
Does Tumor Volume Have a Prognostic Role in Oropharyngeal Squamous Cell Carcinoma? A Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Source and Study Searching
2.3. Data Collection Process
2.4. Study Quality Assessment
2.5. Data Synthesis and Statistical Analysis
3. Results
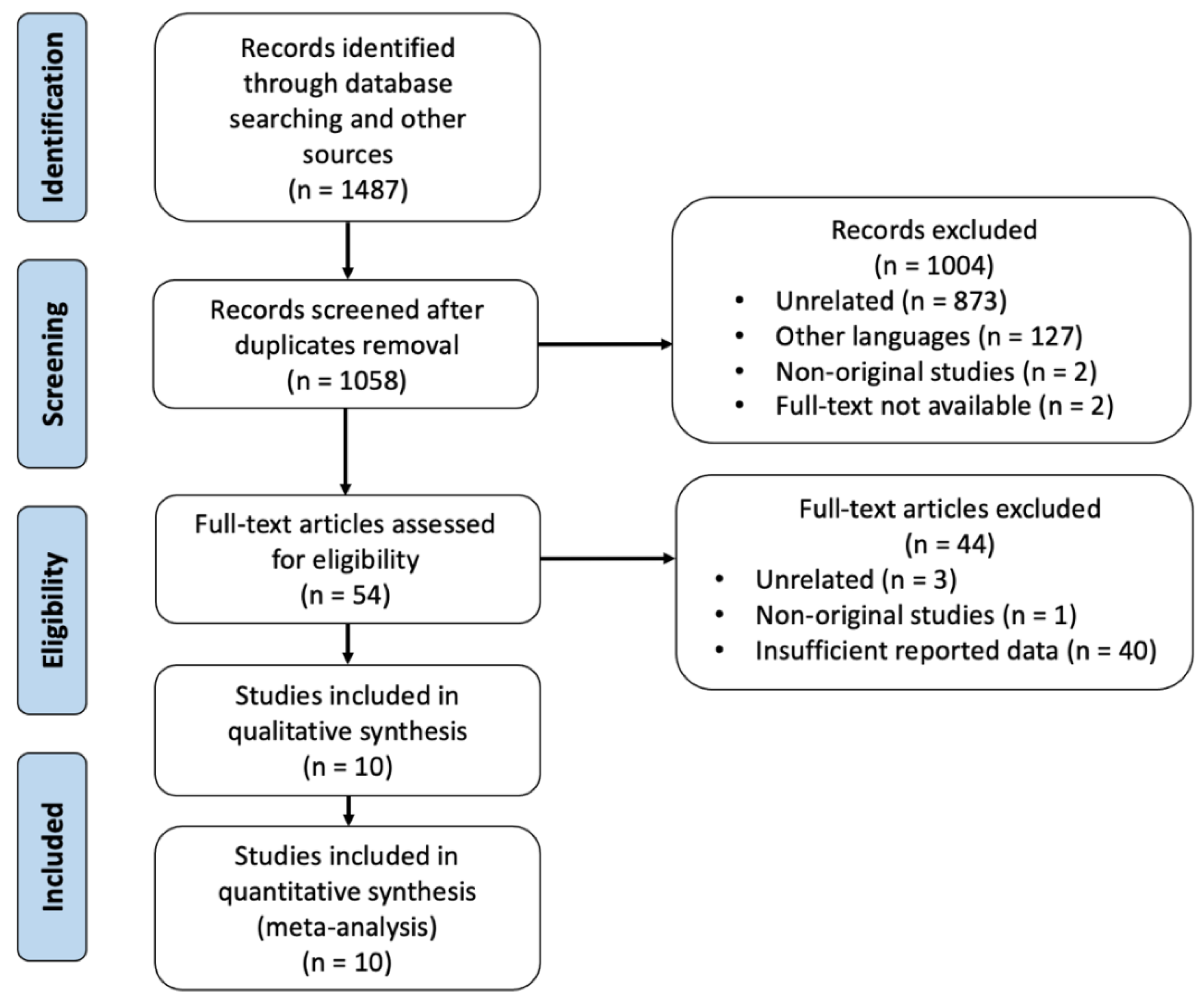
3.1. Search Results and Studies Description
3.2. Methodological Quality and Risk of Bias of Included Studies
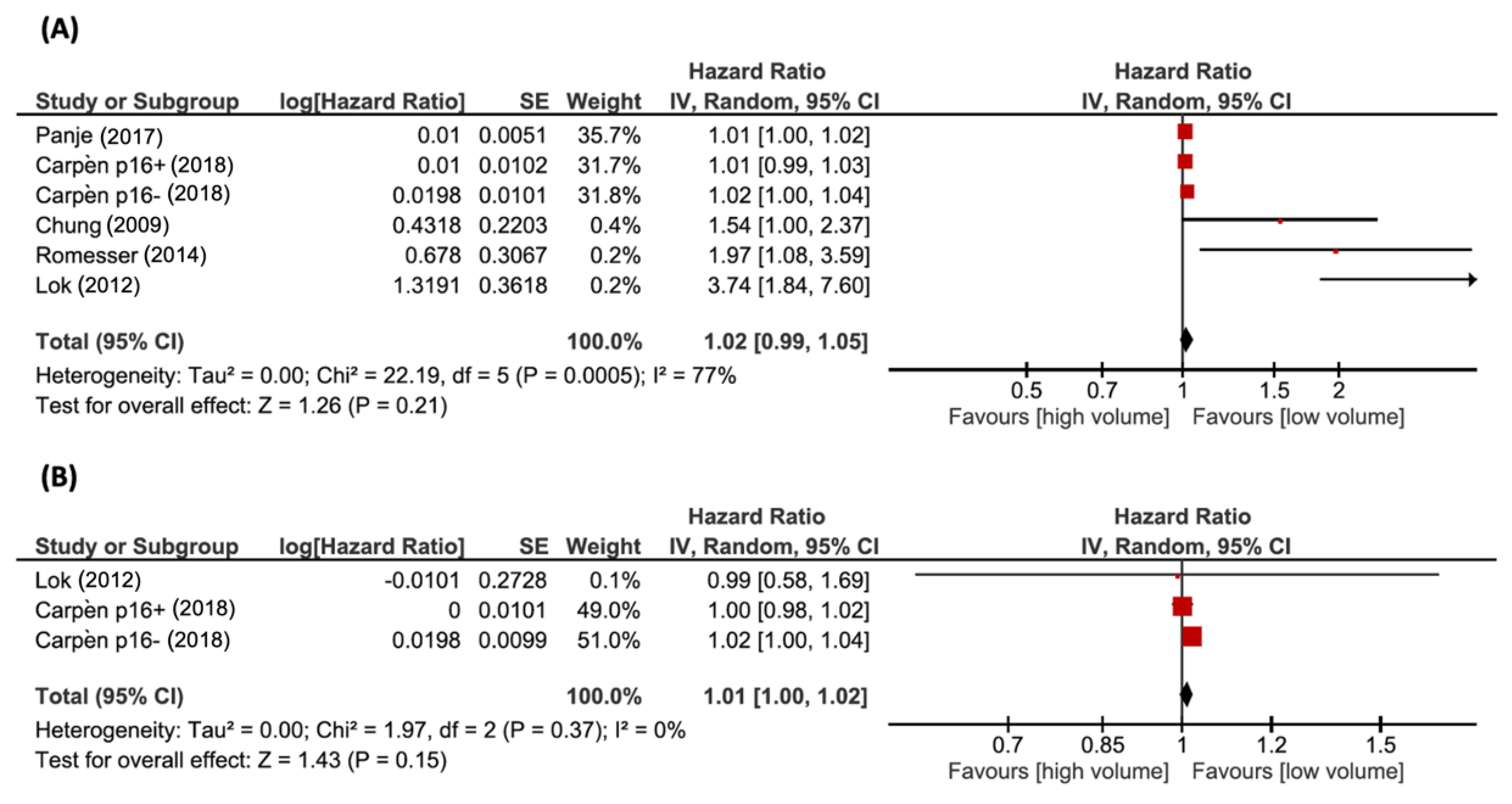
3.3. Overall Survival
3.4. Disease-Free Survival
3.5. Locoregional Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westra, W.H. The Changing Face of Head and Neck Cancer in the 21st Century: The Impact of HPV on the Epidemiology and Pathology of Oral Cancer. Head Neck Pathol. 2009, 3, 78–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States. J. Clin. Oncol. 2011, 29, 4294–4301. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; D’Souza, G.; Westra, W.; Sugar, E.; Xiao, W.; Begum, S.; Viscidi, R. Distinct Risk Factor Profiles for Human Papillomavirus Type 16–Positive and Human Papillomavirus Type 16–Negative Head and Neck Cancers. J. Natl. Cancer Inst. 2008, 100, 407–420. [Google Scholar] [CrossRef] [Green Version]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved Survival of Patients with Human Papillomavirus-Positive Head and Neck Squamous Cell Carcinoma in a Prospective Clinical Trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.H.; Gillison, M.L. Human Papillomavirus in Head and Neck Cancer: Its Role in Pathogenesis and Clinical Implications. Clin. Cancer Res. 2009, 15, 6758–6762. [Google Scholar] [CrossRef] [Green Version]
- Kraas, J.R.; Underhill, T.E.; D’Agostino, R.B., Jr.; Williams, D.W., 3rd; Cox, J.A.; Greven, K.M. Quantitative analysis from CT is prognostic for local control of supraglottic carcinoma. Head Neck 2001, 23, 1031–1036. [Google Scholar] [CrossRef]
- Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Hinerman, R.W.; Mancuso, A.A. Parameters that predict local control after definitive radiotherapy for squamous cell carcinoma of the head and neck. Head Neck 2003, 25, 535–542. [Google Scholar] [CrossRef]
- Hermans, R.; Van den Bogaert, W.; Rijnders, A.; Doornaert, P.; Baert, A.L. Predicting the local outcome of glottic squamous cell carcinoma after definitive radiation therapy: Value of computed tomography-determined tumour parameters. Radiother. Oncol. 1999, 50, 39–46. [Google Scholar] [CrossRef]
