
Associations between Normal Organs and Tumor Burden in Patients Imaged with Fibroblast Activation Protein Inhibitor-Directed Positron Emission Tomography

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Imaging Procedure and Analysis
2.2. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Quantitative Assessment of Normal Organ Radiotracer Uptake and Tumor Burden
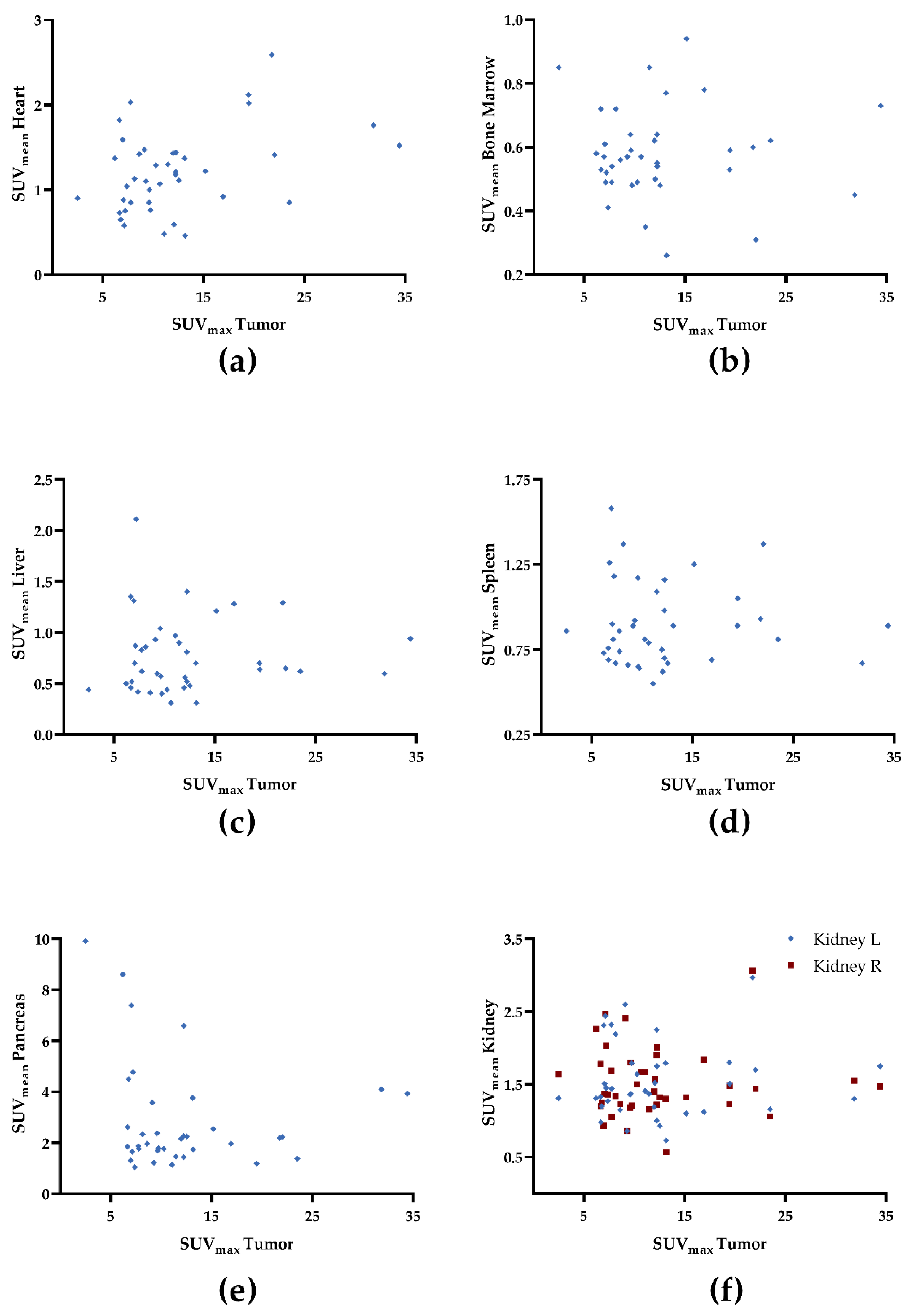
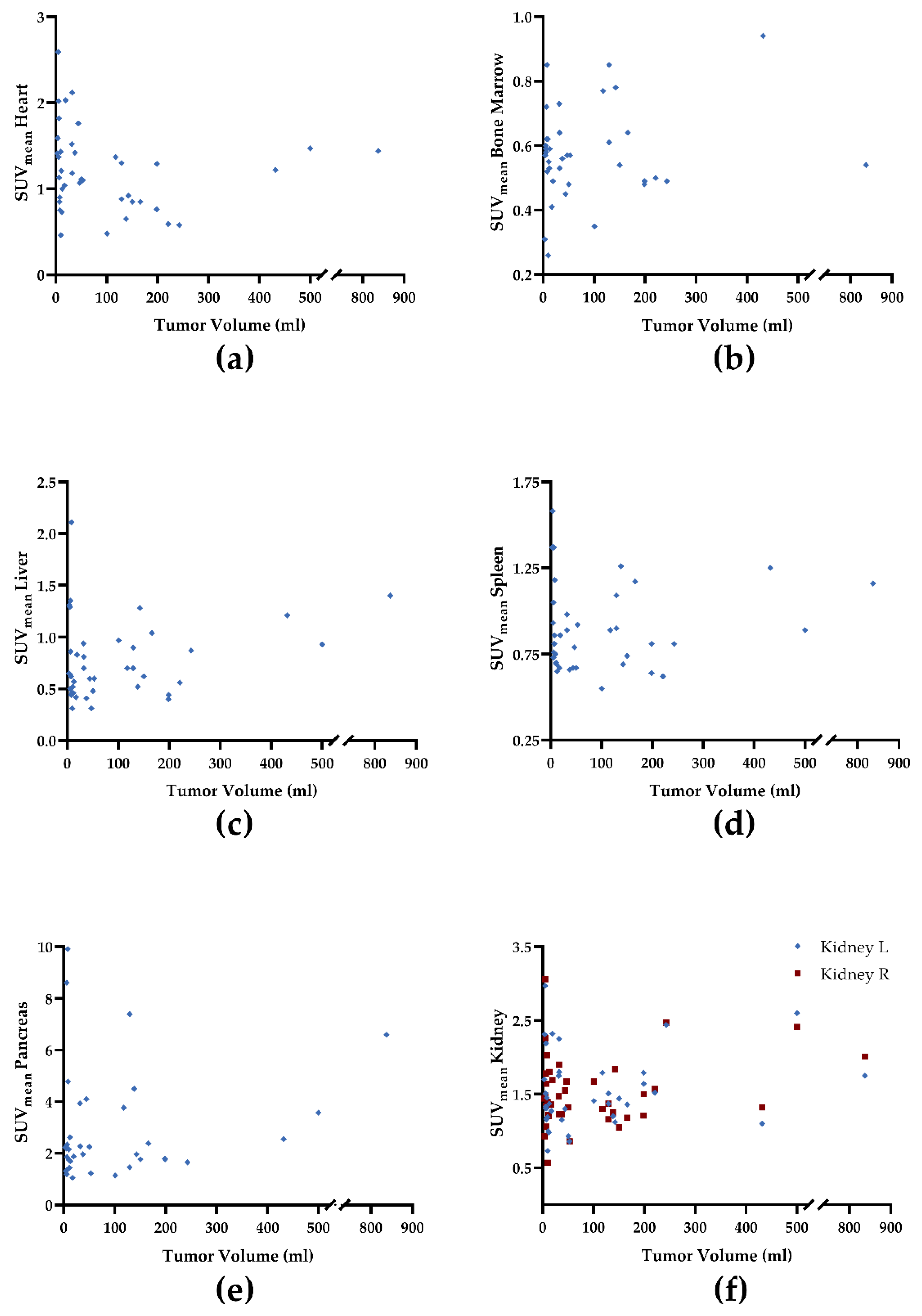
3.3. Correlative Assessment of Normal Organ Radiotracer Uptake and Tumor Burden
3.4. Quantitative and Correlative Assessment of Normal Organ Radiotracer Uptake and Uptake in Post-Surgical Scarring
3.5. Quantitative and Correlative Assessment of Normal Organ Radiotracer Uptake and Tumor Burden in High-Tumor Burden Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kalluri, R. The Biology and Function of Fibroblasts in Cancer. Nat. Rev. Cancer 2016, 16, 582–598. [Google Scholar] [CrossRef]
- Hamson, E.J.; Keane, F.M.; Tholen, S.; Schilling, O.; Gorrell, M.D. Understanding Fibroblast Activation Protein (FAP): Substrates, Activities, Expression and Targeting for Cancer Therapy. Proteom. Clin. Appl. 2014, 8, 454–463. [Google Scholar] [CrossRef]
- Puré, E.; Blomberg, R. Pro-Tumorigenic Roles of Fibroblast Activation Protein in Cancer: Back to the Basics. Oncogene 2018, 37, 4343–4357. [Google Scholar] [CrossRef]
- Gascard, P.; Tlsty, T.D. Carcinoma-Associated Fibroblasts: Orchestrating the Composition of Malignancy. Gene Dev. 2016, 30, 1002–1019. [Google Scholar] [CrossRef]
- Fitzgerald, A.A.; Weiner, L.M. The Role of Fibroblast Activation Protein in Health and Malignancy. Cancer Metast. Rev. 2020, 39, 783–803. [Google Scholar] [CrossRef]
- Barbazán, J.; Vignjevic, D.M. Cancer Associated Fibroblasts: Is the Force the Path to the Dark Side? Curr. Opin. Cell Biol. 2019, 56, 71–79. [Google Scholar] [CrossRef]
- Garin-Chesa, P.; Old, L.J.; Rettig, W.J. Cell Surface Glycoprotein of Reactive Stromal Fibroblasts as a Potential Antibody Target in Human Epithelial Cancers. Proc. Natl. Acad. Sci. USA 1990, 87, 7235–7239. [Google Scholar] [CrossRef] [Green Version]
