
Deep-Tissue Activation of Photonanomedicines: An Update and Clinical Perspectives

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Photonanomedicines and Current Clinical Practice
1.1. Photodynamic Therapy and Photonanomedicines
1.2. Current Clinical Irradiation Strategies for PDT
1.2.1. Interstitial PDT
1.2.2. PDT of Disseminated Disease
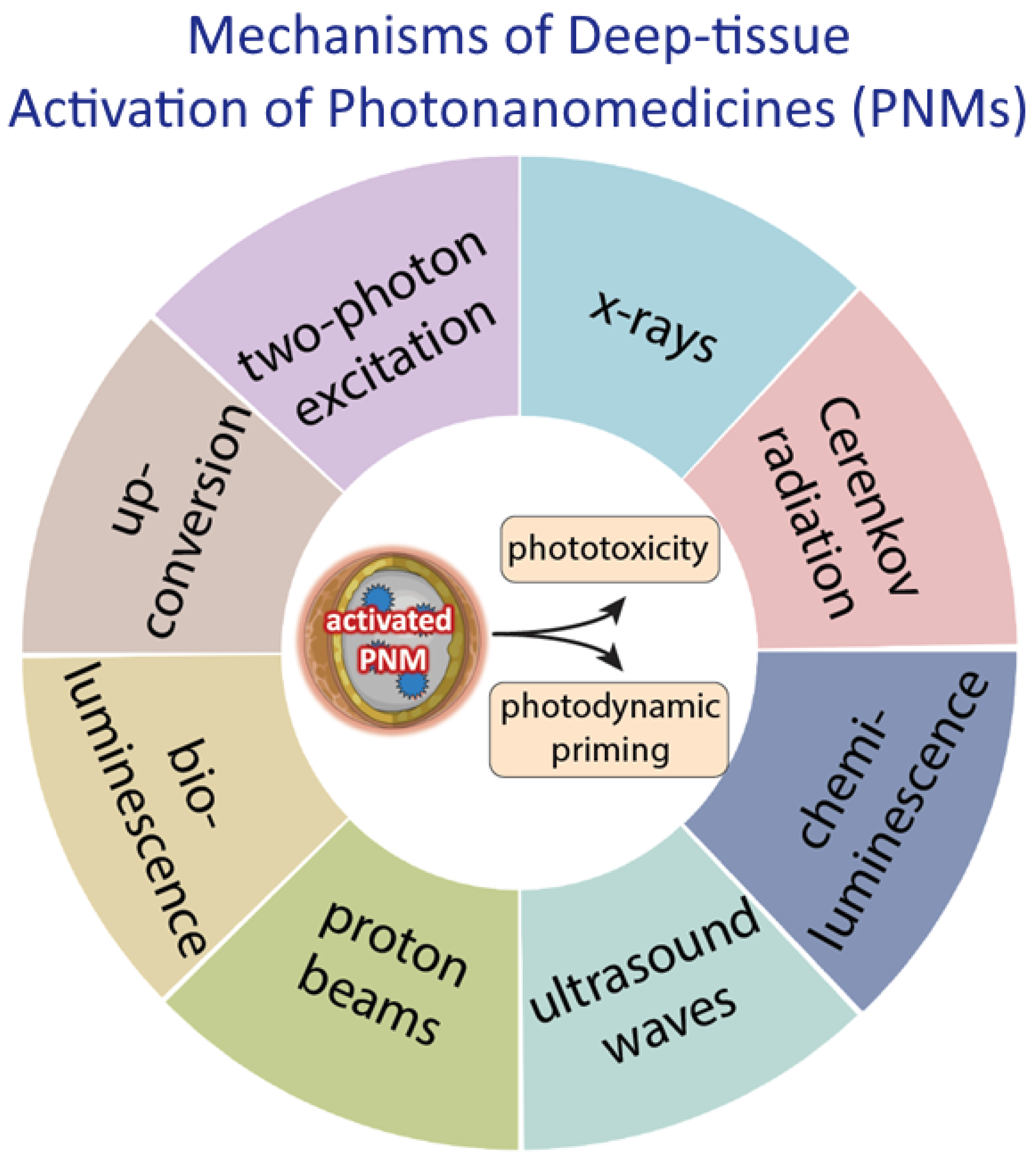
2. State of the Art of Deep-Tissue Activation for PDT
2.1. Two-Photon PDT
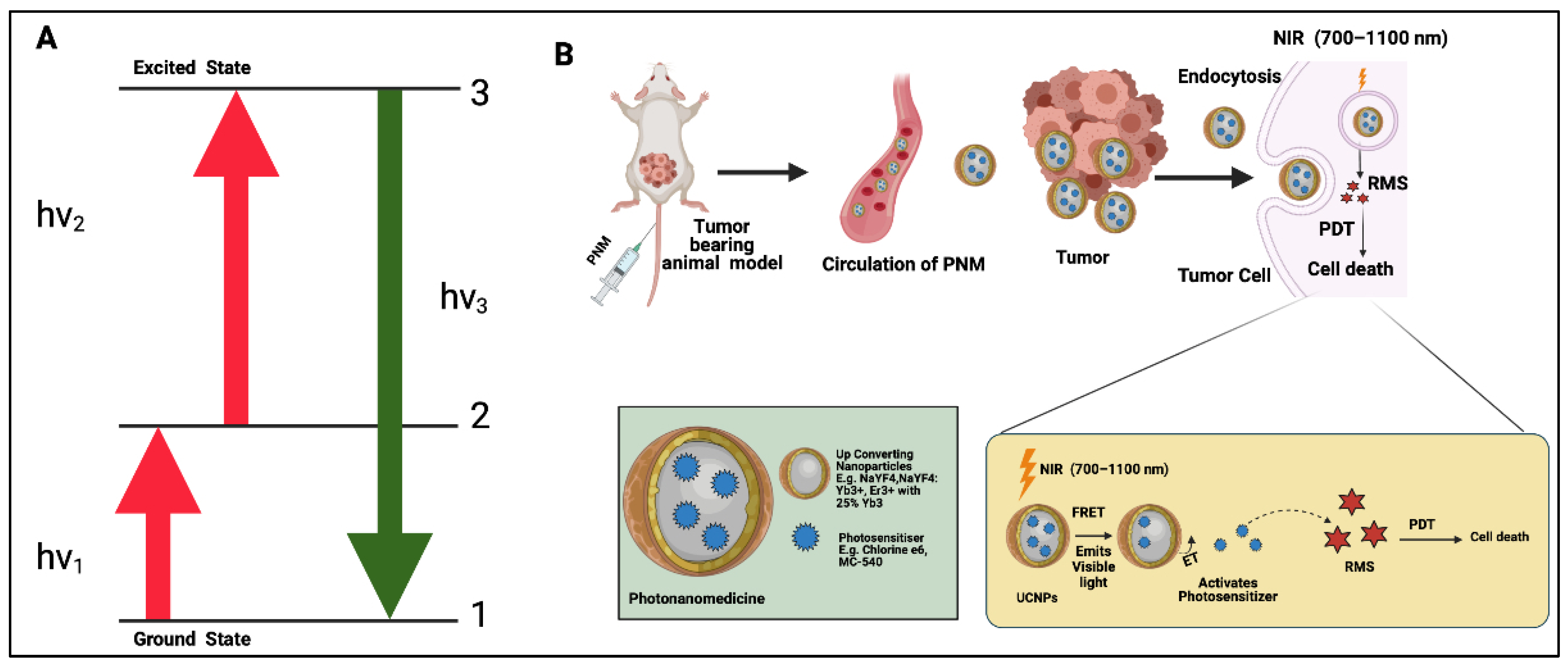
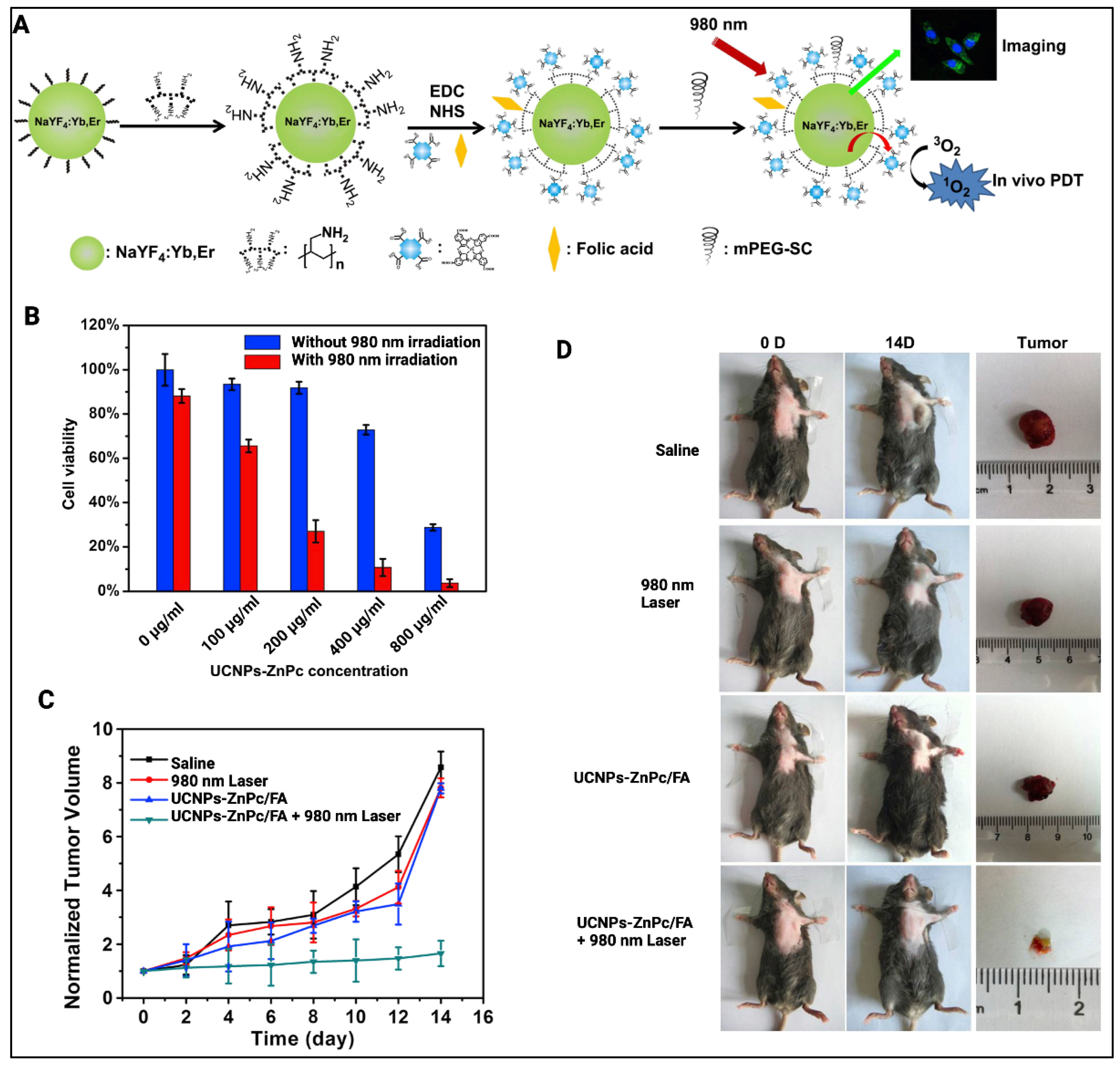
2.2. Upconversion PDT
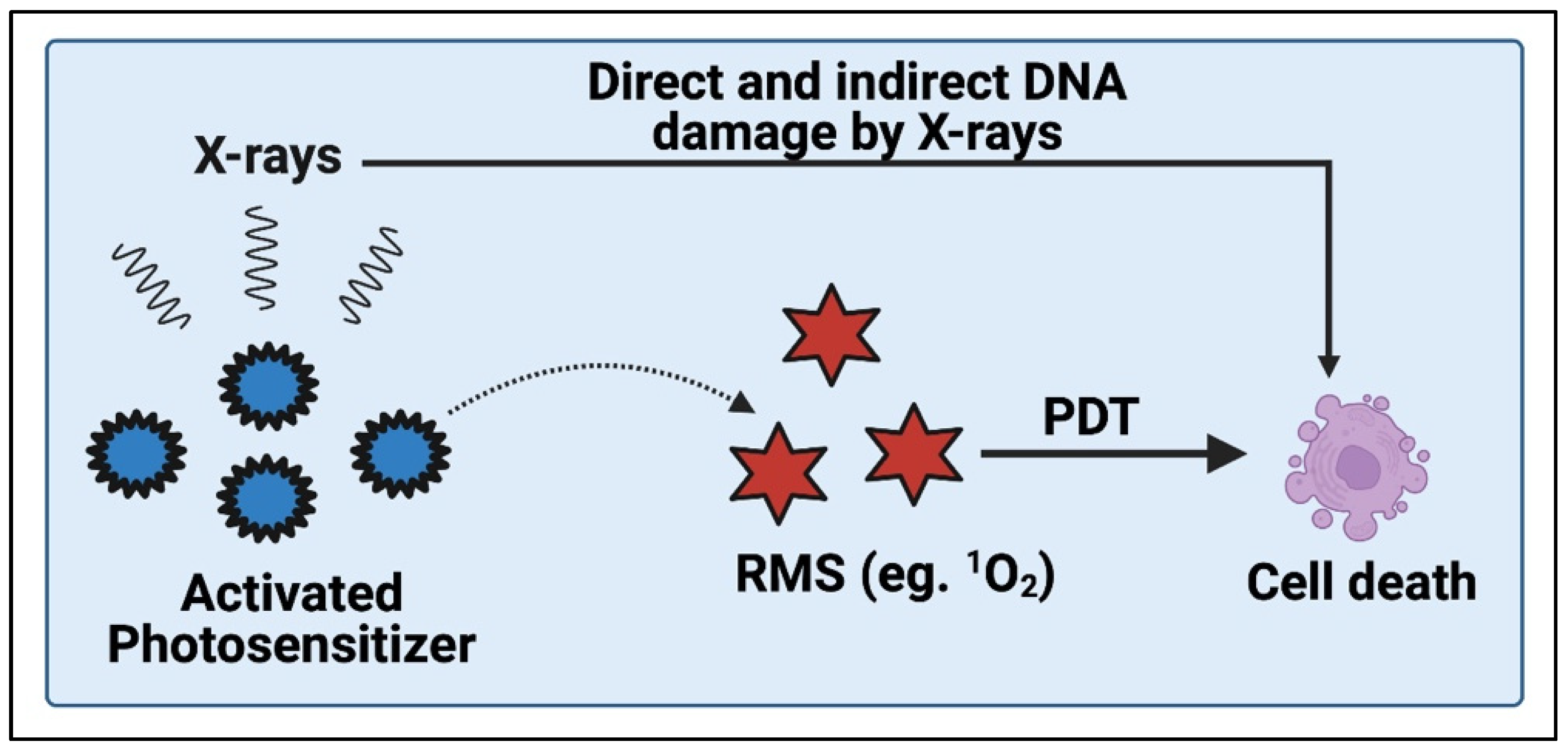
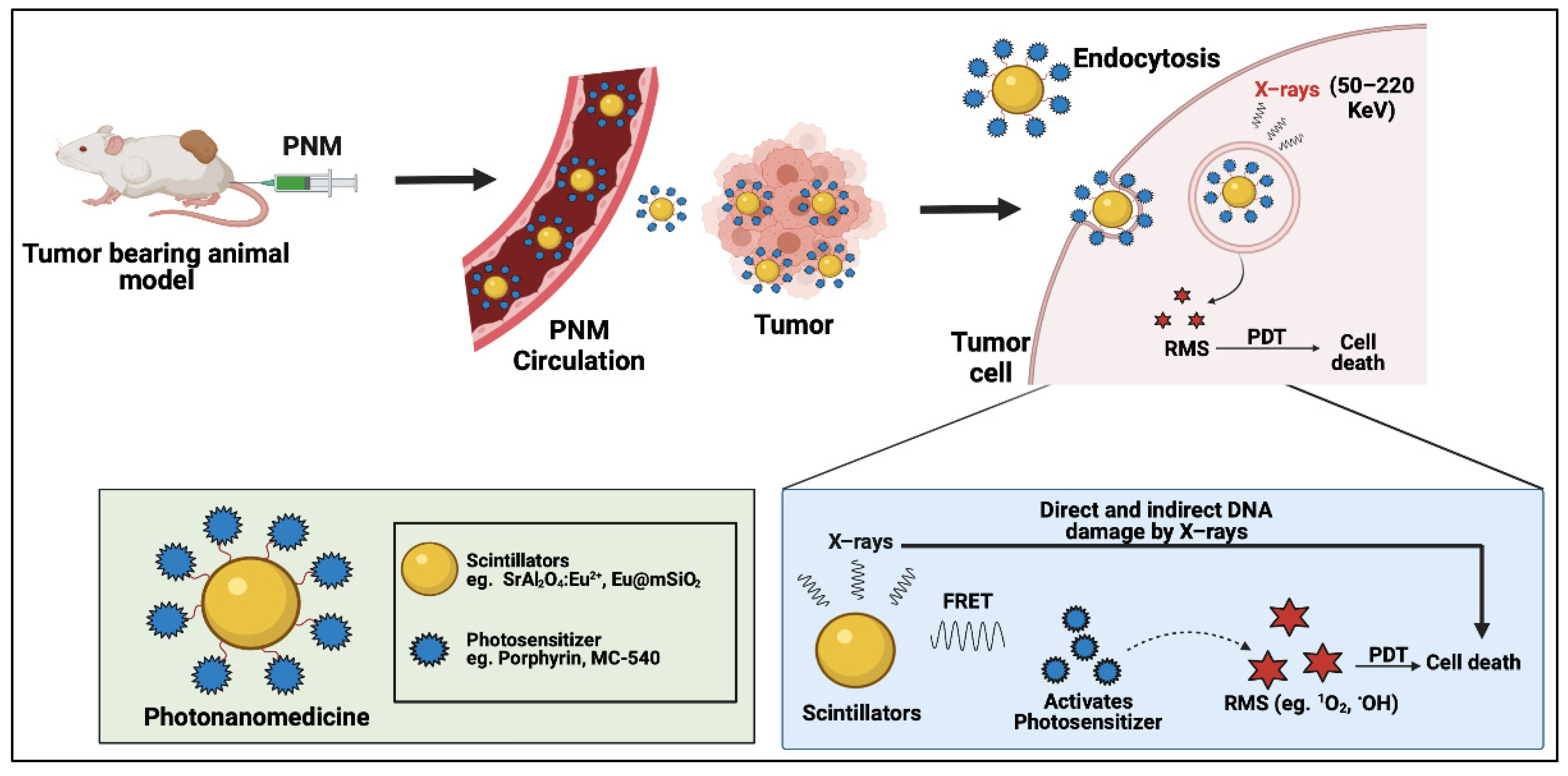
2.3. X-ray PDT
2.4. Cerenkov-Radiation-Induced PDT
2.5. Proton-Dynamic Therapy
2.6. Chemiluminescence and Bioluminescence as FRET Donors for PDT
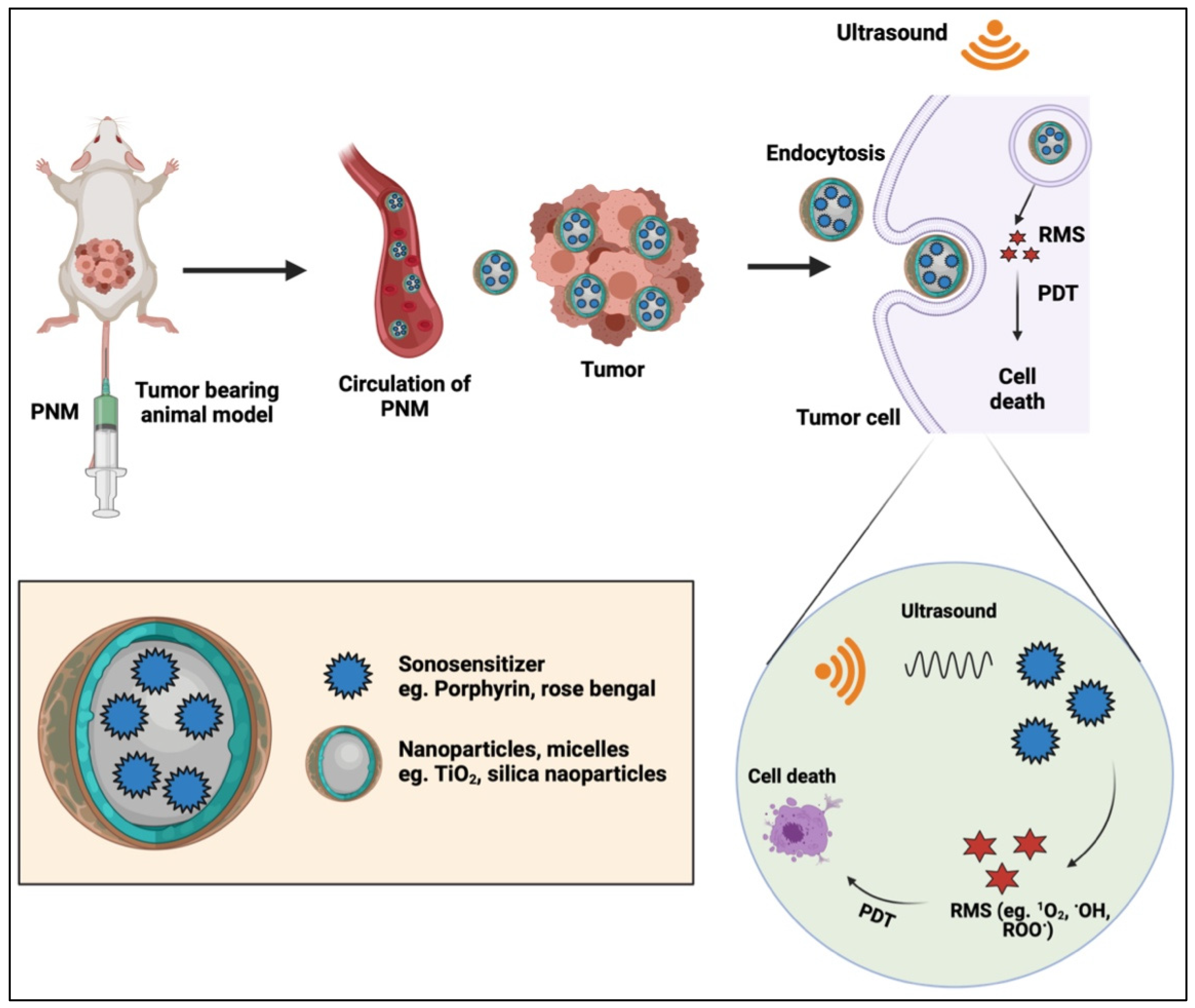
2.7. Sonodynamic Therapy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensitizer | Reactive Molecular Species Detected | Ultrasound Frequency (MHz) | Ultrasound Intensity (W/cm2) | Exposure Time | Reference |
|---|---|---|---|---|---|
| Protoporphyrin IX (using the precursor 5-Aminolevulinic acid) | n.a. | 1.04 | 10 | 5 min | [84] |
| Acridine Orange | 1O2 + •OH | 2 | 2.0 | 60 s | [85] |
| Chlorin e6 | 1O2 + ROO• | 1.56 | 6 | 3 min | [86] |
| C1A1-phthalocyanine | n.a. | 3 | 6.0 | 60 s | [87] |
| DCPH-P-Na(I) | 1O2 | 1 | 0.5 to 2.0 | 10 min | [88] |
| Hematoporphyrin | 1O2 | 1 | 1 | 120 s | [89] |
| Hypocrellin SL052 | n.a. | 1 | 0.4 to 0.8 | 3 min | [90] |
| Indocyanine green | n.a. | 1 | 3.5 | 3 min | [91] |
