
Circulating Cell-Free DNA-Based Comprehensive Molecular Analysis of Biliary Tract Cancers Using Next-Generation Sequencing

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Samples
2.2. Tumor Volume Evaluation
2.3. Histology and Immunohistochemistry
2.4. DNA Isolation
2.5. Next-Generation Sequencing
2.6. Statistical Analysis
3. Results
3.1. Patients Clinicopathological Characteristics
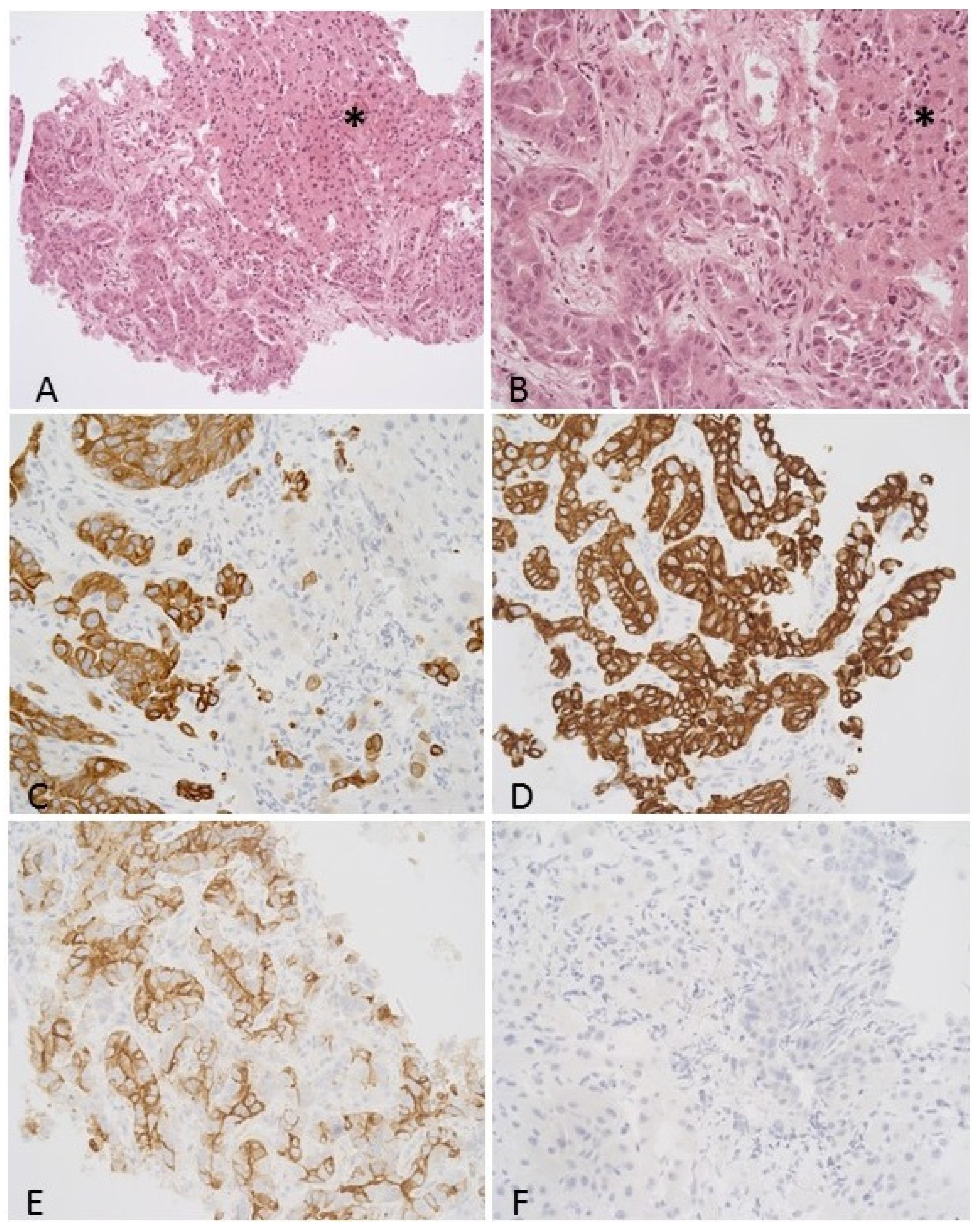
3.2. Histological Features including Immunohistochemistry
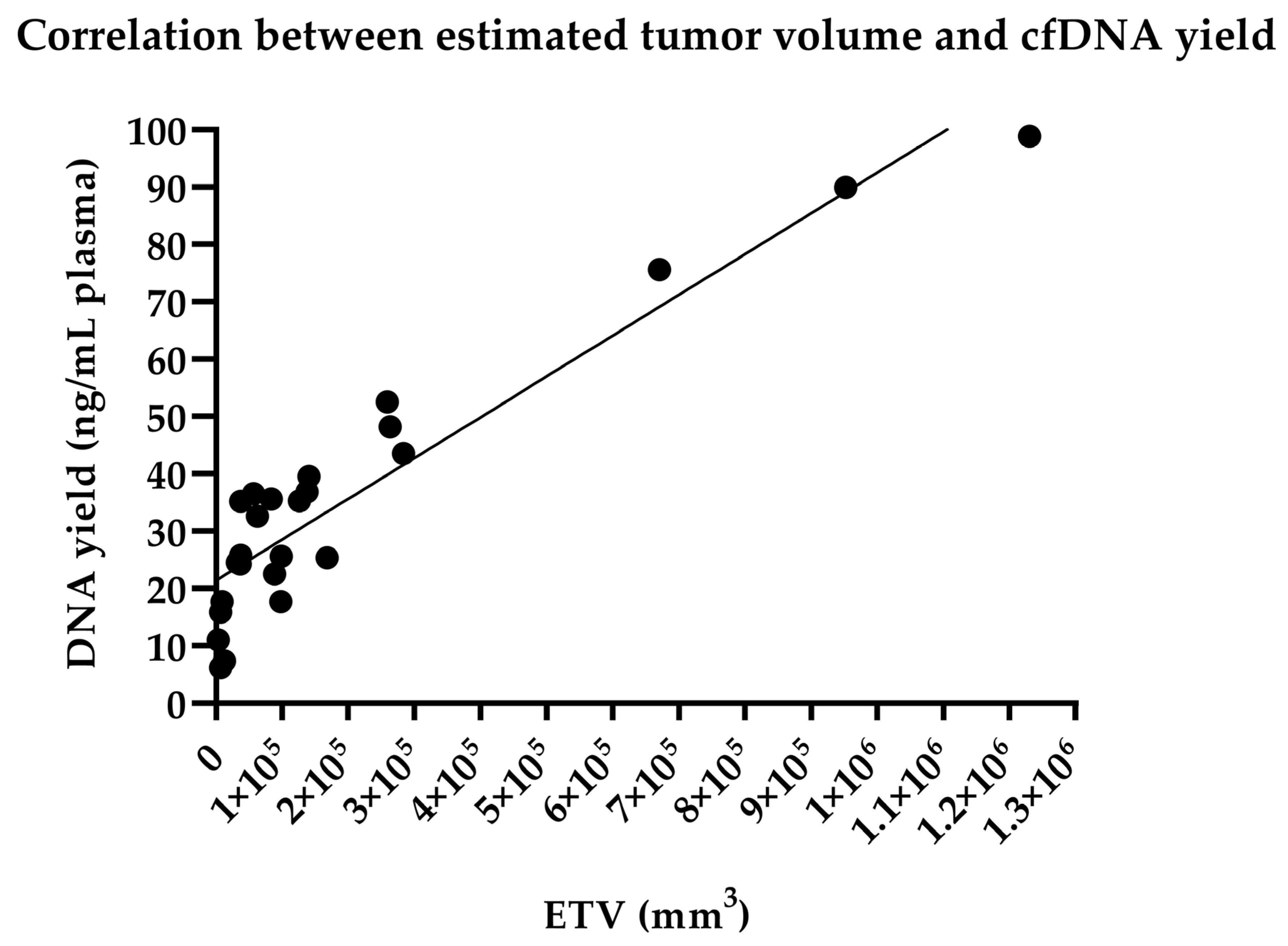
3.3. Correlation Analysis between Estimated Tumor Volume and cfDNA Yield
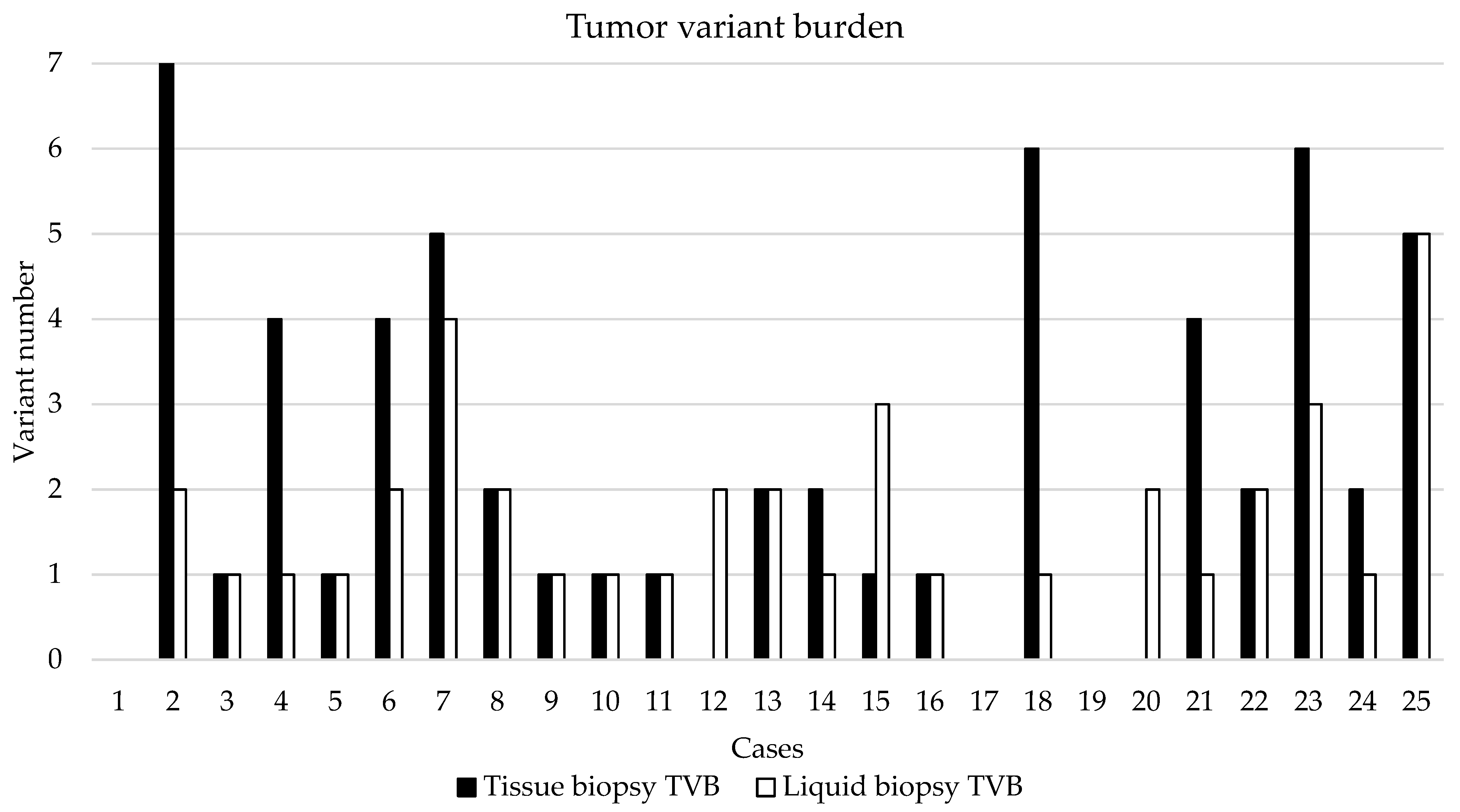
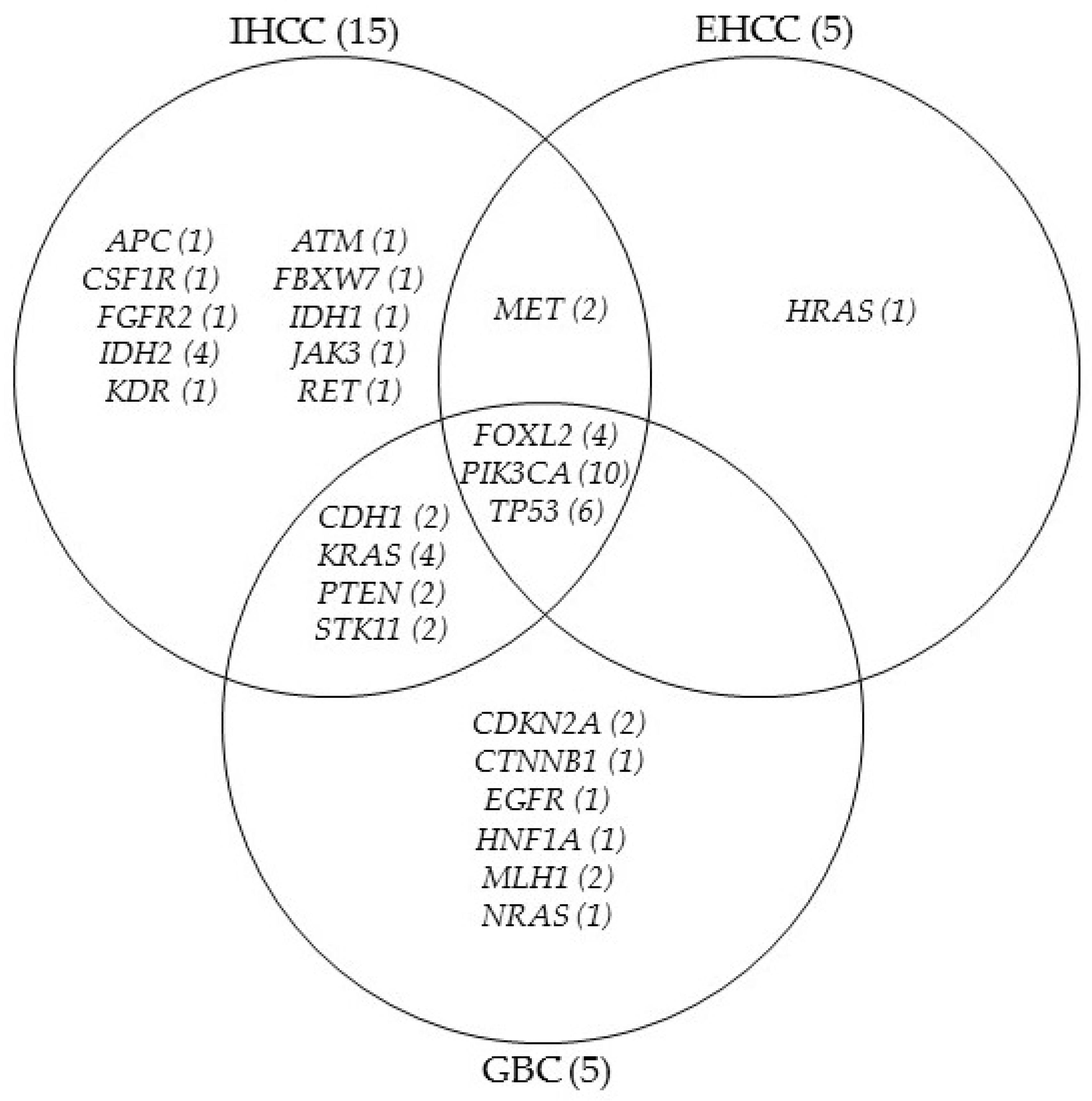
3.4. NGS-Based Mutation Profiling of Genomic and Cell-Free DNA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Noel, M.S.; Hezel, A.F. New and Emerging Treatment Options for Biliary Tract Cancer. OncoTargets Ther. 2013, 6, 1545–1552. [Google Scholar] [CrossRef] [Green Version]
- Weinberg, B.A.; Xiu, J.; Lindberg, M.R.; Shields, A.F.; Hwang, J.J.; Poorman, K.; Salem, M.E.; Pishvaian, M.J.; Holcombe, R.F.; Marshall, J.L.; et al. Molecular Profiling of Biliary Cancers Reveals Distinct Molecular Alterations and Potential Therapeutic Targets. J. Gastrointest. Oncol. 2019, 10, 652–662. [Google Scholar] [CrossRef]
- Putra, J.; de Abreu, F.B.; Peterson, J.D.; Pipas, J.M.; Mody, K.; Amos, C.I.; Tsongalis, G.J.; Suriawinata, A.A. Molecular Profiling of Intrahepatic and Extrahepatic Cholangiocarcinoma Using next Generation Sequencing. Exp. Mol. Pathol. 2015, 99, 240–244. [Google Scholar] [CrossRef] [Green Version]
- Horgan, A.M.; Amir, E.; Walter, T.; Knox, J.J. Adjuvant Therapy in the Treatment of Biliary Tract Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2012, 30, 1934–1940. [Google Scholar] [CrossRef]
- Ma, N.; Cheng, H.; Qin, B.; Zhong, R.; Wang, B. Adjuvant Therapy in the Treatment of Gallbladder Cancer: A Meta-Analysis. BMC Cancer 2015, 15, 615. [Google Scholar] [CrossRef] [Green Version]
- Lamarca, A.; Hubner, R.A.; David Ryder, W.; Valle, J.W. Second-Line Chemotherapy in Advanced Biliary Cancer: A Systematic Review. Ann. Oncol. 2014, 25, 2328–2338. [Google Scholar] [CrossRef]