- Chen, S.W.; Yang, S.N.; Liang, J.A.; Tsai, M.H.; Shiau, A.C.; Lin, F.J. Value of Computed Tomography-Based Tumor Volume as a Predictor of Outcomes in Hypopharyngeal Cancer After Treatment with Definitive Radiotherapy. Laryngoscope 2006, 116, 2012–2017. [Google Scholar] [CrossRef]
- Chua, D.T.; Sham, J.S.; Kwong, D.L.; Tai, K.S.; Wu, P.M.; Lo, M.; Yung, A.; Choy, D.; Leong, L. Volumetric analysis of tumor extent in nasopharyngeal carcinoma and correlation with treatment outcome. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 711–719. [Google Scholar] [CrossRef]
- Pameijer, F.A.; Mancuso, A.A.; Mendenhall, W.M.; Parsons, J.T.; Mukherji, S.K.; Hermans, R.; Kubilis, P.S. Evaluation of pretreatment computed tomography as a predictor of local control in T1/T2 pyriform sinus carcinoma treated with definitive radiotherapy. Head Neck 1998, 20, 159–168. [Google Scholar] [CrossRef]
- Le Tourneau, C.; Velten, M.; Jung, G.M.; Bronner, G.; Flesch, H.; Borel, C. Prognostic indicators for survival in head and neck squamous cell carcinomas: Analysis of a series of 621 cases. Head Neck 2005, 27, 801–808. [Google Scholar] [CrossRef]
- Keberle, M.; Hoppe, F.; Dotzel, S.; Hahn, D. Computertomographische Vorhersagbarkeit Lokaler Rezidive nach primär operativer Resektion von Oropharynxkarzinomen [Prognostic value of pretreatment CT regarding local control in oropharyngeal cancer after primary surgical resection]. Rofo 2003, 175, 61–66. (In German) [Google Scholar] [CrossRef] [PubMed]
- Nathu, R.M.; Mancuso, A.A.; Zhu, T.C.; Mendenhall, W.M. The impact of primary tumor volume on local control for oropharyngeal squamous cell carcinoma treated with radiotherapy. Head Neck 2000, 22, 1–5. [Google Scholar] [CrossRef]
- Been, M.J.; Watkins, J.; Manz, R.M.; Gentry, L.R.; Leverson, G.E.; Harari, P.M.; Hartig, G.K. Tumor volume as a prognostic factor in oropharyngeal squamous cell carcinoma treated with primary radiotherapy. Laryngoscope 2008, 118, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Chao, K.S.; Ozyigit, G.; Blanco, A.I.; Thorstad, W.L.; Deasy, J.O.; Haughey, B.H.; Spector, G.J.; Sessions, D.G. Intensity-modulated radiation therapy for oropharyngeal carcinoma: Impact of tumor volume. Int. J. Radiat. Oncol. Biol. Phys. 2004, 1, 43–50. [Google Scholar] [CrossRef]
- Lok, B.H.; Setton, J.; Caria, N.; Romanyshyn, J.; Wolden, S.L.; Zelefsky, M.J.; Park, J.; Rowan, N.; Sherman, E.J.; Fury, M.G.; et al. Intensity-modulated radiation therapy in oropharyngeal carcinoma: Effect of tumor volume on clinical outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1851–1857. [Google Scholar] [CrossRef] [Green Version]