| Methylene blue | •OH | 2 | 0.24 | 30 s | [92] |
| Photofrin | 1O2 | 1 | 0.5 | 2 min | [93] |
| Phthalocyanine | n.a. | 1 | 2 | 10 min | [94] |
| Protoporphyrin IX (using the precursor 5-Aminolevulinic acid) | 1O2 | 1 | 0.5 | 15 min | [95] |
| Rose bengal | 1O2 | 1 | 1 | 5 min | [96] |
| Rose bengal derivative | 1O2 | 1.92 | 8.3 | 60 s | [97] |
3. Capitalizing on Clinically Available Technologies for Deep-Tissue Activation
4. Perspectives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bhandari, C.; Guirguis, M.; Savan, N.A.; Shrivastava, N.; Oliveira, S.; Hasan, T.; Obaid, G. What NIR Photodynamic Activation Offers Molecular Targeted Nanomedicines: Perspectives into the Conundrum of Tumor Specificity and Selectivity. Nano Today 2021, 36, 101052. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.J.; Lei, Q.; Zhang, X.Z. Recent Advances in Photonanomedicines for Enhanced Cancer Photodynamic Therapy. Prog. Mater. Sci. 2020, 114, 100685. [Google Scholar] [CrossRef]
- Obaid, G.; Broekgaarden, M.; Bulin, A.-L.; Huang, H.-C.; Kuriakose, J.; Liu, J.; Hasan, T. Photonanomedicine: A Convergence of Photodynamic Therapy and Nanotechnology. Nanoscale 2016, 8, 12471–12503. [Google Scholar] [CrossRef] [PubMed]
- Obaid, G.; Jin, W.; Bano, S.; Kessel, D.; Hasan, T. Nanolipid Formulations of Benzoporphyrin Derivative: Exploring the Dependence of Nanoconstruct Photophysics and Photochemistry on Their Therapeutic Index in Ovarian Cancer Cells. Photochem. Photobiol. 2019, 95, 364–377. [Google Scholar] [CrossRef]