- Lindner, T.; Loktev, A.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Jäger, D.; Mier, W.; Haberkorn, U. Development of Quinoline-Based Theranostic Ligands for the Targeting of Fibroblast Activation Protein. J. Nucl. Med. 2018, 59, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Giesel, F.L.; Kratochwil, C.; Lindner, T.; Marschalek, M.M.; Loktev, A.; Lehnert, W.; Debus, J.; Jäger, D.; Flechsig, P.; Altmann, A.; et al. 68Ga-FAPI PET/CT: Biodistribution and Preliminary Dosimetry Estimate of 2 DOTA-Containing FAP-Targeting Agents in Patients with Various Cancers. J. Nucl. Med. 2019, 60, 386–392. [Google Scholar] [CrossRef] [Green Version]
- Watabe, T.; Liu, Y.; Kaneda-Nakashima, K.; Shirakami, Y.; Lindner, T.; Ooe, K.; Toyoshima, A.; Nagata, K.; Shimosegawa, E.; Haberkorn, U.; et al. Theranostics Targeting Fibroblast Activation Protein in the Tumor Stroma: 64Cu and 225Ac Labelled FAPI-04 in Pancreatic Cancer Xenograft Mouse Models. J. Nucl. Med. 2019, 61, 563–569. [Google Scholar] [CrossRef]
- Ferdinandus, J.; Costa, P.F.; Kessler, L.; Weber, M.; Hirmas, N.; Kostbade, K.; Bauer, S.; Schuler, M.; Ahrens, M.; Schildhaus, H.-U.; et al. Initial Clinical Experience with 90 Y-FAPI-46 Radioligand Therapy for Advanced Stage Solid Tumors: A Case Series of Nine Patients. J. Nucl. Med. 2021, 63, 727–734. [Google Scholar] [CrossRef]
- Liu, Y.; Watabe, T.; Kaneda-Nakashima, K.; Shirakami, Y.; Naka, S.; Ooe, K.; Toyoshima, A.; Nagata, K.; Haberkorn, U.; Kratochwil, C.; et al. Fibroblast Activation Protein Targeted Therapy Using [177Lu]FAPI-46 Compared with [225Ac]FAPI-46 in a Pancreatic Cancer Model. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 871–880. [Google Scholar] [CrossRef]
- Xin, L.; Gao, J.; Zheng, Z.; Chen, Y.; Lv, S.; Zhao, Z.; Yu, C.; Yang, X.; Zhang, R. Fibroblast Activation Protein-α as a Target in the Bench-to-Bedside Diagnosis and Treatment of Tumors: A Narrative Review. Front. Oncol. 2021, 11, 648187. [Google Scholar] [CrossRef]
- Beauregard, J.-M.; Hofman, M.S.; Kong, G.; Hicks, R.J. The Tumour Sink Effect on the Biodistribution of 68Ga-DOTA-Octreotate: Implications for Peptide Receptor Radionuclide Therapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 50–56. [Google Scholar] [CrossRef]
- Liu, Y. Super-Superscan on a Bone Scintigraphy. Clin. Nucl. Med. 2011, 36, 227. [Google Scholar] [CrossRef]
