
Prognostic Value of the B12/CRP Index in Older Systemically Treatable Cancer Patients

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Population
3.2. BCI and Geriatric Frailty
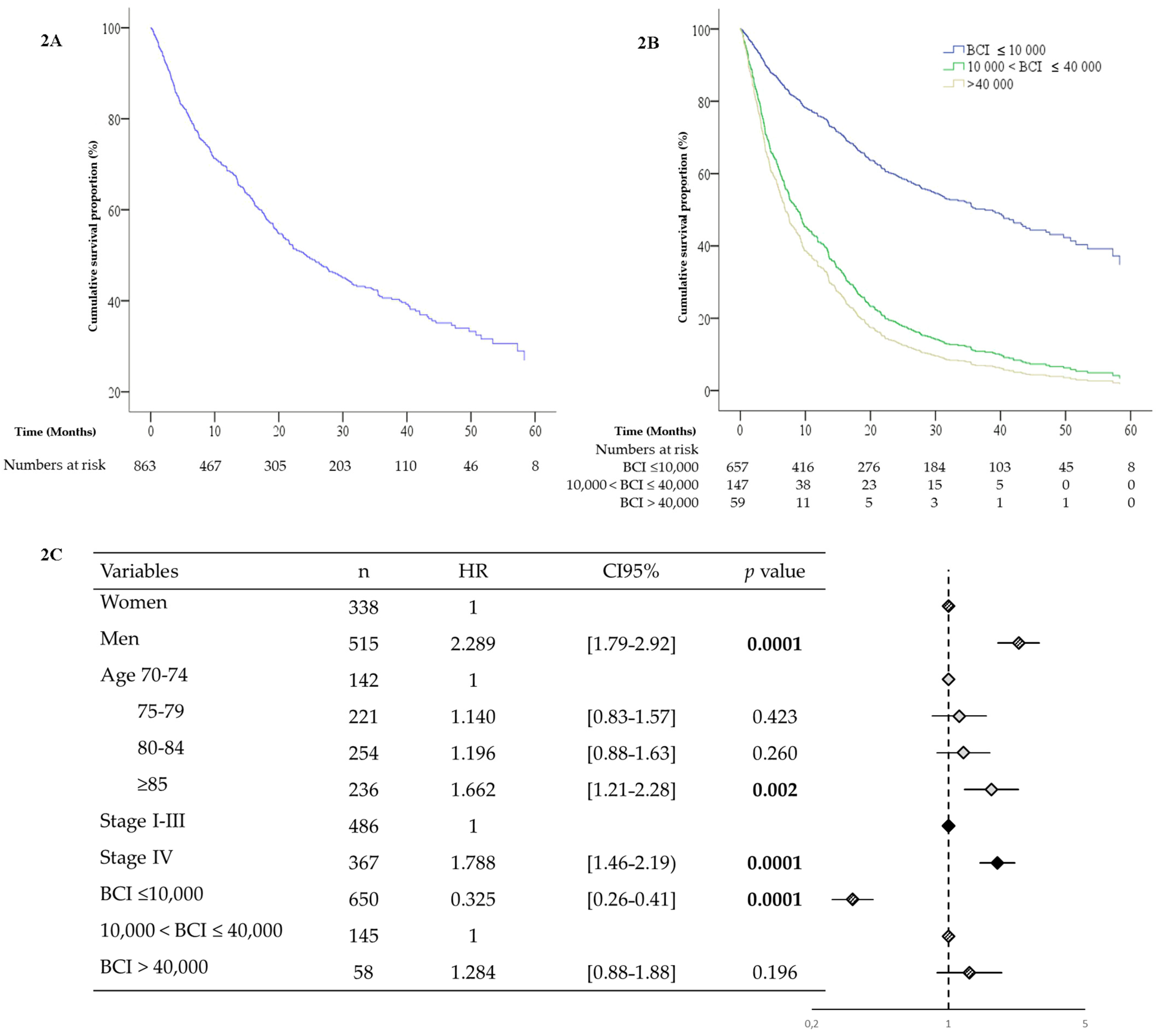
3.3. BCI and Survival
3.3.1. Total Population
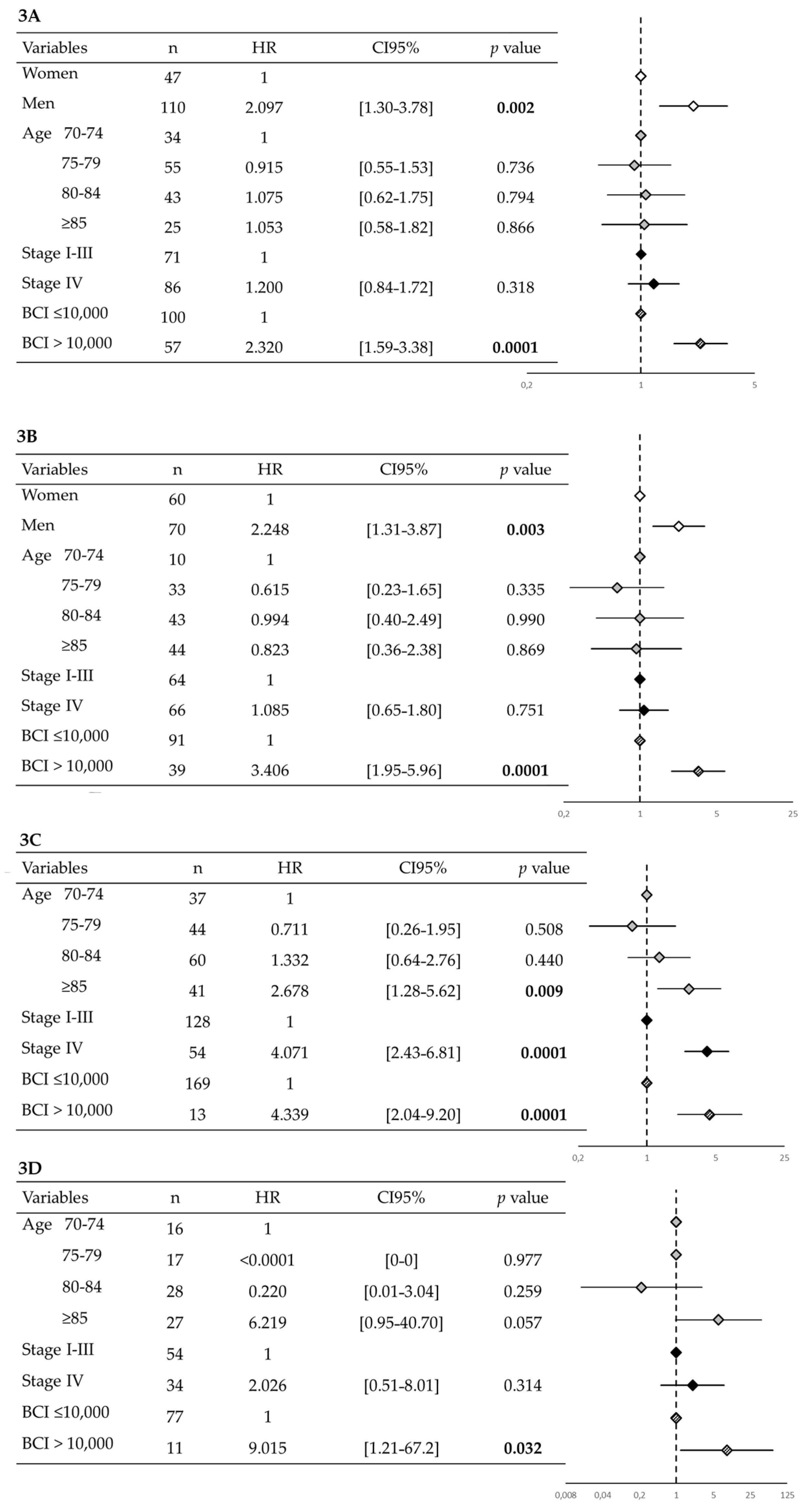
3.3.2. Survival According to Cancer Site
4. Discussion
4.1. Perspectives
4.2. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries and 25 Major Cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.G.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dotan, E.; Walter, L.C.; Browner, I.S.; Clifton, K.; Cohen, H.J.; Extermann, M.; Gross, C.; Gupta, S.; Hollis, G.; Hubbard, J.; et al. NCCN Guidelines® Insights: Older Adult Oncology, Version 1.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 1006–1019. [Google Scholar] [CrossRef] [PubMed]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.S.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-Related Inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Capri, M.; Monti, D.; Giunta, S.; Olivieri, F.; Sevini, F.; Panourgia, M.P.; Invidia, L.; Celani, L.; Scurti, M.; et al. Inflammaging and Anti-Inflammaging: A Systemic Perspective on Aging and Longevity Emerged from Studies in Humans. Mech. Ageing Dev. 2007, 128, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Penninx, B.W.J.H.; Volpato, S.; Harris, T.B.; Bandeen-Roche, K.; Balfour, J.; Leveille, S.G.; Fried, L.P.; Md, J.M.G. Change in Muscle Strength Explains Accelerated Decline of Physical Function in Older Women with High Interleukin-6 Serum Levels. J. Am. Geriatr. Soc. 2002, 50, 1947–1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harneshaug, M.; Kirkhus, L.; Benth, J.Š.; Grønberg, B.H.; Bergh, S.; Whist, J.E.; Rostoft, S.; Jordhøy, M.S. Screening for Frailty among Older Patients with Cancer Using Blood Biomarkers of Inflammation. J. Geriatr. Oncol. 2019, 10, 272–278. [Google Scholar] [CrossRef]