- Spring, B.Q.; Sears, R.B.; Zheng, L.Z.; Mai, Z.; Watanabe, R.; Sherwood, M.E.; Schoenfeld, D.A.; Pogue, B.W.; Pereira, S.P.; Villa, E. A Photoactivable Multi-Inhibitor Nanoliposome for Tumour Control and Simultaneous Inhibition of Treatment Escape Pathways. Nat. Nanotechnol. 2016, 11, 378–387. [Google Scholar] [CrossRef]
- Obaid, G.; Bano, S.; Mallidi, S.; Broekgaarden, M.; Kuriakose, J.; Silber, Z.; Bulin, A.-L.; Wang, Y.; Mai, Z.; Jin, W. Impacting Pancreatic Cancer Therapy in Heterotypic In Vitro Organoids and in Vivo Tumors with Specificity-Tuned, NIR-Activable Photoimmunonanoconjugates: Towards Conquering Desmoplasia? Nano Lett. 2019, 19, 7573–7587. [Google Scholar] [CrossRef]
- McFarland, S.A.; Mandel, A.; Dumoulin-White, R.; Gasser, G. Metal-Based Photosensitizers for Photodynamic Therapy: The Future of Multimodal Oncology? Curr. Opin. Chem. Biol. 2020, 56, 23–27. [Google Scholar] [CrossRef]
- Shafirstein, G.; Bellnier, D.; Oakley, E.; Hamilton, S.; Potasek, M.; Beeson, K.; Parilov, E. Interstitial Photodynamic Therapy—A Focused Review. Cancers 2017, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Shafirstein, G.; Bellnier, D.A.; Oakley, E.; Hamilton, S.; Habitzruther, M.; Tworek, L.; Hutson, A.; Spernyak, J.A.; Sexton, S.; Curtin, L.; et al. Irradiance Controls Photodynamic Efficacy and Tissue Heating in Experimental Tumours: Implication for Interstitial PDT of Locally Advanced Cancer. Br. J. Cancer 2018, 119, 1191–1199. [Google Scholar] [CrossRef]
- Photofrin (Porfimer Sodium) for Injection. Available online: https://www.rxlist.com/photofrin-drug.htm#description (accessed on 9 December 2021).
