
Efficacy and Safety of Trans-Arterial Yttrium-90 Radioembolization in Patients with Unresectable Liver-Dominant Metastatic or Primary Hepatic Soft Tissue Sarcomas

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. TARE Procedure
2.3. Evaluation of Response
2.4. Evaluation of Toxicity
2.5. Statistical Analysis
3. Results
3.1. Patient Baseline Characteristics
3.2. Treatment
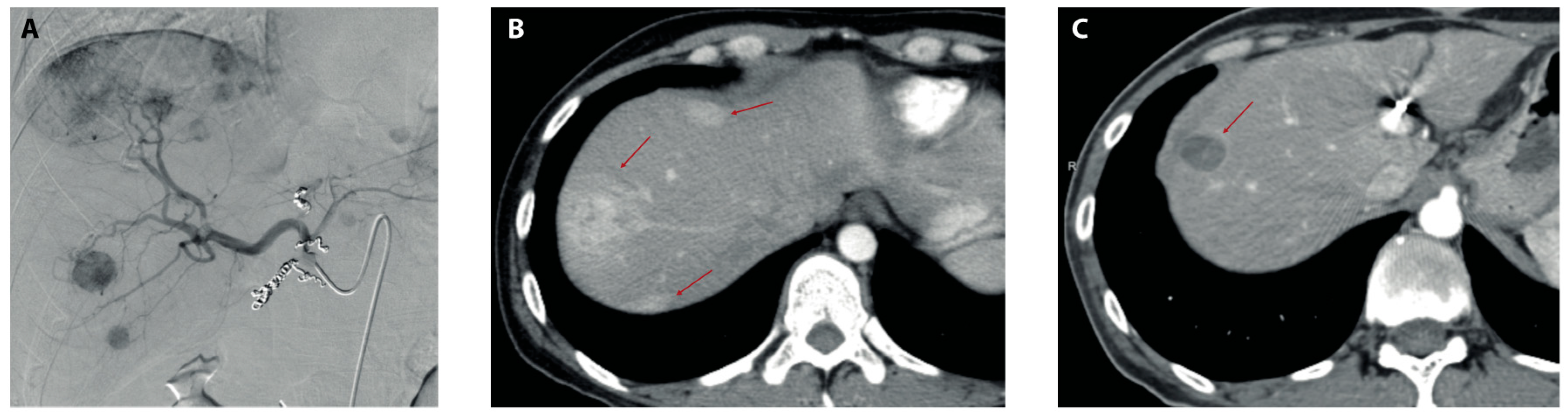
3.3. Radiologic Tumor Response and Follow-Up
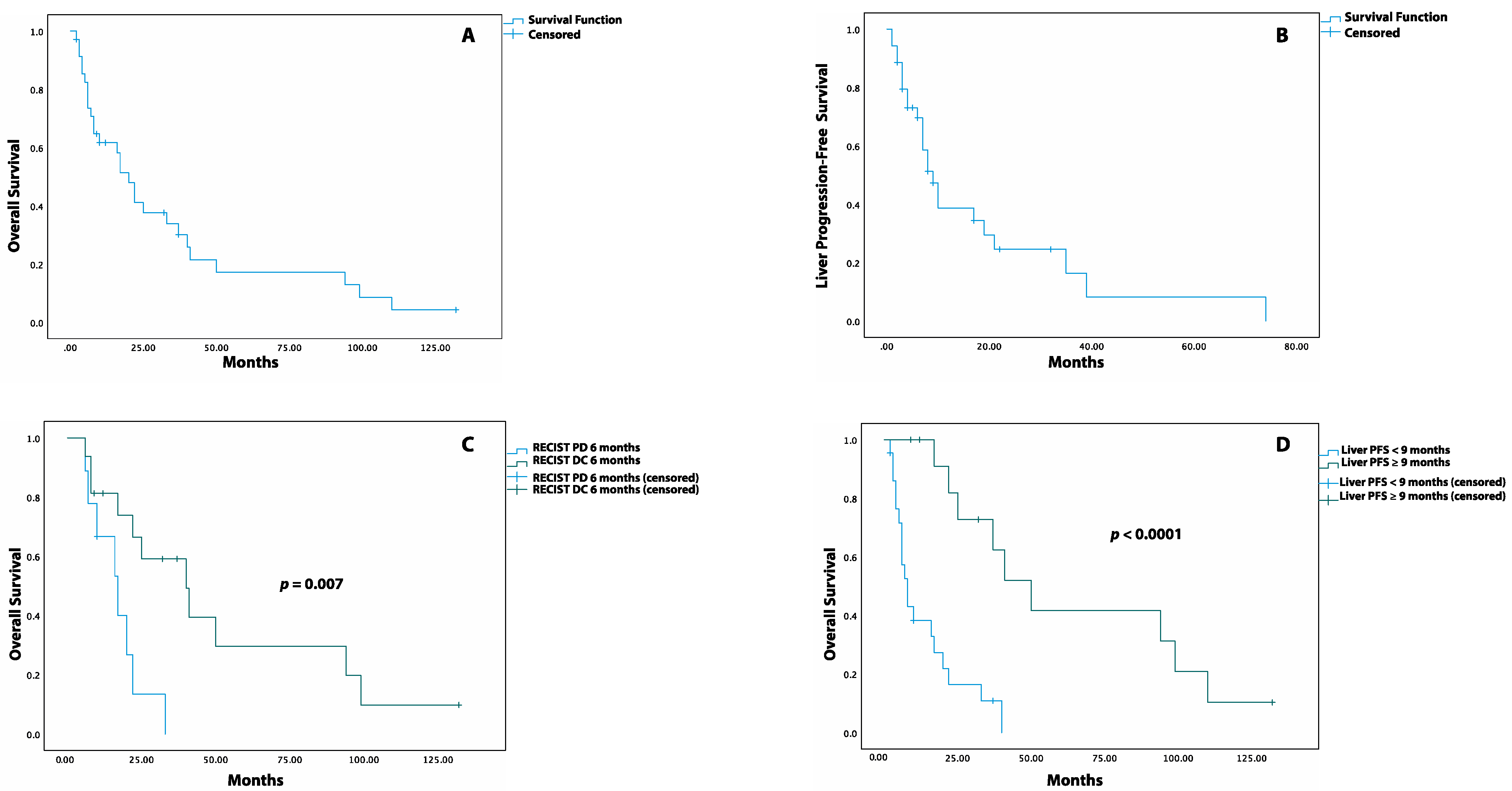
3.4. Overall Survival and Liver Progression-Free Survival
3.5. The Impact of Pre-TARE and Post-TARE Therapy on OS and LPFS
3.6. Multivariate Analysis
3.7. Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Borker, R.; Ewing, J.; Tseng, W.-Y.; Hackshaw, M.D.; Saravanan, S.; Dhanda, R.; Nadler, E. Epidemiology, Treatment Patterns, and Outcomes of Metastatic Soft Tissue Sarcoma in a Community-Based Oncology Network. Sarcoma 2014, 2014, 145764. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, W., Jr.; Donegan, W.L.; Natarajan, N.; Mettlin, C.; Beart, R.; Winchester, D. Adult soft tissue sarcomas. A pattern of care survey of the American College of Surgeons. Ann. Surg. 1987, 205, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.G.; Memos, N.; Thomas, J.M.; Smith, M.J.F.; Strauss, D.C.; Hayes, A.J. Patterns of disease relapse in primary extremity soft-tissue sarcoma. BJS 2016, 103, 1487–1496. [Google Scholar] [CrossRef]
- Christie-Large, M.; James, S.L.; Tiessen, L.; Davies, A.M.; Grimer, R.J. Imaging strategy for detecting lung metastases at presen-tation in patients with soft tissue sarcomas. Eur. J. Cancer 2008, 44, 1841–1845. [Google Scholar] [PubMed]
- Marudanayagam, R.; Sandhu, B.; Perera, M.T.; Bramhall, S.R.; Mayer, D.; Buckels, J.A.; Mirza, D.F. Liver resection for metastatic soft tissue sarcoma: An analysis of prognostic factors. Eur. J. Surg. Oncol. 2011, 37, 87–92. [Google Scholar] [PubMed] [Green Version]
- Jaques, D.P.; Coit, D.G.; Casper, E.S.; Brennan, M.F. Hepatic Metastases from Soft-Tissue Sarcoma. Ann. Surg. 1995, 221, 392–397. [Google Scholar] [CrossRef]
- Okamoto, M.; Matsuoka, M.; Soma, T.; Arai, R.; Kato, H.; Harabayashi, T.; Adachi, H.; Shinohara, T.; Sagawa, T.; Nishiyama, N.; et al. Metastases of soft tissue sarcoma to the liver: A Historical Cohort Study from a Hospital-based Cancer Registry. Cancer Med. 2020, 9, 6159–6165. [Google Scholar] [CrossRef]
- Almogy, G.; Lieberman, S.; Gips, M.; Pappo, O.; Edden, Y.; Jurim, O.; Slasky, B.S.; Uzieli, B.; Eid, A. Clinical outcomes of surgical resections for primary liver sarcoma in adults: Results from a single centre. Eur. J. Surg. Oncol. 2004, 30, 421–427. [Google Scholar] [CrossRef]