- Studer, G.; Lütolf, U.M.; El-Bassiouni, M.; Rousson, V.; Glanzmann, C. Volumetric staging (VS) is superior to TNM and AJCC staging in predicting outcome of head and neck cancer treated with IMRT. Acta Oncol. 2007, 46, 386–394. [Google Scholar] [CrossRef]
- Johnson, C.R.; Thames, H.D.; Huang, D.T.; Schmidt-Ullrich, R.K. The tumor volume and clonogen number relationship: Tumor control predictions based upon tumor volume estimates derived from computed tomography. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 281–287. [Google Scholar] [CrossRef]
- Hermans, R.; de Beeck, K.O.; Van den Bogaert, W.; Rijnders, A.; Staelens, L.; Feron, M.; Bellon, E. The relation of CT-determined tumor parameters and local and regional outcome of tonsillar cancer after definitive radiation treatment. Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 37–45. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzschet, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Methods for the Development of NICE Public Health Guidance; National Institute for Health and Care Excellence (NICE): London, UK, 2012. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010, 7, e1000251. [Google Scholar] [CrossRef]
- Kober, T.; Trelle, S.; Engert, A. Reporting of randomized controlled trials in Hodgkin lymphoma in biomedical journals. J. Natl. Cancer Inst. 2006, 98, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Ziogas, D.C.; Zintzaras, E. Analysis of the quality of reporting of randomized controlled trials in acute and chronic myeloid leukemia, and myelodysplastic syndromes as governed by the CONSORT statement. Ann. Epidemiol. 2009, 19, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [updated March 2011]; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Adrian, G.; Gebre-Medhin, M.; Kjellén, E.; Wieslander, E.; Zackrisson, B.; Nilsson, P. Altered fractionation diminishes importance of tumor volume in oropharyngeal cancer: Subgroup analysis of ARTSCAN-trial. Head Neck 2020, 42, 2099–2105. [Google Scholar] [CrossRef]
- Carpén, T.; Saarilahti, K.; Haglund, C.; Markkola, A.; Tarkkanen, J.; Hagström, J.; Mattila, P.; Mäkitie, A. Tumor volume as a prognostic marker in p16-positive and p16-negative oropharyngeal cancer patients treated with definitive intensity-modulated radiotherapy. Strahlenther. Onkol. 2018, 194, 759–770. (In English) [Google Scholar] [CrossRef] [Green Version]
- Chung, E.J.; Lee, N.J.; Baek, S.K.; Kwon, S.Y.; Woo, J.S.; Jung, K.Y. Clinical efficacy of primary tumor volume measurements: Comparison of different primary sites. Clin. Exp. Otorhinolaryngol. 2009, 2, 78–84. [Google Scholar] [CrossRef]