- Prasad, V.; Baum, R.P. Biodistribution of the Ga-68 Labeled Somatostatin Analogue DOTA-NOC in Patients with Neuroendocrine Tumors: Characterization of Uptake in Normal Organs and Tumor Lesions. Q. J. Nucl. Med. Mol. Imaging 2010, 54, 61–67. [Google Scholar]
- Gaertner, F.C.; Halabi, K.; Ahmadzadehfar, H.; Kürpig, S.; Eppard, E.; Kotsikopoulos, C.; Liakos, N.; Bundschuh, R.A.; Strunk, H.; Essler, M. Uptake of PSMA-Ligands in Normal Tissues Is Dependent on Tumor Load in Patients with Prostate Cancer. Oncotarget 2017, 8, 55094–55103. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.A.; Hänscheid, H.; Leal, J.P.; Javadi, M.S.; Higuchi, T.; Lodge, M.A.; Buck, A.K.; Pomper, M.G.; Lapa, C.; Rowe, S.P. Impact of Tumor Burden on Quantitative [68Ga] DOTATOC Biodistribution. Mol. Imaging Biol. 2019, 21, 790–798. [Google Scholar] [CrossRef] [Green Version]
- Serfling, S.E.; Lapa, C.; Dreher, N.; Hartrampf, P.E.; Rowe, S.P.; Higuchi, T.; Schirbel, A.; Weich, A.; Hahner, S.; Fassnacht, M.; et al. Impact of Tumor Burden on Normal Organ Distribution in Patients Imaged with CXCR4-Targeted [68Ga]Ga-PentixaFor PET/CT. Mol. Imaging Biol. 2022, 1–7. [Google Scholar] [CrossRef]
- Werner, R.A.; Bundschuh, R.A.; Bundschuh, L.; Lapa, C.; Yin, Y.; Javadi, M.S.; Buck, A.K.; Higuchi, T.; Pienta, K.J.; Pomper, M.G.; et al. Semiquantitative Parameters in PSMA-Targeted PET Imaging with [18F]DCFPyL: Impact of Tumor Burden on Normal Organ Uptake. Mol. Imaging Biol. 2020, 22, 190–197. [Google Scholar] [CrossRef]
- Kessler, L.; Ferdinandus, J.; Hirmas, N.; Zarrad, F.; Nader, M.; Kersting, D.; Weber, M.; Kazek, S.; Sraieb, M.; Hamacher, R.; et al. Pitfalls and Common Findings in 68 Ga-FAPI-PET—A Pictorial Analysis. J. Nucl. Med. 2021. [Google Scholar] [CrossRef]
- Serfling, S.E.; Hartrampf, P.E.; Zhi, Y.; Higuchi, T.; Rowe, S.P.; Bundschuh, L.; Essler, M.; Buck, A.K.; Bundschuh, R.A.; Werner, R.A. Interobserver Agreement Rates on Fibroblast Activation Protein Inhibitor–Directed Molecular Imaging and Therapy. Clin. Nucl. Med. 2022; Publish Ahead of Print. [Google Scholar] [CrossRef]