- Martins, A.C.D.A.; Neto, D.C.D.C.; E Silva, J.D.D.-M.; Moraes, Y.M.; Leão, C.S.; Martins, C. Adult primary liver sarcoma: Systematic review. Rev. Colégio Bras. Cir. 2020, 47, e20202647. [Google Scholar] [CrossRef]
- Grimme, F.A.B.; Seesing, M.F.J.; van Hillegersberg, R.; van Coevorden, F.; de Jong, K.P.; Nagtegaal, I.D.; Verhoef, C.; de Wilt, J.H.W. Liver Resection for Hepatic Metastases from Soft Tissue Sarcoma: A Nationwide Study. Dig. Surg. 2019, 36, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Pruitt, A.; Nicol, T.L.; Gorgulu, S.; Choti, M.A. Complete hepatic resection of metastases from leiomyosarcoma pro-longs survival. J. Gastrointest. Surg. 1998, 2, 151–155. [Google Scholar]
- Maluccio, M.A.; Covey, A.M.; Schubert, J.; Brody, L.A.; Sofocleous, C.T.; Getrajdman, G.I.; DeMatteo, R.; Brown, K.T. Treatment of metastatic sarcoma to the liver with bland embolization. Cancer 2006, 107, 1617–1623. [Google Scholar] [CrossRef]
- Weitz, J.; Klimstra, D.S.; Cymes, K.; Jarnagin, W.R.; D’Angelica, M.; La Quaglia, M.P.; Fong, Y.; Brennan, M.F.; Blumgart, L.H.; DeMatteo, R.P. Management of primary liver sarcomas. Cancer 2007, 109, 1391–1396. [Google Scholar] [CrossRef]
- Ratan, R.; Patel, S.R. Chemotherapy for soft tissue sarcoma. Cancer 2016, 122, 2952–2960. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Huang, H.Z.; Zhou, M.T.; Han, S.L. Surgical Treatment and Chemotherapy of Adult Primary Liver Sarcoma: Experi-ences from a Single Hospital in China. Dig. Surg. 2019, 36, 46–52. [Google Scholar]
- Zheng, Y.-W.; Zhang, X.-W.; Zhang, J.-L.; Hui, Z.-Z.; Du, W.-J.; Li, R.-M.; Ren, X.-B. Primary hepatic angiosarcoma and potential treatment options. J. Gastroenterol. Hepatol. 2014, 29, 906–911. [Google Scholar] [CrossRef] [Green Version]
- Salem, R.; Gordon, A.C.; Mouli, S.; Hickey, R.; Kallini, J.; Gabr, A.; Mulcahy, M.F.; Baker, T.; Abecassis, M.; Miller, F.H.; et al. Y90 Ra-dioembolization Significantly Prolongs Time to Progression Compared With Chemoembolization in Patients with Hepatocellular Carcinoma. Gastroenterology 2016, 151, 1155–1163.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.D.; Sze, D.Y.; Padia, S.A.; Lewandowski, R.J.; Salem, R.; Mpofu, P.; Haste, P.M.; Johnson, M.S. Response and Overall Survival for Yttrium-90 Radioembolization of Hepatic Sarcoma: A Multicenter Retrospective Study. J. Vasc. Interv. Radiol. 2018, 29, 867–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Guindalini, F.D.; Botelho, M.P.F.; Harmath, C.B.; Sandrasegaran, K.; Miller, F.H.; Salem, R.; Yaghmai, V. Assessment of Liver Tumor Response to Therapy: Role of Quantitative Imaging. Radiographics 2013, 33, 1781–1800. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (CTCAE—Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermo-Sifiliográficas 2020, 112, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Kromrey, M.L.; Ittermann, T.; vWahsen, C.; Plodeck, V.; Seppelt, D.; Hoffmann, R.T.; Heiss, P.; Kühn, J.P. Reference values of liver volume in Caucasian population and factors influencing liver size. Eur. J. Radiol. 2018, 106, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.P.; Cohalan, C.; Kopek, N.; Enger, S.A. A guide to 90Y radioembolization and its dosimetry. Phys. Med. 2019, 68, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Gil-Alzugaray, B.; Rodriguez, J.; Sola, I.; Martinez-Cuesta, A.; Viudez, A.; Chopitea, A.; Iñarrairaegui, M.; Arbizu, J.; Bilbao, J.I. Liver disease induced by radioembolization of liver tumors: Description and possible risk factors. Cancer 2008, 112, 1538–1546. [Google Scholar] [CrossRef]
- Murthy, R.; Brown, D.B.; Salem, R.; Meranze, S.G.; Coldwell, D.M.; Krishnan, S.; Nunez, R.; Habbu, A.; Liu, D.; Ross, W.; et al. Gastro-intestinal complications associated with hepatic arterial Yttrium-90 microsphere therapy. J. Vasc. Interv. Radiol. 2007, 18, 553–562. [Google Scholar] [CrossRef]
- Llovet, J.M.; Real, M.I.; Montaña, X.; Planas, R.; Coll, S.; Aponte, J.; Ayuso, C.; Sala, M.; Muchart, J.; Solà, R.; et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: A randomised controlled trial. Lancet 2002, 359, 1734–1739. [Google Scholar] [CrossRef]
- Boehm, L.M.; Jayakrishnan, T.T.; Miura, J.T.; Zacharias, A.J.; Johnston, F.; Turaga, K.; Gamblin, T.C. Comparative effectiveness of hepatic artery based therapies for unresectable intrahepatic cholangiocarcinoma. J. Surg. Oncol. 2015, 111, 213–220. [Google Scholar] [CrossRef]
- Bester, L.; Meteling, B.; Boshell, D.; Saxena, A.; Morris, D.L. Current role of transarterial chemoembolization and radioembo-lization in the treatment of metastatic colorectal cancer. Hepat.Oncol. 2014, 1, 215–228. [Google Scholar] [CrossRef]
- Kennedy, A.; Bester, L.; Salem, R.; Sharma, R.A.; Parks, R.W.; Ruszniewski, P. Role of hepatic intra-arterial therapies in metastatic neuroendocrine tumours (NET): Guidelines from the NET-Liver-Metastases Consensus Conference. HPB 2015, 17, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapiro, J.; Duran, R.; Lin, M.; Mungo, B.; Schlachter, T.; Schernthaner, R.; Gorodetski, B.; Wang, Z.; Geschwind, J.F. Transarterial chemoembolization in soft-tissue sarcoma metastases to the liver—The use of imaging biomarkers as predictors of patient survival. Eur. J. Radiol. 2015, 84, 424–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajan, D.K.; Soulen, M.C.; Clark, T.W.; Baum, R.A.; Haskal, Z.J.; Shlansky-Goldberg, R.; Freiman, D.B. Sarcomas Metastatic to the Liver: Response and Survival after Cisplatin, Doxorubicin, Mitomycin-C, Ethiodol, and Polyvinyl Alcohol Chemoembolization. J. Vasc. Interv. Radiol. 2001, 12, 187–193. [Google Scholar] [CrossRef]