- Davis, K.S.; Lim, C.M.; Clump, D.A.; Heron, D.E.; Ohr, J.P.; Kim, S.; Duvvuri, U.; Johnson, J.T.; Ferris, R.L. Tumor volume as a predictor of survival in human papillomavirus-positive oropharyngeal cancer. Head Neck 2016, 38, 1613–1617. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Ahn, Y.C.; Oh, D.; Nam, H.; Kim, Y.I.; Park, S.Y. Tumor volume reduction rate measured during adaptive definitive radiation therapy as a potential prognosticator of locoregional control in patients with oropharyngeal cancer. Head Neck 2014, 36, 499–504. [Google Scholar] [CrossRef]
- Panje, C.; Riesterer, O.; Glanzmann, C.; Studer, G. Neutrophil-lymphocyte ratio complements volumetric staging as prognostic factor in patients treated with definitive radiotherapy for oropharyngeal cancer. BMC Cancer 2017, 17, 643. [Google Scholar] [CrossRef] [Green Version]
- Romesser, P.B.; Lim, R.; Spratt, D.E.; Setton, J.; Riaz, N.; Lok, B.; Rao, S.; Sherman, E.J.; Schöder, H.; Lee, N.Y. The relative prognostic utility of standardized uptake value, gross tumor volume, and metabolic tumor volume in oropharyngeal cancer patients treated with platinum based concurrent chemoradiation with a pre-treatment [(18)F] fluorodeoxyglucose positron emission tomography scan. Oral. Oncol. 2014, 50, 802–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, G.H.; Hamberger, A.D. Causes of failure in irradiation of squamous-cell carcinoma of the supraglottic larynx. Radiology 1974, 111, 697–700. [Google Scholar] [CrossRef] [PubMed]
- Mukherji, S.K.; Schmalfuss, I.M.; Castelijns, J.; Mancuso, A.A. Clinical applications of tumor volume measurements for predicting outcome in patients with squamous cell carcinoma of the upper aerodigestive tract. AJNR Am. J. Neuroradiol. 2004, 25, 1425–1432. [Google Scholar] [PubMed]
- Pameijer, F.A.; Balm, A.J.; Hilgers, F.J.; Muller, S.H. Variability of tumor volumes in T3-staged head and neck tumors. Head Neck 1997, 19, 6–13. [Google Scholar] [CrossRef]
- Costantino, A.; De Virgilio, A.; Spriano, G. Is the current oropharyngeal cancer T classification adequate in the era of HPV and transoral robotic surgery? Oral. Oncol. 2021, 118, 105359. [Google Scholar] [CrossRef]
- Hoebers, F.J.; Pameijer, F.A.; de Bois, J.; Heemsbergen, W.; Balm, A.J.; Schornagel, J.H.; Rasch, C.R. Prognostic value of primary tumor volume after concurrent chemoradiation with daily low-dose cisplatin for advanced-stage head and neck carcinoma. Head Neck 2008, 30, 1216–1223. [Google Scholar] [CrossRef]