- Serfling, S.; Zhi, Y.; Schirbel, A.; Lindner, T.; Meyer, T.; Gerhard-Hartmann, E.; Lapa, C.; Hagen, R.; Hackenberg, S.; Buck, A.K.; et al. Improved Cancer Detection in Waldeyer’s Tonsillar Ring by 68Ga-FAPI PET/CT Imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1178–1187. [Google Scholar] [CrossRef]
- Linz, C.; Brands, R.C.; Kertels, O.; Dierks, A.; Brumberg, J.; Gerhard-Hartmann, E.; Hartmann, S.; Schirbel, A.; Serfling, S.; Zhi, Y.; et al. Targeting Fibroblast Activation Protein in Newly Diagnosed Squamous Cell Carcinoma of the Oral Cavity—Initial Experience and Comparison to [18F]FDG PET/CT and MRI. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3951–3960. [Google Scholar] [CrossRef]
- Giesel, F.L.; Kratochwil, C.; Schlittenhardt, J.; Dendl, K.; Eiber, M.; Staudinger, F.; Kessler, L.; Fendler, W.P.; Lindner, T.; Koerber, S.A.; et al. Head-to-Head Intra-Individual Comparison of Biodistribution and Tumor Uptake of 68Ga-FAPI and 18F-FDG PET/CT in Cancer Patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–9. [Google Scholar] [CrossRef]
- Soret, M.; Bacharach, S.L.; Buvat, I. Partial-Volume Effect in PET Tumor Imaging. J. Nucl. Med. 2007, 48, 932–945. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H.; et al. 68 Ga-FAPI PET/CT: Tracer Uptake in 28 Different Kinds of Cancer. J. Nucl. Med. 2019, 60, 801–805. [Google Scholar] [CrossRef] [Green Version]
- Kreppel, B.; Gonzalez-Carmona, M.A.; Feldmann, G.; Küppers, J.; Moon, E.S.; Marinova, M.; Bundschuh, R.A.; Kristiansen, G.; Essler, M.; Roesch, F.; et al. Fibroblast Activation Protein Inhibitor (FAPi) Positive Tumour Fraction on PET/CT Correlates with Ki-67 in Liver Metastases of Neuroendocrine Tumours. Nukl. Nucl. 2021, 60, 344–354. [Google Scholar] [CrossRef]
- Dendl, K.; Koerber, S.A.; Finck, R.; Mokoala, K.M.G.; Staudinger, F.; Schillings, L.; Heger, U.; Röhrich, M.; Kratochwil, C.; Sathekge, M.; et al. 68Ga-FAPI-PET/CT in Patients with Various Gynecological Malignancies. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–12. [Google Scholar] [CrossRef]
- Syed, M.; Flechsig, P.; Liermann, J.; Windisch, P.; Staudinger, F.; Akbaba, S.; Koerber, S.A.; Freudlsperger, C.; Plinkert, P.K.; Debus, J.; et al. Fibroblast Activation Protein Inhibitor (FAPI) PET for Diagnostics and Advanced Targeted Radiotherapy in Head and Neck Cancers. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2836–2845. [Google Scholar] [CrossRef]
