
Reconstructive Surgery versus Primary Closure following Vulvar Cancer Excision: A Wide Single-Center Experience

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/21-Vulva-fact-sheet.pdf (accessed on 23 February 2022).
- Woelber, L.; Griebel, L.F.; Eulenburg, C.; Sehouli, J.; Jueckstock, J.; Hilpert, F.; de Gregorio, N.; Hasenburg, A.; Ignatov, A.; Hillemanns, P.; et al. Role of tumour-free margin distance for loco-regional control in vulvar cancer-a subset analysis of the Arbeitsgemeinschaft Gynäkologische Onkologie CaRE-1 multicenter study. Eur. J. Cancer 2016, 69, 180–188. [Google Scholar] [CrossRef] [PubMed]
- NCCN Guidelines Version 1.2022, Vulvar Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/vulvar.pdf (accessed on 23 February 2022).
- O'Brien, A.L.; Jadallah, E.; Chao, A.H. Reconstruction of a radical total vulvectomy defect with a single split anterolateral thigh perforator flap: A case report and review of the literature. Microsurgery 2021, 41, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Pavlov, A.; Bhatt, N.; Damitz, L.; Ogunleye, A.A. A Review of Reconstruction for Vulvar Cancer Surgery. Obstet. Gynecol. Surv. 2021, 76, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Confalonieri, P.L.; Gilardi, R.; Rovati, L.C.; Ceccherelli, A.; Lee, J.H.; Magni, S.; Del Bene, M.; Buda, A. Comparison of V-Y Advancement Flap Versus Lotus Petal Flap for Plastic Reconstruction After Surgery in Case of Vulvar Malignancies: A Retrospective Single Center Experience. Ann. Plast. Surg. 2017, 79, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Al-Benna, S.; Tzakas, E. Postablative reconstruction of vulvar defects with local fasciocutaneous flaps and superficial fascial system repair. Arch. Gynecol. Obstet. 2012, 286, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Gentileschi, S.; Servillo, M.; Garganese, G.; Fragomeni, S.; De Bonis, F.; Scambia, G.; Salgarello, M. Surgical therapy of vulvar cancer: How to choose the correct reconstruction? J. Gynecol. Oncol. 2016, 27, e60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- ASA House of Delegates. ASA Physical Status Classification System. 2014. Available online: https://www.asahq.org/resources/clinical-information/asa-physical-status-classification-system (accessed on 23 February 2022).
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynaecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef] [PubMed]
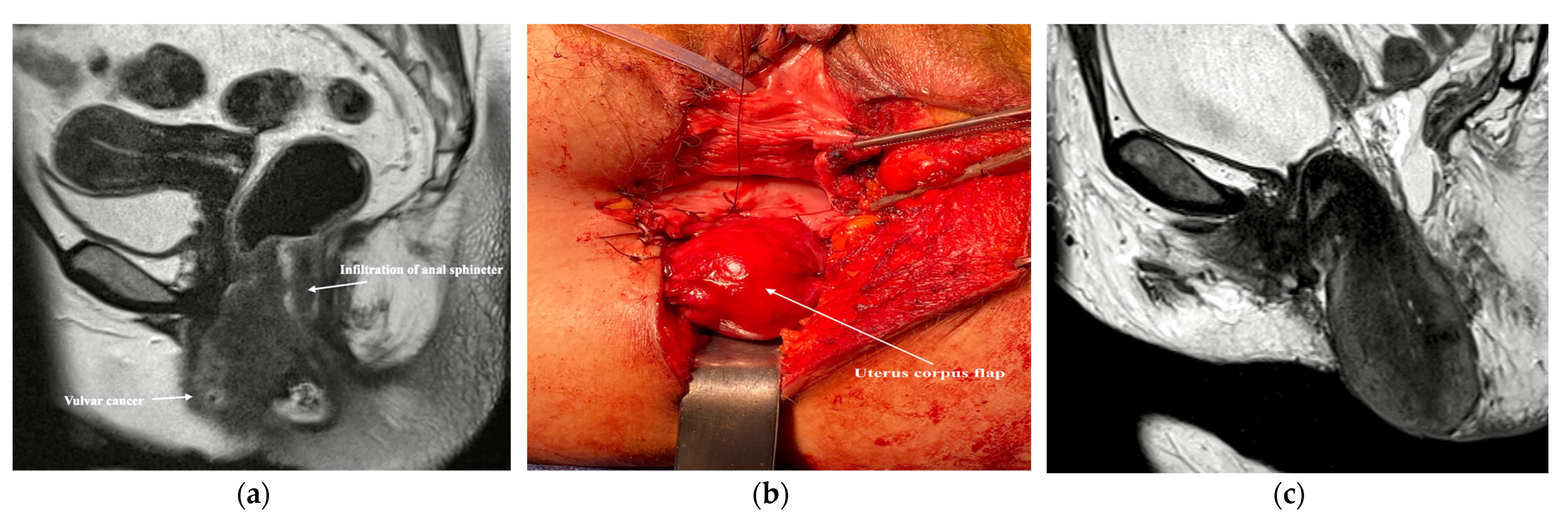