- Krzyston, H.; Morse, B.; Deperalta, D.; Rishi, A.; Kayaleh, R.; El-Haddad, G.; Smith, J.; Druta, M.; Kis, B. Liver-directed treatments of liver-dominant metastatic leiomyosarcoma. Diagn. Interv. Radiol. 2020, 26, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Pierce, D.B.; Johnson, G.E.; Monroe, E.; Loggers, E.T.; Jones, R.L.; Pollack, S.M.; Padia, S.A. Safety and Efficacy Outcomes of Embolization in Hepatic Sarcomas. Am. J. Roentgenol. 2018, 210, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Aguado, A.; Dunn, S.P.; Averill, L.W.; Chikwava, K.R.; Gresh, R.; Rabinowitz, D.; Katzenstein, H.M. Successful use of transarterial radioembolization with yttrium-90 (TARE-Y90) in two children with hepatoblastoma. Pediatr. Blood Cancer 2020, 67, e28421. [Google Scholar] [CrossRef]
- Orue-Echebarria, M.I.; Garciafília, L.; Rodriguez-Bachiller, L.; Díaz-Zorita, B.; Velasco, E.; Ramón, E.; Agra, C.; Rodríguez, A.C. Solitary extrapleural fibrous tumor with hepatic bilobar metastases: Multimodal approach treatment. Clin. Sarcoma. Res. 2020, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Y.; Ji, H.; Zhao, X.; Lu, H. Transarterial Y90 radioembolization versus chemoembolization for patients with hepatocellular carcinoma: A meta-analysis. Biosci. Trends 2015, 9, 289–298. [Google Scholar] [CrossRef] [Green Version]
- Memon, K.; Kulik, L.; Lewandowski, R.J.; Wang, E.; Riaz, A.; Ryu, R.K.; Sato, K.T.; Marshall, K.; Gupta, R.; Nikolaidis, P.; et al. Radio-graphic response to locoregional therapy in hepatocellular carcinoma predicts patient survival times. Gastroenterology 2011, 141, 526–535.e5352. [Google Scholar] [CrossRef]
- Kucuk, O.N.; Soydal, C.; Lacin, S.; Ozkan, E.; Bilgic, S. Selective intraarterial radionuclide therapy with Yttrium-90 (Y-90) mi-crospheres for unresectable primary and metastatic liver tumors. World J. Surg. Oncol. 2011, 9, 86. [Google Scholar] [CrossRef] [Green Version]
- Wasan, H.S.; Gibbs, P.; Sharma, N.K.; Taieb, J.; Heinemann, V.; Ricke, J.; Peeters, M.; Findlay, M.; Weaver, A.; Mills, J.; et al. First-line selective internal radiotherapy plus chemotherapy versus chemotherapy alone in patients with liver metastases from colorectal cancer (FOXFIRE, SIRFLOX, and FOXFIRE-Global): A combined analysis of three multicentre, randomised, phase 3 trials. Lancet Oncol. 2017, 18, 1159–1171. [Google Scholar] [CrossRef] [Green Version]
- Chauhan, N.; Mulcahy, M.F.; Salem, R.; Iii, A.B.B.; Boucher, E.; Bukovcan, J.; Cosgrove, D.; LaFramboise, C.; Lewandowski, R.J.; Master, F.; et al. TheraSphere Yttrium-90 Glass Microspheres Combined with Chemotherapy Versus Chemotherapy Alone in Second-Line Treatment of Patients With Metastatic Colorectal Carcinoma of the Liver: Protocol for the EPOCH Phase 3 Randomized Clinical Trial. JMIR Res. Protoc. 2019, 8, e11545. [Google Scholar] [CrossRef]
