
Impact of Individual Comorbidities on Survival of Patients with Myelofibrosis

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
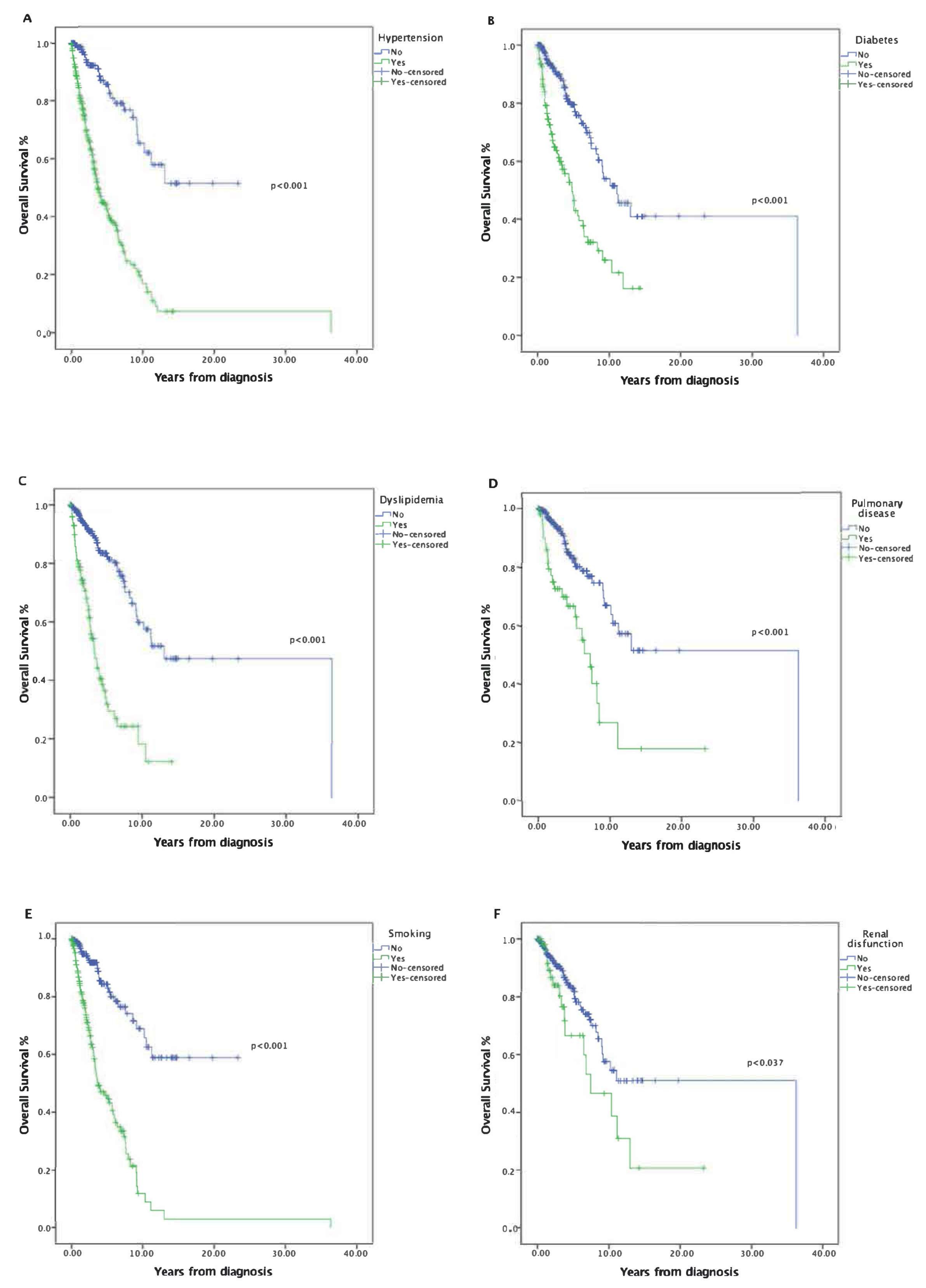
3.2. Impact of Risk Factors on Survival
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
| Comorbidity | Definition |
|---|---|
| Hypertension | Prior medical diagnosis of hypertension. |
| Diabetes | Diabetes Mellitus requiring treatment with insulin or hypoglycemic agents at the time of initiation of conditioning or HbA1c > 7%. |
| Dyslipidemia | Prior medical diagnosis of dyslipidemia. |
| Cardiovascular | Coronary artery disease, congestive heart failure, history of myocardial infarction, or left ventricular ejection fraction ≤ 50%., or prior diagnosis of cerebrovascular disease (diagnostic imaging tests is required). |
| Pulmonary | DLCo1 or FEV1 < 80%. Restrictive Lung Disease or Chronic obstructive pulmonary disease with dyspnea. |
| Renal | eGFRc < 60 mL/min. |
| Hepatic | Serum bilirubin ≥ 1.5 times ULN; ALT or AST ≥ 2.5 times ULN, or chronic hepatitis. |
| HIV | Prior medical diagnosis of HIV by using serological and molecular test. |
| HBV | Prior medical diagnosis of active HBV infection by using serological and molecular test. |
| HCV | Prior medical diagnosis of active HCV infection by using serological and molecular test. |
| Other neoplasm | Malignancy unrelated to the Myelofibrosis which has been treated at any point in the patient’s history, excluding non-melanoma skin cancer |
| Smoking | Someone who has smoked greater than 100 cigarettes (including hand rolled cigarettes, cigars, cigarillos etc) in their lifetime and has smoked in the last 180 days. |
References
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 Revision to the World Health Organization Classification of Myeloid Neoplasms and Acute Leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Barosi, G.; Mesa, R.A.; Thiele, J.; Cervantes, F.; Campbell, P.J.; Verstovsek, S.; Dupriez, B.; Levine, R.L.; Passamonti, F.; Gotlib, J.; et al. Proposed Criteria for the Diagnosis of Post-Polycythemia Vera and Post-Essential Thrombocythemia Myelofibrosis: A Consensus Statement from the International Working Group for Myelofibrosis Research and Treatment. Leukemia 2008, 22, 437–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerquozzi, S.; Tefferi, A. Blast Transformation and Fibrotic Progression in Polycythemia Vera and Essential Thrombocythemia: A Literature Review of Incidence and Risk Factors. Blood Cancer J. 2015, 5, e366. [Google Scholar] [CrossRef] [Green Version]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. (Eds.) WHO Classification of Tumours of the Haematopoietic and Lymphoid Tissues, 4th ed.; IARC: Lyon, France, 2016; ISBN -13 9789283244943. [Google Scholar]
