
The Impact of Cancer-Related Fatigue on HRQOL in Survivors of Childhood Cancer: A DCCSS LATER Study

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Design & Participants
2.2. Measures
2.2.1. Fatigue
2.2.2. HRQOL
2.2.3. Other Measures
2.3. Statistical Analysis
3. Results
3.1. Participants
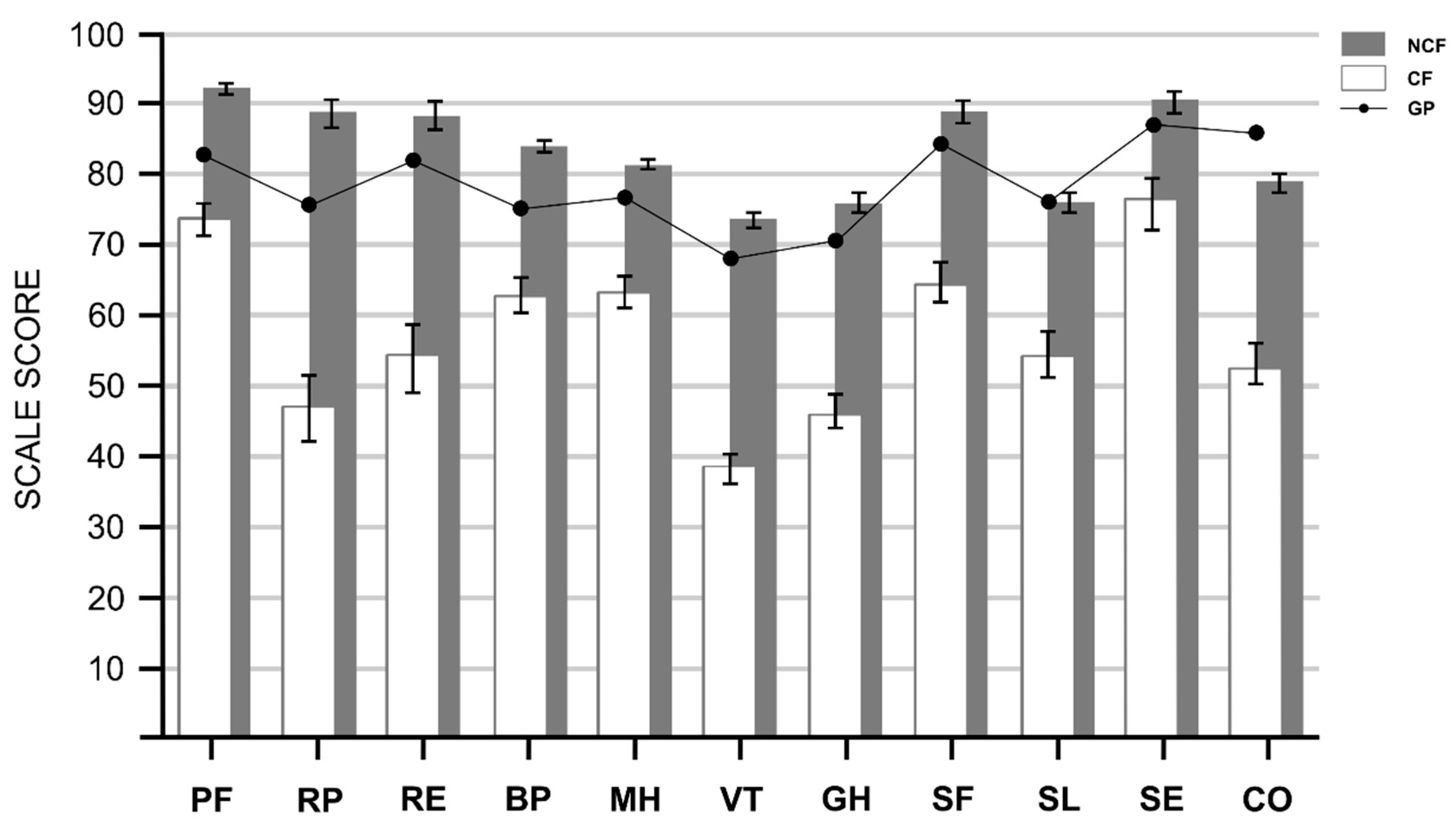
3.2. Chronic Fatigue and HRQOL Scale Scores
3.3. Association Chronic Fatigue with Impaired HRQOL
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Armstrong, G.T.; Chen, Y.; Yasui, Y.; Leisenring, W.; Gibson, T.M.; Mertens, A.C.; Stovall, M.; Oeffinger, K.C.; Bhatia, S.; Krull, K.R.; et al. Reduction in Late Mortality among 5-Year Survivors of Childhood Cancer. New Engl. J. Med. 2016, 374, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Malvezzi, M.; Santucci, C.; Alicandro, G.; Carioli, G.; Boffetta, P.; Dds, K.B.R.; Levi, F.; La Vecchia, C.; Negri, E.; Bertuccio, P. Childhood cancer mortality trends in the Americas and Australasia: An update to 2017. Cancer 2021, 127, 3445–3456. [Google Scholar] [CrossRef] [PubMed]
- Reedijk, A.M.J.; Klein, K.; Coebergh, J.W.W.; Kremer, L.C.; Dinmohamed, A.G.; De Haas, V.; Versluijs, A.B.; Ossenkoppele, G.J.; Beverloo, H.B.; Pieters, R.; et al. Improved survival for children and young adolescents with acute myeloid leukemia: A Dutch study on incidence, survival and mortality. Leukemia 2018, 33, 1349–1359. [Google Scholar] [CrossRef] [PubMed]
- Sitlinger, A.; Zafar, S.Y. Health-Related Quality of Life. Surg. Oncol. Clin. North Am. 2018, 27, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Loonen, J.; Blijlevens, N.M.; Prins, J.; Dona, D.J.; Hartogh, J.D.; Senden, T.; Broeder, E.V.D.-D.; Van Der Velden, K.; Hermens, R.P. Cancer Survivorship Care: Person Centered Care in a Multidisciplinary Shared Care Model. Int. J. Integr. Care 2018, 18, 4. [Google Scholar] [CrossRef]
- Bullinger, M.; Quitmann, J. Quality of life as patient-reported outcomes: Principles of assessment. Dialog-Clin. Neurosci. 2014, 16, 137–145. [Google Scholar] [CrossRef]
- WHOQOL. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- World Health Organization. The Constitution of the World Health Organization. WHO Chron. 1947, 1, 29. [Google Scholar]