- Baum, R.P.; Schuchardt, C.; Singh, A.; Chantadisai, M.; Robiller, F.C.; Zhang, J.; Mueller, D.; Eismant, A.; Almaguel, F.; Zboralski, D.; et al. Feasibility, Biodistribution, and Preliminary Dosimetry in Peptide-Targeted Radionuclide Therapy of Diverse Adenocarcinomas Using 177Lu-FAP-2286: First-in-Humans Results. J. Nucl. Med. 2022, 63, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Cardinale, D.; Dent, S.; Criscitiello, C.; Aseyev, O.; Lenihan, D.; Cipolla, C.M. Cardiotoxicity of Anticancer Treatments: Epidemiology, Detection, and Management. CA Cancer J. Clin. 2016, 66, 309–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werner, R.A.; Thackeray, J.T.; Diekmann, J.; Weiberg, D.; Bauersachs, J.; Bengel, F.M. The Changing Face of Nuclear Cardiology: Guiding Cardiovascular Care toward Molecular Medicine. J. Nucl. Med. 2020, 61, 951–961. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Hess, A.; Koenig, T.; Diekmann, J.; Derlin, T.; Melk, A.; Thackeray, J.T.; Bauersachs, J.; Bengel, F.M. Molecular Imaging of Inflammation Crosstalk along the Cardio-Renal Axis Following Acute Myocardial Infarction. Theranostics 2021, 11, 7984–7994. [Google Scholar] [CrossRef]
- Heckmann, M.B.; Reinhardt, F.; Finke, D.; Katus, H.A.; Haberkorn, U.; Leuschner, F.; Lehmann, L.H. Relationship between Cardiac Fibroblast Activation Protein Activity by Positron Emission Tomography and Cardiovascular Disease. Circ. Cardiovasc. Imaging 2020, 13, 10628. [Google Scholar] [CrossRef]
- Finke, D.; Heckmann, M.B.; Herpel, E.; Katus, H.A.; Haberkorn, U.; Leuschner, F.; Lehmann, L.H. Early Detection of Checkpoint Inhibitor-Associated Myocarditis Using 68Ga-FAPI PET/CT. Front. Cardiovasc. Med. 2021, 8, 614997. [Google Scholar] [CrossRef]
- Toms, J.; Kogler, J.; Maschauer, S.; Daniel, C.; Schmidkonz, C.; Kuwert, T.; Prante, O. Targeting Fibroblast Activation Protein: Radiosynthesis and Preclinical Evaluation of an 18 F-Labeled FAP Inhibitor. J. Nucl. Med. 2020, 61, 1806–1813. [Google Scholar] [CrossRef]