- Moulard, O.; Mehta, J.; Fryzek, J.; Olivares, R.; Iqbal, U.; Mesa, R.A. Epidemiology of Myelofibrosis, Essential Thrombocythemia, and Polycythemia Vera in the European Union. Eur. J. Haematol. 2014, 92, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Srour, S.A.; Devesa, S.S.; Morton, L.M.; Check, D.P.; Curtis, R.E.; Linet, M.S.; Dores, G.M. Incidence and Patient Survival of Myeloproliferative Neoplasms and Myelodysplastic/Myeloproliferative Neoplasms in the United States, 2001–2012. Br. J. Haematol. 2016, 174, 382–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tefferi, A.; Lasho, T.L.; Finke, C.M.; Knudson, R.A.; Ketterling, R.; Hanson, C.H.; Maffioli, M.; Caramazza, D.; Passamonti, F.; Pardanani, A. CALR vs JAK2 vs MPL-Mutated or Triple-Negative Myelofibrosis: Clinical, Cytogenetic and Molecular Comparisons. Leukemia 2014, 28, 1472–1477. [Google Scholar] [CrossRef]
- Vannucchi, A.M.; Lasho, T.L.; Guglielmelli, P.; Biamonte, F.; Pardanani, A.; Pereira, A.; Finke, C.; Score, J.; Gangat, N.; Mannarelli, C.; et al. Mutations and Prognosis in Primary Myelofibrosis. Leukemia 2013, 27, 1861–1869. [Google Scholar] [CrossRef]
- Klampfl, T.; Gisslinger, H.; Harutyunyan, A.S.; Nivarthi, H.; Rumi, E.; Milosevic, J.D.; Them, N.C.C.; Berg, T.; Gisslinger, B.; Pietra, D.; et al. Somatic Mutations of Calreticulin in Myeloproliferative Neoplasms. N. Engl. J. Med. 2013, 369, 2379–2390. [Google Scholar] [CrossRef] [Green Version]
- Tefferi, A. Pathogenesis of Myelofibrosis with Myeloid Metaplasia. J. Clin. Oncol. 2005, 23, 8520–8530. [Google Scholar] [CrossRef]
- Tefferi, A. Primary Myelofibrosis: 2017 Update on Diagnosis, Risk-Stratification, and Management. Am. J. Hematol. 2016, 91, 1262–1271. [Google Scholar] [CrossRef]
- Harrison, C.N.; McLornan, D.P. Current Treatment Algorithm for the Management of Patients with Myelofibrosis, JAK Inhibitors, and Beyond. Hematology 2017, 2017, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kröger, N.M.; Deeg, J.H.; Olavarria, E.; Niederwieser, D.; Bacigalupo, A.; Barbui, T.; Rambaldi, A.; Mesa, R.; Tefferi, A.; Griesshammer, M.; et al. Indication and Management of Allogeneic Stem Cell Transplantation in Primary Myelofibrosis: A Consensus Process by an EBMT/ELN International Working Group. Leukemia 2015, 29, 2126–2133. [Google Scholar] [CrossRef] [PubMed]
- Kröger, N.; Giorgino, T.; Scott, B.L.; Ditschkowski, M.; Alchalby, H.; Cervantes, F.; Vannucchi, A.; Cazzola, M.; Morra, E.; Zabelina, T.; et al. Impact of Allogeneic Stem Cell Transplantation on Survival of Patients Less than 65 Years of Age with Primary Myelofibrosis. Blood 2015, 125, 3347–3350. [Google Scholar] [CrossRef] [Green Version]