- Huggett, M.T.; Jermyn, M.; Gillams, A.; Illing, R.; Mosse, S.; Novelli, M.; Kent, E.; Bown, S.G.; Hasan, T.; Pogue, B.W. Phase I/II Study of Verteporfin Photodynamic Therapy in Locally Advanced Pancreatic Cancer. Br. J. Cancer 2014, 110, 1698–1704. [Google Scholar] [CrossRef] [Green Version]
- Hanada, Y.; Pereira, S.P.; Pogue, B.; Maytin, E.V.; Hasan, T.; Linn, B.; Mangels-Dick, T.; Wang, K.K. EUS-Guided Verteporfin Photodynamic Therapy for Pancreatic Cancer. Gastrointest. Endosc. 2021, 94, 179–186. [Google Scholar] [CrossRef] [PubMed]
- DeWitt, J.M.; Sandrasegaran, K.; O’Neil, B.; House, M.G.; Zyromski, N.J.; Sehdev, A.; Perkins, S.M.; Flynn, J.; McCranor, L.; Shahda, S. Phase 1 Study of EUS-Guided Photodynamic Therapy for Locally Advanced Pancreatic Cancer. Gastrointest. Endosc. 2019, 89, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, J.S.; Mick, R.; Culligan, M.; Stevenson, J.; Fernandes, A.; Smith, D.; Glatstein, E.; Hahn, S.M.; Cengel, K. Photodynamic Therapy and the Evolution of a Lung-Sparing Surgical Treatment for Mesothelioma. Ann. Thorac. Surg. 2011, 91, 1738–1745. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Shen, X.; Li, L.; Guan, Z.; Gao, N.; Yuan, P.; Yao, S.Q.; Xu, Q.H.; Xu, G.Q. Gold Nanorods as Dual Photo-Sensitizing and Imaging Agents for Two-Photon Photodynamic Therapy. Nanoscale 2012, 4, 7712–7719. [Google Scholar] [CrossRef] [PubMed]
- Skripka, A.; Dapkute, D.; Valanciunaite, J.; Karabanovas, V.; Rotomskis, R. Impact of Quantum Dot Surface on Complex Formation with Chlorin E6 and Photodynamic Therapy. Nanomaterials 2019, 9, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Secret, E.; Maynadier, M.; Gallud, A.; Chaix, A.; Bouffard, E.; Gary-Bobo, M.; Marcotte, N.; Mongin, O.; El Cheikh, K.; Hugues, V.; et al. Two-Photon Excitation of Porphyrin-Functionalized Porous Silicon Nanoparticles for Photodynamic Therapy. Adv. Mater. 2014, 26, 7643–7648. [Google Scholar] [CrossRef]
- Zhao, T.; Li, L.; Li, S.; Jiang, X.F.; Jiang, C.; Zhou, N.; Gao, N.; Xu, Q.H. Gold Nanorod-Enhanced Two-Photon Excitation Fluorescence of Conjugated Oligomers for Two-Photon Imaging Guided Photodynamic Therapy. J. Mater. Chem. C 2019, 7, 14693–14700. [Google Scholar] [CrossRef]
- Zhang, P.; Huang, H.; Huang, J.; Chen, H.; Wang, J.; Qiu, K.; Zhao, D.; Ji, L.; Chao, H. Noncovalent Ruthenium(II) Complexes-Single-Walled Carbon Nanotube Composites for Bimodal Photothermal and Photodynamic Therapy with Near-Infrared Irradiation. ACS Appl. Mater. Interfaces 2015, 7, 23278–23290. [Google Scholar] [CrossRef]
- Shen, X.; Li, L.; Wu, H.; Yao, S.Q.; Xu, Q.H. Photosensitizer-Doped Conjugated Polymer Nanoparticles for Simultaneous Two-Photon Imaging and Two-Photon Photodynamic Therapy in Living Cells. Nanoscale 2011, 3, 5140–5146. [Google Scholar] [CrossRef]
- Sun, H.-B.; Tanaka, T.; Kawata, S. Three-Dimensional Focal Spots Related to Two-Photon Excitation. Appl. Phys. Lett. 2002, 80, 3673–3675. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Fei, J.; Zhao, J.; Li, H.; Cui, Y.; Li, J. Hypocrellin-Loaded Gold Nanocages with High Two-Photon Efficiency for Photothermal/Photodynamic Cancer Therapy In Vitro. ACS Nano 2012, 6, 8030–8040. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Cheng, L.; Liu, Z. Upconversion Nanoparticles for Photodynamic Therapy and Other Cancer Therapeutics. Theranostics 2013, 3, 317–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, H.; Tan, M.; Ohulchanskyy, T.Y.; Lovell, J.F.; Chen, G. Recent Progress in Upconversion Photodynamic Therapy. Nanomaterials 2018, 8, 344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Zhang, K.; Zada, S.; Zhang, C.; Meng, X.; Yang, Z.; Dong, H. Upconversion Nanoparticle-Induced Multimode Photodynamic Therapy Based on a Metal-Organic Framework/Titanium Dioxide Nanocomposite. ACS Appl. Mater. Interfaces 2020, 12, 12600–12608. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Tao, H.; Cheng, L.; Liu, Z. Near-Infrared Light Induced in Vivo Photodynamic Therapy of Cancer Based on Upconversion Nanoparticles. Biomaterials 2011, 32, 6145–6154. [Google Scholar] [CrossRef]
- Xia, L.; Kong, X.; Liu, X.; Tu, L.; Zhang, Y.; Chang, Y.; Liu, K.; Shen, D.; Zhao, H.; Zhang, H. An Upconversion Nanoparticle—Zinc Phthalocyanine Based Nanophotosensitizer for Photodynamic Therapy. Biomaterials 2014, 35, 4146–4156. [Google Scholar] [CrossRef]
- Idris, N.M.; Gnanasammandhan, M.K.; Zhang, J.; Ho, P.C.; Mahendran, R.; Zhang, Y. In Vivo Photodynamic Therapy Using Upconversion Nanoparticles as Remote-Controlled Nanotransducers. Nat. Med. 2012, 18, 1580–1585. [Google Scholar] [CrossRef]
- Cui, S.; Yin, D.; Chen, Y.; Di, Y.; Chen, H.; Ma, Y.; Achilefu, S.; Gu, Y. In Vivo Targeted Deep-Tissue Photodynamic Therapy Based on near-Infrared Light Triggered Upconversion Nanoconstruct. ACS Nano 2013, 7, 676–688. [Google Scholar] [CrossRef]
- Gnach, A.; Lipinski, T.; Bednarkiewicz, A.; Rybka, J.; Capobianco, J.A. Upconverting Nanoparticles: Assessing the Toxicity. Chem. Soc. Rev. 2015, 44, 1561–1584. [Google Scholar] [CrossRef]
- Wang, G.D.; Nguyen, H.T.; Chen, H.; Cox, P.B.; Wang, L.; Nagata, K.; Hao, Z.; Wang, A.; Li, Z.; Xie, J. X-ray Induced Photodynamic Therapy: A Combination of Radiotherapy and Photodynamic Therapy. Theranostics 2016, 6, 2295–2305. [Google Scholar] [CrossRef]
- Sun, W.; Zhou, Z.; Pratx, G.; Chen, X.; Chen, H. Nanoscintillator-Mediated X-ray Induced Photodynamic Therapy for Deep-Seated Tumors: From Concept to Biomedical Applications. Theranostics 2020, 10, 1296–1318. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, J.; Ogura, S.I.; Tanaka, T.; Kitagawa, T.; Nakano, Y.; Saito, T.; Takahashi, M.; Akiba, D.; Nishizawa, S. Radiosensitizing Effect of 5-Aminolevulinic Acid-Induced Protoporphyrin IX in Glioma Cells In Vitro. Oncol. Rep. 2012, 27, 1748–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, J.; Misawa, M.; Iwahashi, H. Combined Treatment with X-ray Irradiation and 5-Aminolevulinic Acid Elicits Better Transcriptomic Response of Cell Cycle-Related Factors than X-ray Irradiation Alone. Int. J. Radiat. Biol. 2016, 92, 774–789. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, J.; Misawa, M. Characterization of Reactive Oxygen Species Generated by Protoporphyrin IX under X-ray Irradiation. Radiat. Phys. Chem. 2009, 78, 889–898. [Google Scholar] [CrossRef]