- Ben-Josef, E.; Guthrie, K.A.; El-Khoueiry, A.B.; Corless, C.L.; Zalupski, M.M.; Lowy, A.M.; Thomas, C.R.; Alberts, S.R.; Dawson, L.A.; Micetich, K.C.; et al. SWOG S0809: A Phase II Intergroup Trial of Adjuvant Capecitabine and Gemcitabine Followed by Radiotherapy and Concurrent Capecitabine in Extrahepatic Cholangiocarcinoma and Gallbladder Carcinoma. J. Clin. Oncol. 2015, 33, 2617–2622. [Google Scholar] [CrossRef] [Green Version]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine Compared with Observation in Resected Biliary Tract Cancer (BILCAP): A Randomised, Controlled, Multicentre, Phase 3 Study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Ebata, T.; Hirano, S.; Konishi, M.; Uesaka, K.; Tsuchiya, Y.; Ohtsuka, M.; Kaneoka, Y.; Yamamoto, M.; Ambo, Y.; Shimizu, Y.; et al. Randomized Clinical Trial of Adjuvant Gemcitabine Chemotherapy versus Observation in Resected Bile Duct Cancer. Br. J. Surg. 2018, 105, 192–202. [Google Scholar] [CrossRef]
- Edeline, J.; Benabdelghani, M.; Bertaut, A.; Watelet, J.; Hammel, P.; Joly, J.-P.; Boudjema, K.; Fartoux, L.; Bouhier-Leporrier, K.; Jouve, J.-L.; et al. Gemcitabine and Oxaliplatin Chemotherapy or Surveillance in Resected Biliary Tract Cancer (PRODIGE 12-ACCORD 18-UNICANCER GI): A Randomized Phase III Study. J. Clin. Oncol. 2019, 37, 658–667. [Google Scholar] [CrossRef]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K.; et al. Second-Line FOLFOX Chemotherapy versus Active Symptom Control for Advanced Biliary Tract Cancer (ABC-06): A Phase 3, Open-Label, Randomised, Controlled Trial. Lancet Oncol. 2021, 22, 690–701. [Google Scholar] [CrossRef]
- Tamai, K.; Nakamura, M.; Mizuma, M.; Mochizuki, M.; Yokoyama, M.; Endo, H.; Yamaguchi, K.; Nakagawa, T.; Shiina, M.; Unno, M.; et al. Suppressive Expression of CD274 Increases Tumorigenesis and Cancer Stem Cell Phenotypes in Cholangiocarcinoma. Cancer Sci. 2014, 105, 667–674. [Google Scholar] [CrossRef]
- Fontugne, J.; Augustin, J.; Pujals, A.; Compagnon, P.; Rousseau, B.; Luciani, A.; Tournigand, C.; Cherqui, D.; Azoulay, D.; Pawlotsky, J.-M.; et al. PD-L1 Expression in Perihilar and Intrahepatic Cholangiocarcinoma. Oncotarget 2017, 8, 24644–24651. [Google Scholar] [CrossRef] [Green Version]
- Mody, K.; Starr, J.; Saul, M.; Poorman, K.; Weinberg, B.A.; Salem, M.E.; VanderWalde, A.; Shields, A.F. Patterns and Genomic Correlates of PD-L1 Expression in Patients with Biliary Tract Cancers. J. Gastrointest. Oncol. 2019, 10, 1099–1109. [Google Scholar] [CrossRef]