- Cervantes, F.; Dupriez, B.; Pereira, A.; Passamonti, F.; Reilly, J.T.; Morra, E.; Vannucchi, A.M.; Mesa, R.A.; Demory, J.L.; Barosi, G.; et al. New Prognostic Scoring System for Primary Myelofibrosis Based on a Study of the International Working Group for Myelofibrosis Research and Treatment. Blood 2009, 113, 2895–2901. [Google Scholar] [CrossRef] [PubMed]
- Passamonti, F.; Cervantes, F.; Vannucchi, A.M.; Morra, E.; Rumi, E.; Pereira, A.; Guglielmelli, P.; Pungolino, E.; Caramella, M.; Maffioli, M.; et al. A Dynamic Prognostic Model to Predict Survival in Primary Myelofibrosis: A Study by the IWG-MRT (International Working Group for Myeloproliferative Neoplasms Research and Treatment). Blood 2010, 115, 1703–1708. [Google Scholar] [CrossRef] [PubMed]
- Gangat, N.; Caramazza, D.; Vaidya, R.; George, G.; Begna, K.; Schwager, S.; Van Dyke, D.; Hanson, C.; Wu, W.; Pardanani, A.; et al. DIPSS plus: A Refined Dynamic International Prognostic Scoring System for Primary Myelofibrosis That Incorporates Prognostic Information From Karyotype, Platelet Count, and Transfusion Status. J. Clin. Oncol. 2011, 29, 392–397. [Google Scholar] [CrossRef]
- Vannucchi, A.M.; Guglielmelli, P.; Rotunno, G.; Pascutto, C.; Pardanani, A.; Ferretti, V.; Pacilli, A.; Pancrazzi, A.; Lasho, T.; Hanson, C.A.; et al. Mutation-Enhanced International Prognostic Scoring System (MIPSS) for Primary Myelofibrosis: An AGIMM & IWG-MRT Project. Blood 2014, 124, 405. [Google Scholar] [CrossRef]
- Guglielmelli, P.; Lasho, T.L.; Rotunno, G.; Mudireddy, M.; Mannarelli, C.; Nicolosi, M.; Pacilli, A.; Pardanani, A.; Rumi, E.; Rosti, V.; et al. MIPSS70: Mutation-enhanced international prognostic score system for transplantation-age patients with primary myelofibrosis. J. Clin. Oncol. 2018, 36, 310–318. [Google Scholar] [CrossRef]
- Tefferi, A.; Guglielmelli, P.; Lasho, T.L.; Gangat, N.; Ketterling, R.P.; Pardanani, A.; Vannucchi, A.M. MIPSS70+ version 2.0: Mutation and karyotype-enhanced international prognostic scoring system for primary myelofibrosis. J. Clin. Oncol. 2018, 36, 1769–1770. [Google Scholar] [CrossRef]
- Tefferi, A.; Guglielmelli, P.; Nicolosi, M.; Mannelli, F.; Mudireddy, M.; Bartalucci, N.; Finke, C.M.; Lasho, T.L.; Hanson, C.A.; Ketterling, R.P.; et al. GIPSS: Genetically Inspired Prognostic Scoring System for Primary Myelofibrosis. Leukemia 2018, 32, 1631–1642. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Boluda, J.C.; Pereira, A.; Correa, J.G.; Alvarez-Larrán, A.; Ferrer-Marín, F.; Raya, J.M.; Martínez-López, J.; Pérez-Encinas, M.; Estrada, N.; Velez, P.; et al. Performance of the Myelofibrosis Secondary to PV and ET-Prognostic Model (MYSEC-PM) in a Series of 262 Patients from the Spanish Registry of Myelofibrosis. Leukemia 2018, 32, 553–555. [Google Scholar] [CrossRef] [PubMed]