- van Gorp, M.; Erp, L.M.E.; Maas, A.; Kremer, L.C.M.; Broeder, E.V.D.-D.; Tissing, W.J.E.; Loonen, J.J.; Pal, H.J.H.; Vries, A.C.H.; Heuvel-Eibrink, M.M.; et al. Increased health-related quality of life impairments of male and female survivors of childhood cancer: DCCSS LATER 2 psycho-oncology study. Cancer 2021, 128, 1074–1084. [Google Scholar] [CrossRef]
- van Erp, L.; Maurice-Stam, H.; Kremer, L.; Tissing, W.; van der Pal, H.; de Vries, A.; Heuvel-Eibrink, M.V.D.; Versluys, B.; Loonen, J.; Bresters, D.; et al. Health-related quality of life in Dutch adult survivors of childhood cancer: A nation-wide cohort study. Eur. J. Cancer 2021, 152, 204–214. [Google Scholar] [CrossRef]
- Hult, M.; Pietilä, A.-M.; Saaranen, T. The Factors Predicting Quality of Life Among Unemployed Adults: A Model Based on Salutogenic Approach. Soc. Indic. Res. 2020, 152, 1197–1211. [Google Scholar] [CrossRef]
- IshidaNaoko, Y.; Sakamoto, N.; Kamibeppu, K.; Kakee, N.; Iwai, T.; Ozono, S.; Maeda, N.; Okamura, J.; Asami, K.; Inada, H.; et al. Late effects and quality of life of childhood cancer survivors: Part 2. Impact of radiotherapy. Int. J. Hematol. 2010, 92, 95–104. [Google Scholar] [CrossRef]
- Blaauwbroek, R.; Groenier, K.H.; Kamps, W.A.; Jong, B.M.-D.; Postma, A. Late effects in adult survivors of childhood cancer: The need for life-long follow-up. Ann. Oncol. 2007, 18, 1898–1902. [Google Scholar] [CrossRef] [PubMed]
- Deuren, S.; Penson, A.; Broeder, E.V.D.-D.; Grootenhuis, M.A.; Loo, M.V.D.H.-V.D.; Bronkhorst, E.; Blijlevens, N.M.A.; Streefkerk, N.; Teepen, J.C.; Tissing, W.J.E.; et al. Prevalence and risk factors of cancer-related fatigue in childhood cancer survivors: A DCCSS LATER study. Cancer 2021, 128, 1110–1121. [Google Scholar] [CrossRef]
- Meeske, K.A.; Patel, S.K.; Palmer, S.N.; Nelson, M.B.; Bs, A.M.P. Factors associated with health-related quality of life in pediatric cancer survivors. Pediatr. Blood Cancer 2006, 49, 298–305. [Google Scholar] [CrossRef]
- Mulrooney, D.A.; Ness, K.K.; Neglia, J.; Whitton, J.A.; Green, D.M.; Zeltzer, L.K.; Robison, L.L.; Mertens, A.C. Fatigue and Sleep Disturbance in Adult Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study (CCSS). Sleep 2008, 31, 271–281. [Google Scholar] [CrossRef]