- Allin, K.H.; Bojesen, S.E.; Nordestgaard, B.G. Baseline C-Reactive Protein Is Associated with Incident Cancer and Survival in Patients with Cancer. J. Clin. Oncol. 2009, 27, 2217–2224. [Google Scholar] [CrossRef]
- Geissbuhler, P.; Mermillod, B.; Rapin, C.H. Elevated Serum Vitamin B12 Levels Associated with CRP as a Predictive Factor of Mortality in Palliative Care Cancer Patients: A Prospective Study over Five Years. J. Pain Symptom Manag. 2000, 20, 93–103. [Google Scholar] [CrossRef]
- Salles, N.; Herrmann, F.; Sakbani, K.; Rapin, C.-H.; Sieber, C. High Vitamin B12 Level: A Strong Predictor of Mortality in Elderly Inpatients. J. Am. Geriatr. Soc. 2005, 53, 917–918. [Google Scholar] [CrossRef]
- Carmel, R.; Eisenberg, L. Serum Vitamin B12 and Transcobalamin Abnormalities in Patients with Cancer. Cancer 1977, 40, 1348–1353. [Google Scholar] [CrossRef]
- Ermens, A.A.M.; Vlasveld, L.T.; Lindemans, J. Significance of Elevated Cobalamin (Vitamin B12) Levels in Blood. Clin. Biochem. 2003, 36, 585–590. [Google Scholar] [CrossRef]
- Kelly, L.; White, S.; Stone, P.C. The B12/CRP Index as a Simple Prognostic Indicator in Patients with Advanced Cancer: A Confirmatory Study. Ann. Oncol. 2007, 18, 1395–1399. [Google Scholar] [CrossRef]
- Couderc, A.-L.; Puchades, E.; Villani, P.; Arcani, R.; Farnault, L.; Daumas, A.; Courcier, A.; Greillier, L.; Barlesi, F.; Duffaud, F.; et al. High Serum Vitamin B12 Levels Associated with C-Reactive Protein in Older Patients with Cancer. Oncologist 2020, 25, e1980–e1989. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. the Index of Adl: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Yesavage, J.A. Geriatric Depression Scale. Psychopharmacol. Bull. 1988, 24, 709–711. [Google Scholar] [PubMed]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Mini Nutritional Assessment: A Practical Assessment Tool for Grading the Nutritional State of Elderly Patients. Facts. Res. Gerontol. 1994, (Suppl. 2), 15–60. [Google Scholar]
- Friedman, P.J.; Richmond, D.E.; Baskett, J.J. A Prospective Trial of Serial Gait Speed as a Measure of Rehabilitation in the Elderly. Age Ageing 1988, 17, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Vellas, B.J.; Wayne, S.J.; Romero, L.; Baumgartner, R.N.; Rubenstein, L.Z.; Garry, P.J. One-Leg Balance Is an Important Predictor of Injurious Falls in Older Persons. J. Am. Geriatr. Soc. 1997, 45, 735–738. [Google Scholar] [CrossRef]
- Overcash, J.A.; Beckstead, J. Predicting Falls in Older Patients Using Components of a Comprehensive Geriatric Assessment. Clin. J. Oncol. Nurs. 2008, 12, 941–949. [Google Scholar] [CrossRef]
- Puts, M.T.E.; Monette, J.; Girre, V.; Wolfson, C.; Monette, M.; Batist, G.; Bergman, H. The Fall Rate of Older Community-Dwelling Cancer Patients. Support. Care Cancer 2013, 21, 775–783. [Google Scholar] [CrossRef]
- Stone, C.A.; Lawlor, P.G.; Savva, G.M.; Bennett, K.; Kenny, R.A. Prospective Study of Falls and Risk Factors for Falls in Adults with Advanced Cancer. J. Clin. Oncol. 2012, 30, 2128–2133. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [Green Version]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A Manual of Guidelines to Score the Modified Cumulative Illness Rating Scale and Its Validation in Acute Hospitalized Elderly Patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef]
- Smith, A.D.; Refsum, H. Vitamin B-12 and Cognition in the Elderly. Am. J. Clin. Nutr. 2009, 89, 707S–711S. [Google Scholar] [CrossRef] [Green Version]