- Cardinale, V.; Carpino, G.; Reid, L.; Gaudio, E.; Alvaro, D. Multiple Cells of Origin in Cholangiocarcinoma Underlie Biological, Epidemiological and Clinical Heterogeneity. World J. Gastrointest. Oncol. 2012, 4, 94–102. [Google Scholar] [CrossRef]
- Churi, C.R.; Shroff, R.; Wang, Y.; Rashid, A.; Kang, H.C.; Weatherly, J.; Zuo, M.; Zinner, R.; Hong, D.; Meric-Bernstam, F.; et al. Mutation Profiling in Cholangiocarcinoma: Prognostic and Therapeutic Implications. PLoS ONE 2014, 9, e115383. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, H.; Arai, Y.; Totoki, Y.; Shirota, T.; Elzawahry, A.; Kato, M.; Hama, N.; Hosoda, F.; Urushidate, T.; Ohashi, S.; et al. Genomic Spectra of Biliary Tract Cancer. Nat. Genet 2015, 47, 1003–1010. [Google Scholar] [CrossRef]
- Brandi, G.; Farioli, A.; Astolfi, A.; Biasco, G.; Tavolari, S. Genetic Heterogeneity in Cholangiocarcinoma: A Major Challenge for Targeted Therapies. Oncotarget 2015, 6, 14744–14753. [Google Scholar] [CrossRef] [Green Version]
- Méhes, G. Liquid Biopsy for Predictive Mutational Profiling of Solid Cancer: The Pathologist’s Perspective. J. Biotechnol. 2019, 297, 66–70. [Google Scholar] [CrossRef]
- Rizzo, A.; Ricci, A.D.; Tavolari, S.; Brandi, G. Circulating Tumor DNA in Biliary Tract Cancer: Current Evidence and Future Perspectives. Cancer Genom. Proteom. 2020, 17, 441–452. [Google Scholar] [CrossRef]
- Han, J.-Y.; Ahn, K.S.; Kim, T.-S.; Kim, Y.H.; Cho, K.B.; Shin, D.W.; Baek, W.-K.; Suh, S.-I.; Jang, B.-C.; Kang, K.J. Liquid Biopsy from Bile-Circulating Tumor DNA in Patients with Biliary Tract Cancer. Cancers 2021, 13, 4581. [Google Scholar] [CrossRef]
- Rachiglio, A.M.; Esposito Abate, R.; Sacco, A.; Pasquale, R.; Fenizia, F.; Lambiase, M.; Morabito, A.; Montanino, A.; Rocco, G.; Romano, C.; et al. Limits and Potential of Targeted Sequencing Analysis of Liquid Biopsy in Patients with Lung and Colon Carcinoma. Oncotarget 2016, 7, 66595–66605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mack, P.C.; Banks, K.C.; Espenschied, C.R.; Burich, R.A.; Zill, O.A.; Lee, C.E.; Riess, J.W.; Mortimer, S.A.; Talasaz, A.; Lanman, R.B.; et al. Spectrum of Driver Mutations and Clinical Impact of Circulating Tumor DNA Analysis in Non-Small Cell Lung Cancer: Analysis of over 8000 Cases. Cancer 2020, 126, 3219–3228. [Google Scholar] [CrossRef] [PubMed]