- Jóhannsdóttir, I.M.; Hjermstad, M.J.; Moum, T.; Wesenberg, F.; Hjorth, L.; Schrøder, H.; Mört, S.; Jónmundsson, G.; Loge, J.H. Increased prevalence of chronic fatigue among survivors of childhood cancers: A population-based study. Pediatr. Blood Cancer 2011, 58, 415–420. [Google Scholar] [CrossRef]
- Frederick, N.N.; Kenney, L.; Vrooman, L.; Recklitis, C.J. Fatigue in adolescent and adult survivors of non-CNS childhood cancer: A report from project REACH. Support. Care Cancer 2016, 24, 3951–3959. [Google Scholar] [CrossRef]
- Schulte, F.; Chen, Y.; Yasui, Y.; Leisenring, W.M.; Gibson, T.M.; Nathan, P.C.; Oeffinger, K.C.; Hudson, M.M.; Armstrong, G.T.; Robison, L.L.; et al. Predicting decreased health-related quality of life (HRQL) in adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study (CCSS). J. Clin. Oncol. 2021, 39, 10043. [Google Scholar] [CrossRef]
- Zeltzer, L.K.; Lu, Q.; Leisenring, W.; Tsao, J.C.; Recklitis, C.; Armstrong, G.; Mertens, A.C.; Robison, L.L.; Ness, K.K. Psychosocial Outcomes and Health-Related Quality of Life in Adult Childhood Cancer Survivors: A Report from the Childhood Cancer Survivor Study. Cancer Epidemiol. Biomark. Prev. 2008, 17, 435–446. [Google Scholar] [CrossRef] [Green Version]
- Penson, A.; van Deuren, S.; Bronkhorst, E.; Keizer, E.; Heskes, T.; Coenen, M.J.H.; Rosmalen, J.G.M.; Tissing, W.J.E.; van der Pal, H.J.H.; de Vries, A.C.H.; et al. Methodology of the DCCSS later fatigue study: A model to investigate chronic fatigue in long-term survivors of childhood cancer. BMC Med. Res. Methodol. 2021, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Teepen, J.C.; Kremer, L.; Ronckers, C.M.; van Leeuwen, F.E.; Hauptmann, M.; Dulmen-Den Broeder, V.; Van Der Pal, H.J.; Jaspers, M.W.; Tissing, W.J.; Den Heuvel-Eibrink, V. Long-term risk of subsequent malignant neoplasms after treatment of childhood cancer in the DCOG LATER study cohort: Role of chemotherapy. J. Clin. Oncol. 2017, 35, 2288–2298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazelhoff J, R.C.; Jaspers, M.W.M.; van den Bos, C.; Agtereek, N.; Postma, A.; Hakvoort-Cammel, F.G.A.J.; Bökkerink, J.P.M.; van Dulmen-den Broeder, E.; Versluys, A.B.; Bresters, D.; et al. LATER: A nation-wide registry of 5-yr survivors of childhood cancer in the Netherlands. Abstract. In Proceedings of the 10th International Conference on Long-Term Complications of Treatment of Children and Adolescents for Cancer, Niagara-on-the-Lake, ON, Canada, 6–7 June 2008. [Google Scholar]