- Aparicio, T.; Jouve, J.-L.; Teillet, L.; Gargot, D.; Subtil, F.; Le Brun-Ly, V.; Cretin, J.; Locher, C.; Bouché, O.; Breysacher, G.; et al. Geriatric Factors Predict Chemotherapy Feasibility: Ancillary Results of FFCD 2001-02 Phase III Study in First-Line Chemotherapy for Metastatic Colorectal Cancer in Elderly Patients. J. Clin. Oncol. 2013, 31, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Maione, P.; Perrone, F.; Gallo, C.; Manzione, L.; Piantedosi, F.; Barbera, S.; Cigolari, S.; Rosetti, F.; Piazza, E.; Robbiati, S.F.; et al. Pretreatment Quality of Life and Functional Status Assessment Significantly Predict Survival of Elderly Patients with Advanced Non-Small-Cell Lung Cancer Receiving Chemotherapy: A Prognostic Analysis of the Multicenter Italian Lung Cancer in the Elderly Study. J. Clin. Oncol. 2005, 23, 6865–6872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couderc, A.-L.; Suchon, P.; Saliba-Serre, B.; Rey, D.; Nouguerede, E.; Arcani, R.; Farnault, L.; Daumas, A.; Courcier, A.; Duffaud, F.; et al. Functional Status in Older Patients with Cancer. J. Geriatr. Oncol. 2022, 13, 40–45. [Google Scholar] [CrossRef] [PubMed]
- O’Gorman, P.; McMillan, D.C.; McArdle, C.S. Prognostic Factors in Advanced Gastrointestinal Cancer Patients with Weight Loss. Nutr. Cancer 2000, 37, 36–40. [Google Scholar] [CrossRef]
- Mattox, T.W. Cancer Cachexia: Cause, Diagnosis, and Treatment. Nutr. Clin. Pract. 2017, 32, 599–606. [Google Scholar] [CrossRef]
- Tavares, F. Is the B12/CRP Index More Accurate than You at Predicting Life Expectancy in Advanced Cancer Patients? J. Pain Symptom Manag. 2010, 40, e12–e13. [Google Scholar] [CrossRef]
- Ferlay, J.; Ervik, M.; Colombet, M.; Mery, L.; Pineros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: http://gco.iarc.fr/today/home (accessed on 3 November 2021).