- Gaiser, M.R.; von Bubnoff, N.; Gebhardt, C.; Utikal, J.S. Liquid Biopsy to Monitor Melanoma Patients. J. Dtsch. Dermatol. Ges. 2018, 16, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Mokánszki, A.; Bicskó, R.; Gergely, L.; Méhes, G. Cell-Free Total Nucleic Acid-Based Genotyping of Aggressive Lymphoma: Comprehensive Analysis of Gene Fusions and Nucleotide Variants by Next-Generation Sequencing. Cancers 2021, 13, 3032. [Google Scholar] [CrossRef]
- Rompianesi, G.; Di Martino, M.; Gordon-Weeks, A.; Montalti, R.; Troisi, R. Liquid Biopsy in Cholangiocarcinoma: Current Status and Future Perspectives. World J. Gastrointest. Oncol. 2021, 13, 332–350. [Google Scholar] [CrossRef]
- Samstein, R.M.; Lee, C.-H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor Mutational Load Predicts Survival after Immunotherapy across Multiple Cancer Types. Nat. Genet. 2019, 51, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wu, X.; Wu, H.; Gu, Y.; Shao, Y.; Shao, Q.; Zhu, F.; Li, X.; Qian, X.; Hu, J.; et al. Camrelizumab plus Gemcitabine and Oxaliplatin (GEMOX) in Patients with Advanced Biliary Tract Cancer: A Single-Arm, Open-Label, Phase II Trial. J. Immunother. Cancer 2020, 8, e001240. [Google Scholar] [CrossRef]
- Jusakul, A.; Cutcutache, I.; Yong, C.H.; Lim, J.Q.; Huang, M.N.; Padmanabhan, N.; Nellore, V.; Kongpetch, S.; Ng, A.W.T.; Ng, L.M.; et al. Whole-Genome and Epigenomic Landscapes of Etiologically Distinct Subtypes of Cholangiocarcinoma. Cancer Discov. 2017, 7, 1116–1135. [Google Scholar] [CrossRef] [Green Version]
- Mertens, J.C.; Rizvi, S.; Gores, G.J. Targeting Cholangiocarcinoma. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 1454–1460. [Google Scholar] [CrossRef]
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving Concepts and Therapeutic Strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef] [Green Version]
- Montal, R.; Sia, D.; Montironi, C.; Leow, W.Q.; Esteban-Fabró, R.; Pinyol, R.; Torres-Martin, M.; Bassaganyas, L.; Moeini, A.; Peix, J.; et al. Molecular Classification and Therapeutic Targets in Extrahepatic Cholangiocarcinoma. J. Hepatol. 2020, 73, 315–327. [Google Scholar] [CrossRef]