- Pieper, C.C.; Meyer, C.; Wilhelm, K.E.; Block, W.; Nadal, J.; Ahmadzadehfar, H.; Willinek, W.A.; Schild, H.H. Yttrium-90 Radio-embolization of Advanced, Unresectable Breast Cancer Liver Metastases-A Single-Center Experience. J. Vasc. Interv. Radiol. 2016, 27, 1305–1315. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, M.A.; Wongjarupong, N.; Hassan, M.A.; Taha, W.; Abdalla, A.; Bampoh, S.; Onyirioha, K.; Nelson, M.; Glubranson, L.A.; Wiseman, G.A.; et al. The efficacy, safety, and predictors of outcomes oftransarterial radioembolization for hepatocellular carcinoma: A retrospective study. Expert. Rev. Gastroenterol. Hepatol. 2020, 14, 619–629. [Google Scholar] [CrossRef]
- Kayaleh, R.; Krzyston, H.; Rishi, A.; Naziri, J.; Frakes, J.; Choi, J.; El-Haddad, G.; Parikh, N.; Sweeney, J.; Kis, B. Transarterial Radioembolization Treatment of Pancreatic Cancer Patients with Liver-Dominant Metastatic Disease Using Yttrium-90 Glass Microspheres: A Single-Institution Retrospective Study. J. Vasc. Interv. Radiol. 2020, 31, 1060–1068. [Google Scholar] [CrossRef]
- Titano, J.J.; Kim, E.; Patel, R.S. Yttrium-90 Complications: Prevention and Management. Tech. Vasc. Interv. Radiol. 2019, 22, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.L.; Vallow, L.A.; Johnson, D.W.; Heckman, M.G.; Diehl, N.N.; Smith, A.A.; Tzou, K.S.; Paz-Fumagalli, R.; Kim, S.; Ko, S.J.; et al. Complications after 90Y microsphere radioembolization for unresectable hepatic tumors: An evaluation of 112 patients. Brachytherapy 2013, 12, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Gil-Alzugaray, B.; Chopitea, A.; Iñarrairaegui, M.; Bilbao, J.I.; Rodriguez-Fraile, M.; Rodriguez, J.; Benito, A.; Dominguez, I.; D’Avola, D.; Herrero, J.I.; et al. Prognostic factors and prevention of radioembolization-induced liver disease. Hepatology 2013, 57, 1078–1087. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristic | Number (%) |
|---|---|
| Age at TARE | |
| Median Range | 58 (24–83) |
| Sex | |
| Male Female | 14 (40%) 21 (60%) |
| Baseline ECOG Performance Status | |
| 0 1 2 | 16 (45.7%) 13 (37.2%) 6 (17.1%) |
| Primary Site | |
| Retroperitoneum Liver Uterus Extremities Lung Stomach Other | 9 (25.7%) 7 (20%) 4 (11.4%) 3 (8.6%) 2 (5.7%) 2 (5.7%) 8 (22.9%) |
| Histotype | |
| Leiomyosarcoma Spindle Cell Sarcoma Hemangiopericytoma Hepatic Epithelioid Hemangioendothelioma Gastro-Intestinal Stromal Tumor Angiosarcoma Rhabdomyosarcoma Liposarcoma | 20 (57.1%) 4 (11.4%) 3 (8.6%) 2 (5.7%) 2 (5.7%) 2 (5.7%) 1 (2.9%) 1 (2.9%) |
| Baseline MELD | |
| Median Range | 8 (6–19) |
| Baseline Child-Turcotte-Pugh Class | |