{kind=link}
{kind=link}
{kind=link}
| Variables | Total Population (n = 863) | BCI ≤ 10,000 (n = 657) | 10,000 < BCI ≤ 40,000 (n = 147) | BCI > 40,000 (n = 59) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Gender | |||||||||
| Women | 341 | 39.5 | 269 | 40.9 | 49 | 33.3 | 23 | 39.0 | 0.232 |
| Men | 522 | 60.5 | 388 | 45.0 | 98 | 66.7 | 36 | 61.0 | |
| Age (years) | |||||||||
| 70–74 | 142 | 16.5 | 114 | 17.4 | 17 | 11.6 | 11 | 18.6 | 0.152 |
| 75–79 | 223 | 25.8 | 162 | 24.7 | 46 | 31.3 | 15 | 25.4 | |
| 80–84 | 257 | 29.8 | 190 | 28.9 | 44 | 29.9 | 23 | 39.0 | |
| ≥85 | 241 | 27.9 | 191 | 29.1 | 40 | 27.2 | 10 | 16.9 | |
| Stage IV cancer (n = 853) | 367 | 42.5 | 245 | 37.7 | 86 | 59.3 | 36 | 62.1 | 0.0001 |
| Cancer type (n = 862) | |||||||||
| Prostate | 184 | 21.3 | 171 | 26.0 | 11 | 7.5 | 2 | 3.4 | 0.0001 |
| Thoracic | 183 | 21.2 | 112 | 17.0 | 52 | 35.4 | 19 | 32.2 | |
| Gastrointestinal | 131 | 15.2 | 92 | 14.0 | 25 | 17.1 | 14 | 23.7 | |
| Breast | 90 | 10.4 | 78 | 11.9 | 8 | 5.4 | 4 | 6.8 | |
| Head and neck | 67 | 7.8 | 45 | 6.8 | 20 | 13.7 | 2 | 3.4 | |
| Female reproductive organs | 56 | 6.5 | 43 | 6.5 | 6 | 4.1 | 7 | 11.9 | |
| Urological | 50 | 5.8 | 38 | 5.8 | 8 | 5.5 | 4 | 6.8 | |
| Hematological | 51 | 5.9 | 37 | 5.6 | 10 | 6.8 | 4 | 6.8 | |
| Skin | 35 | 4.1 | 31 | 4.7 | 4 | 2.7 | 3 | 5.1 | |
| Other | 15 | 1.7 | 10 | 1.5 | 2 | 1.4 | 3 | 5.1 | |
| Autonomy (n = 860) | |||||||||
| Unimpaired ADL-IADL | 323 | 37.6 | 284 | 43.4 | 33 | 22.4 | 6 | 10.2 | 0.0001 |
| Impaired ADL or IADL | 224 | 26.0 | 174 | 26.6 | 39 | 26.5 | 11 | 18.6 | |
| Impaired ADL and IADL | 313 | 36.4 | 196 | 30.0 | 75 | 51.0 | 42 | 71.2 | |
| Cognitive impairment (n = 843) | 538 | 63.8 | 389 | 60.3 | 106 | 73.6 | 43 | 79.6 | 0.0001 |
| Mood impairment (n = 845) | 391 | 46.3 | 270 | 41.7 | 89 | 60.8 | 34 | 61.8 | 0.0001 |
| Handgrip Strength 1 (n = 841) | 371 | 44.1 | 242 | 37.5 | 89 | 63.6 | 40 | 71.4 | 0.0001 |
| Mobility impairment (n = 862) | |||||||||
| TUG (>20 s) (n = 824) | 345 | 41.9 | 234 | 37.3 | 72 | 51.4 | 39 | 69.6 | 0.0001 |
| OLBT (<5 s) (n = 766) | 504 | 65.8 | 373 | 63.1 | 86 | 69.4 | 45 | 88.2 | 0.001 |