- Lendvai, G.; Szekerczés, T.; Illyés, I.; Dóra, R.; Kontsek, E.; Gógl, A.; Kiss, A.; Werling, K.; Kovalszky, I.; Schaff, Z.; et al. Cholangiocarcinoma: Classification, Histopathology and Molecular Carcinogenesis. Pathol. Oncol. Res. 2020, 26, 3–15. [Google Scholar] [CrossRef]
- Andersen, J.B.; Spee, B.; Blechacz, B.R.; Avital, I.; Komuta, M.; Barbour, A.; Conner, E.A.; Gillen, M.C.; Roskams, T.; Roberts, L.R.; et al. Genomic and Genetic Characterization of Cholangiocarcinoma Identifies Therapeutic Targets for Tyrosine Kinase Inhibitors. Gastroenterology 2012, 142, 1021–1031.e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sia, D.; Hoshida, Y.; Villanueva, A.; Roayaie, S.; Ferrer, J.; Tabak, B.; Peix, J.; Sole, M.; Tovar, V.; Alsinet, C.; et al. Integrative Molecular Analysis of Intrahepatic Cholangiocarcinoma Reveals 2 Classes That Have Different Outcomes. Gastroenterology 2013, 144, 829–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou-Alfa, G.K.; Macarulla, T.; Javle, M.M.; Kelley, R.K.; Lubner, S.J.; Adeva, J.; Cleary, J.M.; Catenacci, D.V.; Borad, M.J.; Bridgewater, J.; et al. Ivosidenib in IDH1-Mutant, Chemotherapy-Refractory Cholangiocarcinoma (ClarIDHy): A Multicentre, Randomised, Double-Blind, Placebo-Controlled, Phase 3 Study. Lancet Oncol. 2020, 21, 796–807. [Google Scholar] [CrossRef]
- Zhu, A.X.; Macarulla, T.; Javle, M.M.; Kelley, R.K.; Lubner, S.J.; Adeva, J.; Cleary, J.M.; Catenacci, D.V.T.; Borad, M.J.; Bridgewater, J.A.; et al. Final Overall Survival Efficacy Results of Ivosidenib for Patients With Advanced Cholangiocarcinoma with IDH1 Mutation: The Phase 3 Randomized Clinical ClarIDHy Trial. JAMA Oncol. 2021, 7, 1669–1677. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases | Gender | Age (Years) | ETV (mm3) | Metastasis | BTC Subtype | Chemotherapy |
|---|---|---|---|---|---|---|
| 1 | F | 80 | 83,349 | no | IHCC | cisplatin plus gemcitabine, capecitabine, irinotecan |
| 2 | F | 75 | 88,200 | liver | IHCC | gemcitabine, bevacizumab |
| 3 | M | 76 | 56,784 | liver | IHCC | capecitabine, cisplatin plus gemcitabin |
| 4 | M | 59 | 37,044 | no | IHCC | cisplatin plus gemcitabine |
| 5 | M | 68 | 1,680,000 | no | IHCC | cisplatin plus gemcibatine, irinotecan, capecitabine |