- Grinfeld, J.; Nangalia, J.; Baxter, E.J.; Wedge, D.C.; Angelopoulos, N.; Cantrill, R.; Godfrey, A.L.; Papaemmanuil, E.; Gundem, G.; MacLean, C.; et al. Classification and Personalized Prognosis in Myeloproliferative Neoplasms. N. Engl. J. Med. 2018, 379, 1416–1430. [Google Scholar] [CrossRef] [PubMed]
- Rumi, E.; Cazzola, M. Diagnosis, Risk Stratification, and Response Evaluation in Classical Myeloproliferative Neoplasms. Blood 2017, 129, 680–692. [Google Scholar] [CrossRef] [PubMed]
- Saußele, S.; Krauß, M.P.; Hehlmann, R.; Lauseker, M.; Proetel, U.; Kalmanti, L.; Hanfstein, B.; Fabarius, A.; Kraemer, D.; Berdel, W.E.; et al. Impact of Comorbidities on Overall Survival in Patients with Chronic Myeloid Leukemia: Results of the Randomized CML Study IV. Blood 2015, 126, 42–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, M.J.; Churnetski, M.; Alqahtani, H.; Rivera, X.; Kittai, A.; Amrock, S.M.; James, S.; Hoff, S.; Manda, S.; Spurgeon, S.E.; et al. Comorbidities Predict Inferior Outcomes in Chronic Lymphocytic Leukemia Treated with Ibrutinib. Cancer 2018, 124, 3192–3200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naqvi, K.; Garcia-Manero, G.; Sardesai, S.; Oh, J.; Vigil, C.E.; Pierce, S.; Lei, X.; Shan, J.; Kantarjian, H.M.; Suarez-Almazor, M.E. Association of Comorbidities with Overall Survival in Myelodysplastic Syndrome: Development of a Prognostic Model. J. Clin. Oncol. 2011, 29, 2240–2246. [Google Scholar] [CrossRef] [Green Version]
- Storey, S.; Gray, T.F.; Bryant, A.L. Comorbidity, Physical Function, and Quality of Life in Older Adults with Acute Myeloid Leukemia. Curr. Geriatr. Reports 2017, 6, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Khalil, M.M.I.; Lipton, J.H.; Atenafu, E.G.; Gupta, V.; Kim, D.D.; Kuruvilla, J.; Viswabandya, A.; Messner, H.A.; Michelis, F.V. Impact of Comorbidities Constituting the Hematopoietic Cell Transplant (HCT)-Comorbidity Index on the Outcome of Patients Undergoing Allogeneic HCT for Acute Myeloid Leukemia. Eur. J. Haematol 2018, 100, 198–205. [Google Scholar] [CrossRef]
- Sarfati, D.; Koczwara, B.; Jackson, C. The Impact of Comorbidity on Cancer and Its Treatment. CA Cancer J. Clin 2016, 66, 337–350. [Google Scholar] [CrossRef]
- Kallogjeri, D.; Piccirillo, J.F.; Spitznagel, E.L.; Steyerberg, E.W. Comparison of Scoring Methods for ACE-27: Simpler Is Better. J. Geriatr. Oncol. 2012, 3, 238–245. [Google Scholar] [CrossRef] [Green Version]