- Ballal, S.; Yadav, M.P.; Moon, E.S.; Kramer, V.S.; Roesch, F.; Kumari, S.; Bal, C. First-In-Human Results on the Biodistribution, Pharmacokinetics, and Dosimetry of [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2. Pharmaceuticals 2021, 14, 1212. [Google Scholar] [CrossRef]
- Werner, R.A.; Derlin, T.; Lapa, C.; Sheikbahaei, S.; Higuchi, T.; Giesel, F.L.; Behr, S.; Drzezga, A.; Kimura, H.; Buck, A.K.; et al. 18F-Labeled, PSMA-Targeted Radiotracers: Leveraging the Advantages of Radiofluorination for Prostate Cancer Molecular Imaging. Theranostics 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Ilhan, H.; Lindner, S.; Todica, A.; Cyran, C.C.; Tiling, R.; Auernhammer, C.J.; Spitzweg, C.; Boeck, S.; Unterrainer, M.; Gildehaus, F.J.; et al. Biodistribution and First Clinical Results of 18F-SiFAlin-TATE PET: A Novel 18F-Labeled Somatostatin Analog for Imaging of Neuroendocrine Tumors. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 870–880. [Google Scholar] [CrossRef]
- Kou, Y.; Jiang, X.; Yao, Y.; Shen, J.; Jiang, X.; Chen, S.; Lu, H.; Wang, X.; Zhao, M.; Xiao, D.; et al. Physiological Tracer Distribution and Benign Lesion Incidental Uptake of Al18F-NOTA-FAPI-04 on PET/CT Imaging. Nucl. Med. Commun. 2022; Publish Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Hänscheid, H.; Lapa, C.; Buck, A.K.; Lassmann, M.; Werner, R.A. Dose Mapping After Endoradiotherapy with 177Lu-DOTATATE/DOTATOC by a Single Measurement after 4 Days. J. Nucl. Med. 2018, 59, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filss, C.; Heinzel, A.; Miiller, B.; Vogg, A.; Langen, K.-J.; Mottaghy, F. Relevant Tumor Sink Effect in Prostate Cancer Patients Receiving 177Lu-PSMA-617 Radioligand Therapy. Nuklearmed 2018, 57, 19–25. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of patients | 34 | |
| Number of scans | 40 | |
| Age 1 | 62.3 ± 12.5 years | |
| Gender (female) | 16/34 (47.1%) | |
| Tumor entity 2 | NEN | 24/40 (60.0%) |
| PDAC | 6/40 (15.0%) | |
| HCC | 5/40 (12.5%) | |
| Other * | 5/40 (12.5%) | |
| Indication for scan 2 | Primary staging | 14/40 (35.0%) |
| Restaging | 26/40 (55.0%) | |
| Prior therapies 2 | In total | 29/40 (72.5%) |
| Surgery | 22/29 (75.9%) | |
| Chemotherapy | 20/29 (69.0%) | |
| Radiotherapy | 6/29 (20.7%) |
| Parameter | Minimum | Median | Maximum | Mean 1 | SD 1 | ||
|---|---|---|---|---|---|---|---|