| 6 | M | 68 | 37,462 | no | IHCC | cisplatin plus gemcitabine, capecitabine |
| 7 | M | 60 | 259,200 | peritoneum | IHCC | cisplatin plus gemcitabine, trametinib, everolimus |
| 8 | M | 68 | 62,500 | no | IHCC | cisplatin plus gemcitabine |
| 9 | F | 63 | 1,230,187 | no | IHCC | cisplatin plus gemcitabine |
| 10 | M | 53 | 263,250 | no | IHCC | cisplatin plus gemcitabine, irinotecan |
| 11 | M | 70 | 12,800 | no | IHCC | cisplatin plus gemcitabine, irinotecan, capeticabine |
| 12 | F | 61 | 283,500 | no | IHCC | cisplatin plus gemcitabine, capecitabine |
| 13 | M | 75 | 9126 | liver | IHCC | capecitabine, gemcitabine |
| 14 | F | 49 | 140,625 | ovary | IHCC | cisplatin plus gemcitabine |
| 15 | F | 66 | 670,372 | no | IHCC | gemcitabine |
| 16 | F | 64 | 36,162 | no | EHCC | cisplatin plus gemcitabine, capecitabine |
| 17 | M | 43 | 952,544 | no | EHCC | cisplatin plus gemcitabine, irinotecan |
| 18 | M | 51 | 6664 | no | EHCC | cisplatin plus gemcitabine, nivolumab |
| 19 | F | 70 | 98,606 | no | EHCC | cisplatin plus gemcitabine |
| 20 | F | 71 | 32,000 | no | EHCC | cisplatin plus gemcitabine |
| 21 | F | 58 | 6750 | no | GBC | cisplatin plus gemcitabine, irinotecan |
| 22 | M | 70 | 126,000 | no | GBC | cisplatin plus gemcitabine |
| 23 | M | 68 | 3179 | no | GBC | cisplatin plus gemcitabine |
| 24 | F | 71 | 137,312 | no | GBC | cisplatin plus gemcitabine |
| 25 | F | 60 | 98,000 | no | GBC | capecitabine, cisplatin plus gemcitabine |
| Cases | Grading | CK7 | CK8/18 | CK19 | CK20 | CA19.9 | HSA | Arginase | Glypican | PD-L1 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | G2 | + | + | + | − | + | − | − | − | − |
| 2 | G2 | + | + | + | + | + | − | − | − | − |
| 3 | G3 | + | + | + | − | + | − | − | − | − |
| 4 | G2 | + | + | + | − | + | − | − | − | − |
| 5 | G2 | + | + | + | − | + | − | − | − | − |
| 6 | G2 | + | − | + | − | + | − | − | − | − |
| 7 | G2 | + | + | + | − | + | − | − | − | − |
| 8 | G2 | + | + | + | − | + | − | − | + * | − |
| 9 | G2 | + | + | + | + | + | − | − | − | − |
| 10 | G2 | + | + | + | − | + | − | − | − | − |
| 11 | G2 | + | + | + | − | + | − | + | − | − |
| 12 | G3 | + | + | + | + | + | − | − | − | − |
| 13 | G2 | + | + | + | − | − | − | − | − | − |
| 14 | G3 | + | + | + | − | + | − | − | + * | − |
| 15 | G2 | + | − | + | − | + | − | − | − | − |