- Vercoulen, J.H.M.M.; Swanink, C.M.A.; Fennis, J.F.M.; Galama, J.M.D.; van der Meer, J.W.M.; Bleijenberg, G. Dimensional assessment of chronic fatigue syndrome. J. Psychosom. Res. 1994, 38, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Worm-Smeitink, M.; Gielissen, M.; Bloot, L.; van Laarhoven, H.; van Engelen, B.; van Riel, P.; Bleijenberg, G.; Nikolaus, S.; Knoop, H. The assessment of fatigue: Psychometric qualities and norms for the Checklist individual strength. J. Psychosom. Res. 2017, 98, 40–46. [Google Scholar] [CrossRef]
- Penson, A.; Walraven, I.; Bronkhorst, E.; Grootenhuis, M.A.; Tissing, W.J.E.; van der Pal, H.J.H.; de Vries, A.C.H.; Heuvel-Eibrink, M.M.V.D.; Neggers, S.; Versluys, B.A.B.; et al. Assessing fatigue in childhood cancer survivors: Psychometric properties of the Checklist Individual Strength and the Short Fatigue Questionnaire––A DCCSS LATER study. Cancer Med. 2021. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A.; International Chronic Fatigue Syndrome Study Group. The Chronic Fatigue Syndrome: A Comprehensive Approach to Its Definition and Study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 473–483. [Google Scholar] [CrossRef]
- Mchorney, C.A.; Ware, J.E., Jr.; Raczek, A.E. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.; Ma, K.; Keller, S.D. SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Health Assess. Lab. 1993, 8, 23–28. [Google Scholar]
- Aaronson, N.K.; Muller, M.; Cohen, P.D.; Essink-Bot, M.-L.; Fekkes, M.; Sanderman, R.; Sprangers, M.A.; Velde, A.T.; Verrips, E. Translation, Validation, and Norming of the Dutch Language Version of the SF-36 Health Survey in Community and Chronic Disease Populations. J. Clin. Epidemiol. 1998, 51, 1055–1068. [Google Scholar] [CrossRef]
- Bruil, J.; Fekkers, M.; Vogel, T.; Verrips, E. The Validity and Reliability of the TAAQOL: A Health-Related Quality of Life Instrument Comprising Health Status Weighted by the Impact of Problems on Well Being. Qual. Life Res. 2001, 10, 257. [Google Scholar]
- Bruil, J.; Fekkes, M.; Vogel, T.; Verrips, G.H.W. TAAQOL Manual. Available online: https://www.tno.nl/media/4727/vragenlijsten_01032012.pdf (accessed on 7 January 2021).