- Chen, H.; Wang, G.D.; Chuang, Y.J.; Zhen, Z.; Chen, X.; Biddinger, P.; Hao, Z.; Liu, F.; Shen, B.; Pan, Z.; et al. Nanoscintillator-Mediated X-ray Inducible Photodynamic Therapy for In Vivo Cancer Treatment. Nano Lett. 2015, 15, 2249–2256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, E.J.; Giaccia, A.J. Radiobiology for the Radiologist: Seventh Edition; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; ISBN 9781451154184. [Google Scholar]
- Rossi, F.; Bedogni, E.; Bigi, F.; Rimoldi, T.; Cristofolini, L.; Pinelli, S.; Alinovi, R.; Negri, M.; Dhanabalan, S.C.; Attolini, G. Porphyrin Conjugated SiC/SiO x Nanowires for X-ray-Excited Photodynamic Therapy. Sci. Rep. 2015, 5, 7606. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, J.; Murakami, M.; Mori, T.; Iwahashi, H. Verification of Radiodynamic Therapy by Medical Linear Accelerator Using a Mouse Melanoma Tumor Model. Sci. Rep. 2018, 8, 2728. [Google Scholar] [CrossRef]
- Sun, W.; Luo, L.; Feng, Y.; Cai, Y.; Zhuang, Y.; Xie, R.J.; Chen, X.; Chen, H. Aggregation-Induced Emission Gold Clustoluminogens for Enhanced Low-Dose X-ray-Induced Photodynamic Therapy. Angew. Chem. Int. Ed. 2020, 59, 9914–9921. [Google Scholar] [CrossRef]
- Kaščáková, S.; Giuliani, A.; Lacerda, S.; Pallier, A.; Mercère, P.; Tóth, É.; Réfrégiers, M. X-ray-Induced Radiophotodynamic Therapy (RPDT) Using Lanthanide Micelles: Beyond Depth Limitations. Nano Res. 2015, 8, 2373–2379. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.; Hu, J.; Elmenoufy, A.H.; Yang, X. Highly Efficient FRET System Capable of Deep Photodynamic Therapy Established on X-ray Excited Mesoporous LaF3:Tb Scintillating Nanoparticles. ACS Appl. Mater. Interfaces 2015, 7, 12261–12269. [Google Scholar] [CrossRef]
- Hsu, C.C.; Lin, S.L.; Chang, C.A. Lanthanide-Doped Core-Shell-Shell Nanocomposite for Dual Photodynamic Therapy and Luminescence Imaging by a Single X-ray Excitation Source. ACS Appl. Mater. Interfaces 2018, 10, 7859–7870. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Sun, X.; Wang, G.D.; Nagata, K.; Hao, Z.; Wang, A.; Li, Z.; Xie, J.; Shen, B. LiGa5O8:Cr-Based Theranostic Nanoparticles for Imaging-Guided X-ray Induced Photodynamic Therapy of Deep-Seated Tumors. Mater. Horiz. 2017, 4, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhao, K.; Bu, W.; Ni, D.; Liu, Y.; Feng, J.; Shi, J. Marriage of Scintillator and Semiconductor for Synchronous Radiotherapy and Deep Photodynamic Therapy with Diminished Oxygen Dependence. Angew. Chem. Int. Ed. 2015, 54, 1770–1774. [Google Scholar] [CrossRef] [PubMed]
- Lan, G.; Ni, K.; Xu, R.; Lu, K.; Lin, Z.; Chan, C.; Lin, W. Nanoscale Metal–Organic Layers for Deeply Penetrating X-ray-Induced Photodynamic Therapy. Angew. Chem. Int. Ed. 2017, 56, 12102–12106. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zou, X.; Bui, B.; Chen, W.; Song, K.H.; Solberg, T. X-ray Excited ZnS: Cu, Co Afterglow Nanoparticles for Photodynamic Activation. Appl. Phys. Lett. 2014, 10, 1501–1508. [Google Scholar] [CrossRef]
- Borbas, K.E.; Lahaye, D. Photodynamic Therapy of Cancer. Anticancer Ther. 2008, 9, 187–222. [Google Scholar] [CrossRef]
- Bulin, A.L.; Truillet, C.; Chouikrat, R.; Lux, F.; Frochot, C.; Amans, D.; Ledoux, G.; Tillement, O.; Perriat, P.; Barberi-Heyob, M.; et al. X-ray-Induced Singlet Oxygen Activation with Nanoscintillator-Coupled Porphyrins. J. Phys. Chem. C 2013, 117, 21583–21589. [Google Scholar] [CrossRef]
- Clement, S.; Anwer, A.G.; Pires, L.; Campbell, J.; Wilson, B.C.; Goldys, E.M. Radiodynamic Therapy Using Tat Peptide-targeted Verteporfin-encapsulated Plga Nanoparticles. Int. J. Mol. Sci. 2021, 22, 6425. [Google Scholar] [CrossRef]
- Jeremic, B.; Aguerri, A.R.; Filipovic, N. Radiosensitization by Gold Nanoparticles. Clin. Transl. Oncol. 2013, 15, 593–601. [Google Scholar] [CrossRef]
- Jain, S.; Coulter, J.A.; Hounsell, A.R.; Butterworth, K.T.; McMahon, S.J.; Hyland, W.B.; Muir, M.F.; Dickson, G.R.; Prise, K.M.; Currell, F.J. Cell-Specific Radiosensitization by Gold Nanoparticles at Megavoltage Radiation Energies. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 531–539. [Google Scholar] [CrossRef] [Green Version]
- Bulin, A.-L.; Vasil’Ev, A.; Belsky, A.; Amans, D.; Ledoux, G.; Dujardin, C. Modelling Energy Deposition in Nanoscintillators to Predict the Efficiency of the X-ray-Induced Photodynamic Effect. Nanoscale 2015, 7, 5744–5751. [Google Scholar] [CrossRef] [PubMed]
- Roeske, J.C.; Nunez, L.; Hoggarth, M.; Labay, E.; Weichselbaum, R.R. Characterization of the Theorectical Radiation Dose Enhancement from Nanoparticles. Technol. Cancer Res. Treat. 2007, 6, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Bulin, A.; Broekgaarden, M.; Chaput, F.; Baisamy, V.; Garrevoet, J.; Busser, B.; Brueckner, D.; Youssef, A.; Ravanat, J.; Dujardin, C. Radiation Dose-Enhancement Is a Potent Radiotherapeutic Effect of Rare-Earth Composite Nanoscintillators in Preclinical Models of Glioblastoma. Adv. Sci. 2020, 7, 2001675. [Google Scholar] [CrossRef] [PubMed]
- Cline, B.; Delahunty, I.; Xie, J. Nanoparticles to Mediate X-ray-Induced Photodynamic Therapy and Cherenkov Radiation Photodynamic Therapy. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2019, 11, e1541. [Google Scholar] [CrossRef] [PubMed]
- Ran, C.; Zhang, Z.; Hooker, J.; Moore, A. In Vivo Photoactivation without “Light”: Use of Cherenkov Radiation to Overcome the Penetration Limit of Light. Mol. Imaging Biol. 2012, 14, 156–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartl, B.A.; Boucher, D.L.; Marcu, L.; Cherry, S.R. Photodynamic Therapy Activated with Cerenkov Luminescence from Beta-Emitting Radionuclides. In Optical Molecular Probes, Imaging and Drug Delivery; Optical Society of America: Washington, DC, USA, 2013; p. JT2A-11. [Google Scholar]
- Kassis, A.I. Therapeutic Radionuclides: Biophysical and Radiobiologic Principles. Semin. Nucl. Med. 2008, 38, 358–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
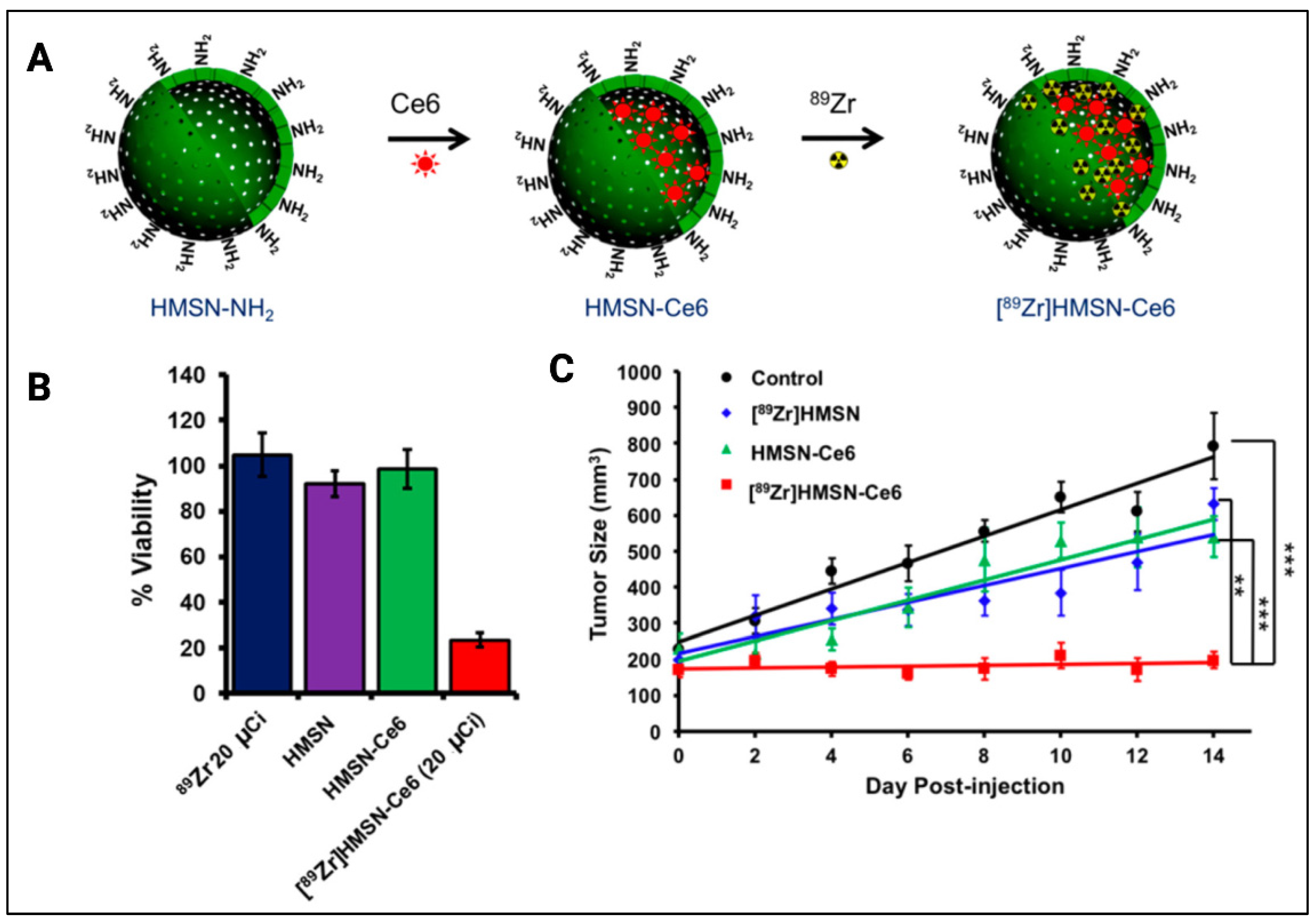
- Kamkaew, A.; Cheng, L.; Goel, S.; Valdovinos, H.F.; Barnhart, T.E.; Liu, Z.; Cai, W. Cerenkov Radiation Induced Photodynamic Therapy Using Chlorin E6-Loaded Hollow Mesoporous Silica Nanoparticles. ACS Appl. Mater. Interfaces 2016, 8, 26630–26637. [Google Scholar] [CrossRef] [Green Version]
- Duan, D.; Liu, H.; Xu, Y.; Han, Y.; Xu, M.; Zhang, Z.; Liu, Z. Activating TiO2 Nanoparticles: Gallium-68 Serves as a High-Yield Photon Emitter for Cerenkov-Induced Photodynamic Therapy. ACS Appl. Mater. Interfaces 2018, 10, 5278–5286. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, N.; Hou, Z.; Shi, J.; Su, X.; Sun, X. Radioiodinated Persistent Luminescence Nanoplatform for Radiation-Induced Photodynamic Therapy and Radiotherapy. Adv. Healthc. Mater. 2020, 10, 2000802. [Google Scholar] [CrossRef]