- Durai, R.; Harilingham, M.; Benziger, H. Uterine flap: A simple method to reconstruct perineal defect following extralevator abdominoperineal resection in women. Ann. R. Coll. Surg. Engl. 2013, 95, 442. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weikel, W.; Hofmann, M.; Steiner, E.; Knapstein, P.G.; Koelbl, H. Reconstructive surgery following resection of primary vulvar cancers. Gynecol. Oncol. 2005, 99, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Benedetti Panici, P.; Di Donato, V.; Bracchi, C.; Marchetti, C.; Tomao, F.; Palaia, I.; Perniola, G.; Muzii, L. Modified gluteal fold advancement V-Y flap for vulvar reconstruction after surgery for vulvar malignancies. Gynecol. Oncol. 2014, 132, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Landoni, F.; Proserpio, M.; Maneo, A.; Cormio, G.; Zanetta, G.; Milani, R. Repair of the perineal defect after radical vulvar surgery: Direct closure versus skin flaps reconstruction. A retrospective comparative study. Aust. N. Z. J. Obstet. Gynaecol. 1995, 35, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Aviki, E.M.; Esselen, K.M.; Barcia, S.M.; Nucci, M.R.; Horowitz, N.S.; Feltmate, C.M.; Berkowitz, R.S.; Orgill, D.G.; Viswanathan, A.N.; Muto, M.G. Does plastic surgical consultation improve the outcome of patients undergoing radical vulvectomy for squamous cell carcinoma of the vulva? Gynecol. Oncol. 2015, 137, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zeng, A.; Yang, J.; Cao, D.; Huang, H.; Wang, X.; You, Y.; Chen, J.; Lang, J.; Shen, K. Outcome of vulvar reconstruction by anterolateral thigh flap in patients with advanced and recurrent vulvar malignancy. J. Surg. Oncol. 2015, 111, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Gentileschi, S.; Caretto, A.A.; Servillo, M.; Stefanizzi, G.; Alberti, C.; Garganese, G.; Fragomeni, S.M.; Federico, A.; Tagliaferri, L.; Moroni, R.; et al. Feasibility, indications and complications of SCIP flap for reconstruction after extirpative surgery for vulvar cancer. Plast Reconstr. Aesthet. Surg. 2021, S1748-6815, 00549-0. [Google Scholar] [CrossRef]
- Gentileschi, S.; Servillo, M.; Garganese, G.; Simona, F.; Scambia, G.; Salgarello, M. Versatility of pedicled anterolateral thigh flap in gynecologic reconstruction after vulvar cancer extirpative surgery. Microsurgery 2017, 37, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Malandrone, F.; Bevilacqua, F.; Merola, M.; Gallio, N.; Ostacoli, L.; Carletto, S.; Benedetto, C. The Impact of Vulvar Cancer on Psychosocial and Sexual Functioning: A Literature Review. Cancers 2021, 14, 63. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.H.; Li, J.Q.; Shi, J.F.; Que, J.Y.; Liu, J.J.; Lappin, J.M.; Leung, J.; Ravindran, A.V.; Chen, W.Q.; Qiao, Y.L.; et al. Depression and anxiety in relation to cancer incidence and mortality: A systematic review and meta-analysis of cohort studies. Mol. Psychiatry 2020, 25, 1487–1499. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients n = 177(%) | Reconstructive Surgery (RS) n = 126 (%) | Primary Closure (PC) n = 51 (%) | p-Value | |
|---|---|---|---|---|---|
| Age at first diagnosis, median (range) years | 70 (28–91) | 71 (28–86) | 67 (35–91) | 0.604 | |
| Charlson’s comorbidity score | 0 | 109 (61.6%) | 84 (66.7%) | 25 (49%) | 0.043 |
| 1–3 | 49 (27.7%) | 32 (25.4%) | 17 (33.3%) | ||
| 4–6 | 17 (9.6%) | 9 (7.1%) | 8 (15.7%) | ||
| ≥7 | 2 (1.1%) | 1 (0.8%) | 1 (2%) | ||
| American Society of Anesthesiologists | ASA 1 | 19 (10.7%) | 12 (9.5%) | 7 (13.7%) | 0.582 |
| ASA 2 | 111 (62.7%) | 83 (65.9%) | 28 (54.9%) | ||
| ASA 3 | 47 (26.6%) | 31 (24.6%) | 16 (31.4%) | ||
| Histology | Keratinizing squamous | 138 (78%) | 97 (77%) | 41 (80.4%) | 0.768 |
| Non keratinizing squamous | 20 (11.3%) | 13 (10.3%) | 7 (13.7%) | ||
| Basaloid | 5 (2.8%) | 4 (3.2%) | 1 (2%) | ||
| Adenocarcinoma | 14 (7.9%) | 12 (9.5%) | 2 (3.9%) | ||
| Grading | G1 | 18 (10.2%) | 10 (7.9%) | 8 (15.7%) | |
| G2 | 117 (66.1%) | 81 (64.3%) | 36 (70.6%) | ||
| G3 | 32 (18.1%) | 26 (20.6%) | 6 (11.8%) | ||
| unknown | 10 (5.6%) | 9 (7.1%) | 1 (2%) | ||
| Tumor volume, median (range) mm | 31 (8–127) | 45 (20–127) | 23 (8–89) | 0.013 | |
| Characteristic | All Patients n = 177 (%) | Reconstructive Surgery (RS) n = 126 (%) | Primary Closure (PC) n = 51 (%) | p-Value | |
|---|---|---|---|---|---|
| Duration of surgery, median (range) minutes | 112 (20–335) | 134 (65–335) | 67 (20–280) | <0.001 | |
| Tumor free margins | 155 (87.8%) | 114 (90.4%) | 41 (80.4%) | 0.111 | |
| Wound healing disorders | 23 (13%) | 16 (12.7%) | 7 (13.7%) | 1.000 | |
| Type of demolitive surgery | Radical vulvectomy | 32 (18.1%) | 24 (19%) | 8 (15.7%) | 0.584 |
| Anterior vulvar resection | 78 (44.1%) | 66 (52.4%) | 12 (23.5%) | 0.001 | |
| Posterior vulvar resection | 22 (12.4%) | 17 (13.5%) | 5 (9.8%) | ||
| Hemivulvectomy left | 15 (8.5%) | 9 (7.1%) | 6 (11.8%) | ||
| Hemivulvectomy right | 12 (6.8%) | 6 (4.8%) | 6 (11.8%) | ||
| Wide excision | 14 (7.9%) | 0 (0%) | 14 (27.5%) | ||