- Kamphuis, M.; Zwinderman, K.; Vogels, T.; Vliegen, H.; Kamphuis, R.; Ottenkamp, J.; Verloove-Vanhorick, S.; Bruil, J. A cardiac-specific health-related quality of life module for young adults with congenital heart disease: Development and validation. Qual. Life Res. 2004, 13, 735–745. [Google Scholar] [CrossRef] [PubMed]
- van Deuren, S.; Boonstra, A.; Broeder, E.V.D.-D.; Blijlevens, N.; Knoop, H.; Loonen, J. Severe fatigue after treatment for childhood cancer. Cochrane Database Syst. Rev. 2020, 2020, CD012681. [Google Scholar] [CrossRef]
- Merchant, J.A.; Kelly, K.M.; Burmeister, L.F.; Lozier, M.J.; Amendola, A.; Lind, D.P.; KcKeen, A.; Slater, T.; Hall, J.L.; Rohlman, D.S.; et al. Employment Status Matters. J. Occup. Environ. Med. 2014, 56, 686–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edgerton, J.; Roberts, L.; Below, S.V. Education and Quality of Life. In Handbook of Social Indicators and Quality of Life Research; Land, K., Michalos, A., Sirgy, M., Eds.; Springer: Dordrecht, The Netherlands, 2012; pp. 265–296. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Streefkerk, N.; Tissing, W.J.E.; Loo, M.V.D.H.-V.D.; Feijen, E.A.M.; Broeder, E.V.D.-D.; Loonen, J.J.; Van Der Pal, H.J.H.; Ronckers, C.M.; Van Santen, H.M.; Berg, M.H.V.D.; et al. The Dutch LATER physical outcomes set for self-reported data in survivors of childhood cancer. J. Cancer Surviv. 2020, 14, 666–676. [Google Scholar] [CrossRef]
- Donders, A.R.T.; van der Heijden, G.J.; Stijnen, T.; Moons, K.G. Review: A gentle introduction to imputation of missing values. J. Clin. Epidemiol. 2006, 59, 1087–1091. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 81. [Google Scholar]
- Marshall, A.; Altman, D.G.; Holder, R.L.; Royston, P. Combining estimates of interest in prognostic modelling studies after multiple imputation: Current practice and guidelines. BMC Med. Res. Methodol. 2009, 9, 57. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis: A Global Perspective; Pearson: London, UK, 2010. [Google Scholar]
- Jones, S.M.W.; Lacroix, A.Z.; Li, W.; Zaslavsky, O.; Wassertheil-Smoller, S.; Weitlauf, J.C.; Brenes, G.A.; Nassir, R.; Ockene, J.K.; Caire-Juvera, G.; et al. Depression and quality of life before and after breast cancer diagnosis in older women from the Women’s Health Initiative. J. Cancer Surviv. 2015, 9, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Crouch, A.; Champion, V.L.; Von Ah, D. Comorbidity, cognitive dysfunction, physical functioning, and quality of life in older breast cancer survivors. Support. Care Cancer 2021, 30, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Jelsness-Jørgensen, L.-P.; Bernklev, T.; Henriksen, M.; Torp, R.; Moum, B.A. Chronic fatigue is associated with impaired health-related quality of life in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2010, 33, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Siciliano, M.; Trojano, L.; Santangelo, G.; De Micco, R.; Tedeschi, G.; Tessitore, A. Fatigue in Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2018, 33, 1712–1723. [Google Scholar] [CrossRef] [PubMed]