- Kotagiri, N.; Sudlow, G.P.; Akers, W.J.; Achilefu, S. Breaking the Depth Dependency of Phototherapy with Cerenkov Radiation and Low-Radiance-Responsive Nanophotosensitizers. Nat. Nanotechnol. 2015, 10, 370–379. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Guo, Y.; Sheng, S.; C. Lun, M.; Tsai, S.-M.; Chin, W.-C.; Hoglund, R.; Li, C. Photodynamic Therapy Excited by Cerenkov Radiation from Cesium-137 Irradiator: In Vitro Studies. Clin. Oncol. Res. 2020, 1–5. [Google Scholar] [CrossRef]
- Howard, M.; Beltran, C.; Sarkaria, J.; Herman, M.G. Characterization of Relative Biological Effectiveness for Conventional Radiation Therapy: A Comparison of Clinical 6 MV X-rays and 137Cs. J. Radiat. Res. 2017, 58, 608–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, W.P.; Kooy, H.; Loeffler, J.S.; DeLaney, T.F. Proton Beam Therapy. Br. J. Cancer 2005, 93, 849–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigalavicius, M.; Mastrangelopoulou, M.; Berg, K.; Arous, D.; Ménard, M.; Raabe-Henriksen, T.; Brondz, E.; Siem, S.; Görgen, A.; Edin, N.F.J.; et al. Proton-Dynamic Therapy Following Photosensitiser Activation by Accelerated Protons Demonstrated through Fluorescence and Singlet Oxygen Production. Nat. Commun. 2019, 10, 3986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, J.R.; Parsons, J.L. Flash Radiotherapy: Current Knowledge and Future Insights Using Proton-Beam Therapy. Int. J. Mol. Sci. 2020, 21, 6492. [Google Scholar] [CrossRef]
- Favaudon, V.; Caplier, L.; Monceau, V.; Pouzoulet, F.; Sayarath, M.; Fouillade, C.; Poupon, M.F.; Brito, I.; Hupé, P.; Bourhis, J.; et al. Ultrahigh Dose-Rate FLASH Irradiation Increases the Differential Response between Normal and Tumor Tissue in Mice. Sci. Transl. Med. 2014, 6, 245ra93, Erratum in Sci. Transl. Med. 2019, 11, 6137–6151. [Google Scholar] [CrossRef]
- Wilson, J.D.; Hammond, E.M.; Higgins, G.S.; Petersson, K. Ultra-High Dose Rate (FLASH) Radiotherapy: Silver Bullet or Fool’s Gold? Front. Oncol. 2020, 9, 1563. [Google Scholar] [CrossRef] [Green Version]
- Favaudon, V.; Lentz, J.-M.; Heinrich, S.; Patriarca, A.; de Marzi, L.; Fouillade, C.; Dutreix, M. Time-Resolved Dosimetry of Pulsed Electron Beams in Very High Dose-Rate, FLASH Irradiation for Radiotherapy Preclinical Studies. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2019, 944, 162537. [Google Scholar] [CrossRef]
- Wu, M.; Wu, L.; Li, J.; Zhang, D.; Lan, S.; Zhang, X.; Lin, X.; Liu, G.; Liu, X.; Liu, J. Self-Luminescing Theranostic Nanoreactors with Intraparticle Relayed Energy Transfer for Tumor Microenvironment Activated Imaging and Photodynamic Therapy. Theranostics 2019, 9, 20–33. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Chen, C.W.; Yu, H.P.; Lin, Y.F.; Lai, P.S. Bioluminescence Resonance Energy Transfer Using Luciferase-Immobilized Quantum Dots for Self-Illuminated Photodynamic Therapy. Biomaterials 2013, 34, 1204–1212. [Google Scholar] [CrossRef]
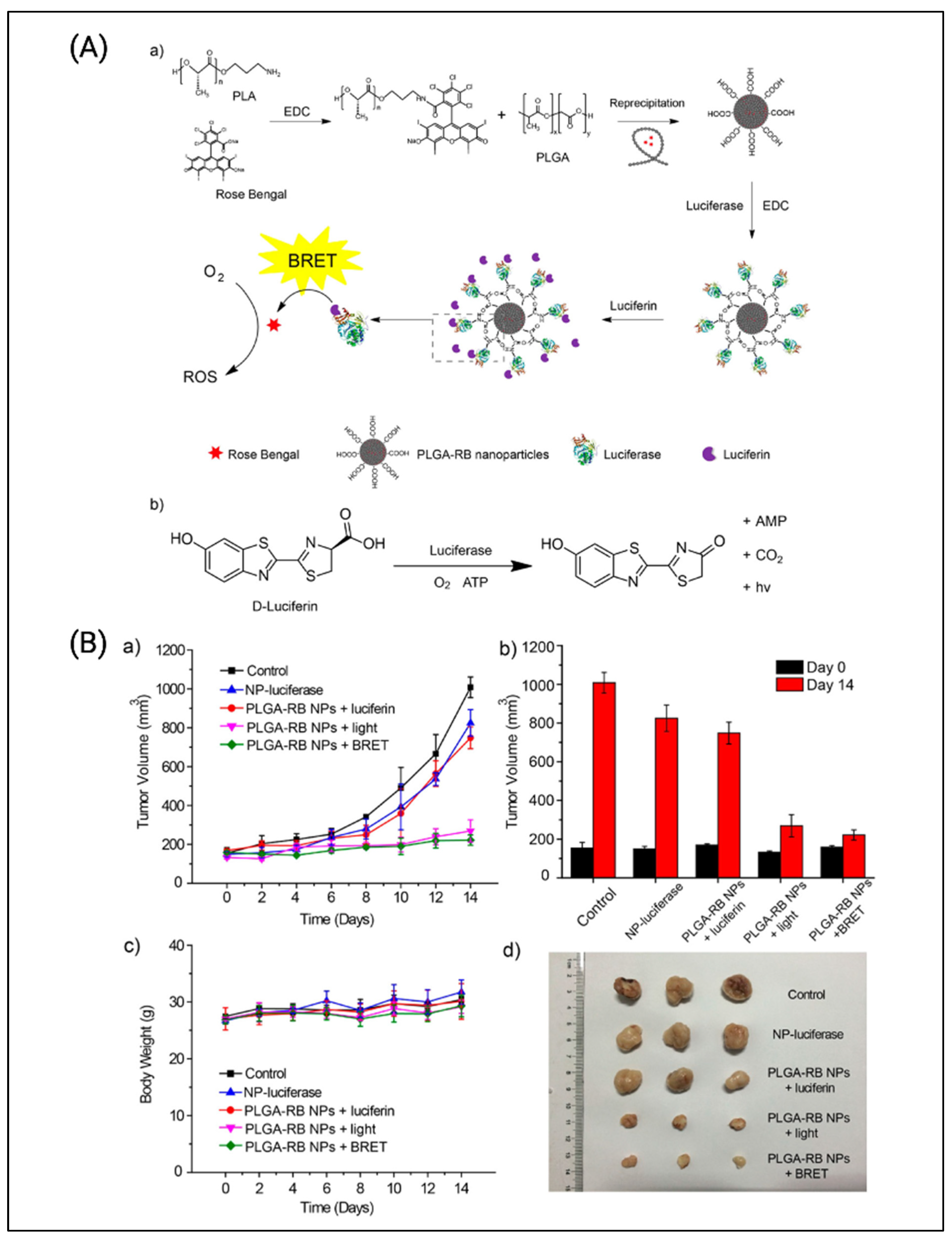
- Yang, Y.; Hou, W.; Liu, S.; Sun, K.; Li, M.; Wu, C. Biodegradable Polymer Nanoparticles for Photodynamic Therapy by Bioluminescence Resonance Energy Transfer. Biomacromolecules 2018, 19, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Song, X.; Wang, Q.; Hu, W.; Shi, W.; Tang, Y.; Wu, Z.; Fan, Q.; Huang, W. Chemiluminescent Organic Nanophotosensitizer for a Penetration Depth Independent Photodynamic Therapy. RSC Adv. 2020, 10, 11861–11864. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Chen, Y.; Zhou, W.; Li, J.; Zhang, Y.; Liu, Y. Mitochondrion-Targeting Chemiluminescent Ternary Supramolecular Assembly for: In Situ Photodynamic Therapy. Chem. Commun. 2020, 56, 8857–8860. [Google Scholar] [CrossRef] [PubMed]
- Tsuru, H.; Shibaguchi, H.; Kuroki, M.; Yamashita, Y.; Kuroki, M. Tumor Growth Inhibition by Sonodynamic Therapy Using a Novel Sonosensitizer. Free Radic. Biol. Med. 2012, 53, 464–472. [Google Scholar] [CrossRef]
- Kessel, D.; Lo, J.; Jeffers, R.; Fowlkes, J.B.; Cain, C. Modes of Photodynamic vs. Sonodynamic Cytotoxicity. J. Photochem. Photobiol. B Biol. 1995, 28, 219–221. [Google Scholar] [CrossRef]
- Rosenthal, I.; Sostaric, J.Z.; Riesz, P. Sonodynamic Therapy––A Review of the Synergistic Effects of Drugs and Ultrasound. Ultrason. Sonochem 2004, 11, 349–363. [Google Scholar] [CrossRef]
- Choi, V.; Rajora, M.A.; Zheng, G. Activating Drugs with Sound: Mechanisms behind Sonodynamic Therapy and the Role of Nanomedicine. Bioconjugate Chem. 2020, 31, 967–989. [Google Scholar] [CrossRef]
- McHale, A.P.; Callan, J.F.; Nomikou, N.; Fowley, C.; Callan, B. Sonodynamic Therapy: Concept, Mechanism and Application to Cancer Treatment. Adv. Exp. Med. Biol. 2016, 880, 429–450. [Google Scholar] [CrossRef]
- McEwan, C.; Owen, J.; Stride, E.; Fowley, C.; Nesbitt, H.; Cochrane, D.; Coussios, C.C.; Borden, M.; Nomikou, N.; McHale, A.P.; et al. Oxygen Carrying Microbubbles for Enhanced Sonodynamic Therapy of Hypoxic Tumours. J. Control. Release 2015, 203, 51–56. [Google Scholar] [CrossRef]
- Borah, B.M.; Cacaccio, J.; Durrani, F.A.; Bshara, W.; Turowski, S.G.; Spernyak, J.A.; Pandey, R.K. Sonodynamic Therapy in Combination with Photodynamic Therapy Shows Enhanced Long-Term Cure of Brain Tumor. Sci. Rep. 2020, 10, 21791. [Google Scholar] [CrossRef]
- Ohmura, T.; Fukushima, T.; Shibaguchi, H.; Yoshizawa, S.; Inoue, T.; Kuroki, M.; Sasaki, K.; Umemura, S.I. Sonodynamic Therapy with 5-Aminolevulinic Acid and Focused Ultrasound for Deep-Seated Intracranial Glioma in Rat. Anticancer Res. 2011, 31, 2527–2534. [Google Scholar] [PubMed]
- Suzuki, N.; Okada, K.; Chida, S.; Komori, C.; Shimada, Y.; Suzuki, T. Antitumor Effect of Acridine Orange under Ultrasonic Irradiation In Vitro. Anticancer Res. 2007, 27, 4179–4184. [Google Scholar] [PubMed]
- Yumita, N.; Han, Q.S.; Kitazumi, I.; Umemura, S.I. Sonodynamically-Induced Apoptosis, Necrosis, and Active Oxygen Generation by Mono-l-Aspartyl Chlorin E6. Cancer Sci. 2008, 99, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Yumita, N.; Umemura, S.I. Ultrasonically Induced Cell Damage and Membrane Lipid Peroxidation by Photofrin II: Mechanism of Sonodynamic Activation. J. Med. Ultrason. 2004, 31, 35–40. [Google Scholar] [CrossRef]