- Bartoszko, J.; Panzarella, T.; McNamara, C.J.; Lau, A.; Schimmer, A.D.; Schuh, A.C.; Sibai, H.; Maze, D.; Yee, K.W.L.; Devlin, R.; et al. Distribution and Impact of Comorbidities on Survival and Leukemic Transformation in Myeloproliferative Neoplasm-Associated Myelofibrosis: A Retrospective Cohort Study. Clin. Lymphoma Myeloma Leuk. 2017, 17, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Newberry, K.J.; Naqvi, K.; Nguyen, K.T.; Cardenas-Turanzas, M.; Florencia Tanaka, M.; Pierce, S.; Verstovsek, S. Comorbidities Predict Worse Prognosis in Patients with Primary Myelofibrosis. Cancer 2014, 120, 2996–3002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lekovic, D.; Gotic, M.; Perunicic-Jovanovic, M.; Vidovic, A.; Bogdanovic, A.; Jankovic, G.; Cokic, V.; Milic, N. Contribution of Comorbidities and Grade of Bone Marrow Fibrosis to the Prognosis of Survival in Patients with Primary Myelofibrosis. Med. Oncol. 2014, 31, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, R.M.; Dueck, A.C.; Geyer, H.L.; Kiladjian, J.J.; Slot, S.; Zweegman, S.; te Boekhorst, P.A.W.; Commandeur, S.; Schouten, H.C.; Sackmann, F.; et al. Myeloproliferative Neoplasm (MPN) Symptom Assessment Form Total Symptom Score: Prospective International Assessment of an Abbreviated Symptom Burden Scoring System among Patients with MPNs. J. Clin. Oncol. 2012, 30, 4098–4103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorror, M.L.; Storer, B.; Storb, R.F. Validation of the Hematopoietic Cell Transplantation-Specific Comorbidity Index (HCT-CI) in Single and Multiple Institutions: Limitations and Inferences. Biol. Blood Marrow Transplant. 2009, 15, 757–758. [Google Scholar] [CrossRef] [Green Version]
- Breccia, M.; Bartoletti, D.; Bonifacio, M.; Palumbo, G.A.; Polverelli, N.; Abruzzese, E.; Bergamaschi, M.; Tieghi, A.; Tiribelli, M.; Iurlo, A.; et al. Impact of Comorbidities and Body Mass Index in Patients with Myelofibrosis Treated with Ruxolitinib. Ann. Hematol. 2019, 98, 889–896. [Google Scholar] [CrossRef]
- Song, H.T.; Cui, Y.; Zhang, L.L.; Cao, G.; Li, L.; Li, G.; Jia, X.J. Ruxolitinib Attenuates Intimal Hyperplasia via Inhibiting JAK2/STAT3 Signaling Pathway Activation Induced by PDGF-BB in Vascular Smooth Muscle Cells. Microvasc. Res. 2020, 132, 104060. [Google Scholar] [CrossRef]
- Hasselbalch, H.C. Perspectives on the Impact of JAK-Inhibitor Therapy upon Inflammation-Mediated Comorbidities in Myelofibrosis and Related Neoplasms. Expert Rev. Hematol. 2014, 7, 203–216. [Google Scholar] [CrossRef]
- Bjørn, M.E.; Hasselbalch, H.C. The Impact of Ruxolitinib Treatment on Inflammation-Mediated Comorbidities in Myelofibrosis and Related Neoplasms. Clin. Case Rep. 2015, 3, 499–503. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, S.H.; Kang, S.H.; Cho, J.H.; Cho, Y.; Oh, I.Y.; Yoon, C.H.; Lee, H.Y.; Youn, T.J.; Chae, I.H.; et al. Blood Pressure Control and Cardiovascular Outcomes: Real-World Implications of the 2017 ACC/AHA Hypertension Guideline. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Laiteerapong, N.; Ham, S.A.; Gao, Y.; Moffet, H.H.; Liu, J.Y.; Huang, E.S.; Karter, A.J. The Legacy Effect in Type 2 Diabetes:Impactofearlyglycemic Control on Future Complications (the Diabetes & Aging Study). Diabetes Care 2019, 42, 416–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storey, B.C.; Staplin, N.; Haynes, R.; Reith, C.; Emberson, J.; Herrington, W.G.; Wheeler, D.C.; Walker, R.; Fellström, B.; Wanner, C.; et al. Lowering LDL Cholesterol Reduces Cardiovascular Risk Independently of Presence of Inflammation. Kidney Int. 2018, 93, 1000–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haybar, H.; Khodadi, E.; Shahjahani, M.; Saki, N. Cardiovascular Events: A Challenge in JAK2-Positive Myeloproliferative Neoplasms. Cardiovasc. Hematol. Disord. Targets 2018, 17, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, H.; Szépligeti, S.; Bak, M.; Ghanima, W.; Hasselbalch, H.C.; Christiansen, C.F. Vascular Diseases in Patients with Chronic Myeloproliferative Neoplasms—Impact of Comorbidity. Clin. Epidemiol. 2019, 11, 955–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golia, E.; Limongelli, G.; Natale, F.; Fimiani, F.; Maddaloni, V.; Pariggiano, I.; Bianchi, R.; Crisci, M.; D’Acierno, L.; Giordano, R.; et al. Inflammation and Cardiovascular Disease: From Pathogenesis to Therapeutic Target. Curr. Atheroscler. Rep. 2014, 16. [Google Scholar] [CrossRef] [PubMed]

| Variable | All Patients n = 668 |
|---|---|
| Median age, years | 68 (25–89) |
| Female, n (%) | 244 (36.5) |
| Hypertension, n (%) | 282 (42.2) |
| Diabetes, n (%) | 124 (18.6) |
| Dyslipidemia, n (%) | 117 (16.0) |
| Cardiovascular disease, n (%) | 105 (15.7) |
| Pulmonary disease, n (%) | 55 (8.2) |
| Renal dysfunction, n (%) | 58 (8.7) |
| Hepatic disease, n (%) | 41 (6.2) |
| HIV, n (%) | 0 (0) |
| HBV, n (%) | 20 (3) |
| HCV, n (%) | 10 (1.5) |
| Other neoplasm, n (%) | 55 (8.2) |
| Smoking, n (%) | 161 (24.1) |
| PMF, n (%) | 411 (61.5) |
| JAK2, n (%) | 375 (56.1) |
| CALR, n (%) | 61 (9.1) |
| Splenomegaly +, n (%) | 371 (55.5) |
| IPSS | |
| Low risk, n (%) | 71 (10.6) |
| Intermediate 1, n (%) | 166 (24.9) |
| Intermediate 2, n (%) | 243 (36.4) |
| High risk, n (%) | 188 (28.1) |
| Variable | HR | 95% CI | p-Value |
|---|---|---|---|
| Age (61.4–76.3 y) * | 2.04 | (1.54–2.69) | <0.001 |
| Age (≥76.3 y) * | 4.43 | (3.23–6.06) | <0.001 |
| Female | 0.76 | (0.61–0.95) | 0.017 |
| Hypertension | 4.96 | (3.26–7.55) | <0.001 |
| Diabetes | 3.01 | (2.07–4.36) | <0.001 |
| Dyslipidemia | 4.65 | (3.11–6.95) | <0.001 |
| Cardiovascular disease | 1.41 | (0.85–2.35) | 0.186 |
| Pulmonary disease | 3.13 | (1.86–5.26) | <0.001 |
| Renal dysfunction | 1.82 | (1.04–3.19) | 0.037 |
| HCV | 4.26 | (1.32–13.75) | 0.015 |
| Other neoplasm | 1.76 | (0.99–3.12) | 0.052 |