| Normal Organs | Heart | SUVmean | 0.46 | 1.20 | 2.59 | 1.22 | 0.48 |
| BM | SUVmean | 0.26 | 0.57 | 0.94 | 0.58 | 0.14 | |
| Liver | SUVmean | 0.31 | 0.65 | 2.11 | |||
| Spleen | SUVmean | 0.55 | 0.86 | 1.58 | |||
| Pancreas | SUVmean | 1.05 | 2.15 | 9.91 | |||
| Kidney R | SUVmean | 0.57 | 1.42 | 3.06 | |||
| Kidney L | SUVmean | 0.73 | 1.41 | 2.97 | |||
| Tumor Burden | SUVmax | 2.48 | 10.5 | 34.4 | |||
| TV | 3.00 | 35.0 | 838 | ||||
| FTA | 11.8 | 313 | 7155 |
| Tumor Burden | |||||
|---|---|---|---|---|---|
| SUVmax | TV | FTA | |||
| Normal Organs | Heart | ρ | 0.29 | −0.30 | −0.16 |
| p | 0.07 | 0.06 | 0.31 | ||
| Bone Marrow | ρ | 0.00 | −0.05 | −0.02 | |
| p | 0.99 | 0.75 | 0.92 | ||
| Liver | ρ | 0.10 | 0.06 | 0.14 | |
| p | 0.53 | 0.73 | 0.38 | ||
| Spleen | ρ | 0.02 | −0.13 | −0.13 | |
| p | 0.91 | 0.43 | 0.42 | ||
| Pancreas | ρ | −0.14 | 0.11 | 0.05 | |
| p | 0.42 | 0.52 | 0.78 | ||
| Right Kidney | ρ | −0.05 | 0.01 | 0.04 | |
| p | 0.75 | 0.97 | 0.80 | ||
| Left Kidney | ρ | 0.00 | 0.06 | 0.10 | |
| p | 0.99 | 0.73 | 0.53 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosmala, A.; Serfling, S.E.; Dreher, N.; Lindner, T.; Schirbel, A.; Lapa, C.; Higuchi, T.; Buck, A.K.; Weich, A.; Werner, R.A. Associations between Normal Organs and Tumor Burden in Patients Imaged with Fibroblast Activation Protein Inhibitor-Directed Positron Emission Tomography. Cancers 2022, 14, 2609. https://doi.org/10.3390/cancers14112609
Kosmala A, Serfling SE, Dreher N, Lindner T, Schirbel A, Lapa C, Higuchi T, Buck AK, Weich A, Werner RA. Associations between Normal Organs and Tumor Burden in Patients Imaged with Fibroblast Activation Protein Inhibitor-Directed Positron Emission Tomography. Cancers. 2022; 14(11):2609. https://doi.org/10.3390/cancers14112609
Chicago/Turabian StyleKosmala, Aleksander, Sebastian E. Serfling, Niklas Dreher, Thomas Lindner, Andreas Schirbel, Constantin Lapa, Takahiro Higuchi, Andreas K. Buck, Alexander Weich, and Rudolf A. Werner. 2022. "Associations between Normal Organs and Tumor Burden in Patients Imaged with Fibroblast Activation Protein Inhibitor-Directed Positron Emission Tomography" Cancers 14, no. 11: 2609. https://doi.org/10.3390/cancers14112609