- Hachimine, K.; Shibaguchi, H.; Kuroki, M.; Yamada, H.; Kinugasa, T.; Nakae, Y.; Asano, R.; Sakata, I.; Yamashita, Y.; Shirakusa, T.; et al. Sonodynamic Therapy of Cancer Using a Novel Porphyrin Derivative, DCPH-P-Na(I), Which Is Devoid of Photosensitivity. Cancer Sci. 2007, 98, 916–920. [Google Scholar] [CrossRef]
- Dai, S.; Hu, S.; Wu, C. Apoptotic Effect of Sonodynamic Therapy Mediated by Hematoporphyrin Monomethyl Ether on C6 Glioma Cells In Vitro. Acta Neurochir. 2009, 151, 1655–1661. [Google Scholar] [CrossRef]
- Rocha, S.; Generalov, R.; Pereira, M.D.C.; Peres, I.; Juzenas, P.; Coelho, M.A.N. Epigallocatechin Gallate-Loaded Polysaccharide Nanoparticles for Prostate Cancer Chemoprevention. Nanomed. 2011, 6, 79–87. [Google Scholar] [CrossRef]
- Nomikou, N.; Sterrett, C.; Arthur, C.; Mccaughan, B.; Callan, J.F.; Mchale, A.P. The Effects of Ultrasound and Light on Indocyanine Green-Treated Tumour Cells and Tissues. ChemMedChem 2012, 7, 1465–1471. [Google Scholar] [CrossRef]
- Komori, C.; Okada, K.; Kawamura, K.; Chida, S.; Suzuki, T. The Sonodynamic Antitumor Effect of Methylene Blue on Sarcoma180 Cells In Vitro. Anticancer Res. 2009, 29, 2411–2415. [Google Scholar]
- Xu, Z.Y.; Wang, K.; Li, X.Q.; Chen, S.; Deng, J.M.; Cheng, Y.; Wang, Z.G. The ABCG2 Transporter Is a Key Molecular Determinant of the Efficacy of Sonodynamic Therapy with Photofrin in Glioma Stem-like Cells. Ultrasonics 2013, 53, 232–238. [Google Scholar] [CrossRef]
- Kolarova, H.; Tomankova, K.; Bajgar, R.; Kolar, P.; Kubinek, R. Photodynamic and Sonodynamic Treatment by Phthalocyanine on Cancer Cell Lines. Ultrasound Med. Biol. 2009, 35, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Sun, X.; Cheng, J.; Xu, H.; Dan, J.; Shen, J.; Zhou, Q.; Zhang, Y.; Meng, L.; Cao, W.; et al. Apoptosis of THP-1 Macrophages Induced by Protoporphyrin IX-Mediated Sonodynamic Therapy. Int. J. Nanomed. 2013, 8, 2239–2246. [Google Scholar] [CrossRef] [Green Version]
- Hou, R.; Liang, X.; Li, X.; Zhang, X.; Ma, X.; Wang, F. In Situ Conversion of Rose Bengal Microbubbles into Nanoparticles for Ultrasound Imaging Guided Sonodynamic Therapy with Enhanced Antitumor Efficacy. Biomater. Sci. 2020, 8, 2526–2536. [Google Scholar] [CrossRef] [PubMed]
- Sugita, N.; Iwase, Y.; Yumita, N.; Ikeda, T.; Umemura, S.I. Sonodynamically Induced Cell Damage Using Rose Bengal Derivative. Anticancer Res. 2010, 30, 3361–3366. [Google Scholar]
- Visible Wavelengths Infrared Wavelengths. Available online: www.modulight.com (accessed on 7 December 2021).
- BioSpec Break in the Clouds. Available online: http://www.biospec.ru (accessed on 7 December 2021).
- Dolak, W.; Schwaighofer, H.; Hellmich, B.; Stadler, B.; Spaun, G.; Plieschnegger, W.; Hebenstreit, A.; Weber-Eibel, J.; Siebert, F.; Emmanuel, K.; et al. Photodynamic Therapy with Polyhematoporphyrin for Malignant Biliary Obstruction: A Nationwide Retrospective Study of 150 Consecutive Applications. United Eur. Gastroenterol. J. 2017, 5, 104. [Google Scholar] [CrossRef]
- DermaInspect|Multiphoton Tomography. Available online: https://mpt-tomography.de/dermainspect/ (accessed on 9 December 2021).
- MPTflex|Multiphoton Tomography. Available online: https://mpt-tomography.de/mptflex/ (accessed on 9 December 2021).
- Aldelaimi, T.N. Laser-Assisted Frenectomy Using 980nm Diode Laser Clinical Application of BIOLASE Epic X (940 Nm) in Orofacial Region View Project. J. Dent. Oral. Disord. Ther. 2014, 2, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Health Management and Leadership Portal|Surgical Laser/Diode/Tabletop 810 Nm, 940 Nm, 980 Nm|CHIROLAS A.R.C. Laser|HealthManagement.Org. Available online: https://healthmanagement.org/products/view/surgical-laser-diode-tabletop-810-nm-940-nm-980-nm-chirolas-a-r-c-laser (accessed on 9 December 2021).
- Caruso, U.; Nastri, L.; Piccolomini, R.; Mazza, C.; Guida, L. Use of Diode Laser 980 Nm as Adjunctive Therapy in the Treatment of Chronic Periodontitis. A Randomized Controlled Clinical Trial. New Microbiol. 2008, 31, 513–518. [Google Scholar]
- Velure S9—Lasering. Available online: https://www.lasering-med.com/velure-s9-en/ (accessed on 9 December 2021).
- YSIO X.Pree with MyExam Companion. Available online: https://www.siemens-healthineers.com/en-us/radiography/digital-x-ray/ysio-xpree (accessed on 9 December 2021).
- Clinical Technologies: Radiation Oncology—UT Southwestern, Dallas, Texas. Available online: https://www.utsouthwestern.edu/education/medical-school/departments/radiation-oncology/facilities/clinical.html (accessed on 9 December 2021).
- Kerja, E.P.T. YSIO X.Pree—A Radiography X-ray System. Angew. Chem. Int. Ed. 1967, 13, 15–38. [Google Scholar]
- TrueBeam|Varian. Available online: https://www.varian.com/products/radiotherapy/treatment-delivery/truebeam (accessed on 9 December 2021).
- Kalantzis, G.; Qian, J.; Han, B.; Luxton, G. Fidelity of Dose Delivery at High Dose Rate of Volumetric Modulated Arc Therapy in a Truebeam Linac with Flattening Filter Free Beams. J. Med. Phys. Assoc. Med. Phys. India 2012, 37, 193. [Google Scholar] [CrossRef]
- History and Technical Overview—Neurosurgery. Available online: https://med.virginia.edu/neurosurgery/services/gamma-knife/for-physicians/history-and-technical-overview/ (accessed on 9 December 2021).
- Leksell Gamma Knife® PerfexionTM|Radiosurgery|Elekta. Available online: https://www.elekta.com/radiosurgery/leksell-gamma-knife-perfexion/ (accessed on 9 December 2021).
- MacDonald, S.M.; Trofimov, A.; Safai, S.; Adams, J.; Fullerton, B.; Ebb, D.; Tarbell, N.J.; Yock, T.I. Proton Radiotherapy for Pediatric Central Nervous System Germ Cell Tumors: Early Clinical Outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 121–129. [Google Scholar] [CrossRef]
- DeLaney, T.F. Clinical Proton Radiation Therapy Research at the Francis H. Burr Proton Therapy Center. Technol. Cancer Res. Treat. 2007, 6, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viera® Breast Performance Software with Clarius HD|Hologic. Available online: https://www.hologic.com/hologic-products/breast-health-solutions/viera-breast-performance-software-clarius-hd#overview (accessed on 7 December 2021).
- Prusator, M.T.; Ahmad, S.; Chen, Y. Shielding Verification and Neutron Dose Evaluation of the Mevion S250 Proton Therapy Unit. J. Appl. Clin. Med. Phys. 2018, 19, 305. [Google Scholar] [CrossRef] [PubMed]
- MEVION S250 Proton Therapy System|Mevion Medical Systems. Available online: https://www.mevion.com/products/mevion-s250-proton-therapy-system (accessed on 9 December 2021).