| Class A Class B | 27 (77.1%) 8 (22.9%) |
| Baseline ALBI grade | |
| Grade 1 Grade 2–3 | 13 (37.1%) 22 (62.9%) |
| Primary Metastases | |
| Yes No | 16 (45.7%) 19 (54.3%) |
| Extrahepatic Disease | |
| Yes No | 22 (62.9%) 13 (37.1%) |
| Chemotherapy Pre-TARE | |
| Yes No | 27 (77.1%) 8 (22.9%) |
| Liver Surgery Pre-TARE | |
| Yes No | 9 (25.7%) 26 (74.3%) |
| Radiotherapy Pre-TARE | |
| Yes No | 16 (45.7%) 19 (54.3%) |
| Liver Involvement | |
| Bilobar Single lobe | 29 (82.8%) 6 (17.1%) |
| Baseline Liver Volume | |
| 1.5 L 1.5 L | 25 (71.4%) 10 (28.6%) |
| Radiologic Tumor Response | RECIST | mRECIST | p-Value (χ2) |
|---|---|---|---|
| 3 months post-TARE | |||
| DC (CR + PR + SD) | 73.3% (22/30) | 80.0% (24/30) | 0.54 |
| ORR (CR + PR) | 13.3% (4/30) | 56.7% (17/30) | 0.0004 |
| PD | 26.7% (8/30) | 20.0% (6/30) | |
| 6 months post-TARE | |||
| DC (CR + PR + SD) | 64.0% (16/25) | 68.0% (17/25) | 0.76 |
| ORR (CR + PR) | 20.0% (5/25) | 52.0% (13/25) | 0.02 |
| PD | 36.0% (9/25) | 32.0% (8/25) | |
| 9 months post-TARE | |||
| DC (CR + PR + SD) | 40.0% (6/15) | 46.7% (7/15) | 0.46 |
| ORR (CR + PR) | 13.3% (2/15) | 40.0% (6/15) | 0.09 |
| PD | 60.0% (9/15) | 53.3% (8/15) |
| Variables | Number (%) | Kaplan–Meier Median OS (Months, 95%CI) | p-Value (Log-Rank) | Cox Proportional Hazards Hazard Ratio (95%CI) | p-Value (Cox) |
|---|---|---|---|---|---|
| RECIST response 3 months | |||||
| DC PD | 22 (62.8%) 8 (22.8%) | 22 (10.9–33.1) 10 (0.0–21.9) | 0.053 | 0.41 (0.16–1.1) | 0.065 |
| RECIST response 6 months | |||||
| DC PD | 16 (45.7%) 9 (25.7%) | 40 (17.6–62.4) 17 (8.1–25.9) | 0.007 | 0.25 (0.08–0.75) | 0.013 |
| RECIST response 9 months | |||||
| DC PD | 6 (17.1%) 9 (25.7%) | 94 (0.0–242.1) 37 (26.7–47.3) | 0.290 | 0.47 (0.1–1.9) | 0.299 |
| Liver PFS | |||||
| 9 months 9 months | 13 (37.1%) 22 (62.9%) | 50 (30.8–69.1) 8 (5.0–10.9) | <0.0001 | 0.14 (0.04–0.4) | <0.0001 |
| TACE post-TARE | |||||
| Yes No | 6 (17.1%) 29 (82.9%) | 99 (90.9–107.0) 16 (4.9–27.0) | 0.003 | 0.14 (0.03–0.6) | 0.009 |
| Repeat TARE | |||||
| Yes No | 5 (14.3%) 30 (85.7%) | 33 (3.7–30.3) 17 (4.9–27.0) | 0.517 | 0.73 (0.3–1.9) | 0.524 |
| Primary Metastases | |||||
| Yes No | 16 (45.7%) 19 (54.3%) | 17 (11.1–22.9) 22 (0.0–57.5) | 0.173 | 1.8 (0.8–4.1) | 0.185 |
| Extrahepatic Metastases | |||||
| Yes No | 22 (62.8%) 13 (37.2%) | 17 (1.6–32.4) 37 (4.6–69.4) | 0.186 | 1.7 (0.8–3.8) | 0.197 |
| Liver Involvement | |||||
| Bilobar Single lobe | 29 (82.8%) 6 (17.1%) | 22 (7.9–35.6) 16 (0.0–35.6) | 0.348 | 0.6 (0.2–1.7) | 0.359 |
| Baseline Liver Volume | |||||
| 1.5 L 1.5 L | 25 (71.4%) 10 (28.6%) | 17 (2.0–32.0) 20 (0.0–49.3) | 0.474 | 1.3 (0.6–3.0) | 0.481 |
| Child-Turcotte-Pugh Class | |||||
| B A | 8 (22.9%) 27 (77.1%) | 6 (4.7–7.3) 22 (13.1–30.9) | 0.018 | 2.6 (1.1–6.2) | 0.025 |