| Smoking | 5.08 | (3.35–7.71) | <0.001 |
| PMF vs. PPV-MF or ET-MF | 1.07 | (0.86–1.33) | 0.534 |
| IPSS Intermediate-1 ** | 1.56 | (0.95–2.55) | 0.740 |
| IPSS Intermediate-2 ** | 3.65 | (2.31–5.77) | <0.001 |
| IPSS High Risk ** | 5.10 | (3.20–8.11) | <0.001 |
| JAK2 | 0.83 | (0.65–1.06) | 0.140 |
| CALR | 0.49 | (0.29–0.83) | 0.009 |
| Splenomegaly + | 1.12 | (0.80–1.58) | 0.509 |
| MPN-SAF (9–31.5) *** | 0.98 | (0.19–5.28) | 0.985 |
| MPN-SAF (≥31.5) *** | 0.60 | (0.05–5.82) | 0.600 |
| Ruxolitinib | 0.04 | (0.01–0.12) | <0.001 |
| Variable | Without Ruxolitinib | With Ruxolitinib | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (61.4–76.3 y) * | 2.57 | (1.12–5.61) | 0.026 | 2.91 | (1.24–6.85) | 0.014 |
| Age (≥76.3 y) * | 4.85 | (1.75–13.41) | 0.002 | 4.23 | (1.53–11.73) | 0.006 |
| Hypertension | 0.99 | (0.52–1.92) | 0.992 | 1.13 | (0.59–2.16) | 0.707 |
| Diabetes | 2.20 | (0.98–4.94) | 0.057 | 1.46 | (0.61–3.49) | 0.394 |
| Dyslipidemia | 1.40 | (0.68–2.87) | 0.365 | 1.07 | (0.48–2.36) | 0.872 |
| Renal dysfunction | 2.08 | (1.023–4.21) | 0.043 | 1.69 | (0.81–3.50) | 0.159 |
| Pulmonary disease | 2.69 | (1.47–4.91) | 0.001 | 2.40 | (1.29–4.47) | 0.006 |
| Smoking | 3.34 | (1.85–6.04) | <0.001 | 3.82 | (2.02–7.24) | <0.001 |
| HCV | 11.49 | (2.74–48.25) | 0.001 | 9.86 | (2.34–41.64) | 0.002 |
| IPSS Intermediate-1 ** | 2.53 | (0.73–8.91) | 0.142 | 2.94 | (0.82–10.52) | 0.096 |
| IPSS Intermediate-2 ** | 4.76 | (1.40–16.22) | 0.013 | 6.90 | (1.95–24.37) | 0.003 |
| IPSS High Risk ** | 11.34 | (3.24–39.7) | <0.001 | 15.97 | (4.22–60.42) | <0.001 |
| CALR | 0.97 | (0.28–3.42) | 0.966 | 0.82 | (0.23–2.89) | 0.763 |
| Ruxolitinib | - | - | - | 0.12 | (0.04–0.43) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Fortes, M.; Hernández-Boluda, J.C.; Álvarez-Larrán, A.; Raya, J.M.; Angona, A.; Estrada, N.; Fox, L.; Cuevas, B.; García-Hernández, M.C.; Gómez-Casares, M.T.; et al. Impact of Individual Comorbidities on Survival of Patients with Myelofibrosis. Cancers 2022, 14, 2331. https://doi.org/10.3390/cancers14092331
García-Fortes M, Hernández-Boluda JC, Álvarez-Larrán A, Raya JM, Angona A, Estrada N, Fox L, Cuevas B, García-Hernández MC, Gómez-Casares MT, et al. Impact of Individual Comorbidities on Survival of Patients with Myelofibrosis. Cancers. 2022; 14(9):2331. https://doi.org/10.3390/cancers14092331
Chicago/Turabian StyleGarcía-Fortes, María, Juan C. Hernández-Boluda, Alberto Álvarez-Larrán, José M. Raya, Anna Angona, Natalia Estrada, Laura Fox, Beatriz Cuevas, María C. García-Hernández, María Teresa Gómez-Casares, and et al. 2022. "Impact of Individual Comorbidities on Survival of Patients with Myelofibrosis" Cancers 14, no. 9: 2331. https://doi.org/10.3390/cancers14092331