| 16 | G1 | + | + | + | − | + | − | − | − | − |
| 17 | G3 | + | + | + | − | + | − | − | − | − |
| 18 | G2 | − | + | + | − | + | − | − | − | − |
| 19 | G2 | + | + | + | − | − | − | − | − | − |
| 20 | G2 | + | + | + | − | + | − | − | − | − |
| 21 | G2 | + | + | + | − | + | − | − | − | − |
| 22 | G2 | + | + | + | + | + | − | − | − | − |
| 23 | G3 | + | + | + | − | + | − | + | − | − |
| 24 | G3 | + | + | + | − | + | − | + | − | − |
| 25 | G2 | + | + | + | − | + | − | − | − | − |
| Cases | Gene | Nucleotide Change | Amino Acid Change | VAF (%) Tissue | VAF (%) LB | Clinical Significance |
|---|---|---|---|---|---|---|
| 2 | KRAS | c.407G>A | p.Ser136Asn | 50 | 21.3 | pathogenic |
| IDH1 | c.395G>T | p.Arg132Leu | 25 | 19.6 | pathogenic | |
| PTEN | c.925G>A | p.Ala309Thr | 20 | 15.2 | benign | |
| FBXW7 | c.239C>T | p.Thr80Ile | 6 | 0 | likely pathogenic | |
| IDH2 | c.332G>A | p.Gly111Asp | 4.6 | 0 | likely benign | |
| CDH1 | c.596C>T | p.Thr199Ile | 4.3 | 0 | likely benign | |
| 3 | PIK3CA | c.1634A>C | p.Glu545Ala | 3 | 3 | pathogenic |
| 6 | FOXL2 | c.536C>G | p.Ala179Gly | 57.6 | 15.2 | benign |
| APC | c.7504G>A | p.Gly2502Ser | 49.5 | 6.7 | likely pathogenic | |
| PIK3CA | c.1634A>C | p.Glu545Ala | 3.8 | 0 | pathogenic | |
| 7 | JAK3 | c.2164G>A | p.Val722Ile | 45.5 | 6.9 | benign |
| TP53 | c.518T>C | p.Val173Ala | 13.2 | 4.9 | pathogenic | |
| KRAS | c.35G>T | p.Gly12Val | 12.8 | 3.6 | pathogenic | |
| 8 | TP53 | c.460G>A | p.Gly154Ser | 4 | 2.1 | pathogenic |
| 9 | FGFR2 | c.827T>G | p.Phe276Cys | 37 | 6.3 | pathogenic |
| 10 | IDH2 | c.515G>T | p.Arg172Met | 24.3 | 21.5 | pathogenic |
| 11 | IDH2 | c.359G>A | p.Arg120Lys | 27.6 | 8.4 | pathogenic |
| 12 | KDR | c.1444T>C | p.Cys482Arg | Low tumor cell ratio | 47.2 | pathogenic |
| STK11 | c.1189G>A | p.Ala397Thr | 46.3 | benign | ||
| 13 | TP53 | c.536A>G | p.His179Arg | 62.6 | 5.6 | pathogenic |
| IDH2 | c.359G>A | p.Arg120Lys | 30.2 | 4.2 | pathogenic | |
| 14 | MET | c.2975C>T | p.Thr992Ile | 0 | 45.8 | pathogenic |
| 15 | CSF1R | c.2916C>G | p.Cys972Trp | 0 | 7.9 | benign |
| RET | c.1946C>T | p.Ser649Leu | 0 | 7.8 | likely pathogenic | |
| FOXL2 | c.536C>G | p.Ala179Gly | 61.6 | 4.5 | benign | |
| 16 | TP53 | c.796G>T | p.Gly266Ter | 29.2 | 5.2 | pathogenic |