| Baseline MELD | |||||
| 9 9 | 8 (22.9%) 27 (77.1%) | 33 (0.0–91.1) 17 (11.2–22.8) | 0.668 | 1.2 (0.5–2.9) | 0.673 |
| Baseline ALBI grade | |||||
| Grade 2–3 Grade 1 | 22 (62.9%) 13 (37.1%) | 16 (2.6–29.4) 33 (10.4–55.6) | 0.308 | 1.5 (0.7–3.4) | 0.318 |
| Chemotherapy Post-TARE | |||||
| Yes No | 22 (62.9%) 13 (37.1%) | 17 (1.9–32.1) 22 (13.7–30.3) | 0.773 | 1.1 (0.5–2.4) | 0.776 |
| Chemotherapy Pre-TARE | |||||
| Yes No | 27 (77.1%) 8 (22.9%) | 17 (3.1–30.9) 33 (9.6–56.4) | 0.619 | 1.2 (0.5–3.2) | 0.624 |
| Liver Surgery Pre-TARE | |||||
| Yes No | 9 (25.7%) 26 (74.3%) | 20 (11.2–28.8) 22 (3.3–40.7) | 0.851 | 0.92 (0.41–2.1) | 0.853 |
| Radiotherapy Pre-TARE | |||||
| Yes No | 16 (45.7%) 19 (54.3%) | 8 (6.1–9.9) 25 (3.5–46.5) | 0.244 | 1.5 (0.73–3.3) | 0.254 |
| Liver-directed therapy Pre-TARE | |||||
| Yes No | 3 (8.6%) 32 (91.4%) | 37 (3.4–70.6) 20 (8.7–31.3) | 0.598 | 0.68 (0.16–2.9) | 0.606 |
| Type of Y90 Microspheres | |||||
| Resin (SIR) Glass (Theraspheres) | 31 (88.6%) 4 (11.4%) | 20 (13.0–26.9) 17 (0.0–46.4) | 0.631 | 0.77 (0.3–2.3) | 0.637 |
| TARE Distribution | |||||
| Bilobar Single Lobe/Segmental | 22 (62.8%) 13 (37.2%) | 22 (10.9–33.1) 16 (0.5–31.6) | 0.181 | 0.57 (0.25–1.3) | 0.193 |
| Baseline ECOG | |||||
| 2 0–1 | 6 (17.2%) 29 (82.8%) | 6 (0.0–12.3) 22 (14.2–29.8) | 0.042 | 2.7 (0.9–7.2) | 0.054 |
| Histotype | |||||
| Leiomyosarcoma Other | 20 (57.1%) 15 (42.9%) | 20 (8.1–31.9) 16 (0.0–53.6) | 0.405 | 0.71 (0.3–1.6) | 0.413 |
| Variables | Number (%) | Kaplan–Meier Median LPFS (Months, 95%CI) | p-Value (Log-Rank) | Cox Proportional Hazards Hazard Ration (95%CI) | p-Value (Cox) |
|---|---|---|---|---|---|
| Primary Metastases | |||||
| Yes No | 16 (45.7%) 19 (54.3%) | 7 (3.4–10.6) 19 (4.1–33.9) | 0.036 | 2.5 (1.1–6.2) | 0.048 |
| Extrahepatic Metastases | |||||
| Yes No | 22 (62.8%) 13 (37.2%) | 8 (3.5–12.5) 9 (5.8–12.2) | 0.748 | 1.1 (0.5–2.7) | 0.754 |
| Liver Involvement | |||||
| Bilobar Single lobe | 29 (82.8%) 6 (17.1%) | 9 (6.4–11.6) 4 (1.9–6.1) | 0.815 | 0.9 (0.3–2.7) | 0.818 |
| Baseline Liver Volume | |||||
| 1.5 L 1.5 L | 25 (71.4%) 10 (28.6%) | 10 (7.6–12.4) 7 (0.8–13.2) | 0.838 | 1.1 (0.4–2.9) | 0.842 |
| Child-Turcotte-Pugh Class | |||||
| B A | 8 (22.9%) 27 (77.1%) | 39 (N/A) 9 (6.3–11.7) | 0.892 | 1.1 (0.3–3.3) | 0.894 |
| Baseline MELD | |||||
| 9 9 | 8 (22.9%) 27 (77.1%) | 9 (0.0–18.8) 8 (4.9–11.1) | 0.984 | 1.0 (0.4–2.8) | 0.984 |
| Baseline ALBI grade | |||||
| Grade 2–3 Grade 1 | 22 (62.9%) 13 (37.1%) | 8 (4.4–11.6) 10 (6.1–13.9) | 0.508 | 0.8 (0.3–1.8) | 0.521 |
| Interim Chemotherapy | |||||
| Yes No | 14 (40%) 21 (60%) | 8 (6.5–9.5) 10 (0.0–22.5) | 0.463 | 1.4 (0.6–3.3) | 0.477 |
| Chemotherapy Pre-TARE | |||||