| Gait speed (<0.8 m/s) (n = 762) | 390 | 51.2 | 299 | 49.9 | 58 | 49.6 | 33 | 71.7 | 0.016 |
| Falls 2 (n = 862) | 155 | 18.0 | 108 | 16.4 | 31 | 21.1 | 16 | 27.6 | 0.059 |
| Malnutrition 3 (n = 863) | 290 | 33.6 | 155 | 23.6 | 87 | 59.2 | 48 | 81.4 | 0.0001 |
| MNA (<17/30) | 119 | 14.4 | 62 | 9.8 | 40 | 28.8 | 17 | 30.9 | 0.0001 |
| BMI (<21) (n = 860) | 165 | 19.1 | 100 | 15.2 | 46 | 31.5 | 19 | 32.8 | 0.0001 |
| Albumin (<35 g/L) (n = 855) | 129 | 15.1 | 42 | 6.4 | 46 | 31.7 | 41 | 70.7 | 0.0001 |
| Polypharmacy 4 (n = 862) | 557 | 64.6 | 399 | 60.8 | 114 | 77.6 | 44 | 74.6 | 0.0001 |
| Severe comorbidities 5 (n = 862) | 466 | 39.9 | 344 | 52.4 | 90 | 61.2 | 32 | 54.2 | 0.156 |
| Anemia 6 (n = 860) | 546 | 63.5 | 380 | 58.1 | 114 | 77.6 | 52 | 63.5 | 0.0001 |
| Thrombocytopenia 7 (n = 858) | 86 | 10.0 | 69 | 10.6 | 10 | 6.8 | 7 | 10.0 | 0.343 |
| B12 8 | |||||||||
| Normal | 697 | 80.8 | 552 | 84.0 | 113 | 76.9 | 32 | 54.2 | 0.0001 |
| Hypo | 38 | 5.8 | 38 | 5.8 | - | - | - | - | |
| Hyper | 128 | 14.8 | 67 | 10.2 | 34 | 23.1 | 27 | 45.8 | |
| CRP (>5 mg/L) | 464 | 53.8 | 258 | 39.3 | 147 | 100 | 59 | 100 | 0.0001 |
| Lymphopenia 9 (n = 853) | 337 | 39.0 | 238 | 36.5 | 66 | 46.5 | 33 | 55.9 | 0.002 |
| Severe renal deficiency 10 (n = 863) | 107 | 12.4 | 66 | 10.0 | 31 | 21.1 | 10 | 16.9 | 0.001 |
| Variables | 10,000 < BCI ≤ 40,000 (n = 147) | BCI > 40,000 (n = 59) | ||||
|---|---|---|---|---|---|---|
| aOR | CI95% | p-Value | aOR | CI95% | p-Value | |
| MODEL A (n = 853) | ||||||
| Gender | ||||||
| Women | 1 | 1 | ||||
| Men | 1.950 | [1.30–2.93] | 0.001 | 1.843 | [1.02–3.34] | 0.043 |
| Age (years) | ||||||
| 70–74 | 1 | 1 | ||||
| 75–79 | 1.901 | [1.01–3.56] | 0.045 | 0.973 | [0.41–2.29] | 0.973 |
| 80–84 | 1.324 | [0.71–2.49] | 0.382 | 0.963 | [0.43–2.15] | 0.927 |
| ≥85 | 1.051 | [0.55–2.00] | 0.881 | 0.310 | [0.12–0.79] | 0.014 |
| Stage | ||||||
| I–III | 1 | 1 | ||||
| IV | 2.452 | [1.68–3.59] | 0.0001 | 2.509 | [1.41–2.29] | 0.002 |
| Autonomy | ||||||
| Unimpaired ADL-IADL | 1 | 1 | ||||
| Impaired ADL or IADL | 2.509 | [1.41–4.48] | 0.005 | 3.343 | [1.20–9.29] | 0.021 |
| Impaired ADL and IADL | 4.069 | [2.50–6.63] | 0.0001 | 14.375 | [5.80–35.66] | 0.0001 |
| MODEL B (n = 853) | ||||||