- Katz, P. Fatigue in Rheumatoid Arthritis. Curr. Rheumatol. Rep. 2017, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Åkerlund, E.; Sunnerhagen, K.S.; Persson, H.C. Fatigue after acquired brain injury impacts health-related quality of life: An exploratory cohort study. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Christen, S.; Roser, K.; Mulder, R.L.; Ilic, A.; Lie, H.C.; Loonen, J.J.; Mellblom, A.V.; Kremer, L.C.M.; Hudson, M.M.; Constine, L.S.; et al. Recommendations for the surveillance of cancer-related fatigue in childhood, adolescent, and young adult cancer survivors: A report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. J. Cancer Surviv. 2020, 14, 923–938. [Google Scholar] [CrossRef]
- Alberts, M.; Smets, E.M.A.; Vercoulen, J.H.M.M.; Garssen, B.; Bleijenberg, G. Verkorte vermoeidheidsvragenlijst: Een praktisch hulpmiddel bij het scoren van vermoeidheid. Ned. Tijdschr. Geneeskd. 1997, 141, 1526–1530. [Google Scholar]
- Penson, A.; van Deuren, S.; Worm-Smeitink, M.; Bronkhorst, E.; Hoogen, F.H.V.D.; van Engelen, B.G.; Peters, M.; Bleijenberg, G.; Vercoulen, J.H.; Blijlevens, N.; et al. Short fatigue questionnaire: Screening for severe fatigue. J. Psychosom. Res. 2020, 137, 110229. [Google Scholar] [CrossRef]
- van Deuren, S.; Broeder, E.V.D.-D.; Boonstra, A.; Gielissen, M.; Blijlevens, N.; Loonen, J.; Knoop, H. Fatigue-Related Cognitive-Behavioral Factors in Survivors of Childhood Cancer: Comparison with Chronic Fatigue Syndrome and Survivors of Adult-Onset Cancer. J. Adolesc. Young-Adult Oncol. 2021, 10, 92–99. [Google Scholar] [CrossRef]
- Boonstra, A.; Gielissen, M.; Broeder, E.V.D.-D.; Blijlevens, N.; Knoop, H.; Loonen, J. Cognitive Behavior Therapy for Persistent Severe Fatigue in Childhood Cancer Survivors: A Pilot Study. J. Pediatr. Hematol. 2019, 41, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Bak, K.; Berger, A.; Breitbart, W.; Escalante, C.P.; Ganz, P.A.; Schnipper, H.H.; Lacchetti, C.; Ligibel, J.A.; Lyman, G.H.; et al. Screening, Assessment, and Management of Fatigue in Adult Survivors of Cancer: An American Society of Clinical Oncology Clinical Practice Guideline Adaptation. J. Clin. Oncol. 2014, 32, 1840–1850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagola, I.; Morales, J.S.; Alejo, L.B.; Barcelo, O.; Montil, M.; Oliván, J.; Álvarez-Bustos, A.; Cantos, B.; Maximiano, C.; Hidalgo, F.; et al. Concurrent Exercise Interventions in Breast Cancer Survivors with Cancer-related Fatigue. Int. J. Sports Med. 2020, 41, 790–797. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Total Cohort CCS (n = 1695) | CCS NCF (n = 1304) | CCS CF (n = 391) | p-Value e |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||
| Sex | <0.001 | |||
| Male | 878 (51.8) | 735 (56.4) | 143 (36.6) | |
| Female | 817 (48.2) | 569 (43.6) | 248 (63.4) | |
| Age at assessment (years) | 0.050 | |||
| <20 | 30 (1.8) | 26 (2.0) | 4 (1.0) | |
| 20–29 | 485 (28.6) | 390 (29.9) | 95 (24.3) | |
| 30–39 | 656 (38.7) | 501 (38.4) | 155 (39.6) | |
| ≥40 | 525 (30.9) | 387 (29.7) | 137 (35.0) | |
| Age at diagnosis (years) | 0.262 | |||
| 0–5 | 770 (45.4) | 605 (46.4) | 165 (42.2) | |
| 5–10 | 458 (27.0) | 350 (26.8) | 108 (27.6) | |
| 10–15 | 370 (21.8) | 272 (20.9) | 98 (25.1) | |
| 15–18 | 97 (5.7) | 77 (5.9) | 20 (5.1) | |
| Primary childhood cancer diagnosis a | 0.259 | |||
| Leukemia | 581 (34.3) | 459 (35.2) | 122 (31.2) | |
| Non-Hodgkin lymphoma b | 210 (12.4) | 165 (12.7) | 45 (11.5) | |
| Hodgkin lymphoma | 121 (7.1) | 95 (7.3) | 26 (6.6) | |