| 18 | MET | c.1124A>G | p.Asn375Ser | 59.7 | 48.21 | pathogenic |
| HRAS | c.182A>G | p.Gln61Arg | 33.3 | 0 | pathogenic | |
| PIK3CA | c.40C>A | p.His14Asn | 7.2 | 0 | likely benign | |
| PIK3CA | c.1634A>C | p.Glu545Ala | 4.6 | 0 | pathogenic | |
| 20 | FOXL2 | c.536C>G | p.Ala179Gly | Low tumor cell ratio | 67.5 | benign |
| PIK3CA | c.1571G>A | p.Arg524Lys | 7.7 | pathogenic | ||
| 21 | NRAS | c.104C>T | p.Thr35Ile | 8.3 | 2.6 | benign |
| 22 | CDKN2A | c.442G>A | p.Ala148Thr | 57.8 | 52 | benign |
| EGFR | c.2543C>T | p.Pro848Leu | 41 | 39 | likely benign | |
| 23 | CDKN2A | c.442G>A | p.Ala148Thr | 49 | 52.8 | benign |
| CDH1 | c.2474C>T | p.Pro825Leu | 46 | 50.7 | pathogenic | |
| HNF1A | c.862delG | p.Pro291GlnfsTer51 | 5.2 | 5.14 | likely pathogenic | |
| TP53 | c.325T>G | p.Phe109Val | 4.9 | 0 | pathogenic | |
| PTEN | c.802G>T | p.Asp268Tyr | 4.6 | 0 | pathogenic | |
| 24 | STK11 | c.842del | p.Pro281ArgfsTer6 | 6.3 | 0 | pathogenic |
| 25 | MLH1 | c.1321G>A | p.Ala441Thr | 46.2 | 49.1 | pathogenic |
| TP53 | c.707_711del | p.Tyr236LeufsTer2 | 12.1 | 3.4 | likely pathogenic | |
| PIK3CA | c.1571G>A | p.Arg524Lys | 11.3 | 5.3 | pathogenic | |
| CTNNB1 | c.133T>C | p.Ser45Pro | 11.2 | 2.4 | pathogenic | |
| KRAS | c.34G>T | p.Gly12Cys | 6.6 | 0 | pathogenic | |
| FOXL2 | c.743T>C | p.Leu248Pro | 0 | 3.1 | likely pathogenic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Csoma, S.L.; Bedekovics, J.; Veres, G.; Árokszállási, A.; András, C.; Méhes, G.; Mokánszki, A. Circulating Cell-Free DNA-Based Comprehensive Molecular Analysis of Biliary Tract Cancers Using Next-Generation Sequencing. Cancers 2022, 14, 233. https://doi.org/10.3390/cancers14010233
Csoma SL, Bedekovics J, Veres G, Árokszállási A, András C, Méhes G, Mokánszki A. Circulating Cell-Free DNA-Based Comprehensive Molecular Analysis of Biliary Tract Cancers Using Next-Generation Sequencing. Cancers. 2022; 14(1):233. https://doi.org/10.3390/cancers14010233
Chicago/Turabian StyleCsoma, Szilvia Lilla, Judit Bedekovics, Gergő Veres, Anita Árokszállási, Csilla András, Gábor Méhes, and Attila Mokánszki. 2022. "Circulating Cell-Free DNA-Based Comprehensive Molecular Analysis of Biliary Tract Cancers Using Next-Generation Sequencing" Cancers 14, no. 1: 233. https://doi.org/10.3390/cancers14010233