| Exentration | 4 (2.3%) | 4 (3.2%) | 0 (0%) | ||
| Clitoris resection | 115 (65%) | 93 (73.8%) | 22 (43.1%) | 0.000 | |
| Partial or total resection of urethra | 37 (20.9%) | 32 (25.4%) | 5 (9.8%) | 0.035 | |
| Partial or total resection of anus | 14 (7.9%) | 14 (11.1%) | 0 (0%) | ||
| Sentinel lymph node staging only | 100 (56.5%) | 74 (58.7%) | 26 (50.1%) | ||
| Inguinal lymph node dissection | 73 (41.2%) | 52 (41.3%) | 21 (41.2%) | ||
| Type of reconstructive surgery | Fasciocutaneous V-Y flap | - | 54 (42.9%) | - | |
| Anterior pedicle labial flap | - | 8 (6.3%) | - | ||
| Posterior pedicle labial flap | - | 11 (8.7%) | - | ||
| Limberg flap | - | 9 (7.1%) | - | ||
| Myocutaneous flaps | - | 20 (15.9%) | - | ||
| Flap combination | - | 22 (17.5%) | - | ||
| Corpus uteri flap | - | 2 (1.6%) | - | ||
| FIGO | IA | 21 (11.9%) | 12 (9.5%) | 9 (17.6%) | |
| IB | 79 (44.6%) | 57 (45.2%) | 22 (43.1%) | ||
| II | 23 (13%) | 18 (14.3%) | 5 (9.8%) | ||
| IIIA | 22 (12.4%) | 16 (12.7%) | 6 (11.8%) | ||
| IIIB | 14 (7.9%) | 12 (9.5%) | 2 (3.9%) | ||
| IIIC | 7 (4%) | 4 (3.2%) | 3 (5.9%) | ||
| IVA | 9 (5.1%) | 5 (4%) | 4 (7.8%) | ||
| IVB | 2 (1.1%) | 2 (1.6%) | - | ||
| Lymph node (LN) status | Not involved | 127 (71.8%) | 94 (74.6%) | 33 (64.7%) | 0.255 |
| 1-2 LN with <5 mm | 21 (11.9%) | 13 (10.3%) | 8 (15.7%) | ||
| >5 mm or >2 LNs or extra capsular infiltration | 25 (14.1%) | 19 (15.1%) | 6 (11.8%) | ||
| No staging | 4 (2.3%) | 0 (0%) | 4 (7.8%) | ||
| Further therapy (Radio-/radiochemotherapy) | 32 (18.1%) | 23 (18.3%) | 9 (17.6%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muallem, M.Z.; Sehouli, J.; Miranda, A.; Plett, H.; Sayasneh, A.; Diab, Y.; Muallem, J.; Hatoum, I. Reconstructive Surgery versus Primary Closure following Vulvar Cancer Excision: A Wide Single-Center Experience. Cancers 2022, 14, 1695. https://doi.org/10.3390/cancers14071695
Muallem MZ, Sehouli J, Miranda A, Plett H, Sayasneh A, Diab Y, Muallem J, Hatoum I. Reconstructive Surgery versus Primary Closure following Vulvar Cancer Excision: A Wide Single-Center Experience. Cancers. 2022; 14(7):1695. https://doi.org/10.3390/cancers14071695
Chicago/Turabian StyleMuallem, Mustafa Zelal, Jalid Sehouli, Andrea Miranda, Helmut Plett, Ahmad Sayasneh, Yasser Diab, Jumana Muallem, and Imad Hatoum. 2022. "Reconstructive Surgery versus Primary Closure following Vulvar Cancer Excision: A Wide Single-Center Experience" Cancers 14, no. 7: 1695. https://doi.org/10.3390/cancers14071695