| Yes No | 27 (77.1%) 8 (22.9%) | 9 (6.1–11.9) 8 (0.0–37.8) | 0.416 | 1.5 (0.5–4.2) | 0.429 |
| Liver Surgery Pre-TARE | |||||
| Yes No | 9 (25.7%) 26 (74.3%) | 10 (0.0–24.6) 9 (6.2–11.8) | 0.595 | 1.3 (0.5–3.1) | 0.606 |
| Radiotherapy Pre-TARE | |||||
| Yes No | 16 (45.7%) 19 (54.3%) | 8 (4.9–11.0) 10 (4.7–15.4) | 0.713 | 0.8 (0.4–1.9) | 0.720 |
| Liver-directed therapy Pre-TARE | |||||
| Yes No | 3 (8.6%) 32 (91.4%) | 8 (1.6–14.4) 10 (5.7–14.3) | 0.248 | 2.0 (0.6–7.1) | 0.272 |
| Type of Y90 Microspheres | |||||
| Resin (SIR) Glass (Theraspheres) | 31 (88.6%) 4 (11.4%) | 9 (6.4–11.6) 7 (2.2–11.8) | 0.911 | 1.1 (0.3–3.8) | 0.913 |
| TARE Distribution | |||||
| Bilobar Single Lobe/Segmental | 22 (62.8%) 13 (37.2%) | 10 (7.4–12.6) 8 (2.9–13.1) | 0.848 | 0.9 (0.3–2.2) | 0.852 |
| Baseline ECOG | |||||
| 2 0–1 | 6 (17.2%) 29 (82.8%) | 8 (N/A) 10 (7.1–10.8) | 0.148 | 2.5 (0.7–9.1) | 0.173 |
| Histotype | |||||
| Leiomyosarcoma Other | 20 (57.1%) 15 (42.9%) | 8 (6.4–9.6) 10 (0.0–22.6) | 0.320 | 0.6 (0.3–1.6) | 0.337 |
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Liver PFS | |||
| 9 months | 0.16 | (0.05–0.50) | 0.002 |
| 9 months | |||
| TACE post-TARE | |||
| Yes | 0.17 | (0.04–0.78) | 0.023 |
| No | |||
| Child-Turcotte-Pugh | |||
| B | 1.5 | (0.63–3.65) | 0.344 |
| A |
| Adverse Reaction | Baseline | 3 Months Post-TARE | ||||||
|---|---|---|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
| Laboratory Abnormalities | ||||||||
| AST Elevation | 9 | 10 | 1 | |||||
| ALT Elevation | 6 | 6 | 1 | |||||
| Hypoalbuminemia | 9 | 7 | 7 | 10 | 4 | |||
| Elevated Alkaline Phosphatase | 16 | 5 | 4 | 4 | ||||
| Hyperbilirubinemia | 5 | 5 | 12 | 2 | 2 | |||
| Hyponatremia | 4 | 5 | 1 | |||||
| Elevated INR | 3 | 1 | 3 | 2 | ||||
| Complications | ||||||||
| REILD | 1 | |||||||
| PUD | 2 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Testa, S.; Bui, N.Q.; Wang, D.S.; Louie, J.D.; Sze, D.Y.; Ganjoo, K.N. Efficacy and Safety of Trans-Arterial Yttrium-90 Radioembolization in Patients with Unresectable Liver-Dominant Metastatic or Primary Hepatic Soft Tissue Sarcomas. Cancers 2022, 14, 324. https://doi.org/10.3390/cancers14020324
Testa S, Bui NQ, Wang DS, Louie JD, Sze DY, Ganjoo KN. Efficacy and Safety of Trans-Arterial Yttrium-90 Radioembolization in Patients with Unresectable Liver-Dominant Metastatic or Primary Hepatic Soft Tissue Sarcomas. Cancers. 2022; 14(2):324. https://doi.org/10.3390/cancers14020324
Chicago/Turabian StyleTesta, Stefano, Nam Q. Bui, David S. Wang, John D. Louie, Daniel Y. Sze, and Kristen N. Ganjoo. 2022. "Efficacy and Safety of Trans-Arterial Yttrium-90 Radioembolization in Patients with Unresectable Liver-Dominant Metastatic or Primary Hepatic Soft Tissue Sarcomas" Cancers 14, no. 2: 324. https://doi.org/10.3390/cancers14020324