- Plataniotis, G.A.; Theofanopoulou, M.E.; Kalogera-Fountzila, A.; Haritanti, A.; Ciuleanou, E.; Ghilezan, N.; Zamboglou, N.; Dimitriadis, A.; Sofroniadis, I.; Fountzilas, G. Prognostic impact of tumor volumetry in patients with locally advanced head-and-neck carcinoma (non-nasopharyngeal) treated by radiotherapy alone or combined radiochemotherapy in a randomized trial. Int. J. Radiat. Oncol. Biol.Phys. 2004, 59, 1018–1026. [Google Scholar] [CrossRef]
- Studer, G.; Glanzmann, C. Volumetric staging in oropharyngeal cancer patients treated with definitive IMRT. Oral. Oncol. 2013, 49, 269–276. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | No. (Male) | Age (Range) | No. p16+ | FU (m) (Range) | Stage | T Site | Tx | Mean pTV (cm3) (Range) | Mean nTV (cm3) (Range) | Mean tTV (cm3) (Range) | Cut-Off Type | Cut-Off pTV (cm3) | Cut-Off nTV (cm3) | Cut-Off tTV (cm3) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [29] CF | RCT | 160 (121) | 58 (35–86) | 69 | 60 (N/A) | N/A | N/A | RT (n = 160) | 23.7 (20.2–27.17) | N/A | N/A | N/A | 23 | N/A | N/A |
| [29] AF | RCT | 164 (118) | 59 (32–80) | 74 | 60 (N/A) | N/A | N/A | RT (n = 164) | 25.3 (21.3–29.28) | N/A | N/A | N/A | 23 | N/A | N/A |
| [30] p16+ | R | 72 (58) | 61 (41.4–84.7) | 72 | 31 (N/A) | I (n = 39) II (n = 15) III (n = 18) IV (n = 0) | N/A | N/A | 23 (16.3–29.7) | 26 (18.1–33.88) | N/A | Mean | 23 | 26 | N/A |
| [30] p16− | R | 19 (14) | 66 (54.9–81.7) | 0 | 31 (N/A) | I (n = 2) II (n = 7) III (n = 0) IV (n = 10) | N/A | N/A | 38 (17.4–58.62) | 13 (0–28.38) | N/A | Mean | 38 | 13 | N/A |
| [17] | R | 31 (N/A) | N/A | N/A | 33 | N/A | N/A | RT (n = 14) CRT (n = 17) | 30.5 (22.7–38.3) | 23.2 (16–30.4) | N/A | N/A | N/A | N/A | N/A |
| [31] | R | 42 (29) | 59.6 (28–85) | N/A | 33.3 (4–105) | I (n = 2) II (n = 6) III (n = 8) IV (n = 26) | BOT (n = 13) SP (n = 3) TF (n = 26) PPW (n = 0) | CRT (n = 6) PS (n = 3) PS+(C)RT (n = 33) | N/A | N/A | N/A | Log-rank test | 3.5 | N/A | N/A |
| [32] | R | 53 (50) | 55.4 (39–81) | 53 | 29 (4–76) | N/A | N/A | RT (n = 1) CRT (n = 52) | 18.8 (13.1–24.46) | 26.75 (16.5–37.01) | 44.49 (32.37–56.61) | N/A | N/A | N/A | N/A |
| [33] | R | 59 (48) | 60 (43–86) | N/A | 41.3 (9.3–73.5) | I (n = 2) II (n = 7) III (n = 12) IV (n = 38) | BOT (n = 12) SP (n = 0) TF (n = 44) PPW (n = 3) | RT (n = 9) CRT (n = 50) | 13.79 (1.1–50.81) | 16.75 (0–140.07) | 30.54 (1.1–148.9) | Log-rank test | 15 | 25 | 35 |
| [18] | R | 340 (293) | N/A | N/A | 34 (5–67) | I (n = 3) II (n = 12) III (n = 62) IV (n = 263) | BOT (n = 162) SP (n = 4) TF (n = 166) PPW (n = 8) | RT (n = 17) CRT (n = 323) SS (n = 44) | 42.53 (4.1–306.6) * | 19.04 (0–442.05) * | N/A | Median | 32.79 | 19.04 | N/A |