| CNS | 158 (9.3) | 114 (8.7) | 44 (11.3) | |
| Neuroblastoma | 97 (5.7) | 70 (5.4) | 27 (6.9) | |
| Retinoblastoma | 8 (0.5) | 5 (0.4) | 3 (0.8) | |
| Renal tumors | 193 (11.4) | 150 (11.5) | 43 (11.0) | |
| Hepatic tumors | 17 (1.0) | 16 (1.2) | 1 (0.3) | |
| Bone tumors | 101 (6.0) | 76 (5.8) | 25 (6.4) | |
| Soft tissue tumors | 124 (7.3) | 88 (6.7) | 36 (9.2) | |
| Germ cell tumors | 56 (3.3) | 46 (3.5) | 10 (2.6) | |
| Other and unspecified c | 29 (1.7) | 20 (1.5) | 9 (2.3) | |
| Period of childhood cancer diagnosis | 0.002 | |||
| 1963–1969 | 28 (1.7) | 21 (1.6) | 7 (1.8) | |
| 1970–1979 | 226 (13.3) | 151 (11.6) | 75 (19.2) | |
| 1980–1989 | 542 (32.0) | 423 (32.4) | 119 (30.4) | |
| >1990 | 899 (53.0) | 709 (54.4) | 190 (48.6) | |
| Childhood cancer treatment d | 0.047 | |||
| Surgery only | 109 (6.4) | 81 (6.2) | 28 (7.2) | |
| Chemotherapy, no radiotherapy | 917 (54.1) | 731 (56.1) | 186 (47.6) | |
| Radiotherapy, no chemotherapy | 93 (5.5) | 68 (5.2) | 25 (6.4) | |
| Radiotherapy and chemotherapy | 568 (33.5) | 417 (32.0) | 151 (38.6) | |
| No treatment/treatment unknown | 8 (0.5) | 7 (0.5) | 1 (0.3) | |
| Recurrence | 0.460 | |||
| No | 1468 (86.6) | 1125 (86.3) | 343 (87.7) | |
| Yes | 227 (13.4) | 179 (13.7) | 48 (12.3) |
| HRQOL Subscale | Unadjusted OR | 95% CI | Adjusted OR a | 95% CI | Adjusted OR b | 95% CI |
|---|---|---|---|---|---|---|
| SF-36 | ||||||
| PF | 4.24 | 3.34–7.66 | 3.68 | 2.01–6.72 | 2.01 | 0.95–4.26 |
| RP | 11.47 | 7.99–16.46 | 10.16 | 7.05–14.66 | 6.34 | 4.19–9.56 |
| RE | 9.13 | 6.58–12.67 | 8.81 | 6.30–12.30 | 4.01 | 2.67–6.04 |
| BP | 10.42 | 5.34–20.33 | 8.52 | 4.33–16.76 | 5.72 | 2.64–12.39 |
| MH | 12.58 | 6.53–24.26 | 14.92 | 7.58–29.34 | 2.47 | 1.04–5.84 |
| VT | 49.66 | 28.63–86.13 | 52.69 | 30.03–92.44 | 30.35 | 16.41–56.16 |
| GH | 13.06 | 8.11–21.03 | 12.05 | 7.43–19.55 | 6.88 | 3.94–12.01 |
| SF | 10.84 | 6.94–16.93 | 10.59 | 6.72–16.71 | 3.87 | 2.26–6.63 |
| TAAQOL | ||||||
| SL | 5.02 | 3.58–7.03 | 4.56 | 3.23–6.43 | n/a * | n/a * |
| SE | 4.44 | 2.99–6.59 | 4.14 | 2.77–6.19 | 2.08 | 1.28–3.38 |
| CO | 6.29 | 4.84–8.19 | 6.07 | 4.63–7.94 | 3.06 | 2.21–4.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penson, A.; Walraven, I.; Bronkhorst, E.; Maurice-Stam, H.; Grootenhuis, M.A.; Van der Heiden-van der Loo, M.; Tissing, W.J.E.; Van der Pal, H.J.H.; De Vries, A.C.H.; Bresters, D.; et al. The Impact of Cancer-Related Fatigue on HRQOL in Survivors of Childhood Cancer: A DCCSS LATER Study. Cancers 2022, 14, 2851. https://doi.org/10.3390/cancers14122851
Penson A, Walraven I, Bronkhorst E, Maurice-Stam H, Grootenhuis MA, Van der Heiden-van der Loo M, Tissing WJE, Van der Pal HJH, De Vries ACH, Bresters D, et al. The Impact of Cancer-Related Fatigue on HRQOL in Survivors of Childhood Cancer: A DCCSS LATER Study. Cancers. 2022; 14(12):2851. https://doi.org/10.3390/cancers14122851
Chicago/Turabian StylePenson, Adriaan, Iris Walraven, Ewald Bronkhorst, Heleen Maurice-Stam, Martha A. Grootenhuis, Margriet Van der Heiden-van der Loo, Wim J. E. Tissing, Helena J. H. Van der Pal, Andrica C. H. De Vries, Dorine Bresters, and et al. 2022. "The Impact of Cancer-Related Fatigue on HRQOL in Survivors of Childhood Cancer: A DCCSS LATER Study" Cancers 14, no. 12: 2851. https://doi.org/10.3390/cancers14122851