- Izadifar, Z.; Izadifar, Z.; Chapman, D.; Babyn, P. An Introduction to High Intensity Focused Ultrasound: Systematic Review on Principles, Devices, and Clinical Applications. J. Clin. Med. 2020, 9, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]












| PNM Precursor | Respective Class of PNM Used Preclinically | Example of Clinical Trial Using PNM Precursor | Clinical Utility | Clinical Format |
|---|---|---|---|---|
| Gadolinium nanoparticles | X-ray scintillators | NCT04899908 | Treating patients with brain metastases | Gadolinium-based nanoparticles |
| Zirconium complexes | Cerenkov-activable PNMs | NCT04758780 | PET/CT imaging in metastatic triple negative breast cancer | 89Zr-labeled girentuximab |
| Titanium dioxide nanoparticles | Cerenkov-activable photocatalytic PNMs | NCT03250520 | Delivery vehicle for platinum acetylacetonate chemotherapy | Platinum acetylacetonate (1%wt) supported by sol-gel technology functionalized with titania platinum |
| Gallium complexes | Radionuclide labeled, Cerenkov-activable PNMs | NCT04023240 | PET/CT imaging of cancer-associated fibroblasts | 68Ga-FAPI (68-Ga-Fibroblast activation protein inhibitor) |
| Ruthenium complexes | Two-photon excited PNMs | NCT03945162 | PDT of non-muscle invasive bladder cancer | TLD-1433 Ruthenium complex |
| Gold nanoparticles | X-ray radiosensitizers | NCT04240639 | Photothermal therapy of prostate neoplasms | Gold-coated silica nanoshells |
| Renilla luciferase | Bioluminescence resonance energy transfer-activable PNMs | NCT00794131 | Safety evaluation of vaccina virus in patients with solid tumors | GL-ONC1 a genetically engineered vaccina virus encoding Renilla luciferase |
| Energy of Applied X-rays (keV) | Dose of Applied X-rays (Gy, If Mentioned) | Reactive Molecular Species Detected | PS (Scintillating/Vehicle Nanoformulation) | Reference |
|---|---|---|---|---|
| 75 | 1 | 1O2 | rose bengal (glutathione-protected gold nanoclusters) | [40] |
| 15 | n.a. | 1O2 | hypericin (GdEuC12 micellar particles) | [41] |
| 75 | n.a. | 1O2 | rose bengal (mesoporous LaF3:Tb nanoscintillators) | [42] |
| 160 | 5 | 1O2 | rose bengal (mesoporous silica nanoparticles with NaLuF4: Gd3+,Eu3+,Tb3+) | [43] |
| 50 | 5 | 1O2 | 2,3-naphthalocyanine (mesoporous silica nanoparticles with LiGa5O8: Cr) | [44] |
| 220 | 8 | •OH | zinc oxide nanoparticles (Ce(III)-doped LiYF4 core-shell nanoscintillator) | [45] |
| 225 | 2 | 1O2 | iridium and ruthenium complexes (Hf6O4 -based metal-organic layers) | [46] |
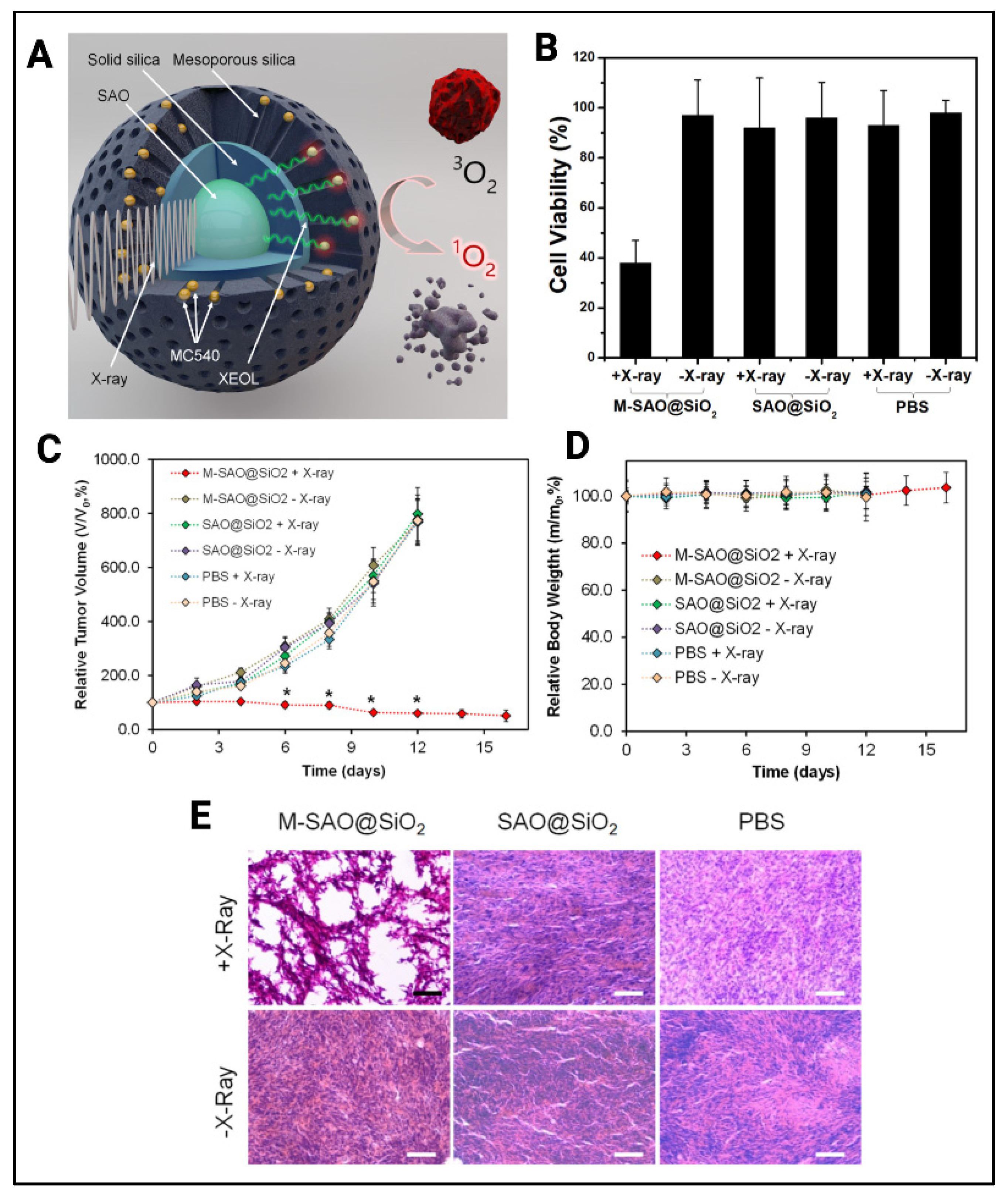
| 50 | 1 to 10 | 1O2 | merocyanine 540 (mesoporous silica coated SrAL2O4: Eu2+ nanoscintillators) | [36] |
| 120 | 2 | 1O2 | tetrabromorhodamine-123 (copper and cobalt co-doped ZnS) | [47] |
| 90 | 3 | 1O2 | protoporphyrin IX (PLGA microspheres with Cerium (III)-doped lanthanum (III) fluoride (LaF3: Ce3+) | [48] |
| 44 | 11 | 1O2, •OH | porphyrin (polysiloxane layered Tb2O3 nanoscintillators) | [49] |
| 6000 | 0.4 to 2 | 1O2 | porphyrin (SiC/SiOx nanowires) | [38] |
| Manufacturer | Model | Clinical Operating Powers | Clinical Utility | Typical Wavelengths and Dose Parameters | Reference |
|---|---|---|---|---|---|
| Modulight | ML7710-PDT laser system | 1 to 15 W | For sterilization of deep tissues | 668 nm, 20 mW/cm2 | NCT02240498 [98] |
| MMOptics | Laser Duo® red laser diode | 100 mW | Treatment of Herpes labialis | 660 nm, 300 J/cm2, 3 J at center of lesion | NCT04037475 |
| BIOSPEC | UFPh-675-01-BIOSPEC | 1000 mW top optical power | Anti-viral treatment for COVID-19 | 650 nm, 36 J/cm2 | NCT04933864 [99] |
| Diomed Inc, An-dover, MA | InGaAIP laser diode | 2000 mW maximum power | Treatment for advanced rectal cancer | 633 ± 3 nm, 200 J/cm2 | NCT01872104 |
| PDT® HGesmbH, Vienna, Austria | 30 or 70 mm radial light applicator | n.a. | Treatment for malignant biliary obstruction | 650 nm with 400 mW/cm2 and 250 J/cm2 during 650 s radiation time | NCT02504957 [100] |
| Manufacturer | Model | Clinical Operating Powers | Clinical Utility | Typical Wavelengths | Reference |
|---|---|---|---|---|---|
| MPT | DermaInspect | 0 to 1.5 W | Diagnosis of dermatological disorder | 720 to 920 nm | [101] |
| MPT | MPTflex | 2 to 50 mW | Diagnosis of dermatological disorder | 710 to 920 nm (45 mW:5 mW pump beam:Stokes beam) | [102] |
| Manufacturer | Model | Clinical Operating Powers | Clinical Utility | Typical Operation Ranges | Reference |
|---|---|---|---|---|---|
| Lasering Medical Laser | Velure S9/1064 | 0.5 to 50 W | Treatment of chronic periodontitis | 980 nm, n.a. | [105,106] |
| A.R.C. Laser | Chirolas A.R.C. Laser | Up to 20 kW | Laser assisted frecnectomy | 980 nm, 8 kW/cm2 | [103,104] |
| Manufacturer | Model | Clinical Operation Ranges | Clinical Utility | Reference |
|---|---|---|---|---|
| Siemens | YSIO X.pree | Up to 150 KeV, 65 kW, 85 kW2 | Diagnosis and therapeutics | [107,108,109] |
| Varian | TrueBeam | 6 and 10 MeV | Radiation therapy for body tumors | [110,111] |
| Manufacturer | Model | Clinical Operating Energies | Clinical Utility | Reference |
|---|---|---|---|---|
| Elekta | Leksell Gamma Knife Perfexion | Co60 decay simultaneously produces combination of: one 315 keV photon, one 1.17 MeV γ-ray and and 1.33 MeV γ-rays | Treating brain tumors | [112,113] |
| Manufacturer | Model | Operation Ranges | Clinical Utility | Typical Dose Parameters | Reference |
|---|---|---|---|---|---|
| IBA (Belgium) | n.a. | 100 to 231 MeV | Treatment of central nervous system germ cell tumors | 30 to 55 Gy | NCT01049230 [114,115] |
| Mevion | S250 Proton Therapy System | 1 to 250 MeV | Treatment of intracranial tumors | 2 Gy fractions up to 400 Gy | [117,118] |
| Manufacturer | Model | Operation Ranges | Clinical Utility | Parameter Details | Reference |
|---|---|---|---|---|---|
| Holologic | Viera Portable Breast Ultrasound | 4 to 14 MHz | Ultrasound sonography of breast | 1 to 20 MHz waveform transmission | [116] |
| Chongqing HAIFU™ Company, Chongqing, China | Model-JC High-Intensity Focused Ultrasound (HIFU) system | 650 and 800 W | HIFU treatment of various solid tumors | No dose limit | [119] |
| Insightec, Haifa, Israel | ExAblate 4000 Type II Neurosystem | 620 to 720 kHz | Magnetic resonance (MR)-guided focused ultrasound System sonodynamic therapy of gliomas | 5 to 60 s pulse duration | NCT04845919 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, N.; Squire, J.; Guirguis, M.; Saha, D.; Hoyt, K.; Wang, K.K.-H.; Agarwal, V.; Obaid, G. Deep-Tissue Activation of Photonanomedicines: An Update and Clinical Perspectives. Cancers 2022, 14, 2004. https://doi.org/10.3390/cancers14082004
Shah N, Squire J, Guirguis M, Saha D, Hoyt K, Wang KK-H, Agarwal V, Obaid G. Deep-Tissue Activation of Photonanomedicines: An Update and Clinical Perspectives. Cancers. 2022; 14(8):2004. https://doi.org/10.3390/cancers14082004
Chicago/Turabian StyleShah, Nimit, John Squire, Mina Guirguis, Debabrata Saha, Kenneth Hoyt, Ken Kang-Hsin Wang, Vijay Agarwal, and Girgis Obaid. 2022. "Deep-Tissue Activation of Photonanomedicines: An Update and Clinical Perspectives" Cancers 14, no. 8: 2004. https://doi.org/10.3390/cancers14082004