| Gender | ||||||
| Women | 1 | 1 | ||||
| Men | 1.9000 | [1.26–2.87] | 0.002 | 1.659 | [0.92–3.00] | 0.094 |
| Age (years) | ||||||
| 70–74 | 1 | 1 | ||||
| 75–79 | 2.027 | [1.06–3.86] | 0.032 | 1.094 | [0.46–2.63] | 0.840 |
| 80–84 | 1.492 | [0.79–2.83] | 0.222 | 1.196 | [0.53–2.71] | 0.668 |
| ≥85 | 1.455 | [0.76–2.79] | 0.258 | 0.550 | [0.21–1.41] | 0.212 |
| Stage | ||||||
| I–III | 1 | 1 | ||||
| IV | 2.226 | [1.51–3.29] | 0.0001 | 2.275 | [1.26–4.10] | 0.006 |
| Malnutrition | ||||||
| No | 1 | 1 | ||||
| Yes | 4.969 | [3.3–7.37] | 0.0001 | 14.348 | [7.16–28.74] | 0.0001 |
| MODEL C (n = 853) | ||||||
| Gender | ||||||
| Women | 1 | 1 | ||||
| Men | 1.892 | [1.21–2.97] | 0.006 | 1.914 | [0.97–3.76] | 0.060 |
| Age (years) | ||||||
| 70–74 | 1 | 1 | ||||
| 75–79 | 1.476 | [0.77–2.84] | 0.244 | 0.779 | [0.32–1.92] | 0.588 |
| 80–84 | 1.359 | [0.71–2.59] | 0.351 | 0.915 | [0.40–2.12] | 0.915 |
| ≥85 | 1.266 | [0.65–2.48] | 0.492 | 0.487 | [0.18–1.29] | 0.149 |
| Stage | ||||||
| I–III | 1 | 1 | ||||
| IV | 2.738 | [1.81–4.14] | 0.0001 | 2.369 | [1.26–4.44] | 0.007 |
| Gait speed (<0.8 m/s) | ||||||
| No | 1 | 1 | ||||
| Yes | 1.027 | [0.68–1.56] | 0.889 | 2.762 | [1.40–5.45] | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montegut, C.; Correard, F.; Nouguerède, E.; Rey, D.; Chevalier, T.; Meurer, M.; Deville, J.-L.; Baciuchka, M.; Pradel, V.; Greillier, L.; et al. Prognostic Value of the B12/CRP Index in Older Systemically Treatable Cancer Patients. Cancers 2022, 14, 169. https://doi.org/10.3390/cancers14010169
Montegut C, Correard F, Nouguerède E, Rey D, Chevalier T, Meurer M, Deville J-L, Baciuchka M, Pradel V, Greillier L, et al. Prognostic Value of the B12/CRP Index in Older Systemically Treatable Cancer Patients. Cancers. 2022; 14(1):169. https://doi.org/10.3390/cancers14010169
Chicago/Turabian StyleMontegut, Coline, Florian Correard, Emilie Nouguerède, Dominique Rey, Thomas Chevalier, Marie Meurer, Jean-Laurent Deville, Marjorie Baciuchka, Vincent Pradel, Laurent Greillier, and et al. 2022. "Prognostic Value of the B12/CRP Index in Older Systemically Treatable Cancer Patients" Cancers 14, no. 1: 169. https://doi.org/10.3390/cancers14010169