| [8] | P | 190 (N/A) | N/A | N/A | 42 (2–241) | N/A | BOT (n = 72) SP (n = 12) TF (n = 106) PPW (n = 0) | CRT (n = 190) | BOT: 24.4 (1.5–235) | N/A | N/A | Median | BOT: 14.75 | N/A | N/A |
| SP: 11.8 (0–99.9) | SP: 5.2 | ||||||||||||||
| TF: 18.2 (0–187.5) | TF: 9.2 | ||||||||||||||
| [34] | P | 187 (134) | 61.6 (36.9–91.4) | N/A | 61.2 (1.7–169) | I (n = 0) II (n = 15) III (n = 35) IV (n = 129) Rec (n = 3) | BOT (n = 84) SP (n = 4) TF (n = 97) PPW (n = 2) | RT (n = 7) CRT (n = 180) | N/A | N/A | 40 (3–216) * | N/A | N/A | N/A | 15/70/130 |
| [35] | R | 100 (86) | 56 (27–81) | N/A | 49 (N/A) | N/A | BOT (n = 53) SP (n = 3) TF (n = 42) PPW (n = 2) | CRT (n = 100) | 40.7 (N/A) * | N/A | N/A | Median | 40.7 | N/A | N/A |
| Study | Multicenter | Aim | Inclusion/Exclusion Criteria | Outcome | Prospective | Consecutive | Main Findings | Stratified |
|---|---|---|---|---|---|---|---|---|
| [30] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [17] | No | Yes | No | Yes | No | Yes | Yes | Yes |
| [31] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [32] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [33] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [18] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [8] | No | Yes | No | Yes | Yes | Yes | Yes | Yes |
| [34] | No | Yes | No | Yes | Yes | Yes | Yes | Yes |
| [35] | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, E.; Accorona, R.; Iocca, O.; Costantino, A.; Malvezzi, L.; Ferreli, F.; Franzese, C.; Scorsetti, M.; Capaccio, P.; Mercante, G.; et al. Does Tumor Volume Have a Prognostic Role in Oropharyngeal Squamous Cell Carcinoma? A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2465. https://doi.org/10.3390/cancers14102465
Russo E, Accorona R, Iocca O, Costantino A, Malvezzi L, Ferreli F, Franzese C, Scorsetti M, Capaccio P, Mercante G, et al. Does Tumor Volume Have a Prognostic Role in Oropharyngeal Squamous Cell Carcinoma? A Systematic Review and Meta-Analysis. Cancers. 2022; 14(10):2465. https://doi.org/10.3390/cancers14102465
Chicago/Turabian StyleRusso, Elena, Remo Accorona, Oreste Iocca, Andrea Costantino, Luca Malvezzi, Fabio Ferreli, Ciro Franzese, Marta Scorsetti, Pasquale Capaccio, Giuseppe Mercante, and et al. 2022. "Does Tumor Volume Have a Prognostic Role in Oropharyngeal Squamous Cell Carcinoma? A Systematic Review and Meta-Analysis" Cancers 14, no. 10: 2465. https://doi.org/10.3390/cancers14102465