3.87] | 0.28 |
| ARDS | 1.24 | [0.47–3.26] | 0.66 |
| Renal replacement therapy | 2.50 | [1.20–5.20] | 0.01 * |
| DIC | 3.70 | [1.62–8.46] | <0.01 * |
| Mechanical ventilation | 4.56 | [2.15–9.65] | <0.01 * |
| Nosocomial infection | 1.73 | [0.91–3.29] | 0.10 |
| Bacteremia | 1.30 | [0.68–2.50] | 0.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le Borgne, P.; Feuillassier, L.; Schenck, M.; Herbrecht, J.-E.; Janssen-Langenstein, R.; Simand, C.; Gantzer, J.; Nannini, S.; Fornecker, L.-M.; Alamé, K.; et al. Comparison of Short- and Long-Term Mortality in Patients with or without Cancer Admitted to the ICU for Septic Shock: A Retrospective Observational Study. Cancers 2022, 14, 3196. https://doi.org/10.3390/cancers14133196
Le Borgne P, Feuillassier L, Schenck M, Herbrecht J-E, Janssen-Langenstein R, Simand C, Gantzer J, Nannini S, Fornecker L-M, Alamé K, et al. Comparison of Short- and Long-Term Mortality in Patients with or without Cancer Admitted to the ICU for Septic Shock: A Retrospective Observational Study. Cancers. 2022; 14(13):3196. https://doi.org/10.3390/cancers14133196
Chicago/Turabian StyleLe Borgne, Pierrick, Léa Feuillassier, Maleka Schenck, Jean-Etienne Herbrecht, Ralf Janssen-Langenstein, Celestine Simand, Justine Gantzer, Simon Nannini, Luc-Matthieu Fornecker, Karine Alamé, and et al. 2022. "Comparison of Short- and Long-Term Mortality in Patients with or without Cancer Admitted to the ICU for Septic Shock: A Retrospective Observational Study" Cancers 14, no. 13: 3196. https://doi.org/10.3390/cancers14133196